hypoadrenalism feb 2015
TRANSCRIPT

Hypoadrenalism – Case Presentation Dr. Adam Stokes
ST4 in Anaesthesia & ICM
24th February 2015

Overview
1. Case Presentation
2. Adrenal Physiology
3. Hypoadrenalism 1. Causes
2. Clinical Features
3. Diagnosis
4. Treatment

Case Presentation - Background ! 40 year old man
! PMH: Subclinical hypothyroidism (2008) – not on replacement
! Admission Sept 2014 with right flank pain, no cause found
! DH: Nil regular, NKDA.
! SH: Non-smoker, occasional alcohol, worked up until last 2 weeks, living with parents.

Case Presentation ! Presentation
! 1/12 Hx of lethargy, weakness, muscular spasms
! 1/52 Hx of nausea and vomiting, hiccups
! 2-3/7 Hx of repeated vomiting, occasionally blood tinged, patient reports feeling “slow”
! Saw GP 2/7 ago- plan for bloods and f/u, but parents concerned and rang 111, who advised 999.

Case Presentation ! Assessment on admission
! Resp: RR 18, Sats 100% on air
! CVS: HR 80, BP 130/73, paramedics reported no postural drop.
! Neuro: GCS 14/15, mild confusion/slowness in speech, PERLA, BM 4.9, afebrile.
! GI: Abdo soft non-tender, BS active
! Tanned skin, but not obviously pigmented mucous membranes.

Case Presentation ! Initial results/management in ED
! Lab- Na<100, K 5.7, Cl 67, Ur 6.1, Cr 74 CRP 36, Hb 17.5 WCC 4.1, Plt 166
! CXR: NAD ! ECG: NAD ! ABG: pH 7.44, pCO2 3, pO2 10.6, Lac 0.7, BE -8.6, Na
<100, Cl 69 ! Random cortisol and TFTs sent ! Treatment:
! Metoclopramide ! Lansoprazole ! Saline 1000ml (commenced prior to Na result) ! Hydrocortisone 100mg

Case Presentation ! Next 24 hours in HDU
! Arterial line inserted for frequent ABGs
! Urine and plasma osmolalities sent, urinary Na
! Results: TFTs - T4 14.5 (N), TSH 29.7 (high), plasma osmolality 212, urine 836, urine Na 71, random cortisol 110
! Slow Na correction with 1.8% NaCl
! CT head: Thrombosed cerebral artery aneurysm in circle of Willis (?significance), nil else

Case Presentation ! Day 3
! Short synacthin test performed: 30min cortisol 290, 60min 275: positive test for primary hypoadrenalism
! Levothyroxine commenced, and after results of synacthin test, fludrocortisone/hydrocortisone replacement started
! Patient became more agitated/confused (required DOLS)
! Renin/Aldosterone/ACTH and autoantibody screen sent.

Case Presentation ! Days 4 -10
! Gradual improvement in mental condition and weakness with Na up to 130
! CT head discussed with Neuro SGH- probably incidental but will f/u in due course
! Discharged with f/u in Endo clinic in 2/52
! Results: ! ACTH high. ! Renin high. ! Aldosterone normal. ! Thyroid autoantibodies positive. ! Adrenal autoantibodies weakly positive.

Adrenal Physiology
Hypothalamus Pituitary
Adrenal Cortex
(Glomerulosa)
Adrenal Cortex
(Fasiculata)
Adrenal Cortex
(Reticularis)
ACTRH
ACTH
Trauma Temp Hypoglycaemia Exercise Stress

Adrenal Physiology
Zona glomerulosa Aldosterone
Na+ & water retention.
K+ secretion.
Zona fasiculata Cortisol and corticosterone
Gluconeogenesis
Proteolysis
Lipolysis
RBCs, plts, neuts.
Gastric acid & ulcers.
Reactivity to catecholeamines.
Reduced collagen & osteoporosis.
Anti-inflammatory.
Immunosuppression. Zona reticularis
Androgens (& small amount of
cortisol)
ACTH K+ RAAS

Hypoadrenalism ! Causes
! Clinical features
! Diagnosis
! Treatment
Causes
! Secondary
! Mass lesions – pituitary adenomas
! Pituitary surgery / radiation
! Isolated ACTH deficiency (autoimmune or genetic)
! Infiltrative lesions
! Infarction (Sheehans)
! TBI
! Tertiary ! Chronic high dose
glucocorticoid therapy ! Mass lesions ! Radiation ! Infiltrative lesions – e.g.
sarcoidosis ! TBI ! Infections
! Primary Adrenal Insufficiency
! Idiopathic / Autoimmune
! Infectious adrenalitis
! Bilateral adrenal infarct
! Metastatic disease
! Drugs

Clinical Features ! Depends on rate & extent of loss of adrenal
function, whether mineralocorticoid production is preserved and degree of stress. ! Adrenal crisis
! Chronic primary adrenal insufficiency
! Secondary or tertiary adrenal insufficiency

Clinical Features ! Adrenal Crisis
! Occurs in:
! Undiagnosed primary adrenal insufficiency subject to serious infection/stress.
! Known primary adrenal insufficiency who does not take sufficient glucocorticoid during infection/stress.
! Bilateral adrenal infarct/haemorrhage.
! Less frequently with secondary/tertiary adrenal insufficiency.
! Abrupt withdrawal of glucocorticoid therapy.
Clinical Features ! Adrenal Crisis:
! Features: ! Shock (predominant feature) ! Anorexia, N&V, weight loss. ! Weakness, fatigue, lethargy, confusion, coma. ! Abdo pain. ! Hypoglycaemia. ! Fever. ! Hyponatraemia, hyperkalaemia, hypercalcaemia,
eosinophilia. ! Hyperpigmentation or vitiligo. ! Autoimmune endocrine deficiencies e.g. hypothyroid

Clinical Features ! Chronic Primary Adrenal Insufficiency
! May have features of glucocorticoid, mineralocorticoid and androgen deficiency.
! Insidious onset
! Non-specific features.
! Difficult to diagnose.
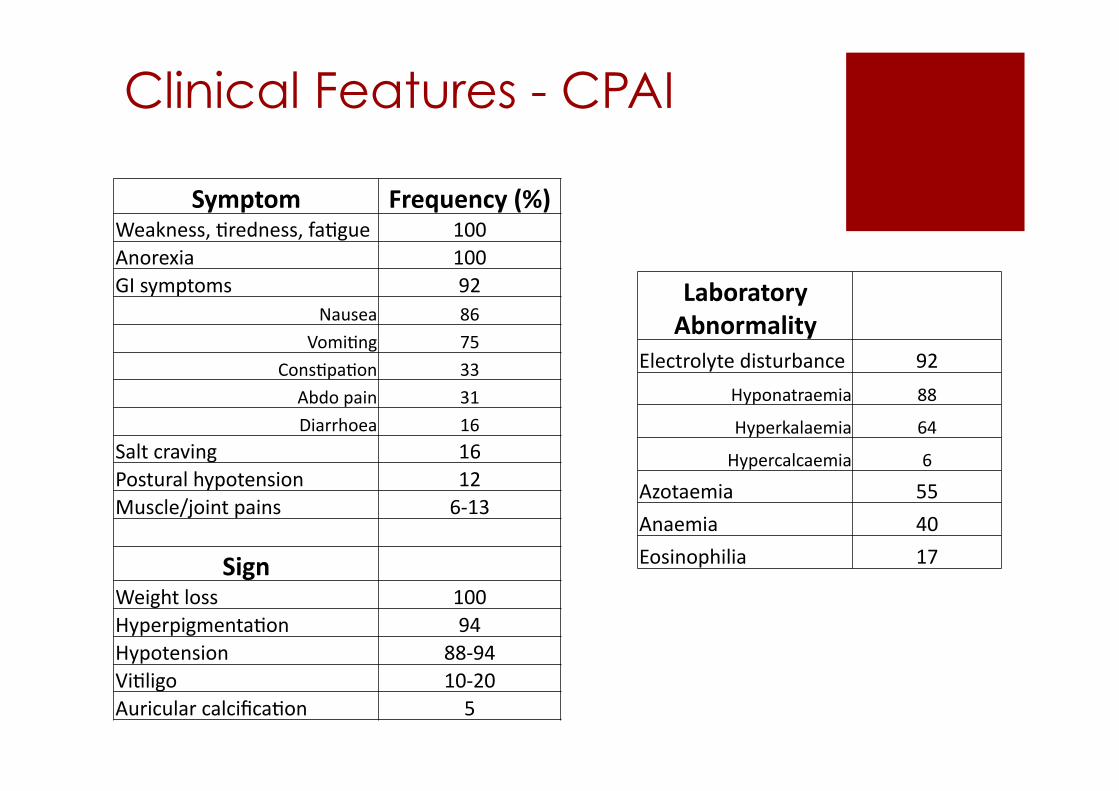
Clinical Features - CPAI
Symptom Frequency (%) Weakness, )redness, fa)gue 100 Anorexia 100 GI symptoms 92
Nausea 86
Vomi)ng 75
Cons)pa)on 33
Abdo pain 31
Diarrhoea 16 Salt craving 16 Postural hypotension 12 Muscle/joint pains 6-‐13
Sign Weight loss 100 Hyperpigmenta)on 94 Hypotension 88-‐94 Vi)ligo 10-‐20 Auricular calcifica)on 5
Laboratory Abnormality
Electrolyte disturbance 92
Hyponatraemia 88
Hyperkalaemia 64
Hypercalcaemia 6
Azotaemia 55
Anaemia 40
Eosinophilia 17

Clinical Features ! Secondary or Tertiary Adrenal Insufficiency
! Similar to chronic primary adrenal insufficiency with the following exceptions:
! Hyperpigmentation not present as ACTH not increased.
! Dehydration not present, and less hypotension.
! Hyperkalaemia not present, reflecting presence of aldosterone.
! Less GI symptoms.
! Hypoglycaemia more common.
! Manifestations of pituitary/hypothalamic tumour.

Diagnosis ! Three stage process:
1. Demonstrating inappropriately low cortisol
2. Determine if cortisol deficiency is independent/dependent of ACTH deficiency + evaluation of mineralocorticoid secretion in pts without ACTH deficiency.
3. Seeking treatable cause of the primary disorder.

Diagnosis – Low Cortisol ! Serum cortisol conc
! Morning serum cortisol conc ! Low is strongly suggestive of adrenal insufficiency
! Morning salivary cortisol conc ! For screening
! Afternoon/night serum cortisol ! No value
! Urinary cortisol ! Low in adrenal insufficiency, but can be low-normal in partial
insufficiency. Thus, unsuitable for screening.
! Short ACTH stimulation test

Diagnosis – Level of defect ! Need to measure basal plasma ACTH, renin and
aldosterone conc. ! If primary, ACTH high. Will have high renin, low
aldosterone, raised K+ and decreased Na+.
! If secondary/tertiary, ACTH low. Renin and aldosterone usually unaffected.
! Prolonged ACTH test will help distinguish between primary and secondary/tertiary.
! Differentiation between secondary and tertiary by ACTRH – although not really important.

Diagnosis - Aetiology ! Pituitary CT or MRI.
! Abdominal CT.
! CXR, urine culture for TB.
! CT directed percutaneous fine needle aspiration of enlarged adrenal glands.

Treatment – Adrenal Crisis ! Emergency Measures
! Large IV access ! Bloods – U&E, glucose, cortisol, ACTH. ! Saline 2000 – 3000ml ! Dexamethasone 4mg IV BD (does not affect cortisol measurement)
or hydrocortisone 100mg QDS. ! Supportive measures
! Subacute Measures ! Continue saline for 24 – 48 hours ! Treat precipitants ! Perform short ACTH stimulation test ! Determine type of insufficiency. ! Taper glucocorticoids over 1-3 days ! Begin mineralocorticoid replacement with fludrocortisone.
Treatment – Chronic Adrenal Insufficiency ! Glucocorticoid Replacement
! Dexamethasone 0.25-0.75mg or prednisolone 2.5-7.5mg PO, supplemented with hydrocortisone 5-10mg in afternoon PRN.
! Alternatively, hydrocortisone 15-20mg OM & 5-10mg in afternoon.
! Monitor ACTH.
! Mineralocorticoid Replacement ! Fludrocortisone 0.05 – 0.2mg PO. ! Liberal salt intake. ! Monitor postural BPs, HR, oedema, K+, and renin.
! Androgen Replacement ! Dehydroepiandrosterone 25-50mg PO in women.
! Other ! Patient education ! Medic–alert bracelet

Thank you!