identifying and - nami - greater des moines · web viewrequire an additional data element per...
TRANSCRIPT
A Study of Iowa’s MCOs’ Provider Networks
Provider networks of Iowa’s Medicaid MCOs (Managed Care Organizations) are the source of all health care of Iowa’s Medicaid enrollees. Without adequate provider networks, Iowa taxpayers are paying its MCOs for delayed, even inaccessible health care. Delayed care is more expensive care.
Health care providers enter an MCO’s network by signing a contract agreeing to accept the MCO’s set reimbursement rates and payment conditions. Providers will not sign a network contract if the MCO’s reimbursements are insufficient or are not timely paid. To ensure the provider network structure works for patients, CMS (Centers for Medicaid and Medicare Services) charges states to ensure MCO provider networks are adequate by area of care/specialty/license type, and by urban/suburban/rural areas.
1. Assessment of Iowa’s MCO Provider Network DatasetThe Summer of 2016 much dissatisfaction was expressed by Iowa MCO insureds and providers. Iowa newspapers covered the story. One of the reporters, Jason Clayworth, investigative reporter, the Des Moines Register, contacted Nicole Keller and Cara Keller, AMOS (A Mid-Iowa Organizing Strategy) researchers who assessed the adequacy of mental health care providers of Iowa’s 2016 ACA exchange insurers. Clayworth sent the researchers a DHS (Department of Human Services) dataset (dated of July, 2016) containing all the records of all of Iowa’s MCO providers. Clayworth asked the researchers to see if any information related to provider network adequacy could be gleaned from the dataset.
Several sources (Iowa legislators, newspapers, advocates, etc.) had tried to use the dataset to find the truth about the adequacy of Iowa’s MCO provider networks. The dataset contains 169,444 provider records. Each record has 11 variables relevant to assessing network adequacy. Relevant variables include the provider’s name, unique NPI number (National Provider Identifier - a unique number assigned to each provider by CMS), provider’s practice address(es), and specialty areas of practice.
The dataset has at least one record for each unique address at which a provider provides care, thus a single provider who works at multiple addresses will have multiple records in the dataset. Example: A provider that works half days at 10 different locations in a week will have 10 legitimate records in the dataset. If that same provider is contracted with all 3 MCOs, the dataset will have 30 legitimate records for that provider.
There appears to be no quality oversight of the records to ensure accurate, complete and standardization of entries. Many records have missing, incomplete, and obviously incorrect data. Example: 15,042 records have NPI numbers that do not match the structure of the NPI number and 375 records do not have an NPI number. Without standardized data, adequacy measures are compromised. In addition, certain data necessary so adequacy assessment is not in the dataset.
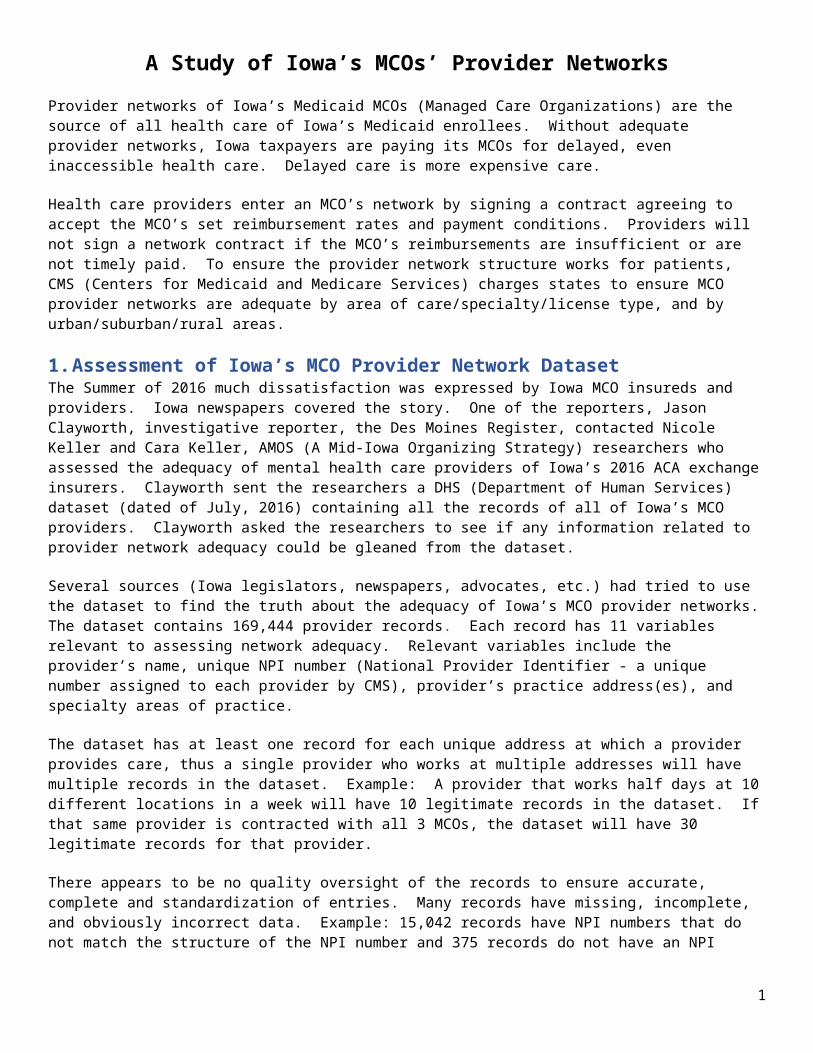
2. Identifying and Counting Locations Where Providers Deliver CareIdentifying and counting locations where health care is provided is essential in provider adequacy assessment. It is especially important for Iowans living in rural areas. It was expected most provider addresses in the MCO dataset would be in Iowa or within 60 miles (reasonable commuter distance) of Iowa’s border. It was expected that a few providers (suppliers, testing services, tele-med providers, etc.) would have addresses outside of Iowa. Following are 4 maps showing each city/state where at least 1 provider address in the dataset is located. The first map graphs the location of all individual and institutional providers of all 3 MCOs combined. The next 3 maps graphs locations of providers for each Iowa MCO.
1
This first map (above) begs the question: Are there this many suppliers outside of Iowa providing personal care for Iowa’s Medicaid enrollees?
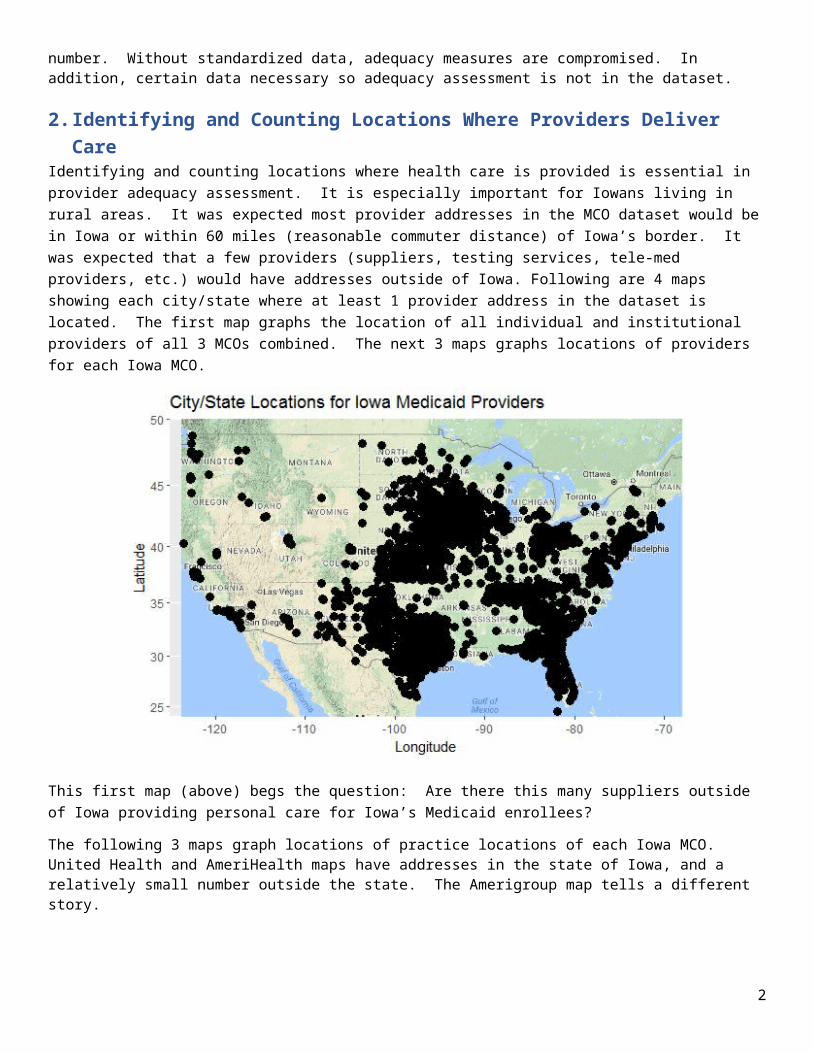
The following 3 maps graph locations of practice locations of each Iowa MCO. United Health and AmeriHealth maps have addresses in the state of Iowa, and a relatively small number outside the state. The Amerigroup map tells a different story.
2
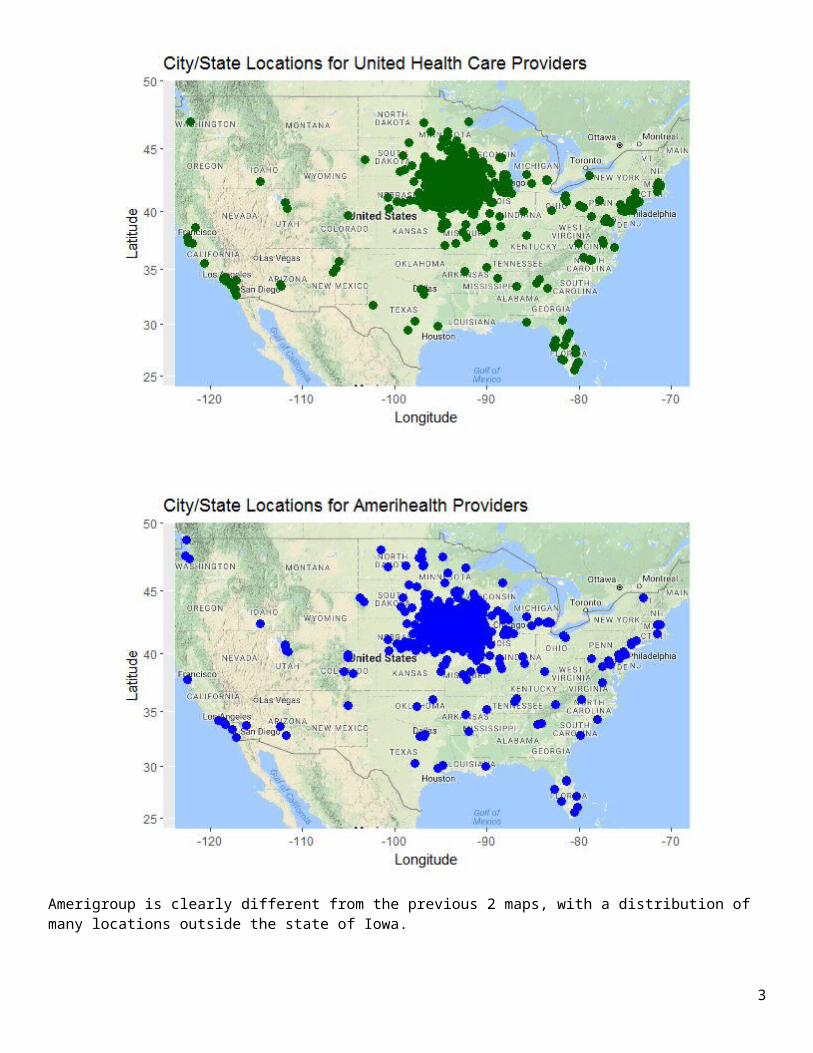
Amerigroup is clearly different from the previous 2 maps, with a distribution of many locations outside the state of Iowa.
Amerigroup is the outlier with the greatest number of out-of-Iowa providers. The map suggests Amerigroup’s Iowa provider list includes all providers in all the states for which Amerigroup provides MCO services. Researchers dived into Amerigroup’s provider records located in Tennessee to learn more. There are 671 provider records with addresses in Tennessee, but these records have only 31 unique NPI numbers, a.k.a. unique providers. Below is a list of the 10 most frequently occurring NPI numbers of this group of 671 providers.
3

NPI Frequency1114020401 1431245221092 1001053357905 991639451909 921093711996 911023107281 391417954165 381609858729 271346271251 81053335729 5
This analysis begs several questions:
1) Does the institutional provider, NPI 1114020401, specialty - “Home Community Based Services” actually provide care at 143 Iowa locations?
2) Should providers who provide in-person care outside of a set radius of Iowa’s border be considered in provider adequacy assessments for Iowa Medicaid enrollees?
The specialty area for NPI# 1114020401 is Home Community Based Service. The map below shows the locations by city/state of home community based service providers for Iowa Medicaid members in the Amerigroup MCO. It begs the question, what is a legitimate home community based service provider for Iowans?
3. Identifying and Counting Providers The dataset has 30,911 providers, as measured by unique NPI#s. Amerigroup has contracts with 30,386 of them, Amerihealth has contracts with 26,496 of them, and United Health has contracts with 20,083 of them. It is important to understand that these numbers do not indicate a count of providers. If a provider worked half days at 10 different locations per week and contracted with all three MCOs, s/he could be listed 30 times (.1 FTE X 10 half days X 3 MCOs = 30 records).
4

Below is a map showing the locations for individual provider, NPI 1841233889, who is listed in the dataset 3 times at 25 locations, and 1 additional location to make 76 records. Locations are mapped at the city/state level below. It is unreasonable to think that each of these locations are getting full time support from the 1 individual provider. When Iowa’s DHS counts provider numbers, do they count this provider as 1 provider, 26 providers, or 76 providers?
The AMOS mental health study identified reasons why some providers had unbelievable numbers of records. 1) Some records were duplicated. 2) Some institutions registered all their providers at all their locations, even though they work at only 1 or 2. 3) Some providers consult or supervise other providers, but do not provide direct patient care at the indicated locations. It appears the MCO provider network dataset has some of the same problems.
The state needs to dictate a specific data record design along with guiding rules. Then state needs to confirm the integrity of the data provided by the MCOs by applying data tests to the entire dataset, mailings to confirm provider addresses of practice and secret shopper calls to a random sampling to confirm validity of data. Signs of deliberately misleading or irresponsible maintenance of MCOs submitted data should result in fines and more concentrated oversight.
4. Identifying Data Needed to Assess Provider Adequacy Locations of practice addresses: More than 30% of the data set, 52,132 records, show a location that is not in the
state of Iowa. DHS needs to establish rules for inclusion of out-of-state providers in Iowa’s MCO provider network lists.
Require an additional data element per record – FTE (full time equivalent) worked at each address. This is element is required to accurately measure the availability of health care. Full-time is 1 FTE, one half day per week is .1 FTE. DHS should not consider any record with less than .1 FTE when assessing adequacy.
Establish the NPI# as the key data element in DHS’s combined dataset of all Iowa MCOs. There will be multiple practice locations per NPI# and there will be multiple MCOs per NPI#, per multiple locations. Cap FTEs per NPI# at 1.0.
Require all medical license and specialty area(s) of practice per location per NPI#. Perform provider adequacy assessments prior to MCO contract amendments and renewals, no less than annually.
5

5. Assessing Adequacy by Enrollee AddressResearchers geo mapped MCO networks of providers’ addresses of practice. Researchers were prepared to overlay geo mapped enrollee residence zip codes, but were unable to do. DHS did not respond to 2 requests for blind Medicaid enrollee zip code data. Geo mapping MCO providers vs. enrollees would have revealed inadequacies in urban, suburban, small town vs. rural areas of specific health care specialty areas.
6. Remedying on MCO Provider Network InadequaciesAn MCO should not be disqualified for network adequacy unless there are providers operating in the area who will not contract with the MCO or commercial insurer, presumably due to low reimbursements and/or untimely payment of reimbursements. If a disqualifying inadequacy is not remedied, the MCO should be prevented from enrolling Medicaid insureds in the area. Affected insureds should move their enrollment to an alternate MCO that satisfies the provider adequacy test in the area.
If the MCOs’ network inadequacy is the result of the state’s or a region’s inadequate provider workforce, it is the state’s responsibility to remediate. DHS is not responsible for statewide or regional inadequacies; Iowa’s Department of Public Health (IDPH) is. This level of inadequacy affects Medicaid enrollees and commercially insured Iowans. This affects both Iowa taxpayers and Iowa insureds. An inadequate statewide or regionalized healthcare workforce cannot provide timely quality health care. Iowa taxpayers are paying for Medicaid health care that is not available. Iowa health insurance consumers are paying for health care that is not available. It is undeniable that it results in unnecessary suffering, premature death, fewer Iowa jobs, higher insurance premiums and higher taxes. Health care provider inadequacy must be addressed effectively and quickly.
There are several strategies available to remedy health care provider inadequacy in areas of the state and across the state. IDPH can provide funds to increase medical residencies in Iowa, fund specialty programs in Iowa colleges and universities, forgive educational loans and grant scholarships to motivate existing providers to advance their credentials, and/or recruit providers from other states.
7. Taking It A Step FurtherThe state of Iowa could deliver much added value to Medicaid and commercial insurers and enrollees with no impact on the state budget. Combining the work of measurement and enforcement of health care provider adequacy for MCOs and commercial insurers with a single state licensing and credentialing system and a single state provider directory could work very well. It would reduce insurers’ cost of licensing, credentialing, speed providers entrance into our state’s health care workforce, and eliminate insurers' costs of building and maintaining provider directories. This entire state operation could be funded by insurer fees. Insurer fees would be much lower than their current costs for providing these functions. The lower costs would be reflected in lower Medicaid costs and lower insurance premiums.
6