iga nephropathy and psoriatic arthritis that improved with
TRANSCRIPT
1085
□ CASE REPORT □
IgA Nephropathy and Psoriatic Arthritis that Improvedwith Steroid Pulse Therapy and Mizoribine in Combinationwith Treatment for Chronic Tonsillitis and Epipharyngitis
Tomohiro Kaneko 1, Akiko Mii 1, Megumi Fukui 1, Kiyotaka Nagahama 2,
Akira Shimizu 2 and Shuichi Tsuruoka 1
Abstract
A 65-year-old man was admitted to our hospital with edema and renal dysfunction. He had received a di-
agnosis of psoriatic arthritis at 50 years of age. As a renal biopsy showed IgA nephropathy (IgAN), bilateral
tonsillectomy was performed, and one course of steroid pulse therapy with an oral steroid and mizoribine
were subsequently administered. The patient’s proteinuria gradually reduced in association with an improve-
ment in the renal function. In addition, the rash and arthralgia were ameliorated. In this case, adding treat-
ment for chronic epipharyngitis accelerated the curative effects, and focal infection therapy consisting of im-
munosuppressive drugs was effective for both IgAN and psoriatic arthritis.
Key words: IgA nephropathy, psoriatic arthritis, focal infection treatment
(Intern Med 54: 1085-1090, 2015)(DOI: 10.2169/internalmedicine.54.3510)
Introduction
It has been reported that the administration of steroid
pulse therapy after bilateral tonsillectomy is effective in
cases of IgA nephropathy (IgAN). The palatine tonsils are a
central component of the nasopharynx-associated lymphoid
tissue (NALT), which forms part of Waldeyer’s tonsillar
ring. These tonsils take in antigens invading from the oral
and nasal cavities and subsequently form antibodies. It has
also been demonstrated that the number of IgA plasma cells
is increased in the palatine tonsils in IgAN patients and that
IgA1-positive cells are present among the dendritic cells of
the tonsillar follicles. In addition, there are many reports
suggesting the presence of quantitative and qualitative ab-
normalities in Galβ1 and 3GalNAc in O-linked glycans in
hinge regions. O-glycosylation abnormalities are of particu-
lar interest as a principal cause of IgAN (1).
Focal infection is a clinical state in which chronic local-
ized inflammation in one part of the body causes reactive
organic or functional disabilities in distal locations. The
most frequent site of origin is the tonsils. Typical diseases
caused by tonsillar focal infection include orthopedic disor-
ders, such as sternocostoclavicular hyperostosis and reactive
arthritis, and cutaneous diseases, such as palmoplantar pus-
tulosis and erythema nodosum, in addition to IgAN and pur-
pura nephritis. Psoriasis may also present with the exacerba-
tion of rashes due to infection of the upper respiratory tract
and tonsillitis. Furthermore, it has been widely reported that
tonsillectomy is effective for treating tonsillar focal dis-
eases (2).
Psoriatic arthritis is a form of chronic inflammatory ar-
thritis accompanying bone and cartilage lesions, which coex-
ist in 4-30% of psoriasis cases (3). In addition, deformation
or articular destruction are observed at five or more loca-
tions in 55% of patients whose articular symptoms devel-
oped more than 10 years previously. Such patients are
treated in accordance with guidelines for rheumatoid arthri-
tis, and the administration of a tumor necrosis factor-alpha
(TNF-α) inhibitor is often considered in intractable
cases (4).
We experienced a case of IgAN with coexisting psoriatic
1Division of Nephrology, Department of Internal Medicine, Nippon Medical School, Japan and 2Department of Analytic Human Pathology, Nip-
pon Medical School, Japan
Received for publication June 21, 2014; Accepted for publication September 15, 2014
Correspondence to Dr. Tomohiro Kaneko, [email protected]
Intern Med 54: 1085-1090, 2015 DOI: 10.2169/internalmedicine.54.3510
1086
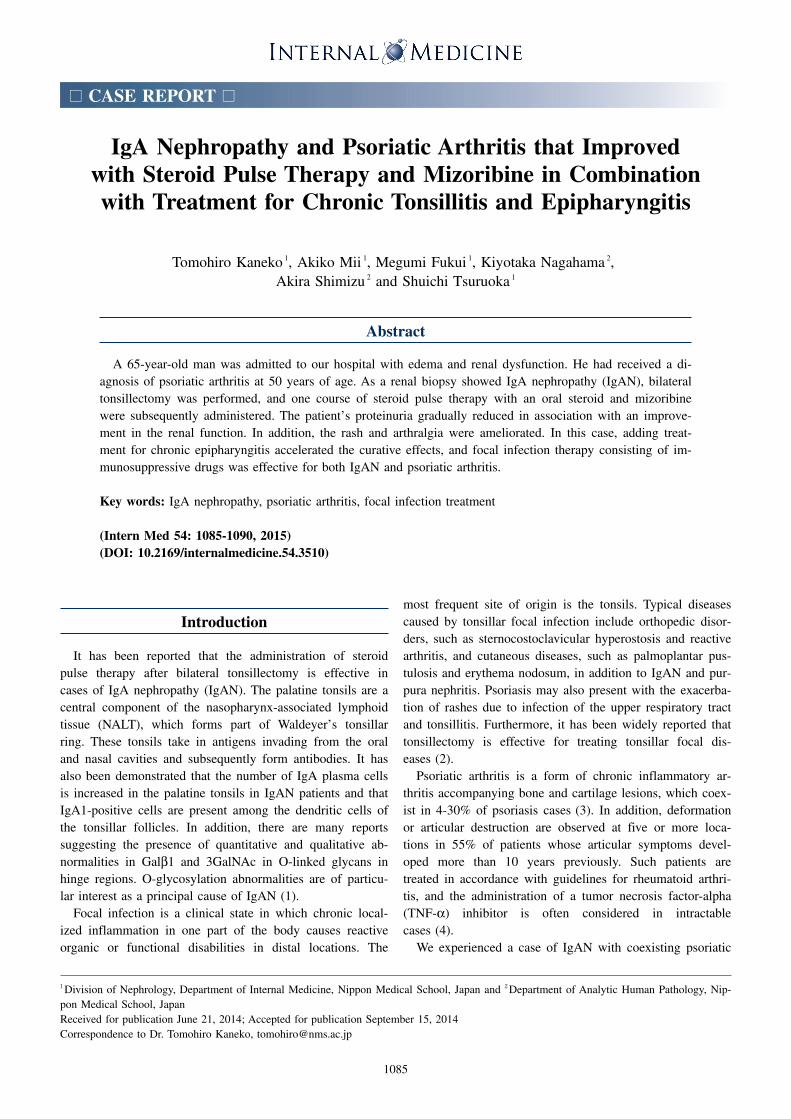
Figure 1. Appearance of the skin before and 18 months after tonsillectomy. a: Carnation maculae with a scale attached margin were observed across the patient’s entire body before tonsillectomy. b: The rash nearly disappeared 18 months after tonsillectomy.
a
b
Table. Laboratory Data at Admission
Peripheral blood Serological testWBC 5, IgG 1,321 mg/d RBC 397 × 104 IgA 648 mg/Hb 1 IgM 94 mg/Hct 35.5 % CH50 > 60 U/mPlt 25.7 × 104/ C3 147 mg/
Blood chemistry C4 44 mg/TP RF 3 IU/mAlb 3.6 g/d ACPA 0.4 U/mAST 22 IU/ ANA < 40A T 18 IU/ MPO-ANCA < 10 EU
H 205 IU/ PR3-ANCA < 10 EUT-Cho 189 mg/ HBs-ag negative
-Cho 111 mg/ HCV-ab negativeTG 155 mg/ T A negativeUA 7.2 mg/ Urinalysis BUN 31.3 mg/ Gravity 1.018Cre 1.83 mg/ pH 5.5Na 137 mEq/K 4.2 mEq/Cl 105 mEq/ (3+)Ca 8.7 mg/ Glucose (-)Pi 3.2 mg/ Ketone (-)CRP 0.67 mg/dHbA1c(NGSP) 6.1%
Protein 3+2.8 g/day
Occult blood
arthritis in which we performed tonsillectomy and adminis-
tered steroids and mizoribine (MZR) in addition to treatment
for the focal infection. Consequently, the patient’s rash, ar-
thralgia and renal function improved and the hematuria
completely disappeared.
Case Report
A 65-year-old man scheduled for a renal biopsy had been
visiting a local doctor for the treatment of psoriatic arthritis
since 50 years of age. The psoriatic arthritis was refractory
and had been treated with steroids, cyclosporin and vitamin
D ointment. The patient reported strong joint pain, and non-
steroidal anti-inflammatory drugs (NSAIDs) were used em-
pirically. In addition, he had been prescribed antihyperten-
sives (a calcium channel blocker and angiotensin II receptor
blocker) since 60 years of age. Bilateral edema in the lower
extremities was observed approximately one month prior to
the renal biopsy. A local doctor identified proteinuria and re-
nal function impairment, and the patient was therefore re-
ferred to our department for hospitalization. As shown in
Fig. 1a, carnation maculae with a scale attached margin
were observed across his entire body. Table shows the find-
ings of the laboratory workup performed on admission; ane-
mia and high blood IgA in addition to hematuria, protein-
uria and renal function impairment were observed. The renal
biopsy, performed the day after admission, showed almost
half (of a total of approximately 30) of the glomeruli to be
Intern Med 54: 1085-1090, 2015 DOI: 10.2169/internalmedicine.54.3510
1087
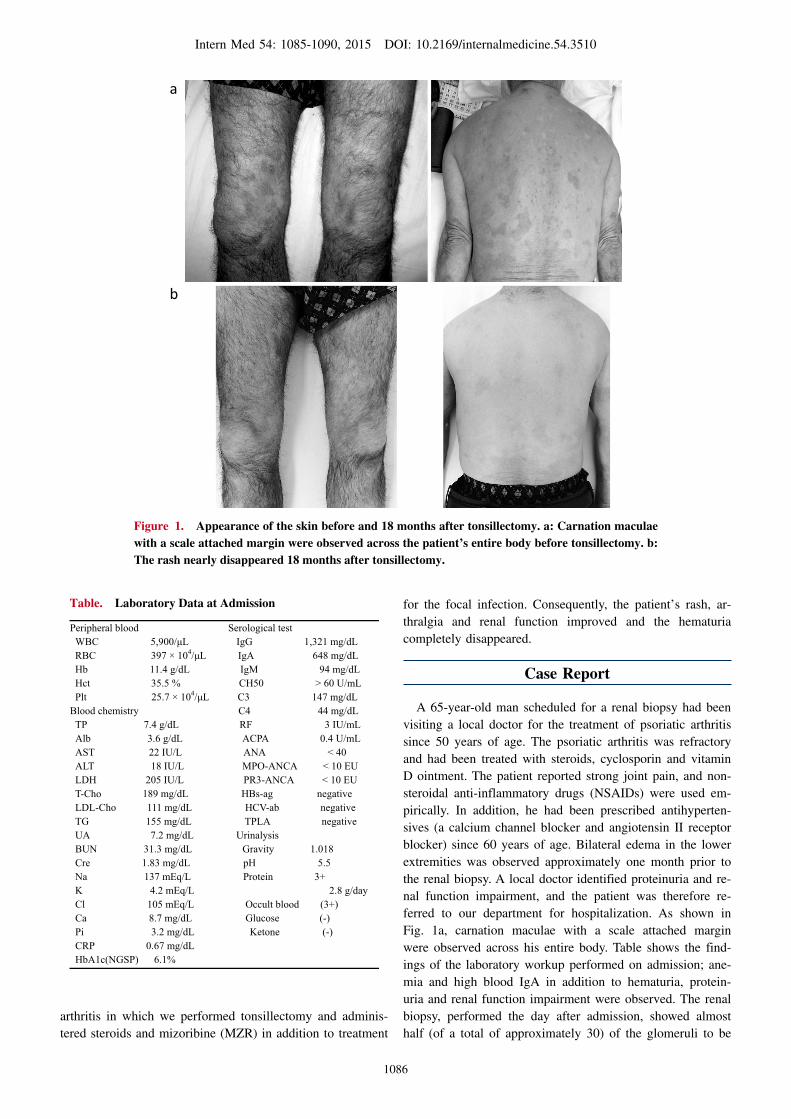
Figure 2. Findings of the renal biopsy. A total of 30 glomeruli were included in the renal biopsy samples, 16 of which had deteriorated (arrowhead in A) with tubular atrophy in addition to intersti-tial fibrosis in 30% of the renal cortex [A: Periodic acid methenamine silver (PAM) stain, ×400]. Focal segmental proliferative lesions were noted in five to six glomeruli (arrow in A), and small endocapil-lary proliferative lesions with inflammatory cell infiltration were evident in two glomeruli [B: Peri-odic acid-Schiff (PAS) stain, ×800]. Small fibrin exudation was seen in Bowman’s space, possibly as-sociated with a necrotizing glomerular lesion in one glomerulus (C: PAM stain, ×800). On immunohistochemistry, deposition of IgA (arrowheads in D) and C3 (arrowheads in E) was noted in a mesangial granular pattern (D: IgA stain; E: C3 stain; D, E: ×600). On electron microscopy, small electron-dense deposits (arrowheads in F) were evident in paramesangial areas (×5,000).
PAM ×400
×5,000
obsolescent, with slight segmental mesangial proliferative le-
sions in five to six glomeruli (Fig. 2). Endocapillary prolif-
eration with inflammatory cell infiltration was noted in two
glomeruli, and a small necrotizing lesion was evident in one
glomerulus, reflecting an active lesion. Furthermore, one
glomerulus exhibited segmental sclerosis with a fibrous cres-
cent, reflecting a chronic lesion. Glomerular adhesion was
observed in two glomeruli, and tubulointerstitial lesions had
progressed into 30% of the renal cortex. Immunohistochem-
istry showed deposition of IgA and C3 in mesangial areas.
The diagnosis was IgAN, M0, E1, S1 and T1 according to
the Oxford classification and grade IIIC based on the Japa-
nese histological grade. This status indicated the presence of
active lesions, including small necrotizing lesions, with
chronic lesions progressing to IgAN.
Bilateral tonsillectomy was performed one month after the
renal biopsy. Although treatment with NSAIDs and cy-
closporine was halted after the biopsy, the patient’s serum
creatinine level increased to 1.93 mg/dL. Additionally, ster-
oid pulse therapy was administered one week after tonsillec-
tomy. As follow-up treatment, prednisolone at a dose of 30
mg/day was administered for one month, after which the
dose was reduced to 30 mg every other day. Simultaneously,
MZR was started at a dose of 150 mg/day. Unfortunately,
the patient developed diabetes developed after receiving the
steroid pulse therapy, and it was necessary to prescribe a
dipeptidyl peptidase-4 inhibitor until the steroid dose could
be reduced. Meanwhile, the rash and arthralgia improved,
but did not disappear, immediately after tonsillectomy, while
the serum IgA level, which decreased after the procedure,
gradually increased again. Taking into consideration the ex-
istence of other focal infections, we started treatment [appli-
cation of 1% zinc chloride and Japanese apricot extract (MK
615) nose drops] for the upper pharynx 10 months after ton-
sillectomy. As shown in the figure, both the rash (Fig. 1b)
and arthralgia nearly disappeared soon after the treatment
Intern Med 54: 1085-1090, 2015 DOI: 10.2169/internalmedicine.54.3510
1088
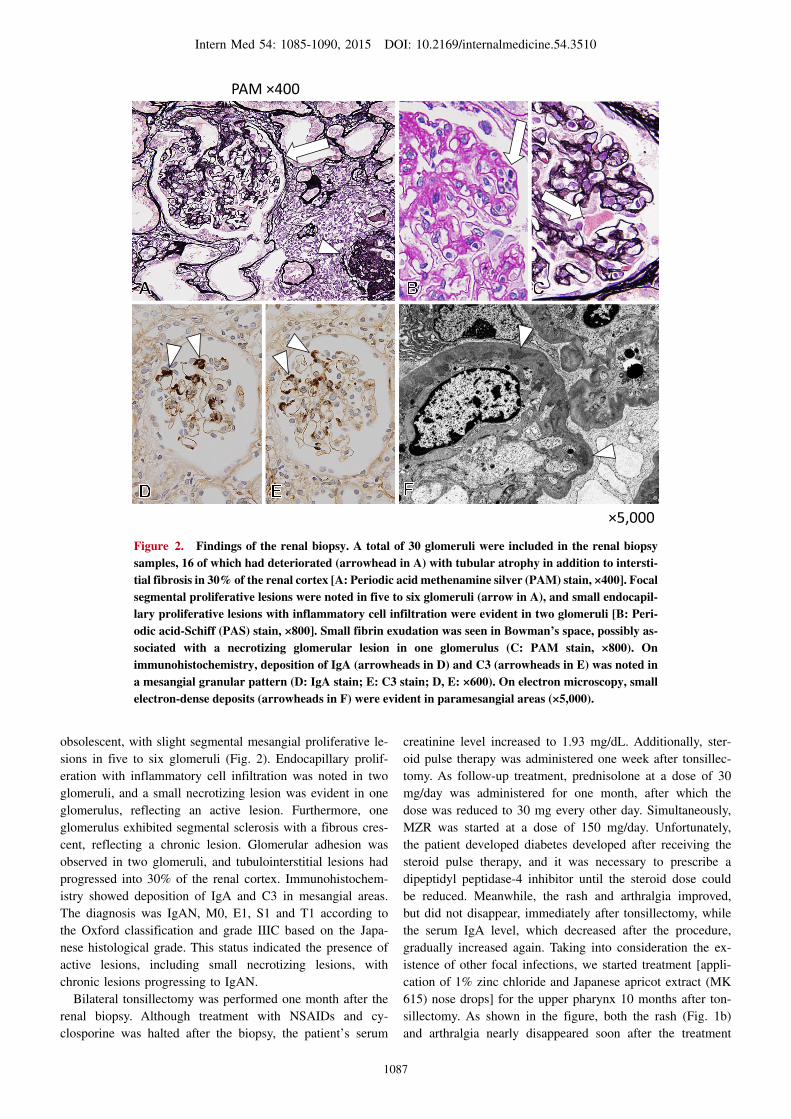
Figure 3. Clinical course
methylprednisolone0.5g/day
0
1
2
3
4
5
U-P
ro/C
r (g/
g)
Ser
um C
r (m
g/dL
)
1.0
2.0
3.0
U-Pro/CrSerum Cr
Tonsillectomy
prednisolone30
30
mizoribine150
25
100
20 15 10
75
5 mg every other day
mg a day
mg a day
Start of treatments for chronic epipharyngitis
month0 3 6 9 12 15
U-OB3+ 3+ 3+ 2+ 2+ 1+ 1+ 1+ ± –±
18
1+ ± –
Serum IgA 648 705 287 317 355 315 364 442 517 498 483 472 mg/dL
for chronic epipharyngitis. There was no need for antiphlo-
gistic analgesics. The IgA level decreased again, and the he-
maturia completely disappeared. In addition, the doses of
steroids and MZR were reduced without signs of worsening,
and the patient’s proteinuria and renal function gradually
improved. Twenty months after tonsillectomy, the serum cre-
atinine level had decreased from 1.93 to 1.55 mg/dL
(Fig. 3).
Discussion
Performing tonsillectomy combined with steroid pulse
therapy for IgAN at an early stage is expected to keep urine
abnormalities in remission (5). However, the therapeutic ef-
fect is unclear in cases in which a longer time has elapsed
from the onset of symptoms and/or patients with a history
of prior renal dysfunction. In the current case, the renal bi-
opsy showed that nearly half of the glomeruli were obsoles-
cent and the tubulointerstitial lesion had progressed. There-
fore, the pathological diagnosis was IgAN with few active
lesions, although the lesions were predominantly chronic.
We previously reported that the use of steroid pulse therapy
in combination with MZR following tonsillectomy is effec-
tive in improving urinary findings and preserving the renal
function when treating IgA nephropathy in patients with re-
nal impairment (6, 7).
It is recognized that the administration of MZR combined
with 14-3-3 protein and HSP60 enhances the transcriptional
activity of glucocorticoid receptors and thus the effect of
steroids (8). It has also been reported that MZR inhibits the
action of α3β1 integrin and decreases the motility of
fibroblast-specific protein-1-positive fibroblasts, both of
which are involved in the progression of interstitial fibrosis
in patients with IgAN (9).
It was recently demonstrated that activated macrophages
play an important role in the pathology of IgAN (10). Addi-
tionally, steroid-induced increases in transforming growth
factor-β production by macrophages are reportedly sup-
pressed by the concomitant use of MZR. MZR not only po-
tentiates steroidal anti-inflammatory effects, but also pre-
vents the progression of chronic lesions, such as those in-
volving tissue fibrosis and sclerosis, by inhibiting activated
macrophages.
Steroid therapy is usually terminated within six months to
one year. However, in this case, we continued treatment
with low-dose steroids due to the patient’s joint pain. Con-
sequently, the serum creatinine level temporarily worsened
after starting this therapy. We consider two possible causes
underlying this phenomenon: (a) the high dose of steroids
temporarily deteriorated the patient’s renal function and in-
duced glucose tolerance, and (b) the treatment of one course
of steroid pulse therapy combined with MZR takes longer to
achieve an effect than three courses of steroid pulse therapy
alone. In our experience, we have observed improvements in
the renal function several months after beginning MZR
treatment.
In this case, the patient’s rash caused by psoriatic arthritis
and arthralgia significantly improved soon after starting the
above therapy. Psoriatic arthritis is a form of chronic inflam-
matory arthritis accompanying psoriasis of the skin. This
disease is diverse, and, in some patients, progressive joint
lesions cause functional disturbances. The appearance of a
rash may significantly decrease the quality of life (QOL) of
the patient from both mental and physical perspectives to
the same degree as malignant tumors (11). It has been re-
ported that T cells, especially Th1 cells, play a central role

Intern Med 54: 1085-1090, 2015 DOI: 10.2169/internalmedicine.54.3510
1089
in the clinical onset of psoriasis. For example, a recent re-
port indicated that Th1 cells, Th17 cells and regulatory T
cells (Treg) are mutually and intricately associated with
chronic clinical states (12). It is therefore expected that inhi-
bition of TNF-α, an inflammatory cytokine, reduces inflam-
mation, suppresses epidermal growth and normalizes abnor-
mal cornification. Effects on articular symptoms are also ex-
pected, and joint breakdown may be inhibited. TNF-α in-
hibitors, such as infliximab and adalimumab, are increas-
ingly used in refractory cases. However, the burden of these
drugs is high, and it has been reported that serious side ef-
fects occur at approximately twice the rate in patients older
than 65 years of age than in those younger than 65 years of
age (13).
Tonsillectomy has been shown to be very effective for
palmoplantar pustulosis, sternocostoclavicular hyperostosis
and IgAN. It has also been documented that these diseases
coexist with one another at a high rate. Many reports have
indicated that tonsillectomy has far-reaching effects on pso-
riasis, rheumatoid arthritis and Behçet’s disease in addition
to the diseases listed above. Nyfors et al. described 74 cases
of psoriasis vulgaris treated with tonsillectomy, reporting
improvements in the rashes in 53 cases (72%) (2).
It has been speculated that an abnormal immune response
in the tonsils causes and/or worsens the diseases described
above. For example, Takahara reported that, on quantitative
immunohistological analyses of tonsillar tissues, the overall
area of T cell nodules is significantly expanded, whereas
that of B-lymphoid follicles is reduced, and the number of
apoptotic cells is elevated in tonsils obtained from patients
with psoriasis and palmoplantar pustulosis than in those
with recurrent tonsillitis. The area of T cell nodules and
number of apoptotic cells are significantly larger in the ton-
sils of patients exhibiting a complete recovery after tonsil-
lectomy than in those without a complete recovery (14).
In the present case, the rash initially improved after ton-
sillectomy and was further ameliorated after starting treat-
ment for chronic epipharyngitis. It was recently reported that
laryngological sources of infection are found in 44% of pa-
tients with psoriatic arthritis (15). Moreover, the effective-
ness of cholecystectomy in removing the inflammatory fo-
cus as a treatment for psoriasis has also been reported (16).
These facts suggest the presence of various factors in the
pathogenesis of psoriasis and the contribution of multiple in-
flammatory foci in addition to the tonsils.
The mucosal surface of the upper pharynx forces back
pathogenic microbes, such as bacteria and viruses, that are
continuously intruding, while possessing mechanisms which
allow it to coexist with resident microbiota. Secretory IgA
performs a crucial function in this system. The lumen sur-
face of the upper pharynx is covered with lymphocytes in a
state of activation, and class II antigen-positive ciliated epi-
thelial cells with an antigen-presenting ability are present in
the tonsillar crypt epidermis. It has also been reported that
the phenotype of lymphocytes obtained by scratching the
epipharynx closely resembles that of lymphocytes in the
palatine tonsils (17). Chronic epipharyngitis may be a cause
of focal infection related to the development of secondary
diseases.
The present patient was diagnosed with coexisting chronic
epipharyngitis, as the application of a winding cotton swab
containing 1% zinc chloride solution caused bleeding and
scratching pain. We directly applied zinc chloride, which
causes tissue convergence and corrosion and possesses an
antibacterial activity, in addition to nose drops comprising
MK615 to treat the patient’s chronic epipharyngitis. MK615
is a compound made by condensing and extracting Japanese
apricot and has been reported to have various effects, in-
cluding antitumor, anti-inflammatory and liver-supporting
functions. MK615 inhibits the release of cytokines, such as
TNF-α and IL-6, and may represent a useful therapeutic
agent for chronic periodontitis, a condition that is also re-
ported to cause focal infections (18, 19). In our facility, we
have used nose drops containing MK615 for chronic epipha-
ryngitis for several years. The curative effect is high, based
on our experience, with no concerns regarding safety. Nev-
ertheless, further studies are required to investigate the ef-
fects of local MK615 application as an adjunctive treatment.
Bleeding and pain resulting from the application of zinc
chloride to the epipharynx was reduced via successive appli-
cations in this case. At the same time, the patient’s rash and
arthralgia were further alleviated and the hematuria com-
pletely disappeared. However, it is necessary to accumulate
further cases involving this treatment in order to confirm
whether these agents are effective in cases of chronic
epipharyngitis.
In summary, we experienced a case of IgAN with coexist-
ing psoriatic arthritis in which we administered steroids and
MZR in addition to treatment for focal infection. Conse-
quently, the patient’s rash, arthralgia and renal function im-
proved and the hematuria completely disappeared. Although
this is a single case report, our findings indicate that combi-
nation treatment for focal infection, including steroids and
MZR, is effective for multiple pathological conditions that
may share a common source.
The authors state that they have no Conflict of Interest (COI).
References
1. Hiki Y, Iwase H, Kokubo T, et al. Association of asialo-galactosyl
beta 1-3N-acetylgalactosamine on the hinge with a conformational
instability of Jacalin-reactive immunoglobulin A1 in immuno-
globulin A nephropathy. J Am Soc Nephrol 7: 955-960, 1996.
2. Nyfors A, Rasmussen PA, Lemholt K, et al. Improvement of re-
calcitrant psoriasis vulgaris after tonsillectomy. J Laryngol Otol
90: 789-794, 1976.
3. Zachariae H. Prevalence of joint disease in patients with psoriasis:
implications for therapy. Am J Clin Dermatol 4: 441-447, 2003.
4. Mease PJ. Psoriatic arthritis - update on pathophysiology, assess-
ment, and management. Bull NYU Hosp Jt Dis 68: 191-198,
2010.
5. Hotta O, Miyazaki M, Furuta T, et al. Tonsillectomy and steroid
pulse therapy significantly impact on clinical remission in patients

Intern Med 54: 1085-1090, 2015 DOI: 10.2169/internalmedicine.54.3510
1090
with IgA nephropathy. Am J Kidney Dis 38: 736-743, 2001.
6. Kaneko T, Hirama A, Ueda K, et al. Methylprednisolone pulse
therapy combined with mizoribine following tonsillectomy for im-
munoglobulin A nephropathy: clinical remission rate, steroid spar-
ing effect, and maintenance of renal function. Clin Exp Nephrol
15: 73-78, 2011.
7. Kaneko T, Shimizu A, Tsuruoka S, et al. Efficacy of steroid pulse
therapy in combination with mizoribine following tonsillectomy
for immunoglobulin A nephropathy in renally impaired patients. J
Nippon Med Sch 80: 279-286, 2013.
8. Takahashi S, Wakui H, Gustafsson JA, et al. Functional interaction
of the immunosuppressant mizoribine with the 14-3-3 protein.
Biochem Biophys Res Commun 274: 87-92, 2000.
9. Nishitani Y, Iwano M, Yamaguchi Y, et al. Fibroblast-specific pro-
tein 1 is a specific prognostic marker for renal survival in patients
with IgAN. Kidney Int 68: 1078-1085, 2005.
10. Ikezumi Y, Suzuki T, Karasawa T, et al. Contrasting effects of
steroids and mizoribine on macrophage activation and glomerular
lesions in rat thy-1 mesangial proliferative glomerulonephritis. Am
J Nephrol 31: 273-282, 2010.
11. Rapp SR, Feldman SR, Exum ML, et al. Psoriasis causes as much
disability as other major medical diseases. J Am Acad Dermatol
41: 401-407, 1999.
12. Di Cesare A, Di Meglio P, Nestle FO. The IL-23/Th17 axis in the
immunopathogenesis of psoriasis. J Invest Dermatol 129: 1339-
1350, 2009.
13. Schneeweiss S, Setoguchi S, Weinblatt ME, et al. Anti-tumor ne-
crosis factor alpha therapy and the risk of serious bacterial infec-
tions in elderly patients with rheumatoid arthritis. Arthritis Rheum
56: 1754-1764, 2007.
14. Takahara M, Bandoh N, Imada M, et al. Effect of tonsillectomy
on psoriasis and tonsil histology. J Otolaryngol Jpn 104: 1065-
1070, 2001.
15. Brzewski P�, Spa�kowska M, Podbielska M, et al. The role of
focal infections in the pathogenesis of psoriasis and chronic urti-
caria. Postepy Dermatol Alergol 30: 77-84, 2013.
16. Nomura K, Mizutani H, Inachi S, et al. Remission of pustular
psoriasis after cholecystectomy: role of focal infection in pustu-
larization of psoriasis. J Dermatol 22: 122-124, 1995.
17. Hotta O. Chronic epipharyngitis and its possible focal-infection
role. Stomato-pharyngol 23: 37-42, 2010.
18. Nakagawa A, Sawada T, Okada T, et al. New antineoplastic agent,
MK615, from UME (a Variety of) Japanese apricot inhibits growth
of breast cancer cells in vitro. Breast J 13: 44-49, 2007.
19. Morimoto Y, Kikuchi K, Ito T, et al. MK615 attenuates Porphy-
romonas gingivalis lipopolysaccharide-induced pro-inflammatory
cytokine release via MAPK inactivation in murine macrophage-
like RAW264.7 cells. Biochem Biophys Res Commun 389: 90-94,
2009.
Ⓒ 2015 The Japanese Society of Internal Medicine
http://www.naika.or.jp/imonline/index.html