ihi high impact leadership framework - case...
TRANSCRIPT

Executive Quality Academy
Institute for Healthcare Improvement
IHI High Impact Leadership Framework Barbara Balik EdD, RN
[email protected] 16, 2015
ACMA Leadership
Conference
Learning Objectives
Describe IHI’s High Impact Leadership Framework and its
three major components
Explain how High Impact Leadership can enable leaders to
achieve the Triple Aim – better health, better care, lower costs
Define strategies for applying the High Impact Leadership
Framework to your department, organization, and community
Field of Dreams

Executive Quality Academy
Institute for Healthcare Improvement

Executive Quality Academy
Institute for Healthcare Improvement
What You Know
Two Questions
Why did you get into
healthcare?
Why have you stayed?
The Heart of Leadership, Balik & Gilbert
© 2010 Balik and Gilbert All Rights Reserved
Think of a Leader
A leader who influenced How you describe them
A leader who made a
positive difference
One you learned great
positive lessons from
A leader who helped you
grow
Think of a phrase or a few
words that describes them
The Heart of Leadership, Balik & Gilbert
© 2010 Balik and Gilbert All Rights Reserved

Executive Quality Academy
Institute for Healthcare Improvement
Triple Aim
Care better than we’ve ever seen, health
better than we’ve ever known, at a cost
we can all afford
Leading Improvement and Innovation
“Every system is perfectly designed to
produce the results it gets.”
Dr. Paul Batalden
11
As leaders you own the results
IHI High-Impact Leadership for Improvement and
Innovation
An update on IHI thinking
– What is required for improvement and innovation today
Guide
– For leaders at all levels to achieve Triple Aim results for
the populations that they serve
– IHI White Paper
– http://www.ihi.org/resources/Pages/IHIWhitePapers/HighImpactL
eadership.aspx

Executive Quality Academy
Institute for Healthcare Improvement
There is no cookie cutter (or magic carpet!) approach
– Framework is designed to help identify where leaders should focus efforts, resources and tactics
– Agnostic to popular personal leadership theories
– Leaders have to adapt to their specific organizational culture, capabilities, and challenges
Leading Improvement
A useful definition…
Leadership is a process of social influence, which
maximizes the efforts of others, towards the
achievement of a goal
Kevin Kruse Forbes.com What is Leadership April 9, 2013
Kevin Kruse
Swensen S, Pugh M, McMullan C, Kabcenell A. High-Impact Leadership: Improve Care, Improve the Health of Populations, and Reduce
Costs. Cambridge, MA: Institute for Healthcare Improvement; 2013. Available on www.ihi.org.
High-Impact Leadership:Care better than we’ve ever seen, health better than we’ve ever known, at a cost we
can all afford

Executive Quality Academy
Institute for Healthcare Improvement
Swensen S, Pugh M, McMullan C, Kabcenell A. High-Impact Leadership: Improve Care, Improve the Health of Populations, and Reduce
Costs. Cambridge, MA: Institute for Healthcare Improvement; 2013. Available on www.ihi.org.
IHI High-Impact Leadership FrameworkWhere Leaders Focus Efforts
High-Impact Leadership BehaviorsWhat Leaders Do to Make a Difference
Swensen S, Pugh M, McMullan C, Kabcenell A. High-Impact Leadership: Improve Care, Improve the Health of Populations, and Reduce
Costs. Cambridge, MA: Institute for Healthcare Improvement; 2013. Available on www.ihi.org.
Mental Models
Here is Edward Bear, coming downstairs now, bump, bump,
bump, on the back of his head, behind Christopher Robin. It
is, as far as he knows, the only way of coming downstairs, but
sometimes he feels that there really is another way, if only he
could stop bumping for a moment and think of it.
Winnie-The-Pooh, A.A. Milne

Executive Quality Academy
Institute for Healthcare Improvement
Mental Models
How leaders think shapes behavior
– Beliefs, theories and assumptions provide a “lens” through
which leaders view and filter challenges and define the
universe of potential solutions and actions
Mental Models Evolve Over Time20
Improve Facilities
and & technology
Improve Customer Service
Improve the Patient
Experience
Patients & Families
Partners in Care
Physicians as
Customers
Physician Cooperation
Physician Engagement
Physicians as Leaders
Manage resources & inputs
Manage length of stay and access
Remove waste from processes
Redesign care
Meet accreditation requirements
Meet public reporting & compliance
requirements
Use Quality data for
improvement
Use Quality data for payment
Leadership
Issue
Patient
Satisfaction
Role of
Physicians
Reduce Cost
Performance
Measurement
10‘s80‘s 00‘s90‘s
Mental Models Evolve Over Time –
Case Managers
21
Manage length of
stay
Instructions for going
home
Doing For Patients
hospital to home
Partner with Patients across
continuum
Silos
UR Nurses/SW
Integrating within
departments
Expansion to Case
Management
Leaders in Triple Aim
Cut costs
Manage length of stay and access
Understand root of costs
Redesign care for
value
Meet insurance
requirements
Teaching, preparing for
discharge
Reduce readmissions
Improve patient
satisfaction
Triple Aim Outcomes
Leadership
Issue
Patient care role
Case Manager
Roles
Resource Mgmt
Performance
Measurement
10‘s80‘s 00‘s90‘s

Executive Quality Academy
Institute for Healthcare Improvement
Mental Models: Cost vs. Value
Clinical
Processes
Direct Inputs
•Supplies
•Labor
Measures
•Patient Experience
•Clinical
•Engagement
•Financial
•Value across
the continuumIndirect Inputs
•Structure
•Technology
Traditional
Strategy:
Control Inputs
Support
Processes
*waste = unintended
variation, rework, error,
valueless care, needless
complexity, etc.
Quality
Strategy:
Redesign and
Remove Waste*
Changing the Way We Think About Health Care
What’s the Matter?
What matters to you?
IHI High-Impact Leadership – Mental Models
Individuals and families as partners in their care
Compete on value with continuous reduction in
operating cost
Reorganize services to align
with new payment systems
Everyone is an improver

Executive Quality Academy
Institute for Healthcare Improvement
Swensen S, Pugh M, McMullan C, Kabcenell A. High-Impact Leadership: Improve Care, Improve the Health of Populations, and Reduce
Costs. Cambridge, MA: Institute for Healthcare Improvement; 2013. Available on www.ihi.org.
IHI High-Impact Leadership FrameworkWhere Leaders Focus Efforts
Swensen S, Pugh M, McMullan C, Kabcenell A. High-Impact Leadership: Improve Care, Improve the Health of Populations, and Reduce
Costs. Cambridge, MA: Institute for Healthcare Improvement; 2013. Available on www.ihi.org.
IHI High-Impact Leadership FrameworkWhere Leaders Focus Efforts

Executive Quality Academy
Institute for Healthcare Improvement
Leadership BehaviorsDriven by Persons and Community
• Communicate that we are always people
• “patient” is a temporary condition
• Nothing about me without me
• What if nothing was designed or improved for patients and community members without their being part of the process?
• Communicate why and model partnerships
• Spend time learning about health and healthcare from community members
– Social service agencies, community health, education, public safety, law enforcement
• Assure health literacy and shared decision making
Leadership BehaviorsDriven by Persons and Community
How leaders think about challenges and solutions
– Who leaders talk and think with – how define partners
– Where leaders get their ideas and who view as experts
– How leaders understand the lived experience of
patients and community members
– What data leaders use for decisions and its source
– The boundaries leaders eliminate to improve the health
of the community
– How leaders describe their work – their
accountabilities
When We are at Our Best . . .
This is how we demonstrate Driven by Person and
Community:

Executive Quality Academy
Institute for Healthcare Improvement
Current State
Large barrier to “Driven by Person and Community”
– We already think we are!
Deeply embedded belief (hubris?) that we – within
healthcare – are the experts vs. merged expertise:
– People are experts in their own health and lived experience
– Healthcare professionals as experts in content
Pervasive systems that reinforce those beliefs
– Dismissive treatment of patients
– Systemic disrespect – waiting; wasteful systems for everyone*
*Lucian L. Leape, MD, Miles F. Shore, MD, Jules L. Dienstag, MD, Robert J. Mayer, MD, Susan Edgman-Levitan, PA, Gregg S. Meyer, MD, MSc,
and Gerald B. Healy, MD. A Culture of Respect, Part 1: The Nature and Causes of Disrespectful Behavior by Physicians. Acad Med.
2012;87:845–852. A Culture of Respect, Part 2: The Nature and Causes of Disrespectful Behavior by Physicians. Acad Med. 2012;87:853–858.
Barbara Balik
What Patients and Families Want
Dignity and respect
Information sharing
Participation
Collaboration
Institute for Patient- and Family-Centered Care
Partnerships - Words Matter
Not ‘engagement’ – they already are
Experience is the whole deal – safety, quality, respect
To – For – With � Co-design
o “Nothing about me without me”
o Co-design care, systems, policies
o Change the balance of power*
*Don Berwick, Change from the Inside Out; JAMA 2015

Executive Quality Academy
Institute for Healthcare Improvement
Personal Characteristics
Passion for Patient Care is a Personal Value
1I do not know if others
know of my commitment to patient care
5Many know of my
commitment but not everyone; I lack
consistency in words/actions about
patient care as a personal value
10My passion for patient
care shows up in everything I do; my
colleagues would say my actions demonstrate it
How will I find out?
© 2010 Barbara Balik and Jack Gilbert . All Rights Reserved
The Heart of Leadership, Balik & Gilbert
© 2010 Balik and Gilbert All Rights Reserved
Leadership Behaviors
Disciplined Action
Meeting Questions – How many times?Executive Team
Sample Questions “How does this strategy/tactic improve patient care?”
“How does this reduce variation in care?”
“What patients developed complications in the past 24 hours? What
have we learned from that?”
“What patients or community members have we asked about this?”
“What value does this add to patient care and patient experience?”
“What patients/family members or community members do we have
on teams?”
“What other organizations are helping us with this strategy?”
© 2010 Barbara Balik and Jack Gilbert . All Rights Reserved
The Heart of Leadership, Balik & Gilbert
© 2010 Balik and Gilbert All Rights Reserved
Shape Culture
Engage Across Boundaries
Create Vision & Build Will
Deliver ResultsDevelop
Capability
Driven by
Persons &
Community
IHI High-Impact Leadership Framework

Executive Quality Academy
Institute for Healthcare Improvement
Culture
What is it?
– The total learned, shared, taken-for-granted
assumptions that a group has learned throughout
its history; base of daily behavior
– Deep, broad, stable– Schien, Corporate Culture Survival Guide, 1999
– Seen in behavior
– Changed over time by working on behaviors that
eventually shift mental models
How Culture is Embedded
Primary• What leaders do, pay attention to,
measure and reward on a
regular basis
• How leaders react to critical incidents and organizational crises
• Deliberate role modeling, teaching and coaching
• Observed criteria by which leaders allocate rewards and status
• Observed criteria by which leaders recruit, select, promote, and terminate organizational members
Secondary• Organizational design and
structure
• Organizational systems and procedures
• Organizational rites and rituals
• Design of physical space and buildings
• Stories, legends and myths about people and events
• Formal statements of organizational philosophy, values and creed
E. Schein, Organizational Culture and Leadership,1994
Or This?This?

Executive Quality Academy
Institute for Healthcare Improvement
Culture - What is it?
Finish the statement:
– This is an organization where . . .
What Culture do You Want?
Current State Desired State
Where are you in the Journey?

Executive Quality Academy
Institute for Healthcare Improvement
Doing To – When:
We say – you do: schedules; visiting hours
We waste your time – come to the clinic & wait
We assume we know what the community needs
Information is not shared or understandable
Health sciences students lack skills to partner with patients
Participation in research studies is not equitable
We determine if you are compliant
There is helplessness – when the patient/family say:– I don’t know what is the plan of care or what happens next
– I don’t know who is in charge of my care
– I don’t feel like you know me
Barbara Balik
Doing For – When:
We keep the patient or community member in mind when designing or improving programs, research studies – then ask
We design the teams to help you – without you
We manage your expectations about waiting, what healthcare can do, or what the community needs
Early use of health literacy
We teach you – lots & lots & lots
We are beginning to get it about cross-continuum but don’t know much about the white spaces
We assume we know everything about health and healthcare
Barbara Balik
Doing For – Service Design
What Matters to You?

Executive Quality Academy
Institute for Healthcare Improvement
Doing For
“We are really good
about caring what you
think about us. We are
not good about caring
what you think.”– Catherine Lee, VP Service Excellence, McLeod
Regional Medical Center
Barbara Balik
Doing With – When:
Patient/family and community member advisors are essential team members to design or improve programs that follow the patient journey; to design research or evaluation outcomes
All key decisions are mutual – including who is on my team
All staff are viewed as caregivers and are skilled in respectful communication and teamwork
Health Literacy is everywhere in patient care
Senior leaders model that patient’s safety and community well-being guide all decisions
Staff, providers, leaders are recruited for values and talent
Barbara Balik
Doing With – Mental Health Design

Executive Quality Academy
Institute for Healthcare Improvement
Where are you in doing to-for-with?
To-For-With Assessment
1. Individually – Complete 1-2 examples in each category
2. Review as a group at your table
3. What do your lists tell you? What gets in the way of doing with?
Doing To – Patients, Families, Community Members
Doing For – Patients, Families, Community Members
Doing With – Patients, Families, Community Members
Barbara Balik
Shape Culture
Engage Across Boundaries
Create Vision & Build Will
Deliver ResultsDevelop
Capability
Driven by
Persons &
Community
IHI High-Impact Leadership Framework
Executive Quality Academy
Institute for Healthcare Improvement
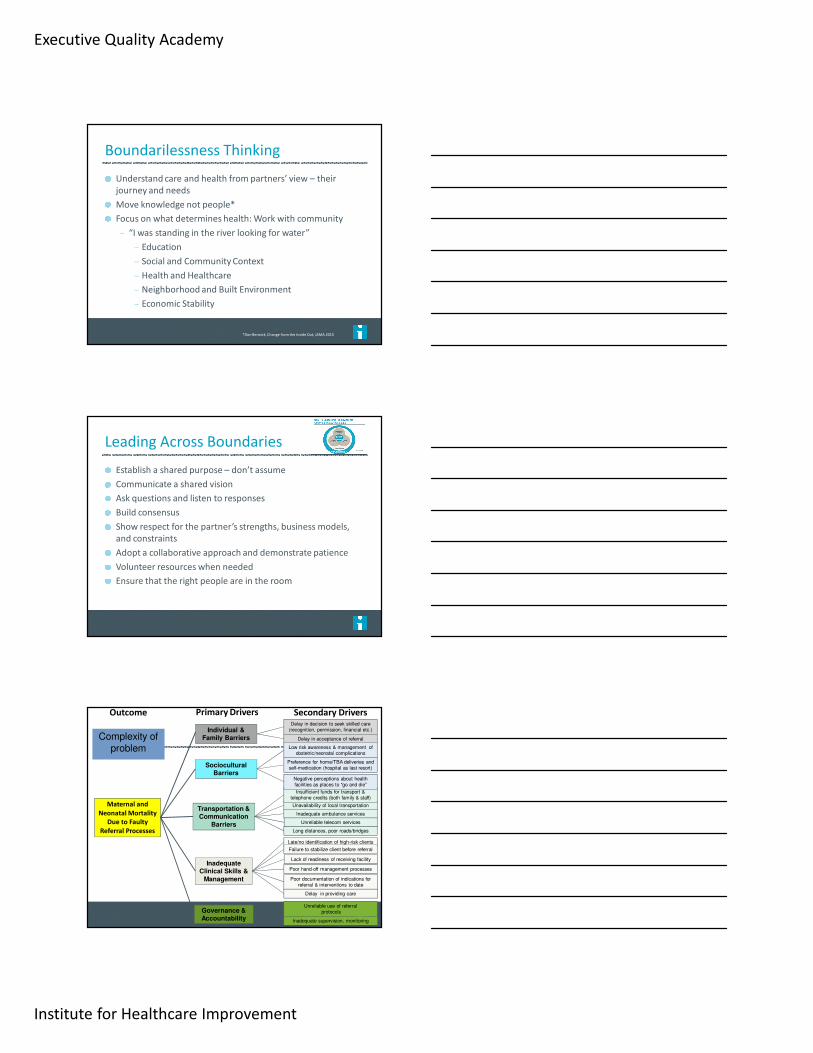
Understand care and health from partners’ view – their
journey and needs
Move knowledge not people*
Focus on what determines health: Work with community
– “I was standing in the river looking for water”
– Education
– Social and Community Context
– Health and Healthcare
– Neighborhood and Built Environment
– Economic Stability
Boundarilessness Thinking
*Don Berwick, Change from the Inside Out; JAMA 2015
Leading Across Boundaries
Establish a shared purpose – don’t assume
Communicate a shared vision
Ask questions and listen to responses
Build consensus
Show respect for the partner’s strengths, business models,
and constraints
Adopt a collaborative approach and demonstrate patience
Volunteer resources when needed
Ensure that the right people are in the room
Maternal and
Neonatal Mortality
Due to Faulty
Referral Processes
Inadequate Clinical Skills &
Management
Transportation & Communication
Barriers
Sociocultural Barriers
Late/no identification of high-risk clients
Failure to stabilize client before referral
Poor documentation of indications for referral & interventions to date
Lack of readiness of receiving facility
Poor hand-off management processes
Unreliable use of referralprotocols
Unavailability of local transportation
Insufficient funds for transport & telephone credits (both family & staff)
Long distances, poor roads/bridges
Inadequate ambulance services
Unreliable telecom services
Preference for home/TBA deliveries and self-medication (hospital as last resort)
Delay in decision to seek skilled care (recognition, permission, financial etc.)
Delay in acceptance of referral
Low risk awareness & management of obstetric/neonatal complications
Negative perceptions about health facilities as places to “go and die”
Primary Drivers Secondary DriversOutcome
Delay in providing care
Governance & Accountability Inadequate supervision, monitoring
Individual & Family BarriersComplexity of
problem

Executive Quality Academy
Institute for Healthcare Improvement
• Be consistently person-centered in word and deed.
• Be consistently person-centered in word and deed.
Person-centeredness
• Be a regular, authentic presence at the frontline and a visible champion of improvement.
• Be a regular, authentic presence at the frontline and a visible champion of improvement.
Frontline Engagement
• Remain focused on the vision and strategy.
• Remain focused on the vision and strategy.Relentless Focus
• Require transparency about results, progress, aims, and defects.
• Require transparency about results, progress, aims, and defects.Transparency
• Encourage and practice system-thinking and collaboration across boundaries.
• Encourage and practice system-thinking and collaboration across boundaries.Boundarilessness
High-Impact Behaviors
Swensen S, Pugh M, McMullan C, Kabcenell A. High-Impact Leadership: Improve Care, Improve the Health of Populations, and Reduce
Costs. Cambridge, MA: Institute for Healthcare Improvement; 2013. Available on www.ihi.org.
Team Engagement
Can each person answer yes each day?
– Am I treated with dignity and respect by
everyone?
– Do I have what I need so I can make a contribution
that gives meaning to my life?
– Am I recognized and thanked for what I do?
Through the Eyes of the Workforce: Creating Joy, Meaning, and Safer Health Care. 2013. Lucian Leape institute of the National Patient Safety
Foundation; NPSF.org
Another View – Engaging Others
Choice/Respect
Mastery
Purpose
Barbara Balik; Modified from D. Pink, Drive

Executive Quality Academy
Institute for Healthcare Improvement
What are Vital Few Behaviors?
Those few behaviors that:
─ Move rapidly toward the desired outcome
─ Are teachable, coachable, observable
Often in evidence already:
─ E.g. To help low achieving children read: more praise than
punishment; constantly alternate teaching and questioningFrom: Patterson et al. Influencer: The Power to Change Anything (2007)
Heart of LeadershipWhat We Learned from Transformational
Leaders
Words and actions matchAuthenticityHumility
Passion for patient care isa personal value
IntelligentHungry for LearningReflective
Personal Characteristics
Organizational Characteristics
Grow others
Positive future orientationAims highChallenges status quo
Transformational Results through a Single-Brain Organization
Patient care constancy of focus
Disciplined actionPart of the team,part of the solution Genuinely care
about and trust others
Engage everyone
The Heart of Leadership, Balik & Gilbert
© 2010 Balik and Gilbert All Rights Reserved

Executive Quality Academy
Institute for Healthcare Improvement
The patient matters most to her
He is unwavering about the mission; he has a constancy of purpose
She has a strong sense of integrity of what’
’’
’s right for patients---she lives and breathes it
Personal Characteristics
Passion for Patient
Care is a Personal
Value
The Heart of Leadership, Balik & Gilbert© 2010 Balik and Gilbert All Rights Reserved
She is not distracted by the crisis of the day; she doesn’
’’
’t jump around or vacillateOur strategic plan is alive and well: What is best for the patient? What will make a perfect experience for the patient?
Organizational Characteristics
Patient Care
Constancy of Focus
Disciplined Action
The Heart of Leadership, Balik & Gilbert
© 2010 Balik and Gilbert All Rights Reserved
Enough
I pray you enough sun to keep your attitude bright no matter how gray the day may appear
I pray you enough rain to appreciate the sun even more
I pray you enough happiness to keep your spirit alive and everlasting
I pray you enough gain to satisfy your wanting
I pray you enough challenges to think
outrageously big!

Executive Quality Academy
Institute for Healthcare Improvement
Resources
ResourcesNew Rules for Radical Redesign in Health Care
Change the balance of power by co-producing health and well-being in partnership with patients,
families and communities.
Standardize what makes sense to reduce unnecessary variation and increase the time available for
individualized care.
Customize to the individual's needs, values and preferences, guided by the understanding of what
matters to the person, in addition to the typical "What's the matter?”
Promote well-being and focus on outcomes that matter the most to people, appreciating that their
health and happiness may not require health care.
Create joy in work by cultivating and mobilizing the pride and happiness of the health care workforce.
Make it easy, continually reducing waste and all non-value-added requirements and activities for
patients, families and clinicians.
Move knowledge, not people, exploiting all helpful capacities of modern digital care and continually
substituting better alternatives for visits and institutional stays.
Collaborate and cooperate, recognizing that the health care system is embedded in a network that
extends beyond traditional walls.
Assume abundance by using all the assets that can help to optimize the social, economic and physical
environment, especially those brought by patients, families and communities.
Return the money from health care savings to other public and private purposes.
Berwick, D., et al. Change From the Inside Out: Health Care Leaders Taking the Helm, 3/26/2015
http://jama.jamanetwork.com
Balik, B., Gilbert, J. (2010). The Heart of Leadership: Inspiration and Practical Guidance for Transforming Your Health Care Organization. Chicago: AHA Press.
Balik B, Conway J, Zipperer L, Watson J. The Patient and Family Experience. IHI Innovation Series white paper. Cambridge, Massachusetts: Institute for Healthcare Improvement; 2011.
Braaten, J, Bellhouse, D. Improving Patient Care by Making Small Sustainable Changes. Nursing Economics, May-June 2007, Vol 25, No. 3, 162-66.
Collins, J. (2009). How the Mighty Fall. NY: Harper Collins
Collins, J. (2001). Good to Great, NY: Harper Business.
Collins, J. (2005). Good to Great & the Social Sectors: A Monograph to Accompany Good to Great. Boulder, CO: www.jimcollins.com
Duhigg, C. (2012). The Power of Habit: Why We Do What We Do in Life and Business. NY: Random House.
Edmondson, A. (2012). Teaming: How Organizations Learn, Innovate, and Compete in the Knowledge Economy. San Francisco: Jossey-Bass.
Gilbert, J. (2007). Strengthening the Ethical Wisdom: Tools for Transforming Your Healthcare Organization. Chicago: Health Forum
Resources
Barbara Balik

Executive Quality Academy
Institute for Healthcare Improvement
Resources
Heath, C. & D. (2010). Switch: How to Change Things When Change is Hard. NY: Random House.
Heifetz, R. (1994). Leadership Without Easy Answers. Cambridge, MA: Belknap Press.
Heifetz, R., Grashow, A., Linsky, M. (2009). The Practice of Adaptive Leadership. Boston: Harvard Business Press.
Kenagy, J. (2009). Designed to Adapt. Second River Publishing.
Kouzes, J., Posner, B. (2002). The Leadership Challenge. San Francisco: Jossey-Bass.
Kouzes, J., Posner, B. (2003). Encouraging the Heart: A Leader’s Guide to Rewarding & Recognizing Others. San Francisco: Jossey-Bass.
Krause, T. (2007). NASA after Columbia & Lessons for Healthcare. National Patient Safety Board of Governors presentation. June 2007.
Keroack, M., Youngbird, B., Cerese, J., Krsek, C., Prellwitz, L., Trevelyan, E. Organizational factors associated with high performance in quality & safety in academic medical centers. Academic Medicine 82: 1178-1186, December 2007
Barbara Balik
ResourcesMoss Kanter, R. (2004). Confidence: How Winning Streaks & Losing Streaks Begin & End. NY: Crown Business.
Patterson, et al., (2008). Influencer. New York: McGraw-Hill.
Pink, D. (2009). Drive: Surprising Truth About What Motivates Us. NY: Riverhead Books.
Rother, M. (2010). Toyota Kata: Managing People for Improvement, Adaptiveness, and Superior Results. NY: McGraw Hill.
Schein, E. (1999). The Corporate Culture Survival Guide: Sense & Nonsense About Cultural Change. San Francisco: Jossey-Bass.
Schein, E. (2004). Organizational Culture & Leadership, 3rd Edition. San Francisco: Jossey-Bass.
Senge, P., Kleiner, A., Roberts, C., Ross, R., Roth, G., Smith, B., (1999). The Dance of Change: The Challenges of Sustaining Momentum in Learning Organizations. New York: Doubleday.
Spear, S. (2010). The High Velocity Edge. New York: McGraw Hill.
Barbara Balik
Resources
Spear, S., Bowen, HK. Decoding the DNA of the Toyota Production System. Harvard Business Review, Sept-Oct 1999; 77; 99-106.
Spear, S. Learning to Lead at Toyota. Harvard Business Review, May 2004; 78-86.
Spear, S. Fixing Health Care from the Inside, Today. Harvard Business Review, Sept 2005; 78-91.
Spear, S., Schmidhofer, M. Ambiguity & Workarounds as Contributors to Medical Error. Annals of Internal Medicine, April, 19, 2005, Vol. 142, No. 8, 627-630.
Tucker, A. & Edmondson, A. Why Hospitals Don’t Learn from Failures: Organizational & Psychological Dynamics that Inhibit System Change. California Management Review, Vol. 45. No 2, Winter 2003, 55-72.
Weick, K., Sutcliffe, K. (2001). Managing the Unexpected: Assuring High Performance in an Age of Complexity. San Francisco: Jossey-Bass.
Barbara Balik

Executive Quality Academy
Institute for Healthcare Improvement
Heart of LeadershipAdditional resources
Four Personal Characteristics
Patient care is my North Star
My actions show commitment to that North Star
Words and Actions Match;
Authenticity; Humility
Words and Actions Match;
Authenticity; Humility
Care about and Trust OthersCare about and Trust Others
Passion for Care is a Personal ValuePassion for Care is a Personal Value
Intelligent; Hungry for
Learning;Reflective
Intelligent; Hungry for
Learning;Reflective
Others can count on what I say
Others at all levels say I build trustI do not consider myself superior to anyone
I am comfortable not knowing
I am hungry to learn from anyone and anythingI regularly step back from everyday pressures
I genuinely care about the welfare of others
I trust others unless given good reason not to
© 2010 Barbara Balik and Jack Gilbert . All Rights Reserved
The Heart of Leadership, Balik & Gilbert© 2010 Balik and Gilbert All Rights Reserved
Five Organizational Characteristics
•I have a bold aspiration not easily attained•I am always challenging others to reach for “the next best”
Patient Care Constancy;
Disciplined Action
Patient Care Constancy;
Disciplined Action
Part of the Team and the SolutionPart of the Team and the Solution
Grow OthersGrow Others
Positive Future Orientation;
Aims High; Challenges Status
Quo
Positive Future Orientation;
Aims High; Challenges Status
Quo
Engage EveryoneEngage Everyone
•I have an unrelenting and primary focus on the safety and quality of care
•I am known for developing disciplined processes
•I make sure everyone in our organization has a voice•I reach out regularly to engage others at all levels
•I don’t make significant decisions alone•I seek diverse views to reach the best solutions
•I often see talents in others before they do•Helping others realize their potential is thrilling for me
© 2010 Barbara Balik and Jack Gilbert . All Rights Reserved
The Heart of Leadership, Balik & Gilbert© 2010 Balik and Gilbert All Rights Reserved

Executive Quality Academy
Institute for Healthcare Improvement
Organizational CharacteristicsPatient Care Constancy of Focus -Disciplined Action
Capacity Description
Our Performance Improvement (PI) system is ………
The expectations of all leaders to demonstrate PI competency is …
Percent of leaders who can successfully guide complex PI activities is …
How do I demonstrate PI skills in my work?
© 2010 Barbara Balik and Jack Gilbert . All Rights Reserved
The Heart of Leadership, Balik & Gilbert© 2010 Balik and Gilbert All Rights Reserved
Words and actions matchAuthenticityHumility
Passion for patient care isa personal value
IntelligentHungry for LearningReflective
Personal Characteristics
Organizational Characteristics
Grow others
Positive future orientationAims highChallenges status quo
Transformational Results through a Single-Brain Organization
Patient care constancy of focus
Disciplined actionPart of the team,part of the solution Genuinely care
about and trust others
Engage everyone
The Heart of Leadership, Balik & Gilbert© 2010 Balik and Gilbert All Rights Reserved
There’’’
’s a “““
“thereness”””
”
when she’’’
’s with others. She will swivel her chair, move in, and doesn’
’’
’t look at her computer while listeningHe has a desire to be with and around people to hear what is important to them, what they need
Personal Characteristics
Genuinely Care
About and Trust
Others
The Heart of Leadership, Balik & Gilbert© 2010 Balik and Gilbert All Rights Reserved

Executive Quality Academy
Institute for Healthcare Improvement
Personal Characteristics
Genuinely Care About & Trust Others
Describe when have you experienced this from
another leader?
What do you do daily to demonstrate this?
Encourage the Heart reflections:I express high expectations about what people are capable of accomplishingI personally acknowledge people for their accomplishmentsI get to know, at a personal level, the people I work with
© 2010 Barbara Balik and Jack Gilbert . All Rights Reserved
The Heart of Leadership, Balik & Gilbert© 2010 Balik and Gilbert All Rights Reserved
Organizational Characteristics
She finds out what is good in people, exposes it, grows it, and helps you master it in pursuit of the group goal.
She hired me with no hospital operations experience… She said she was looking for leadership skills and that operations could be taught.
Grow Others
© 2010 Barbara Balik and Jack Gilbert All Rights Reserved
The Heart of Leadership, Balik & Gilbert© 2010 Balik and Gilbert All Rights Reserved
Organizational Characteristics
Grow OthersThe people I am currently mentoring:
I am clear on the successor(s) for my position
Yes: Who?:
Why them?:
I am growing this person’s skills to move into the position –
list:
No:
Who is someone I might identify
An example of when I hired non-traditional people when
filling positions is …
© 2010 Barbara Balik and Jack Gilbert . All Rights Reserved
The Heart of Leadership, Balik & Gilbert© 2010 Balik and Gilbert All Rights Reserved