i clinical epidemiology roundsi - wordpress.com · i clinical epidemiology roundsi disagreements...
TRANSCRIPT
I CLINICAL EPIDEMIOLOGY ROUNDS I
Disagreements over clinical find-ings, diagnoses and managementdecisions are ubiquitous in med-
. and their discussion providesa fitting start to the Journal's clin-ical epidemiology rounds. Those ofus generating these rounds oftenconfront such disagreements in ourclinical practices, and we are pain-fully aware that they can result inboth the failure to help patientswho could be helped and the viola-tion of Hippocrates' admonition"Above all, do no harm".2 For ex-ample, to conclude that a patienthas hypertension when, in fact, hisor her blood pressure is normal isto subject the patient to the damageof being labelled hypertensive3 andto the cost and risk of the life-longuse of antihypertensive drugs. Simi-larly, the re-evaluation of a groupof children in whom organic cardiacdisease had been diagnosed resultedin the discovery that most of theactivity restriction and social dys-function had occurred among chil-dren with normal hearts who werethe victims of diagnostic error.4 Onthe other hand, if early rectal can-cer is missed in a woman withhemorrhoids and rectal bleeding thechance for cure may be lost.
In the first of our series of clin-ical epidemiology rounds we willpresent a number of cases of clin-ical disagreement to show how oftenit occurs in history-taking, in per-forming physical examinations, ininterpreting the results of diagnos-tic tests and in arriving at a clinicaldiagnosis, and will then considerthe etiology of clinical disagree-ment. In the second of our series, tobe published in the next issue, wewill present a set of clinical man-Reprint requests to: Dr. DL. Sackett,McMaster University Health SciencesCentre, 1200 Main St. W, Hamilton,Ont. L8N 3Z5
euvers for the prevention and con-trol of clinical disagreement, and astrategy clinicians can use to meas-ure and improve the accuracy andprecision of their clinical measure-ments and decisions.
Clinical disagreements can be oftwo sorts. First, our clinical judge-ment about a symptom, sign ordiagnosis can be shown to be wrong(inaccurate) in the light of other,"harder" evidence such as fromroentgenography, biopsy or autop-sy. Second, our clinical judgementcan be shown to be inconsistent(imprecise) if simultaneous clinicalexamination of the same patient byother clinicians (or a second ex-amination by us) leads to disagree-ment about the presence of specificpoints in the history or the physicalexamination. In either case clinicaldisagreement has occurred. Fur-thermore, the fact that two clini-cians agree is no sure protectionfrom error, for both may be wrong.Most studies of clinical disagree-ment focus on inconsistencies be-tween clinicians and, because theyinclude cases in which clinicians areconsistent but inaccurate, under-estimate the extent of the problem.
How often does clinical
disagreement occur?
History-taking
Case 1: A 46-year-old travellingsalesman has undergone proximalgastric vagotomy and pyloroplastyfor duodenal ulcer and you are as-sessing his response to surgery. Heis free of pain, has a fair appetiteand has not been troubled by nau-sea, reflux, vomiting, epigastric full-ness or dysphagia. However, youelicit a history of "dumping" severeenough to seriously interfere withhis job. A recent consultation notefrom the patient's surgeon, on the
other hand, indicates that thedumping is "mild'..Comment: A crucial element in
deciding whether to operate on onepatient with peptic ulcer is an as-sessment of the results of similaroperations performed on other pa-tients with peptic ulcer. Were theirsymptoms relieved? Did the proce-dure result in new, equally disablingsymptoms? Were the patients ableto return to full function at homeand on the job? Because the surgi-cal outcome in such patients is de-termined by a carefully taken,thorough history, conclusions aboutthe value of the operation dependon the skill, objectivity and con-sistency with which the history isobtained.How consistent are such his-
tories? If two clinicians interviewedthe same patient would they agreeabout the results of that patient'soperation for peptic ulcer - thatis, would the interobserver consist-ency be high? Unfortunately, evenseasoned clinicians often disagree.Indeed, after interviewing separatelya group of patients who had under-gone operations for peptic ulcer,two senior clinicians in a Britishhospital agreed in less than twothirds of the cases about whetherthe operation had been successful(using the Visick system for classi-fying symptoms and their severity).5Thus, at least one of these seasonedclinicians was wrong about the suc-cess of a patient's operation at leastone third of the time. Indeed, theclinicians conducting this studyquestioned whether the results ofulcer operations performed at dif-ferent centres could ever be com-pared as long as the problem ofclinical disagreement remains.
Other examples abound. Whenthree cardiologists interviewed 57men with chest pain, 54% of the
CMA JOURNAL/SEPTEMBER 20, 1980/VOL. 123 499
men were judgcd by at least oneclinician to have a history com-patible with angina pectoris.6 How-ever, in only 30% of the 57 pa-tients did all three clinicians agreeabout the history, and if one ofthe cardiologists concluded that agiven patient had angina pcctoris,the other two agreed with him only55% of the time.
Physical examination
Case 2: A 38-year-old executivewith primary hypertension had afifth-phase diastolic blood pressureof 115 mm Hg. After 6 weeks ofstep 2 therapy (a thiazide and a/.-adrenergic blocker) the diastolicpressure has fallen to 95 mm Hg.Although your examinations of heroptic fundi have consistently re-vealed only early arteriovenouscrossing changes, an ophthalmol-ogist who examined her earlier thisweek (during a visit for refraction)reported a small flame-shaped hem-orrhage near the left disc.Comment: Is clinical disagree-
ment less of a problem in physicalexamination? The quick answer isNo. Clinicians who examine thesame patient often disagree. Indeed,the clinician who examines thesame patient twice often disagreeswith his or her own earlier findings.
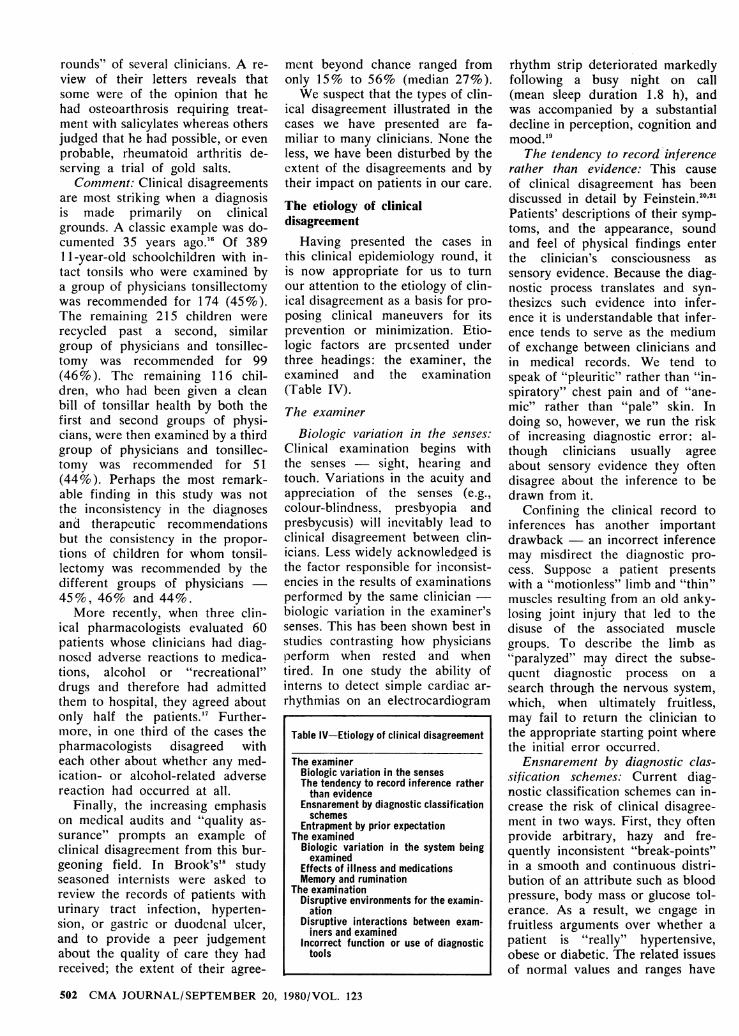
Examination of the optic fundusis a universally accepted componentof the physical examination of apatient suspected of having cardio-vascular disease or diabetes, and inhypertensive patients it may pro-vide a better index of prognosisthan measurement of the blooiJpressure. However, when two clini-cians examined the same set of 100photographs of the optic fundus theresults in Table I were generated.7Using the Keith-Wagener system ofclassification the clinicians agreedthat 46 patients had little or noretinopathy (grade 0 or 1) and thata further 32 patients had moderateor severe retinopathy (grade IIor 111) (interobserver agreement[46 + 32]/100 or 78%). Thus,they agreed with each other morethan three quarters of the time,which is better than the agreementabout the histories of patients whohad undergone operations for pep-tic ulcer.
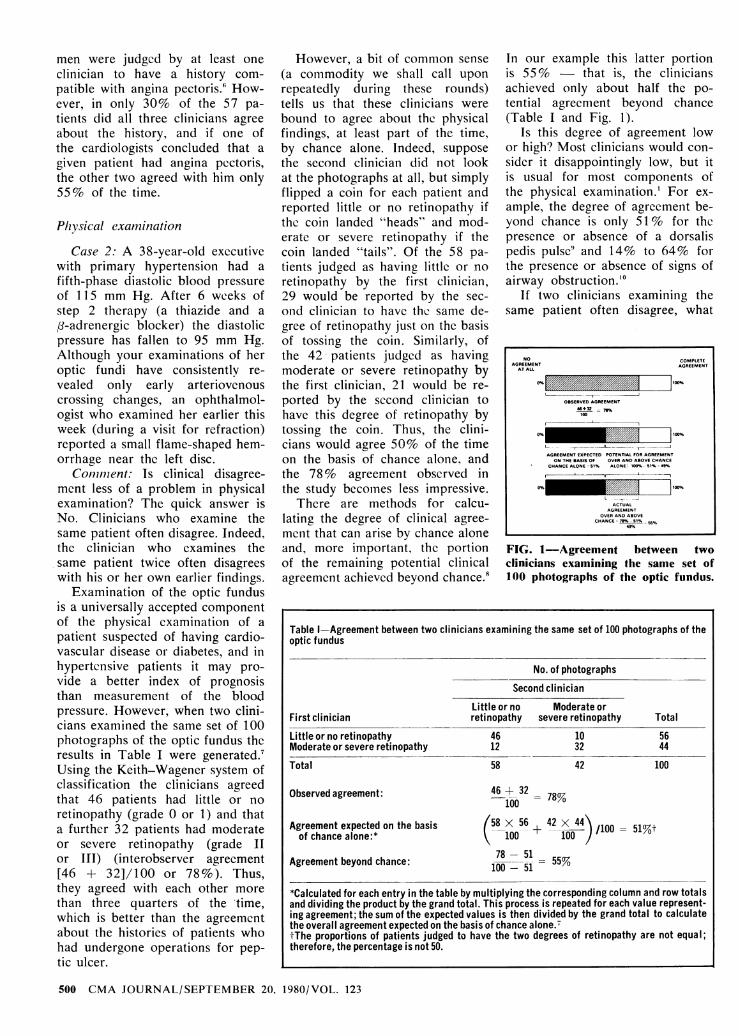
However, a bit of common sense(a commodity we shall call uponrepeatedly during these rounds)tells us that these clinicians werebound to agree about the physicalfindings, at least part of the time,by chance alone. Indeed, supposethe second clinician did not lookat the photographs at all, but simplyflipped a coin for each patient andreported little or no retinopathy ifthe coin landed "heads" and mod-erate or severe retinopathy if thecoin landed "tails". Of the 58 pa-tients judged as having little or noretinopathy by the first clinician,29 would be reported by the see-ond clinician to have the same de-gree of retinopathy just on the basisof tossing the coin. Similarly, ofthe 42 patients judged as havingmoderate or severe retinopathy bythe first clinician, 21 would be re-ported by the second clinician tohave this degree of retinopathy bytossing the coin. Thus, the clini-cians would agree 50% of the timeon the basis of chance alone1 andthe 78% agreement observed inthe study becomes less impressive.
There are methods for calcu-lating the degree of clinical agree-ment that can arise by chance aloneand, more important, the portionof the remaining potential clinicalagreement achieved beyond chance.0
In our example this latter portionis 55% - that is, the cliniciansachieved only about half the po-tential agreement beyond chance(Table I and Fig. I).
Is this degree of agreement lowor high? Most clinicians would con-sider it disappointingly low, but itis usual for most components ofthe physical examination.' For ex-ample, the degree of agreement be-yond chance is only 51 % for thepresence or absence of a dorsalispedis pulse and 14% to 64% forthe presence or absence of signs ofairway obstruction."'
If two clinicians examining thesame patient often disagree, what
NO COMPLETE
AGREEMENT AGREEMENT
10+32 ,.
FIG. i-Agreement between twoclinicians examining the same set of100 photographs of the optic hindus.
Table Agreement between two clinicians examining the same set of 100 photographs of the
optic fundus
No. of photographs
First clinician
Little or no retinopathyModerate or severe retinopathyTotal
Observed agreement:
Agreement expected on the basisof chance alone:*
Agreement beyond chance:
Second clinician
Little or no Moderate orretinopathy severe retinopathy
46 1012 3258 42
46 -1- 32100
Total
5644
100
78%
(58x 56 42x 44'\100 ± 100 .) /100
78 - 51100 - 51 55%
51%t
*Calculated for each entry in the table by multiplying the corresponding column and row totalsand dividing the product by the grand total. This process is repeated for each value represent-ing agreement; the sum of the expected values is then divided by the grand total to calculatethe overall agreement expected on the basis of chance alone.7tThe proportions of patients judged to have the two degrees of retinopathy are not equal;therefore, the percentage is not 50.
500 CMA JOURNAL/SEPTEMBER 20. 1980/VOL. 123

Table Il Agreement between two examinations of the same set of 100 photographs of theoptic fundus by one clinician
No. of photographs
Second examination
69
*Hemoglobin level 11.6 g/dl or less and serum iron level less than 12.5 ..imol/l (70 mg/dl).
rounds" of several clinicians. A re-view of their letters reveals thatsome were of the opinion that hehad osteoarthrosis requiring treat-ment with salicylates whereas othersjudged that he had possible, or evenprobable, rheumatoid arthritis de-serving a trial of gold salts.
Comment: Clinical disagreementsare most striking when a diagnosisis made primarily on clinicalgrounds. A classic example was do-cumented 35 years ago.16 Of 38911-year-old schoolchildren with in-tact tonsils who were examined bya group of physicians tonsillectomywas recommended for 174 (45%).The remaining 215 children wererecycled past a second, similargroup of physicians and tonsillec-tomy was recommended for 99(46%). The remaining 116 chil-dren, who had been given a cleanbill of tonsillar health by both thefirst and second groups of physi-cians, were then examined by a thirdgroup of physicians and tonsillec-tomy was recommended for 51(44%). Perhaps the most remark-able finding in this study was notthe inconsistency in the diagnosesand therapeutic recommendationsbut the consistency in the propor-tions of children for whom tonsil-lectomy was recommended by thedifferent groups of physicians -45%, 46% and 44%.More recently, when three clin-
ical pharmacologists evaluated 60patients whose clinicians had diag-nosed adverse reactions to medica-tions, alcohol or "recreational"drugs and therefore had admittedthem to hospital, they agreed aboutonly half the patients.'7 Further-more, in one third of the cases thepharmacologists disagreed witheach other about whether any med-ication- or alcohol-related adversereaction had occurred at all.
Finally, the increasing emphasison medical audits and '.quality as-surance" prompts an example ofclinical disagreement from this bur-geoning field. In Brook's'8 studyseasoned internists were asked toreview the records of patients withurinary tract infection, hyperten-sion, or gastric or duodenal ulcer,and to provide a peer judgementabout the quality of care they hadreceived; the extent of their agree-
ment beyond chance ranged fromonly 15% to 56% (median 27%).We suspect that the types of clin-
ical disagreement illustrated in thecases we have presented are fa-miliar to many clinicians. None theless, we have been disturbed by theextent of the disagreements and bytheir impact on patients in our care.
The etiology of clinicaldisagreement
Having presented the cases inthis clinical epidemiology round, itis now appropriate for us to turnour attention to the etiology of clin-ical disagreement as a basis for pro-posing clinical maneuvers for itsprevention or minimization. Etio-logic factors are prcsented underthree headings: the examiner, theexamined and the examination(Table IV).
The examiner
Biologic variation in the senses:Clinical examination begins withthe senses - sight, hearing andtouch. Variations in the acuity andappreciation of the senses (e.g.,colour-blindness. presbyopia andpresbycusis) will inevitably lead toclinical disagreement between clin-icians. Less widely acknowledged isthe factor responsible for inconsist-encies in the results of examinationsperformed by the same clinician -biologic variation in the examiner ssenses. This has been shown best instudies contrasting how physiciansperform when rested and whentired. In one study the ability ofinterns to detect simple cardiac ar-rhythmias on an electrocardiogram
rhythm strip deteriorated markedlyfollowing a busy night on call(mean sleep duration 1.8 h), andwas accompanied by a substantialdecline in perception, cognition andmood.19
The tendency to record inferencerather than evidence: This causeof clinical disagreement has beendiscussed in detail by Feinstein.20'21Patients' descriptions of their symp-toms, and the appearance, soundand feel of physical findings enterthe clinician's consciousness assensory evidence. Because the diag-nostic process translates and syn-thesizes such evidence into infer-ence it is understandable that infer-ence tends to serve as the mediumof exchange between clinicians andin medical records. We tend tospeak of "pleuritic" rather than "in-spiratory" chest pain and of "ane-mic" rather than "pale" skin. Indoing so, however, we run the riskof increasing diagnostic error: al-though clinicians usually agreeabout sensory evidence they oftendisagree about the inference to bedrawn from it.
Confining the clinical record toinferences has another importantdrawback - an incorrect inferencemay misdirect the diagnostic pro-cess. Suppose a patient presentswith a "motionless" limb and "thin"muscles resulting from an old anky-losing joint injury that led to thedisuse of the associated musclegroups. To describe the limb as"paralyzed" may direct the subse-quent diagnostic process on asearch through the nervous system,which, when ultimately fruitless,may fail to return the clinician tothe appropriate starting point wherethe initial error occurred.
Ensnarement by diagnostic clas-sitication schemes: Current diag-nostic classification schemes can in-crease the risk of clinical disagree-ment in two ways. First, they oftenprovide arbitrary, hazy and fre-quently inconsistent "break-points"in a smooth and continuous distri-bution of an attribute such as bloodpressure, body mass or glucose tol-erance. As a result, we engage infruitless arguments over whether apatient is "really" hypertensive,obese or diabetic. The related issuesof normal values and ranges have
Table IV Etiology of clinical disagreement
The examinerBiologic variation in the sensesThe tendency to record inference ratherthan evidence
Ensnarement by diagnostic classificationschemes
Entrapment by prior expectationThe examined
Biologic variation in the system beingexamined
Effects of illness and medicationsMemory and rumination
The examinationDisruptive environments for the examin-
ationDisruptive interactions between exam-
iners and examinedIncorrect function or use of diagnostictools

been discussed elsewhere.22Second, clinical disagreement
arises when different diagnostic cri-teria are applied to the same clin-ical entity by different professionals.For example, unanimous agreementamong emergency room clinicians,"preventive" cardiologists, electro-cardiographers, and clinical andanatomic pathologists that a patienthad suffered a heart attack wouldrequire the simultaneous occurrenceof specific signs and symptoms, thedocumentation of increased riskfactors, specific electrophysiologicchanges on the electrocardiogram,the excceding of critical levels ofcardiac enzymes in the peripheralblood, and specific gross and mi-croscopic anatomic features. Theanalogy to the argument among theblind men over the essence of anelephant comes to mind, but in ourdiagnostic situation we are dealingwith the beast's footprints and ef-fluvia as well.
Entrapment by prior expectation:We tend to find what we expect orhope to find. The power and con-sistency of this cause for observererror were well demonstrated in thetonsillectomy study described ear-lier.'6 That expectation still influ-ences clinical diagnosis is evidentin the electronic age. For example,in a more recent study fetal heartrates determined from auscultationby house officers were comparedwith those computed from simul-taneous fetal electrocardiographicmonitoring.2' The house officersand the monitors agreed whenthe fetal heart rates were "normal"(130 to 150 beats/mi. However,when the electrocardiogram showedfetal heart rates above 150 or below130 beats/mm the house officersconsistently lowered or raised theirestimates so they would be closerto the "normal" values.
The examined
Biologic variation in the systembeing examined: Most cliniciansrecognize that clinical attributessuch as height, weight, blood pres-sure and pulse will vary from hourto hour and from day to day de-pending on such factors as position,diet, fluid intake, stress and exer-cise. Furthermore, we usually knowthat if the blood pressure is sur-
prisingly high or low one day, itwill tend to return to a more usuallevel the next week (this phenom-enon of regression toward the meanhas been discussed elsewhere").However, what we may overlook isthat this biologic variation is alsothe rule for many "exact" measure-ments, including electrocardio-grams, left ventricular end-diastolicpressures and ejection fractions.'4"5It follows that such variation willlead to inconsistencies in the clin-ical descriptions of patients and,when the variation crosses a criticalboundary, in diagnoses.
Effects of illness and medica-tions: This cause of inconsistencyand inaccuracy arises when the dis-ease or the agents administered inits treatment affect the patient'sability to provide a cogent and ac-curate history or alter the physicalor laboratory indices of the disease.For example, in many hypertensivepatients the blood pressure returnsto normal following a myocardialinfarction; also, angina pectorismay disappear. Similarly, analgesicsmay mask the physical signs andcloud the recall of patients withacute intra-abdominal disorders.Memory and rumination: Pa-
tients, especially those with chronicor serious illnesses, often ruminateover past events in search of acogent cause for their troubles.Repeated history-taking reinforcesrumination and reorganizes scat-tered memories into orderly pat-terns of recalled events. Thus, re-peated histories may exhibit sub-stantial change and evolution, re-sulting in equally substantial incon-sistencies in the occurrence or tim-ing of important prior healthevents (and not inconsiderableconsternation during professorialrounds).
The examination
Disruptive environments for theexamination: The environment inwhich the examination is carriedout can affect both senses andsensibilities. Attempts at cardiacauscultation on jetliners are futile,and the noise levels in some emer-gency rooms effectively swamp allbut the loudest Korotkoff sounds.Artificial or dim lighting can renderthe detection of jaundice or cya-
nosis impossible. A shivering pa-tient in a cold examining room willwelcome neither a prolonged clin-ical interview nor the cold steel ofdiagnostic instruments. Privacy maybe a prerequisite for the disclosureof information about the family(e.g., epilepsy, consanguinity or insanity), the operative history (e.g.,an illegal abortion) or exposure tovenereal disease.
Disruptive interactions betweenexaminers and examined: Althougheffective communication betweenclinicians and patients is widely ac-knowledged as a prerequisite forappropriate management in bothbehaviourally" and biologicallyoriented'7 clinical journals, the ef-fect of faulty communication onclinical disagreement has not oftenbeen quantified. A study of a ran-dom sample of 155 patient inter-views conducted in a private familydoctor's practice revealed that onefifth of the interviews failed to un-earth important features, such asmelena or urinary frequency, inthe history of the patient's presentillness or in the past history.'8 Sur-prisingly, the investigators foundthat such lapses were greatest notwhen patients were at odds withtheir physicians but when theylavished their physicians with "ex-cessive" praise. Furthermore, pa-tients from different ethnic back-grounds are known to focus theirsymptoms onto different body sites;the failure of clinicians to recog-nize this and the "social distance"between them and their patientshas been offered as one explana-tion for the wide variations in theincidence of nonorganic diagnosesreported among different ethnicgroups living in identical physical,social and economic environments."
The effects of apprehension onthe acquisition of clinical informa-tion in an unfamiliar setting can besubstantial, as any clinician knowswho has attempted to soothe afrightened patient labelled hyper-tensive in a shopping plaza screen-ing program. Similarly, painful ex-aminations, such as palpation of atender abdominal mass, may alteror obscure important clinical find-ings.
Incorrect function or use of diag-nostic tools: A mercury manometer
CMA JOURNAL/SEPTEMBER 20. 1980/VOL. 123 503

with a low reservoir or a defectiveaneroid manometer with a hiddenpin-stop can give falsely low bloodpressure readings. Indeed, 40(13%) of 310 aneroid manometersexamined in seven hospitals in Mi-chigan were shown to produce er-rors of 7 mm Hg or more whenthe measurements were comparedwith those of a mercury mano-meter.30 An inappropriate cuff widthor the too-rapid deflation of a cuffcan also lead to systematic er-rors; some individuals have beenshown to choose certain terminalnumbers (digits 8, 0 or 2) overothers (digits 4 or 6) when report-ing blood pressure measurements.3'Similar faults have been identifiedin the manufacture, maintenanceand use of other diagnostic tools.
Conclusion
This round has identified a num-ber of causes of clinical disagree-ment in the history and physicalexamination, in the interpretationof the results of diagnostic testsand in the act of diagnosis itself.On the basis of these causes, a setof clinical strategies has been de-veloped for preventing or at leastreducing clinical disagreement. Thenext round in this series will pre-sent these strategies and a set oftactics that clinicians can use todetermine and to improve the ac-curacy and precision of their clin-ical measurements and decisions.
We thank our students, housestaffand colleagues for their encourage-ment and criticism, and Drs. E.J.M.Campbell. AR. Feinstein, F.J. Ingel-finger, W.M. Goldberg and W.B.Spaulding for reviewing earlier ver-sions of this manuscript.
References
I. KORAN LM: The reliability of clin-ical methods, data and judgments[two parts]. N Engi I Mcd 293: 642,695; 1975
2. HIPPOCRATES: Epidemics, hook I,section 11 of The Genuine Works ofHippocram'cs, ADAMS F (trans), Wil-liams & Wilkins, Baltimore, 1939,p 104
3. 1-LAYNES RB, SACKEIT DL, TAYLORDW, et al: Increased absenteeismfrom work after detection and la-beling of hypertensive patients. NEngi I Mcd 299: 741, 1978
4. BERGMAN AB, STAMM SJ: The mor-bidity of cardiac nondisease inschoolchildren. N Engi I Med 276:1008, 1967
5. HALL R, HORROCKS IC, CLAMP SE,et al: Observer variation in assess-ment of resLIlts of surgery for pepticLllceration. Br Med 1 1: 814, 1976
6. ROSE GA: Jschemic heart disease.Chest pain qLlestionnaire. Mi/bankMciii Fund Q 43: 32, 1965
7. AoKI N, HORIBE H, OFINO Y, et al:Epidemiological evaluation of fun-dLlscopic findings in cerebrovasculardiseases. III. Observer variability andreproducibility for fundiiscopic find-ings. Jpn Circ 1 41: 11, 1977
8. LIGHT RI: Measures of responseagreement for qualitative data: somegeneralizations and alternatives. Psy'-c/wi Bull 76: 365, 1971
9. MEADE 1W, GARDNER N4J, CANNONP, et al: Observer variability in re-cording the peripheral pulses. BrHeart 1 30: 661. 1968
10. GODFREY S. EDWARDS RH, CAMP-BELL El, et al: Repeatability of phy-sical signs in airways obstruction.ihorax 24: 4, 1969
11. CHAMBERLAIN I, GINKS 5, ROGERSP. et al: Validity of clinical exam-ination and mammography asscreening tests for breast cancer.Lancel 2: 1026, 1975
12. BL\CKBURN H, I3LOMGvIsT G, FREI-MAN A, et al: The exercise electro-cardiogram: differences in interpre-tation. Report of a technical groupon exercise electrocardiography. A inI Cardiol 21: 871. 1968
13. FAIRBANKS VE: Is the peripheralblood film reliable for the diagnosisof iron deficiency anemia? Am ICliii Padiol 55: 447, 1971
14. DEIRE KM, WRIGHT E, MURPHYML, et al: Observer agreement inevalLlating coronary angiograms. Ci,-culation 52: 979, 1975
15. Zi. LM, MILLER SW, DINsMoRERE, et al: Interobserver variabilityin coronary angiography. Circula-lion 53: 627. 1976
16. BAKWIN H: Pseudodoxia pediatrics.N Engi I Med 232: 691, 1945
17. KARCH FE, SMITH CL. KERZNER B,et al: Adverse drug reactions - amatter of opinion. Cliii PharinacolTlier 19: 489, 1976
18. BROOK RH: Quality of Care Assess-inent; a Coin parison of Fire Meth-od. of Peer Review (DHEW publno HRA-74-3100), US Health Re-sources Administration, Bureau ofHealth Services Research and Evalu-ation, Rockville, Md, 1973
19. FRIEDMAN RC, BIGGER IT, KORN-FELD DS: The intern and sleeploss. N Engi 1 Med 285: 201, 1971
20. FEINSTEIN AR: Scientific method-ology in clinical medicine. IV. Ac-qLlisition of clinical data. Ann internMed 61: 1162, 1964
2 Idenv Clinical Ji.di..,nen, XVilliams& Wilkins, Baltimore, 1967, p 4.f
22. SACKETT DL: Clinical diagnosis andthe clinical laboratory. Cliii InvestMed 1: 37, 1978
23. DAY E, MADDERN L, WooD C: Atis-cultation of foetal heart rate: anassessment of its error and signif-icance. Br Med 1 4: 422, 1968
24. SPODICK DH: On experts and ex-pertise: the effect of variability inobserver performance. Am I Cardiol36: 592, 1975
25. MCANULTY JI-I, KREMKAU EL,ROSCH I: Spontaneous changes inleft ventricular function between se-quential studies. Am I Cardiol 34:23, 1974
26. HOORNAERT F. PIERLOOT R: Trans-ference aspects of doctor-patient re-lationship in psychomatic patients.I. Br I Vied Psvchol 49: 261, 1976
27. KIRscH'r JP: Communication be-tween patients and physicians (E).Ann Inter,i Med 86: 499, 1977
28. SNYDER D, LYNCH JJ, Giuss L:Doctor-patient communications in aprivate practice. I Fain Praci 3: 271,1976
29. ZoI.\ 1K: Pathways to the doctor- from person to patient. Soc SciMed 7: 677, 1973
30. PERLMAN LV, CHIANG BN, KELLERJ, et al: Accuracy of sphygmoma-nometers in hospital practice. ArchIntern Med 125: 1000, 1970
31. KANTOR 5, WINKELSTEIN W JR,SACKETT DL, et al: A method forclassifying blood pressLire: an em-pirical approach to the redLiction ofmisclassification due to response in-stability. Am J Epideiniol 84: 510,1966
I BOOKS Icontinued from page 488
ANTIMICROBIAL PROPHYLAXIS INSURGERY. M.R.B. Keighley and D.W.Burdon. 241 pp. lIlust. Pitman MedicalPublishing Co. Ltd., Tunbridge Wells,Kent, 1979. Price not stated. ISBN0-272-79522-4
ANTIMICROBIAL THERAPY. 3rd ed.Benjamin M. Kagan. 542 pp. lIlust. W.B.Saunders Company Canada, Ltd., Tor-onto, 1980. $42. ISBN 0-7216-5234-4
AN AUTHOR'S GUIDE TO THE COPY-RIGHT LAW. Warren L. Patton. 192 pp.II lust. Lexington Books, Lexington,Massachusetts; D.C. Heath CanadaLtd., Toronto, 1980. S23.95. ISBN 0-669-O0740.4
BASIC ATLAS OF CROSS-SECTIONALANATOMY. Walter J. Bo, IsadoreMeschan and Wayne A. Krueger. 357pp. lIlust. W.B. Saunders CompanyCanada, Ltd., Toronto, 1980. $49.20.ISBN 0-7216-1767-0
continued on page 536
504 CMA JOURNAL/SEPTENIBER 20, 1980/VOL. 123