icc keynote presentation 2013 n ryan
TRANSCRIPT

RECENT ADDITIONS IN THE
TREATMENT OF COUGH
D R . N I C O L E R Y A N , A / D I P A P P S C , B S C , P H D
P R I O R I T Y R E S E A R C H C E N T R E F O R A S T H M A
A N D R E S P I R A T O R Y D I S E A S E
F A C U L T Y O F H E A L T H A N D M E D I C I N E
T H E U N I V E R S I T Y O F N E W C A S T L E
A N D H U N T E R M E D I C A L R E S E A R C H I N S T I T U T E ( H M R I )
1 S T I N T E R N A T I O N A L C H I N E S E C O U G H C O N F E R E N C E ,
8 - 1 0 N O V E M B E R 2 0 1 3 .
I C C 2 0 1 3 K E Y N O T E S P E A K E R P R E S E N T A T I O N |
W W W . N E W C A S T L E . E D U . A U
2
Recent Additions in the Treatment of Cough
• What Are They?
• Non-Pharmacological (Behavioural)
• Pharmacological
• Why Needed?
• Cough: Huge clinical problem
• Worldwide
• High prevalence of ‘Refractory’
Cough
• Treatments limited and ineffective

I C C 2 0 1 3 K E Y N O T E S P E A K E R P R E S E N T A T I O N |
W W W . N E W C A S T L E . E D U . A U3
• Where Did They Come From?
• Otolaryngology: Recognition of upper
airway involvement
• Proximity
• Inputs from upper and lower airways
into larynx/pharynx
• Laryngeal Hypersensitivity
• Cough Hypersensitivity Syndrome
• Allied Health: Speech
Pathologists/Physiotherapists
Recent Additions in the Treatment of Cough

4
•Refractory chronic cough primarily occurs in:• middle-aged women w long-standing dry CC
• often follows a RTI
• causes significant symptoms and quality of life impairment.
• Potential explanations for refractory chronic cough:• organ-specific autoimmune disease of the airways
• neurogenic airway inflammation
• non-acid gastro-oesophageal reflux
• a laryngeal sensory neuropathy or irritability.
REFRACTORY CHRONIC COUGH
I C C 2 0 1 3 K E Y N O T E S P E A K E R P R E S E N T A T I O N |
W W W . N E W C A S T L E . E D U . A U

5
Laryngeal Hypersensitivity
common element
different initiating mechanisms
Inflammation
injury from chemical and/or mechanical causes
much in common with neuralgias and
neuropathic pain syndromes
recognised ‘trigger’
Provides new insights
potential mechanisms
treatments for refractory cough
I C C 2 0 1 3 K E Y N O T E S P E A K E R P R E S E N T A T I O N |
W W W . N E W C A S T L E . E D U . A U

NON-PHARMACOLOGICAL TREATMENTS FOR CC
• Speech Pathology
• Gay et al, J Clin Psychiatry. 1987
• Blager et al, J Commun Disord. 1988
• Murry et al, Annals of Otology, Rhinology &
Laryngology. 2006
• SPEICH-C (Vertigan, 2006; Ryan, 2009 & 2010)
• Physiotherapy (Patel, 2011)
• Psychotherapy
• Gay & Blager (case reports include psychotherapy)
• and SPEICH-C (Vertigan RCT, Ryan studies include
Psychoeducational counselling)
I C C 2 0 1 3 K E Y N O T E S P E A K E R P R E S E N T A T I O N |
W W W . N E W C A S T L E . E D U . A U6

FOCUS: SPEECH PATHOLOGY MANAGEMENT FOR
COUGH
I C C 2 0 1 3 K E Y N O T E S P E A K E R P R E S E N T A T I O N |
W W W . N E W C A S T L E . E D U . A U7

I C C 2 0 1 3 K E Y N O T E S P E A K E R P R E S E N T A T I O N |
W W W . N E W C A S T L E . E D U . A U8
Demographic data and co-morbid medical conditions of study
participants that had been treated before inclusion in the study, Vertigan
et al, Thorax 2006.
Mean (SD) age (years) 59.4 (13.6)
Sex (M/F) 64/23
Asthma* 18 (20.7%)
Reflux_ 41 (47%)
ACE inhibitors 10 (11.5%)
Allergies 52 (59.8%)
PNDS` 44 (50.6%)
Smoking 2 (2.3%)ACE, angiotensin converting enzyme; PNDS, postnasal drip syndrome. *Previous asthma treatment included inhaled corticosteroid
and long acting bronchodilator. _Previous reflux treatment was proton pump inhibitors. `Previous PNDS treatment included topical
nasal steroids and ingested antihistamines.
I C C 2 0 1 3 K E Y N O T E S P E A K E R P R E S E N T A T I O N |
W W W . N E W C A S T L E . E D U . A U9
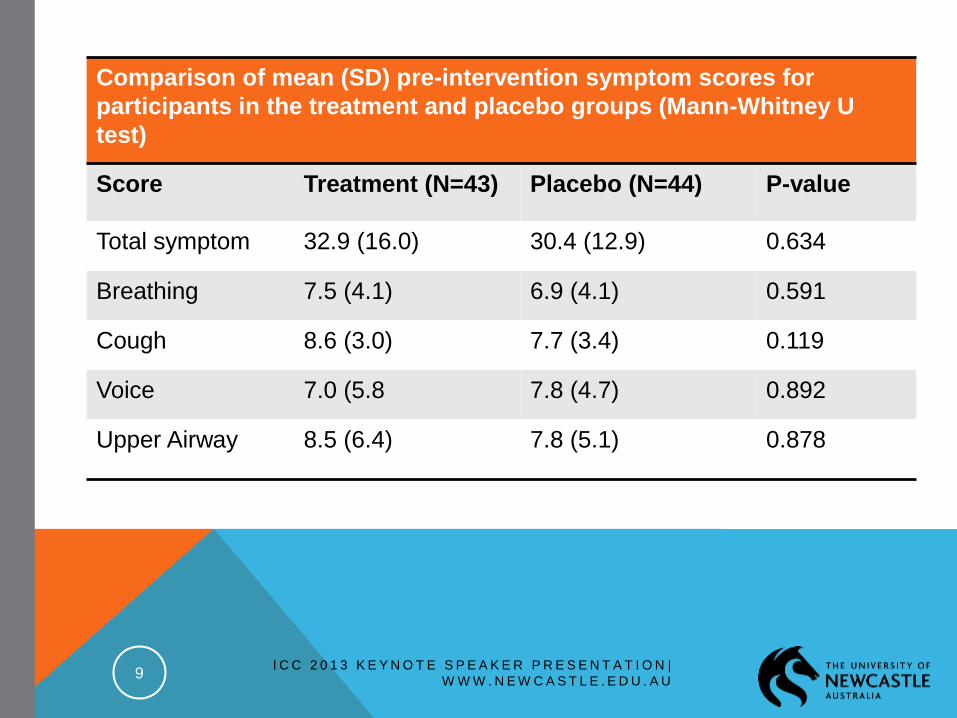
Comparison of mean (SD) pre-intervention symptom scores for
participants in the treatment and placebo groups (Mann-Whitney U
test)
Score Treatment (N=43) Placebo (N=44) P-value
Total symptom 32.9 (16.0) 30.4 (12.9) 0.634
Breathing 7.5 (4.1) 6.9 (4.1) 0.591
Cough 8.6 (3.0) 7.7 (3.4) 0.119
Voice 7.0 (5.8 7.8 (4.7) 0.892
Upper Airway 8.5 (6.4) 7.8 (5.1) 0.878
I C C 2 0 1 3 K E Y N O T E S P E A K E R P R E S E N T A T I O N |
W W W . N E W C A S T L E . E D U . A U10
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
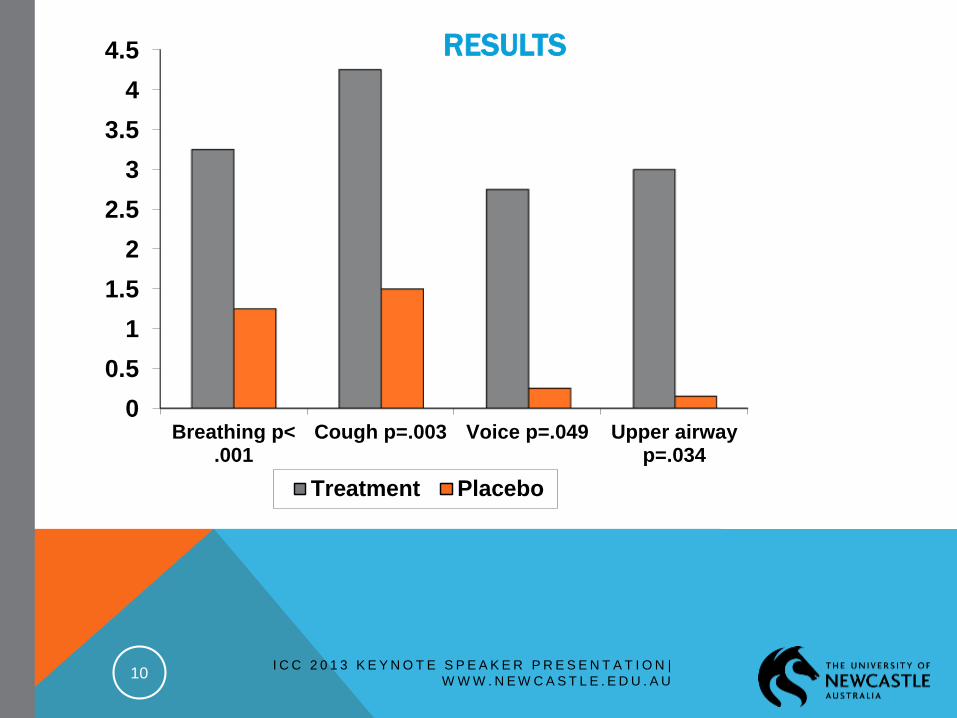
Breathing p<.001
Cough p=.003 Voice p=.049 Upper airwayp=.034
Treatment Placebo
RESULTS

CAUSE FOR FURTHER INVESTIGATION
FROM THE VERTIGAN RCT INVESTIGATING THE
EFFICACY OF SPEECH PATHOLOGY
MANAGEMENT OF CHRONIC COUGH THE
FOLLOWING QUESTIONS REMAINED:
1) MECHANISM BEHIND IMPROVEMENT
2) COUGH SUPPRESSION=REDUCED COUGH
SENSITIVITY?
3) LARYNGEAL HYPERSENSITIVITY: PVCM/VCD
PRESENTS WITH COUGH, DOES SPEECH
PATHOLOGY INTERVENTION ADDRESS BOTH?
11I C C 2 0 1 3 K E Y N O T E S P E A K E R P R E S E N T A T I O N |
W W W . N E W C A S T L E . E D U . A U

12
PVCM and EAHR are both manifestations of laryngeal
hypersensitivity. 56% of CC patients have PVCM.
I C C 2 0 1 3 K E Y N O T E S P E A K E R P R E S E N T A T I O N |
W W W . N E W C A S T L E . E D U . A U
-1.0 -0.5 0.5 1.0 1.5 2.0
-1.50
-1.25
-1.00
-0.75
-0.50
-0.25
0.25
0.50
0.75
Log CRS
Lo
g D
RS
r= -0.65, p= 0.02

I C C 2 0 1 3 K E Y N O T E S P E A K E R P R E S E N T A T I O N |
W W W . N E W C A S T L E . E D U . A U13
Subject Characteristics, Median (IQR) unless otherwise stated
Number, (M/F) 17 (8/9)
Age, years 61 (20)
Age Range, years 34-83
Cough Duration, months 60 (147)
FEV1, %predicted 88.2 (16.7)
FVC, %predicted 88.5 (20.3)
Auditory perceptual voice analysis, % abnormal 63

I C C 2 0 1 3 K E Y N O T E S P E A K E R P R E S E N T A T I O N |
W W W . N E W C A S T L E . E D U . A U14
pre Rx post Rx0
5
10
15
20
*
LC
Q S
co
re (
un
its
)
Pre Rx Post Rx0
1
2
3
4
5
6
7
8
9
10
11
*
Co
ug
h S
co
re (
un
its)
P=0.002
P=0.003
P=0.04
Results
pre Rx post Rx0
1
2
3
4
5
6
7
8
*
LD
Q S
co
re (
un
its)

I C C 2 0 1 3 K E Y N O T E S P E A K E R P R E S E N T A T I O N |
W W W . N E W C A S T L E . E D U . A U15
Change in C5 and CT after Speech Pathology
Intervention on Cough Reflex Sensitivity
Baseline Post Rx0
1
2
3
p<0.0001
Co
ug
h R
efl
ex S
en
sit
ivit
y
Lo
g1
0C
5 (
uM
ol/
L)
Baseline Post Rx0
1
2
3p=0.001
Lo
g10C
ou
gh
Th
resh
old
(uM
ol/
L)
Mea
n
I C C 2 0 1 3 K E Y N O T E S P E A K E R P R E S E N T A T I O N |
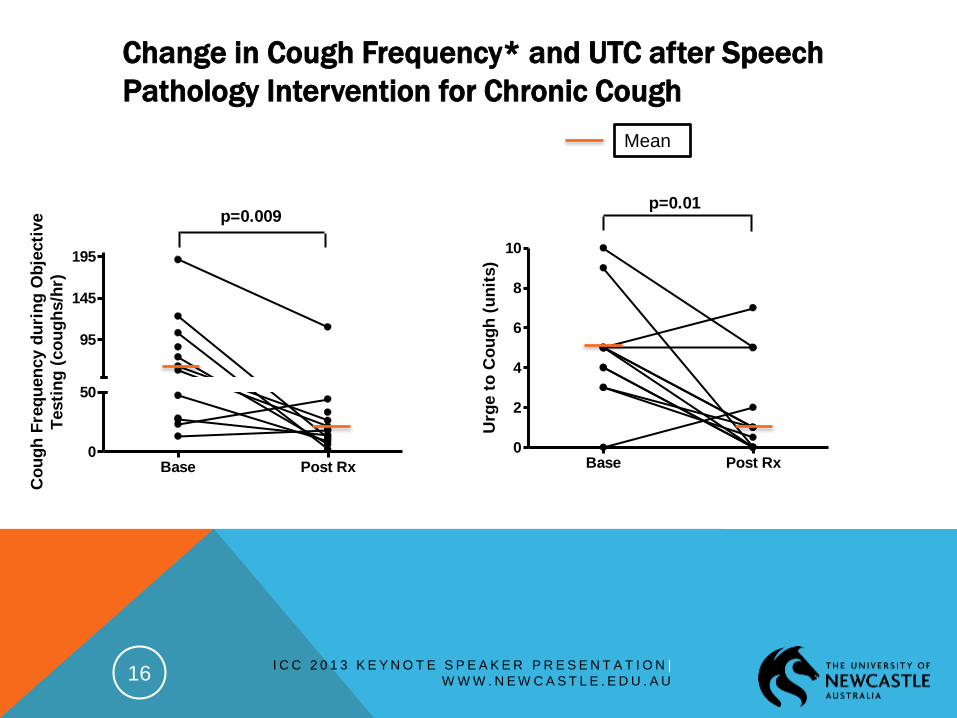
W W W . N E W C A S T L E . E D U . A U16
Change in Cough Frequency* and UTC after Speech
Pathology Intervention for Chronic Cough
Base Post Rx0
50
p=0.009
95
145
195
Co
ug
h F
req
uen
cy d
uri
ng
Ob
jecti
ve
Testi
ng
(co
ug
hs/h
r)
Base Post Rx0
2
4
6
8
10
p=0.01
Urg
e t
o C
ou
gh
(u
nit
s)
Mean

SPEECH PATHOLOGY TREATMENT FOR
OUTPATIENTS
SP standard treatment for adult chronic cough
patients in Australia, ref: CICADA Australian cough
guidelines and assessment, 2010.
At JHH in Newcastle the SP program is tailored to
individuals based on assessment and ongoing
management.
Recently, the LCM was utilised into the cough clinic
with the intent of having an objective cough measure
before and after treatment.
I C C 2 0 1 3 K E Y N O T E S P E A K E R P R E S E N T A T I O N |
W W W . N E W C A S T L E . E D U . A U17

18
PHARMACOLOGICAL TREATMENTS FOR CCChronic/Neuropathic Pain medication
Gabapentin
Case Series: 1) Lee & Woo, Ann Otol Rhinol Laryngol
2005; 2) Mintz & Lee, Am J Med, 2006
RCT: Ryan et al, The Lancet, 2012
Retrospective study: Van de Kerkhove et al, Cough, 2012
Amitriptyline
Case Series: Bastian et al, Otolaryngol Head Neck Surg,
2006
RCT: Jeyakumar et al, Laryngoscope, 2006
Pregabalin
Retrospective Audit: Halum et al, Laryngoscope, 2009 for
SLN
I C C 2 0 1 3 K E Y N O T E S P E A K E R P R E S E N T A T I O N |
W W W . N E W C A S T L E . E D U . A U19

Neuropathic Pain
abnormal sensation
pain triggered by a
lower level exposure
to a known painful
stimulus
pain triggered by a
non-painful stimulus
20
Refractory CC
abnormal throat
sensation
increased cough
sensitivity in response
to known tussigens
cough triggered in
response to
nontussive stimuli
such as talking or cold
air
neuropathic response
I C C 2 0 1 3 K E Y N O T E S P E A K E R P R E S E N T A T I O N |
W W W . N E W C A S T L E . E D U . A U
suggests sensitisation
of the cough reflex

FOCUS: GABAPENTIN FOR COUGH
I C C 2 0 1 3 K E Y N O T E S P E A K E R P R E S E N T A T I O N |
W W W . N E W C A S T L E . E D U . A U21

AIM: Establish whether gabapentin is an effective
treatment in patients with refractory CC.
HOW: Investigate subjective and objective
measures of cough before, during and after
treatment.
Hypothesis: People with RCC will have ↓ cough
severity and CF & ↑ cough quality of life after Rx
with gabapentin compared to placebo.
I C C 2 0 1 3 K E Y N O T E S P E A K E R P R E S E N T A T I O N |
W W W . N E W C A S T L E . E D U . A U22

PARTICIPANT CHARACTERISTICS AT
BASELINE
Placebo Gabapentin p-value
N 30 32
Age, yr # 60·9 (12·9) 62·7 (14·0) 0·596
Male/Female 10/20 12/20 0·732
Non/ex-smoker 16/14 20/12 0·465
Pack years * 5 (13) 4 (5) 0·101
Cough duration,
months *
48 (138) 36 (132) 0·746
# Mean(sd), student’s t test; * Median (IQR), Wilcoxon ranksum test
I C C 2 0 1 3 K E Y N O T E S P E A K E R P R E S E N T A T I O N |
W W W . N E W C A S T L E . E D U . A U23

PARTICIPANT CHARACTERISTICS AT
BASELINEEfficacy Variables Placebo Gabapentin p-value
LCQ # 12·1 (3·9) 13·3 (3·1) 0·145
Cough VAS, mm # 44·2 (21·3) 43·6 (29·6) 0·934
CRS C5, GEM
(logSD), µM
4·31 (0·49) 6.31 (0·6) 0·297
Cough frequency,
GEM (logSD)
coughs/hour
68·8 (1·9) 45·3 (1·9) 0·102
# Mean(sd), student’s t test; * Median (IQR), Wilcoxon ranksum test; § n(%), chi square test or Fisher’s exact test.
I C C 2 0 1 3 K E Y N O T E S P E A K E R P R E S E N T A T I O N |
W W W . N E W C A S T L E . E D U . A U24

I C C 2 0 1 3 K E Y N O T E S P E A K E R P R E S E N T A T I O N |
W W W . N E W C A S T L E . E D U . A U25
Gabapentin/Placebo Dose Schedule

INCLUSION CRITERIA
26
• Chronic cough (> 8 weeks duration)
• Male or female between ages of 18 and 80 years
• Non-smoker or ex-smoker
•Negative investigations and/or treatment trials:
• asthma, GORD and rhinitis
•Informed consent obtained
I C C 2 0 1 3 K E Y N O T E S P E A K E R P R E S E N T A T I O N |
W W W . N E W C A S T L E . E D U . A U

27
Randomisation
1. Assessed for eligibility
(n =65)
2. Excluded (n = 3)
3. Randomised (n = 62)
4a. Allocated to
intervention
(Gabapentin) (n = 32)
Allo
ca
tio
n
En
rolm
en
t
4b. Allocated to
intervention
(Placebo) (n = 30)
Fo
llo
w u
p 6a. Lost to follow up
(n = 2) (DNA) Discontinued intervention (n = 4)
6b. Lost to follow up (n = 0) Discontinued intervention
(n = 4)
An
aly
sis
7a. Analysed (n = 32) Excluded from analysis
(n = 0)
7b. Analysed (n = 30) Excluded from analysis
(n = 0)
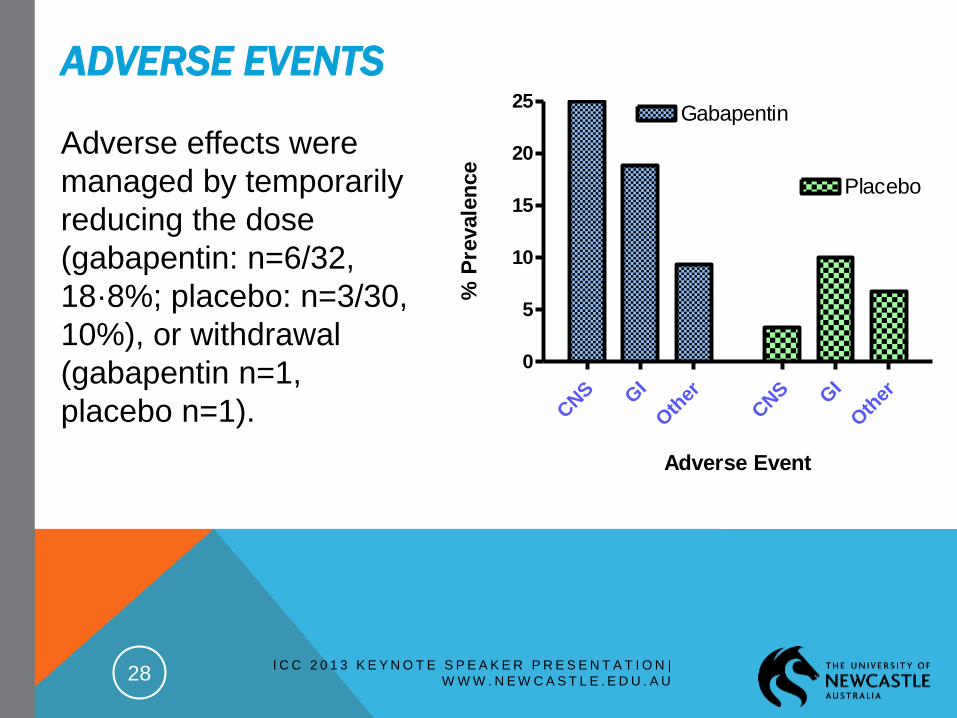
ADVERSE EVENTS
I C C 2 0 1 3 K E Y N O T E S P E A K E R P R E S E N T A T I O N |
W W W . N E W C A S T L E . E D U . A U28
CNS G
I
Oth
er
CNS G
I
Oth
er
0
5
10
15
20
25Gabapentin
Placebo
Adverse Event%
Pre
vale
nce
Adverse effects were
managed by temporarily
reducing the dose
(gabapentin: n=6/32,
18·8%; placebo: n=3/30,
10%), or withdrawal
(gabapentin n=1,
placebo n=1).

PRIMARY OUTCOME: THE LCQ
29
0 1 2 3 4 510
11
12
13
14
15
16
17
18
Visit No
LC
Q
On Rx Reducing Rx to
Withdrawal
P=0.004
I C C 2 0 1 3 K E Y N O T E S P E A K E R P R E S E N T A T I O N |
W W W . N E W C A S T L E . E D U . A U
Gabapentin

OUTCOME MEASURE: COUGH SEVERITY BY VAS
30
0 1 2 3 4 520
35
50
65
Visit No
Co
ug
h V
AS
(m
m)
Gabapentin
On Rx Reducing Rx to
Withdrawal
I C C 2 0 1 3 K E Y N O T E S P E A K E R P R E S E N T A T I O N |
W W W . N E W C A S T L E . E D U . A U
P=0.029
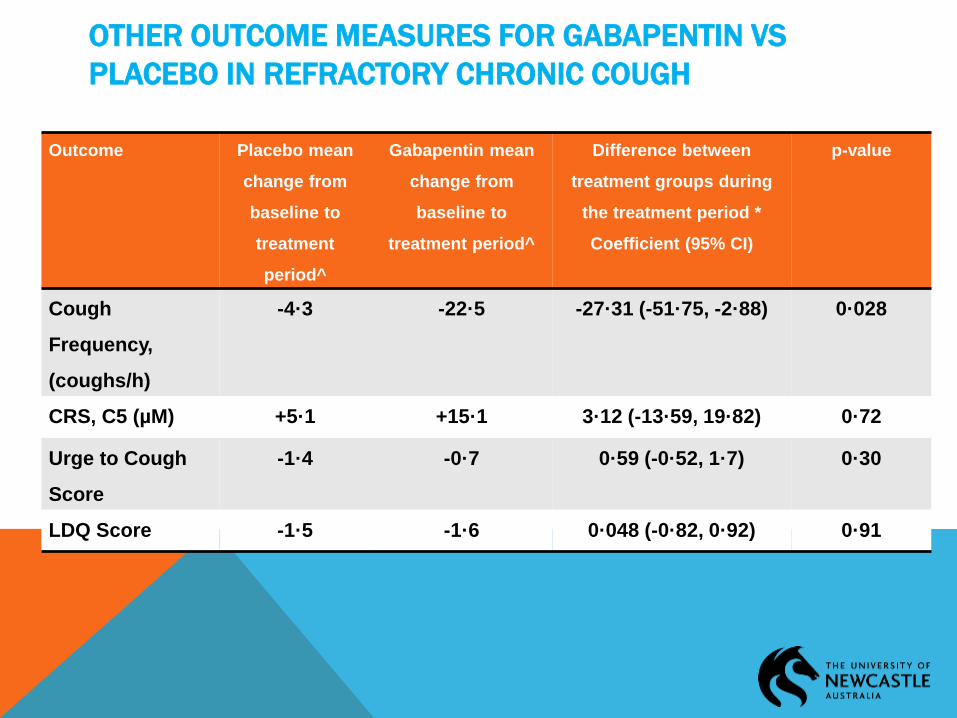
OTHER OUTCOME MEASURES FOR GABAPENTIN VS
PLACEBO IN REFRACTORY CHRONIC COUGH
Outcome Placebo mean
change from
baseline to
treatment
period^
Gabapentin mean
change from
baseline to
treatment period^
Difference between
treatment groups during
the treatment period *
Coefficient (95% CI)
p-value
Cough
Frequency,
(coughs/h)
-4·3 -22·5 -27·31 (-51·75, -2·88) 0·028
CRS, C5 (µM) +5·1 +15·1 3·12 (-13·59, 19·82) 0·72
Urge to Cough
Score
-1·4 -0·7 0·59 (-0·52, 1·7) 0·30
LDQ Score -1·5 -1·6 0·048 (-0·82, 0·92) 0·91

CENTRAL SENSITISATION RESPONSE TO GABAPENTIN
32
LCQ Placebo-CS Placebo+CS Gaba-CS Gaba+CS p-value
N, (%) 10/30 (33·3%) 20/30 (66·7%) 13/32 (40·6%) 19/32 (59·4%)
Baseline, V1 12·2(9·9) 12·9(9·5) 13·9(9·5) 13·5(8·6)
V2 14·1(11·5) 13·6(10·7) 15·0(9·5) 16·2(10·1) ≥0·213
V3 13·7(12·2) 14·2(10·4) 15·3(8·7) 17·1(10·6)* 0·001
Adjusted p-value for significance is 0 ·0042, *p=0·0006 v Placebo-CS, p=0·0003 v Placebo+CS, p=0·021 v GABA-CS, V=Visit.
I C C 2 0 1 3 K E Y N O T E S P E A K E R P R E S E N T A T I O N |
W W W . N E W C A S T L E . E D U . A U
CONCLUSIONS
Double-blind RCT investigating the Rx of refractory
chronic cough w gabapentin.
Gabapentin improved patients’ symptoms; cough
quality of life, cough severity, and cough
frequency.
Therefore may be considered as a potential
treatment option.
This study supports a central mechanism
33 I C C 2 0 1 3 K E Y N O T E S P E A K E R P R E S E N T A T I O N |
W W W . N E W C A S T L E . E D U . A U

COUGH RECEPTOR ANTAGONISTS
For TRPV1
V112220
BCTC
JNJ17203212
For TRPA1
GRC 17536 (Also effective in neuropathic pain, good
safety profile)
HC – 030031 (comparative to pregabalin for
neuropathic pain)
I C C 2 0 1 3 K E Y N O T E S P E A K E R P R E S E N T A T I O N |
W W W . N E W C A S T L E . E D U . A U34

SUMMARY
Significant clinical problem: limited, often ineffective
Rxs
‘Cough hypersensitivity syndrome’: unifying
diagnosis for cough phenotypes
Sensory neuropathic chronic cough, Laryngeal
Hypersensitivity
investigation of new and effective treatments
Recent Additions in the Treatment of Cough:
Non-pharmaceutical, eg:Speech Pathology
Pharmaceutical:neuromodulating drugs used in chronic
neuropathic pain, eg: Gabapentin
TRPV1 and TRPA1 antagonists
35 I C C 2 0 1 3 K E Y N O T E S P E A K E R P R E S E N T A T I O N |
W W W . N E W C A S T L E . E D U . A U

Acknowledgements: Professor Peter Gibson
Dr Anne Vertigan
Ms Sarah Bone
Dr Surinder Birring
Funding: John Hunter Hospital Charitable Trust Fellowship
HMRI Early Career Travel Award, sponsored by Stroud Rodeo, and
The First International Chinese Cough Conference.