how data can improve health care what we don’t know can hurt us
DESCRIPTION
How data can improve health care What we don’t know can hurt us. Gov 2.0 September 10, 2009 Elliott Fisher, MD, MPH Director, Population Health and Policy The Dartmouth Institute for Health Policy and Clinical Practice. The current conundrum. Rising costs a serious threat - PowerPoint PPT PresentationTRANSCRIPT

How data can improve health careWhat we don’t know can hurt us
Gov 2.0
September 10, 2009Elliott Fisher, MD, MPHDirector, Population Health and PolicyThe Dartmouth Institute for Health Policy and Clinical Practice
11

The current conundrum
Rising costs a serious threatMedicare Trust Fund – runs dry 2017
Cost of family coverage projected to double ($12,298 to $23,842 by 2020)
Two million Americans affected by medical bankruptcy each year
BarriersFear of rationing, of change, that lower cost = lower quality
Ignorance of where the money’s going in health careof how to do better
Data can help: four examplesRegional variations in spending and quality: where’s the waste?
Identifying high-performing systems -- from whom we can learn
Supporting change in clinical practice
Motivating change in health systems

Per-capita Medicare SpendingTrends: 1992 to 2006
Miami 5.0
Salem, OR 2.3
E. Long Island 4.0
Boston 3.0San Francisco 2.4
Annual GrowthRate
Source: Slowing the Growth of Health Care Spending: Lessons from Regional Variation. Fisher, Skinner, Bynum, New England Journal of Medicine, February 26, 2009
US Avg 3.5
33

What does higher spending buy?(1) Fisher et al. Ann Intern Med: 2003; 138: 273-298 (2) Baicker et al. Health Affairs web exclusives, October 7, 2004(3) Fisher et al. Health Affairs, web exclusives, Nov 16, 2005(4) Skinner et al. Health Affairs web exclusives, Feb 7, 2006(5) Sirovich et al Ann Intern Med: 2006; 144: 641-649(6) Fowler et al. JAMA: 299: 2406-2412
Not better care orbetter outcomes
44
More “supply-sensitive services”

Lack of support for improvement, care management and coordination.
Local organizational support: Develop virtual or real integrated systems to support practice.
Payment system that rewards morecare, increased capacity, high margintreatments, entrepreneurial behavior.
Payment reform: foster accountability for capacity – and behavior: capitation or global shared savings.
Underlying problem Key principles
Moving forwardAddressing the underlying causes of rising costs, poor quality
55
Failure to recognize role of localsystem (e.g. capacity) as cost-driver.
Local accountability: Fosteraccountability for total costs – and capacity at local level.
Assumption that more is better.Equating less care with rationing.
Measurement: Comprehensive performance measures: outcomes, patient experience.

Data on regional performanceMarked variations highlight opportunities to improve
66
Everett, WASacramento, CALa Crosse, WICedar Rapids, IATemple, TX
Portland, MESayre, PARichmond, VAAsheville, NCTallahassee, FL
“How do they do that?”conference
Lighter colors = lower spending
Partici-pants
Qualifying Regions
All Others
Medicare Spending
$6,773 $7,098 $8,562
Hospital Days
1.52 1.56 1.90
Spending for Imaging(last 2 yrs)
$633 $662 $843
Hospital Quality Score
95% 95% 93%

Benchmarks of efficiencyPotential savings from achieving high performance
77
Everett, WASacramento, CALa Crosse, WICedar Rapids, IATemple, TX
Portland, MESayre, PARichmond, VAAsheville, NCTallahassee, FL
Category of Care
Potential Savings
Medicare spending
16%
Hospital days 17%
Specialist visits 36%
“How do they do that?”conference
Lighter colors = lower spending

How do they do that?Some preliminary insights
Common elements across regionsShared aims; “accountable” to the community;
Physician engagement as leaders; support for professional values
Strong primary care foundation
Use of data to support work; professional feedback; peer review
Data feedback – a critical componentOrganizational accountability – integrated systems to support feedback
Data itself – actual performance of providers

Data to improve qualitySupport for process management
Ch 7. BC James, JS Lazar. A health system’s use of clinical programs to build quality infrastructure. In: Practice-Based Learning and Improvement Second Edition. EC Nelson, PB Batalden, JS Lazar, Eds.
Intermountain Health Care
Focus on managing defined clinical populations
Care pathways defined by multi-disciplinary team
Protocols implemented through EHR with process, outcome tracking and feedback
Scientific review / updating on monthly basis.

Data to address variationsPartners Healthcare
Stafford RS Am J Heart 2003, 145:979-85.
Physician level (n = 117) Low: 0.0% High: 24.6%
Practice level (n = 10) Low: 1.0% High: 8.1%
Baseline variation in ordering
Impact of Individualized Feedback and Education.

Data to address variationsPartners Healthcare
May 29, 2008 Presentation at Federal Trade CommissionTom Lee, MD (Partners Healthcare System) (with permission)
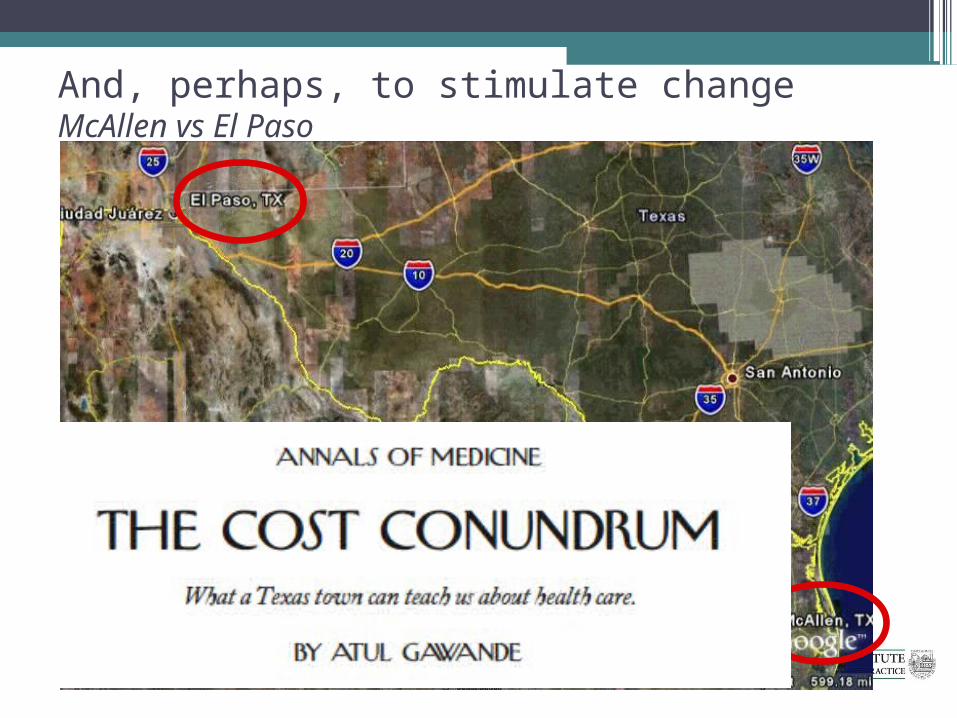
And, perhaps, to stimulate changeMcAllen vs El Paso