hta and clinical practice guidelines as tools for ... · health technology assessment to guide...
TRANSCRIPT

1
HTA and clinical practice guidelines as tools for knowledge translation
Health technology assessment to guide clinical practice
8th Guideline International Network Conference
29 August 2011
Dr Mabel Yap
Director (Health Services Research & Evaluation)
Ministry of Health, Singapore
Guidelines International Network
Conference 2011 “Linking Evidence, Policy, and Practice
Focus of presentation
Use of HTA/CPG methodology in
development of Integrated Care Pathways
(ICP) in Singapore

2

3
Our Healthcare System
Ministry of Health Singapore
To ensure access to good and
affordable healthcare that is
appropriate to needs
To promote good health and
reduce illness
To pursue medical excellence
Championing a healthy
nation with our people
-- to live long,
live well &
with peace of mind
Our Vision Our Mission
4
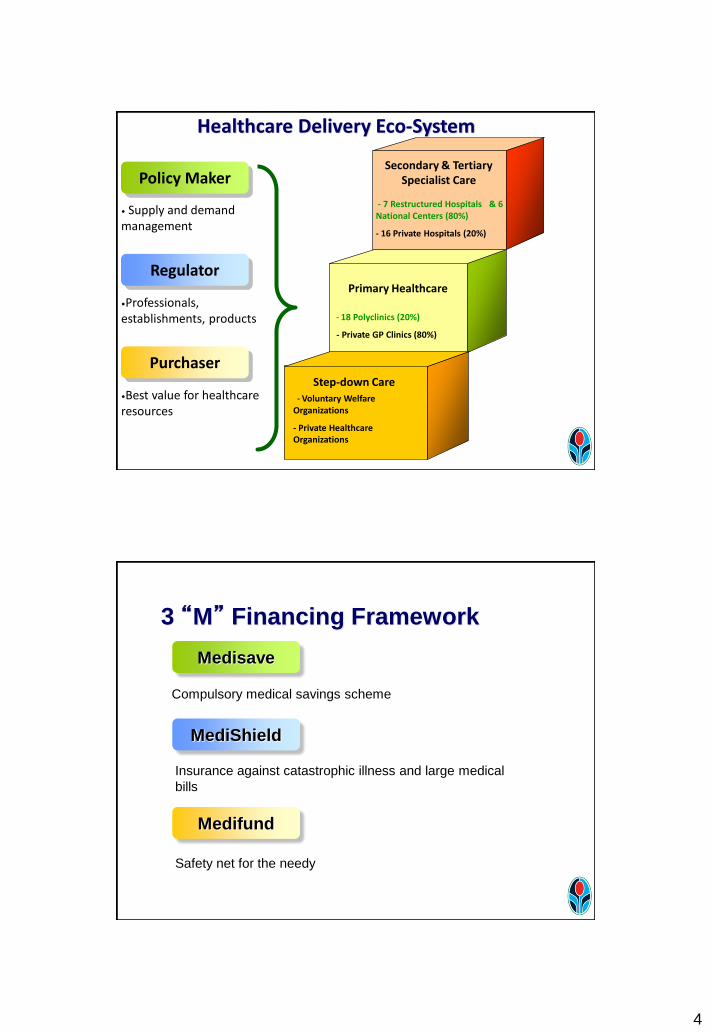
Primary Healthcare
- 18 Polyclinics (20%)
- Private GP Clinics (80%)
Step-down Care
- Voluntary Welfare Organizations
- Private Healthcare Organizations
Healthcare Delivery Eco-System
Secondary & Tertiary Specialist Care
- 7 Restructured Hospitals & 6 National Centers (80%)
- 16 Private Hospitals (20%)
• Supply and demand management
•Professionals, establishments, products
•Best value for healthcare resources
Policy Maker
Regulator
Purchaser
Compulsory medical savings scheme
Insurance against catastrophic illness and large medical
bills
Safety net for the needy
Medisave
MediShield
Medifund
3 “M” Financing Framework

5
Compulsory savings scheme Singapore is the first country to implement medical savings account on a nationwide basis in 1984
Prior to Medisave, medical services were financed through general taxation. However, rapid healthcare cost inflation in the 1970s and evidence of ever-increasing demand for health services in developed countries showed that this was unsustainable
7% ~ 9.5% of monthly salary goes to Medisave Account
9 of 10 Singaporeans admitted to hospitals use Medisave to pay their bills
Medisave
Medisave is primarily for hospitalisation
expenses, but also covers step-down care and
certain expensive outpatient expenses
The Ministry has extended the use of Medisave
to co-pay costs of chronic disease management
programmes (CDMP) at outpatient settings, for
diabetes, hypertension, lipid disorder, stroke,
asthma, COPD, schizophrenia, major
depression .
Medisave

6
Medishield Catastrophic medical insurance scheme
Protects against the very large hospital bills that Medisave may
not be sufficient to cover
Reduces the need to over-save for catastrophic (low-probability,
but high-cost) events
Opt-out scheme to encourage participation; lower
administrative and enforcement costs
More than 90% of working population subscribes to MediShield
and private Shield plans
Covers hospitalisation expenses and expensive
outpatient treatment (e.g. kidney dialysis, chemotherapy,
radiotherapy)
Endowment fund of $1.7 billion in 2009; target to
increase to $2 billion
Interest income used to help needy Singaporeans pay
for their medical expenses
Safety net for Singaporeans who cannot afford medical
expenses, even after government subsidy, Medisave
and MediShield
Ensures no Singaporean is denied access to basic
medical care because of inability to pay
Medifund
7
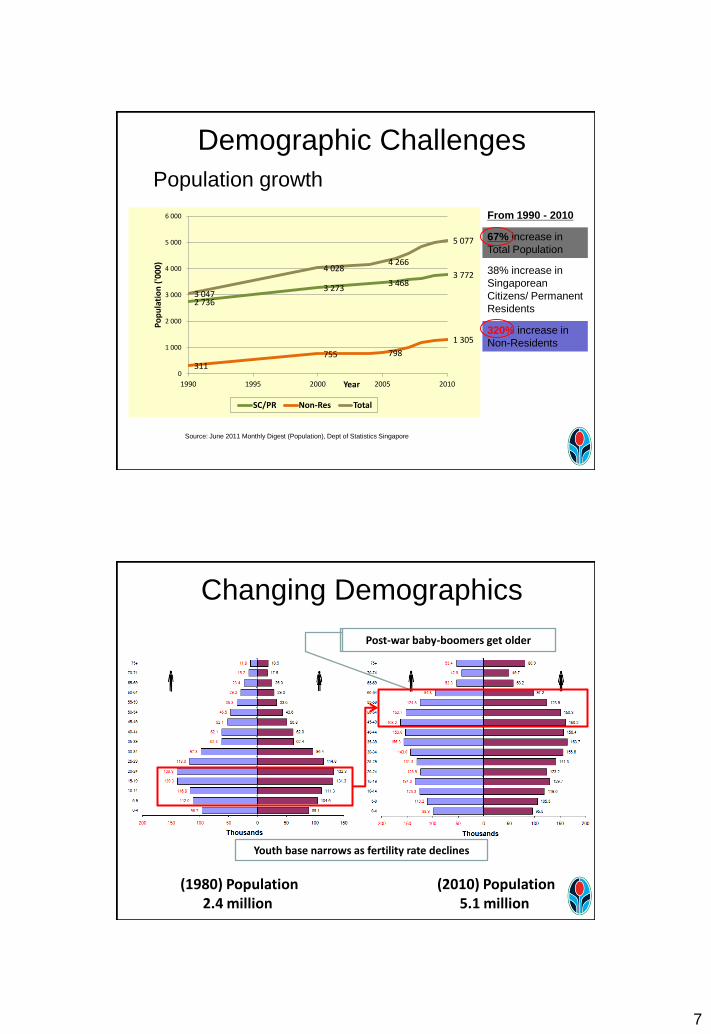
Population growth
Demographic Challenges
2 736
3 273 3 468
3 772
311
755 798
1 305
3 047
4 028 4 266
5 077
0
1 000
2 000
3 000
4 000
5 000
6 000
1990 1995 2000 2005 2010
Po
pu
lati
on
('0
00
)
Year
SC/PR Non-Res Total
38% increase in
Singaporean
Citizens/ Permanent
Residents
67% increase in
Total Population
From 1990 - 2010
320% increase in
Non-Residents
Source: June 2011 Monthly Digest (Population), Dept of Statistics Singapore
Changing Demographics
(1980) Population 2.4 million
(2010) Population 5.1 million
Post-war baby-boomers get older
Youth base narrows as fertility rate declines

8
Shift in Disease Burden : From Mortality to Morbidity
Diabetes Mellitus
Mental Disorders
Neurological, vision & hearing
disorders
Cardiovascular diseases
Cancers
Others Total
Cardiovascular
Cancers
Diabetes
Neurological, vision & hearing
Mental
BURDEN OF DISEASE BY BROAD CAUSE GROUP SINGAPORE (2007)
YLL YLD
Top 5 Diseases by DALYs
Neurological, vision & hearing disorders, Mental disorders, and Diabetes – make up 35% of BoD
> 50% of total Disability-Adjusted Life-Years (DALYs) due to living with ill health or disability (YLD)
Need for Integration of Care
Rehab
CentresFamily
Physician
Polyclinic
Palliative
Care
Screening
&
Prevention
Nursing
Homes
Community
Hospital
Restructured
Hospital
Home
Episodic Care
Silos
SYSTEMS
Prevention and Early Diagnosis
Primary Care Secondary/
Tertiary Care (Outpatient)
Secondary/ Tertiary Care (Inpatient)
Step Down Care
End-of-Life Care

9
Rehab Centres
Family Physician
Polyclinic
Palliative Care
Screening & Prevention
Nursing Homes
Community Hospital
Restructured Hospital
Home
Integration- Provider to provider journey
Integrate Public, Private and People sector
Centred around the
patient
2a. Right-site rehab and
subacute care in
Community Hospitals to
reduce stay in RHs
5. Day rehab &
care services
INTERMEDIATE CARE LONG-TERM CARE
6. Community
nursing services
7. Caregiver
training
PRIMARY CARE
12. “One Family
Physician for
Every
Singaporean”
1. Aged Care
Assessment
Services to triage
elderly patients and
develop discharge
plan
4. Comprehensive Care
Needs Assessment to
recommend services
needed to maintain
elderly at home 3. Transitional Post-
Acute Home Care to
reduce stay in RH and
enable early
discharge to home
11. Integrated
Screening and
Prevention Programme
8. Fall
prevention
9. Care Coordination
and Case Management
Home
10. Information and
Referral
Integrated Clinical Pathways
National Electronic Health Records
2b. Patients with
serious acute
conditions
escalated to AMCs
13. Primary Care Networks and
Disease Management Units
DEVELOPING NEW SERVICES

10
5 Integrated Care Pathways
20
Stroke
Diabetes
Acute Heart
Syndrome
Hip Fracture
Chronic Obstructive
Lung Disease
Rehab
Implementation RHS Team #1
1.RHS Dr, Nurses, AHP 2.AIC Rep 3.MOH Rep
Implementation Teams (Customised to each Regional Health System)
etc
Clinical Team (National) (Development of care elements)
Each ICP workgroup consists of :
Implementation RHS Team #2
1.RHS Dr, Nurses, AHP 2.AIC Rep 3.MOH Rep
Implementation RHS Team #3
1.RHS Dr, Nurses, AHP 2.AIC Rep 3.MOH Rep
Integrated Care Pathways Project
Role of HTA
• To provide the evidence-base for safe and effective
interventions for various care pathways
Deliverables:
a. Develop framework for integrated care pathways
b. Prioritise interventions for inclusion in ICP
c. Identify gaps where more research can be done
11
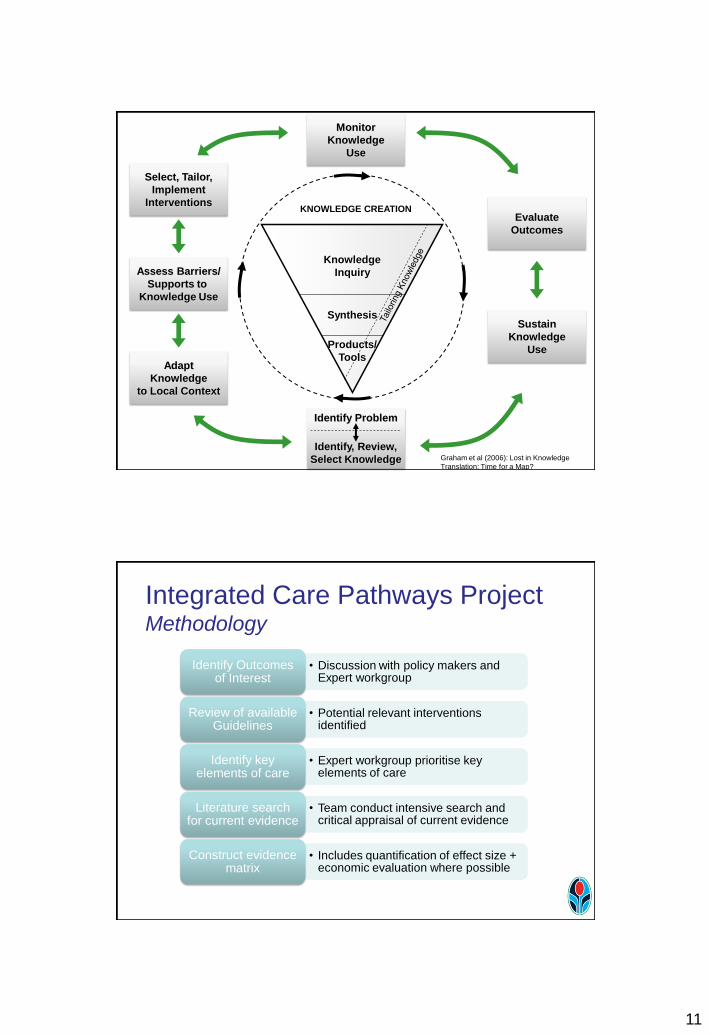
Identify Problem
Identify, Review,
Select Knowledge
Monitor
Knowledge
Use
Sustain
Knowledge
Use
Evaluate
Outcomes
Adapt
Knowledge
to Local Context
Assess Barriers/
Supports to
Knowledge Use
Select, Tailor,
Implement
Interventions
Products/
Tools
Synthesis
Knowledge
Inquiry
KNOWLEDGE CREATION
Graham et al (2006): Lost in Knowledge
Translation: Time for a Map?
Integrated Care Pathways Project Methodology
• Discussion with policy makers and Expert workgroup
Identify Outcomes of Interest
• Potential relevant interventions identified
Review of available Guidelines
• Expert workgroup prioritise key elements of care
Identify key elements of care
• Team conduct intensive search and critical appraisal of current evidence
Literature search for current evidence
• Includes quantification of effect size + economic evaluation where possible
Construct evidence matrix

12
CASE STUDY Integrated Care Pathways for Stroke
8 outcomes identified
1. Mortality 2. Symptom-to-Needle Time 3. Recurrent Vascular Events 4. Length of Stay 5. Functional Outcome 6. Complications 7. Depression 8. Stroke Misdiagnosis
• Discussion with policy makers and Expert workgroup on outcomes of interest for management of Acute Stroke
Identify Outcomes of
Interest

13
Searched for and reviewed clinical practice guidelines to identify expert consensus on interventions Clinical practice guidelines appraised with AGREE instrument: 12 guidelines considered to be “recommended”
• Potential relevant interventions identified
Review of available
Guidelines
Interventions recommended in guidelines extracted and presented to expert workgroup
Expert workgroup identified four interventions as potential key elements of ICP:
1. Acute Stroke Service 2. Early Specialist Assessment for TIA 3. Early Administration of IV Alteplase 4. Stroke Rehabiliation
• Expert workgroup prioritise key elements of care
Identify key elements of care

14
- PubMed (MEDLINE)
- EMBASE
- US National Guideline Clearinghouse (NGC)
- Canadian Medical Association (CMA) Infobase
- Scottish Intercollegiate Guidelines Network (SIGN) website
- UK National Institute for Health and Clinical Excellence (NICE) website
- Australian National Health and Medical Research Council (NHMRC) website
• Team conduct intensive search and critical appraisal of current evidence
Literature search for current evidence
- Critically appraised articles, applying SIGN levels of evidence - Summarised and quantified effect size of outcome measures
• Team conduct intensive search and critical appraisal of current evidence
Literature search for current evidence

15
Graphic presentation of clinical benefits
• Includes quantification of effect size + economic evaluation where possible
Construct evidence matrix
So What?

16
Identify Problem
Identify, Review,
Select Knowledge
Monitor
Knowledge
Use
Sustain
Knowledge
Use
Evaluate
Outcomes
Adapt
Knowledge
to Local Context
Assess Barriers/
Supports to
Knowledge Use
Select, Tailor,
Implement
Interventions
Products/
Tools
Synthesis
Knowledge
Inquiry
KNOWLEDGE CREATION
Graham et al (2006): Lost in Knowledge
Translation: Time for a Map?
MOH took necessary
actions to make
changes to relevant
health policies.
Funding provided to
one RHS to pilot the
recommendations
Programme
monitoring, data
collection
Programme
evaluation through
KPIs and targets
Key elements to be
incorporated into the
standards of care for
RHS
Other ICPs in Singapore
• Hip Fracture: – Similar methodology looking across the whole
spectrum of care from pre-hospitalisation, acute
phase, rehabilitation and community.

17
• Diabetes Mellitus: – Focused HTA reviews on certain aspects of DM care
that the expert workgroup feels need more evidence
for:
1. Universal screening of diabetes
2. Effectiveness of hospital glucose teams
3. Discharge care plans for hospitalised DM
patients
4. Frequency of scheduled glucose monitoring
5. Influenza vaccination for people with DM
• Chronic Obstructive Pulmonary Disease: – Reviews of economic evaluations on identified
treatment modalities for COPD which will contribute
towards expert workgroup’s recommendations
Cost-Effective
Not cost-
effective
Insufficient
Evidence
Inhaled
Corticosteroids Triple therapy Indacaterol
Seretide Roflumilast
Symbicort Endobronchial
valves
Spiriva Pulmonary
rehabilitation

18
In conclusion
• Evidence-based approach adopted for policy
and programme development by MOH
• HTA methodology applied to develop
integrated care pathways
• Developing the pathway alone is insufficient
for implementation. Important to include
knowledge translation processes.
Policy
Impact
Thanks to ICP Project Team,
especially Drs KH Pwee and Jeff Loke