how do geneticists and genetic counselors counsel women from high-risk breast cancer families?
TRANSCRIPT
P1: GDW/GDB
Journal of Genetic Counseling [jgc] PH021-296948 February 4, 2001 12:25 Style file version Nov. 19th, 1999
Journal of Genetic Counseling, Vol. 10, No. 2, 2001
How Do Geneticists and Genetic Counselors CounselWomen from High-Risk Breast Cancer Families?
Elizabeth Lobb,1,4 Phyllis Butow,1 Bettina Meiser,2 Katherine Tucker,2
and Alexandra Barratt 3
This qualitative study asked Australian Genetic Counselors and Clinical Geneti-cists working in cancer genetics to describe their practice when a woman attendsa consultation about her family history and her risk of developing breast cancer.Twenty-nine out of 36 Clinical Geneticists/Genetic Counselors returned the ques-tionnaire (82%). Participants identified the key goals of the consultation as (a)identifying the individual needs and concerns of the woman, (b) providing infor-mation on genes and chromosomes, (c) giving an individual risk assessment in thecontext of supportive interaction, and (d) discussing the pros and cons of genetictesting and putting a surveillance plan into place. Respondents emphasized thedual importance of counseling/support and information provision in this setting,suggesting that one could not be given without the other. Implications for clinicalpractice are discussed.
KEY WORDS: genetic counseling; familial breast/ovarian cancer; genetic counselors/geneticistsperceptions.
INTRODUCTION
Family history is an important factor in the pathogenesis of a variety of cancerswith 5–10% of cancers attributed to an inherited cancer predisposition. Two breastcancer predisposition genes with high penetrance,BRCA1andBRCA2, have been
1Medical Psychology Research Unit, Department of Psychological Medicine, University of Sydney,Sydney NSW 2006, Australia.
2Hereditary Cancer Clinic, Prince of Wales Hospital, Sydney, NSW 2031, Australia.3Department of Public Health and Community Medicine, University of Sydney, Sydney, NSW 2006,Australia.
4Correspondence should be directed to Elizabeth Lobb, Medical Psychology Research Unit,Department of Psychological Medicine, University of Sydney, NSW 2006, Australia; e-mail:[email protected].
185
1059-7700/01/0400-0185$19.50/1C© 2001 National Society of Genetic Counselors, Inc.
P1: GDW/GDB
Journal of Genetic Counseling [jgc] PH021-296948 February 4, 2001 12:25 Style file version Nov. 19th, 1999
186 Lobb, Butow, Meiser, Tucker, and Barratt
localized and cloned (Hallet al., 1990; Miki et al., 1994; Woosteret al., 1994,1995).BRCA1andBRCA2mutations are associated with an increased lifetimerisk of developing breast cancer of up to 85%, and a lifetime risk of developingovarian cancer (which varies with different mutations) of 15–60% (Easton, 1997;Struewinget al., 1997). Genetic testing for those with a strong family history ofthe disease is now possible. However, the lack of a functional assay, the presenceof hundreds of unclassified variants, and the low mutation-detection rate makeinterpretation of the tests difficult. Estimates of the proportion of breast cancersassociated with mutations inBRCA1andBRCA2range from 3% to 5%. Thus,the vast majority of breast cancers arise as a result of more complex interactionsbetween genetic and environmental factors.
The training and practice of genetic counselors differs between countries(Kenen and Smith, 1995). The majority of clinical genetics services, with or withoutgenetic counseling, are provided by physicians who are trained medical geneticists(Beisecker and Marteau, 1999). In the United States and Canada, a significant de-gree of genetic counseling is provided by genetic counselors trained at the Master’sdegree level (Andrewset al., 1994; Harris, 1998), and in Europe social workers,psychologists, and geneticists provide counseling (Skirton, 1999). Genetic coun-seling in the United Kingdom is usually provided by a multidisciplinary team thatincludes medical geneticists and nonmedical counselors, the majority of whomhave nursing backgrounds (Skirton, 1999).
Cancer genetic services in Australia offer testing through specialized familialcancer clinics that usually include a physician (clinical geneticist or oncologist) anda genetic counsellor, and are often linked to oncology services. The Counselors aregenetic counselors, oncology nurses, social workers, or psychologists with exper-tise in oncology or genetics (National Health & Medical Research Council, 1999).The Human Genetics Society of Australasia has developed an accredited trainingprogram for both general genetic and cancer genetic counselors. These clinicsprovide a comprehensive service including risk assessment, genetic testing, andadvice regarding early detection and prevention (Kirk and Tucker, 1997). Referralis necessary, and genetic counseling and testing are currently available in both theState-funded health system and in the private sector. Management guidelines forfamilial cancer clinics have recently been developed by the National Health andMedical Research Council. These guidelines suggest pre- and postgenetic test-ing counseling, and fully informed consent (National Health & Medical ResearchCouncil, 1999). Predictive testing is almost always restricted to those where afamily specific mutation is known.
It is suggested that research into the process of genetic counseling shouldexamine the views and roles of both the counselors and counselees (Michieet al.,1997; Kessler, 1992). Clinical geneticists’ attitudes and practice toward testingfor breast cancer susceptibility genes in the United Kingdom was assessed usinga series of case scenarios (Lucassen and Houlston, 2000). Several studies sought
P1: GDW/GDB
Journal of Genetic Counseling [jgc] PH021-296948 February 4, 2001 12:25 Style file version Nov. 19th, 1999
How Do Geneticists and Genetic Counselors Counsel Women? 187
to define the role of the genetic nurse practitioner (Farnish, 1988; Skirtonet al.,1997), and two studies have examined the objectives of genetic counseling fromthe perspective of the provider (Michieet al., 1998, 1999).
The current study asked Australian clinical geneticists and genetic counselorsabout their perceptions of consultations with women from high-risk breast cancerfamilies. They were also asked how they perceived their role in interactions withthese women. This survey was undertaken as part of a larger study of geneticcounseling in women from high-risk breast cancer families. The larger study isexploring the actual process of genetic counseling, using transcripts from audio-taped genetic counseling consultations.
METHODS
Participants
A comprehensive list of professionals working within genetics was compiledusing the membership of the Human Genetic Counselors Society of Australasia.Those professionals working specifically in cancer genetics were identified by keypersonnel working in cancer genetics in each state. A brief qualitative survey wasmailed to this subgroup of clinical geneticists and genetic counselors. A reminderletter and a second copy of the questionnaire were mailed 3 weeks after the firstcontact if the questionnaire was not returned.
Participants were asked to provide some basic demographic and professionaldetails and to respond to five open-ended questions: (a) to identify their goals/aimsin consultations with women from high-risk breast cancer families; (b) to definethe content of genetic counseling for women from these families; (c) to list theinformation they usually provide in the first consultation; (d) to provide their viewson why women come for genetic counseling; and (e) to describe the importanceof counseling skills in their role as a genetic counselor/geneticist.
As an adjunct to this final question, participants were asked to make a mark ona 10-cm Visual Analogue Scale to indicate their beliefs regarding the importance ofcounseling in cancer genetics. This line was anchored by two quotes characterizingextreme views on this issue, as follows:
Anchor A: The provider of genetic counseling has a greater concern for the subjectivemeaning of content issues, as well as for its inter-personal consequences. His/her centralfocus may be on here and now issues. Many providers would view the problems with whichcounselees come to genetic counseling as life crises, understandable only in the contextof their overall life histories as individuals, as members of a family, and as members of aspecific group. (Kessler, 1997)
Anchor B: The provider of genetic counseling has an over-riding concern with the accuratediagnosis of genetic disease, the precise calculation of genetic risk, and other content matters.His/her focus is generally oriented along a past-future dimension; the past reflected in thepedigree information, the future in predictive risk figures. Often he/she approaches the
P1: GDW/GDB
Journal of Genetic Counseling [jgc] PH021-296948 February 4, 2001 12:25 Style file version Nov. 19th, 1999
188 Lobb, Butow, Meiser, Tucker, and Barratt
genetic counseling encounter as a self-contained problem-solving situation, an end to itself.(Kessler, 1997)
Data Analysis
The open-ended responses in the questionnaire were analyzed using theconstant-comparative method proposed by Glaser and Strauss (1967). This in-volves coding each unit of meaning (i.e., specific response), and comparing andcontrasting these to identify recurring regularities and discrete categories. Theresearch team met regularly to review the coding and resolve differences in thelabeling and categorizing of responses until consensus was reached. This resultedin the development of an analytic framework of 40 discrete categories of informa-tion from the questionnaires. The frequency with which these categories appearedwas then analyzed using a qualitative data analysis package (NUD*IST; Richards,1998). NUD*IST is a package which organizes qualitative data and allows allexamples within a particular category to be easily extracted.
RESULTS
Thirty-six questionnaires were mailed. Twenty-nine questionnaires were re-turned (82% return rate). The mean age of participants was 38 years (range 24–58 years). Five participants were male (four of the male participants were clini-cal geneticists) and 24 were female. Seven respondents were clinical geneticists,20 were genetic counselors, and the remaining participants’ areas of expertiseincluded oncology (1) and nursing (1). Nineteen participants indicated that theyworked both in general and cancer genetics and nine participants indicated thatthey worked in cancer genetics only. The length of time participants had workedin the area of genetics ranged from 5 months to 12 years with a median of 4 years.
The Consultation With a Woman From a High-RiskBreast Cancer Family
Table I provides an overview of perceived aims in the consultation with awoman from a high-risk breast cancer family. The most commonly cited goal oraim of genetic counseling for women from high-risk breast cancer families wasidentifying the individual needs and concerns of the woman (see Table I) as it wasacknowledged that “not everyone wants the same thing from a consultation.” Asone geneticist succinctly explained
I very much support the view that patients are not problems to be assessed and fixed. Theycome with similar problems but are also responding to environment, society, family, finan-cial circumstances, ethnic background, experience with cancer etc. etc.—all are different.(Clinical Geneticist)

P1: GDW/GDB
Journal of Genetic Counseling [jgc] PH021-296948 February 4, 2001 12:25 Style file version Nov. 19th, 1999
How Do Geneticists and Genetic Counselors Counsel Women? 189
Table I. Goals or Aims/Definition of Genetic Counseling
20–25 responsesIdentify needs and concerns of womanRisk assessment
17–20 responsesDiscuss genetic testingDiscuss surveillanceDiscuss genes and chromosomes
10–17 responsesProvide accurate informationRecord and verify family historyPros and cons of genetic testingAssist in decision-makingExplore issues related to personal/family history of breast cancer
5–10 responsesExplore potential impact of genetic testing on womanProvide supportExplore potential impact of genetic testing on familyEnsure understandingProvide follow-up/back-upAnswer questions
<5 responsesObtain informed consent for genetic testEnroll in researchDiscuss clinical trialsDescribe services available at genetic centreAssist in providing information to familyDiscuss ethics/moral issuesDiscuss insuranceWoman’s perception of her riskProvide written material
Provision of both an individual and family risk assessment was consideredanother key goal. This risk assessment might include a numeric estimate of indi-vidual risk, and clarification and discussion of the woman’s perceived risk. Manyrespondents emphasized the importance of basing this risk assessment on accurate,verified, family history data.
Other respondents felt that being given a risk figure was not the focus of theconsultation:
Most clients are not requesting specific risk figures when seeking genetic counseling, butcome to explore the many facets of the disease and its impact on self/family and otherimportant relationships. This can be both medical/genetic and most often always emotional.(Genetic Counselor)
Thus, providing information on genetic risk alone was considered by somerespondents to be insufficient. Some respondents felt that high-risk women wantedthe geneticist /counselor to explore the impact of familial risk on themselves andtheir families. Respondents also perceived that they were expected to explore the
P1: GDW/GDB
Journal of Genetic Counseling [jgc] PH021-296948 February 4, 2001 12:25 Style file version Nov. 19th, 1999
190 Lobb, Butow, Meiser, Tucker, and Barratt
women’s concerns, fears, social support, and individual coping strategies. As onerespondent said,
Often this (risk assessment) cannot be undertaken without a psychotherapeutic process ofallowing the consultand to express their concerns for family and self and what they see asthe major issues. (Genetic Counselor)
Indeed some respondents felt that exploration of such issues formed the majorpart of genetic counseling. As one respondent said,
I define genetic counseling as recognizing and exploring issues that are relevant for aparticular family member. For example, previous family history, what happened, how thathas affected the client’s view of breast cancer, what the outcomes have been for the family,what position/age the person was when she (first) became aware of family history and theimpact that has had on her (e.g. mother diagnosed with breast cancer when going throughadolescence). (Genetic Counselor)
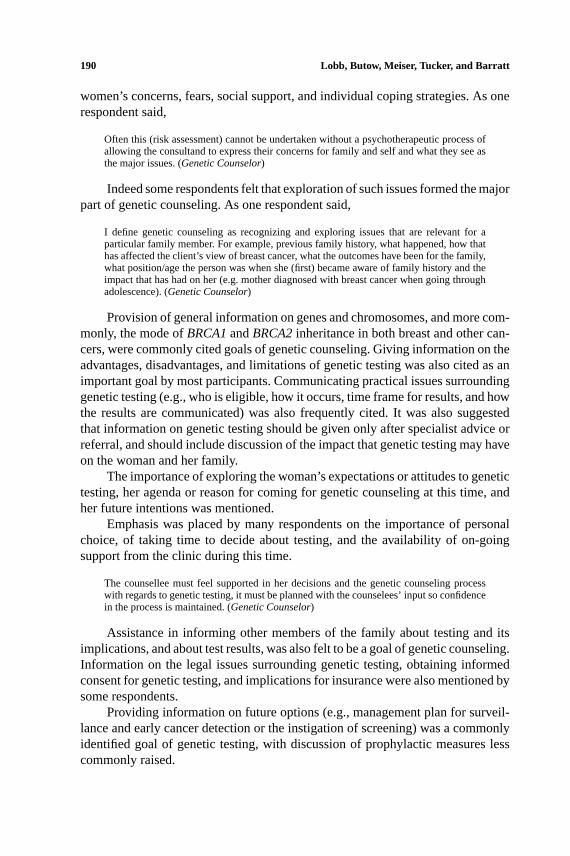
Provision of general information on genes and chromosomes, and more com-monly, the mode ofBRCA1andBRCA2inheritance in both breast and other can-cers, were commonly cited goals of genetic counseling. Giving information on theadvantages, disadvantages, and limitations of genetic testing was also cited as animportant goal by most participants. Communicating practical issues surroundinggenetic testing (e.g., who is eligible, how it occurs, time frame for results, and howthe results are communicated) was also frequently cited. It was also suggestedthat information on genetic testing should be given only after specialist advice orreferral, and should include discussion of the impact that genetic testing may haveon the woman and her family.
The importance of exploring the woman’s expectations or attitudes to genetictesting, her agenda or reason for coming for genetic counseling at this time, andher future intentions was mentioned.
Emphasis was placed by many respondents on the importance of personalchoice, of taking time to decide about testing, and the availability of on-goingsupport from the clinic during this time.
The counsellee must feel supported in her decisions and the genetic counseling processwith regards to genetic testing, it must be planned with the counselees’ input so confidencein the process is maintained. (Genetic Counselor)
Assistance in informing other members of the family about testing and itsimplications, and about test results, was also felt to be a goal of genetic counseling.Information on the legal issues surrounding genetic testing, obtaining informedconsent for genetic testing, and implications for insurance were also mentioned bysome respondents.
Providing information on future options (e.g., management plan for surveil-lance and early cancer detection or the instigation of screening) was a commonlyidentified goal of genetic testing, with discussion of prophylactic measures lesscommonly raised.
P1: GDW/GDB
Journal of Genetic Counseling [jgc] PH021-296948 February 4, 2001 12:25 Style file version Nov. 19th, 1999
How Do Geneticists and Genetic Counselors Counsel Women? 191
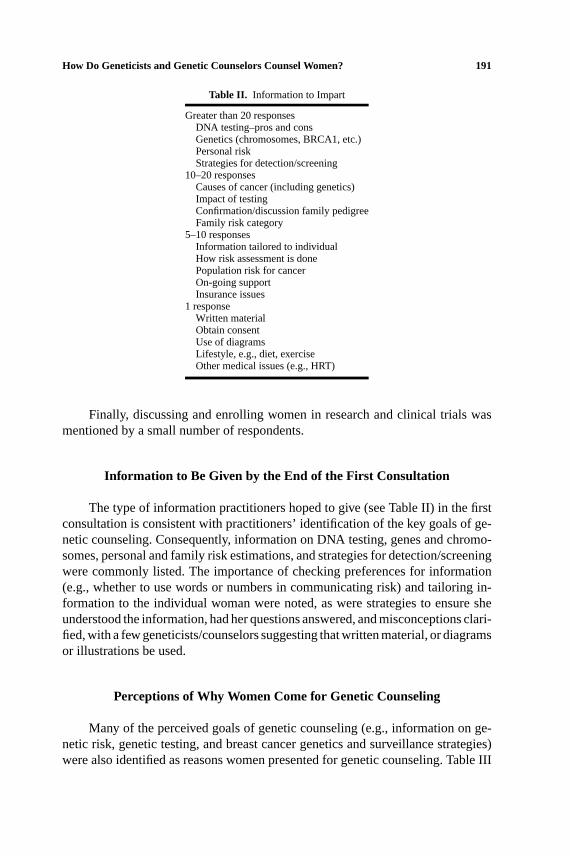
Table II. Information to Impart
Greater than 20 responsesDNA testing–pros and consGenetics (chromosomes, BRCA1, etc.)Personal riskStrategies for detection/screening
10–20 responsesCauses of cancer (including genetics)Impact of testingConfirmation/discussion family pedigreeFamily risk category
5–10 responsesInformation tailored to individualHow risk assessment is donePopulation risk for cancerOn-going supportInsurance issues
1 responseWritten materialObtain consentUse of diagramsLifestyle, e.g., diet, exerciseOther medical issues (e.g., HRT)
Finally, discussing and enrolling women in research and clinical trials wasmentioned by a small number of respondents.
Information to Be Given by the End of the First Consultation
The type of information practitioners hoped to give (see Table II) in the firstconsultation is consistent with practitioners’ identification of the key goals of ge-netic counseling. Consequently, information on DNA testing, genes and chromo-somes, personal and family risk estimations, and strategies for detection/screeningwere commonly listed. The importance of checking preferences for information(e.g., whether to use words or numbers in communicating risk) and tailoring in-formation to the individual woman were noted, as were strategies to ensure sheunderstood the information, had her questions answered, and misconceptions clari-fied, with a few geneticists/counselors suggesting that written material, or diagramsor illustrations be used.
Perceptions of Why Women Come for Genetic Counseling
Many of the perceived goals of genetic counseling (e.g., information on ge-netic risk, genetic testing, and breast cancer genetics and surveillance strategies)were also identified as reasons women presented for genetic counseling. Table III
P1: GDW/GDB
Journal of Genetic Counseling [jgc] PH021-296948 February 4, 2001 12:25 Style file version Nov. 19th, 1999
192 Lobb, Butow, Meiser, Tucker, and Barratt
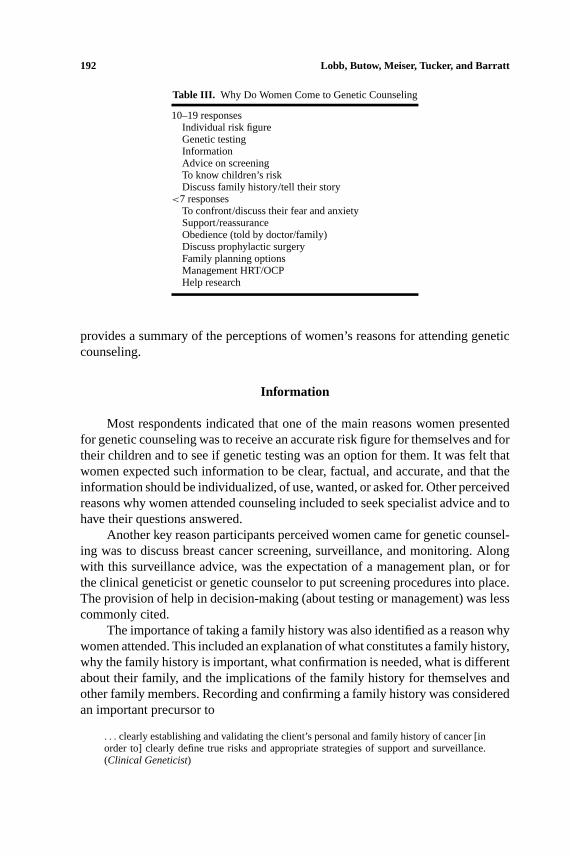
Table III. Why Do Women Come to Genetic Counseling
10–19 responsesIndividual risk figureGenetic testingInformationAdvice on screeningTo know children’s riskDiscuss family history/tell their story
<7 responsesTo confront/discuss their fear and anxietySupport/reassuranceObedience (told by doctor/family)Discuss prophylactic surgeryFamily planning optionsManagement HRT/OCPHelp research
provides a summary of the perceptions of women’s reasons for attending geneticcounseling.
Information
Most respondents indicated that one of the main reasons women presentedfor genetic counseling was to receive an accurate risk figure for themselves and fortheir children and to see if genetic testing was an option for them. It was felt thatwomen expected such information to be clear, factual, and accurate, and that theinformation should be individualized, of use, wanted, or asked for. Other perceivedreasons why women attended counseling included to seek specialist advice and tohave their questions answered.
Another key reason participants perceived women came for genetic counsel-ing was to discuss breast cancer screening, surveillance, and monitoring. Alongwith this surveillance advice, was the expectation of a management plan, or forthe clinical geneticist or genetic counselor to put screening procedures into place.The provision of help in decision-making (about testing or management) was lesscommonly cited.
The importance of taking a family history was also identified as a reason whywomen attended. This included an explanation of what constitutes a family history,why the family history is important, what confirmation is needed, what is differentabout their family, and the implications of the family history for themselves andother family members. Recording and confirming a family history was consideredan important precursor to
. . . clearly establishing and validating the client’s personal and family history of cancer [inorder to] clearly define true risks and appropriate strategies of support and surveillance.(Clinical Geneticist)
P1: GDW/GDB
Journal of Genetic Counseling [jgc] PH021-296948 February 4, 2001 12:25 Style file version Nov. 19th, 1999
How Do Geneticists and Genetic Counselors Counsel Women? 193
Information on the risks and benefits of hormone replacement therapy andthe oral contraceptive pill were less commonly cited reasons for women attendinggenetic counseling.
Emotional Support
Many counselors believed that women saw genetic counseling as an opportu-nity to discuss their experiences of having a family history of breast cancer and theimpact of that history on their lives. Respondents also nominated the opportunityto express emotions and receive support and reassurance in a safe environment,with a health professional who does not have an immediate role in the care of eitherthemselves or their family, who has a shared rapport, and is willing to listen to themwith empathy. It was also felt that the counseling relationship should be honest andopen, nonjudgmental, confidential, compassionate, sensitive, and client-focussed.Counseling skills that were supportive, and explored the woman’s coping strate-gies, as well as her feelings about the impact of genetic testing on herself and herfamily, were identified as the client-focussed goals of genetic counseling. As onerespondent said,
The area of breast cancer is one with much suffering, physical and emotional, guilt andanxiety. Counselees expect to be able to express their fears, test their family beliefs andto be heard in an empathic manner. Support may often be necessary. At the same timeinformation must be gained, and given, as skillfully as possible. (Genetic Counselor)
Respondents also felt women presented to receive a “yes” or “no” answer asto whether they had a mutation in a breast cancer gene, and that women mightexpect the consultation to lower their anxiety and to be given advice on how to telltheir families about the findings.
One respondent suggested that women were being “obedient” to their doctoror family who had told them to come to genetic counseling, and had little ideawhat services were available, for example, “some women don’t know why theirdoctor sent them.” Others believed women attended for altruistic reasons (to helpresearch).
The Importance of Counseling Skills in Their Roleas a Genetic Counselor/Geneticist
All respondents considered counseling skills to be vital in supporting clients“when (they are) making difficult decisions about their cancer history.” We consid-ered the views of geneticists and genetic counselors separately. The average dis-tance from the anchor which emphasized counseling on the 10-cm LASA line was4.1cm for clinical geneticists (n = 7) and 3.8 cm for genetic counselors (n = 22).These scores indicate a tendency toward a counseling approach as opposed to a
P1: GDW/GDB
Journal of Genetic Counseling [jgc] PH021-296948 February 4, 2001 12:25 Style file version Nov. 19th, 1999
194 Lobb, Butow, Meiser, Tucker, and Barratt
problem-solving approach (where equal emphasis on both would have received ascore of 5). In response to this question, one geneticist said,
The fundamental issue in cancer genetic counseling is mortality, and this must be placed inthe context of a person’s values and personal philosophy. The “reductionist” view B missesthe core of this human interaction; the risk and so forth could be provided by a computer.(Clinical Geneticist)
Another respondent said,
The question (how important are counseling skills) is peculiar—how important is breathing.(Genetic Counselor)
However, the majority of respondents determined that “both views are equallyimportant and deserve equal weight if the consultation is to be effective” (ClinicalGeneticist).
Other essential components of genetic counseling identified in this survey,were to understand and listen to the consultand, to empathize with and empowerher, and to recognize issues and to help her work through these issues. Addressingclients’ needs and concerns was seen as important in building trust, rapport, andlowering anxiety and was seen to play a strong role in creating a more suitableenvironment for discussing the more complex issues of genetics, genetic testing,and personal risk. As one geneticist said,
The genetic counseling session is 10% facts and 90% support. (Clinical Geneticist)
Again, just as giving individualized information was seen to be important,the role of counseling was similarly qualified.
In general, counseling skills are important, however, it is really dependent on the individual’scircumstances (i.e., perception of risk, unresolved grief issues due to death of relativesetc.). Some women need information only, whereas others require a great deal of emotionalsupport. (Genetic Counselor)
One geneticist highlighted the importance of working in a multi-disciplinaryteam saying,
I am not trained in counseling, and I rely on members of my team to fill that vital role.(Clinical Geneticist)
Likewise, acknowledging the mutuality of roles, one genetic counselor said,
I define genetic counseling as a discussion which focuses on the woman’s concerns withrespect to inheritance, risk, testing, and family/personal issues related to the presence ofbreast cancer in the family (other concerns such as screening and preventative behavioursare more appropriately addressed by medical staff in clinic). (Genetic Counselor)
The practical difficulties of time restraints and workload were also noted byrespondents:
Although addressing problems through counseling is very important, issues cannot al-ways be solved within the genetic counseling time frame. Discussion must empower

P1: GDW/GDB
Journal of Genetic Counseling [jgc] PH021-296948 February 4, 2001 12:25 Style file version Nov. 19th, 1999
How Do Geneticists and Genetic Counselors Counsel Women? 195
the individual even after their genetic counseling sessions are complete. (GeneticCounselor)
Comparison Between Responses From Clinical Geneticistsand Genetic Counselors
Generally, there was little difference in the responses given by clinical ge-neticists and genetic counselors. Both groups were in agreement on the key goalsand aims of genetic counselling, the information to be given at the first session,and why women come for genetic counseling. However, four items received lowercitations from clinical geneticists than from genetic counselors. These included,“recording and verifying family history” (3 citations from clinical geneticists outof a reported 10–17 citations); “assistance in decision making” (1 citation out of10–17 citations); “exploring the potential impact of genetic testing on the woman”(2 out of 5–10 citations), and “exploring issues related to personal/family history”(2 out of 5–10 citations). Similarly, 1 clinical geneticist (out of 10–19 responses)cited to “discuss family history/tell her story” as a reason women attend geneticcounseling. An area that was cited by clinical geneticists and not genetic coun-selors was “answering questions about hormone replacement therapy and the oralcontraceptive pill.”
DISCUSSION
This was a qualitative survey designed to identify the range of views clinicalgeneticists and genetic counselors hold about their consultations with women fromhigh-risk breast cancer families by open-ended questioning. An absence or a lowcitation of particular items does not necessarily indicate that they are consideredto be of low importance. It should also be noted that what geneticists and geneticcounselors say is important and what they actually do and say during the geneticcounseling session may be different. The current study is unable to elucidatethis question. However, in the related study referred to in the introduction, wehave audio-taped, transcribed, and coded 160 genetic counseling sessions whichare currently being analyzed and these data will allow us to examine this issue.Nevertheless, the current data does raise some useful issues that might be furtherexplored using a quantitative methodology.
In general, the results of this survey indicate that genetic counselors andclinical geneticists in Australia align their practice closely to “The National BestPractice Guidelines for Familial Cancer Clinics” produced by the National BreastCancer Center in Australia. These guidelines recommend that
a familial cancer clinic for breast cancer should provide a comprehensive service for womenwho seek advice because they are either at high risk or believe they may be at high risk of de-veloping breast cancer. This includes risk assessment, genetic counseling, advice regardingcancer prevention/early detection and the offer of genetic testing if appropriate.

P1: GDW/GDB
Journal of Genetic Counseling [jgc] PH021-296948 February 4, 2001 12:25 Style file version Nov. 19th, 1999
196 Lobb, Butow, Meiser, Tucker, and Barratt
It is not surprising that the provision of information and reassurance wereboth identified by respondents as key elements in the genetic counseling encounter.Indeed when given the opportunity to weigh one against the other, most respon-dents placed themselves close to the middle. Michieet al. (1997) reported thatof 131 women attending genetic counseling, 79% expected to receive informa-tion, and 50% expected to receive reassurance. Indeed, many respondents stronglyemphasized that risk figures could not be given in isolation, without a precedingdiscussion of the woman’s previous experience with cancer, and the implicationsrisk figures might hold for her. Even further, some respondents felt that the riskdiscussion was often a secondary goal of genetic counseling, with reassurance andsupport having priority.
Respondents used a rich array of words to describe the attributes they felt ge-netic counselors should display, including being “honest and open, nonjudgmental,confidential, compassionate, sensitive and client-focussed.” They also believed thatcoping skills, social support, and psychosocial needs should be assessed and ad-dressed. These goals reflect the unique nature of cancer genetic counseling, whichdeals with a population whose family histories usually carry an enormous cancerburden with accompanying psychological consequences. Given that not all geneti-cists and genetic counselors have had formal psychological training, such high ex-pectations of the service they should offer may lead to burnout. This may also pointto a need for communication skills training for geneticists and genetic counselingto help them deal effectively with the specific psychosocial issues raised in geneticcounseling. Such training is currently being undertaken and evaluated in Australia.
Some writers have suggested that, given the current limitations of genetictesting, and in particular the high possibility of a noninformative result, genetictesting should not be offered at all (Cunningham-Burley and Boulton, 1999). Thisgroup of Australian geneticists and genetic counselors appeared keenly aware ofthese limitations, and frequently cited the need to discuss the disadvantages oftesting and the impact that genetic testing may have on the woman and her family.Information on the legal issues surrounding genetic testing, obtaining informedconsent for genetic testing, and implications for insurance were also mentioned bysome respondents. Indeed, many respondents favored client autonomy, rather thana paternalistic approach where the counselor makes the decision not to presentinformation at all. The importance of personal choice, of taking time to decideabout testing, and the availability of on-going support from the clinic during thistime were mentioned.
It is perhaps not surprising that general information relating to breast can-cer, including risk factors, previous treatment, and possible recurrence was notidentified either as a reason women came for genetic counseling or informationthat would be given to them. It would be assumed that women who are affectedwith breast cancer and attending for genetic counseling would have received thisinformation from their medical/radiation oncologist or surgeon.
P1: GDW/GDB
Journal of Genetic Counseling [jgc] PH021-296948 February 4, 2001 12:25 Style file version Nov. 19th, 1999
How Do Geneticists and Genetic Counselors Counsel Women? 197
Despite the fact that provision of individualized care was the single mostcommonly cited goal of genetic counseling, few respondents mentioned specificcommunication strategies to achieve this end. Such strategies might include inves-tigating the woman’s personal agenda for attending genetic counseling, assessingher current level of understanding of breast cancer genetics and genetic testing,asking her preference for involvement in decision making, eliciting her preferredformat for risk communication, and providing written information. As this was aqualitative study with open-ended questions, it is hard to assess the implicationsof low citations. It may be that clinicians felt these strategies were implicit or self-evident, and therefore did not mention them. Alternatively, perhaps such strategiesmay not be given high priority. If the latter explanation is true, then there is poten-tial for improving practice in this area. Other recent studies have highlighted theimportance of accurately assessing individual women’s expectations and needs.
A recent U.K. study documented the consultand’s agenda at the genetic clinic,and explored whether geneticists recognized that agenda (Shankaret al., 1999).The authors found statistically significant differences between consultands andgeneticists’ ratings of the importance of an issue. For example 90% of consultandsconsidered written information important compared to only 70% of geneticists.This study highlighted the usefulness of asking the consultand exactly what infor-mation they would like, and in what format.
Similarly, in a recent study, women attending a familial breast cancer clinicin the United Kingdom, gave personal risk, awareness of family history, risk tofamily members, reassurance, genetic testing, breast screening, and prevention astheir main reasons for attending (Brainet al., 2000). These women were comparedon demographic and medical variables, and on psychological variables includinggeneral anxiety, cancer worry, perceived risk, and attitudes toward prophylacticsurgery and genetic testing. Important differences in the psychological character-istics of these groups were found, which were unrelated to the reported familyhistory. In particular, women who primarily wanted genetic testing felt extremelyvulnerable to developing breast cancer, were more likely to be considering pro-phylactic surgery, and perceived fewer limitations of testing. Those women whoprimarily wanted reassurance were highly anxious about the disease. These resultshighlight the utility of determining women’s expectations at the beginning of acancer genetics consultation.
The key role of screening strategies in the management of familial breastcancer risk is highlighted in this study, with a management plan and the discussionof future screening options mentioned even more frequently than genetic testingor risk communication. It is difficult to determine if the low citation of discussionabout prophylactic mastectomy or oophorectomy is meaningful; it may well bethat respondents placed this option under the more general heading of “screen-ing/preventative management.” However, it could be of concern if women want toconsider this option for future risk management and it is not raised for discussion.
P1: GDW/GDB
Journal of Genetic Counseling [jgc] PH021-296948 February 4, 2001 12:25 Style file version Nov. 19th, 1999
198 Lobb, Butow, Meiser, Tucker, and Barratt
Differences in responses between clinical geneticists and genetic counselorsmay be explained by differences in individual clinic practices. For example, in themajority of cancer genetic clinics, gathering information and verifying the familyhistory is usually done by the genetic counselor prior to the clinic appointment.In some clinics, the session is conducted by the genetic counselor and the clinicalgeneticist is brought into the consultation to either give a risk assessment or answerspecific questions. This may explain the low citation given to responding to issuesrelating to the woman’s personal or family history of breast cancer and discussingthe impact of genetic testing, as it may be assumed these issues had been coveredpreviously in the consultation. Assistance with decision making again may reflectthe directive versus nondirective argument in genetic counseling.
Future research could usefully explore the issues raised in this paper further,using quantitative methodology.
ACKNOWLEDGMENT
This research is supported by a University of Sydney Cancer Research FundGrant.
REFERENCES
Andrews LB, Fullarton JE, Holtzman NA, Motulsky, AG (1994) Personal issues in human genetics. In:Assessing Genetic Risks: Implications for Health and Social Policy. Washington, DC: NationalAcademy Press, pp 202–233.
Beisecker BB, Marteau TM (1999) The future of genetic counseling: An international perspective.Nature Genet22:133–137.
Brain K, Gray J, Norman P, Parsons E, Clarke A, Rogers C, Mansel R, Harper P (2000) Why do womenattend familial breast cancer clinics?J Med Genet37:197–202.
Cunningham-Burley S, Boulton M (1999) The social context of the new genetics. In:Handbook ofSocial Studies in Health & Medicine. London: Sage, pp 174–186.
Easton DF (1997) Breast cancer genes—What are the real risks?Nature Genet16:210–211.Farnish S (1988) A developing role in genetic counseling.J Med Genet25:392–395.Glaser BG, Strauss A (1967)The Discovery of Grounded Theory: Strategies for Qualitative Research.
Chicago: Aldine.Hall JM, Lee MK, Newman B, Morrow JE, Anderson LA, Huey B, King, MC (1990) Linkage of
early-onset familial breast cancer to chromosome 17q21.Science250:1684–1689.Harris R (1998) Genetic counseling and testing in Europe.J.R. Coll. Physicians Lond. 32:335–338.Kenen RH, Smith ACM (1995) Genetic counseling for the next 25 years: Models for the future.J Genet
Couns4:115–124.Kessler S (1992) Process issues in genetic counseling. In:Psychosocial Aspects of Genetic Counseling.
NY: Wiley-Liss, pp 1–10.Kessler S (1997) Psychological aspects of genetic counseling. IX: Teaching and counseling.J Genet
Couns6:287–295Kirk J, Tucker K (1997) National Breast Cancer Centre National Best Practice Guidelines for Familial
Cancer Clinics. Sydney: National Health & Medical Research Council’s National Breast CancerCentre.
Lucassen AM, Houlston R (2000) Clinical geneticists’ attitudes and practice towards testing for breastcancer susceptibility.J Med Genet37:157–160.

P1: GDW/GDB
Journal of Genetic Counseling [jgc] PH021-296948 February 4, 2001 12:25 Style file version Nov. 19th, 1999
How Do Geneticists and Genetic Counselors Counsel Women? 199
Michie S, Allanson A, Armstrong D, Weinman J, Bobrow M, Marteau TM (1998) Objectives of geneticcounseling: Differing views of purchasers, providers and users.J Pub Health Med20:404–408.
Michie S, McDonald V, Marteau TM (1997) Genetic counseling: Information given, recall and satis-faction.Patient Edu Couns32:101–106.
Michie S, Smith JA, Heaversedge J, Read S (1999) Genetic counseling: Clinical geneticists’ views.J Genet Couns8:275–287.
Miki Y, Swensen J, Sharruck-Eidens D (1994) A strong candidate for the breast and ovarian cancersusceptibility gene BRCA1.Science266:1885–1892.
National Health and Medical Research Council (1999, November)Familial Aspects of Cancer: A Guideto Clinical Practice. Canberra: National Health and Medical Research Council.
Richards L (1998)QSR NUD*IST—Non-Numerical Unstructured Data*Indexing Searching and The-orising. Qualitative Solutions and Research Pty. Ltd.
Shankar A, Chapman P, Goodship, J (1999) Genetic counseling: Do we recognise and meet consultands’agendas?J Med Genet36:580–582.
Skirton H (1999) Genetic nurses and counselors—preparation for practice with families at risk offamilial cancer.Dis Markers15: 145–147.
Skirton H, Barnes C, Walford-Moore J (1997) The role and practice of the genetic nurse: Report of theAGNC Working Party.J Med Genet34: 141–147.
Struewing, JP, Hartge P, Wacholder S, Baker SM, Berlin M, McAdams M, Timmerman M, LawrenceBS, Brody C, Tucker MA (1997) The risk of cancer associated with specific mutations of BRCA1and BRCA2 among Ashkenazi JewsNEJM335:1401–1408.
Wooster R, Neuhausen SL, Mangion J, Quirk Y, Ford D, Collins N (1994) Localisation of a breastcancer susceptibility gene BRCA2, to chromosome 13q12–13.Science265:2088–2090.
Wooster R, Bignell G, Lancaster J, Swift S, Seal S, Mangion J (1995) Identification of the breast cancersusceptibility gene BRCA2.Nature378:789–792.