how minor is minor? collision forces and injuryaomevents.com/media/files/crash...
TRANSCRIPT
HOW MINOR IS MINOR?
COLLISION FORCES AND
INJURY
Robert AndersonHall Technical
Adj. Assoc. Prof., University of Adelaide
OUTLINE
• Trends in low level impact leading to occupants seeking medical
treatment
• The physics of collisions
• How crash forces are transmitted to the occupant
• Human tolerance / risks of injury
• Reconstruction methodologies
WHAT ARE THE MOST COMMON MINOR
INJURY CRASHES?
• Rear end crashes account for the majority
• 30% of rear end crashes lead to doctor treatment, only
slightly less than property damage only
• 60% of doctor treatments after crashes are due to rear end
crashes

REAR END CRASH NUMBERS OVER TIME
Introduction
of new scheme

Data for NSWSource: Sydney Morning Herald, September 10 2016

COMMON QUESTIONS ABOUT
REAR-END CRASHES• What does the evidence say about the speed of the
vehicle(s) involved in the crash?
• What occupant motions are likely and what forces were
acting on the occupant(s) during the crash
• What injuries might be expected given the severity of the
crash?

PHYSICS OF A REAR END CRASH
• Pre-crash phase
• Crash phase
• (Post crash phase)

PRE-CRASH
• Speed
• Determines initial kinetic energy
• Determines distance travelled during driver reaction
• Distance
• With speed, determines the time available for braking
• Braking
• Duration and level determines speed lost prior to impact
CRASH PHASE
• Momentum and energy
• Speed and ratio of vehicle mass determines change in velocity / average acceleration
levels
• Acceleration of vehicle
• For the struck vehicle, acceleration defines the severity of the crash
• Occupant response
• Acceleration, and the characteristics of the occupant’s restraint (seat), determines the
response of the occupant and the likelihood of injury.
POST CRASH PHASE
• After the exchange of momentum, vehicles continue to move
• A struck vehicle may go on to strike another vehicle in front
• A second (usually more minor) collision may occur
• Movements of vehicles post crash can indicate the severity of the first
crash and hence are a starting point for reconstruction
CRASH PHASE
• crash pulse - delta v - characterises general severity
• Injury mechanisms
• Seat and seat belt effects
• Motion of the head and neck
• Any subsequent frontal collision

SERIOUS INJURY MODES TO THE
CERVICAL SPINE

EXPERIMENTAL STUDIES
MOTION OF THE CERVICAL SPINE
MOTION OF THE CERVICAL SPINE
CASR Road Safety Research Report | Vehicle improvements to reduce the number and severity of rear end crashes 19
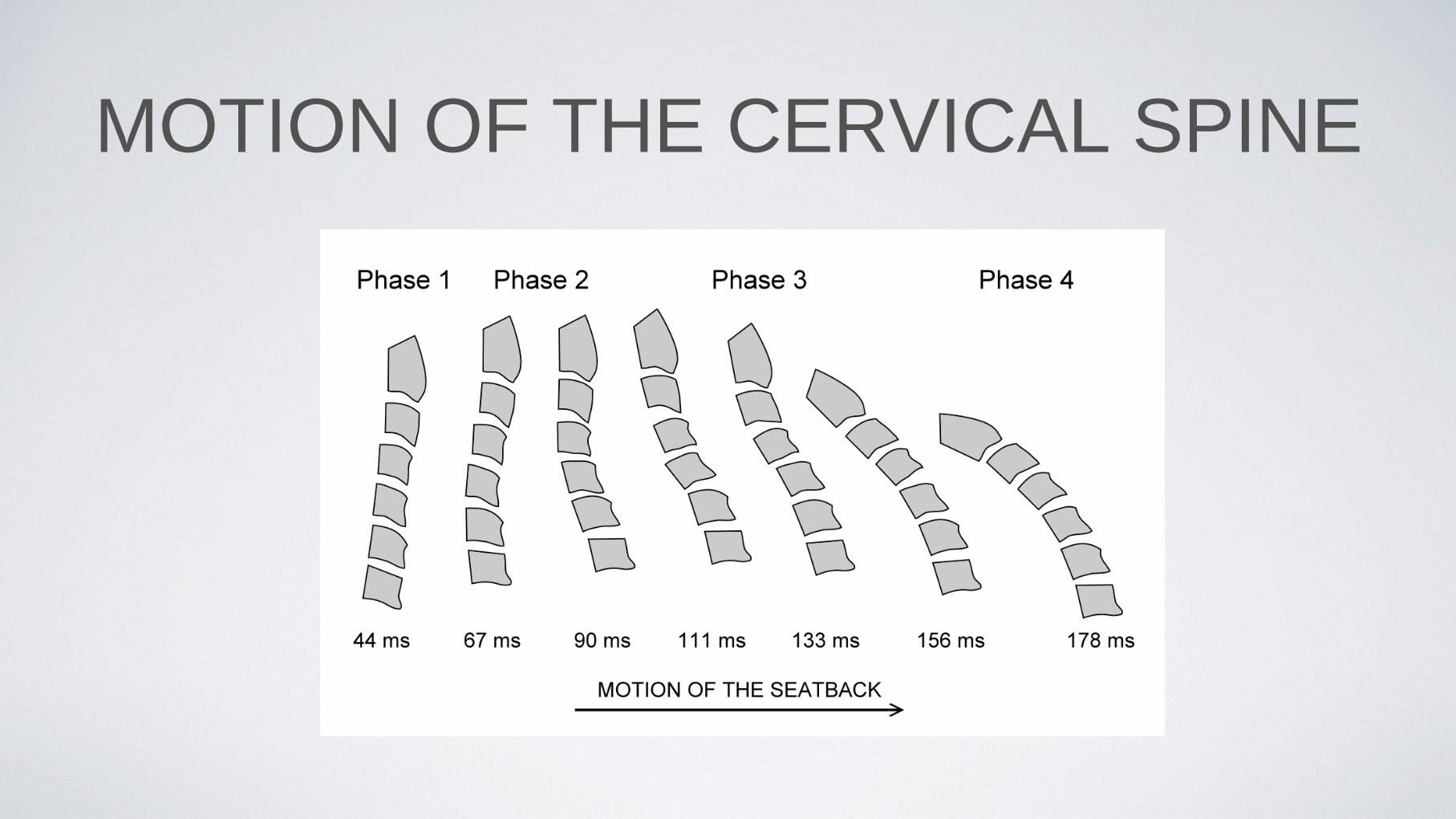
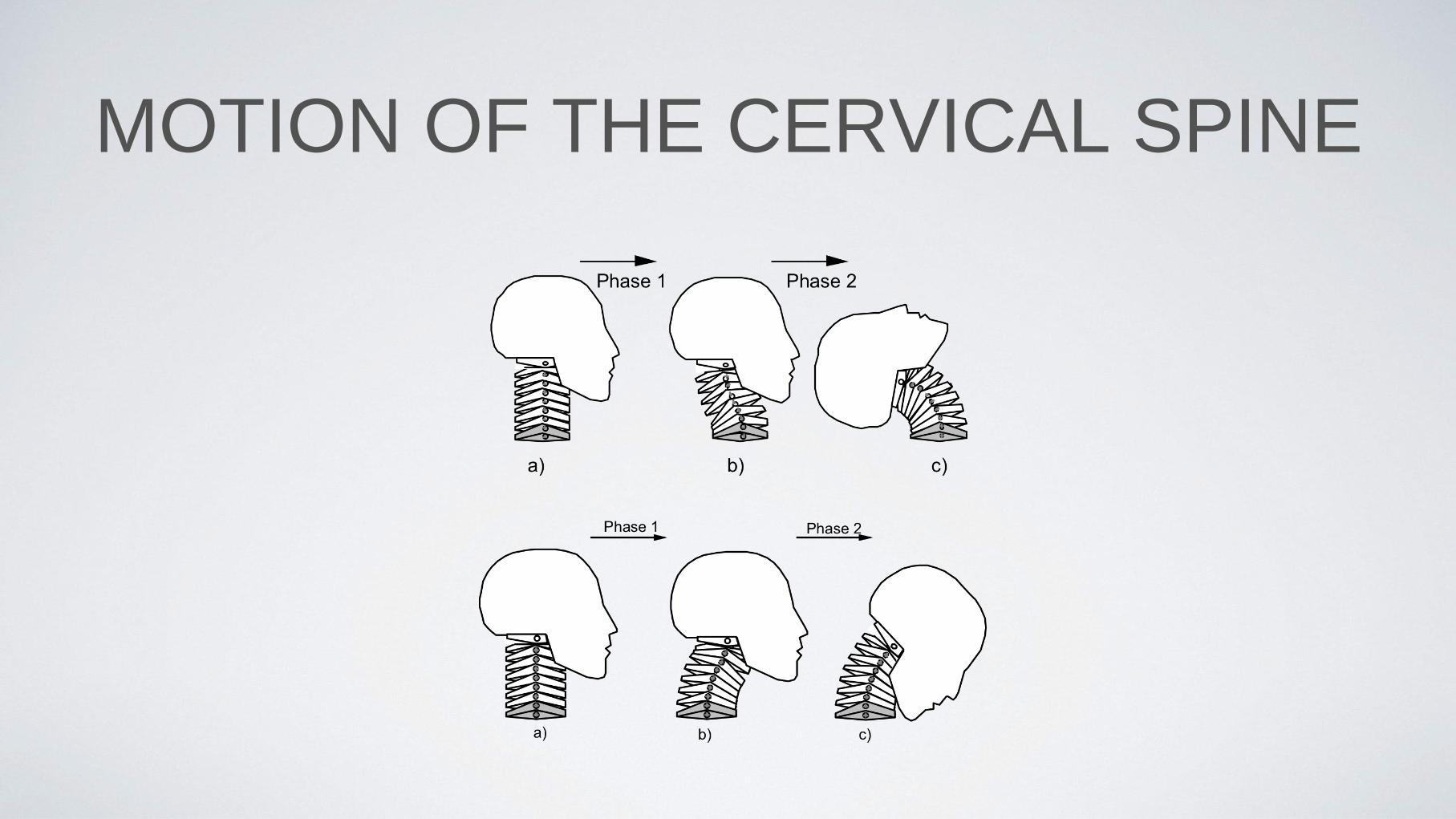
Figure 3.1 shows the kinematic sequence of the motion of the cervical spine during
whiplash motion, in the absence of an effective head restraint, in a rear impact. The
extension of the neck brought about by the forces transmitted to the seat (upper panel of
Figure 3.1) produces two distinct phases of neck motion: in Phase 1, the top and bottom of
the cervical spine are approximately parallel, and the mass of the head causes it to lag the
forward motion of the thorax. This ‘retraction’ phase causes the cervical spine to assume an
‘s’ shape. In phase 2, the continued forward motion of the thorax leads to the neck to
assume a full extension (or hyper-extension). During this phase, the thorax may be
rebounding from the seat back.
The lower panel of Figure 3.1 shows the continuation of the rebound of the occupant. The
two phases show that the neck may assume a reverse-‘s’ shape, followed by neck flexion.
High energy in the rebound phase, coupled w ith restraint by the seat belt can increase the
magnitude of these motions in the rebound phase.
Further detail on the kinematics of the head and neck can be found in Gibson (2006).
Figure 3.1 Cervical spine motion during whiplash motion (reproduced from Svensson et al., 2005)
3.3 General principles of restraint design and designing for whiplash prevention
While biomechanics of whiplash injury is still the subject of research, basic principles of
restraint design can be applied to reduce forces on the neck in a rear impact. For any type of
restraint to be effective, several principles have to be observed. These include:
· eliminating ‘slack’ in the restraint system,
· maximising the proportion of the occupant’s kinetic energy that is absorbed by the
vehicle structure, and minimising the proportion absorbed by the restraint (this
keeps the forces placed on the occupant low),

WHEN IS INJURY LIKELY TO
OCCUR?• There are three distinct periods that are hypothesised to have the potential to cause injury to
the neck
• Early in the impact event during the head retraction period and leading to the ‘S’ shape of
the neck (Phase 2);
• Due to the impact with the head restraint, if it is poorly positioned with respect to the head
and neck at the time of contact (Phase 3);
• Due to hyperextension for a severe impact with a poorly fitted head restraint or without one
(Phase 4); and,
• During the rebound into the seat belt (Phase 4).

SEATS ARE A FORM OF RESTRAINT
• Seats are a form of restraint, just like seat belts or airbags
• Allow occupants to ride down an impact
• Just like all restraints, “slack” degrades performance
• Just like all restraints, performance is improved if ride-down can occur over the
longest distance
• Head rests should be close to the head
• Controlled “collapse” can reduce forces
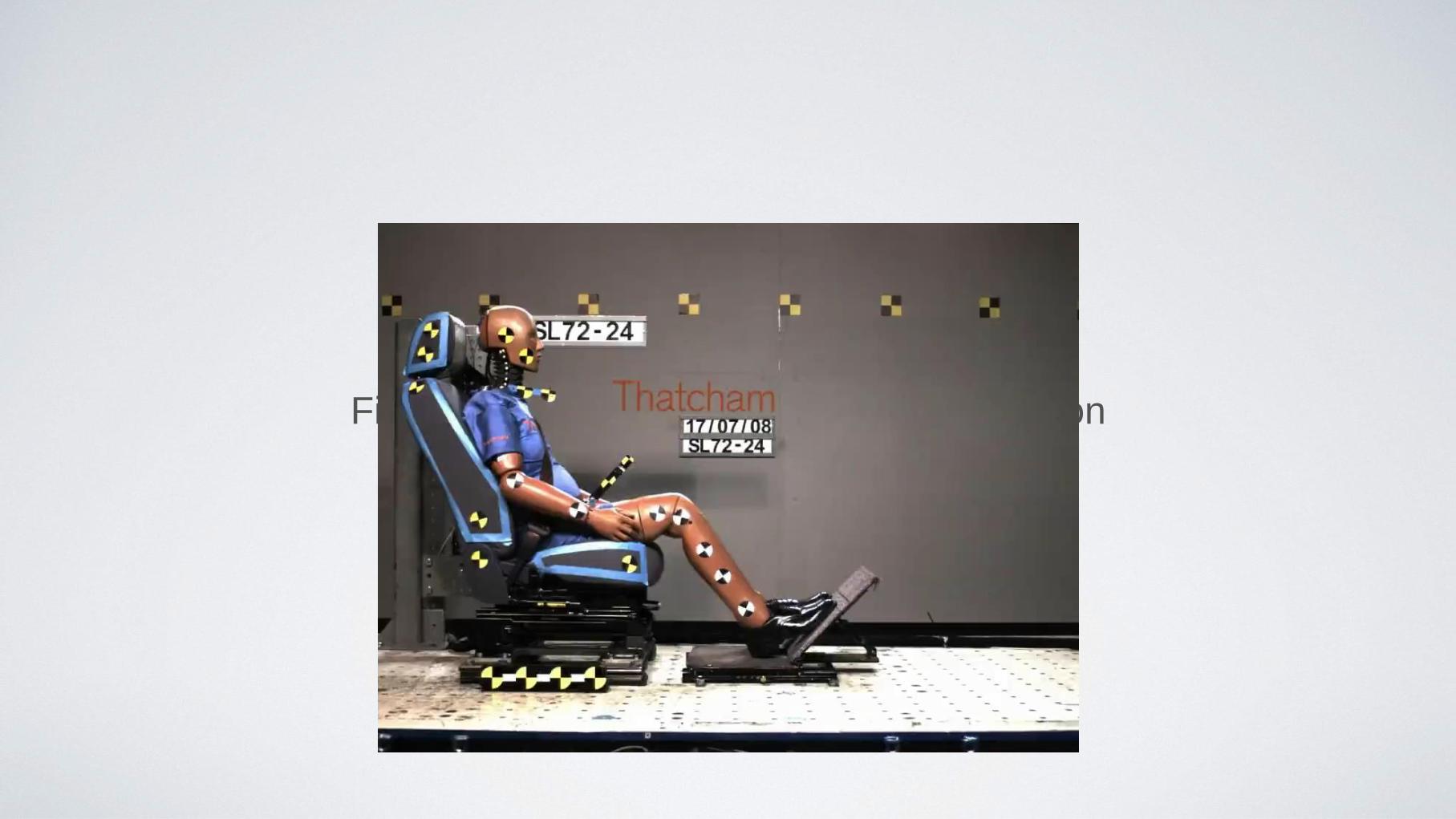
Find video of thatcham test I put in Cameron
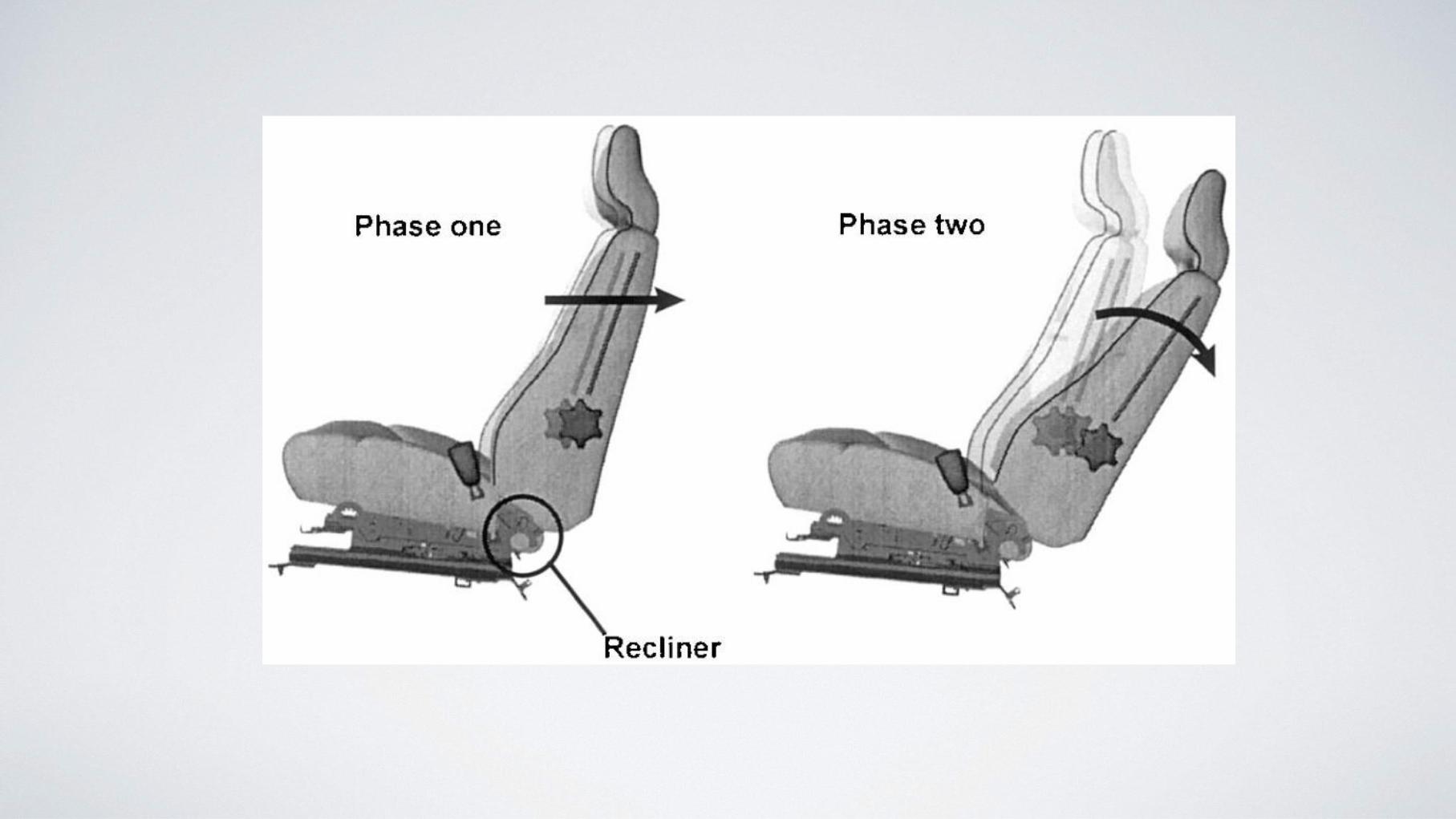
22 CASR Road Safety Research Report | Vehicle improvements to reduce the number and severity of rear end crashes
while the head comes into contact w ith the head rest. During the second phase, the seat
back reclines under load extending the distance over which the occupant is brought to rest.
The intention is to reduce the accelerations applied to the occupant during the collision
(Jakobssen, 2000). The two phases are shown in Figure 3.2.
Figure 3.2 The mechanism of the Volvo WhiPS seat (reproduced from Jakobsson et al., 2000)
The WHIPS seat has been shown to reduce many of the head-neck kinematics thought to
be associated w ith whiplash injury (Welcher and Szabo, 2001).
3.4.3 Passive seats: the Toyota Whiplash Lessening (WIL) seat
Toyota’s objectives in the development of the WIL seat were to decrease neck motion
throughout the rear-impact event, and to control the energy dissipation of the occupant. At
the initial stages of a rear impact, the headrest moves toward the head and upward, the
upper portion of the seat moves away from the upper body, while the remaining seat back
maintains its support to the thorax. The overall effect is to allow the upper body to sink
further into the seat, lessening differential motion between the thorax and head. The seat
also yields somewhat, increasing the distance over which the occupant’s energy is
dissipated, lowering acceleration.
To date, in-field benefits of the WIL system have not been observed; evaluations have not
found any measureable reductions in the incidence of WAD w ith the system (Kullgren et al.,
2007). Results of testing have been equivocal also (e.g. ADAC, 2007).
3.4.4 Pro-active head restraints: Mercedes-Benz Neck-Pro, BMW pyrotechnic head restraint
Pro-active head restraints are those that automatically move up and forward at the start of
the crash, actuated by crash sensors on the bumper, or w ithin the car. The Mercedes-Benz
Neck-Pro seat has a deployable spring loaded head restraint that moves forward and upward
in the initial stages of a rear impact to remove the gap between the head of the occupant
and the head restraint. No real-world evaluations of this seat were identified for this review,
but the IIHS has consistently rated this seat as ‘good’ in its dynamic evaluations.
The BMW pyrotechnic head restraint is similar in principle, but uses a gas filled cartridge to
propel the head restraint upward during a rear-end crash. It is available on a limited number
of models only and these are all rated as good test programs.
CRASH SEVERITY AND INJURY
SEVERITY
• What do we expect to see in rear end crashes with respect to severity?
• Up to 12 km/h change in velocity (i.e. ~ 24 km/h impact speed)
• No motions of the neck outside the normal range
• In 25 out of 767 volunteer tests produced transient soreness for less than one day.
Two tests produced soreness for less than 2 weeks.
• Conservatively applied, absolute limit for no initial signs is 8 kph

CRASH SEVERITY AND INJURY
SEVERITY
• In very low speed crashes, (under 8 kph change in speed) we do
not expect to see forces on the neck and back that are outside the
experience of everyday activities
• Vehicle accelerations typically < 3 g
• Forces generated in the neck are often just a few percent of the
levels thought to be cause serious injury

REAR CRASH IMPACT FORCES IN
CONTEXT• Series of tests where a passenger vehicle was accelerated by a low speed
side-swipe with a truck
• Vehicle accelerations ~ 2 - 3 g
• Head accelerations ~ 4 - 6 g
• Similar to crowd jostle, chair kick, hop off step, chair plop, sneeze,
playground swing
• Less than falling down, soccer ball strike
CRASH SEVERITY AND INJURY
SEVERITY
• One of the great difficulties in explaining reported neck injury
severity is that outcomes often do not alway reflect crash
severity

2 CASR Road Safety Research Report |Whiplash associated disorders: a comprehensive review
Table 1.1 The Quebec Classification of Whiplash-Associated Disorders
Grade Clinical presentation
0 No complaint about the neck
No physical signs
I Neck complaint of pain, stiffness or tendernessonly
No physical signs
II Neck complaint, and
Musculoskeletal signs*
III Neck complaint, and
Neurological signs✝
IV Neck complaint, and
Fracture dislocation
* Musculoskeletal signs include decreased range of motion andpoint tenderness
✝ Neurological signs include decreased or absent deep tendonreflexes, weakness and sensory deficits
The implication is that the Classification is an ordered categorical scale with each successive
grade severer than the previous one (Spitzer, Skovron et al., 1995, suggest that the
Classification corresponds “ roughly” to severity). However, w ithin each classification, there
is no provision for including any assessment of the severity of the symptom, so that
someone suffering from intense pain w ith no other signs, might be assessed as WAD-I
alongside an individual with only mild pain.
It is also worth noting that the Classification was devised with two axes: the grade of WAD
that corresponds to severity (Table 1.1) on a “ clinical-anatomic” axis and a second grade on
a time axis that categorises, for each clinical-anatomic grade, the time to recovery: The time
categories are: less than 4 days, 4-21 days, 22-45 days, 46-180 days and greater than 180
days (chronic).
Although the Québec Task Force proposed a second axis to deal w ith the duration of
symptoms of WAD, time-to-recovery is often used as an independent outcome measure,
and some research art icles imply that, by definit ion, a useful scale that grades
injury/symptomology on presentation should predict the course of the injury. Hartling, Brison
et al. (2001) evaluated the utility of the Québec Classification of WAD in correctly predicting
the prognosis of patients as measured by the probability of still having WAD at 6, 12, 18 and
24 months. They conclude that the Classification system is useful in the clinical setting
despite somewhat inconclusive statistics. While the odds of still having WAD appeared to
increase w ith the Grade on presentation, the relationship was weak and it is hard to
envisage the clinical utility of the Classification in predicting time-to-recovery on the basis
their findings. They did, however, find that physical range-of-motion of the neck might be
useful as a prognostic tool.
Suissa et al. (2001) produced a better estimate of the utility of the Québec classification of
WAD in a retrospective review of 2843 claimants from the Société de l’assurance
automobile du Québec. The study examined the prognostic value of the initial signs and
symptoms and then reclassified individuals according to the Québec classification of WAD.
Groups of individuals classified as having Grades II or III WAD had different rates of recovery
from those having Grade I WAD. However, the authors found many better prognostic
factors with which to classify people presenting with a whiplash injury (see later sections).
1.2.3 Chronic whiplash injury (“ late whiplash syndrome”)
Chronic whiplash or “ late whiplash syndrome” includes the collection of symptoms and
signs that exist in a patient beyond a period in which recovery might normally be expected.
CRASH SEVERITY AND INJURY
SEVERITY
• One of the great difficulties in explaining reported neck injury
severity is that outcomes often do not alway reflect crash
severity
• Some have proposed ‘bio-psychosocial’ models of whiplash
injury in order to explain prognoses of whiplash associated
disorders

MEASURING RISK FROM ACTUAL
CRASHES
SWEDISH FOLKSAM / SAFER CRASH
STUDY
• 175 rear end impacts
• Crash pulses were measured
• Participants provided self-reports of injury intensity and
duration
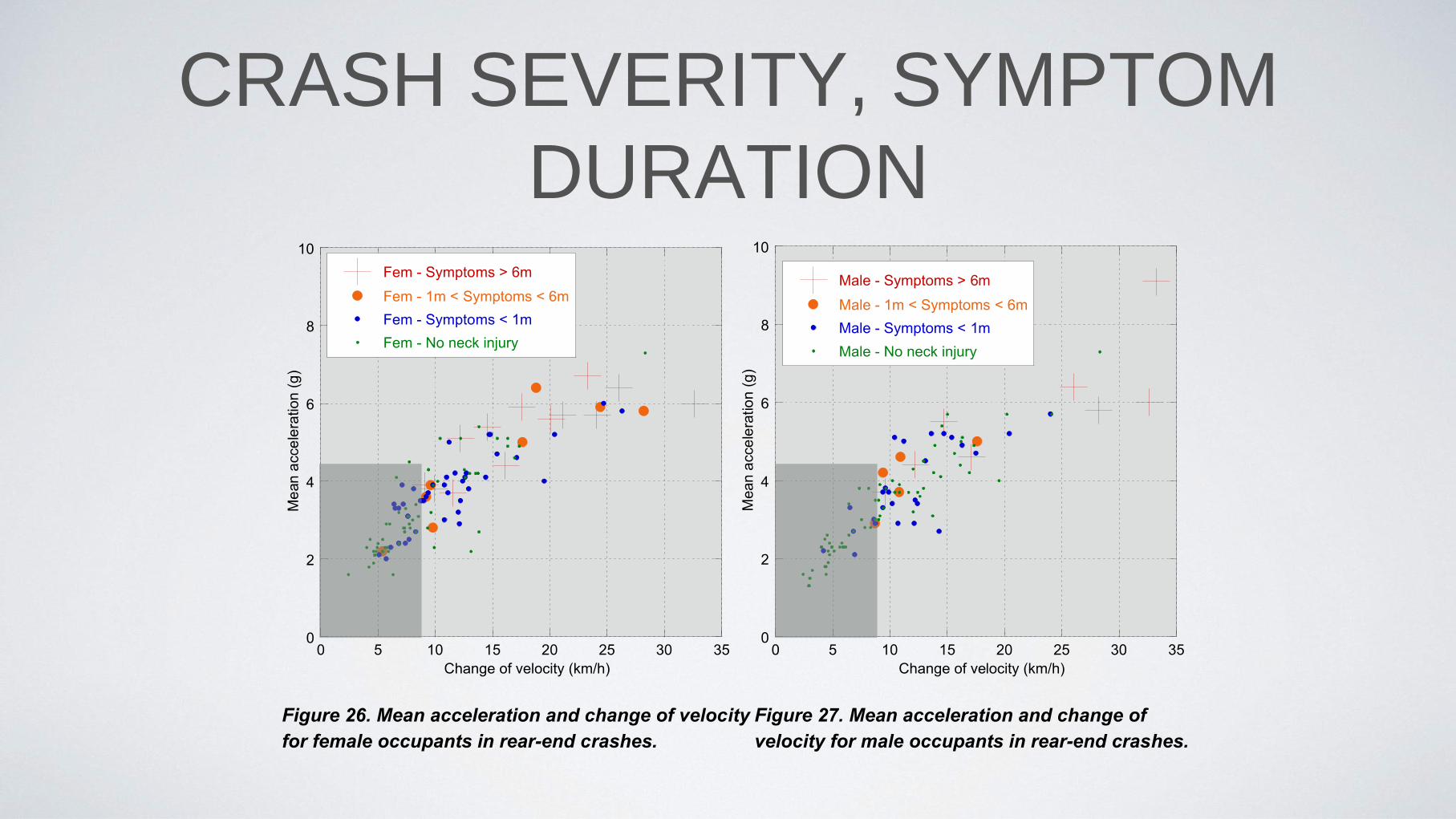
CRASH SEVERITY, SYMPTOM
DURATION

ASCERTAINING SEVERITY FROM
DAMAGE• Physical evidence after a low level impact is often subtle
• However, the damage caused is a consequence of energy absorption
• If this energy absorption can be estimated, then the speed and severity can be
determined
• Ideally this speed can be corroborated from other directions
• e.g. vehicle accelerated from stationary into rear of vehicle, struck vehicle hit
the car in front etc.

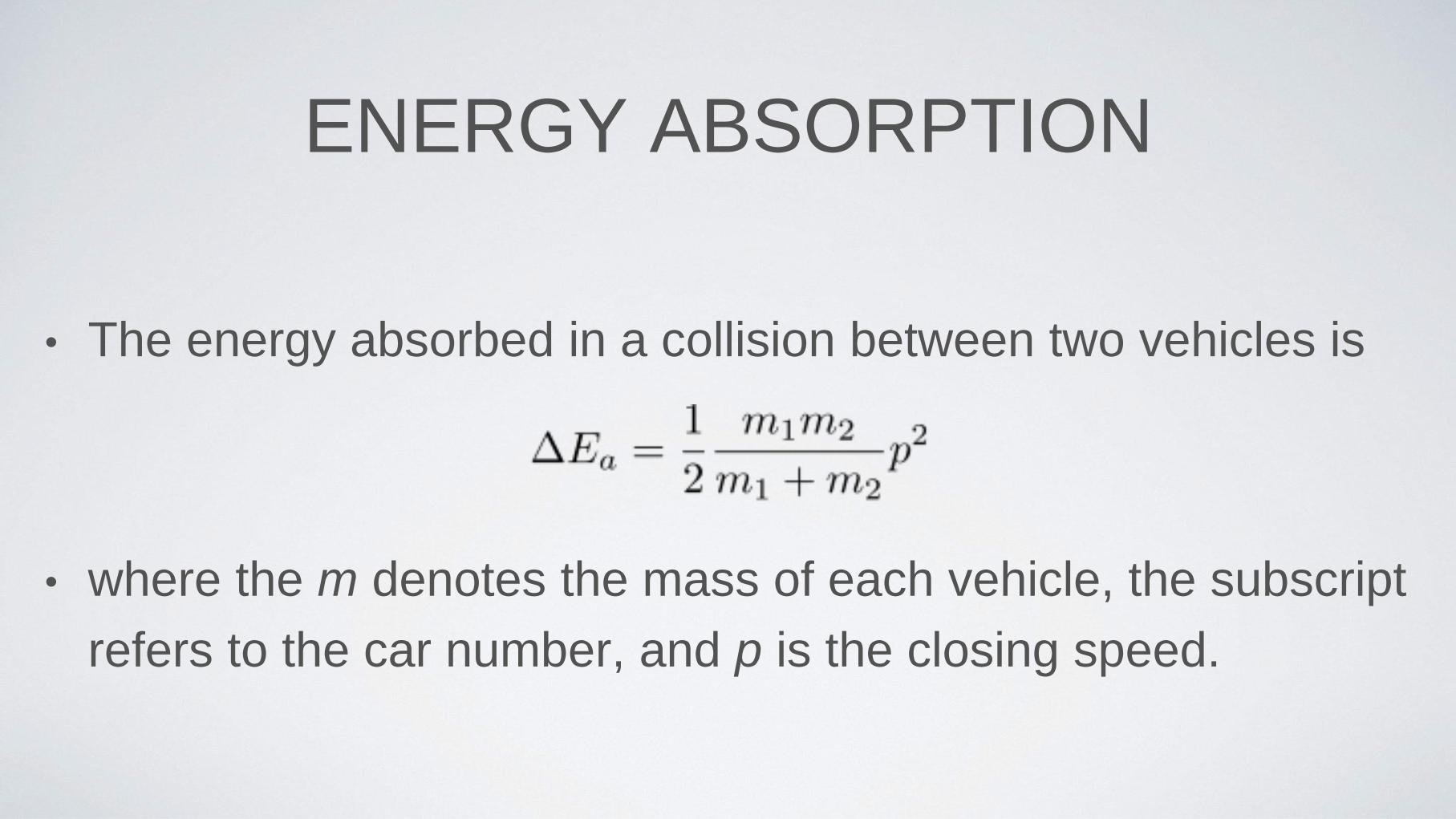
ENERGY ABSORPTION
• The energy absorbed in a collision between two vehicles is
• where the m denotes the mass of each vehicle, the subscript
refers to the car number, and p is the closing speed.
STAGED TESTS
• Known speed, known energy absorption

USING THIS INFORMATION
• Generally describes damage
• Often, subject vehicle model has been tested so a more direct
comparison can be made
• Its extremely important to adjust for the differences between the test
and the subject crash
• Barrier tests are very stiff and against an unyielding mass

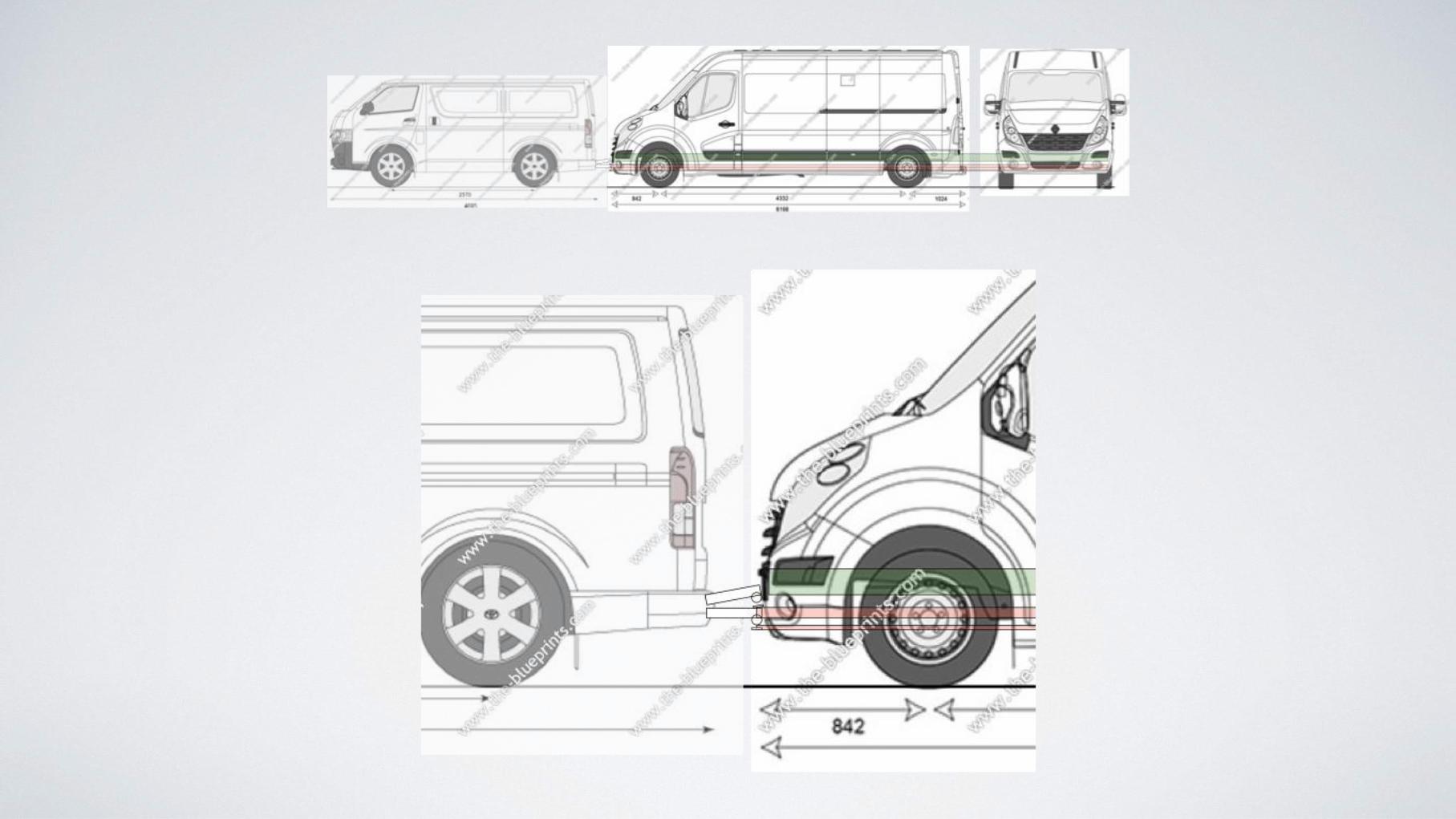
DEFORMATION DISTANCE
• Damaged components usually are nearest
the impact surface
• The depth of damage indicates the
maximum deformation of the vehicle


SPECIAL CASES
• tow bars can transmit forces forward to the area of a vehicle
near the back of the boot. Bumpers can be undamaged but
there is deformation away from the impact point
• tow bars an bull bars can “sharpen” the impact. This may
have some effect on injury risk.
FINAL POINTS
• Rear-end collisions are one of the most common crash types, and associated
with WAD
• General principles of momentum and energy can be used to reconstruct them
• For the struck occupant, the seat is the restraint system. Normal restraint
principles apply
• Crash severity often very low and disproportionate numbers of claimants
require no real medical intervention at the time of injury

FINAL POINTS
• Reasons for WAD appear to be complex, and the literature makes
clear that compensation systems do affect rates of WAD.
• Then why to anti-whiplash seats work?
• The key seems to be the prevention of any initial pain
• If pain is present then for some people, other factors may turn the very
minor crash into a big problem