identifying and communicating clinically meaningful drug-drug interactions
TRANSCRIPT
http://jpp.sagepub.com/Journal of Pharmacy Practice
http://jpp.sagepub.com/content/early/2014/08/07/0897190014544793The online version of this article can be found at:
DOI: 10.1177/0897190014544793
published online 8 August 2014Journal of Pharmacy PracticeScott D. Nelson, Joanne LaFleur, Emily Hunter, Melissa Archer, Carin Steinvoort, CarrieAnn Maden and Gary M. Oderda
Drug Interactions−Identifying and Communicating Clinically Meaningful Drug
Published by:
http://www.sagepublications.com
On behalf of:
New York State Council of Health-system Pharmacists
can be found at:Journal of Pharmacy PracticeAdditional services and information for
http://jpp.sagepub.com/cgi/alertsEmail Alerts:
http://jpp.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
What is This?
- Aug 8, 2014OnlineFirst Version of Record >>
by guest on December 3, 2014jpp.sagepub.comDownloaded from by guest on December 3, 2014jpp.sagepub.comDownloaded from
Research Article
Identifying and Communicating ClinicallyMeaningful Drug–Drug Interactions
Scott D. Nelson, PharmD1, Joanne LaFleur, PharmD, MSPH1,Emily Hunter, PharmD, MLS1, Melissa Archer, PharmD2,Carin Steinvoort, PharmD2, CarrieAnn Maden, PharmD, BCPS2,and Gary M. Oderda, PharmD, MPH1
AbstractObjective: Providing care to patients with comorbid medical problems may result in complicated, multiple drug therapy regimens,increasing the risk of clinically meaningful drug–drug interactions (DDIs). The purpose of this article is to describe the prevalenceof DDIs and provide examples on how to identify and intervene on DDIs. Methods: We described DDI data from the Utah DrugRegimen Review Center, where adult Medicaid patients were reviewed by pharmacists from 2005 to 2009. Patients were selectedby the number of prescriptions filled per month (>7) or having a high RxRisk score. Summary: A total of 8860 patients werereviewed, and 16.6% had at least 1 clinically meaningful DDI. Patients with DDIs were slightly younger (mean age 45.2 vs 48.2),more likely to be female (75.0% vs 68.9%), and had more prescriptions per month (13.4 vs 12.5) compared to patients without (P <.001). Pharmacodynamic DDIs were more prevalent (80.2%) than pharmacokinetic. Pharmacodynamic DDIs mainly occurred withdrugs used to treat psychiatric/seizure/sleep disorders (69.4%) and pain/migraine (56.6%). Pharmacokinetic DDIs mainly occurredwith drugs used to treat psychiatric/seizure/sleep disorders (53.2%), cardiovascular diseases (46.3%), and infectious diseases(29.6%). Conclusions: Clinically meaningful DDIs are common in patients with complex medication regimens. A systematicapproach for identifying DDIs, determining clinical significance, formulating patient-specific recommendations, and communicatingrecommendations is important in pharmacy practice.
Keywordscommunity pharmacy services, drug interactions, pharmacodynamics, pharmacokinetics
Background
Practitioners today are responsible for providing care to
patients with many comorbid medical problems. In doing
so, prescribers utilize multiple drug therapy regimens,
complicated recommendations from clinical practice guide-
lines, and consumer-driven health care demands resulting
in complex medication regimens for patients. The complex-
ity of a drug therapy regimen can be defined by the number
of medications being prescribed combined with the different
dosing schedules for each of the medications.1 These com-
plex medication regimens contribute to an estimated
US$177.4 billion (equivalent to approximately US$240 bil-
lion in 2013) per year spent on drug-related morbidity and
mortality resulting from nonadherence, therapeutic failures,
and drug–drug interactions (DDIs).2 Prescribers often rely
on pharmacists to detect DDIs that may be overlooked, yet
identifying and addressing DDIs can be difficult for phar-
macist interns, newly licensed professionals, and even some
experienced pharmacists. Mastery of DDI detection is
important for ensuring optimal drug therapy, especially in
patients with complex drug regimens.
DDIs can be divided into 2 main types: pharmacodynamic
and pharmacokinetic interactions. Pharmacodynamic interac-
tions can occur in 2 ways: (1) a drug antagonizing the effects
of another drug, resulting in a lower than expected therapeutic
effect and (2) 2 drugs exhibiting additive effects. Pharmacoki-
netic interactions relate to the body’s effect on a drug; these
DDIs are due to alterations in absorption, distribution, metabo-
lism, or excretion that result from the combination of 2 drugs.
In any given week, more than 80% of adults in the United
States take some type of medication including prescription
drugs, over-the-counter treatments, herbals, and vitamins.3
Among these medication users, nearly one-third take 5 or more
prescriptions, leading to an increased risk of DDIs. It is
1 L.S. Skaggs Pharmacy Institute, Department of Pharmacotherapy, University
of Utah College of Pharmacy, Salt Lake City, UT, USA2 Utah Medicaid Drug Regimen Review Center, Salt Lake City, UT, USA
Corresponding Author:
Scott D. Nelson, L.S. Skaggs Pharmacy Institute, University of Utah College
of Pharmacy, 30 South 2000 East, 4th Floor, Salt Lake City, UT 84112, USA.
Email: [email protected]
Journal of Pharmacy Practice1-6ª The Author(s) 2014Reprints and permission:sagepub.com/journalsPermissions.navDOI: 10.1177/0897190014544793jpp.sagepub.com
by guest on December 3, 2014jpp.sagepub.comDownloaded from

estimated that a DDI occurs in up to 11% of patients.4 Although
the severity of DDIs is widely variable, clinically meaningful
DDIs, such as interactions that are likely to cause patient harm
or be life threatening if not detected, occur in about 0.81% of
visits where the patient was prescribed 2 or more medications.5
Additionally, each additional medication prescribed doubles
the likelihood of a clinically meaningful DDI.5
At the Utah Medicaid Drug Regimen Review Center
(DRRC), pharmacists check patients’ pharmacy records for a
variety of drug-related problems. These problems include phar-
macokinetic and pharmacodynamic DDIs as well as other
issues including polypharmacy, therapeutic duplications, and
dose discrepancies. A program description and definitions for
all drug-related problems have been previously published.6
Much of the available literature on DDIs is limited to inter-
actions between specific drugs,7 drug classes,8 or patient popu-
lations9 rather than discussing DDIs in general. The goal of this
article is to describe some of the most common clinically
meaningful DDIs found by pharmacists and to provide insight
into the identification and potential solutions of these prob-
lems. This article may serve as a reference for pharmacists
dealing with DDIs in complex patients seen in a variety of prac-
tices, and the technique described here can empower pharma-
cists to make appropriate DDI-related interventions.
Methods
Program Description
The analysis set for this study was extracted from data previously
collected by the DRRC as a routine part of their operations.6 The
DRRC was established in 2001 with the primary goal of aiding in
the management of pharmaceutical therapy for medically com-
plex patients to improve the health of Medicaid recipients. Med-
icaid enrollees are chosen for DRRC evaluation based on several
different factors, such as selecting the patients with the top num-
ber of prescriptions they had filled within any given month (>7),
or the patients with the top RxRisk score.10,11 The RxRisk tool
provides an estimated risk assessment based on automated phar-
macy and demographic data.12 Patients were reviewed if they had
not already been reviewed in the previous 12 months.
After patients were listed for review, pharmacists evaluated
their pharmacy claims for potential drug-related problems,
including DDIs. Data available to pharmacists for review
included diagnoses and procedure codes submitted with medi-
cal claims since 2001, all prescription and nonprescriptions
pharmacy claims paid by Medicaid in the month of review and
the prior year, and prior DRRC recommendations if the patient
had previously been reviewed. After review, the pharmacist
would fax a letter to the physician with formal evidence-
based recommendations if a drug-related problem was found.
Patients and Data Set
In this descriptive study, we identified all adult Medicaid
patients who were reviewed by DRRC pharmacists from
2005 to 2009. For patients who were reviewed more than once
during the 4-year study period, only data from the first review
were used. A data set was constructed that contained age and
gender, month and date of review, number of prescriptions in
the month of review, all drug-related problems that were iden-
tified by pharmacists, and a pharmacist’s note about each spe-
cific DDI, including drugs of interest. This project was
reviewed by the University of Utah Institutional Review Board
(IRB) and determined to be nonhuman subjects research
because no identifiable, individual, or private information was
used by the researchers.
Outcomes
The outcome of interest was the prevalence of clinically
meaningful DDIs found from the selected cohort. A clinically
meaningful DDI was defined as an interaction that is likely to
cause patient harm or be life threatening if not detected. An
investigator classified the DDIs based on the pharmacists’ text
note as either ‘‘pharmacokinetic’’ or ‘‘pharmacodynamic’’ and
into disease state categories for the interacting drugs including
allergy/cough/cold, asthma/chronic obstructive pulmonary dis-
ease (COPD), cardiovascular, contraception, diabetes/endocrine,
gastrointestinal, genitourinary, gout, immunologic disease, infec-
tious disease, nutritional supplementation, pain/migraine, and
psych/seizure/sleep, and other.
Data Analysis
Descriptive statistics were used to characterize patient demo-
graphics, frequencies, and percentages of DDIs overall by
pharmacokinetic/pharmacodynamic classification and by ther-
apeutic category for the implicated drugs. Simple univariate
comparisons were done to compare patient demographics in
patients with and without DDIs using the Student’s t test, for
continuous variables, and the chi-square test, for categorical
variables. This study used STATA 12 statistical software.13
Results
Patients
As summarized in Figure 1, there were 202 299 patients who
filled at least 2 prescriptions during the same month between
January 2005 and December 2010. Of those, 11 067 patients
were flagged as eligible for review due to the number of fills
or RxRisk score during the month of review. Pharmacists
excluded 2207 of the patients for various reasons including
(1) not enough claims history, (2) no useful intervention could
be made based on the patient’s disease state, or (3) the patient
was incorrectly identified by the system as having >7 medica-
tions but upon pharmacist review had fewer than 7 unique med-
ications due to multiple fills of the same medication in a month.
The remaining 8860 patients comprised the cohort for this
study. The mean (standard deviation) age of the cohort was
47.7 (16.4), and 69.9% were female. The mean (standard devia-
tion) number of prescriptions per patient in the review month
was 12.6 (3.5). Patients’ characteristics are summarized in
2 Journal of Pharmacy Practice
by guest on December 3, 2014jpp.sagepub.comDownloaded from
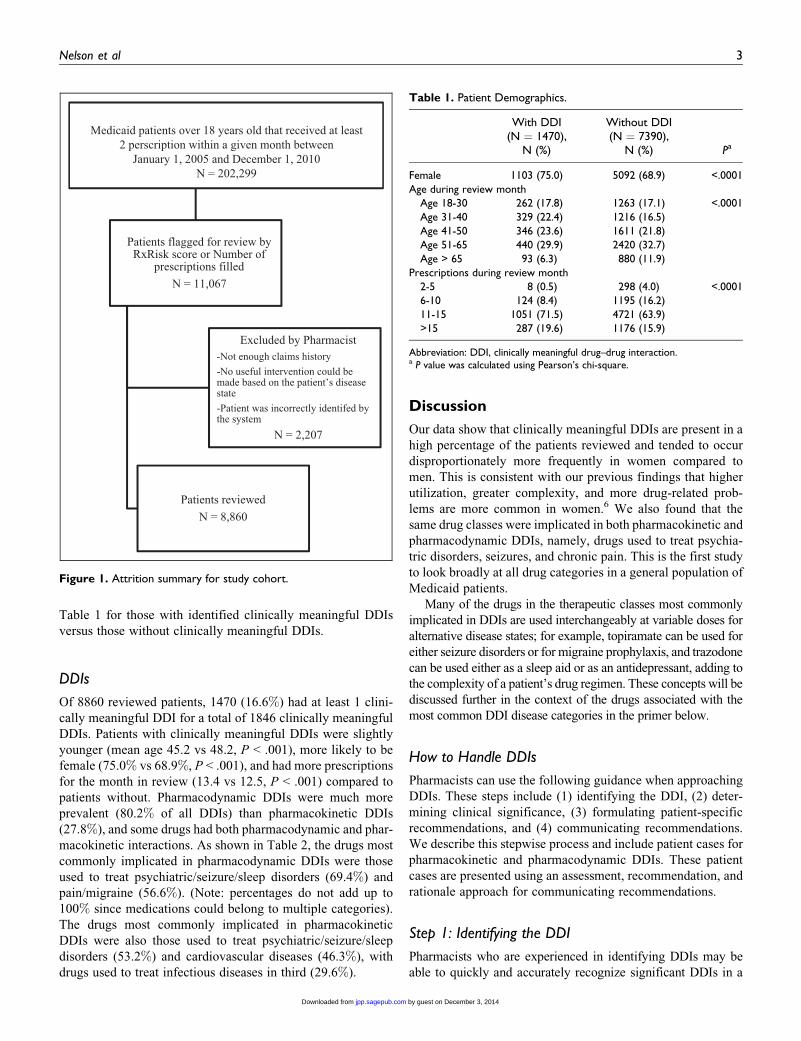
Table 1 for those with identified clinically meaningful DDIs
versus those without clinically meaningful DDIs.
DDIs
Of 8860 reviewed patients, 1470 (16.6%) had at least 1 clini-
cally meaningful DDI for a total of 1846 clinically meaningful
DDIs. Patients with clinically meaningful DDIs were slightly
younger (mean age 45.2 vs 48.2, P < .001), more likely to be
female (75.0% vs 68.9%, P < .001), and had more prescriptions
for the month in review (13.4 vs 12.5, P < .001) compared to
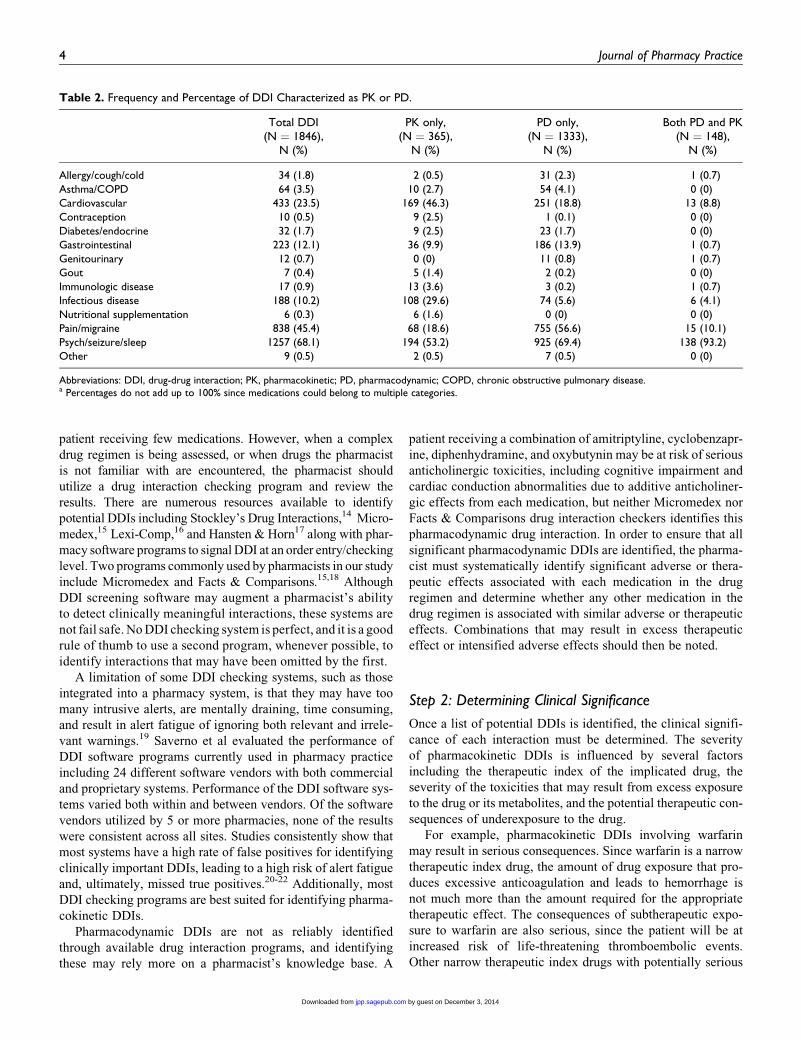
patients without. Pharmacodynamic DDIs were much more
prevalent (80.2% of all DDIs) than pharmacokinetic DDIs
(27.8%), and some drugs had both pharmacodynamic and phar-
macokinetic interactions. As shown in Table 2, the drugs most
commonly implicated in pharmacodynamic DDIs were those
used to treat psychiatric/seizure/sleep disorders (69.4%) and
pain/migraine (56.6%). (Note: percentages do not add up to
100% since medications could belong to multiple categories).
The drugs most commonly implicated in pharmacokinetic
DDIs were also those used to treat psychiatric/seizure/sleep
disorders (53.2%) and cardiovascular diseases (46.3%), with
drugs used to treat infectious diseases in third (29.6%).
Discussion
Our data show that clinically meaningful DDIs are present in a
high percentage of the patients reviewed and tended to occur
disproportionately more frequently in women compared to
men. This is consistent with our previous findings that higher
utilization, greater complexity, and more drug-related prob-
lems are more common in women.6 We also found that the
same drug classes were implicated in both pharmacokinetic and
pharmacodynamic DDIs, namely, drugs used to treat psychia-
tric disorders, seizures, and chronic pain. This is the first study
to look broadly at all drug categories in a general population of
Medicaid patients.
Many of the drugs in the therapeutic classes most commonly
implicated in DDIs are used interchangeably at variable doses for
alternative disease states; for example, topiramate can be used for
either seizure disorders or for migraine prophylaxis, and trazodone
can be used either as a sleep aid or as an antidepressant, adding to
the complexity of a patient’s drug regimen. These concepts will be
discussed further in the context of the drugs associated with the
most common DDI disease categories in the primer below.
How to Handle DDIs
Pharmacists can use the following guidance when approaching
DDIs. These steps include (1) identifying the DDI, (2) deter-
mining clinical significance, (3) formulating patient-specific
recommendations, and (4) communicating recommendations.
We describe this stepwise process and include patient cases for
pharmacokinetic and pharmacodynamic DDIs. These patient
cases are presented using an assessment, recommendation, and
rationale approach for communicating recommendations.
Step 1: Identifying the DDI
Pharmacists who are experienced in identifying DDIs may be
able to quickly and accurately recognize significant DDIs in a
Table 1. Patient Demographics.
With DDI(N ¼ 1470),
N (%)
Without DDI(N ¼ 7390),
N (%) Pa
Female 1103 (75.0) 5092 (68.9) <.0001
Age during review monthAge 18-30 262 (17.8) 1263 (17.1) <.0001
Age 31-40 329 (22.4) 1216 (16.5)
Age 41-50 346 (23.6) 1611 (21.8)Age 51-65 440 (29.9) 2420 (32.7)
Age > 65 93 (6.3) 880 (11.9)Prescriptions during review month
2-5 8 (0.5) 298 (4.0) <.00016-10 124 (8.4) 1195 (16.2)
11-15 1051 (71.5) 4721 (63.9)>15 287 (19.6) 1176 (15.9)
Abbreviation: DDI, clinically meaningful drug–drug interaction.a P value was calculated using Pearson’s chi-square.
Medicaid patients over 18 years old that received at least2 perscription within a given month between
January 1, 2005 and December 1, 2010N = 202,299
Patients flagged for review by RxRisk score or Number of
prescriptions filledN = 11,067
Excluded by Pharmacist-Not enough claims history-No useful intervention could be made based on the patient’s disease state-Patient was incorrectly identifed by the system
N = 2,207
Patients reviewedN = 8,860
Figure 1. Attrition summary for study cohort.
Nelson et al 3
by guest on December 3, 2014jpp.sagepub.comDownloaded from
patient receiving few medications. However, when a complex
drug regimen is being assessed, or when drugs the pharmacist
is not familiar with are encountered, the pharmacist should
utilize a drug interaction checking program and review the
results. There are numerous resources available to identify
potential DDIs including Stockley’s Drug Interactions,14 Micro-
medex,15 Lexi-Comp,16 and Hansten & Horn17 along with phar-
macy software programs to signal DDI at an order entry/checking
level. Two programs commonly used by pharmacists in our study
include Micromedex and Facts & Comparisons.15,18 Although
DDI screening software may augment a pharmacist’s ability
to detect clinically meaningful interactions, these systems are
not fail safe. No DDI checking system is perfect, and it is a good
rule of thumb to use a second program, whenever possible, to
identify interactions that may have been omitted by the first.
A limitation of some DDI checking systems, such as those
integrated into a pharmacy system, is that they may have too
many intrusive alerts, are mentally draining, time consuming,
and result in alert fatigue of ignoring both relevant and irrele-
vant warnings.19 Saverno et al evaluated the performance of
DDI software programs currently used in pharmacy practice
including 24 different software vendors with both commercial
and proprietary systems. Performance of the DDI software sys-
tems varied both within and between vendors. Of the software
vendors utilized by 5 or more pharmacies, none of the results
were consistent across all sites. Studies consistently show that
most systems have a high rate of false positives for identifying
clinically important DDIs, leading to a high risk of alert fatigue
and, ultimately, missed true positives.20-22 Additionally, most
DDI checking programs are best suited for identifying pharma-
cokinetic DDIs.
Pharmacodynamic DDIs are not as reliably identified
through available drug interaction programs, and identifying
these may rely more on a pharmacist’s knowledge base. A
patient receiving a combination of amitriptyline, cyclobenzapr-
ine, diphenhydramine, and oxybutynin may be at risk of serious
anticholinergic toxicities, including cognitive impairment and
cardiac conduction abnormalities due to additive anticholiner-
gic effects from each medication, but neither Micromedex nor
Facts & Comparisons drug interaction checkers identifies this
pharmacodynamic drug interaction. In order to ensure that all
significant pharmacodynamic DDIs are identified, the pharma-
cist must systematically identify significant adverse or thera-
peutic effects associated with each medication in the drug
regimen and determine whether any other medication in the
drug regimen is associated with similar adverse or therapeutic
effects. Combinations that may result in excess therapeutic
effect or intensified adverse effects should then be noted.
Step 2: Determining Clinical Significance
Once a list of potential DDIs is identified, the clinical signifi-
cance of each interaction must be determined. The severity
of pharmacokinetic DDIs is influenced by several factors
including the therapeutic index of the implicated drug, the
severity of the toxicities that may result from excess exposure
to the drug or its metabolites, and the potential therapeutic con-
sequences of underexposure to the drug.
For example, pharmacokinetic DDIs involving warfarin
may result in serious consequences. Since warfarin is a narrow
therapeutic index drug, the amount of drug exposure that pro-
duces excessive anticoagulation and leads to hemorrhage is
not much more than the amount required for the appropriate
therapeutic effect. The consequences of subtherapeutic expo-
sure to warfarin are also serious, since the patient will be at
increased risk of life-threatening thromboembolic events.
Other narrow therapeutic index drugs with potentially serious
Table 2. Frequency and Percentage of DDI Characterized as PK or PD.
Total DDI(N ¼ 1846),
N (%)
PK only,(N ¼ 365),
N (%)
PD only,(N ¼ 1333),
N (%)
Both PD and PK(N ¼ 148),
N (%)
Allergy/cough/cold 34 (1.8) 2 (0.5) 31 (2.3) 1 (0.7)
Asthma/COPD 64 (3.5) 10 (2.7) 54 (4.1) 0 (0)Cardiovascular 433 (23.5) 169 (46.3) 251 (18.8) 13 (8.8)
Contraception 10 (0.5) 9 (2.5) 1 (0.1) 0 (0)
Diabetes/endocrine 32 (1.7) 9 (2.5) 23 (1.7) 0 (0)Gastrointestinal 223 (12.1) 36 (9.9) 186 (13.9) 1 (0.7)
Genitourinary 12 (0.7) 0 (0) 11 (0.8) 1 (0.7)Gout 7 (0.4) 5 (1.4) 2 (0.2) 0 (0)
Immunologic disease 17 (0.9) 13 (3.6) 3 (0.2) 1 (0.7)Infectious disease 188 (10.2) 108 (29.6) 74 (5.6) 6 (4.1)
Nutritional supplementation 6 (0.3) 6 (1.6) 0 (0) 0 (0)Pain/migraine 838 (45.4) 68 (18.6) 755 (56.6) 15 (10.1)
Psych/seizure/sleep 1257 (68.1) 194 (53.2) 925 (69.4) 138 (93.2)Other 9 (0.5) 2 (0.5) 7 (0.5) 0 (0)
Abbreviations: DDI, drug-drug interaction; PK, pharmacokinetic; PD, pharmacodynamic; COPD, chronic obstructive pulmonary disease.a Percentages do not add up to 100% since medications could belong to multiple categories.
4 Journal of Pharmacy Practice
by guest on December 3, 2014jpp.sagepub.comDownloaded from

toxicities include lithium, digoxin, carbamazepine, cyclospor-
ine, insulin, and phenytoin.
The severity of pharmacodynamic DDIs is also influenced
by the severity of the toxicities that are involved or the conse-
quences of diminished therapeutic activity of at least one of
the involved drugs. Multiple sources may provide information
that may help determine the significance of an interaction.
Clinical trial data and kinetics studies may help the pharma-
cist understand the individual drugs involved in the interac-
tion including the dosage ranges and drug serum levels
associated with therapeutic, subtherapeutic, or toxic effects
of a drug, and the incidence and severity of adverse effects.
This information combined with kinetics studies and case
reports involving the DDI are very helpful in determining the
significance of an interaction.
Clinical references, including DDI programs, may or may
not adequately summarize this information and the pharmacist
may need to refer to multiple secondary references and/or the
primary literature to properly assess the interaction. Some drug
interaction warnings are based on a single case report or are
simply theoretical. When information is lacking, the pharma-
cist must rely on clinical judgment and, if available, expert con-
sensus to determine the significance of the DDI.
Step 3: Formulating Patient-Specific Recommendations
Once the general significance of each DDI is determined, the
pharmacist can begin to formulate patient-specific recommen-
dations. Most recommendations involve one of the following:
changing the doses, changing the drug, discontinuing a drug,
or monitoring the patient without changing the drug regimen.
Factors that will determine the appropriate action in a given
patient include the doses of the drugs involved, the patient’s
age, any underlying disease states, the efficacy of the current
drug regimen, and whether the patient is experiencing adverse
consequences from the interaction.
Step 4: Communicating Recommendations
Whether written or spoken, the pharmacist should communi-
cate recommendations to the prescriber in an organized
manner. A brief summary of important observations, a clear
recommendation, and a rationale to support the recommen-
dation should be given. The following case examples illus-
trate these principles.
Pharmacokinetics Case
A pharmacist is asked to review the drug regimen of a 57-year-
old woman and provide written recommendations to the
patient’s prescriber. This patient has a history of hypertension,
hyperlipidemia, migraine, and knee pain due to arthritis. Her
drug regimen includes simvastatin 40 mg daily, verapamil SR
240 mg daily (for both migraine prophylaxis and hypertension),
acetaminophen 650 mg 3 times a day daily for arthritis pain, and
sumatriptan 50 mg daily for acute migraine. After identifying
all potential DDIs, determining their clinical significance, and
reviewing the patient’s chart to formulate patient-specific rec-
ommendations, the pharmacist prepares the following recom-
mendations for the prescriber:
Simvastatin/verapamilAssessment. This patient has diagnoses codes for hyperten-
sion, migraines, hyperlipidemia, and has been filling prescrip-
tions for simvastatin 40 mg daily and verapamil SR 240 mg
daily, a combination that is contraindicated due to a significant
DDI.
Recommendation. Consider changing the simvastatin to a sta-
tin that does not interact with verapamil. Rosuvastatin 5 mg
daily and pravastatin 80 mg daily have similar LDL-lowering
effects.
Rationale. Dosages of simvastatin exceeding 10 mg daily are
contraindicated in patients receiving verapamil. Verapamil has
been shown to increase peak simvastatin serum concentrations
by 2.6-fold, increasing the risk of myopathy and rhabdomyoly-
sis. Changing the statin rather than changing verapamil is likely
the best option because verapamil is treating 2 disease states,
hypertension and migraines.
References. Yeo KR, Yeo WW. Inhibitory effects of verapa-
mil and diltiazem on simvastatin metabolism in human liver
microsomes. Br J Clin Pharmacol. 2001;51(5):461-470.
Jacobson TA. Comparative pharmacokinetic interaction pro-
files of pravastatin, simvastatin, and atorvastatin when coad-
ministered with cytochrome P450 inhibitors. Am J Cardiol.
2004;94(9):1140-1146.
Pharmacodynamics Case
A pharmacist is asked to review the drug regimen of a 42-
year-old man and provide written recommendations to the
patient’s prescriber. This patient has a history of seasonal
allergies, anxiety, postherpetic neuralgia, and fatigue. His
drug regimen includes lorazepam 1 mg twice daily for anxi-
ety, amitriptyline 50 mg daily for postherpetic neuralgia, and
cetirizine 10 mg daily for allergies. After identifying all
potential DDIs, determining their clinical significance and
reviewing the patient’s chart to formulate patient-specific rec-
ommendations, the pharmacist prepares the following recom-
mendation for the prescriber:
Concomitant sedating medicationsAssessment. This patient has a diagnosis of chronic fatigue
and is receiving multiple medications that may cause sedation,
including lorazepam, amitriptyline, and cetirizine.
Recommendation. Consider a trial of less-sedating alterna-
tives to each of his medications. Possible alternatives include
(1) a nonsedating serotonin reuptake inhibitor, such as sertra-
line or citalopram, or you could use a nonbenzodiazepine
anxiolytic such as buspirone in place of lorazepam for anxiety,
(2) a topical treatment, such as capsaicin, or a less-sedating
Nelson et al 5
by guest on December 3, 2014jpp.sagepub.comDownloaded from
tricyclic antidepressant, such as nortriptyline, in place of ami-
triptyline for postherpetic neuralgia, and (3) a nasal steroid,
such as fluticasone, or a less-sedating, second-generation anti-
histamine, such as loratadine, in place of cetirizine to treat
nasal allergy symptoms.
Rationale. This recommendation will help reduce and/or
resolve this patient’s fatigue or rule out additive sedative
effects of this patient’s medications as a cause of fatigue.
Limitations
This is a generalized article to help pharmacists recognize and
communicate potentially clinically meaningful DDIs in their
patients. Not all patients will have many chronic medications
or are only taking an interacting medication acutely, which may
limit the external validity of the patient characteristics; however,
the tools provided can be used in all patients. In the selection
process, patients were selected for review by the number of med-
ications filled or the RxRisk score; these differences in the selec-
tion processes may introduce small differences in patient
demographics of the study; they do not affect the overall results.
Additionally, there were some significant changes in the DRRC
during this time frame. In January 2006, Medicare Part D went
into effect, and in November 2008 the number of patients
selected for review was cut from 300 to 150 per month.
Conclusion
Clinically meaningful DDIs are somewhat common, especially
in patients with complex medication regimens. Using a sys-
tematic approach for identifying and intervening on DDI is
important, such as (1) identifying the DDI, (2) determining
clinical significance, (3) formulating patient-specific recom-
mendations, and (4) communicating recommendations.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to
the research, authorship, and/or publication of this article.
Funding
The author(s) received the following financial support for the research,
authorship, and/or publication of this article: Dr. Oderda received fund-
ing from the Utah Department of Health to support the Drug Regimen
Review Center.
References
1. Muir AJ, Sanders LL, Wilkinson WE, Schmader K. Reducing
medication regimen complexity: a controlled trial. J Gen Intern
Med. 2001;16(2):77-82.
2. Ernst FR, Grizzle AJ. Drug-related morbidity and mortality:
updating the cost-of-illness model. J Am Pharm Assoc (Wash).
2001;41(2):192-199.
3. Preventing Medication Errors: Quality Chasm Series. Washington,
DC: The National Academies Press; 2007.
4. Jankel CA, Speedie SM. Detecting drug interactions: a review of
the literature. DICP. 1990;24(10):982-989.
5. Aparasu R, Baer R, Aparasu A. Clinically important potential
drug-drug interactions in outpatient settings. Res Social Adm
Pharm. 2007;3(4):426-437.
6. LaFleur J, McBeth C, Gunning K, Oderda L, Steinvoort C, Oderda
GM. Prevalence of drug-related problems and cost-savings opportu-
nities in medicaid high utilizers identified by a pharmacist-run drug
regimen review center. J Manag Care Pharm. 2006;12(8):677-685.
7. Phelan KM, Mosholder AD, Lu S. Lithium interaction with the
cyclooxygenase 2 inhibitors rofecoxib and celecoxib and other
nonsteroidal anti-inflammatory drugs. J Clin Psychiatry. 2003;
64(11):1328-1334.
8. Langballe EM, Engdahl B, Selbaek G, Nordeng H. Concomitant
use of anti-dementia drugs with psychotropic drugs in Norway–
a population-based study. Pharmacoepidemiol Drug Saf. 2011;
20(12):1319-1326.
9. Hines LE, Murphy JE. Potentially harmful drug-drug interactions
in the elderly: a review. Am J Geriatr Pharmacother. 2011;9(6):
364-377.
10. Farley JF, Harley CR, Devine JW. A comparison of comorbidity
measurements to predict healthcare expenditures. Am J Manag
Care. 2006;12(2):110-119.
11. Sloan KL, Sales AE, Liu CF, et al. Construction and characteris-
tics of the RxRisk-V: a VA-adapted pharmacy-based case-mix
instrument. Med Care. 2003;41(6):761-774.
12. Fishman PA, Goodman MJ, Hornbrook MC, Meenan RT,
Bachman DJ, O’Keeffe Rosetti MC. Risk adjustment using
automated ambulatory pharmacy data: the RxRisk model. Med
Care. 2003;41(1):84-99.
13. StataCorp. 2011. Stata Statistical Software: Release 12. College
Station, TX: StataCorp LP).
14. Stockley IH, Baxter K. Stockley’s Drug Interactions: A Source Book
of Interactions, Their Mechanisms, Clinical Importance and Man-
agement. 7th ed. London; Chicago: Pharmaceutical Press; 2006.
15. Micromedex Healthcare Series. Greenwood Village, CO: Thomson
Reuters (Healthcare) Inc; Updated periodically.
16. Lexi-Comp Online. Hudson, OH: Lexi-Comp, Inc.; Updated
periodically.
17. Hansten PD, Horn JR. The Top 100 Drug Interactions 2012: A
Guide to Patient Management. Clearwater, FL: H & H Publica-
tions; 2012.
18. Drug Facts & Comparisons. Facts & Comparisons1 eAnswers
[online]. Baltimore, MD: Wolters Kluwer Health, Inc.; Updated
periodically.
19. Cash JJ. Alert fatigue. Am J Health Syst Pharm. 2009;66(23):
2098-2101.
20. Saverno KR, Hines LE, Warholak TL, et al. Ability of pharmacy
clinical decision-support software to alert users about clinically
important drug-drug interactions. J Am Med Inform Assoc.
2011;18(1):32-37.
21. Abarca J, Colon LR, Wang VS, et al. Evaluation of the performance
of drug-drug interaction screening software in community and hos-
pital pharmacies. J Manag Care Pharm. 2006;12(5):383-389.
22. Hazlet TK, Lee TA, Hansten PD, et al. Performance of commu-
nity pharmacy drug interaction software. J Am Pharm Assoc
(Wash). 2001;41(2):200-204.
6 Journal of Pharmacy Practice
by guest on December 3, 2014jpp.sagepub.comDownloaded from