ibogaine, an anti-addictive drug: pharmacology and time … et... · human & experimental...
TRANSCRIPT

Human & Experimental Toxicology (2008) 27: 181-194
www.het.sagepub.com
Ibogaine, an anti-addictive drug:pharmacology and time to go furtherin development. A narrative reviewR Maciulaitls', V KontrimaviÈiüté^••^ FMM BressoUe^ and V Briedis^
'Department of Basic and Clinical Pharmacology. Kaunas University of Medicine, Lithuania; ^ClinicalPharmacokinetic Laboratory, Faculty of Pharmacy, University Montpellier L France: ''Department ofAnalytical and Toxicological Chemistry, Kaunas University of Medicine. Lithuania: and '^Department ofPharmaceutical Technology and Social Pharmacy, Kaunas University of Medicine, Lithuania
Ibogaine is an Índole alkaloid derived from the bark ofthe root of the African shrub Tabernanlhe iboga. Psycho-active properties of ibogaine have been known for dec-ades. More recently, based on experimental data fromanimals and anectodal reports in human, it has beenfound that this drug has anti-addictive efFecls. Severalpatents were published between 1969 and 1995. Thepharmacology of ihogaine is quite complex, affectingmany different neurotransmitter systems simultaneously.However, Ihe pharmacülogicai targets underlying the
Introduction
The development process ofthe medicinal product isa system consisting of many operational aspectsdesigned to solve certain organizational, scientific,and regulatory questions.^'^ Ideally one can have aclear view about this system, meet the needs, andhave a product on the market. The real problemsare the practicalities that hinder implementation ofideal principles and make product failed. Bib-liographical review of ibogaine development mightbe one of the learning case studies that we canlearn from others. Ibogaine is one ofthe psychoactiveíndole alkaloids naturally occurring in the West Afri-can shrub Tabernanthe iboga. The major compo-nents of T. iboga root bark extracts are ibogaine(approximately 80%). ibogaline (15%), and iboga-mine (up to 5%1. which confirms the complexity ofthe extract.^ From the results ofthe preclinical stud-ies and anecdotal reports from American and Euro-pean addict self-help groups, ibogaine could be apromising drug in addiction therapy. Unfortunately,lost opportunities to confirm a positive benefit riskbalance during both preclinical and clinical develop-ments as well as losses of financial supports havelead to the stopping of the ibogaine development inthe treatment of drug dependence. Future will showthe strategy one will obtain and outcome thereof -
[forraspondence to: Dr Françoise Brossolle, PhD, Laboratoire dePhiirmacocinétique Ciiniquo. Faculté de Pharmacie Montpellier.15 Avenue Charles Flahaull. B.P. 14491, 34093 MontpellierCedex 5, France. Email: [email protected]
© 2008 SAGE Publications
physiological and psychological actions of ihogaine arenot completely understood. Ihogaine is rapidly melaho-lized in the hody in norihogaine. The purpose oí this arti-cle was to review data from the literature concerningphysicochemical properties, hio-analytical methods, andpharmacology of ihogaine: this article will he focused onthe use of this drug as anti-addictive agent.
Key words; bioanalytical nielhods: iliogaino: noribogaintí; phar-marodynamic studies: pharmacokincUcs: safety
will we forget about this novelty in addictive therapyor will we have a finalized development.
The mechanism of action of ibogaine in the treat-ment of drug addiction appears to be distinct fromother existing p harm ac o therapeutic approaches. Thepurpose of this article was to review data from theliterature concerning physicochemical properties,bio-analytical methods, and pharmacology of ibo-gaine; this article will be focused on the use of thisdrug as anti-addictive agent.
To identify articles for this review, we useInternet-based Grateful Med to access electronicdatabases: MEDLINE and Currents Contents 1957-2007. We searched, without language limitations,for the subject terms "ihogaine", "noribogaine","mechanism of action", "quantification", "pharma-cokinetics", and "pharmacodynamics". We furthernarrowed the search hy using the terms "anti-addictive properties", "animals", "healthy volun-teers", and "dependent patients". We then improvedtlie search using the terms "withdrawal signs" and"drug craving". We identified additional citationsfrom the reference sections of articles retrieved andconsulted these articles. We completed this searchusing the website "google.com" and the engine"Copernic".
History
Ibogaine is a naturally occurring plant Índole alka-loid. The root bark of the Apocynaceous shrubT. iboga is the most frequently cited source of
10,1177/0960327107087802

Ibogaine, an anti-addictive drugR Maciulaitis, et al.
182
ibogaine. The Iboga tree is the central pillar of theBwiti religion practiced in West-Central Africa,mainly Gabon. Cameroon, and the Republic of theCongo, which uses the alkaloid-containing roots ofthe plant for its psychoactive properties in a numberof ceremonies. Ibogaine is also used by indigenouspeoples in low doses to combat fatigue, hunger, andthirst." Other sources of ibogaine are Voacangatbouarsii var. Ortusa.,^ Tahernnfímontana austniUs''',and Tabernaemontana orientalis7 Although knownfor many centuries for tribes in West Africa, researchof ihogaino ¡itarted in late 19th century. The firstdescription of T. iboga is published in 19B5 from spe-cimens ofthe plant brought to France from Gabon." Apublishfîd description of the ceremonial use ofT. iboga in Gabon appears in 1885." Ibogaine wasfirst extracted and crystallized from the T. iboga rootin 1901."*"'^ Ibogaine structure has been establishedin 1957 through chemical studies,'^ and X-ray crys-tallographic investigations have fixed the configura-tion ofthe ethyl group. "* Moreover, •'C nuclear mag-netic resonance data'^ were reported in comparisonwith several iboga similar structures. The total syn-thesis of ibogaine and its availability in the form ofthe racomate was reported in 1966."'
The intßrest of ibogaine to contemporary pharma-cology is that this drug possesses anti-addictiveproperties. Between 1969 and 1995, tlie anti-addictive properties of ibogaine and its use in thetreatment of heroin, cocaine, amphetamine abuse,alcohol, and nicotine dependence, and even somedrug abuse have been patented in the United Statesand in France. A French patent for the psychothera-peutic use of ihogaine at a dosage of 4—5 mg/kg waspublished in 1969.'" US patents have been pub-lished by Lotsof for the use of ibogaine in opioidwithdrawal, dependence on cocaine and other sti-mulants, alcohol, nicotine, and polysubstanceabuse.'^"^^ These patents claim that an oral or rectal4-25 mg/kg dose of ibogaine interrupts addictivedrug behavior for a period of 6-36 months.
ChemistryIbogaine (12-methoxyibogamine. (6R, 6aS, 7S, 9R)-7-ethyl-2-methoxy-6, 6a, 7, 8, 9, 10, 12, 13-octahydro-5H-6, 9-methanopyrido[l',2':l,2|azepino[4,5-6iindole)has a molecular weight of 310.44 (Figure l). Extrac-tion of ibogaine from T. iboga shrub requires profes-sional training. N4ainly haloalkanes or alcohols wereused for extraction. Chromatography was the methodof choice for its purification. Extraction of ibogainefrom T. iboga root bark using diluted vinegar andammonia was described. ' This drug can also heobtained semisynthetically from voacangine-' or syn-
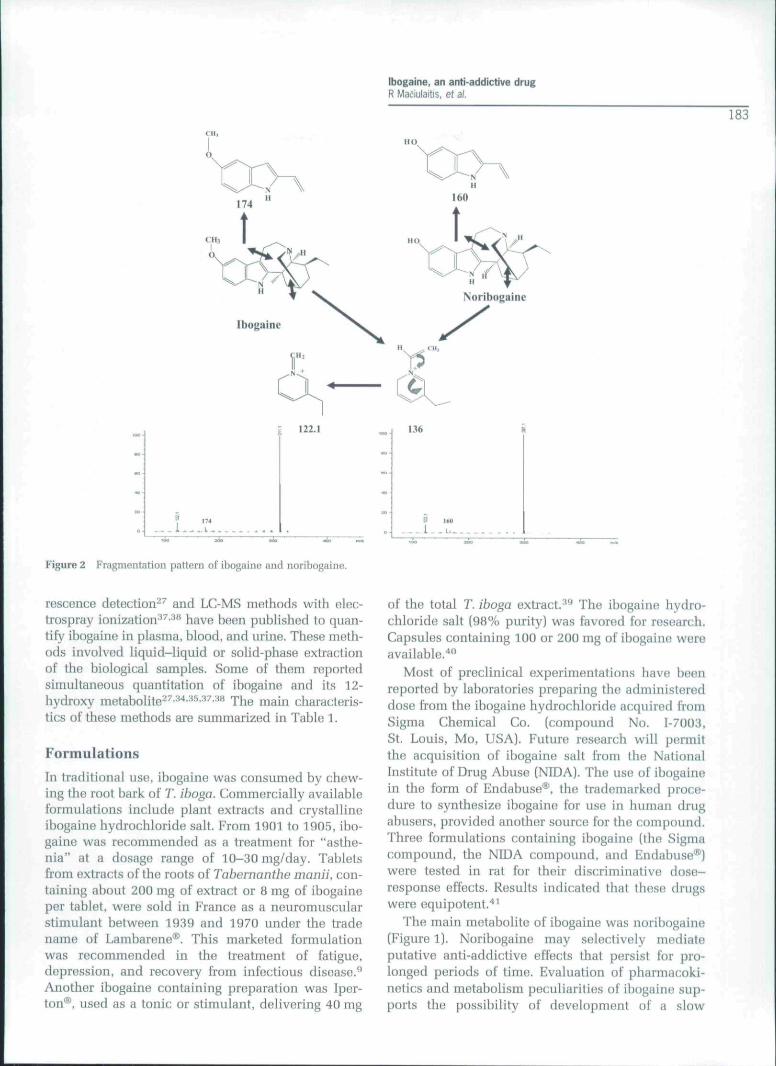
thetically from nicotinamide hy way of a 13 or 14 stepprocess.^'' although extraction from the iboga root is asimpler metliod for obtaining the compound. Ibogainehas B melting point of 153 °C and a pK . of 8,1 in 80%methylcellosolve; its heptano/water partition coeffr-cient of 28 confirms the lipophilicity of the com-pound. Recently, a stmctiiral analysis of ibogainoand of its main active metabolite, noribogaine (or 12-hydroxyibogamino. (6R. 6aS. 7S. 9R)-7-ethyl-6, 6a, 7.8, 9, 10, 12, 13-octahydro-5H-6, 9-methanopyrido[l',2':1.2lazepino|4,5-/jlkidol-2-ol. Figure 1), usingFourrier transform-infrared spectroscopy, lD and 2Dnuclear magnetic rnsonanco spectroscopy, and liquidchromatography-electrospray mass spectrometry(LG/HSI-MS) has been published.^'' In accordancewith the article of Taylor.-^ a fragmentation pattern ijiLC/ESI-MS is proposed (Figure 2). Ibogaine and nori-bogaint! in solution suffer facile autoxidation underlight- and heat-exposure giving iboluteine and ibo-chine. and desmethoxyiboluteine and desmetJioxyi-bochine, respectively. '*" ' Recently, it has beenshown that at 20 °C with daylight exposure, ibogaine(22.4 ng/mL] and noribogaine (25 ng/niL) showed amonoexponential decrease in cfrug concentrations:the corresponding half-lives were 81,5 min for ibo-gaine and 11 min for noribogaine.^''
Analytical methodsIbogaine was determined in complex mixtures ofT. iboga and in biological matrices (brain homogenate,urine, and plasma) by spectrophotometry.^** thin-layerchromatography,^-' or gas chi'omatography withñame ionization,^^^"* nitrogen-specific''^ or mass-spoctrometric (electron impact or chemical ioniza-tion)''^"''^ detection. Most of these methods involveda derivatization procedure. A method for determiningopiate agonists including ibogaine by liquidchromatography-atmospheric-pressure chemical-ionization mass spectrometry procedure has heenalso described (LC/APCI-MS). * ' Recently, a high per-formance liquid cliromatography method with fluo-
R = O H NoribogaïncR = OCH3 Ibogaine
Figure 1 Molecular structurefi of ibogaine and noribogaine.
[bogaine, an antj-addictive drugR Maciulaitis, ef ai.
»o.
122.1
Figure 2 Kragmentation pattern of ibogaine and noribogaine.
136
183
rescence detection^^ and LC-MS methods with elec-trospray ionization^^'^" have been published to quan-tify ibogaine in plasma, blood, and urine. These meth-ods involved liquid-liquid or solid-phase extractionof the biological samples. Some of Uiem reportedsimultaneous quantitation of ibogaine and its 12-hydroxy metaboHte - - -''- ''-- ^ The main characteris-tics of these methods are summarized in Table 1.
Formulations
In traditional use, ibogaine was consumed by chew-ing the root hark of T. iboga. Commernially availableformulations include plant extracts and crystallineibogaine hydrochloride salt. From 1901 to 1905, ibo-gaine was recommended as a treatment for "asthe-nia" at a dosage range of 10-30 mg/day. Tabletsfrom extracts of the roots of Tabernanthe nmnii, con-taining about 200 mg of extract or 8 mg of ibogaineper tablet, were sold in France as a neuromuscularstimulant between 1939 and 1970 under the ti-adename of Lambarene®. This marketed formulationwas recommended in the treatment of fatigue,depression, and recovery from infectious disease.^Another ibogaine containing preparation was Iper-ton®, used as a tonic or stimulant, delivering 40 mg
of the total T. iboga extract. ** The ibogaine hydro-chloride salt (98% purity) was favored for resoarch.Capsules containing 100 or 200 mg of ibogaine wereavailable.*"
Most of preclinical experimentations have beenreported by laboratories preparing the administereddose from the ibogaine hydrochloride acquired fromSigma Chemical Co. (compound No. 1-7003,St. Louis, Mo, USA). Future research will pormitthe acquisition of ibogaine salt from the NationalInstitutti of Drug Abuse (NIDA). The use of ibogainein tlie form of Endabuse®, the trademarked proce-dure to synthesize ibogaine for use in human drugabusors, provided another source for the compound.Three formulations containing ihogaine (the Sigmacompound, the NIDA compound, and Endabuse®)were tested in rat for their discriminative dosti-response effects. Results indicated tliat these drugswere equipotent.''^
The main metabolite of ibogaine was noribogaine(Figure 1). Noribogaine may selectively mediateputative anti-addictive effects that persist for pro-longed periods of time. Evaluation of pharmacoki-netics and metabolism peculiarities of ibogaine sup-ports the possibility of development of a slow

(bogaine, an anti-addictive drugR Macjulaitis, ei al.
184
.3
iz*-• in
X d
3-5 *d œ a,H" Ë 2
C8 H
O ^ Ci-
3. in
.. o
aoooJ J
X
uT
te r-
ta
3 ^ Z "p ^ Oa"~ „ ^ ' " ''S" X c -y X u
3 œ .|^ D m g
Z ' :
3 S
"U j i lu ta
II il
.5 Ö
á z
'u a
3 Ë
i j Q -J
"2 ¿•' l j , ! a3 3 X -- 3 —
Q m u
Ë ="- ^ i : CD
I,D
.25
nic
kn
E Ö -J-
^ P ^- | i c ; g
. l' M Ö
Q
1= <u'^3w ,yd-ss S
taQ
y 0)
32 n
ickn
d - £"^ S
B~
¿"D
g Ö
1
o n
S o£Z
S-5£-
- - " S 2 ' "=
Öl 13 m CQ t - CÛ CL a, en
.s s
.10lo
.getOQOâ
4 f
"3000
c•aocO
e
-S3ocO
XIoc'CO o
ao
9 o
C O Q• r a o
ce - J
.9'3oco
•a S«-2oc co 3a z
.s od -9o •cSZ
1iO 00 Bî " ^
I ^ >2 = î^£ Z
0) -a
'^.B E^'^.g B ; E¿ Ë.2 S ^ "c ,2 "3 "^ "ü .2 ^
O c/5 O W O
qso "
.il2 o
11
tí o00 T
¡rira
c "
trim
tal.
^ Uli
'So:(Q n
trim
u 3
a u c2 ^ -
«0
"il
tl
i
lis•e g ó
E iS g
E Ëc a
a; u Q
« ^ ~«I m >
P ° n

Ibogaine, an anti-addictive drugR Maciulaitis, et al
185release formulation of noribogaine as an anticravingmedication for opiates and psychostimulants.^
Preclinical pharmacokinetics
AbsorptionStudies in rats showed dose-dependent and gender-dependent bioavailability after oral route suggestingthat ibogaine absorption, and/or first pass elimina-tion, is non-linear.*^ After oral administration of Iper-ton® capsules, containing 40 mg of natural extract ofT. iboga, a substantial sex difference in rat brain andplasma concentrations of ibogaine was observed.^'These data were consistent with those of Pearl,eta}.,^^ reporting that plasma levels of ibogaineafter oral administration were approximately three-fold higher in female than in male rats, and the bio-availability of ihogaine was approximately twofoldhigher in female than in male.'*^ After oral adminis-tration of 5 and 50 mg/kg to rat, the bioavailahilitywas 16% and 71% in female and 7% and 43% inmale, respectively/^
DistributionAn intriguing property of ibogaine is its prolongedduration of action when behavioral and neurochem-ical effects are identified after one or more days fol-lowing oral, intraperitoneal (i.p.), or subcutaneousadministration. Pharmacokinetics of ibogaine in ratwere consistent with a two-compartment model, butthe extremely high concentrations found in adiposetissues suggests the possibility of more complexpharmac o kinetics.'*'* One hundred times greater con-centrations in fat and 30 times greater concentra-tions in brain, than in plasma found 1 h after admin-istration were consistent with the highly lipophilicnature of ibogaine.'*^ It was proposed that prolongedactions of ibogaine could be explained by adiposetissue reservoir with release and metahoUsm toactive metabolite noribogaine over an extendedperiod of time.* '*^
Another depot might be the platelets or otlierblood components, as concentrations of ibogainewere higher in the whole blood than in plasma.^The concentrations of ibogaine and noribogainehave been measured in rat brain following both oraland i.p. admimstrations [40 mg/kg i.p.. 50 mg/kg peros.). ^^*^ The signitlcance of micromolar interactionsof ibogaine and noribogaine with various radioligandbinding sites was related to the concentration of theparent drug and its metabolite in brain. Concentra-tions of thesü two drugs in rat cerebral cortex, stria-tum, brainstem, and cerebellum were measured15 min, 1 and 2 h following drug administration. Itwas shown that ihogaine was rapidly detected in
brain following oral administration. Noribogainewas detected at the earliest time point (15 min) con-sistent with a first pa.ss motaholism of the parentdnig."^" After i.p. and oral administi'ations of Ihogainein rat, maximum concentrations were 11-15 LM inthe whole blood and tlie brain for ibogaine. and21.9 ^M in the whole blood and 9,8-11.3 MM in thebrain for noribogaine. In the whole blood and in thebrain, area under concentration-time curve (AUC)values were 9- and 1.8-times higher for noribogainethan for ihogaine, respectively. The AUC ratios(brain/whole hlood) were equal to 2 for ihogaine and0.4 for noribogaine."^^ These results report that nori-bogaine reaches significant concentrations in brainfollowing both routes of administration in rat. Thus,the concentrations of norihogaine in brain may acti-vate processes that cause the desired effects of sup-pressing opiate withdrawal signs and diminishingdrug craving.
MetabolismIbogaine is metabolized by cytochrome P4502D6(CYP2D6) into a major (active) metabolite -noribogaine.^'* An important aspect is that this iso-form is subjected to polymorphic expression partic-ularly in Caucasians. From in-vitro study usinghuman liver microsomes, Obach, efa/.^" reportedthat two (or more) enzymes were involved in thisreaction. These authors identified two kineticallydistinguishable ibogaine O-demethylases involvedin this reaction corresponditig, to high [Kf^\,> 200 \iM] and low [KM, 0.1 ^M) values ofthe appar-ent Michaelis constant. The importance ofthe routeof administration has been underlined, indicatingthat the noribogaine/ibogaine concentration ratio inthe bloodstream was higher when ibogaine isinjected by the i.p. route rather than by tho intrave-nous route.^' As well as, higher concentrations ofibogaine in plasma, brain, kidney, liver, and fatwere observed following subcutaneous versus i.p.administration suggesting a substantial "first pass"effect after i.p. administration involving hepaticextraction."* '
It seems tliat noribogaine could be a safer andpossihly more efficacious alternative to ibogaine asa medication for the treatment of various types ot"addiction.'^*
EliminationThe half-life of ibogaine in rat was 1-3 h. s-^s.ai xhiselimination half-life could be underestimated since3-h post-dose ibogaine conc:entrations remainedvery high in fat."*'' Ibogaine and noribogaine areexcreted via the renal and the gastrointestinal tract(60-70% ofthe administered dose in 24 h in raf"^].

Ibogaine. an anti-addictive drugR Maeiulaitis, et al.
186
Pharmacodynamic studies in animals andmechanism of action
Primary and secondary pharmacologySeveral reviews have reported the pharmacologicalprofile of ibogaine."- ' '-'*''' ^ It has been shown thatibogaine and noribogaine interact with multiple hind-ing sites witliin the central nervous system (CNS),including iV-methyl-n-aspartate (NMDA) receptor-coupled ion channels, K-opioid (K, and K^). ^i-opioidand 02. serotonin (5-HT2 and 5-HT:j). muscarinic (M,and M2) receptors and monoamine uptake sites, andnicotinic acetylcholine receptors. The pharmacologi-cal profile of noribogaine is different from that ofiboga i ne.'* ' ^"'' Ibogaine is more potent than noribo-gaine (i) in binding to the NMDA receptor in braintissue"*^ ••'•'' and (ii) as a stimulator of thehypothalamic-pituitary-adrenal axis. *- ^ Althoughibogaine and 5-HT display chemical similaritiüs,because both molecules contain an Índole as part oftheir structure, norihogaine is much more potent thanibogaine in its ability to elevate extracellular 5-HT inthe brain. ' Thus, this drug is 10-times more potent inbinding to serotonin transporter and inhibiting reup-take of serotonin. ' - ^"-'' Noribogaine is also (i)much more potent than ibogaine for binding to \x-opioid receptor and is a full p-opioid agonist'*'' - - '**"^ and (ii) more potent binding to KI and less potentbinding to K opioid receptors. Affinities of ibogaineand noribogaine to some of these receptors arereported in Table 2.'*'' Although not apparent in bind-ing studios, fimctional studies indicate significantactivity of ibogaine as a non-competitive antagonistat the nicotinic acetylcholine receptor.''
Conflicting results were reported about the alter-ation of extracellular dopamine levels in the nucleusaccumbens. According to Baumann. etaij'^ neitheribogaint! nor its metabolite significantly altereddopamine levels, whereas Glick, efa/. *'' ^ reportedthat these two drugs cause significant decreases indopamine levels.
Signal transduction pathways were examinedduring several preclinical trials. The examinationof discriminative stimulus effects of ibogaino andnoribogaine in rats in relation to their concentrationsin hlood plasma and brain regions and to receptorsystems suggested that norihogaine may be themajor entity that produces the discriminative effectof ihogaine.^'' It has been reported that the observedincrease in phosphoinositide hydrolysis by noribo-gaine should be accompanied by an activation ofprotein kinase C which mediated a variety of long-term changes and might be involved in the behav-ioral effects of ibogaine.''" The selective increase inreceptor-mediated inhibition of adenyl cyclaseactivity caused by ibogaine and noribogaine mightalso be involved in the pharmacological activity ofthese compounds.'*' Recently, it has been shownthat the remedial effect of ibogaine as anti-addictive drug is mediated, at least partially,through an influence on energy metabolism.'^-Among the recent proposals for ibogaine mechan-isms of action is the activation of the glial cellline-derived neurotrophic factor (GDNF) pathwayin the ventral tegmental area of the brain.®-'' Thiswork has principally been accomplished in preclin-ical ethanol research, where 40 mg/kg of ibogainecaused increase of RNA expression of GDNF inkeeping with reduction of ethanol intake in the ratand absence of neurotoxicity or cell death. Short-term ibogaine exposure results in a sustainedincrease in GDNF expression, resulting in anincrease in GDNF mRNA leading to protein expres-sion and to the corresponding activation of theGDNF signaling pathway.'*''
It was also shown that ibogaine and noribogainemay stimulate the secretion of corticosterone fromthe adrenal cortex and prolactine from the anteriorpituitary.^^ These two drugs also caused similarincrease in plasma prolactine. Relevance of thesephysiological changes for primary or secondarypharmacology should he elucidated more in thofuture.
Table 2 Affinities of ibogaine and noribogaine to some receptors (according to Mash, et al.*
¡bogaine Noribogaine Phnrmacodynamic activity
IC50.
5-HT transporter (RTI-55 DAT sites)Opioidergic
Mil (DAMGO)Kappa 1 (lJ6959;i)Kappa 2 (IOXY)
ClutaminorgicNMDA (MK-801)
0.5
11.025.023.8
5.2
0.04
0.164.2
92.3
;ti.4
Reuptake blocker
AgonistPartial agonist (?)Partial agunist (?)
Channel blo(;kcr
DAT. dopamine transporters; NMDA, N-methyl-oaspartatti,

Ibogaine, an anti-addictive drugR Maí-iulaiíis, et ai
187
Anti-addictive activity in animalsNMDA, opioid, and serotonin receptors have beentargeted successfully for many years as anti-addictive treatment of opioid and/or cocaineaddiction.®^-^^ Activities of both ibogaine and nori-bogfiino on tliese receptors provided a biologicalplausibility to expect anti-addictive efficacy for ibo-gaine in human also. Initial findings, suggestive ofthe efficacy of ibogaine in animal models of addic-tion, including diminished opioid self-administration and withdrawal'''''"''^ and diminishedcocaine self-administration/'' were published in late1i)80s and in early 1990s.
Animal models of addiction were used to studythe activity of ibogaine in the treatment of drugdependence. The administration of ibogainereduced self-administration of cocaine, morphine,heroin, alcohol, and reduced nicotine preference.^The decrease in cocaine consumption has beendescribed in mice after L.p. administration of two40 mg/kg dose at 6 h intervaP^ and in rat after i.p.administration of 2.5-80 mg/kg given as single orrepeated doses (daily or weekly, n = 3).67.70.72According to Cappendijk and Dzoljic, the maximumeffects were observed when ibogaine was givenweekly for 3 weeks/" The decrease in opiate con-sumption has been described after administration of2.5-80 mg/kg ibogaine in morphine- and heroin-dependent rat.' ' -- ^
Ibogaine also eliminates some of the signs of opi-ate withdrawal precipitated by naloxone or naltrex-one in morphine-dependent rats given 20, 40, or80 mg/kg ibogaine i-p.' "- '* and monkeys given 2 or8 mg/kg ibogaine subcutaneously/^-^^ However,Sharpe and Jaffe '' failed to report that ibogaineadministered subcutaneously attenuated naloxone-precipitated withdrawal in rat receiving 5. 10, 20,and 40 mg/kg of ibogaine. Conflicting results wereobserved in mice. At doses ranging from 40 to80 mg/kg i.p., a reduced naloxone-precipitated jump-ing in morphine-dependent mice was observed^^''";however, opposite effects were found after a30 mg/kg i.p. dose.' ' These discrepancies might berelated to ibogaine administration: before ''- *' orafter ^ naloxone administration.
Although ibogaine has diverse effects on the CNS,the pharmacological targets underlying the physio-logical and psychological actions of ibogaine arenot completely understood.
Preclinical safety studies
Several safety studies were performed during pre-clinical development. These studies raised several
safety concerns, mainly neurotoxicity and possiblecardiotoxicity.
Multiple laboratories have reported on the degen-eration of cerebellai' Purkinje cells in rat receivingi.p. administration of ibogaine at a dose of40-100 mg/kg,•' • ' •*'" These include abnormalmotor behavior (such as tremors, ataxia) related tohistologically proven neurotoxicity.™ Single-doseinvestigations showed that a 25 mg/kg i.p. dosewas found to correspond to a no-observed-adverse-effect-level (NOAEL)."' Helsley. et al.observed no evidence of neurntoxicity in a studywhere rats received 10 mg/kg of ibogaine per day for60 days."^ However, the neurotoxic effects of iho-gaine may occur at levels higher than thoseobserved to have effects on opioid withdrawal andself-administration. The monkey appears to be lesssensitive to potential ibogaine neurotoxicity thanthe rat.'' Mash, et al. observed no evidence of neuro-toxicity in monkeys treated for 5 days with repeatedoral doses of ibogaine of 5-25 mg/kg or siibcutane-ously administered doses of 100 mg/kg.'* Anotherspecies difference in sensitivity is the mouse,which unlike the rat showed no evidence of cerebel-lar degeneration at a 100 mg/kg i.p. dose ofibogaine."''
Animal studies showed certain cardiotoxicities.Observed cardiotoxicity could be dose dependent.No changes in resting heart rate or hlood pressurewere found at a dose of ibogaine of 40 mg/kg i.p.,which has been used in drug withdrawal or self-administration studies. Higher doses of ibogaine(100 and 200 mg/kg) decreased the heart rate with-out an effect on blood pressure.'*'' However,Binienda, etal.^^^ found a significantly decreasedheart rate in rats given ibogaine 50 mg/kg i.p. Thelethal dose 50% of ibogaine was 145 mg/kg i.p. and327 mg/kg intragastrically in the rat, and 175 mg/kgi.p. in the mouse.^^
In conclusion, preclinical development showedthat ihogaine is acting on several mediators in CNSthat have been targeted in treatment of drug-dependence. Nenrotoxiciy and cardiotoxicity aresafety concerns to be investigated further. No suffi-cient long-term safety non-clinical studies are avail-able. All these data make further investigation ofibogaine's activity as potential therapeutic agent bio-logically plausible.
Clinical pharmacokinetic andpharmacodynamic studies
Clinical studiesClinical development of ibogaine has continued forsome decades. Development was governed by

Ibogaine, an anti-addictive drugR Maeiulaitis, et ai.
188
several sponsors handed over management form onehand to other. Development was carried by severalseparate academicians and companies.
The first phar maco dynamic studies of ibogainehave been performed during 1901-1905. First anti-addictive attempts were done by Harris Isbell in1955, administering doses of ibogaine of up to300 mg to eight already detoxified morphine addictsat the United States. Addiction Research Centre inLoxingfon, Kentucky." In 1962-1963, Lotsof adminis-tered ibogaine at the dose of 6-19 mg/kg. to 19 indi-viduals including seven subjects with opioid depen-dence who noted an apparent effect on acutewithdrawal symptomatology.^^-^^ In 1967-1970, theWorld Health Assembly classified ibogaine with hal-lucinogens and stimulants as a "substance likely tocause dependency or endanger human health". In1970, the US Food and Drug Administration (FDA)classified ibogaine as a Schedule I Controlled Sub-stance, along with other psychedelics such as LSDand mescaline. The International Olympic Commit-tee banned ibogaine as a potential doping agent.Thus, sales of Lambiu-ène® were stopped in France."Since that time, several countries, including Sweden,Denmark, Belgium, Switzerland, and recently (sinceMarch 2007) France, have bamied the sale and pos-session of ibogaine.
The available data from private clinics describedin scientific reports, where ibogaine has been usedfor informal addiction treatment, stated that ibo-gaine has been taken orally at an average dose of19.3 ± 6.9 mg/kg."' •"• Another study reported sixheroin-addicted individuals and one subject whowere addicted to codeine treated with ibogaine atdoses ranging from 700 to 1800 mg."*"
From 1989 to 1993, treatments were conductedoutside of conventional medical settings in the Neth-erlands involving the International Coalition ofAddict Self-Help, Dutch Addict Self Help, and NDAInternational.*^"" In 1991, NIDA Medication Devel-opment Division began its ibogaine project. This ini-tiative was based on case reports end preclinical evi-dence suggesting possible efficacy. The majorobjectives of the ibogaine project were preclinicaltoxicological evaluation and development of ahuman protocol. In August 1993. FDA AdvisoryPanel meeting formally considered InvestigationalNew Drug Application filed by Dr Deborah Mash.Professor of Neurology at the University of Miami.Approval for human trials was given with 1, 2, and5 mg/kg of ibogaine dosage levels. The Phase I doseescalation study began in December 1993, but activ-ity was eventually suspended.'*'* From October 1993to December 1994, phase I/n protocols were dis-cussed by the NTDA and fixed doses of ibogaine of
150 and 300 mg versus placebo for the indication ofcocaine dependence were proposed.""'-' The nextyear, a NIDA ibogaine review meeting decided toend the ibogaine project but to continue to supportsome preclinical research on iboga alkaloids. A fatal-ity occurred during a heroin detoxification treatmentof a 24-year-oId women in the Netherlands in ]ime1993. This incident was a significant factor in theNIDA decision not to fruid a clinical trial of ibogainein 1995." But the drug-addicted persons continuetaking purified ibogaine hydrochloride powders ora whole plant extract that contains an unidentifiednumber of other biologically active compounds.Some practically applied recommendations instructtaking between 2 and 6 g of powdered iboga.''"
Some clinical experiences were gained duringmid 1990s to 2001. At that time, ibogaine was avail-able in alternative settings and studies based on aconventional medical model were carried out inPanama and in St Kitts. Informal protocols weredeveloped in the United States, Slovenia, Britain,the Netherlands, and the Czech Republic. The ibo-gaine mailing Ust began in 1997 and heralded anincreasing utilization of the Internet within the ibo-gaine medical subculture.
In early 2006, the creation of a non-profit founda-tion addressing the issue of providing ibogaine forthe purpose addiction interruption within establish-ment drug treatment care was formed in Sweden(Stiftelsen Iboga's web site, accessed march 2007).
PharmacokineticsPharmacokinetic data relative to ibogaine in humanare limited."•''''• ' '•"' Most of these studies have beencarried out in drug-dependent patients. Followingsingle oral doses of ibogaine (500-800 mg) to indi-vidual subjects, maximum ihogaine and noribogaineblood concentrations of 30-1250 ng/mL and 700-1200 ng/mL were obtained approximately 2 and 5 hafter drug administration, respectively.'*-'-'' ' Thereaf-ter, ibogaine was cleared rapidly from the blood,whereas noribogaine concentrations remained high.Indeed, concentrations of noribogaine measured at24 h post-dose were in the range of 300-800 ng/mLwhereas those of ibogaine were about 100 timeslower. From blood concentration-time profiles of ibo-gaine published by Mash, et ti/.,**' -''" after an oraldose of 800 mg, the steady-state volume of distribu-tion uncorrtîcted for bioavailability was about 13 I/kgand the half-life of the terminal part of the curveswas 4-7 h. Ibogaine being metabolized hy theCYP2D6 into noribogaine, the pharmacokinetic pro-file of this drug was different in extensive and poormetabolizers. After single oral doses of ibogaine(10 mg/kg), maximum concentrations of noribogaine

Ibogaine, an anti-addictive drugR Maciulaitis, ef al.
189were nine times lower in poor metabolizers [n = 3)than in extensive metabolizers {n = 24). whereasmaximum concentrations of ibogaine were about18% higher comparing to extensive metabolizers.This gap reflects speculation that conversion rate ofthe parent compound to noribogaine in CYP2D6 defi-cient subjects may reflect the metabolic contributionof other cytochromes [CYP2C9. CYP3A4J. The bloodAUC vaines, poor metabolizers versus extensivemetabolizers, were almost three times higher for ibo-gaine and four times lower for noribogaine. TheseAUC levels were more representative for understand-ing systemic exposures in extensive and poor meta-bolizers. In extensive metabolizers, the blood AUCratio, noribobaine/ibogaine, was approximately 3.Thus, the contribution of noribogaine to the totalpharmacodynamic effect of the parent drug was sig-nificant. The calculated terminal half-Hfe of ibogainein this study was 7.45 b in extensive metabolizers.
In a recent study, Kontrimaviciûté, efaA"^reported for the first time the tissue distribution ofibogaine and norihogaine, in a subject dead after apoisoning itivolving ingestion of root hark of theshrub T. iboga. The highest concentrations of ibo-gaine and noribogaine were found in spleen, liver,brain, and lung. The tissue/sub-clavian blood con-centration ratios averaged 1.78, 3.75, 1.16, and 4.64for ibogaine and 0.83. 2.43. 0.90, and 2.69 for nori-bogaine. for spleen, liver, brain, and lung, respec-tively. Very low concentrations of the two drugswere found in the prostatic tissue. No compounds
Table 3 Pharmacokinetic paramßters from clinical studiss
were detected in the cardiac tissue. Both ihogaineand noribogaine are secreted in the bile and crossthe blood—brain barrier.
Results are summarized in Table 3.
Pliarmacodynamic effectsSome case-report studies showed that ibogaine isactive as psycliotropic agent with possible anti-addictive activity in acute opioidwithdrawal.•*'^^"^'"^ After administration of ibo-gaine, individuals can experience (i) certain subjec-tive new experience and (ii) reductions of drug crav-ing and withdrawal signs and symptoms.
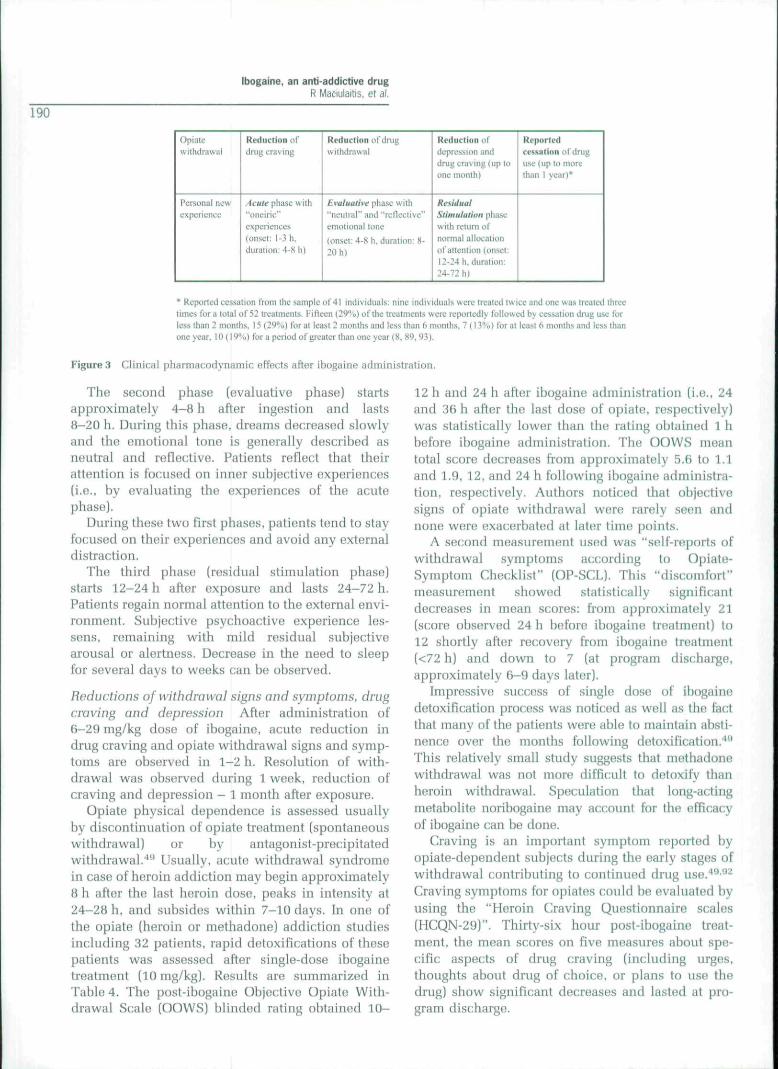
Subjective new experiences described bv patientstreated with ibogaine Preliminary data shows thatpatients experience several different phases thatmay be categorized into acute, evaluative, and resid-ual stimulation stages [Figure 3)."
The first phase (acute phase) is experiencedwithin flrst 1-3 h after exposure and lasts 4-8 h.During tliis phase, patients report panoramic deliv-ery of long-term memory, mainly visual; "visions" or"waking dream" states experiencing contact withtranscendent beings, passage along a lengthy path,floating, etc. Although visual experiences are notreported by all patients and seem depend of drugexposure, it is also noticed that they were associatedand enhanced with eye closure. Unfortunately, dif-ference between these dreams and hallucinationsare not clear enough.
ibogaine dosesibogaine
C,,,,.x, ng/mLVJF, I/kgf]/2 (last phase), hAiJCti..24i,, ngxh/mLTissular distribution (tissue/blood
concentration ratios)
Noribogaine
C,nnx. ng/mLC241T ng/mLAUCiv_24i,, ngxh/mLTissular distribution (Ussue/blood
concenlratioii ratios)
500-800 mg
230-1250134-7—Spleen: 1.78Liver: 3.75Brain: 1.16Lung: 4.64Bile: 1.97
5700-1200300-800—Spleen: 0,83Liver: 2.43Brain: 0.90Lung: 2,69Bile: 0.54
Extensive metoholizersin = 24r10 mg/kg
1.7737—7.53936—
6.2949—14705—
Poor metaboHzers(n = 5/""
10 mg/kg
2.5896——11471—
3.2105—3646—
/I. numliur of .subjects; C^conciîntratinn-time curve;
x. maximum concentration: /,„„«, time of C,,,,, ; C-^AU- concentration 24 h post-doso: AUCo_:.4,, steady-state volume of distribution: Í.,,. half-life.
area under
IbogaJne, an anti-addictive drugR MaOiulaitis, et al.
190
opiatewithdrawal
Personal newexperience
Kvductiunordrug craving
Acute phase wilh"tinL-iric"experiences(onset: I-.Í h.duration: 4-Sh)
Reduction ol'iimgwithdrawal
Evaluative phase with"neutral" and "rcncclivc"emotional tone
(onsci: 4'X li. duration: X-20 h)
Reduction ofdepression anddrug craving (up toone tnonth)
ResidualStimulation ;iliiist:with rcttim ufluirnial alluciilumül'aiicnlicín (unset:I2-Ü4h. diiratiun:24-72 hi
RepurlvdceAüution ul drii^uselupioniorethan 1 year)*
• Reported eessal i on from thesatupleof 41 individuals nine individuals were treated (wieeandonc was treated threelimes fora total of 52 treuinicnts, I'illcen (2'3''-'o) tiftlic ircutmcnts were reportedly followed by cessaliun dnig use torless ihan 2 months. 15 (2')''«) for at least 2 months and icss thuii 6 nionths. 7 ( i }."<, ) for at leysl 6 months und less thanone yctir. 10 (19%) for u period of greater thnn one year (8. H9, 93).
Figure 3 Clinical pharmacodynamic effects after ibogaine administration.
The second phase [evaluative phase) startsapproximately 4-8 h after ingestion and lasts8-20 h. During tliis phase, dreams decreased slowlyand the emotional tone is generally described asneutral and reflective. Patients reflect that theirattention is focused on inner subjective experiences(i.e., hy evaluating liie experiences of the acutephase).
During these two first phases, patients tend to stayfocused on their experiences and avoid any externaldistraction.
The third phase (residual stimulation phase)starts 12-24 h after exposure and lasts 24-72 h.Patients regain normal attention to the external envi-ronment. Subjective psychoactive experience les-sens, remaining with mild residual suhjectivearousal or alertness. Decrease in the need to sleepfor several days to weeks can he observed.
Reductions of withdrawal signs and symptoms, drugcraving and depression After administration of6-29 nig/kg dose of ibogaine, acute reduction indrug craving and opiate withdrawal signs and symp-toms are observed in 1-2 h. Resolution of with-drawal was observed during 1 week, reduction ofcraving and depression - 1 month after exposure.
Opiate physical dependence is assessed usuallyby discontinuation of opiate treatment (spontaneouswithdrawal) or by antagonist-precipitatedwithdrawal.'*^ Usually, acute withdrawal syndromein case of heroin addiction may begin approximately8 h after the last heroin dose, peaks in intensity at24-28 h, and subsides within 7-10 days. In one ofthe opiate (heroin or methadone] addiction studiesincluding 32 patients, rapid detoxifications of thesepatients was assessed after single-dose ibogainetreatment (10 mg/kg). Results are summarized inTable 4. The post-ibogaine Objective Opiate With-drawal Scale (OOWS) blinded rating obtained 10-
12 h and 24 h after ihogaine administration (i.e., 24and 3fi h after the last dose of opiate, respectively)was statistically lower than the rating obtained 1 hbefore ibogaine administration. The OOWS meantotal score decreases from approximately 5.6 to 1.1and 1.9, 12, and 24 h following ihogaine administra-tion, respectively. Authors noticed that objectivesigns of opiate withdrawal were rarely seen andnone were exacerbated at later time points.
A second measurement used was "self-reports ofwithdrawal symptoms according to Opiate-Symptom Checklist" (OP-SCL). Tbis "discanifort"measurement showed statistically significantdecreases in mean scores: from approximately 21(score observed 24 h before ibogaine treatment) to12 shortly after recovery from ibogaine treatment(<72 h) and down to 7 (at program discharge,approximately 6-9 days later).
Impressive success of single dose of ibogainedetoxification process was noticed as well as the factthat many ofthe patients were able to maintain absti-nence over the months following detoxification.''''This relatively small study suggests that methadonewithdrawal was not more difficult to detoxify thanheroin withdrawal. Speculation that long-actingmetabolite noribogaine may account for the efficacyof ibogaine can be done.
Craving is an important symptom reported byopiate-dependent subjects during tlie early stages ofwithdrawal contributing to continued drug use.'*'*"^Craving symptoms for opiates could be evaluated byusing the "Heroin Craving Questionnaire scales(HCQN-29)". Thirty-six hour post-ibogaine treat-ment, the mean scores on five measures about spe-cific aspects of drug craving (including urges,thoughts about drug of choice, or plans to use thedrug) show significant decreases and lasted at pro-gram discharge.

Ibogaine, an anti-addictive drugR Maiiulailis, ef a!.
191Evaluation of patients using Beck Depression
Inventory scores showed also significant reductionof scores both at program discharge and at 1-monthfollow-up assessments.''"•^''
Subjects undergoing cocaine detoxification alsoreported significant decrease in drug-craving 36 hpost-ibogaine treatment and at discharge for threeof the five category scales of the Cocaine CravingQuestionnaire (CCQN)-45 (anticipation of positiveoutcomes, relief of negative states, and lack ofcontrol).
Tbere is only limited retrospective experience inlong-term outcomes (Figure a].«-»"-*» No clear nega-tive or positive conclusions could be drawn. Itseems that relapses could he attempted with ibo-gaine re-challenge, as this was done several timesin anecdotal cases.
It seems that pharmacodynamic effects experi-enced by patients varied and may be related todose. bioavailability. and interindividualvariabilities.** Sequential pattern of clinical pharma-codynamic effects could be summarized as pre-sented in Figure 3.
Clinical safety
Neurotoxicity observed in animal studies was alsonoticed in human studies (e.g., effects on posturalstability, body tremor, and appendicular tremor]. In1994, a fatal case of woman treated with ibogainewas reported. Fifteen months before her death, thiswoman had undergone four separate treatmentswith ibogaine in rather high dosages (ranging from10 to 30 mg/kg). Death was not attributed to ibogainebut was related to mesenteric arterial tlirombosisrelated to chronic cellulitis.*-"
Similar to the findings in animals, some cardiacside-effects were also observed during clinicalinvestigations.^""* Thirty-nine patients dependent
on cocaine and/or heroin, who received fixed oraldoses of ibogaine of 500, 600, 800, or 1000 mg,were monitored. Six suhjects exhibited some signifi-cant decrease of resting pulse rate; one of them evi-denced a significant decrease in blood pressure(attributed to a transient vasovagal response). Noevidence of electrocardiogram abnormalities wasshowed. There were hypotensive episodes (respon-sive to volume repletion) noticed during ibogainetlierapy in some cocaine-dependent subjects.•'^
The safety of ibogaine was also evaluated in morethan 150 drug-dependent subjects receiving H, 10, or12 mg/kg ibogaine.'^" The most frequent side-effectsencountered were nausea and mild tremor, andataxia earliest after drug administration. A hypoten-sion was obsen'ed in some cocaine-dependent sub-jects, who required close monitoring of blood pres-sure. No other significant adverse events were seenunder the study conditions; and, therefore, there areno clear evidences till now that there are big issuesin tolerance after single dose of ibogaine.
In conclusion, clinical development could be con-sidered as started only and needs essential explor-atory program first.
Main unanswered questions
Experience available in public domain suggests thatibogaine might have some activity in anti-addictiontreatment. Although data seems quite promising,several issues remain to be elucidated first beforemoving fiu-ther towards controlled pivotal clinicaltrials. Four major product development issues to besolved relates to the areas of pharmaceutical formu-lation development and starting clinical exploratorystudies:
1) Is ibogaine pharmaceutical formulation devel-oped enough to ensure proper constant composi-tion form certain active ingredients?
Table 4 Effects uf single-dose ibogaine (10 mg/kg) on opiate withdrawal signs
Time after Time afterthe. ¡así opiate done, h tha ibogaine dose, h
OOWS OP-SCL HCQN-29-' BDI
Before ibogaine treatment
Dischargel-month follow-up
2436
10-122436<72h6-9 days
5.6 (11.1*1.9*
h) 21
12'7"
(24 h) 3
1
1
.26-4.88
.57-3.67
.22-2,85***
Iti,9
10.4
3.0**2.29**
OOWS. Objeclivo Opiate VVitlidrawal Scale; OP-SCL. Opiate-Symptom Checklist; HCQN-29. Heroin Craving Questionnaire scales (sub-scaics: desirn to use, intention to use. anticipation of positive outcomes, relief of negative states and lack of control); BDI. BeckDepression inventory scores."According tu the subscale.*P<0.05; **i*< 0.0005; •**P<ü.Oüül.

Ibogaine, an anti-addictive drugR Maciulaitis, et al.
192
2) What is ibogaines' pharmacodynamic activity incontrolled exploratory trial in drug-dependentstabilized subjects?
3) What is ibogaines' potential for abuse by drug-dependent subjects (in both pharmacodynamicand economic measurements)?
4) What is the most rational dosage range to be stud-ied in dose-response studies in treatment ofsome drug dependences [first, in opiate and/orcocaine dependencies?
References
1 Smitli. CG. O'Domiell. J. The process of new drug dis-covery and development. 2nd ed. New York: InformaHealthcare: 2006.
2 Atkinson. A|. Abemethy, D. Daniels, C, Dedrick, R.Markey, S. Principies of clinical pharmacülogy. 2nded. Amsterdam: Boston Elsevier/Academic Press;2007.
3 Jenks. CW. Extraction studies of Tabernanthe ibogaand Voacanga africana. Nat Prod Lett 2002; 16: 71-76.
4 Mash. DC. Kovera, CA, Buck, BE. Norenberg, MD.Shapshak. P. Hearn, WL. Medication development ofibogaine as a phannacoUierapy for drug dependence.Ann N Y Acad Sei 1998; 844: 274-292.
5 Coldblatt. A. Hootele. C, Pécher. J. The alkaloids ofVocanga TbouarsH Var. Obtusa. Phytochemistty1970; 9: 1293-1298.
6 Andrade. MT. Pinto. AC. Rozende, CM. Carvalho. MP.Epifaniü, RA. Indole alkaloids from Tabemaemontnnaaustralis (Muëll. Arg) Miers that inhibit acotylcholin-esterase enzyme. Bioorg Med Chem 2005; 13: 4092-4095.
7 Knox, [R, Slobhe. J. Alkaloids of Ervatamia orientaUs.Isolation of alkaloids and structural identification oftwo dimers. Aunt J Chem 1975; 28: 1813-1856.
8 Alper. KR, Ibogain«: a revie-w. The alkaloids.Academic Press. San Diego, Caiifornia; 2001.
9 Goutarel, R. Gollnhofer, O, Sillans, R. Pharmacody-namics and therapeutic applications of Iboga and Ibo-gaiiiB. Psychedf^lic Monogr Essays 1993: 6: 71-111.
10 Dybowski. E. Plant Chemi.stry Concerning Ihoga. ilsexcitement-producing properties, its composition,and the new alkaloid it contains, ibogaiue. C R AcadSd 1901; 133: 748.
11 Haller, A, Heckel. E. Sur l'ihogaine. principe actifd'une plante du genre Tabernaemontana. originairedu Congo. Compt Hend Acad Sei 1901; 133: 850-853.
12 Lambert. M. Heckel. E. Sur la racine d'Iboga et l'ibo-gaine. Cawpt Rend Acad Sei 1901; 133: 1236-1238.
13 Taylor, WI. Ihoga alkaloids. U. The structures of ibo-gaine. ihogamine and tahernanthine. / Am Chem Soc1957; 79: 3298-3299.
14 Arai, G, Coppola. J, Jeffrey, GA. The structure of ibo-gaine. Acta Cryst 1960; 13; 553-564.
15 Wenkert, E. Cochran, DW, GotlUeb. HE, Hagaman, EW.13C-NMR. Spectroscopy of naturally occurring sub-stances. XLV. lhoga alkaloids. Helv Chim Ada 1976;59; 2437-2442.
ConclusionExperience available in public domain suggests thatibogaine might have some activity in anti-addictiontreatment, but current data are not sufficient to dofurtlier in development. Data gathered during morethan 100 years of pharmaceutical, non-clinical, andclinical developments need to be validated. Goodlaboratory and clinical practice environment isessential for future investigations. Several majorobjectives of preclinical and clinical investigationssbould focus on core-identified questions first.
16 Büchi, C. Coffen. DL. Kocsis. K. Sonnet. PE, Ziegler,FE. The total synthesis of ihoga alkaloids. ¡Am ChemSoc 1966: 88: 3099-3109.
17 Bocher. DP, Naranjo, C. French Special Drug patentNo. 138.081:081713m. Inst Class A61k. 1969.
18 Lotsof, HS. Inventor rapid method for interrupting thenarcotic addiction syndrome. US patent 4,499,096.1985.
19 Lotsof. HS. Inventor rapid method for interrupting thecocaine anH amphetamine abuse syndrome. US patent4.587.243. 1986.
20 Lotsof. HS. Inventor rapid method for attenuating thealcohol dependency syndrome. US patent 4.857,523.1989.
21 Lotsof. HS. Inventor rapid method for interrupting orattenuating poly-drug dependency .syndrome. US pat-ent 5,152,994. 1992.
22 Lotsof. HS. Inventor rapid method for interrupting orattenuating the nicotine/tobacco dependency syn-drome. US patent 5.026,697. 1991.
23 Shulgin, A, Shulgin, A. TIHKAL. The Continuation.Tryptamines I Have Known and Loved. TransformPress, Berkeley, California; 1997.
24 KoutrimaviCiûtê. V. Mathieu, O. Balas. L. Escale, R.Blayac, |P. Bressolle, FMM. Ihogaine and noribogaine:structural analysis and stability studies. Use of LG-MSto determine alkaloid contents from root bark ofTabernnnthe ¡boga. / Liquid Chromatogr Analyt Tech-no} Biomed Life Sei 2007; 30; 1077-1092.
25 Taylor. WI. The ihoga and Vocanca alkaloids. Thealkaloids. Chemistry and Physiology. AcademicPress. San Diego. California; 1965.
26 Popik. P, Skolnick. P. Pharmacology of ibogaine andibogaine-related alkaloids. The alkaloids. Academicpress; 1999.
27 Ktmtrimaviiiûtè, V. Larroque. M. Briedis. V. Margout.D, Bressolle, F. Quantitation of ihogaine and 12-hydroxy-ihogaine in human plasma by liquid chroma-tography with fluorimetric detection. / Cbromatogr BAnalyt Technol Biomed Life Sei 2005; 822: 285-293.
28 Dhahir. HI. Jain, NC. Forney. RB. Methods for thedetection and determination of ibogaine in l)iülogit:almaterials. ¡Forensic Sei 1971; 16: 103-108.
29 Bertol, E, Mari, F, Froldi, R. Détection de l'ibogaïnedans les liquides organiques, ¡Chromatogr 1970; 117:239-241.
30 Daguino. D. Schripsema. J, Peltenhurg. A, Verpoorte, R.Teunis, K-. Gapillary gas Chromatographie analysis ofindole alkaloids: investigation of the indole alkaloidspresent in Tabernaemontana divaricata cell suspensionculture.//VnfProt/1991: 54; 1558-1563.

ibogaine, an anti-addicttve drugR Mai;iulaitis, ei al.
19331 Cartoni, GP, Giarusso, A. Gas Chromatographie deter-
mination of ibogaine in biological fluids. / Chromatogr1972; 71; 154-158.
32 Gallagher. CA. Hough. LB, Keefner. SM. Seyed-Mozaffari. A, Archer, S, Glick, SD. Identification andquantification of the indole alkaloid ihogaine in hio-logical samples by gas chromatography-mass spec-trometry. Biochem Pharmacol 1995; 49; 73-79.
33 Ley, FR, leffcoat, AR, Thomas, BF. Determination ofihogaine in plasma by gas chromatography-chemicalionization mass spectrometry. / Chromatogr A 1996;723; 101-109.
34 Hearn. WL. Pablo, J. Hime, GW, Mash, DC. Identifica-tion and quantitation of ibogaine and ano-demethylated metabolite in brain and biologicalfluids using gas chromatography-mass spectrometry.} Anal Toxicol 1995; 19; 427-434.
35 Alburges, ME, Foltz, RL, Moody, DE. Determination ofihogaine and 12-hydroxy-ibogamine in plasma by gaschromatography-positive ion chemical ionization-mass spectrometry. ¡Anal Toxicol 1995; 19; 381-386.
36 Bogusz, MJ. Maier. RD, Kniger, KD, Kohls. U. Determi-nation of common drugs of abuse in body fluids usingone isolation procedure and liquid cliromatography-atmospheric-pre.ssure chemical-ionization mass spec-trometry. //Ino/ Toxicol 1998; 22:549-558.
37 Konti-imaviciûtc. V, Breton, H. Mathieu. O, Mathieu-Daudé. [C. Bressoüe, F. Liquid chromatography-electrospray mass spectrometry determination of ibo-gaine and noribogaine in human plasma and wholehtood. Application to a poisoning involving Taber-nanthe iboga root. / Chromatogr B Analyt Techno!Biomed Life Sei 2006; 843; 131-141.
38 KontrimaviCifitè. V, Breton. H, Barnay. F. Mathieu-Daudé. JC, Bressolle, F. Liquid chromatography-electrospray mass spectrometry determination of ibo-gaine and 12-hydroxy-ibogaminB in human urine.Chromatographia 2006; 63: 533-541.
39 Naranjo, C. Psychotherapeutic possibilities of newfantasy-enbancing drugs. Clin Toxicol 1969; 2; 209-224.
40 Sheppard. SG. A preliminary investigation of ibogaine;case reports and recommendations for further study./ Subst Abuse Treat 1994; 11; 379-385.
41 Schechter. MD. Gordon, TL. Comparison of the behav-ioral effects of ibogaine from three sources; mediationof discriminative activity. Eur / Pharmacol 1993; 249;79-84.
42 Pearl, SM, Hough, LB, Boyd, DL, Click, SD. Sex differ-ences in ihogaine antagonism of morphine-inducedlocomotor activity and in ibogaine hrain levels andmetaholism. Pharmacol Biochem Behav 1997; 57:809-815.
43 leffcoat. AR, Cook, CE, Hill. JM. Coleman, DP. Pollack,CM. Disposition of [3H1 ibogaine in the rat. NationalInstitute on Drug Ahuse Research Monograph Series,Bethesda. 1994; 141; 309.
44 Hough, LB, Bagal, AA, Glick, SD. Pharmacokineticcharacterization of the indole alkaloid ibogaine inraLs. Methods Find Exp Clin Pharmacol 2000; 22; 77-81.
45 Huugh. LB. Pearl. SM. Glick. SD. Tissue distribution ofibogaine after intraperitoneal and subcutaneousadministration. Life Sai 1996; 58; 119-122.
46 Glick, SD, Pearl, SM, Caí, J. Maisonneuve, IM.Ibogaine-like effects of noribogaine in rats. Brain Res1996; 713; 294-297.
47 Zubaran. C, Shoaib. M, Stolernian, IP, Pablo, ), Mash,DC. Noribogaine generalization to the ihogaint! slimu-lus: correlation with norihogaine concentration in ratbrain. Neuropsvchophnrmarohgv 1^99: 21; 119-126.
48 Staley, JK, Ouyang, Q. Pablo, |. Hearn. WL, Flynn. DD,Rotlnnan, RB. Pharma(;ologic;al screen for activities of12-hydroxyihogamine; a primary metabolite of theindole alkaloid ibogaine. Psychopharmacology 1996;127; 10-18.
49 Mash. DC. Kovera, CA. Pablo, J, Tyndale. R. Ervin, FR.Kamlet, JD. fhogaine in the treatment of heroin with-drawal. Alkaloids Clwm Biol 20Ü1; 56; 155-171.
50 Obach, RS. Pablo. I. Mash. DC. Cytochrome P4502D6catalyzes Üie 0-deniethylalion of the psychnactivealkaloid ibogaino to 12-hydroxyibogamine. DrugMetab Dispos 1998; 26; 764-768.
51 Baumann. MH. Rothman. RB. Pablo. J. Mash. DC. Invivo neurobiological effects of ibogaine and its O-desmethyl metabolite, 12-hydroxyibogaine (noriho-gaine) in rats. / Pharmacol Exp Ther 2001; 297: 531-539.
52 Zubaran. G. Ibogaine and uorihogaine; comparing par-ent compound to metaholite. CNS Drug Reviews 2000;6; 219-240.
53 Mash. DC. Staley. IK. Baumann, MH, Rothman, RB.Hearn. WL. Identification of a primary metabolite ofibogaine that targets serotonin transporters and ele-vates serotonin. Life Sei 1995; 57; 45-50.
54 Baumann. MH. Pablo. I. Ali. SF. Rothman. RB. Mash.DC. Comparative neuropharmacology of ibogaine andits O-desniethyl metabolite, noribogaine. Alkaloids2001; 56; 79-113.
55 Baumann. MH, Pablo, f. Ali. SF. Rothman, RB. Mash.DC. Noribogaine (12-hydroxyihogamine); a biologi-cally active metabolite of the antiaddit;tive drug ibo-gaine. Ann NY Acad Sei 2000; 914; 354-368.
56 Mash. DC. Kovera. CA, Pablo, ]. Tyndale. R. Ervin. FR,Williams, IG. Ibogaine; complex pharmacokinetics.concerns for safety, and preliminary efficacy mea-sures. Ann N Y Aead Sei 2000; 914; 394-401. '
57 Pablo. JP. Mash. DG. Noribogaine stimulates naloxone-sensitive |35SÍ GTPgammaS binding. Neu rove port1998; 9; 109-114.
58 Mash. DC, Kovera. CA. Buck. BE, Norenherg. MD,Shapshak, P, Hearn, WL. Medication development ofibogaine as a pharmacotherapy for drug dependence.Ann M ' Acad Sei 1998; 844; 2'74-292.
59 Click. SD, Maisonneuve. IS. Mechanisms of antiaddic-tive actions of ibogaine. Ann N Y Acad Sei 1998; 844;214-226.
fiO Rabin, RA, Winter, }C. Effects of ibogaine and noribo-gaine on phosphoinositide hydrolysis. Brain Res 1996;731; 226-229.
61 Rabin, RA. Winter. fC. Ibogaine and noribogainepotentiate the inhihition of adenylyl cyclase activityby opioid and 5-HT receptors. Eur J Pharmacol 1996;316; 343-348.
62 Paêkulin. R, lamnik, P. ¿ivin, M, Raspor, P, Strukelj. B.Ibogaine effects brain energy metaholism. Eur } Phar-maeol 2006; 552; 11-14.
63 He, DY. McGough. NN, Ravindranatban, A, Jeanblanc.]. Logrip, ML. Phomluong, K. et al. Glial cell line-

Ibogaine, an anti-addictive drugR Mac-iulaitis, ei al.
194derived neurotrophic factor mediates the desirableactions of the anti-addiction drug ¡hogaine gains alco-hol consumption. / Ntiumsci 2Ü05; 25; fil9-fi28.
64 He. DY. Ron, D. Autoregulation of glial cell line-derived neurotrophic tactor expression: implicationsfor the long-lasting actions of the anti-addiction drug.Ibogaine. FASEB ¡ 2Q0e,: 20: 2420-2422.
65 Gonzalez, G, Oiiveto. A, Kosten, TR. Treatment of her-oin (diamorphine) addiction: current approaches andfuture prospects. Drugs 2002; 62: 1331-1343.
66 Gorntick, DA. Gardner, EL, Xi, ZX. Agents in develop-ment for the management of cocaine abuse. Drugs2004:64; 1547-1573.
67 Glick. SD, Rossman, K, Steindorf, S, Maisonneuve. IM,Garlson. M. Effects and afterc ffects of ibogaine on mor-phine stilf-adniinistration in rats. Eur f Pharmacol1991: 195: 341-345.
68 Dzoljic, ED. Kaplan. CD, Dzoljic. MR. Effect of ibo-gaine on naloxone-precipitated withdrawal syndromein chronic morphine-dependent rat.s. Arch int Phar-niacodvn Thev 1988: 294: 64-70.
69 Glick, SD, Gallagher, GA. Hough. LB. Rossman, KL,Maisonneuve. IM. Differential effects of ibogaine pre-treatment on brain levels of morphine and [+)-amphetamine. Bmin Res 1992; 588: 173-176.
70 Gappendijk. SL. Dzoljic, MR. hihlbilory effects of ibo-gaine on cocaine self-administration in rats. Eur JPharmacol 1993; 241: 261-265.
71 Sershen. H, Hasbim. A. Lajtba. A. Ibogaine reducespreference for cocaine consmnption in G57BL/6Bymice. Pharmacoi Biochem Behav 1994; 47: 13-19.
72 Glick. SD, Knehne, ME. Raucci. ), Wilson. TE. Larson,D, Keller, RW. et a¡. Effects of iboga alkaloids on mor-pbine and cocaine self-administration in rats; relation-sbip to treniorigenic effects and to effects on tlopaminerelease in nucleus accumbens and striatum. Brain Bes1994; 657: 14-22.
73 Dworkin, SI, Gleeson, S, Meloni, D, Koves, TR. Martin.T. Effects of ibogaine on responding maintained byfood. c:ocaine and heroin reinforcement in rats.Psychopharmacology 1995; 117: 257-261.
74 Glick, SD, Rossman. K, Rao. NC. Maisonneuve. IM.Effects of ibogaine on acute signs of morphine with-drawal in rats: independence from tremor. Neurophar-macology 1992; 31: 497-500.
75 Aceto. MD, Bowman. ER. Harris. LS, May. EL. Depen-dence studies on new compounds in tbe rhesus mon-key, rat and mouse. NIDA Res Monogr 1989: 95; 578-631.
76 Aceto. MD. Bowman. ER. Harris. LS. May, EL, Depen-dence studies of new compounds in the rhesus mon-key and mouse. NIDA Res Monogr 1990; 105: 640-681.
77 Sharpe. LG. Jaffe, JH. Ibogaine fails to reducenaloxone-precipitated witbdrawal in tbe morpbine-dependent rat. Ntniroreport 1990; 1: 17-19.
78 Popik. P. Layer. RT. Fossnm. LH. Braveniste. M.Gtíter-Douglass. B. Witkin, JM. et oi. NMDA antagonistproperties of the putative antiaddictive drug, ibogaine./ Pharmacol Exp Ther 1995: 275: 753-760.
79 Frances. B, Gout. R. Cros. J, Zajac. JM. Effects of ibo-gaine on naloxone-precipilated wilbdrawal inmorpbine-dependent mice. Fundam CUn Pharmacol1992; 6: 327-332.
80 O'Hearn. E, Molliver, ME. Tbe olivocerebellar projec-tion mediates ibogaine-induced degeneration of Pur-kinje cells: a model of indirect, trans-synaptic excito-toxicity. / Nmirosci 1997; 17: 8828-8841.
81 Xu. Z, Chang. LW. Slikker. W, Ali. SF. Rountree. RL.Scallet, AG. A dose-response study of ibogaine-induced neuropathology in tbe rat cerebellum. ToxicolSci 2000: 57: 95-101,
82 Helsley, S, Dlugos. CA, Pentney, R|. Rabin, RA.Winter, JC. Effects of cbronic ibogaine treatment oncerebellar Purkinje cells in the rat. Brain Res 1997;759; 306-308.
83 Scallet. AG, Ye, X. Rountree. R, Nony, P. Ali. SF, Ibo-gaine produces neurodegeneration in rat. but notmouse, cerebellum. Nourohistological biomarkers ofPurkinje cell loss. Ann N Y Acad Sei 1996; 801: 217-226.
84 Glick, SD. Maisonneuve, IM, Szumlinski, KK. Meclian-isms of action of ibogaine: relevance to putative thera-peutic effects and development of a safer iboga alka-loid congener. Alkaloids Ciiem Bid 2001; 56: 39-53.
85 Biniiinda. Z. Beaudoin, MA. Thorn, BT, Prapurna, DK.Johnson. JR. Fogle, CM. Alteration of electroencepha-logram and monoamine concentrations in rat brain fol-lowing ibogaine treatment. Ann JV Y Acad Sei 1998;844; 265-273.
86 Alper. KR. Lotsof. HS, Frenken, GM, Luciano, DJ,Bastiaans. J. Treatment of acute opioid withdrawalwith ibogaine. Aw ¡Addict 1999; 8: 234-242.
87 Alper. KR, Lotsof. HS. Frenken. GM. Luciano. DI.Bastiaans. J, Ibogaine in acute opioid withdrawal. Anopen label case series. Ann N Y Acad Sei 2000; 909:257-259,
88 Lotsof. HS. Ibogaine in tbe treatment of chemicaldependence disorders: Clinical Perspectives (APreliminary Review]. Multidisciplinary Associationfor Psychedelic Studies Bulletin: 1995: 5: 16-27.
89 MDD-NIDA, Draft protocol: Rising Dose ToleranceStudy using single administration to assess tbe safetyand preliminary efficacy of ibogaine for the treatmentof cocaine and/or heroin dependency. Rockville.Maryland: NIDA: 1993.
90 Vastag. B. Addiction treatment strives for legitimacy./aji]a2002; 288; 9-101.
91 Kontrimavidiûté. V. Mathieu, O. Mathieu-Daudé, IG.Vainauskas, P, Casper. T, Bac;[:ino. E, et al. Distribu-tion of ibogaine and noribogaine in a man following apoisoning involving root bark of the Tabernantheiboga sbrub. ¡Ana! Toxicol 2006; 30: 434^40.
92 Best. SE. Olivieto. AH. Kosten. TR. Opioid addiction -recent advances in detoxification and maintenancetherapy, CNS Drugs 1996; 6: 301-.114.
93 Lotsof. HS. Ibogaine in tbe treatment of chemicaldependency disorders. Pre.sonted to ihe NIDA-Sponsored Ibogaine Review Meeting. Rockville. MD.March 1995,
94 Masb, DC, Allen-Ferdinand, K. Mayor. M. Kovera. CA,Ayafore, JF, Williams, IC, et al. Ibogaine: Clinit;«!observations of safety after single dose administra-tions. Problems of Dnig Dependence 1998;Proceedings of tbe Sixtietb Annual Meeting. TheCollege of Problems on Drug Dependence. Inc. NIDAResearch Monograph. US Dept. of Health and HumanServices. Betbesda. Maryland. 1999; 179: 294.
