iccs e-newsletter csi spring 2012 weina chen, md, phd medical director, hematopathology...
TRANSCRIPT

ICCS e-newsletter CSISpring 2012
Weina Chen, MD, PhD
Medical Director, Hematopathology
Ameripath/Quest Diagnostics
Dallas, Texas
Case History
The patient is a 70-year old female presented with mild leukocytosis. She has no prior history of any significant diseases and is asymptomatic.

Complete blood count
WBC 10.70NE 50%LY 39.4%MO 9.3%EO 0.7%BASO 0.6%
RBC 4.41HGB 12.7HCT 37.7%MCV 85.5MCHC 33.70RDW 12.6PLT 211.0

Work-up and evaluation
Bone marrow (BM) aspirate and biopsy were procured.
Flow cytometric analysis was performed on marrow aspirate and results from selected 4-color tubes are provided for review.

Flow cytometric analysis
• Acquisition Beckman Coulter Epics XL (FCS2.0, System II)
• Analyzed by Paint-A-Gate software (adapted to Coulter)
• Tubes (FITC/PE/ECD/PC5)
– Tube 1: Kappa/lambda/45/19+20
– Tube 2: 5/19/45/10
– Tube 3 : 8/4/45/38
– Tube 4: 15/117/45/34
– Tube 5: 20/10/19/38
– Tube 6: FMC-7/23/5/19
– Tube 7: Kappa/Lambda/5/19

Tube 1: Kappa/lambda/45/19+20
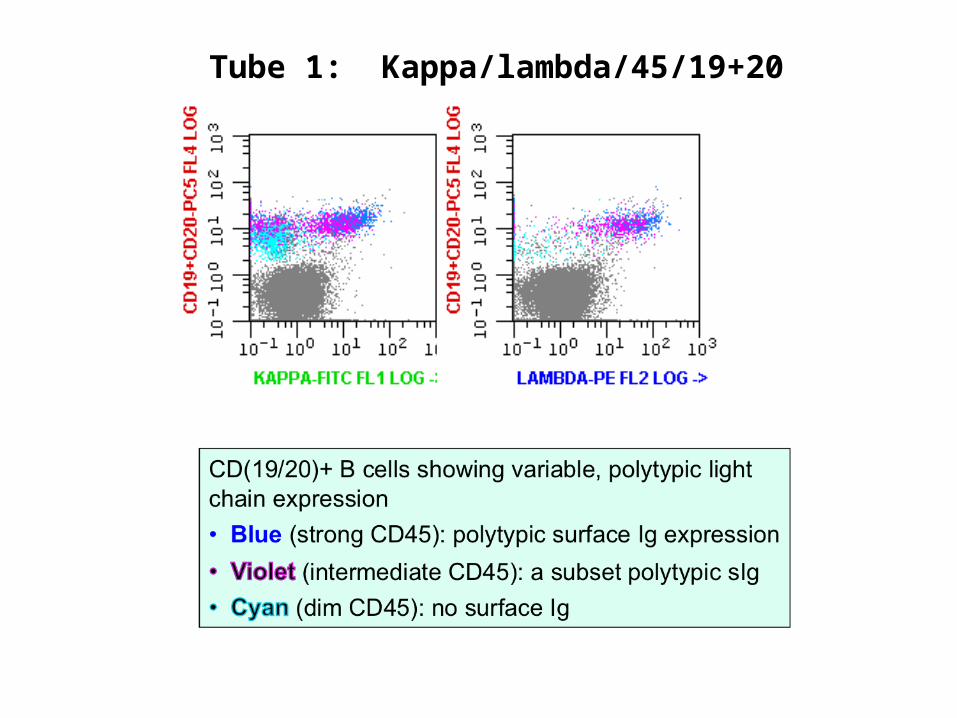
Tube 1: Kappa/lambda/45/19+20

Tube 2: 5/19/45/10

Tube 3 : 8/4/45/38

Tube 4: 15/117/45/34

Tube 5: 20/10/19/38

Tube 6: FMC-7/23/5/19

Tube 7: Kappa/Lambda/5/19
[In addition, CD13-, CD33- (data not shown); Tdt not tested]
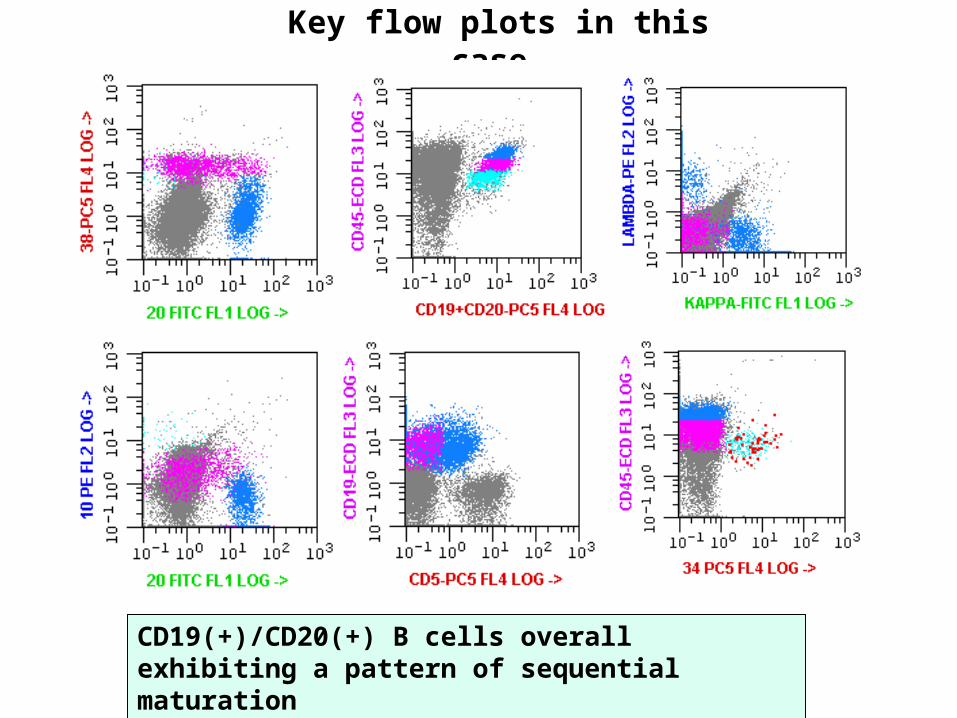
Key flow plots in this case
CD19(+)/CD20(+) B cells overall exhibiting a pattern of sequential maturation

Morphologic evaluation
Marrow infiltrated by abundant small to medium-sized lymphoid cells with mature morphologic features although nuclear irregularity/convolution and small cytoplasmic vacuoles observed in a few scattered lymphoid cells.

CD20 CD34CD79a
Tdt CD10
Immunohistochemical evaluation
A prominent CD79a(+) B-lymphoid hyperplasia of mostly CD10(+) B lymphocytes with increased Tdt(+) cells, some in clusters exceeding 3 or 4 cells

Questions…
• There is an expansion of B cells overall exhibiting a spectrum of maturation.
• Are these normal maturing B-cell precursors (hematogones) or B-lymphoblasts?

A few words on hematogones…
• Hematogones always express consistent, reproducible, complex spectrum of sequential antigen expression and lack aberrant antigen expression.
• This defines hematogones into three stages of maturation– Stage 1 hematogones express CD34, high levels of CD10 and CD38, a
moderate level of CD22, and absence of CD20.
– Intermediate stage 2 hematogones downregulate CD34 completely and CD10 partially, while increasing expression of CD22 and CD20.
– Stage 3 hematogones upregulate CD20 expression reaching the intensity of mature B cells, and CD10 and CD38 are slightly down-regulated with increasing expression of polytypic surface immunoglobulin light chains.
– Subsequently, these cells mature into CD20(+), CD10(-) mature B cells.
– CD5 is expressed on normal, polytypic B cells in a continuum, predominantly at later stages of maturation, specifically on stage 3 hematogones and mature B cells.

Comparison to a case with hematogone hyperplasia
A case with hematogone (HG) hyperplasia case (bottom plots):
Blue, mature B cells; Green, stage 2+3 HG; yellow, stage I HG

Comparison to a case with hematogone hyperplasia
A case with hematogone (HG) hyperplasia case (bottom plots):
Blue, mature B cells; Green, stage 2+3 HG; yellow, stage I HG
Questions…
• These B cells exhibit a spectrum of maturation reminiscent of hematogones and unusual for neoplastic lymphoblasts.
• Are these hematogones???

Answer…
• No• These are B-lymphoblasts.
• The key finding in this case (on BM sample)
– Cytogenetics: 46, XX, t(9;22)(q34;q11.2)[17]/46, XX [3]
– Positive FISH for t(9;22)/BCR-ABL1 in 79% of interphase cells
Answer…
• Differential diagnosis
– An early chronic myelogenous leukemia (CML) with background hematogone hyperplasia (but the usual morphologic features of CML not apparent)
– Lymphoid blast crisis of CML (but no history of CML)
– An early B-lymphoblastic leukemia with t(9;22)(q34;q11.2);BCR-ABL1

Favored Diagnosis
B-lymphoblastic leukemia with t(9;22)(q34;q11.2);BCR-ABL1
Based on the high percent of t(9;22) positive cells (~70%), the entire B-cell population or the majority of B cells including polytypic B cells seems neoplastic.

A few words on B-lymphoblastic leukemia with t(9;22)(q34;q11.2);BCR-ABL1
• The most frequently observed chromosomal abnormality in adult B-ALL (25% vs. 3-5% in children)
• Involving the ABL1 oncogene on chromosome 9 and the guanosine triphosphate–binding protein BCR on chromosome 22
• The resultant fusion protein having abnormal tyrosine kinase activity, leading to disturbances in proliferation, survival, and adhesion
• In about 70% of cases of BCR-ABL1+ B-ALL, the expressed protein being 190 kDa, rather than the 210 kDa typically seen in CML
• Associated with a poor prognosis in both children and adults
Unusual features in this case• Unusual presentation: close to normal CBC with differential at
presentation
• Unusual morphology: mature morphologic features with mild cytological atypia
• Unusual immunophenotype: maturation spectrum reminiscent of hematogones (with only subtle deviation)
• Unusual, indolent clinical course
– Follow-up BM in 5 months (with only imatinib mesylate tx)
• Close to normal CBC, asymptomatic
• Persistent, but decreased B-lymphoblasts (similar phenotype)
• RT-PCR: positive BCR-ABL1, p190, further supporting B-ALL

What are the clues to avoid misdiagnosis?
• No apparent causes for hematogone hyperplasia• Common causes for hematogone hyperplasia:
• Reactive conditions: AIDS, immune dysregulation, copper deficiency), BM involved by metastatic tumors• Regenerative conditions: post-chemotherapy and stem-cell transplant• Relatively high number of hematogones in children
• Subtle immunophenotypic deviation from hematogones• Less distinct “ladder” of CD45 on subsets of B cells• Tdt positive cells, some in clusters exceeding 3 or 4 cells
• The need to add new markers to distinguish hematogones from lymphoblasts
• CD81, CD123
Take home messages
• The immunophenotype of B-lymphoblasts is variable.
• While the majority of cases having distinct immunophenotypic aberration deviated from hematogones, rare cases with immunophenotypic feature reminiscent of hematogones do exist.
• Careful immunophenotypic analysis, clinical correlation for causes of hematogone hyperplasia, ancillary studies (cytogenetics, FISH/molecular studies) are the key elements to reach a correct diagnosis.

References1. Weir EG, Cowan K, LeBeau P, Borowitz MJ. A limited antibody panel can distinguish B-precursor acute lymphoblastic leukemia from normal B precursors with four color flow cytometry: implications for residual disease detection. Leukemia 1999;13:558-67.
2. McKenna RW, Washington LT, Aquino DB, Picker LJ, Kroft SH. Immunophenotypic analysis of hematogones (B-lymphocyte precursors) in 662 consecutive bone marrow specimens by 4-color flow cytometry. Blood 2001;98:2498-507.
3. McKenna RW, Asplund SL, Kroft SH. Immunophenotypic analysis of hematogones (B-lymphocyte precursors) and neoplastic lymphoblasts by 4-color flow cytometry. Leuk Lymphoma 2004;45:277-85.
4. Chen W, Karandikar NJ, McKenna RW, Kroft SH. Stability of leukemia-associated immunophenotypes in precursor B-lymphoblastic leukemia/lymphoma: a single institution experience. Am J Clin Pathol 2007;127:39-46.
5. Seegmiller AC, Kroft SH, Karandikar NJ, McKenna RW. Characterization of immunophenotypic aberrancies in 200 cases of B acute lymphoblastic leukemia. Am J Clin Pathol 2009;132:940-9.
6. Loken MR, Shah VO, Dattilio KL, Civin CI. Flow cytometric analysis of human bone marrow. II. Normal B lymphocyte development. Blood 1987;70:1316-24.
7. Ryan DH, Chapple CW, Kossover SA, Sandberg AA, Cohen HJ. Phenotypic similarities and differences between CALLA-positive acute lymphoblastic leukemia cells and normal marrow CALLA-positive B cell precursors. Blood 1987;70:814-21.
8. Campana D, Coustan-Smith E. Detection of minimal residual disease in acute leukemia by flow cytometry. Cytometry 1999;38:139-52.
9. Fuda FS, Karandikar NJ, Chen W. Significant CD5 expression on normal stage 3 hematogones and mature B Lymphocytes in bone marrow. Am J Clin Pathol 2009;132:733-7.

10. Hurwitz CA, Gore SD, Stone KD, Civin CI. Flow cytometric detection of rare normal human marrow cells with immunophenotypes characteristic of acute lymphoblastic leukemia cells. Leukemia 1992;6:233-9.
11. Hurwitz CA, Loken MR, Graham ML, et al. Asynchronous antigen expression in B lineage acute lymphoblastic leukemia. Blood 1988;72:299-307.
12. Kurec AS, Belair P, Stefanu C, Barrett DM, Dubowy RL, Davey FR. Significance of aberrant immunophenotypes in childhood acute lymphoid leukemia. Cancer 1991;67:3081-6.
13. Muzzafar T, Medeiros LJ, Wang SA, Brahmandam A, Thomas DA, Jorgensen JL. Aberrant underexpression of CD81 in precursor B-cell acute lymphoblastic leukemia: utility in detection of minimal residual disease by flow cytometry. Am J Clin Pathol 2009;132:692-8.
14. Hassanein NM, Alcancia F, Perkinson KR, Buckley PJ, Lagoo AS. Distinct expression patterns of CD123 and CD34 on normal bone marrow B-cell precursors ("hematogones") and B lymphoblastic leukemia blasts. Am J Clin Pathol 2009;132:573-80.
15. Muehleck SD, McKenna RW, Gale PF, Brunning RD. Terminal deoxynucleotidyl transferase (TdT)-positive cells in bone marrow in the absence of hematologic malignancy. Am J Clin Pathol 1983;79:277-84.
16. Rimsza LM, Larson RS, Winter SS, et al. Benign hematogone-rich lymphoid proliferations can be distinguished from B-lineage acute lymphoblastic leukemia by integration of morphology, immunophenotype, adhesion molecule expression, and architectural features. Am J Clin Pathol 2000;114:66-75.
17. Sutton L, Vusirikala M, Chen W. Hematogone hyperplasia in copper deficiency. Am J Clin Pathol 2009;132:191-9; quiz 307.