icap ethiopia - columbia...
TRANSCRIPT
Background • Maternal mortality rate (MMR) is estimated at 676 per 100,000 live births
[Ethiopian Demographic and Health Survey (EDHS) of 2011] • Neonatal mortality is estimated at 37 per 1,000 live births (EDHS, 2011), making
Ethiopia one of the five countries that contribute to half of newborn deaths in Africa • As of 2008, only 51% of hospitals were providing comprehensive emergency obstetric
and newborn care (EmONC) and only 1% of the health centers were considered basic EmONC (BEmONC) facilities (FMOH EmNOC needs assessment, 2008)
• In 2011, ICAP initiated interventions with Dire Dawa Administration Regional Health Bureau (RHB) to improve health services using the Prevention of Mother to Child Transmission (PMTCT) platform
Objectives • Improve delivery and quality of emergency obstetric and newborn services
Method • ICAP, in collaboration with Dire Dawa Administration RHB, initiated MNCH
interventions using the PMTCT platform at 16 public health facilities • Standard of Care (SOC) assessment tools for MNCH services were developed. This
included 13 measurement parameters from antenatal care (ANC) clinics, six from labor and delivery (L&D) and six from postnatal care (PNC), which were pilot tested at the 16 facilities
• Health care providers at ANC clinics and L&D wards were given training and regular on-site clinical mentorship
• ICAP developed and distributed job aids on the active management of the third stage of labor, manual removal of placenta and vacuum delivery.
• Infrastructure of the L&D wards was enhanced • Bi-weekly criteria-based audits (CBA) and monthly progress review meetings were
conducted with facility staff • Baseline assessment if SOC indicators was conducted in March 2011 • Follow up SOC assessment was conducted in October 2011, May 2012, and February
2013 • The data was extracted from patient charts (19 from each of the 16 ANC clinics and
labor and delivery wards) seen during the month prior to the SOC assessment
Achievements • Multi-disciplinary teams were established in all 16 facilities & met regularly • CBA initiated in all facilities and compared current practice against standards • Referral linkage across the health network strengthened (i.e., establishment of feedback
mechanism including introduction of feedback boxes) • All supported facilities were ready to perform all the 7 BEmONC signal functions • Parenteral antibiotics and anticonvulsants which had not previously been allowed at the
health center level were introduced at health centers • During the 24 month period between 2011-2013:
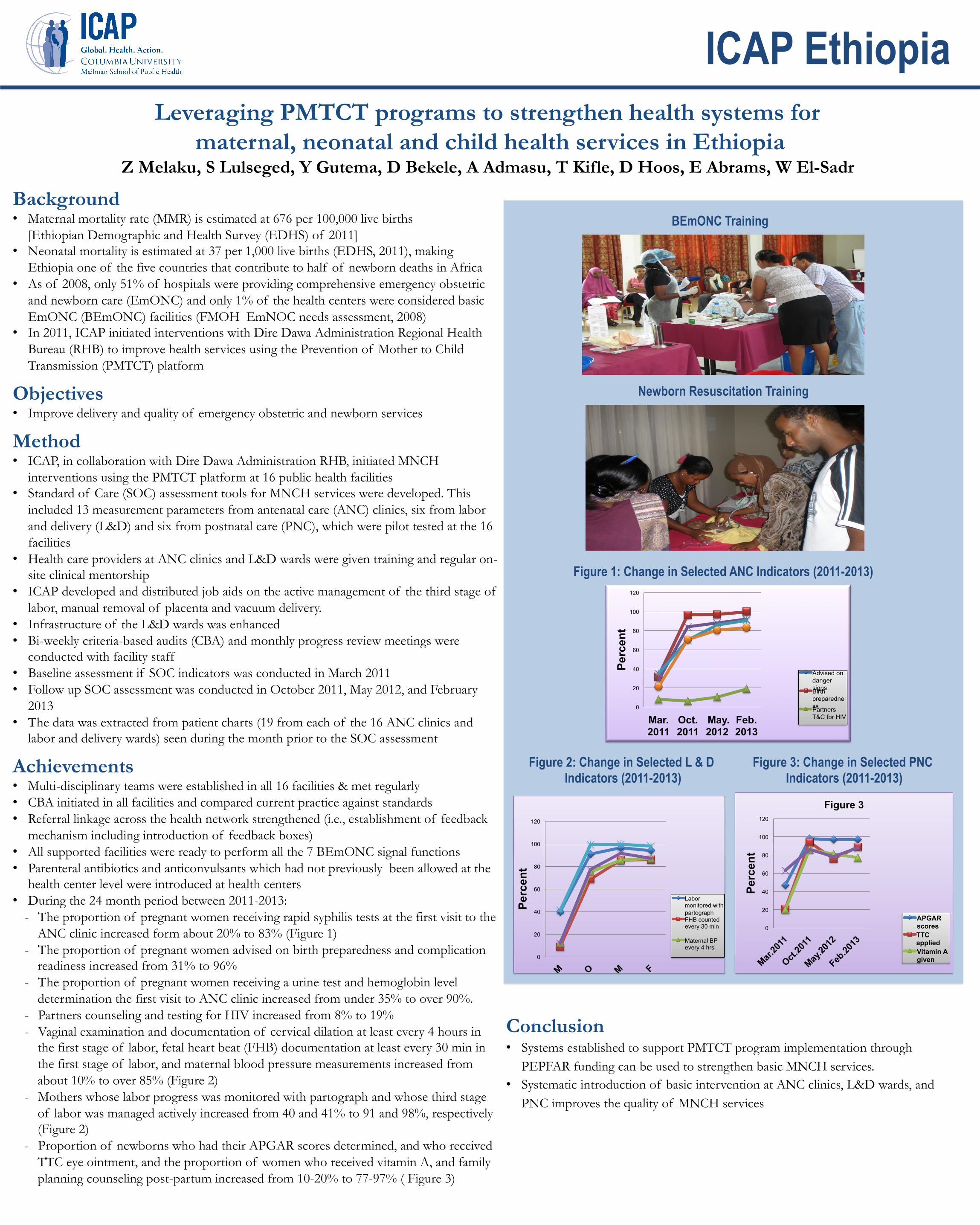
- The proportion of pregnant women receiving rapid syphilis tests at the first visit to the ANC clinic increased form about 20% to 83% (Figure 1)
- The proportion of pregnant women advised on birth preparedness and complication readiness increased from 31% to 96%
- The proportion of pregnant women receiving a urine test and hemoglobin level determination the first visit to ANC clinic increased from under 35% to over 90%.
- Partners counseling and testing for HIV increased from 8% to 19% - Vaginal examination and documentation of cervical dilation at least every 4 hours in
the first stage of labor, fetal heart beat (FHB) documentation at least every 30 min in the first stage of labor, and maternal blood pressure measurements increased from about 10% to over 85% (Figure 2)
- Mothers whose labor progress was monitored with partograph and whose third stage of labor was managed actively increased from 40 and 41% to 91 and 98%, respectively (Figure 2)
- Proportion of newborns who had their APGAR scores determined, and who received TTC eye ointment, and the proportion of women who received vitamin A, and family planning counseling post-partum increased from 10-20% to 77-97% ( Figure 3)
Leveraging PMTCT programs to strengthen health systems for maternal, neonatal and child health services in Ethiopia
Z Melaku, S Lulseged, Y Gutema, D Bekele, A Admasu, T Kifle, D Hoos, E Abrams, W El-Sadr
BEmONC Training
Newborn Resuscitation Training
Conclusion • Systems established to support PMTCT program implementation through
PEPFAR funding can be used to strengthen basic MNCH services. • Systematic introduction of basic intervention at ANC clinics, L&D wards, and
PNC improves the quality of MNCH services
0
20
40
60
80
100
120
Mar. 2011
Oct. 2011
May. 2012
Feb. 2013
Perc
ent
Advised on danger signs Birth preparedness Partners T&C for HIV
0
20
40
60
80
100
120
Perc
ent
Labor monitored with partograph FHB counted every 30 min
Maternal BP every 4 hrs
0
20
40
60
80
100
120
Perc
ent
Figure 3
APGAR scores TTC applied Vitamin A given
Figure 1: Change in Selected ANC Indicators (2011-2013)
Figure 2: Change in Selected L & D Indicators (2011-2013)
Figure 3: Change in Selected PNC Indicators (2011-2013)
ICAP Ethiopia