i n t e g r i t y - s e r v i c e - e x c e l l e n c e 122 nd mdg 48r – rsv training brian j....
TRANSCRIPT

I n t e g r i t y - S e r v i c e - E x c e l l e n c e
122nd MDG
48R – RSV TrainingBrian J. Dykstra, Col, SFS, INANG
AE Overview

Indiana Air National Guard
Disclaimer
• The content is mine and not official DoD, USAF, or ANG doctrine/policy
• I used notes and pictures from other sources on the Kx exchange as well as the internet
• I have been deployed as a CCATT doc in Balad 2007, Bagram 2008, Ramstein 2011, and as a SME in Bagram/Kuwait 2014-15 (while deployed as a SME I flew a number of AE missions on C130s), March ‘15 I flew the weekly PACAF AE mission
• I have no commercial relationships or any conflicts of interest

Indiana Air National Guard
Objectives
• RSV Training for AEo Medical Clearance for AE (perform 5); suitable substitute if unable
to perform clearances: Read relevant sections of Flight Surgeon’s Guide and SGP Tactics Guide
• AE Overviewo Medical / Flight Surgeon concerns and responsibilities for AE and
AE patient processingo What is AEo Capabilities of AEo Process of AEo Definitions/Acronyms

Indiana Air National Guard
AE Definition
• AE is the movement of patients under medical supervision to and between medical treatment facilities by air transportationo AE specifically refers to United States Air Force evacuation
movement of regulated casualties, using organic airframes, with AE aircrew specifically trained for this mission
• Capabilitieso Integrated control of casualty movement by air transporto Clinical & Ops support personnel to complete the missiono Inflight and ground support personnel; equipmento En route staging capability (ERPSS): ASF/MASF/CASF

Indiana Air National Guard

Indiana Air National Guard
Guidance
• Some Regs:o AFPD 10-29, World Wide AE Ops – Establishes policy and assigns
responsibilities for AE Opso AFI 41-307o AFI 10-2912 o AFTTP 3-42.5

Indiana Air National Guard
Basic Movement Process
• Point of Injury (POI)• CASEVAC to 1st MTF/CSF then MEDEVAC to ASF• At ASF PMR (Patient Movement Request) placed into TRAC2ES
(TRANSCOM Regulating Command & Control Evacuation System) to move patient AEROVAC
• Request vs Requiremento Physicians at originating or accepting facilities submit requests for
movement, timing, destinationo Validating Flight Surgeon and PMRC validate those requests into
airlift “requirements”

Indiana Air National Guard
Basic Movement Process Con’t
• Validation by FS (VFS) occurs at PMRC (Patient Movement Requirement Center)
• VFS brings medical leadership and decision making to the process of prioritizing use of aviation assetso 1st question VFS asks is whether patient should fly at all
• Validation vs Clearanceo Clearance to move by air is done at the MTF, i.e. is patient stable
for flighto Validation for AE, located at PMRCo AE clearance is a medical care event; validation is a logistic, not a
medical event

Indiana Air National Guard
Basic Movement Process Con’t
• Transformation from a request into airlift requirement: the Patient Movement Clinical Coordinator (PMCC) at the PMRC obtains necessary clinical data and medical equipment requirements from attending physician prior to manifesting patient for movement
• PMRC provides medical regulating and AE scheduling for transport to next higher level of careo AE airlift planners of AE Control Team (AECT) w/in Air Mobility
Division (AMD) of the Air Operations Center (AOC) recognize and respond only to validated requirements
o AE airlift planners work closely w/ the PMRC in coordination
• AOC identifies and tasks aircraft and resources

Indiana Air National Guard
FS Responsibilities
• Local clearance authority, i.e. is patient physiologically ready for air travel & Category (urgent, priority, routine)
• May fly as medical attendant (MA) if necessary• If at an ASF (Aeromedical Staging Facility): Evaluates/manages
patients• Interacts w/ originating physician by defining level of care & care
plan en routeo Assess appropriateness of AEo Ensure patient stability / stabilized (if CCATT required)
• Assess movement precedence – determine priority• Works closely with VFS• Begins/completes the 3899 - PMR

Indiana Air National Guard
FS Responsibilities
• Clearing FS must consider:o Ability to travel vs need for definitive careo Flight schedules and prep timeo Travel time, including possible stops
Some flights around the AOR make multiple stopso Medical capabilities/resources at any stopso Attendant (medical/non-med) qualifications

Indiana Air National Guard
3899 - PMR

Indiana Air National Guard
Patient Precedence (Priority)
• Urgento Temporarily “stabilized”o Goal: movement w/n 12 hourso Life, limb, eyesighto ISS – In-system select (cargo mission disrupted to support AE
mission)o Most likely needs CCATT
• Priorityo Stabilizedo w/n 24 hours, can’t wait for next scheduled flight, may be ISS
• Routineo Stable, capable of waiting up to 72 hrs on next scheduled mission

Indiana Air National Guard
Fixed Wing Options

Indiana Air National Guard
Stresses of Flight
• Altitude/Decreased PaO2• Barometric pressure changes• Thermal changes (especially KC135s and C130s)• Decreased humidity• Noise• Vibration• Fatigue• Gravitational Forces• Long days

Indiana Air National Guard
Altitude Restriction
• Altitude restriction requires lower flight level which can lead to:o Increased fuel consumption – enough fuel for mission/flighto Lower altitude decreases speed and increases flight timeo May increase turbulence due to weather

Indiana Air National Guard
Altitude / Hypoxia
• Does the patient prior to flight need supplemental oxygen?• Will the patient during flight need supplemental oxygen?• What is the Hgb?
o If Hgb <8mg/dL, can only transport if anemia is chronic & stable and not related to bleeding, if Hct <25% need VFS concurrence
• Chronic low Hgbo 8.5-10mg – O2 available
o 7.0-8.5mg – O2 at 2L for flighto <7.0mg – AE VFS approval
• Post-Op anemiao 9.0-10mg – O2 available
o 8.0-9.0mg – O2 at 2L for flighto <8.0mg – AE VFS approval

Indiana Air National Guard
Humidity & Temperature
• At altitude, the air is much drier which can affect pulmonary secretionso O2 needs bubblero Vented patients need the HME
• C130 & KC135’s are very difficult with temperature controlo Significant temperature difference between the top and bottom of
the cabin
• Also consider temperature during transport to and from plane

Indiana Air National Guard
Barometric Pressure
• Complications of increased pressure/volume in body cavitieso Abdominal surgery
Abdominal compartment syndrome Respiratory embarrassment pushing up on the diaphragm Decreased blood return to the chest leading to decreased cardiac output
due to compression of great vessels in abdomen and increased intrathoracic pressure
Ostomy bags – need to vent collection bagso Chest
Pneumothorax – Need a Heimlich valveo Pain may increase – sinuses, ear drums
• ET & Tracheostomy tubes – check cuff at altitude and then upon landing
• Eye/Globe injuries – air in the globe

Indiana Air National Guard
Vibration
• Ortho patientso Fractureso External Fixators
• Other injuries & surgeries• Increases muscle fatigue to maintain balance
o May result in increased lactate due to muscular use which can then increase need for minute ventilation – is the patient capable to meet this demand for increased ventilation

Indiana Air National Guard
G-Forces
• For most part not a big deal• G-forces are primarily applicable to the neuro patients• Different planes fly at a different angle of attack at cruise• Generally keep head forward facing

Indiana Air National Guard
Noise
• Increases stress & fatigue• Difficult to communicate – both from patient to AE crew and
amongst AE crew• Make sure patients have ear protection, especially important for
those who can’t insert the foamies

Indiana Air National Guard
Fatigue
• Due to the overall stresses of flight, even if patient is relatively stable the stresses of flight can lead to increased fatigueo Noiseo Vibrationo Temperature changeso Low humidityo Long dayo Long flight

Indiana Air National Guard
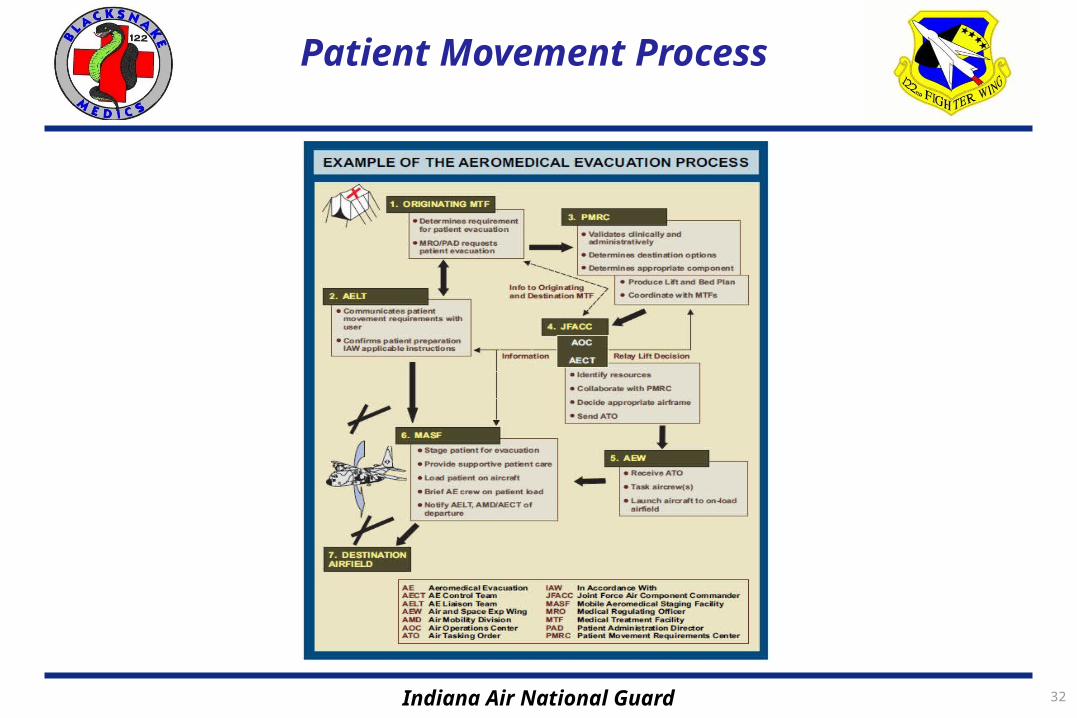
AE Process
• Originating MTF determines requirement for AEo MRO/PAD requests patient AE to AELT and PMRC
• AELT (AE Liaison Team)o Communicates pt movement requirementso Confirms pt prep
• PMRC (Patient Movement Requirement Center)o Validates clinically & administrativelyo Determines destinations optionso Determines appropriate componento Produces Lift and Bed Plan b/t originating & destination MTV

Indiana Air National Guard

Indiana Air National Guard
Contingency AE Structure

Indiana Air National Guard
Process Con’t
• JFACC (Joint Forces Air Component Commander)o AOC/AECT
Identifies resources Collaborates w/ PMRC Decides appropriate airframe Send ATO to AEW
• AEWo Receives ATO, tasks aircrew, launches aircraft to on-load airfield
• MASFo Stages pt for evac, supports pt careo Loads pt on aircraft, briefs AE crew on pt loado Notifies AELT, AMD/AECT of departure

Indiana Air National Guard
AE System Components
• AE Squadrono C2o AECMs (AE Crew Mbrs)o AELT (AE Liaison Teams)o AEOT (AE Operations Teams)o AE Support Cello AECT (AE Control Team)o AEOC (AE Operations Center)
• Ground Medical/MTFso Support Equipmento Specialized Equipmento ERPSS (En Route Patient Staging System)

Indiana Air National Guard
AE Squadron
• C2o Manpower: 8o AFMS officer cmd assigned to OG of the AMW
• AECMso Basic: 2FN & 3AETs (AE Techs); but can be augmentedo Requires AEOT support of mission launch, recovery, management,
supporto Directed by AOC in control of the airlift mission
• AELTo Manpower: 2o Immediate coordination b/t user service & USAF AE Systemo Highly mobile; embedded
Indiana Air National Guard
AE Squadron
• AEOTo Manpower: 8o Operational & mission management support to airfields conducting
AE opso Crew scheduling/mgt for AE crews & CCATTso Coordinates support requirements, aircraft configuration, logistics
& support, ramp operations
• AE Support Cello Manpower: 4o Admin, logistical, AGE maintenance, Comms

Indiana Air National Guard
AE Squadron
• AECTo Medical personnel trained in AE command & control attached w/n
the AMD of the AOCo Responsible for:
Ops planning Scheduling Tasking Execution Monitoring in coordination w/ air mobility controllers Coordinates w/ the J-4 medical branch on the JTF staff and the PMRC
on patient movement requirements and priorities
Indiana Air National Guard 32
Patient Movement Process

Indiana Air National Guard
Patient Classification
• 1 – Psycho 1A – severely ill, requiring close supervision: sedated, restrained,
on a dressed littero 1B – mod to severely ill: sedated, litter, restraints availableo 1C – cooperative, reliable, mod severe psych inpatient traveling
ambulatory status
• Litter categorieso 2A – who may or cannot ambulate and may be unable to perform
self care, requires assistance in event of emergencyo 2B – able to ambulate and sit in a seat, should be able to ambulate
in event of an emergency

Indiana Air National Guard
Patient Classifications con’t
• Ambulatory categorieso 3A – Inpatient, non-psych, requirement medical treatment, assistance or
observation en route (usually minimal), or returning from inpatient visit at a MTF
o 3B – Recovering inpatient, returning to home station, requires no medical attention en route
o 3C – Ambulatory drug or alcohol substance abuse inpatient going for treatment
• Infant categories: 4A – E• Outpatient categories: 5A-F• Attendant categories
o 6A – medical attendant (physician, nurse, tech)o 6B – non-medical attendant

Indiana Air National Guard
QUESTIONS