how cancer programs are responding to covid-19 and
TRANSCRIPT

Presented by
Service Line Strategy Advisor
How cancer programs are responding to COVID-19 and planning for future market trends

© 2020 Advisory Board • All rights reserved • advisory.com
‹#›
Road mapRoad map2
How cancer programs are responding to COVID-19 1
2 Growth outlook for oncology services
3 Key trends and imperatives for the oncology service line

© 2020 Advisory Board • All rights reserved • advisory.com
3
Tracking the spread
Jan 11, 2020
Chinese government
reports first death
due to new virus that
began spreading in
late 2019
Jan 13, 2020
The first case
outside of China
is confirmed in
Thailand
Jan 30, 2020
WHO declares global
emergency
Cases reported in Japan,
South Korea, India, the
Philippines
Jan 31, 2020
Russia, Spain, Sweden,
UK confirm first cases
9,800 reported cases, 213
deaths worldwide
Feb 14-21, 2020
First cases reported
in Egypt, Iran, Israel
as the virus spreads
to the Middle East
Feb 1, 2020
Cases reported in
Australia, Canada,
Germany, Singapore,
the UAE, the US,
Vietnam
Feb 28, 2020
Nigeria, Lithuania, Wales
report first cases
The US reports its first death,
near Seattle
Feb 24-27
Kuwait, Bahrain, Iraq,
Afghanistan, Oman, Brazil,
Norway, Romania, Greece,
Georgia, Pakistan, North
Macedonia report cases
Mar 24, 2020
>392,000
reported cases,
>17,000 deaths
worldwide
Two months after the first reported death, COVID-19 circled the globe
Advisory Board interviews and analysis.
Source: “A Timeline of the Coronavirus,” The New York Times, March 4th, 2020.

© 2020 Advisory Board • All rights reserved • advisory.com
4
Coronavirus cases in the United States
96 million cases
4.8 million hospitalizations
480,000 deaths
Estimate of possible effects
33,404 cases
54 jurisdictions reporting cases
400 deaths
Current COVID-19 cases
6-50 reported cases
51-100 reported cases
101-500 reported cases
Current as of March 23, 2020
Advisory Board interviews and analysis.
Source: “Coronavirus Disease 2019 (COVID-19) in the US,” CDC,
March 11, 2020. “One slide in a leaked presentation for US hospitals
reveals that they’re preparing for millions of hospitalizations as the
outbreak unfolds,” Business Insider, February 27th, 2020.
501-1,000 reported cases
1,001-5,000 reported cases
5,001 or more reported cases

© 2020 Advisory Board • All rights reserved • advisory.com
5
Source: https://www.cms.gov/newsroom/fact-sheets/medicare-telemedicine-health-care-provider-fact-sheet
Protecting cancer patients critically important
Advisory Board interviews and analysis.
Sample strategies to reduce patient and staff risk
• Cancelling in-person events, activities,
meetings
• Encouraging work from home when
possible
• Restricting employee personal travel
• Planning for impending supply
shortages
• Rescheduling non-essential visits
• Fast-tracking injections
• Separating lab and infusion visits
• Encouraging appointments during
extended hours
• Minimizing patient “touches”
• Screening patients before visits
• Implementing rapid triage protocols for
suspected cases
• Restricting entry and number of visitors
• Offering onsite “drive-thru” testing and
testing tents
• Deploying telehealth
CMS broadens access to telehealth for Medicare beneficiaries
• Effective March 6, 2020 for the duration of this emergency, CMS
will reimburse for telehealth visits, virtual check-ins, and e-visits
• Includes all beneficiaries in all settings in all parts of the country
• Allows use of everyday communication technology, such as
FaceTime, Skype
REGISTER NOW
Join our upcoming webinar on How COVID-
19 is transforming telehealth—now and in
the future on Thursday, March 26th at 3pm ET

© 2020 Advisory Board • All rights reserved • advisory.com
6
Make sure patients can easily find the info they need
Advisory Board interviews and analysis.
Read our full take on the
Oncology Rounds, as
well as links to related
ASCO and NCCN
resources
Creating dedicated cancer
program webpages
Sharing in-the-moment updates
through social media
Making eye-catching
in-person signage
• Use webpage to house all
material pertaining to COVID-19,
including updated cancer
program policies and patient
information
• Check out a few examples:
• Seattle Cancer Care
Alliance
• Roswell Park
• MD Anderson
• Winship Cancer Institute
• The University of Kansas
Cancer Center
• GW Cancer Center
• Share constantly-evolving
information and updates through
Facebook, Twitter, and other
social media outlets
• Create short videos for patients
on YouTube
• Create colorful, easy-to-
understand signage in the
cancer center
• Ensure all employees are
equipped to answer patients’
questions and explain changes
in policy as appropriate
• Ensure consistency with website,
email, and hotline information
© 2020 Advisory Board • All rights reserved • advisory.com
7
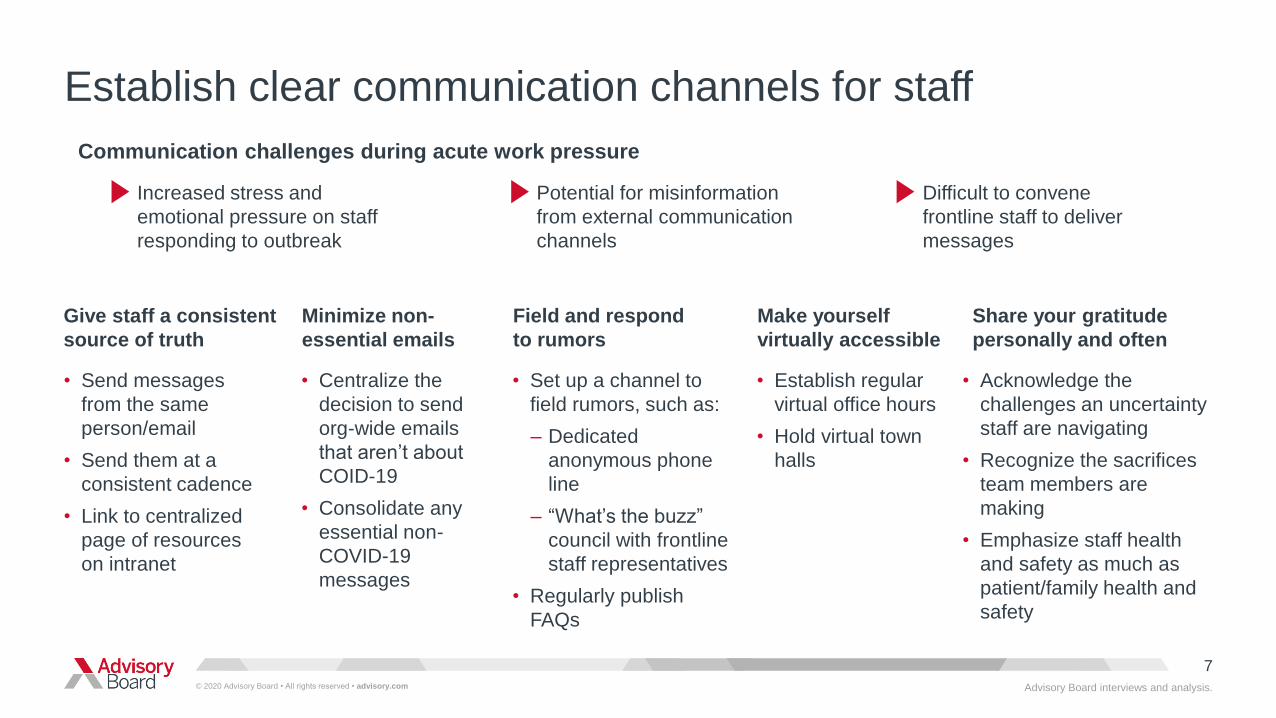
Establish clear communication channels for staff
Communication challenges during acute work pressure
Give staff a consistent
source of truth
• Send messages
from the same
person/email
• Send them at a
consistent cadence
• Link to centralized
page of resources
on intranet
Increased stress and
emotional pressure on staff
responding to outbreak
Potential for misinformation
from external communication
channels
Difficult to convene
frontline staff to deliver
messages
Advisory Board interviews and analysis.
Minimize non-
essential emails
• Centralize the
decision to send
org-wide emails
that aren’t about
COID-19
• Consolidate any
essential non-
COVID-19
messages
Field and respond
to rumors
• Set up a channel to
field rumors, such as:
– Dedicated
anonymous phone
line
– “What’s the buzz”
council with frontline
staff representatives
• Regularly publish
FAQs
Share your gratitude
personally and often
• Acknowledge the
challenges an uncertainty
staff are navigating
• Recognize the sacrifices
team members are
making
• Emphasize staff health
and safety as much as
patient/family health and
safety
Make yourself
virtually accessible
• Establish regular
virtual office hours
• Hold virtual town
halls

© 2020 Advisory Board • All rights reserved • advisory.com
8
How to respond today and how to prepare for the long-term impact
Your top resources for COVID-19 readiness
Advisory Board interviews and analysis.
To access the top COVID-19 resources,
visit advisory.com/covid-19
CDC's health care personnel
preparedness checklist
CDC's hospital preparedness checklist
CDC's COVID-19 case tracker
CDC’s infection prevention and control
recommendations for COVID-19 patients
Links to external resources, such as:
Rebuild the Foundation for a
Resilient Workforce
Anatomy of an Outbreak: COVID-19 and
the U.S. Health Care Delivery System
Managing clinical capacity
Coronavirus scenario planning: 12 situations
hospital leaders should prepare for
Advisory Board resources, such as:

© 2020 Advisory Board • All rights reserved • advisory.com
‹#›
Road mapRoad map9
How cancer programs are responding to COVID-19 1
2 Growth outlook for oncology services
3 Key trends and imperatives for the oncology service line

© 2020 Advisory Board • All rights reserved • advisory.com
10
Lung cancer projected to have highest incidence increase
1. .
Cancer incidence five-year growth projections, by tumor site
Service Line Strategy Advisor research and analysis.
Increase in incidence expected for all cancer types
Source: Advisory Board’s Cancer Incidence Estimator.
13%
11% 11% 11%10%
9%8%
7% 7%
4%
15%
Hematological GI Urologic Melanomas of
the skin
Lung and
bronchus
National estimates, 2018-2023
10% Combined five-year growth
Head and
neck
Brain and
other nervous
system
Breast Gynecologic Thyroid Other

© 2020 Advisory Board • All rights reserved • advisory.com
11
IP medical oncology expected to decrease
1. Includes biopsies from service lines of dermatology, ENT, gastroenterology, general surgery,
gynecology, orthopedics, thoracic surgery, and urology.
2. Positron emission tomography.
3. Inpatient and outpatient surgery service utilization broken out by skin, urological, GI, gynecological,
prostate, colorectal, hematological, head and neck, thoracic, breast, neurological, and other tumor sites.
Outpatient, inpatient oncology service volume growth
Service Line Strategy Advisor research and analysis.
OP service volumes also expected to increase, led by surgery
Source: Advisory Board’s Oncology Market Estimator.
22%
14%
10%
3% 3%
9%
2%
27%
3%
-4%
National estimates, 2018-2023
11% Combined five-year growth
Inpatient
Outpatient
OP radiation
therapy
OP
chemotherapy
IP medical
oncology
Overall IP
surgery3
Overall OP
surgery3
Biopsy1 Colonoscopy MammographyBreast
ultrasound
PET2
Screening/diagnostics

© 2020 Advisory Board • All rights reserved • advisory.com
12
Expect decline in IP surgeries for most tumor sites
Outpatient, inpatient cancer surgery volume growth, by tumor site
Service Line Strategy Advisor research and analysis.
Growth expected across the board for OP surgeries
Source: Advisory Board’s Oncology Market Estimator..
31% 29%
24% 23%
15%
11% 11% 10% 9%
4%2%
9%
-10% -11%
-4%
11%
-8% -7%
-2%
7%
13%
Urological
(non-prostate)GI (non-
colorectal)
Gynecological ProstateSkin
National estimates, 2018-2023
26% Combined five-year growth
Colorectal Hematological Head and
neck
Thoracic Breast
Outpatient
Inpatient
Neurological1
1. There is no growth projection for outpatient neurological cancer surgery volumes because
neurological cancer surgeries are performed in the inpatient setting, so there are no baseline
outpatient neurological cancer surgery volumes from which growth can be projected.

© 2020 Advisory Board • All rights reserved • advisory.com
13
Source: Advisory Board’s Market Scenario Planner..
Technology top detractor from OP utilization, care management from IP utilization
Aging population is biggest growth driver across care settings
Service Line Strategy Advisor research and analysis.
Outpatient1, inpatient2 oncology growth drivers
Outpatient
National estimates, 2018-2023
Inpatient
+3.5%+3.5%
+3.7%
-9.3%
-3.0%
-1.7%
-6.2%+0.0%
-2.9%+5.2%
+1.8%
+2.5%
+3.5%
+0.0% +0.0% +3.9%
1. Outpatient chemotherapy and radiation therapy.
2. Inpatient medical/hematology oncology and radiation oncology.

© 2020 Advisory Board • All rights reserved • advisory.com
‹#›
Road mapRoad map14
How cancer programs are responding to COVID-19 1
2 Growth outlook for oncology services
3 Key trends and imperatives for the oncology service line

© 2020 Advisory Board • All rights reserved • advisory.com
15
Three trends impacting the oncology service line
Service Line Strategy Advisor research and analysis.
Cancer care is becoming more complex as patient demographics shift and clinical innovations abound1
Payers’ efforts to control oncology spend directly threaten providers’ growth 3
2 Cancer patients are demanding a seat at the decision-making table

© 2020 Advisory Board • All rights reserved • advisory.com
16
Source: Jemal, A, et al, “The Cancer Atlas,” American Cancer Society, 3 (2019),
www.canceratlas.cancer.org .; “State Chronic Conditions Dashboard,” CMS, 2019. https://cms.gov/research-
statistics-data-and-systems/statistics-trends-and-reports/chronic-conditions/ccdashboard.
Caring for an older, more complex, and costly population
Oncology Roundtable interviews and analysis.
Percentage of Medicare cancer patients with comorbidities
2017
Beneficiaries with 4
or more conditions
account for 75% of
total Medicare spend
Increasing comorbidities related
to aging population
• Most older adults diagnosed with
cancer present with at least one other
chronic condition
• Aging population of survivors
drives increasing rate of
cancer-related morbidity
• Screens for risk of comorbidities and
methods to mitigate their effects are
increasingly important
• Cancer patients with comorbidities
incur higher cancer treatment costs
7% 26% 30% 37%
Cancer only 1-2 comorbidities 3-4 comorbidities 5 or more comorbidities
Cancer treatment not only is complicated
by comorbidities, but also can cause them
Cardiotoxicity of chemotherapy is a major
concern and drives the rise of cross-
specialty care (i.e., cardio-oncology)
Trend 1: Cancer care is becoming more complex as patient demographics shift and clinical innovations abound

© 2020 Advisory Board • All rights reserved • advisory.com
17
Influx of new drugs adds to complexity of care
Oncology drugs for 17 different
indications launched in 2018
15
Cancer drugs currently in
late-stage development
> 700
Source: IQVIA, “Global Oncology Trends 2019,” 2019, Iqvia.com/-/media/iqvia/pdfs/institute-reports/global-oncology-trends-2019.pdf.
Of drugs in late-stage development:
• 450 are immunotherapies
• 98 are cell, gene, or nucleotide therapies
Over half of new therapies have orphan
drug indication, are delivered orally, or
include a predictive biomarker on their label
Service Line Strategy Advisor research and analysis.
Drug launches in 2018
Drugs in development
Oncology drugs for 89 different
indications across 23 cancer types
launched between 2014-2018
57Expansion in pipelines of cancer drugs
in late-stage development in 2018
alone, and 63% expansion since 2013
19%Of late-stage R&D dedicated to
oncology by world’s 14 largest
pharmaceutical companies
1/3
Of drugs approved in
2018 were personalized
40%Of current clinical
trials use biomarkers
>1/3

© 2020 Advisory Board • All rights reserved • advisory.com
18
Plan to manage more complex patients and more complex treatment
Prepare your care team for increasing complexity of care
Service Line Strategy Advisor research and analysis.
Key imperative 1
Provide coordinated, multidisciplinary care
Grow cross-service line specialties (e.g., cardio-oncology, geriatric oncology)
Improve transitions back to primary care
Equip the care team to adopt treatment innovations
Include new expertise on the care team (e.g., molecular scientists, bioethicists, data managers)
Provide training and support to help physicians implement and stay up to date on clinical innovations
Provide comprehensive education and support to patients
Account for increased physician and nurse time needed to manage patients receiving complex therapies
Develop a principled approach to prioritize between investments in clinical innovations
© 2020 Advisory Board • All rights reserved • advisory.com
19
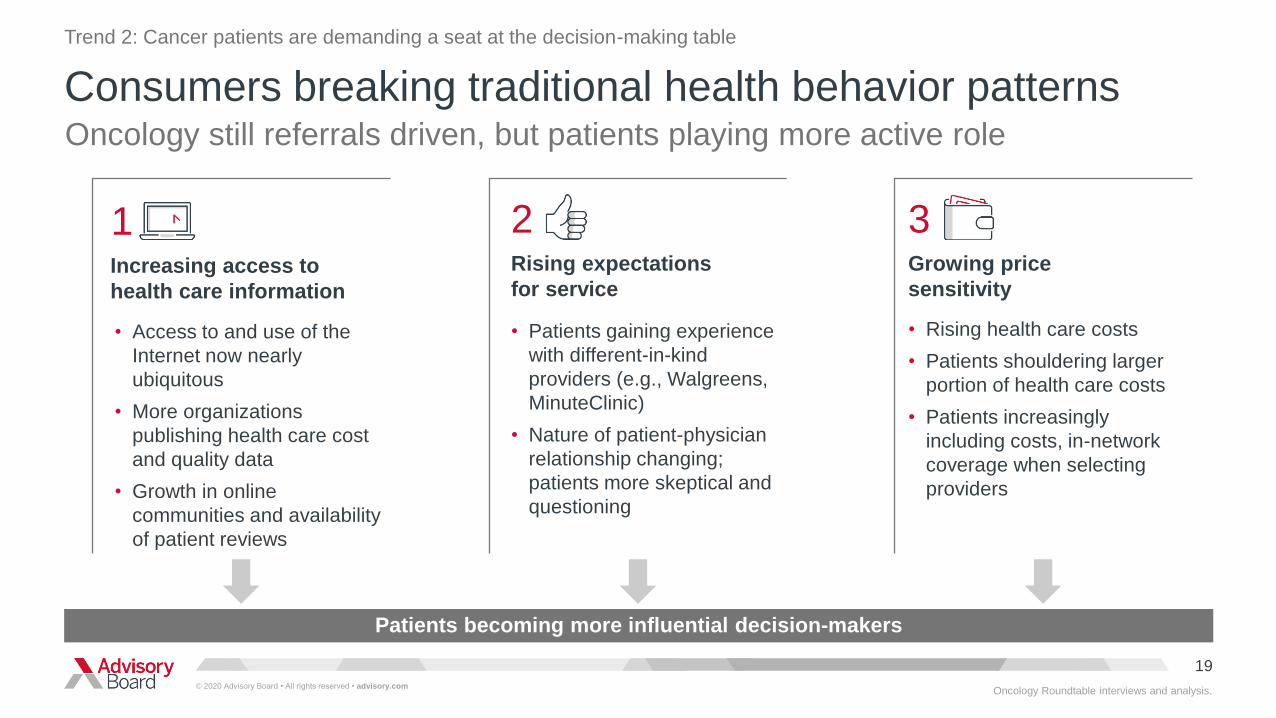
Consumers breaking traditional health behavior patterns
Patients becoming more influential decision-makers
Increasing access to
health care information
1
• Access to and use of the
Internet now nearly
ubiquitous
• More organizations
publishing health care cost
and quality data
• Growth in online
communities and availability
of patient reviews
Rising expectations
for service
2
• Patients gaining experience
with different-in-kind
providers (e.g., Walgreens,
MinuteClinic)
• Nature of patient-physician
relationship changing;
patients more skeptical and
questioning
Growing price
sensitivity
3
• Rising health care costs
• Patients shouldering larger
portion of health care costs
• Patients increasingly
including costs, in-network
coverage when selecting
providers
Oncology still referrals driven, but patients playing more active role
Trend 2: Cancer patients are demanding a seat at the decision-making table
Oncology Roundtable interviews and analysis.

© 2020 Advisory Board • All rights reserved • advisory.com
20
0.8
1.4
1.6
2.9
3.1
3.4
4.8
4.9
5.5
6.5
10.8
11.1
12.3
13.3
17.5
Source: 2019 Cancer Patient Experience Survey.
Clinical quality is king
Oncology Roundtable interviews and analysis.
Doctor who specializes in my particular cancer
Technology and treatment options
Clinical quality (e.g., survival rates)
In-network for my insurance
Accreditation (e.g., Commission on Cancer)
Patient support services
Costs I’m responsible for
Reputation (e.g. US News “top doctors” report)
When deciding where to go for care, which feature is most and least important to you?
n=1,201 cancer patients
Recommendation from my doctor
Recommendation from my family and friends
Location
Availability of appointments
Facility and amenities
Customer service
Availability of clinical trials
Mean utility scores
Did you know?
“Doctor who specializes in my particular cancer”
ranked as the most important factor in both our
2015 and 2019 surveys. In 2015, 43% of patient
ranked it #1. In 2019, that increased to 52%.

© 2020 Advisory Board • All rights reserved • advisory.com
21
The internet is a key source of information for patients
Cancer patients doing their research
Oncology Roundtable interviews and analysis.
3%
3%
3%
4%
4%
5%
7%
12%
15%
19%
23%
33%
34%
81%
Other
Community website, forum, or blog
Employee health navigation site
General ratings website
I did not consult any resources
Social media website
Medicare or other government website
Medical-focused ratings website
Major search engine
Cancer-specific website
Family, friends, or colleagues
My health insurance company
Cancer center, physician practice website
My doctor
Which of the following resources did you use when deciding where to go for your cancer care?
n=1,201 cancer patients
of cancer patients searched online
when deciding where to go for care
48%
average number of sites consulted
by patients searching online
2.1
Source: 2019 Cancer Patient Experience Survey.
© 2020 Advisory Board • All rights reserved • advisory.com
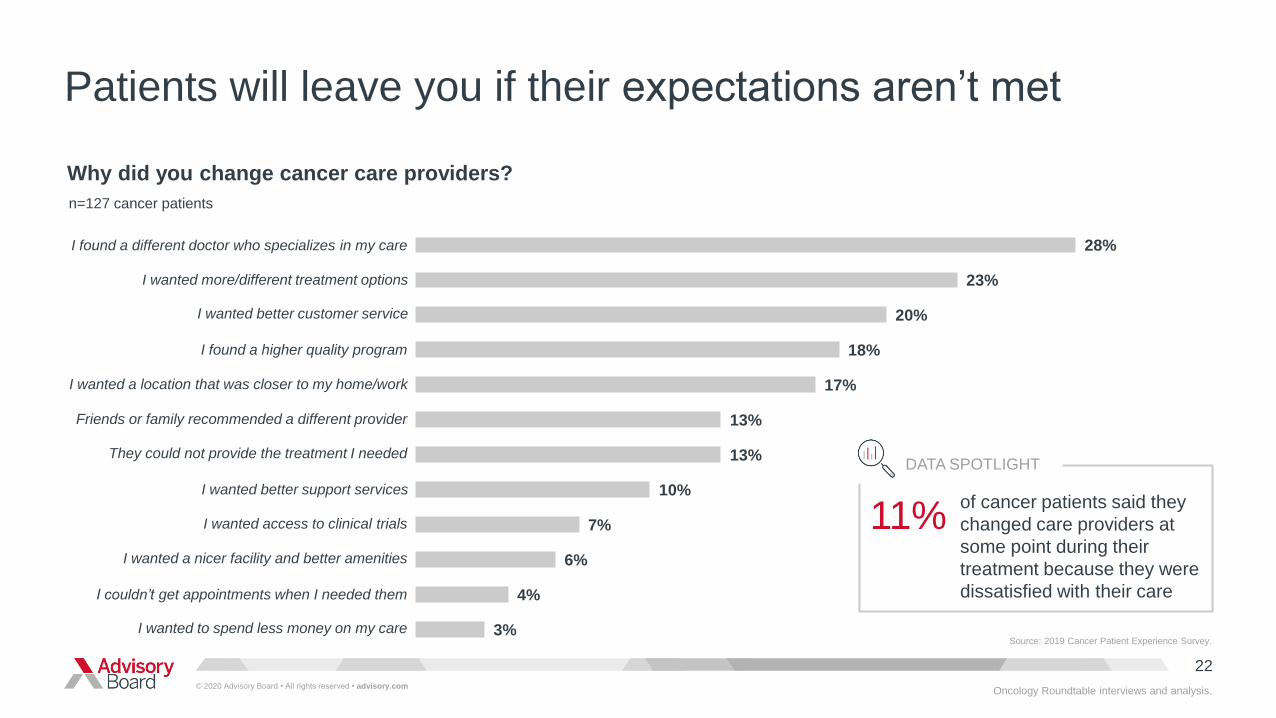
22
Patients will leave you if their expectations aren’t met
3%
4%
6%
7%
10%
13%
13%
17%
18%
20%
23%
28%
Why did you change cancer care providers?
n=127 cancer patients
I found a different doctor who specializes in my care
I wanted more/different treatment options
I found a higher quality program
I wanted a location that was closer to my home/work
They could not provide the treatment I needed
Friends or family recommended a different provider
I wanted better support services
I wanted better customer service
I wanted access to clinical trials
I wanted a nicer facility and better amenities
I couldn’t get appointments when I needed them
I wanted to spend less money on my care
DATA SPOTLIGHT
of cancer patients said they
changed care providers at
some point during their
treatment because they were
dissatisfied with their care
11%
Oncology Roundtable interviews and analysis.
Source: 2019 Cancer Patient Experience Survey.

© 2020 Advisory Board • All rights reserved • advisory.com
23
Convenience and coordination is of the utmost importance
Oncology Roundtable interviews and analysis.
Source: 2019 Cancer Patient Experience Survey.1.52.1
2.3
2.3
3.0
3.3
3.5
3.5
4.4
4.5
4.6
5.4
5.9
6.7
7.1
9.0
9.2
10.9
11.0
All of my care takes place in one building
Specialized symptom management
Multidisciplinary care clinics
Nurse phone line for help with symptoms
Survivor support services after finishing treatment
Patient education services
Help scheduling and coordinating my appointments
Support services for my family
Online portal to view test results, contact care team
Help with nutrition
Extended hours of operation
Complementary and alternative medicine
Access to genetic testing and counseling
Parking that is convenient and affordable
Free or discounted transportation
One point of contact to help me understand my care
Financial counseling
Social and mental health services during treatment
Religious and spiritual services
Which services would have been most valuable and least valuable to you?
Mean utility scores
n=1,201 cancer patients

© 2020 Advisory Board • All rights reserved • advisory.com
24
Cancer patients want to be involved in care decisions
Oncology Roundtable interviews and analysis.
Source: 2019 Cancer Patient Experience Survey.
3%
38%
50%
7%2%
I make the decisionswith little or no input
from my doctor
I make the decisionsafter seriously
considering my doctor'sopinion
My doctor and I makethe decisions together
My doctor makes thedecisions after
seriously consideringmy opinion
My doctor makes thedecisions with little or
no input from me
What is your preferred level of control when making decisions about your cancer treatment?
n=1,201 cancer patients

© 2020 Advisory Board • All rights reserved • advisory.com
25
Invest in services that cancer patients value most
Service Line Strategy Advisor research and analysis.
Key imperative 2
Design a patient-centered and convenient care experience to retain cancer patients throughout treatment
Offer specialized symptom management, co-located services, multidisciplinary clinics, and one point of
contact to help patients understand care
Engage patients in treatment decisions
Promote clinical quality online and strengthen referring provider relationships to attract cancer patients
Understand which quality measures and proxies for clinical quality are most meaningful to patients and
promote these on the cancer center’s website
Make the cancer center’s website easy to find and navigate
Understand what referring physicians are looking for in a cancer provider and craft a compelling message that
speaks to their needs

© 2020 Advisory Board • All rights reserved • advisory.com
26
Source: 2019 Trending Now In Cancer Care Survey.
Providers agree on reimbursement changes as top threat
Oncology Roundtable research and analysis.
49%48%
40%37%
34%32%
26%25%25%
24%21%21%21%
20%18%
15%13%
9%7%7%
2%
Cost of drugs
Marketplace competition
Physician alignment around services or program goals
Network strategy and integration
Managing staff and physician burnout from oncology field
Cuts to fee-for service reimbursement
Access to capital
Health IT
Quality reporting requirements
Increasing patient consumerism
Increasing expectations and needs of referring physicians
Which of the following are the biggest threats to future cancer program growth at your organization?1
Percentage of respondents that ranked threat in top five, 2019n=124
Reimbursement requirements from payers2
Shifting reimbursement away from fee-for-service to value based care3
Uncertainties in drug pricing reform policies4
Cost of new treatment processes/equipment5
Workforce planning6
Insurance shifting additional costs to patients7
Site-of-care policies issued by private payers8
Shifting drug channels9
Changes in health care coverage10
Shifting patient demographics11
1. Respondents were asked to rank up to five threats.
2. For example, prior authorization.
3. For example, Oncology Care Model, Radiation Oncology Model.
4. For example, 340B, changes to Medicare Part B drug pricing.
5. For example, new LINACS, CAR T-cell therapy.
6. For example, managing staff shortages, retaining
staff, recruiting staff.
7. For example, high-deductible health plans.
8. Only first infusion can be delivered in HOPD setting.
9. For example, PBMs, specialty pharmacies, white bagging.
10. For example, repeal of the individual
mandate, potential expansion of Medicare.
11. For example, having to care for an
older comorbid population.
Trend 3: Payers’ efforts to control oncology spend directly threaten providers’ growth

© 2020 Advisory Board • All rights reserved • advisory.com
27
125
137
151
173
2010 2014 2018
1. All numbers in 2010 US dollars.Source: Mariotto, A. et al, “Projections of the cost of cancer care in the United States: 2010-2020,” J Natl Cancer Inst. 103, no. 2, (2011):117-128.
ncbi.nlm.nih.gov/pubmed/21228314.; “Financial Burden of Cancer Care,” National Cancer Institute, 2019. progressreport.cancer.gov/after/economic_burden..
Oncology Roundtable interviews and analysis.
Estimated US direct cancer care costs
Billions USD1, 2010 - 2020
US cancer care expenditures in the billions–and rising
207A more aggressive
projection, accounting for
increases in the use of
targeted chemotherapies
2020

© 2020 Advisory Board • All rights reserved • advisory.com
28
Rising costs driving purchasers to target cancer spend
Oncology Roundtable interviews and analysis.
1
Drug costs
• Drug pricing reform
• 340B reimbursement
• Prior authorization
• Pathways
2
• Site neutrality
• Site-of-care policies
Site of care
3
Provider choice
• Network design
• Centers of excellence
• Value-based partnerships
Three areas of focus for payers and employers to control costs
© 2020 Advisory Board • All rights reserved • advisory.com
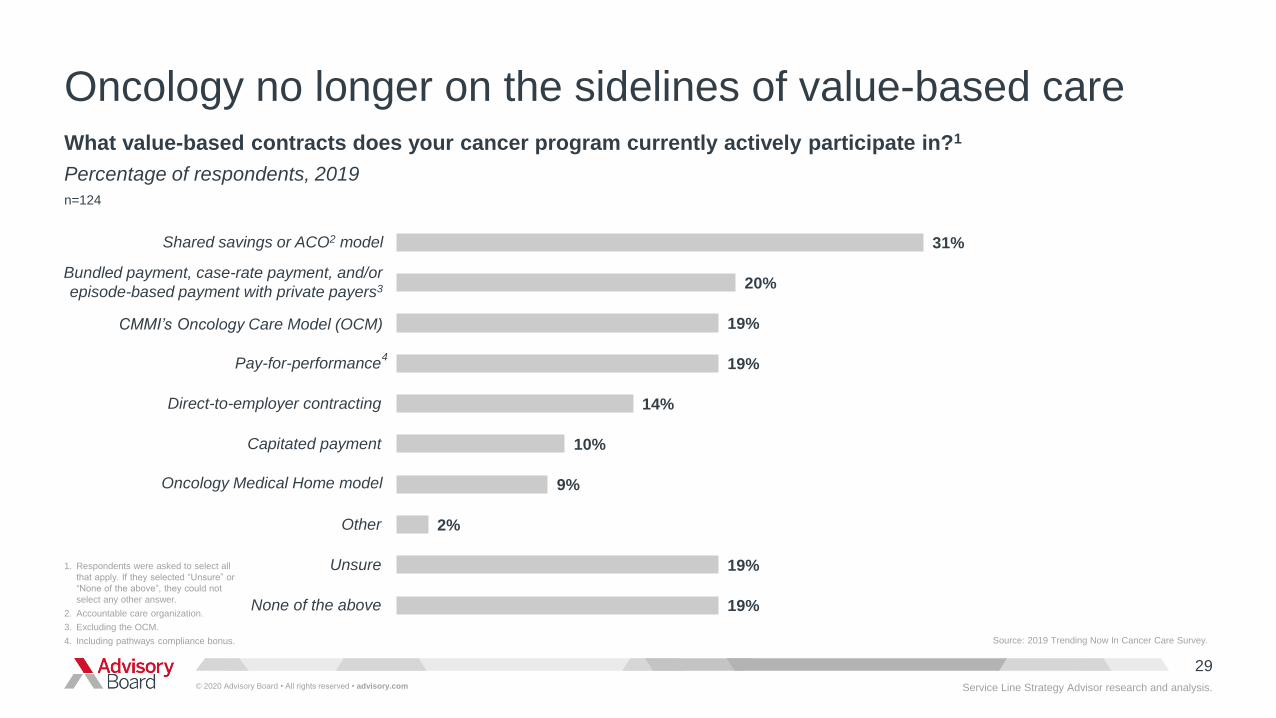
29
1. Respondents were asked to select all
that apply. If they selected “Unsure” or
“None of the above”, they could not
select any other answer.
2. Accountable care organization.
3. Excluding the OCM.
4. Including pathways compliance bonus.
Oncology no longer on the sidelines of value-based care
Service Line Strategy Advisor research and analysis.
What value-based contracts does your cancer program currently actively participate in?1
Percentage of respondents, 2019
n=124
Source: 2019 Trending Now In Cancer Care Survey.
31%
20%
19%
19%
14%
10%
9%
2%
19%
19%
Pay-for-performance
Direct-to-employer contracting
Capitated payment
Other
Unsure
None of the above
Shared savings or ACO2 model
Bundled payment, case-rate payment, and/or
episode-based payment with private payers3
CMMI’s Oncology Care Model (OCM)
Oncology Medical Home model
4

© 2020 Advisory Board • All rights reserved • advisory.com
30
Source: “CMS announces additional opportunities for clinicians to join innovative care approaches under the Quality Payment Program,” Centers for Medicare & Medicaid
Services, https://www.cms.gov/Newsroom/MediaReleaseDatabase/Press-releases/2016-Press-releases-items/2016-10-25.html; “Oncology Care Model Overview,”
Association of Community Cancer Centers, http://oi.accc-cancer.org/advocacy/OCM-Overview.asp; Strawbridge L, ACCC Oncology Care Model Collaborative Workshop
at the ACCC 44th Annual Meeting and Cancer Business Summit, Washington, DC, March 16, 2018; Hubbard A, “RO-APM: What we know, what we don’t and what it all
means,” ASTRO Blog, February 14, 2019, https://www.astro.org/Blog/February-2019/RO-APM-What-we-know,-what-we-don%E2%80%99t-and-what-it-all.
No end in sight for oncology payment reform
Service Line Strategy Advisor research and analysis.
Radiation Oncology Model
Proposed rule released July 2019; final rule
delayed, but expected by July 2022 at the latest
Prospective payment for radiation therapy services
provided to patients with one of 17 included
cancer during a 90-day episode of care subject to
a discount factor of 4% for professional component
and 5% for technical component; participants can
earn back withholds based on clinical data
reporting, quality measure reporting and
performance, and patient experience performance
Mandatory participation for all HOPDs, physician
group practices, and freestanding centers within
randomly selected CBSAs2
Oncology Care First Model
RFI for five-year pilot that would begin in January
2021 after the final OCM episode has started
Prospective monthly population payment that
“bundles” reimbursement for E&M, drug
administration, and seven enhanced services (e.g.,
patient navigation, electronic patient-reported
outcomes) for all medical oncology patients1; total
cost of care accountability for six-month episode with
opportunity to achieve a bonus based on costs and
quality for Part B and D chemotherapy patients only
Optional participation for physician group practices
and HOPDs that are paid under HOPPS
1. This includes patients receiving chemotherapy and hormonal therapy only, along with
patients who are not receiving any cancer-related drugs, such as survivors, who are still
seeing their medical oncologist as part of follow-up care.
2. Core-Based Statistical Areas.

© 2020 Advisory Board • All rights reserved • advisory.com
31
Build an agile organization that can adapt to unexpected reimbursement changes
Put the right infrastructure in place
Service Line Strategy Advisor research and analysis.
Key imperative 3
Take a principled approach to care transformation required to succeed under value-based contracts
Evaluate organizational readiness to adopt value-based contracts; consider organizational leadership and
culture, data analytics capability, and patient access and cross-continuum focus
Prioritize investments that will help you succeed under fee-for-service and value-based contracts, such as
evidence-based care, improved access, symptom management, and data infrastructure
Understand organization’s top opportunities for cost savings
Focus on prevention, informed screening, survivorship, and end-of-life care as levers to reduce total
population costs
Implement no-regret strategies to ensure financial sustainability
Understand financial performance and identify areas for improvement
Refine staffing model and processes in place to manage prior authorization and revenue cycle requirements
Invest in cancer patient financial navigation to improve patient care and revenue capture

© 2020 Advisory Board • All rights reserved • advisory.com
32
Program success hinges on adaptation to shifting landscape
Service Line Strategy Advisor research and analysis.
1
As cancer care becomes more complex, care teams will need new expertise and more training
Caring for more complex patients will require cancer programs to provide well-coordinated multidisciplinary care
delivered by a diverse and culturally competent team, while delivering more complex treatments will require cancer
programs to evaluate new investments to remain competitive, and to provide training, support, and new expertise to
help the core care team implement treatment innovations
3Rapidly changing reimbursement landscape necessitates cancer programs be agile to survive
Start by implementing no-regret strategies to ensure financial sustainability; tackling low-hanging fruit to improve quality
and reduce costs in a value-based world; and designing and optimizing network to manage patients within the system
at the lowest-cost, most appropriate site of care
2Cancer programs must invest in what matters most to patients to contend with increasing consumerism
Attracting patients requires cancer programs to differentiate themselves on quality, strengthen relationships with
referring providers, and develop an online presence; retaining patients requires cancer programs to provide a patient-
centered and convenient care experience

© 2020 Advisory Board • All rights reserved • advisory.com
33
How to respond today and how to prepare for the long-term impact
Your top resources for COVID-19 readiness
Advisory Board interviews and analysis.
To access the top COVID-19 resources,
visit advisory.com/covid-19
Links to external resources, such as:Advisory Board resources, such as:
CDC's hospital preparedness checklist Anatomy of an Outbreak: COVID-19 and
the U.S. Health Care Delivery System
CDC's health care personnel
preparedness checklist
Rebuild the Foundation for a
Resilient Workforce
CDC’s infection prevention and control
recommendations for COVID-19 patients
Coronavirus scenario planning: 12 situations
hospital leaders should prepare for
CDC's COVID-19 case tracker Managing clinical capacity
REGISTER NOW
Webinar on How COVID-19 is transforming telehealth—
now and in the future on Thursday, March 26th at 3pm ET
