identifying information management challenges faced...
TRANSCRIPT

IDENTIFYING INFORMATION
MANAGEMENT CHALLENGES FACED BY
HOME HEALTHCARE PROFESSIONALS
MANAGING OLDER ADULTS’ TRANSITIONS
FROM HOSPITAL TO HOME CARE
Alicia Arbaje, M.D., M.P.H. Assistant Professor of Medicine, Director of Transitional Care Research
Division of Geriatric Medicine and Gerontology
Second International Home Care Nurses Organization Conference
23-26 Sept., 2014
Singapore

Care Transitions out of the Hospital
Common, complicated,
and costly
Older adults are
particularly vulnerable
Going home with home
care is especially risky
2
Coleman, 2003; Arbaje, 2014; Murtaugh, 2002
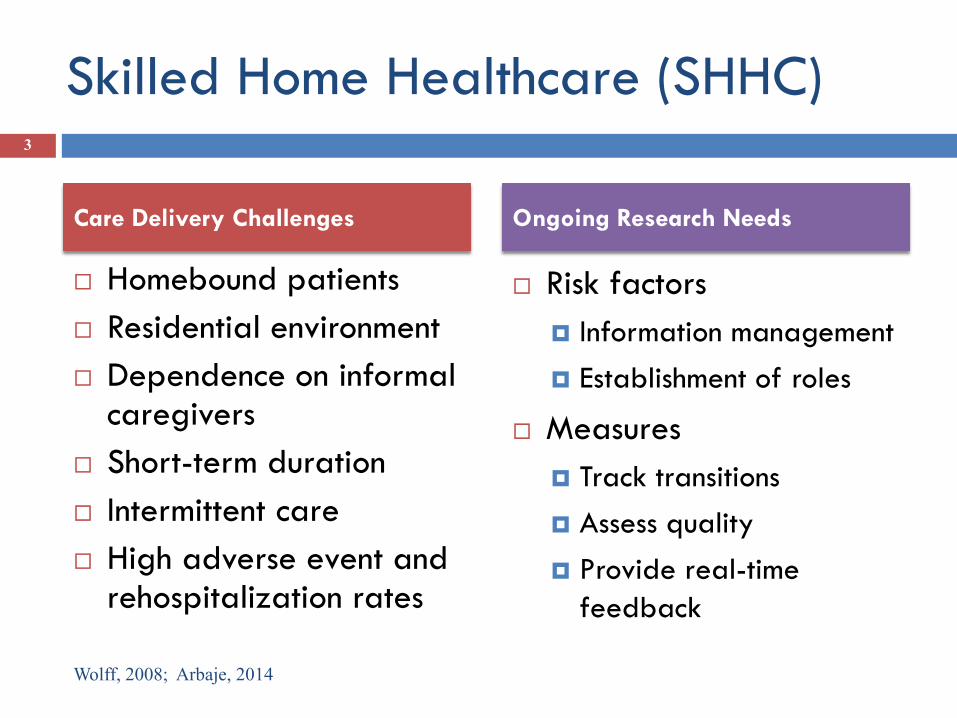
Skilled Home Healthcare (SHHC)
Homebound patients
Residential environment
Dependence on informal caregivers
Short-term duration
Intermittent care
High adverse event and rehospitalization rates
Risk factors
Information management
Establishment of roles
Measures
Track transitions
Assess quality
Provide real-time
feedback
3
Wolff, 2008; Arbaje, 2014
Care Delivery Challenges Ongoing Research Needs
Role of Human Factors
Engineering to Improve Transitions
Carayon, 2012; Gurses, 2011; Russ, 2013
4
Goal of human factors science is to promote efficiency, safety and effectiveness by improving the design of technologies, processes and work systems
Supports the cognitive and physical work of healthcare professionals
Promotes high quality, safe care for patients
Evaluates individual work system components and their interactions with each other
Proactively understand risks in complex systems
Qualitative and quantitative research methods
Helpful for errors that occur across multiple people or settings

Study Objectives 5
For older adults requiring SHHC services
after hospital discharge:
Identify critical tasks in SHHC workflow
Identify challenges faced by SHHC
professionals in information management

6
Study Population
Older Adults
Aged ≥ 65 years
Can speak English or Spanish
Hospitalized on a medical service
Referred for nursing SHHC after hospital discharge
Family Caregivers
Unpaid
Assist the older adult with at least one healthcare task (e.g.,
taking medication)
SHHC Providers
Employed by participating sites
Directly provide care to, or arrange services for, an eligible
older adult
9 med/surg units, 2 hospitals, 1SNF, 1SHHC agency

Transitions of Care From Hospital to Home Health Care
Settings 7
Location
Referral
• Hospital
• Discharge planner
• Home care services coordinator
Admission
• SHHC agency
• Intake staff
• Field staff
Initial evaluation
• Home
• Field staff
• Older adult
• Caregiver
Follow-up evaluation
• Home
• Field staff
• Older adult
• Caregiver
Process
flow
Care
providers
Period of study: t0 → 2-6 days after discharge
1-3 days after DC Close to hospital
discharge (t0) 1-3 days after home visit

Internal
Environment
Physical environment
a person operates
within.
Ex: patient home
Hospital/SHHC Work System
The objects used
to perform tasks.
Ex: electronic
medical record
Outside factor affecting tasks
performed in the system.
Ex: insurance policies
Actions performed
within the work
system
Home
Care
Nurse
Caregiver Older
Adult
Home Care
Coordinator
Any person or team of people
that interacts within the work
system.
Policies,
procedures, and
culture of the
system
Ex: safety
culture.
Organization
Care
Transitions
Processes
• Information
Management
• Establishment
of Roles
Outcomes
Serious
safety
events
30-day
hospital
readmission
Patient/
Caregiver
satisfaction
Overall
care
transition
quality
Human Factors Conceptual Framework
Outcomes
External Environment
Tasks
Tools,
Technology
Person
Internal Environment
8

Intake Nurse Scheduler
HCC
Assistant
Patient Caregiver
Home Care
Coordinator
Nurse
Case
Manager
Physician
Discuss
home care
options
Inform
patient of
agency
details
Fax
referral to
intake
Fax
additional
documents
Train
patient and
caregiver on
discharge
Insurance
Expert
Verify
insurance
Ensure
acceptance Create
EHR
POST –HOSPITAL DISCHARGE ADMISSION TO HOME CARE PRE-HOSPITAL DISCHARGE
Identify
referrals,
gather info,
complete
referrals
Send
patient
referral to
intake
Enter
patient info
and send to
scheduler Start of
care visit
scheduled/
completed
Refer to
skilled
provider
Helps
gather info
and
complete
referrals
Patient Caregiver
Primary Care
Physician
Place
additional
orders/requests
clarification

Information Management-Related Challenges
10
Cross-Team Challenges
Difficulty obtaining
information from multiple sources
Difficulty managing
multiple players in one transition
Communication breakdown
after patient discharge
Physician Accessibility Challenges
Incomplete information to
prepare referral
Lack of physician ownership
Limited access to PCP
Difficulty identifying PCP
Patient-Related
Changes in patient status
Uncertainty in care plans
Unclear expectations
about home care
Challenges communicating with patient
Tools and Technology
Multiple electronic systems
Electronic Paper Electronic
No coordination or cognitive aids
Incomplete or missing
information

Risk Prioritization
11 INFORMATION MANAGEMENT How often does the risk factor occur during care
transitions?
How likely is the risk factor to contribute to: • Serious pt safety events* • 30d hospital readmission • Negative pt experience • Overall quality of care tx
Risk Factor for Suboptimal Care Transition Rarely
(-) Sometimes
(+/-)
Very often
(+) Unlikely
Somewhat likely
Very likely
Home care provider gathers information from multiple sources
Home care provider receives incomplete and/or missing information
Home care provider experiences communication breakdown with physicians during care transition
Home care provider encounters physician who does not have the information needed to assume responsibility for patient
Home care provider experiences has challenges regarding changing care plans
* E.g., falls, adverse drug reactions, clinical deterioration

In Their Own Words…
“The ideal transition would be … being given
adequate notice [about] what the needs of the
patient are … [and] not at the last minute when
they are ready to go out the door.”
12 Home care coordinator

In Their Own Words…
“I’d say about 50% of the time there seems to be
something that requires a call to the doctor to get
straightened out.”
13 Home care nurse

Implications 14
Home care agencies and patients
Improve SHHC workflow and
documentation
Facilitate information exchange
among healthcare providers
Organize the scheduling of home care
visits
Design of patient/caregiver
educational tools
Researchers
Integration of HFE and HSR
Predictive validity

Current Approaches Study
Risk factors Patient level Healthcare organization
Home environment
Target processes Discharge planning
One-way communication
Information management
Establishment of roles
Systems redesign
Communication networks
Settings Hospital
Skilled/long-term care
Hospital
Home healthcare agency
Home
Data sources Medical records
Administrative data
Patient report
Organizational data
Healthcare providers
Family caregivers
Methods Health Services Research
(HSR)
HSR + Human Factors
Engineering + CBPR
Intervention Coaches
Navigators
Index to identify and reduce
potential safety risks
Current Approaches to Improving Care
Transitions and Contribution of the Study 15

Future directions
16

Research Team and Funding
Division of Geriatrics and Armstrong Institute
Bruce Leff, MD
Ayse Gurses, PhD
Elizabeth Tanner, PhD, RN
Albert Wu, MD, MPH
Mahiyar Nasarwanji, PhD
Nicole Werner, MA
JH Home Care Group
Mary Myers, RN, VP and COO
Kim Carl, RN, BSN, Director of HH Services
Dawn Hohl, RN, PhD, Director of HH Coordinators
Funding
Agency for Healthcare Research and Quality
National Patient Safety Foundation
Johns Hopkins Clinical Research Scholars
Division of Geriatric Medicine and Gerontology
JHU School of Nursing Center for Innovative Care in Aging

Discussion 18
Contact Information
Alicia I. Arbaje, M.D., M.P.H.

Supplementary information 19

Domains with Example Items
• Difficulty reading hand-written care plans
• Difficulty using equipment or supplies
• Lack of access to electronic medical record
Technology and Tools
• Unclear expectations about role of home care
• Ambiguity in responsibility for patient after DC
• Provider takes on tasks beyond normal duties
Establishment of Roles
• Challenges communicating with team members
• Challenges reconciling medications
• Patient located in distant geographic area
SHHC Provider
• Does not understand care plan
• Dissatisfied with discharge process
• Challenges obtaining medications
Patient/ Caregiver
20

Patient Perspectives
Pre-hospital discharge
Time when patient finds out about discharge vs. actual time of discharge
Instruction and discharge instructions although provided tend to be forgotten
Admission to home care
Not sent home with all medications
Transportation challenges
Delay in setting up home care admission visit
Post-hospital discharge
Adhering to care plan
Difficulty with equipment delivery and utilization
Family/caregiver issues
21

In Their Own Words…
“We had no inclination that we were leaving [the
hospital].”
“I come up from [therapy], lunch is sitting there, and
in the same breath they go, ‘Pack up your bags,
you’re going home’.”
22 Older adults and caregivers

Home Care Coordinator Perspectives
Pre-hospital discharge
Patient discharged before home care recommendation
Incomplete information to prepare referral
Challenges associated with multiple systems and sources of information
Challenges identifying eligible patients
Difficulty communicating with PCP
Admission to home care
Updating medication list as care plan changes
23

Home Care Nurse Perspectives
Post-hospital discharge
Challenges with medication reconciliation at patient’s home
Equipment not sent home with patient
Challenges reading hand written referrals
Lack of PCP ownership
Communication breakdown after discharge
24

In Their Own Words…
“If I don’t have the correct information… simple
things like …the address is completely wrong, the
phone number is wrong, the phone number is not in
service… then I can spend the day spinning wheels
calling here and there, calling emergency numbers
and trying to find the patient.”
25 Home care nurse