house bill 1103 report to the legislature · modern medical board – 4shb 1103 pilot project...
TRANSCRIPT

House Bill 1103 Report To The Legislature Pursuant to Fourth Substitute House Bill 1103, Sections 29 and 30 (Chapter 134, Laws of 2008) January 2013
Publication Number 631-041
For more information or additional copies of this report contact:
Office of the Assistant Secretary Health Systems Quality Assurance PO Box 47852 Olympia, Washington 98504
Phone: (360) 236-4600 Fax: (360) 236-2901
Mary C. Selecky Secretary

Contents Page Contents SECTION 1 1 Executive Summary 3 Health Systems Quality Assurance Division - implementation of HB 1103 (2008) and Secretary’s Recommendations 14 Introduction
18 Performance Measures and Comparative Analysis 18 Licensing Activity Comparative Analyses 22 Disciplinary Activity Comparative Analyses 32 Personnel and Business Processes Activity Comparative Analyses 35 Budgetary Comparative Analyses 36 Regulatory Activity Comparative Analyses 39 National Research Regarding Regulatory Effectiveness and Patient Safety SECTION 2 Washington State Medical Quality Assurance Commission – Efficient, Transparent, Responsive: A Safer Patient, a Respected Profession, a Modern Medical Board – 4SHB 1103 Pilot Project Report SECTION 3 Washington State Nursing Care Quality Assurance Commission – 1103 Report,
Comparison of Performance Outcomes

Health Systems Quality Assurance Division HB 1103 Report 1 SECTION 1
EXECUTIVE SUMMARY The Washington state legislature enacted Fourth Substitute House Bill 1103 (HB 1103) in 2008. The law changed many provisions impacting regulation of health professions. The Department of Health - Health Systems Quality Assurance (HSQA) division was responsible for implementing many aspects of HB 1103. Among other changes to health profession regulation, HB 1103 established mandatory five-year pilot projects for the Medical Quality Assurance Commission (MQAC) and the Nursing Care Quality Assurance Commission (NCQAC). The pilot projects gave these two commissions increased authority over budget and staffing. The legislation creating the pilot projects required that MQAC and NCQAC negotiate performance-based expectations with the Secretary of Health regarding:
o Effectiveness of licensing and disciplinary activities; o Efficiency, timeliness and personnel resources; o Budgetary activity; and o Regulatory activities, including timelines, consistency of decision making, and
performance levels. The pilot period ends June 30, 2013. The legislation also required a report to the legislature on the results of the pilot projects. The report was to compare various aspects of performance before and after the pilot project period, as well as results from a review of national research regarding regulatory effectiveness and patient safety. Although the bill sets a December 2013 due date, the department, MQAC and NCQAC decided to provide this report prior to the end of the pilot. Implementation of the MQAC and NCQAC pilot projects in 2008 coincided with a major reorganization in HSQA, where the end result was consolidation of administrative and regulatory models along functional (rather the individual program) lines. This report provides the results of fourteen performance-based expectations that were negotiated early in the pilot project period. It also provides a platform for HSQA, MQAC, and NCQAC to provide individual perspectives on the pilot project experience, performance results and other contextual information. HSQA Summary: The current framework for health profession regulation under the umbrella of HSQA is effective. Health profession licensing and disciplinary activities are organized along functional lines. This structure retains subject matter expertise, but allows for breadth and depth of coverage, easy sharing of best practices, and operational efficiencies that provide economy of scale for a complex regulatory system. As such, this frame work has the resiliency, flexibility, and accountability needed for implementation of many changes to the health care system coming in the immediate and near future. These include implementation of the federal Affordable Care Act, the “Triple Aim” for health care delivery, and the Washington “Agenda for Change” action agenda for public health. Based on a review of the performance measures required in HB 1103 which show comparable improvement by all boards and commissions and other available information, the Secretary recommends retaining the current business model for MQAC and NCQAC as created by the bill in 2008: She also recommends;
• No expansion of the model beyond MQAC and NCQAC because other boards and commissions are performing efficiently while fully integrated within the department;
• Statutory clarification regarding staff compliance with state and agency policies which is necessary for risk management purposes and consistent with the 2007 State Auditor’s recommendations on health profession regulation and other statutory provisions; and

Health Systems Quality Assurance Division HB 1103 Report 2 SECTION 1
• Review of the statute requiring operating agreements in order to clarify the authority, roles, and responsibilities between the department and the pilot commissions and provide a dispute resolution process.
See these links to the following sections of this report. National Research Regarding Regulatory Effectiveness and Patient Safety: Page 38 MQAC Summary: SECTION 2 NCQAC Summary: SECTION 3

Health Systems Quality Assurance Division HB 1103 Report 3 SECTION 1
HEALTH SYSTEMS QUALITY ASSURANCE DIVISION Observations on Implementation of HB 1103 (2008) and Secretary Recommendations: Overall, the comparisons contained in the Performance Measures - Comparative Analysis portion of this report support several conclusions.
• From a review of data from the department’s Integrated Licensing and Renewal System (ILRS), there does not appear to be consistent use of this common data base between HSQA and MQAC and NCQAC. This makes data comparisons difficult when the goal is to compare timeliness and effectiveness across all health professions.
• The evidence does not to support the pilot model extending beyond MQAC and NCQAC. Analysis of the performance measures shows that other healthcare professions managed under the HSQA “umbrella” structure either perform as well as the pilot models, or are trending in that direction. The unique nature of the MQAC and NCQAC and their licensees supports continuing the pilot model into the future for them.
• Where a HSQA board, commission or Secretary profession does appear to be under - performing compared to MQAC or NCQAC, a more detailed analysis needs to occur before conclusions about effectiveness or timeliness can be made due to differences in data entry, collection and analysis among HSQA, MQAC and NCQAC. Many variables may contribute to the superficial appearance of whether performance is better or worse.
• The opportunities for a common vision for patient safety, supported by common business practices, should be acknowledged. Under the current model, the Chiropractic Quality Assurance Commission received the 2012 Dr. Earl L. Wiley Outstanding Licensing Board award acknowledging the important role DOH and the commission together play in patient safety.
• The recommendations in the 2007 Health Professions Performance Audit are consistent with HSQA’s current organizational structure (on a functional basis) which is providing consistent, timely, and quality support and regulation for the health professions not in the pilot model.
• Washington State is known as a leader in having a health profession disciplinary system that models the national trend in health care delivery including:
o Inter-profession coordination and integration: a team approach; o Elimination of variation: consistency in approach and results; and o Implementation of best (most efficient) and evidence based practices.
Based on the data and information provided in the previous section of this report, and additional background details provided below, the Secretary of Health recommends the following legislative action:
• The Uniform Disciplinary Act should be preserved for all professions. This way, Washington will remain a national model for having a regulatory system that reflects national trends in health care delivery regarding inter-profession coordination, minimizing variation, and integration of best evidence based practices.
• The HB 1103 business model for budget and staffing authority for the Medical Quality Assurance Commission (MQAC) and Nursing Care Quality Assurance Commission (NCQAC) should continue in some form, but should not be extended to include other professions. There is no evidence to support the idea that expanding the current pilot

Health Systems Quality Assurance Division HB 1103 Report 4 SECTION 1
project model to other boards or commissions would have a positive impact on performance or patient safety. Expansion of this business model would not be consistent with the national trends for health care delivery or best practices recognized above. Changes to the current pilot model are needed to:
o Require compliance by commission members and staff with state and agency administrative rules, policies and procedures. Examples include public disclosure, back history checks, disciplinary activities, legislation and lobbying.
o Require that the executive directors for the two commissions will be hired in consultation with the Secretary of the Department of Health.
o Define the hiring authority for MQAC and NCQAC staff. o Provide procedures to resolve disputes that cannot be resolved between the
commissions and the department, including submission to a neutral third party such as the Office of Financial Management.
o Amend the current statute requiring joint operating agreements and provide clarity regarding authority, roles and responsibilities, if needed.
The following information is intended to support and explain the Secretary’s recommendations. Current regulatory framework: The following section of this report outlines the various components of HB 1103 that involved the most comprehensive changes to the health profession disciplinary process in many years. The data and information summary in the previous section shows some variation between the pilot commissions and the professions under the HSQA “umbrella.” Overall, however, performance is comparable or trending toward comparable performance. As a result, it is difficult to say that one model is better, or worse, than another. Differences for any individual performance measure have credible explanations. In reality, we know there are differences between HSQA, MQAC and NCQAC regarding staff resources, staff activities across a variety of activities, and common practices for inputting data into the ILRS system that is used to try to make cross-profession comparisons. Consistency with the 2007 health professions performance audit: HB 1103 reinforced and implemented recommendations from the 2007 Performance Audit final report, which focused on eliminating the risk from variations in common business practices across HSQA. The audit recommended a number of action steps to make changes in organizational structure and processes. These changes were designed to enhance regulatory effectiveness and improve patient safety. They also provided consistent processes and procedures for health care provider applicants and licensees. This consistency is vital to the risk associated with claims of disparate or arbitrary licensing or disciplinary actions. The performance audit validated a major reorganization that was already under way. Like the audit, the purpose of the reorganization was to enhance regulatory effectiveness and improve patient safety. One focus of the reorganization was to shift common business practices that were performed in separate organizational units to a more unified, functional structure. The reorganization plan was carefully planned so that subject matter expertise would be maintained, and work teams would benefit from implementing best practices and efficiencies. The HSQA reorganization coincided with implementation of the MQAC and NCQAC pilot projects established under HB 1103. Since July 2008, leadership at the department has worked very closely with those two commissions and their executive directors to ensure successful implementation of the pilot projects. More importantly, we have worked to achieve our common mission – protecting and improving the health of people in Washington State. Together, our

Health Systems Quality Assurance Division HB 1103 Report 5 SECTION 1
focus has been patient safety and exploring different models to impact the efficiency and effectiveness of our regulatory mandates and authorities. Implications for implementation of the Patient Protection and Affordable Care Act: The health care delivery system must be recognized as a critical component of implementation of health care reform. The way health care is delivered must be resilient, responsive, and receptive to doing business differently in the future. A common operational structure for health profession regulation, as is currently the case for HSQA, is the most effective and efficient way to provide a resilient and responsive system for changes that will result from federal health reform and future state legislation. Consistency with the Triple Aim in health care: The “Triple Aim” is a three-fold goal of improving the experience of care, improving the health of populations, and reducing per capita costs of health care. In order to be a viable and valuable part of this evolving health care delivery system, the regulatory arm of the health care delivery system must also reflect these same values and goals. Under the HSQA umbrella approach, integrated health care professions provide efficiencies that help reduce costs of health care and facilitate cross-profession coordination. The Agenda for Change: An Action Agenda for Public Health: Since 2010, public health leaders in Washington have been actively engaging in efforts to define the role of public health for the future. The role of the health care delivery system as a key partner in public health has been acknowledged. In addition the critical need for public health to partner with the health care delivery system is recognized one of the cornerstones of the action agenda for public health today and in the future. A coordinated framework for health care profession regulation under HSQA is critical to success in moving this action agenda for public health forward. Additional Background and Context: Purpose of the Department of Health. The following background and contextual information is intended to provide a more comprehensive overall understanding of the department’s role and the legislative intent behind its creation. The Department of Health was created by the legislature in 1989. The intent of this action, as set forth in RCW 43.70.005, included the following statements:
• The legislature recognizes the need for a strong, clear focus on health issues in state government…
• It is the intent of the legislature to form such focus by creating a single department in state government with the primary responsibilities for the preservation of public health monitoring health care costs, the maintenance of minimal standards for quality in health care delivery, and the general oversight and planning for all the state's activities as they relate to the health of its citizenry.
• It is the intent of the legislature…to ensure that this new health agency delivers quality health services in an efficient, effective, and economical manner that is faithful and responsive to policies established by the legislature.
The 1989 legislature further declared, in RCW 43.70.020, that the department “shall be organized consistent with the goals of providing state government with a focus in health and serving the people of this state” and should have:

Health Systems Quality Assurance Division HB 1103 Report 6 SECTION 1
• “Clear lines of authority which avoid functional duplication within and between sub-elements of the department”;
• “A clear and simplified organizational design promoting accessibility, responsiveness, and accountability to the legislature, the consumer, and the general public”; and “Decentralized authority and responsibility, with clear accountability”.
In addition, the department should be a “single point of access for persons receiving like services from the department…” Health Profession Regulation within the Department of Health Health Systems Quality Assurance is the division within the department responsible for regulating the health care delivery system in Washington. This encompasses everything from emergency services to primary care to hospice, and includes both health care providers and facilities. Approximately one of every fourteen adults in Washington holds one or more credentials issued by the department through HSQA. Our efforts to ensure patient safety through licensing and discipline of providers and facilities affect every citizen in this state on countless occasions during their lives. The work we do in HSQA is performed in partnership with many stakeholders. Of those, the most crucial relationships we maintain are with the seventeen health profession boards and commissions under the department’s “agency umbrella.” These boards and commissions range from the Board of Pharmacy, founded June 15, 1891, to the Board of Naturopathy, created by the legislature in 2011. The history of each board and commission is unique, but they were all placed within the department because they have the similar purpose of protecting the public through thoughtful regulation of their members. Since the department’s inception in 1989, we have consistently sought to improve the quality of our work while still accomplishing the stated intent of the legislature. However, as our work grew, we found our professions becoming increasingly isolated. Credentialing and disciplinary work for boards and commissions was done by a few staff members dedicated to that profession. This led to inconsistent standards, practices and outcomes even among very similar professions such as allopathic and osteopathic physicians. HSQA Quality Improvement Initiatives HSQA has implemented several quality improvement initiatives that have increased consistency, coordination, and efficiency across health care professions. These changes have also improved the ability of all professions, including MQAC and NCQAC, to meet HB 1103 performance measure targets. As noted, above, the 2007 performance audit of HSQA by the State Auditor found inconsistencies in credentialing and discipline by individual professions to be a high risk to the agency and the public. It recommended standardizing business practices and internal controls within the division. The findings of the performance audit accelerated existing plans for a reorganization of HSQA. Rather than maintaining existing silos, similar tasks and duties were identified and organized into a functional structure. The change was implemented in July 2008 to achieve the following objectives:
• Improve patient safety;

Health Systems Quality Assurance Division HB 1103 Report 7 SECTION 1
• Increase public confidence in our ability to protect public health; • Apply a thorough approach to system improvements; • Increase span of control of supervisors with clear lines of authority and
accountability; and • Increase efficient delivery of services.
Under the prior model, one staff member could be responsible for many different steps in the regulatory process without any system of checks and balances. Under the functional model, duties are separated to ensure both subject matter expertise in a focused set of tasks and additional review by another staff member. For example, all credentialing activities are now consolidated in the office of Customer Service Office (OCS). OCS serves as the entry point for the credentialing of health care providers and facilities. This has resulted in: • Greater consistency through more efficient and standardized processes and procedures; • Increased accountability and quality assurance through separation of duties; • Enhanced ability to collect reliable data and use it to further improve processes; and • The ability to make consistent changes to applications for all professions such as the recent
replacement of “mental retardation” with “intellectual disabilities.” These changes have resulted in better customer service and patient safety. Credentialing health care practitioners is the first step in assuring the availability of qualified, safe and competent health care providers and facilities in Washington. Another major HSQA milestone was the implementation of Integrated Licensing and Regulatory System (ILRS) in February 2008. ILRS is an electronic data base used to process and track initial applications, renewals, inspections, complaints, investigations and disciplinary actions. It replaced eight separate, outdated systems. The data in ILRS can be easily retrieved and used to evaluate and improve performance. In addition to the unprecedented ability to perform meaningful quality improvement projects, we are now better able to respond to stakeholder and legislative inquiries quickly and with quality information. However, this is entirely based upon the data being entered consistently in both time and manner. If one program or profession fails to abide by the department’s data entry standards, the resulting information and reports can be rendered inaccurate or misleading. Key Legislative Changes During this same period of critical change and improvement, the Legislature passed three bills focused on improving patient safety by strengthening the department’s ability to screen applicants and take meaningful action under the Uniform Disciplinary Act (UDA), the law under which all health care profession discipline is performed. The first bill, HB 2974, was passed in 2006. This bill:
• Granted the Secretary authority to make rules requiring all health care providers to report certain acts or findings of misconduct committed by another provider;
• Mandated the summary suspension of any health care provider prohibited from practicing in another state due to unprofessional conduct;
• Required the disciplining authorities to consider prior complaints when deciding whether to authorize investigation of a current complaint;

Health Systems Quality Assurance Division HB 1103 Report 8 SECTION 1
• Added language clarifying that “safeguarding the public’s health and safety is the paramount responsibility of every disciplining authority”; and
• Directed the Washington State Patrol (WSP) to notify the department of certain felony convictions so we can determine whether the crime was committed by a credentialed health care provider.
The second bill was HB 2674 (2008). Under this bill, the department reached a significant landmark for patient safety in Washington when it abolished the registered counselor profession in July 2010. More than 14,000 registered counselors were successfully transferred into eight newly created counselor professions with specific education, training and oversight requirements. HB 2674 has substantially reduced the public safety risk presented by unqualified mental health practitioners. The third bill was HB 1103, the origin of this report. The opening paragraph of HB 1103 declares:
From statehood, Washington has constitutionally provided for the regulation of the practice of medicine and the sale of drugs and medicines. This constitutional recognition of the importance of regulating health care practitioners derives not from providers' financial interest in their license, but from the greater need to protect the public health and safety by assuring that the health care providers and medicines that society relies upon meet certain standards of quality.
This statement embodies the belief that patient health and safety must always be the first consideration of health care regulation. Whether the regulatory authority is the Secretary of Health, a board or a commission, it must always strive to protect the public. Professional associations exist to represent the needs and desires of the practitioners. Because of this, the regulatory authorities and corresponding association(s) may sometime disagree on certain issues but this can almost always be leveraged into productive conversations and collaborative efforts. HB 1103 contained numerous changes to health profession discipline. For example:
• Required all disciplining authorities (the Secretary, boards and commissions) to adopt procedures to ensure substantially consistent application of the Uniform Disciplinary Act;
• Made the Secretary the disciplining authority for all complaints alleging that a license holder has committed an act or acts of unprofessional conduct involving sexual misconduct after the board or commission determines the case does not involve clinical expertise or standard of care issues;
• Directed the Secretary to adopt rules establishing a uniform sanctioning schedule that must be applied in all disciplinary actions for all health professions;
• Permitted disciplining authorities to order permanent revocation if the provider can never be rehabilitated or regain the ability to practice with reasonable skill and safety;
• Created a quicker and more efficient process for denying a credential or granting it with conditions;
• Allowed disciplining authorities to issue citations and assess fines to providers for failure to produce documents, records, or other items when requested;
• Expanded the WSP’s duty to report convictions to the department to include all felonies; and
• Enhanced the ability to screen applicants by authorizing: o The Secretary to receive criminal history record information that includes
nonconviction data;

Health Systems Quality Assurance Division HB 1103 Report 9 SECTION 1
o The Secretary to require fingerprint-based national background checks where Washington background check under is inadequate; and
o All disciplining authorities to consider the results of the background checks performed by the Secretary on behalf of the disciplining authority, or any other background check that reveals a conviction or a series of arrests demonstrate a pattern of behavior that may pose a risk to patient safety when deciding whether or not to issue an initial license.
Performance Measures The implementation of ILRS in 2008 allows us to track performance in levels of detail and accuracy not previously possible. We are very confident that reports retrieved from ILRS are highly accurate as long as the data is entered in a consistent manner. Procedures in place in HSQA guarantee that data is entered in the same fashion by all CSO staff for every profession we credential. Similarly, all investigators and staff attorneys enter their data consistently. As a result, the performance data for HSQA boards, commissions and Secretary professions compares “apples with apples.” The commissions participating in the pilot commissions have not always chosen to use ILRS in the same way as HSQA. As such, we are not confident that a side by side comparison is a true reflection of actual performance. In addition, there were differences in resources which in part may be accounted for by differences in case complexity. For example, in the 2009-11 biennium, MQAC legal staff, comprised of six staff attorneys, completed disciplinary action in 256 cases. By comparison, in the same time period, HSQA legal staff, comprised of 20 attorneys, completed disciplinary action in 1,979 cases1
. This equates to an almost eight-fold increase in production by less than a four-fold increase in staff, despite the fact that HSQA staff attorneys carry a significantly higher caseload than MQAC staff attorneys. The average HSQA staff attorney caseload reached an all-time low of 50.9 at the end of fiscal year 2012, whereas the average MQAC staff attorney caseload was 39.9.
Regardless of these concerns, HSQA’s performance during the pilot period has shown significant improvement in several areas, including the critical area of investigation and discipline.
• The percentage of cases in the investigation step that were over 170 days was reduced by more than 12 percentage points between fiscal years 2010 and 2012.
• The percentage of cases in the case disposition step that were over 140 days was reduced 17 percentage points for Secretary cases and 21 percentage points for nursing commission cases between fiscal years 2010 and 2012 (HSQA legal staff handle nursing cases).
• The percentage of informal resolutions and formal orders that comply with the sanction schedule increased by more than 8 percentage points for HSQA boards and commissions and 10 percentage points for nursing cases (HSQA legal staff handle nursing cases).
Benefits of an Umbrella Agency Structure Many of the legislative changes discussed above clearly rely on the Secretary’s broad authority as the head of the department to accomplish tasks on behalf of all disciplining authorities. For example, the Secretary was required to consult with the boards and commissions when creating the sanction schedule, but the ultimate duty to make rules that would apply to all professions was
1 Source; 2009-11 Health Professions Discipline and Regulatory Activities (UDA) report.

Health Systems Quality Assurance Division HB 1103 Report 10 SECTION 1
given to the entity with the overall responsibility and accountability for health care regulation. The ability to assign implementation of a law requiring consistency among professions to the Secretary allows for a timely and effective product. Assigning the same project to seventeen boards and commission is unlikely to produce similar results. A prime example of the benefit of coordination through an umbrella agency is the pain management rules for chronic noncancer pain. The legislature passed HB 2876 (2010) in response to the state’s growing rate of opioid related deaths and overdoses. Five boards and commissions (medical, nursing, dental, osteopathy and podiatry) were required to adopt rules to guide providers with authority to prescribe opioids for long-term use. The rules were mandated to be effective by July 1, 2011, less than thirteen months after the effective date of the bill. The bill did not call for a single set of rules by the Secretary, but it did include a statement that the boards and commissions “shall work collaboratively to ensure the rules are as uniform as practicable.”2
This provision encompassed the belief that all patients receiving similar treatment deserve the same level of care regardless of the credential of the health care provider.
Staff from HSQA’s Office of the Assistant Secretary policy team took the lead in coordinating rulemaking efforts and reaching consensus on a strategy with the boards and commissions. A workgroup consisting of representatives from each board and commission was established and facilitated by policy team members. Those staff members guided the process, led five public stakeholder meetings, drafted the language based on concepts agreed upon by the board and commission members, and shepherded the rules through the formal adoption process. The rules were adopted on time, contained the elements required by the statute and reflected the uniformity desired by the legislature and governor. There are numerous other benefits inherent to being part of an umbrella agency.
• Infrastructure such as information technology, human resources, communications and other common business functions can be leveraged to benefit the entire agency at a lower per capita cost.
• Assistive professions can be developed and implemented in consultation with the boards and commissions for the primary providers.
• Centralized rulemaking ensures that unforeseen impacts to other professions are identified and addressed before the rules are effective.
• Steering committees for credentialing and enforcement issues allow discussion of common issues by members from across the division, including staff supporting the boards and commissions. The steering committees propose changes and enhancements to credentialing and enforcement based on best practices, benchmarking data, technology, legislation and emerging case law.
• Legislative initiatives such as the bills related to licensing military members, spouses and domestic partners, and HB 1493, the 2011 transparency in discipline bill, are coordinated to ensure consistent outcomes for all professions, efforts are not duplicated, and subject matter expertise is grown and consolidated.
• One-stop-shopping for the public, health care employers, legislative staff, media and other stakeholders:
2 This section was vetoed by Governor Gregoire for unrelated reasons. However, she clearly directed the department to abide by this language despite the veto.

Health Systems Quality Assurance Division HB 1103 Report 11 SECTION 1
o Complaint intake for all health care professions. Complainants often refer to the provider as “doctor” without specifying the actual credential type. We are able to accept these calls without additional questioning or inconvenience for the caller.
o One call center that can direct callers to the appropriate staff for any profession. Since 2008, HSQA contracts with interpreters to support callers to our call center and program areas who have different language preferences. This contract also allows for translation services for written correspondence.
o A single web site that includes a provider search feature covering all credentialed health care providers, a single complaint form for any health profession, and individual information and application pages for each profession.
• Staffing levels that allow for depth and cross-training so that individual illnesses, emergencies or position vacancies do not have such a significant impact.

Health Systems Quality Assurance Division HB 1103 Report 12 SECTION 1
Current HSQA Projects and Innovations In the continuous cycle of evaluation and quality improvement, HSQA has several exciting projects in process that enhance our ability to protect public health while effectively and efficiently regulating health care professions. These are projects that benefit a wide variety of providers from nursing assistants to physicians, and are a trademark benefit of an umbrella agency. The Prescription Monitoring Program has been operating for a year and the state is already seeing the first indications of savings, both in terms of human life and financial costs. ILRS, our electronic data base, can now process on-line renewals for more than half of the 83 health professions. Payment can be made by credit card or electronic check. This option has been a frequent request by providers across Washington. The remaining professions will have on-line renewal capability by April 2013. We plan to begin accepting on-line applications for initial credentialing of eight professions by June 2013. HSQA is piloting technology to move away from paper-based environment. In August 2012, we began an electronic imaging/filing project. All new license applications and associated paper documents such as references, exam scores, transcripts and other documents are being captured electronically, through a scan and indexing process. We are now capturing additional data for analysis, including the time it takes to scan documents. This information will help determine the success of the project. We are in the first phase of conducting an in-depth review of health profession rules. Healthcare education, technology and treatment modalities have changed drastically in the past decade. It is vital that our regulations enhance, rather than inhibit, the most modern and effective practices. Teams comprised of HSQA’s program, policy, rulemaking and legal staff will be participating in this important project. These innovations are effective and cost efficient because they are implemented under the coordinated and consistent HSQA structure. Conclusion As we move into the future of health care and health reform, HSQA remains fluid, adaptable and responsive to change. We envision that health care will become more integrated and more team-based. Patients are better served when their needs can be met through a coordinated approach, both from the providers who treat them and the regulatory system entrusted with preserving public health. The current structure of HSQA within the department’s umbrella agency is key to effective coordination of the health care system. We believe that separation of professions from the department would have immediate negative impacts:
• Consistency in professional regulation would be reduced. Laws, rules and processes would no longer be implemented or applied in the same manner;
• Unnecessary costs and inefficiencies would be created as each group duplicates efforts and equipment related to identical business functions. These costs would be passed on to health care providers in the form of increased licensing fees. Those costs would then be passed on to patients and third party payors.
• The legislature would lose its ability to direct the Secretary to take action related to all health care providers.

Health Systems Quality Assurance Division HB 1103 Report 13 SECTION 1
• The public, including health care employers, would be denied the ability to have all their licensing, complaint and public records disclosure activities handled seamlessly by a single entity.
These results are the exact opposite of what the legislature envisioned when it created the Department of Health in 1989. The “Performance Measures – Comparative Analysis” in section 1 describes how the department, MQAC and NCQAC developed and monitored the performance-based measures required by HB 1103. They focus on consistent, timely regulation of health care professionals and show consistent improvement or positive trends by each group. The evaluation of these performance measures has shaped the conclusions and recommendations in this report. DOH and HSQA have proven to be an effective regulatory organization for all health care professions in Washington. We work closely and collaboratively with our boards and commissions to credential qualified, competent and safe providers; establish standards for patient care and safety through the rule making process; and take appropriate disciplinary action when necessary to protect the public.

Health Systems Quality Assurance Division HB 1103 Report 14 SECTION 1
HEALTH SYSTEMS QUALITY ASSURANCE DIVISION HB 1103 REPORT Introduction The Washington State Legislature enacted Fourth Substitute House Bill 1103 (HB 1103) in 2008. This law changed many provisions impacting the regulation of health professions in our state. Significant changes to health care provider discipline were made in areas such as conducting background checks, hearing processes, applying sanctions, and reporting unprofessional conduct. The Department of Health - Health Systems Quality Assurance (HSQA) division is responsible for management and oversight of all of these activities and was charged with implementing many provisions of HB 1103. HB 1103 also established mandatory five-year pilot projects for the Medical Quality Assurance Commission (MQAC) and Nursing Care Quality Assurance Commission (NCQAC). The Chiropractic Quality Assurance Commission and the Dental Quality Assurance Commission were allowed to participate on a voluntary basis but both declined. The pilot projects for MQAC and NCQAC began July 1, 2008 with a statutory end date June 30, 2013. The pilot projects authorized the two commissions to each hire its own executive director and permit that executive director to carry out the administrative duties of the commission and manage the staff assigned to the commission. The commissions were also authorized to propose their own biennial budgets for the Secretary of Health (Secretary) to submit to the Office of Financial Management. HB 1103 also required MQAC and NCQAC to negotiate with the Secretary to develop performance-based expectations focusing on consistent, timely regulation of health care professionals. Implementation of the MQAC and NCQAC pilot projects coincided with the official start date for a major reorganization in HSQA that was already under way by July 1, 2008. The purpose of the HSQA reorganization was to improve regulatory effectiveness and improve patient safety. The reorganization was consistent with recommendations in the 2007 Performance Audit report (discussed below), which focused on eliminating risk that could occur from variations in common business practices across the HSQA division. In implementing the pilot projects, both MQAC and NCQAC incorporated all functions related to licensing and investigating the professions under their jurisdictions. Both commissions retained a dedicated commitment to regulatory efficiency and patient safety. For all other professions, policy development, licensing, investigations and legal support (including legal support for NCQAC) were centralized into functionally aligned offices. An organizational chart showing HSQA relationships to MQAC and NCQAC is shown on the next page.

Health Systems Quality Assurance Division HB 1103 Report 15 SECTION 1
Health Systems Quality Assurance Organization Chart

Health Systems Quality Assurance Division HB 1103 Report 16 SECTION 1
HB 1103 requires that the Secretary, MQAC and NCQAC submit a report to the governor and the legislature on the results of the pilot projects.3
The report must compare the effectiveness in licensing and disciplinary activities, efficiency with respect to timeliness and personnel resources, budgetary activity, and ability to meet performance measures. The report must also review national research regarding regulatory effectiveness and patient safety. This report evaluates outcomes of 14 performance measures negotiated by HSQA, MQAC and NCQAC.
At the beginning of the pilot projects, the department developed Memoranda of Understanding and joint operating agreements with MQAC and NCQAC. These documents describe the roles and responsibilities of the two commissions and the department to implement the pilots and work together to accomplish the public protection work vital to the commissions and the department. Other boards and commissions have similar operating agreements, with the exception of the Board of Pharmacy. Health professions in Washington are regulated by either the Secretary or seventeen boards and commissions.4
• Boards:
o Board of Denturists o Board of Hearing and Speech o Board of Massage o Board of Naturopathy5
o Board of Nursing Home Administrators
o Board of Occupational Therapy Practice o Board of Optometry o Board of Osteopathic Medicine and Surgery o Board of Pharmacy o Board of Physical Therapy o Podiatric Medical Board o Examining Board of Psychology o Veterinary Board of Governors
• Commissions:
o Chiropractic Quality Assurance Commission o Dental Quality Assurance Commission o Medical Quality Assurance Commission o Nursing Care Quality Assurance Commission
3 HB 1103 sections 29 and 30 require this report be prepared by December 15, 2013. However, the department, MQAC and NCQAC believe that the legislature’s intent was that this report be delivered to the legislature prior to the June 30, 2013, end of the pilot. 4 Two professions have split authority. The Board of Massage and the Board of Denturists have licensing authority but the Secretary is the disciplining authority. 5 The Board of Naturopathy was created by the Legislature effective July 22, 2011. Prior to that date, the naturopathy profession was regulated by the Secretary.

Health Systems Quality Assurance Division HB 1103 Report 17 SECTION 1
HSQA, including MQAC and NCQAC, coordinates regulation of more than 380,000 health care providers in 83 professions. This includes 20 new professions created by legislation or initiative since 2007. The Secretary, boards and commissions determine whether applicants meet minimum licensing requirements, investigate complaints of unprofessional conduct, take appropriate disciplinary action if unprofessional conduct is found, and oversee compliance with sanctions. In addition to licensing and disciplinary activities, HSQA also supports the boards and commissions in developing the rules that define qualifications to practice and other standards based on authority granted by the legislature. During the 2009-11 biennium, the department (including MQAC and NCQAC):
• Issued more than 120,000 new credentials. • Renewed more than 580,000 existing credentials. • Processed more than 17,600 new complaints while working on more than 3,600
complaints received prior to the 2009-11 biennium. • Issued more than 2,400 disciplinary orders. • Responded to more than 21,500 requests for public records.
[k1]

Health Systems Quality Assurance Division HB 1103 Report 18 SECTION 1
PERFORMANCE MEASURES - COMPARATIVE ANALYSES HB 1103 required the Secretary, MQAC and NCQAC to negotiate performance-based expectations focused on consistent, timely regulation of health care professionals. The bill required a report comparing the activities of MQAC, NCQAC, other HSQA boards and commissions and the department during the HB 1103 pilot period on these subjects:
• Effectiveness of licensing and disciplinary activities; • Efficiency, timeliness and personnel resources; • Budgetary activity; and • Regulatory activities, including timelines, consistency of decision making, and
performance levels. HB 1103 also required the department, MQAC and NCQAC to review and summarize national research and data regarding regulatory effectiveness and patient safety.
Early in the pilot project period, HSQA, MQAC and NCQAC met the statutory requirement of negotiating agreed performance measures. The following sections address these topics and make the comparisons and evaluations required by HB 1103. In certain areas, the necessary historical baseline data was limited or unavailable; the narrative explains when these circumstances occurred.
LICENSING ACTIVITY COMPARATIVE ANALYSES The credentialing sections in HSQA, MQAC and NCQAC work to ensure public safety by verifying that applicants for health care credentials comply with regulatory requirements to practice in their respective professions, and issuing credentials only to qualified providers, emergency medical services, and facilities. The credentialing sections provide the department’s first opportunity to assess an applicant’s fitness to practice, and often trigger further review for potential denial or restriction. Several changes and events in recent years impacted the overall system and processes for issuing new health professions credentials: New professions: Since 2007, the following 20 new health professions were created by the legislature or by voters via initiative:
• 2007: Athletic trainer, dental assistant, expanded function dental auxiliary, retired medical worker
• 2008: Agency affiliated counselor, certified counselor, certified advisor, chemical dependency professional trainee, marriage and family therapist associate, mental health counselor associate, licensed social worker associate, licensed social worker-independent clinical associate, radiologist assistant
• 2009: Speech-language pathology assistant, genetic counselor • 2010: Cardiovascular invasive specialist • 2011: Home care aides • 2012: Medical assistant, reflexology, dental anesthesia assistant
New background check responsibilities: Pursuant to HB 1103, in January 2009 a designated agency Background Check Unit was established in the HSQA Office of Customer Service (OCS). The unit began conducting federal fingerprint-based background checks on new applicants who provide an out of state address within the United States. This is in addition to processing information from the in-state criminal

Health Systems Quality Assurance Division HB 1103 Report 19 SECTION 1
history checks conducted by the Washington State Patrol for every health profession applicant.
OCS managers worked with MQAC and NCQAC to create a process that allows the Background Check Unit to complete finger–print based background checks for MQAC and NCQAC applicants without a paper copy of the application. In March 2009, OCS added new technology and staff training to begin electronic fingerprint card scanning, improving turnaround time for fingerprint based FBI background checks.
New technology and online systems: In February of 2008, HSQA began implementation of the Integrated Licensing and Renewal System (ILRS), replacing five legacy credentialing systems with a single database system for all regulated health professions and facilities. In December 2011, OCS began piloting a system for online renewal of health profession credentials. Full implementation was started in June 2012 and is being implemented in phases with professions being added to the online renewal system monthly. By July 2013, more than 380,000 licensed health professions will have the option of renewing their credentials online.
Basic steps in the HSQA credentialing process include:
License Application
1DOH Revenue Case Receipt
Process
2Intake Process
4Background
Checks ProcessGrant or Deny
Refer to Case Management
3Review Process
5Issue License
No
No
Health Systems Quality Assurance Credentialing Process
Yes
• Step 1 Revenue Cash Receipt: Applications and payments are received by the DOH Revenue Office.
• Step 2 Intake: Applications are sorted, stamped with date received, and file created.
• Step 3 Review: Applications and supporting documents are reviewed for verification of credential specific requirements.
• Step 4 Background Checks: Washington State Patrol (WSP) background check and National Health Integrity and Portability Data Bank (HIPDB) check for all applications. Fingerprint based FBI background checks are completed on applicants with out of state addresses.
• Step 5: Issue the license or refer the application to Case Management.
Health Systems Quality Assurance Division HB 1103 Report 20 SECTION 1
While HSQA, MQAC, and NCQAC credentialing staff follow the same global credentialing process at a high level, there are differences in the order of the flow and detailed process steps. The MQAC and NCQAC processes have some differences in credentialing procedures that the individual commissions have determined based on their regulatory authority. These differences present a challenge in a comparative assessment of timeliness for professions regulated by the MQAC, NCQAC, other boards or commissions, or by the Secretary. Performance Measure 1.1: Health care credentials issued within 14 days after receiving all required application documents The performance measure 1.1 timeframe of fourteen days was established prior to the HB 1103 pilot period. OCS staff credential all health professions with the exception of professions regulated by MQAC (allopathic physicians and physician assistants) and NCQAC (registered nurses, licensed practical nurses, advanced registered nurse practitioners and nursing technicians). Over 35,000 credentials issued during the baseline period of July 2007 through January 2008 were evaluated for comparison. During this period 93.9 percent of credentials were issued within fourteen days after receipt of all required application documents and fees. Accurate tracking of performance measure 1.1 required use of the new ILRS licensing system implemented during 2008. ILRS tracks the last date of contact with each credential applicant (the date when all required credentialing documents are received). ILRS is used by HSQA, MQAC and NCQAC to track credentialing activity, but not always in the same manner. With ILRS at full operation in 2009, nearly 75,000 credentials were evaluated during the period of July 1, 2009 through June 30, 2012 (FY 2010 – FY 2012) to determine whether they were issued within the performance measure 1.1 timeframes. Outcomes for each comparison group improved during the evaluation period.
Health Systems Quality Assurance Division HB 1103 Report 21 SECTION 1
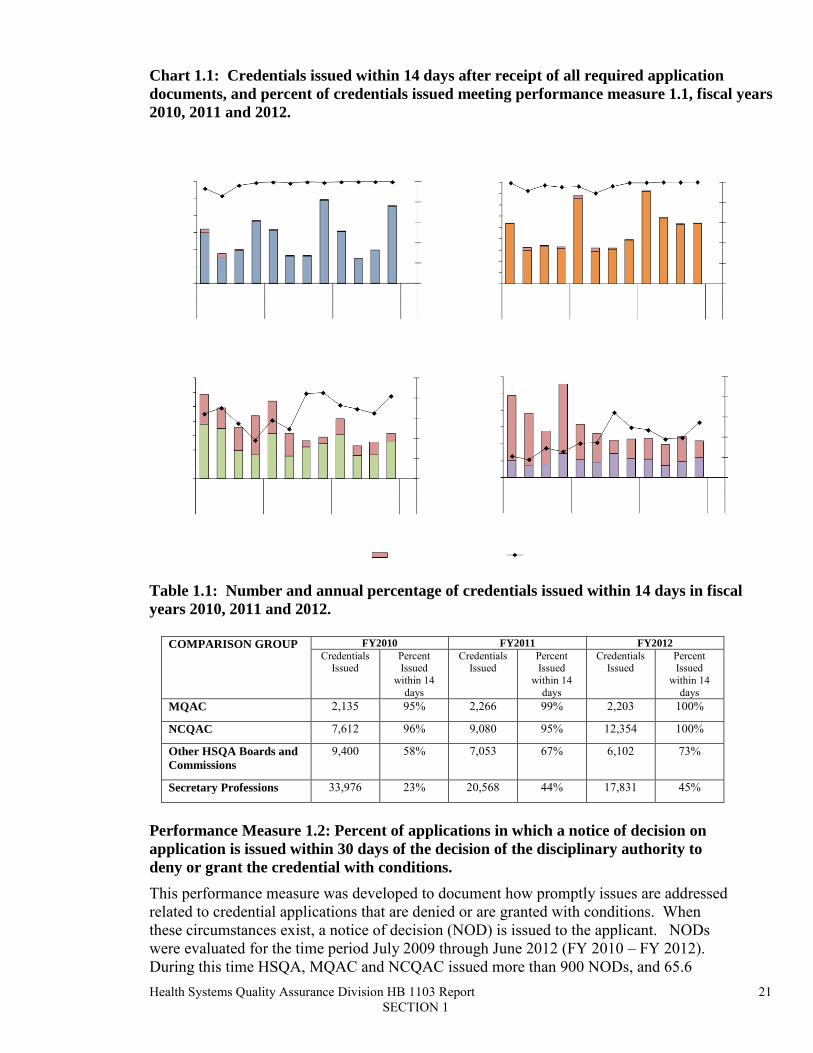
Chart 1.1: Credentials issued within 14 days after receipt of all required application documents, and percent of credentials issued meeting performance measure 1.1, fiscal years 2010, 2011 and 2012.
Table 1.1: Number and annual percentage of credentials issued within 14 days in fiscal years 2010, 2011 and 2012.
COMPARISON GROUP FY2010 FY2011 FY2012 Credentials
Issued Percent Issued
within 14 days
Credentials Issued
Percent Issued
within 14 days
Credentials Issued
Percent Issued
within 14 days
MQAC 2,135 95% 2,266 99% 2,203 100%
NCQAC 7,612 96% 9,080 95% 12,354 100%
Other HSQA Boards and Commissions
9,400 58% 7,053 67% 6,102 73%
Secretary Professions 33,976 23% 20,568 44% 17,831 45%
Performance Measure 1.2: Percent of applications in which a notice of decision on application is issued within 30 days of the decision of the disciplinary authority to deny or grant the credential with conditions. This performance measure was developed to document how promptly issues are addressed related to credential applications that are denied or are granted with conditions. When these circumstances exist, a notice of decision (NOD) is issued to the applicant. NODs were evaluated for the time period July 2009 through June 2012 (FY 2010 – FY 2012). During this time HSQA, MQAC and NCQAC issued more than 900 NODs, and 65.6

Health Systems Quality Assurance Division HB 1103 Report 22 SECTION 1
percent of NODs were issued within 30 days. There was no comparison data available for this performance measure before pilot period because use of NODs was first authorized in HB 1103. Chart 1.2: NODs issued within 30 days, fiscal years 2010, 2011 and 2012.
Table 1.2: Number of NODs issued in fiscal years 2010, 2011 and 2012, and percent issued within 30 days meeting performance measure 1.2.
COMPARISON GROUP FY 2010 FY 2011 FY 2012
Notices of Decision
Issued
% Issued within
30 days
Notices of Decision Issued
% Issued within
30 days
Notices of Decision
Issued
% Issued within
30 days MQAC 14 69% 8 100% 2 100%
NCQAC 0 N/A 11 91% 25 100%
Other HSQA Boards and Commissions
34 56% 56 45% 69 77%
Secretary Professions 267 57% 263 56% 157 92%
DISCIPLINARY ACTIVITY COMPARATIVE ANALYSES Health professions in Washington are regulated by either the Secretary or one of seventeen boards and commissions6
6 Two professions have split authority. The Board of Massage and the Board of Denturists have licensing authority but the Secretary of Health is the disciplining authority.
. Pursuant to RCW 18.130.062, the Secretary is the sole disciplining authority in cases where the complaint alleges only an act or acts of sexual misconduct without clinical

Health Systems Quality Assurance Division HB 1103 Report 23 SECTION 1
expertise or standard of care issues. Investigators, in-house staff attorneys, and health law judges within the department support the work on health profession disciplinary activity. Steps in the disciplinary process for health care professionals include:
Step 1: The department, board or commission receives a report alleging unprofessional conduct by a health care professional.
Step 2: The disciplining authority assesses the report and determines whether the report should be investigated as a complaint, or if the case should be closed without investigation.
Step 3: If authorized, an investigation is performed to gather facts, statements, records and other evidence related to the complaint.
Step 4: The disciplining authority reviews the investigation report and evidence and determines whether to close the complaint, take informal action, or take formal legal action.
Step 5: If legal action is appropriate, an adjudicative proceeding is initiated. For Secretary professions, a health law judge issues a final agency decision. For boards and commission with disciplining authority, a panel of the board or commission makes the final decision. Following resolution through either settlement or hearing, compliance with the order is monitored. If the licensee is non-compliant, further action may be initiated. Performance Measures 2.1 through 2.7 HB 1103 required the Secretary, MQAC and NCQAC to compare the effectiveness of disciplinary activities commission before and during the pilot project, and with the disciplinary
Health Systems Quality Assurance Division HB 1103 Report 24 SECTION 1
activities of other health profession boards and commissions during the same time periods. In preparation, the Secretary, boards and commissions began tracking the following performance measures related to the disciplinary process:
Performance Measure 2.1 - Intake/assessment done within 21 days Performance Measure 2.2 - Investigations done within 170 days Performance Measure 2.3 - Case disposition done within 140 days Performance Measure 2.4 - Current investigations over 170 days Performance Measure 2.5 - Current cases in case disposition over 140 days Performance Measure 2.6 - Orders that comply with the sanction schedule Performance Measure 2.7 - Sexual misconduct cases transferred to the Secretary of Health within 14 days
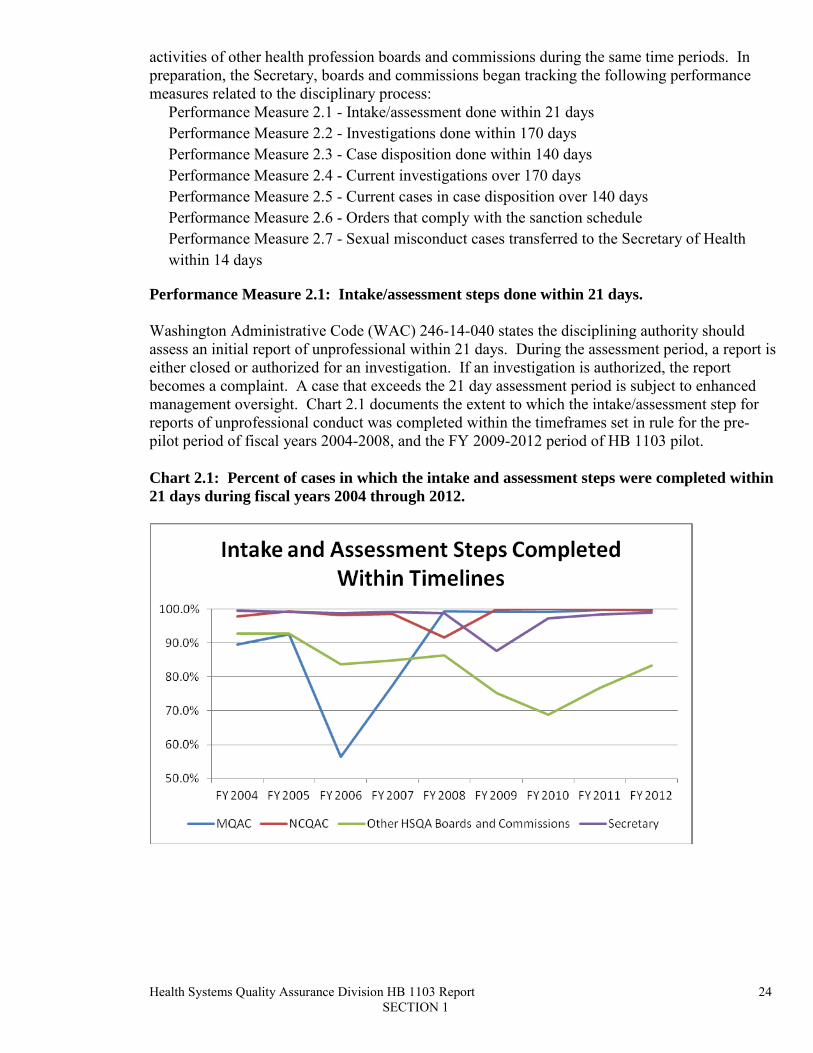
Performance Measure 2.1: Intake/assessment steps done within 21 days. Washington Administrative Code (WAC) 246-14-040 states the disciplining authority should assess an initial report of unprofessional within 21 days. During the assessment period, a report is either closed or authorized for an investigation. If an investigation is authorized, the report becomes a complaint. A case that exceeds the 21 day assessment period is subject to enhanced management oversight. Chart 2.1 documents the extent to which the intake/assessment step for reports of unprofessional conduct was completed within the timeframes set in rule for the pre-pilot period of fiscal years 2004-2008, and the FY 2009-2012 period of HB 1103 pilot. Chart 2.1: Percent of cases in which the intake and assessment steps were completed within 21 days during fiscal years 2004 through 2012.

Health Systems Quality Assurance Division HB 1103 Report 25 SECTION 1
Table 2.1: Percent of cases in which the intake and assessment steps were completed within 21 days during fiscal years 2004 through 2012.
Intake & Assessment Steps Completed within 21 Days
MQAC NCQAC Other HSQA Boards /
Commissions
Secretary Professions
Pre-Pilot Performance (FY 2004-2008)
83.1% 97.1% 88.1% 99.0%
Pilot Period Performance (FY 2009-2012)
99.5% 99.8% 76.1% 95.5%
Performance Measure 2.2: Investigations done within 170 days. WAC 246-14-050 defines an investigation as “the process of gathering information which examines the complaint and the situation surrounding the complaint.” The basic time period for investigation is 170 days. A case that exceeds the 170 day investigation period is subject to enhanced management oversight. Chart 2.1 documents the extent to which the investigation step was completed within the timeframe set in rule. Chart 2.2: Percent of cases in which the investigation step was completed within 170 days during fiscal years 2004 through 2012.

Health Systems Quality Assurance Division HB 1103 Report 26 SECTION 1
Table 2.2: Percent of cases in which the investigation step was completed within 170 days during fiscal years 2004 through 2012.
Investigation Step Completed within 170 Days
MQAC NCQAC Other HSQA Boards /
Commissions
Secretary Professions
Pre-pilot Performance (FY 2004-2008)
76.6% 69.5% 73.6% 79.5%
Pilot Period Performance (FY 2009-2012)
86.9% 45.9% 71.5% 71.7%
Performance Measure 2.3: Case disposition done within 140 days. WAC 246-14-060 defines case disposition as “the process of deciding whether to issue a statement of charges on a complaint, to take informal action, or to close a complaint without action.” It includes the processes necessary to implement the decision such as board or commission member evaluation of the investigation, expert witness review, and drafting and serving legal documents. A case that exceeds the 140 day case disposition period is subject to enhanced management oversight. Chart 2.3 documents the extent to which the case disposition step was completed within the timeframe set in rule. Chart 2.3: Percent of cases in which the case disposition step was completed within 140 days during fiscal years 2004 through 2012.

Health Systems Quality Assurance Division HB 1103 Report 27 SECTION 1
Table 2.3: Percent of cases in which the case disposition step was completed within 140 days during fiscal years 2004 through 2012.
Case Distribution Step Completed within 140 Days
MQAC NCQAC Other HSQA Boards /
Commissions
Secretary Professions
Pre-pilot Performance (FY 2004-2008)
79.4% 81.8% 73.6% 83.0%
Pilot Period Performance (FY 2009-2012)
87.0% 80.3% 73.3% 84.4%
Performance Measure 2.4: Current investigations over 170 days. An investigation that is not completed in 170 days or less remains in the investigation step until finished. This measure includes investigations completed on day 171 or beyond. Cases where the investigation is not completed within timelines are given enhanced management oversight to ensure that the investigation is finished without unnecessary delays. Chart 2.4 documents the extent to which pending cases in the investigation step were beyond the timeframe set in rule. Chart 2.4: Percent of open cases in the investigation step that were over 170 days during fiscal years 2010, 2011 and 2012.

Health Systems Quality Assurance Division HB 1103 Report 28 SECTION 1
Table 2.4: Percent of open cases in the investigation step that were over 170 days during fiscal years 2010, 2011 and 2012.
Investigation Step Exceeded 170 Days
MQAC NCQAC Other HSQA Boards /
Commissions
Secretary Professions
FY 2010 Performance 4.9% 61.8% 25.9% 26.7%
FY 2011 Performance 6.3% 50.0% 23.4% 19.6%
FY 2012 Performance 2.5% 42.0% 13.5% 14.8%
Challenges specific to the investigation step:
• Lack of cooperation by necessary parties such as the licensee, complainant or witnesses. • Complainant hesitation to sign a whistleblower release. • Difficulty in obtaining necessary documents and evidence such as patient records, written
statements and criminal history records. • Necessity to issue formal subpoenas to gather information in some situations such as
mental health and counseling cases. • Geographic challenges of reaching licensees, complainants and witnesses throughout the
state. • Restriction on travel due to budget concerns • Court decisions that increased the time to complete tasks, such as a ruling regarding our
use of subpoenas for information added. Performance Measure 2.5: Current cases in case disposition more than 140 days. A case where the case disposition step is not completed in 140 days or less remains in that step until finished. This measure includes cases where the case disposition step was completed on day 141 or beyond. Cases where the case disposition step is not completed within timelines are given enhanced management oversight to ensure that the case moves forward without unnecessary delays. Chart 2.5 documents the extent to which pending cases in the case disposition step were beyond the timeframe set in rule.

Health Systems Quality Assurance Division HB 1103 Report 29 SECTION 1
Chart 2.5: Percent of open cases in the case disposition step that were over 140 days during fiscal years 2010, 2011 and 2012.
Table 2.5: Percent of open cases in the case disposition step that were over 140 days during fiscal years 2010, 2011 and 2012.
Case Disposition Step Exceeded 140 Days
MQAC NCQAC Other HSQA Boards /
Commissions
Secretary Professions
FY 2010 Performance 35.2% 49.4% 37.4% 54.6%
FY 2011 Performance 26.9% 36.1% 35.7% 45.4%
FY 2012 Performance 30.1% 28.0% 33.8% 36.0%
Challenges specific to the case disposition step:
• Includes time for review by board and commission members, expert witnesses, and the Office of the Attorney General.
• May include time spent negotiating an informal resolution which ultimately proves unsuccessful.
• Pending criminal charges may require the disciplinary action to wait for resolution. Performance Measure 2.6: Percent of orders and stipulations to informal disposition that comply with the sanction schedule. In 2006, the Secretary developed sanction schedule guidelines for Secretary regulated professions. The guidelines provided a framework to ensure that disciplinary cases involving similar facts and similar patient harm or risk of harm resulted in substantially similar sanctions. The guidelines were later adopted by the boards and commissions.

Health Systems Quality Assurance Division HB 1103 Report 30 SECTION 1
HB 1103 required each of the boards and commissions to appoint a representative to review the Secretary’s sanction schedule guidelines and collaborate to develop a uniform sanction schedule to apply to all professions. The sanction schedule rules, found in WAC 246-16-800 through 890, went into effect January 1, 2009. The rules apply to formal orders and informal stipulations. Because the sanction schedule did not exist prior to 2006, there are only two fiscal years of pre-pilot data to compare. Chart 2.6 documents the percent of final decisions in Secretary, board, and commission profession cases that comply with the sanction schedule guidelines/rules. Chart 2.6: Percent of orders or stipulations to informal disposition that comply with the sanction schedule during fiscal years 2007 through 2012.
Table 2.6: Percent of orders or stipulations to informal disposition that comply with the sanction schedule during fiscal years 2007 through 2012.
Final Orders or Stipulations to Informal Dispositions Complying with Guideline Rule
MQAC NCQAC Other HSQA Boards /
Commissions
Secretary Professions
Pre-Pilot Compliance with Guidelines (FY 2007-2008)
60.0% 84.8% 82.3% 97.0%
Pilot Period Compliance with Rules (FY 2009-2012)
99.2% 95.7% 90.7% 90.6%

Health Systems Quality Assurance Division HB 1103 Report 31 SECTION 1
Performance Measure 2.7: Sexual misconduct cases transferred to the Secretary of Health within 14 days HB 1103 Sec. 5 designated the Secretary as the sole disciplining authority in cases where the complaint alleges only an act or acts of sexual misconduct without clinical expertise or standard of care issues. This provision is codified in RCW 18.130.062:
With regard to complaints that only allege that a license holder has committed an act or acts of unprofessional conduct involving sexual misconduct, the Secretary shall serve as the sole disciplining authority in every aspect of the disciplinary process, including initiating investigations, investigating, determining the disposition of the complaint, holding hearings, preparing findings of fact, issuing orders or dismissals of charges as provided in RCW 18.130.110, entering into stipulations permitted by RCW 18.130.172, or issuing summary suspensions under RCW 18.130.135. The board or commission shall review all cases and only refer to the Secretary sexual misconduct cases that do not involve clinical expertise or standard of care issues.
The purpose behind this law was to decrease the time needed to investigate and take disciplinary action on cases that do not require the special knowledge and expertise of board and commission members. Because this provision did not exist prior to 2008, there is no pre-pilot data to compare. Chart 2.7 documents how promptly boards and commissions refer sexual misconduct cases to the Secretary once they have determined the case does not involve standard of care or clinical expertise. Chart 2.7: Cases involving sexual misconduct where the board or commission determines it does not involve standard of care or clinical expertise and transfers the case to the Secretary within 14 days, November 2008 through June 2012.
0.0%
20.0%
40.0%
60.0%
80.0%
100.0%
MQAC NCQAC Other HSQA Boards and Commissions
Percent of Sexual Misconduct Cases Transferred Within 14 Days November 2008 - June 2012
33 34 Cases Cases
30 Cases

Health Systems Quality Assurance Division HB 1103 Report 32 SECTION 1
Table 2.7: Cases involving sexual misconduct where the board or commission determines it does not involve standard of care or clinical expertise and transfers the case to the Secretary within 14 days, November 2008 through June 2012.
MQAC NCQAC Other HSQA Boards / Commissions
Sexual misconduct cases identified 34 cases 33 cases 30 cases
Cases transferred to the Secretary within 14 days
34 cases (100%)
33 cases (100%)
25 cases (83.3%)
Cases returned to board or commission due to clinical expertise or standard of care issues
7 cases (20.6%)
10 cases (30.3%)
3 cases (10%)
PERSONNEL AND BUSINESS PROCESSES ACTIVITY COMPARATIVE ANALYSIS This section describes efforts by HSQA, MQAC and NCQAC to improve personnel and business process efficiencies as a result of the 2007 State Auditor’s final report and performance measures established under HB 1103. Table 3.a: Staffing levels during the HB 1103 pilot period.
Fiscal Year MQAC FTE (full-time equivalents)
NCQAC FTE HSQA FTE HSQA, MCQAC & NCQAC Total
FY2009 34 26 385 445 FY2010 34 26 382 442 FY2011 35 34 420 489 FY2012 39 37 441 517 FY2013 37 37 449 523
Note: HSQA full-time equivalent (FTE) allotments include staffing for the thirteen health profession boards as well as the Chiropractic Quality Assurance Commission and Dental Quality Assurance Commission. HSQA FTEs exclude the Public Health Emergency Preparedness and Response unit, managed at the agency level in the Office of the Secretary. HSQA staffing increased from 385 FTE in July 2008 to 449 FTE as of July 2012. The majority of staffing increases were the result of the addition of new health professions and other legislative requirements, and decision packages to increase the credentialing, disciplinary, and regulatory performance of HSQA, MQAC and NCQAC. The total increase resulted in 64 FTE for HSQA, three FTE for MQAC, and eleven FTE for NCQAC.

Health Systems Quality Assurance Division HB 1103 Report 33 SECTION 1
Performance Measure 3.1: Number of completed investigations v. number of investigators. This measure compares the number of investigations completed to the investigator staffing levels for three groups of investigators: HSQA’s Office of Investigation and Inspection (OII), and investigation staff for MQAC and NCQAC. OII conducts investigations for all health professions except those regulated by MQAC and NCQAC. OII has the additional responsibility of investigating complaints alleging the unlicensed practice of any health profession, as well as cases involving sexual misconduct without clinical expertise or standard of care issues. Chart 3.1: Investigations completed per investigator each month during fiscal years 2010, 2011 and 2012.
During the baseline period of March through June 2009, on average OII completed 8.4 cases per investigator each month, MQAC completed 9.1 cases per investigator each month, and NCQAC completed 6.9 cases per investigator each month. Prior to the HB 1103 pilot period, OII provided investigator staffing for MQAC and NCQAC, so no pre-pilot comparison data is available for MQAC and NCQAC investigation staffing. During the three years from July 2009 to June 2012, on average OII investigators completed an average of 7.4 cases per investigator each month, MQAC investigators completed an average of 9.2 cases per investigator each month, and NCQAC completed an average of 8.0 cases per investigator each month. Performance Measure 3.2: Number of completed investigations that are assigned to a staff attorney for legal review or production of documents v. number of staff attorneys. This measure assesses average case load per staff attorney7
. It includes active cases which had been forwarded from investigation but excludes cases resulting from initial applications which are generally resolved with a notice of determination. It also excludes cases found to be in compliance and closed cases.
7 Staff attorneys are the department’s in-house legal staff. They prepare documents related to the disciplinary process and resolve the majority of cases through settlement negotiations.

Health Systems Quality Assurance Division HB 1103 Report 34 SECTION 1
Note: In Chart 3.2, “HSQA/NCQAC” reflects both HSQA and NCQAC investigations. NCQAC uses HSQA’s Office of Legal Service (OLS) staff attorneys, whereas MQAC employs separate staff attorneys. Chart 3.2: Average number of investigations assigned to a staff attorney.
Prior to the HB 1103 pilot period, OLS provided legal staffing for MQAC and NCQAC, so no pre-pilot comparison data is available for the commissions’ legal staffing. Between July 2009 and June 2012, caseloads were assessed on a monthly basis. OLS (for HSQA and NCQAC) had an average total caseload of 1,188 cases during FY2010, while the MQAC legal unit had an average total caseload of 288. The average staff attorney caseloads were 89.8 and 57.7, respectively. The high average case level in OLS was largely due to low staffing levels. Using the workload staffing model described after performance measure 3.3 below, attorneys were added in the second quarters of fiscal year 2011 and in fiscal year 2012 to bring staffing levels up to the current 20 staff attorneys. This allowed OLS to reduce average case loads per staff attorney from almost 90 cases in fiscal year 2010 to 50.9 cases in the fourth quarter of fiscal year 2012. At the same time the MQAC legal unit reduced the average caseload per staff attorney from 57.7 cases in fiscal year 2010 to 39.9 in the fourth quarter of fiscal year 2012.
Performance Measure 3.3: Percent of employee evaluations completed on time.
HSQA, MQAC and NCQAC adopted Performance Measure 3.3 to assess the percent of employee performance evaluations completed on time. This measure mirrors the agency-wide target of 100% on-time evaluation completions. Completion rates were tracked and reported on a semi-annual basis, for employee evaluations due between the January 1 - June 30, and July 1 - December 31 periods. The pre-pilot baseline for comparison was the completion rate for fiscal year 2008 – 65%. Since prior to the HB 1103 pilot HSQA

Health Systems Quality Assurance Division HB 1103 Report 35 SECTION 1
provided staffing for MQAC and NCQAC, no pre-pilot data is available for these Commissions.
Between July 1, 2009 and June 30, 2012, HSQA, MQAC and NCQAC evaluation completion rates were 93%, 96% and 94%, respectively. Approximately 1,285 evaluations were due and 1,198 were completed on-time.
Chart 3.3: Percentage of employee evaluations completed on time.
95% 96% 94%
0%
20%
40%
60%
80%
100%
HSQA MQAC NCQAC
Percent of Evaluations On-Time
Evaluations done within timeline Evaluations overdue
BUDGETARY ACTIVITY COMPARATIVE ANALYSIS Performance measure 4.1: Operating expenditure versus actual budget, and Performance measure 4.2: Revenue generated versus operating expenditures. Two measures were developed to monitor programs’ budget management. The first compares spending to allotment, the second compares spending to revenue. Results of both performance measures are displayed together in Chart 4.1/4.2. Budget data is reviewed on a quarterly basis. The goal of these measures is that program spending be within allotment and sustainable from program revenue. In some cases program allotment exceeds revenue received during the period. This is possible because the programs compared in this measure have the ability to use unspent revenue from prior biennia. HSQA program budgets were grouped into four comparison groups: MQAC, NCQAC, other HSQA boards and commissions, and Secretary professions.

Health Systems Quality Assurance Division HB 1103 Report 36 SECTION 1
Chart 4.1/4.2: Revenues generated compared to actual budget (allotment) and operating expenditures for HSQA boards/commissions, Secretary professions, MQAC and NCQAC during fiscal years 2011 and 2012.
Each profession is required by RCW 43.70.250 to be self supporting. Revenues for healthcare professions are deposited into one account, but are managed by the individual profession. The account is required to maintain a positive balance (reserve) from one biennium to the next. The four groups of professions depicted in the graphs all had positive revenue balances at the beginning of fiscal year 2011. This chart shows that each comparison group spent less than it received in revenue and allotment in fiscal years 2011 and 2012. The division as a whole (including MQAC and NCQAC) spent 18 percent less than allotment and 22 percent less than revenue. This compares favorably to the pre-pilot baseline, fiscal year 2008, where spending exceeded allotment by roughly 2 percent and revenue by 24 percent. REGULATORY ACTIVITY COMPARATIVE ANALYSES Beginning in FY 2006, HSQA management recognized that reducing the time period to adopt rules was needed to meet its strategic goals and to help protect and improve the public health. Prior to FY 2006, the average time to adopt a health profession standard rule was 22.8 months. An informal guideline was established to complete less complex standard rules within 12 months, and to finish more complex standard rules in not more than 30 months. The overall goal was completing standard rules in an average of 18 months or less; this goal was carried over into performance measure 5.1.
0.0 0.5 1.0 1.5 2.0 2.5
Q1 Q2 Q3 Q4 Q1 FY11 FY12
$ Millions
NCQAC
Revenue Allotment Expenditure
0.0 1.0 2.0 3.0 4.0 5.0
Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 FY11 FY12
$ Millions
Other HSQA Boards and Commissions
0.0 0.5 1.0 1.5 2.0 2.5
Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 FY11 FY12
$ Millions
MQAC
0.0 1.0 2.0 3.0 4.0 5.0
Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 FY11 FY12
$ Millions
Secretary Professions
0.0 0.5 1.0 1.5 2.0 2.5
Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 FY11 FY12
$ Millions
NCQAC

Health Systems Quality Assurance Division HB 1103 Report 37 SECTION 1
“Standard” rules are WAC revisions that require filing of the three primary rule making public notices under Part III of chapter 34.05 RCW, the Washington Administrative Procedure Act:
• Preproposal statement of inquiry notice (CR-101); • Proposed rule making notice (CR-102) and mandatory public hearing/comment
period; and • Permanent rule making order (CR-103P final adoption notice).
Performance Measure 5.1: Rules adopted within eighteen months. Performance was measured starting from the date a CR-101 notice was filed initiating rule making, to the date a CR-103P notice was filed formally adopting the final rule. Other types of abbreviated rule making (expedited, exception and emergency rules) are not included in performance measure 5.1.8
Since a rules performance standard was initiated, timeliness has generally improved for MQAC, NCQAC, other HSQA boards and commissions, and Secretary profession and cross-profession rules. From FY 2006 through FY 2012, the average time to adopt a standard rule fell from 22.8 months to the current average of 17.4 months. Table 5.1: Number of standard rules adopted and percent of standard rules in place within 18 months of filing the CR-101 for fiscal years 2006 through 2012.
Rules adopted based on fiscal year initiated, and Percent of adopted rules meeting Performance Measure 5.1
MQAC Rules NCQAC Rules Other HSQA Board/Commission
Rules
Secretary Profession and
Cross-Profession Rules
Pre-pilot Performance FY 2006 through FY 2008
3 rules
67%
3 rules
67%
33 rules
70%
15 rules
80%
Pilot Period Performance FY 2009
n/a 1 rule
100%
11 rules
72.7%
5 rules
60%
Pilot Period Performance FY 2010
1 rule
100%
4 rules
100%
9 rules
88.9%
3 rules
100%
Pilot Period Performance FY 2011
n/a n/a 1 rule
100%
1 rule
0%
Pilot Period Performance FY 2012
n/a n/a 1 rule
100%
n/a
Rulemaking moratorium 2010-12. As noted previously, Executive Orders 10-06 and 11-03 suspended non-critical rule making through December 31, 2012. As a result, work on 19 health profession rules was stopped in November 2010. About 40 other rule revisions that did not meet moratorium standards as critical were delayed to 2013.
8 Expedited rules under RCW 34.05.353 do not require a CR-101 or public hearing, but do require an expedited rule proposal notice (CR-105) and waiting period prior to final adoption. Exception is a DOH designation of rules that are exempt from filing of a CR-101 notice under RCW 34.05.310(4). Emergency rules under RCW 34.05.350 are temporary and cannot become permanent without completing a standard or exception rule making process.

Health Systems Quality Assurance Division HB 1103 Report 38 SECTION 1
Executive Orders 10-06 and 11-03 will impact the ability of the department and health boards and commissions to meet Performance Measure 5.1. Each of the 19 rules suspended in 2010 will have been inactive for more than 25 months - none of these rules will meet the performance target.

Health Systems Quality Assurance Division HB 1103 Report 39 SECTION 1
NATIONAL RESEARCH REGARDING REGULATORY EFFECTIVENESS AND PATIENT SAFETY HB 1103 directed the department, MQAC and NCQAC to review summaries of national research and data on regulatory effectiveness and patient safety. The two seminal works on health regulatory structures and effectiveness, referenced in many later studies or reports, are Shimberg’s 1980 “Occupational Licensing: A Public Perspective,” and reports emanating from the Pew Commission’s comprehensive Taskforce on Health Care Workforce Regulation in the 1990s. The following are brief summaries from these two sources and other national research and data reviewed for this report.
Shimberg evaluates five models of regulatory board management. In “Occupational Licensing: A Public Perspective” Benjamin Shimberg describes five models of licensing board organization: 9
• Model A: All boards are autonomous. All regulatory and administrative functions are separate between boards.
• Model B: All boards are autonomous, but less so than in Model A. Boards have control over licensing matters, discipline and staffing. But a central agency may be responsible for housekeeping functions such as space management, fee collection, issuing credentials and other routine functions.
• Model C: Boards are autonomous in many areas, but a central agency has greater authority over budgets, personnel, records, and possibly complaints, investigations or disciplinary hearings, even when the boards continue to approve disciplinary actions.
• Model D: Boards are not fully autonomous. The central agency may provide a wide range of services, or the boards may delegate certain authorities or functions to the central agency, such as preparing/scoring examinations, setting professional standards, or recommending disciplinary action. Certain board actions may be subject to review by the central agency.
• Model E: The regulatory system is run by the agency head, or a commission/council with final decision-making authority on all substantive matters. Individual boards, if they do exist, are strictly advisory. The central agency may delegate functions to the individual boards.
Shimberg reviewed how regulatory boards are organized in all 50 states, and found that Washington State’s health regulatory boards and many other boards followed model D, while certain other non-health profession boards in the state followed models B or C. (At that time, Shimberg classified the previous board for hearing aid dealers and fitters under model C. That group’s regulatory functions are now incorporated into the Washington State Board of Hearing and Speech.)
9 Shimberg, Benjamin, with Esser, Barbara, and Kruger, Daniel. “Occupational Licensing – A Public Perspective.” Center for Occupational Assessment, Educational Testing Service 1982.

Health Systems Quality Assurance Division HB 1103 Report 40 SECTION 1
Pew taskforce offers ten recommendations on health care regulation reform. The Pew Commission’s Taskforce on Health Care Workforce Regulation in 1997 offered ten new approaches to improve to health care workforce regulation.10
1. States should use standardized and understandable language for health professions regulation and its functions to clearly describe them for consumers, provider organizations, businesses, and the professions.
Some of these recommendations have been implemented in Washington State:
2. States should standardize entry-to-practice requirements and limit them to competence assessments for health professions to facilitate the physical and professional mobility of the health professions.
3. States should base practice acts on demonstrated initial and continuing competence. States should explore pathways to allow all professionals to provide services to the full extent of their current knowledge, training, experience and skills.
4. States should redesign health professional boards and their functions to reflect the interdisciplinary and public accountability demands of the changing health care delivery system.
5. Boards should educate consumers to assist them in obtaining the information necessary to make decisions about practitioners and to improve the board’s public accountability.
6. Boards should cooperate with other public and private organizations in collecting data on regulated health professions to support effective workforce planning.
7. States should require each board to develop, implement and evaluate continuing competency requirements to assure the continuing competence of regulated health care professionals.
8. States should maintain a fair, cost-effective and uniform disciplinary process to exclude incompetent practitioners to protect and promote the public’s health.
9. States should develop evaluation tools that assess the objectives, successes and shortcomings of their regulatory systems and bodies to best protect and promote the public’s health.
10. States should understand the links, overlaps and conflicts between their health care workforce regulatory systems and other systems which affect the education, regulation and practice of health care practitioners and work to develop partnerships to streamline regulatory structures and processes.
National scope of practice advisory board recommended. The Citizen Advisory Center (CAC) in 2010 recommended forming a nationwide advisory board to assist state legislatures and regulatory agencies seeking to adopt or revise laws affecting health profession scope of practice.11
10 Gragnola, Christine M., and Stone, MD, Elizabeth. “Considering the Future of Health Care Workforce Regulation.” Responses from the field to the Pew Health Professions Commission’s December 1995 report. December 1997.
CAC noted, “Presently, scope of practice laws and the process by
11 Swankin, David A, LeBuhn, Rebecca, and Gulish, Artem. “Reforming Scopes of Practice – Building a Better Mousetrap to Address Scope of Practice Issues.” Citizen Advocacy Center, July 2010.

Health Systems Quality Assurance Division HB 1103 Report 41 SECTION 1
which they are enacted and amended in the majority of states are inadequate to address workforce and access to care challenges. Nor do they properly or consistently reflect health professionals’ education and training. The creation of a national-level advisory organization composed of experts from variety of different professions, consumer representatives, economists and policy experts would go a long way toward bringing rationality and consistency to scope of practice decisions. This Scope of Practice Advisory Board will have to be formed, administered and funded in ways that uphold its credibility in the field and protect its independent professional judgment from any undue influence. Such organization could provide state legislatures with an unbiased source of evidence and expert opinion on which to base legislative scope of practice decisions.” CAC suggested that this group would be a public-private partnership between the federal government, the health care industry and the public. The national board would track data on safety and quality of care research, educational requirements, initiatives by health professions, as well scope of practice laws of the states. CAC toolkit for scope of practice laws and regulation. In a related 2010 whitepaper to its recommendations on a national scope of practice advisory board, the CAC suggests that state address their health care scope of practice laws and regulations to more effectively deal with shortages in the health care workforce and to meet the growing demand for health care practitioners under federal Patient Protection and Affordable Care Act.12
“Depending on how they are written and implemented, scope of practice laws (and regulations) either limit or promote access to care, thereby affecting the quality and cost of services for millions of consumers,” CAC said. And though many professions encourage members to learn new skills that could enable them to provide services outside their current scope of practice, CAC said outdated scope laws tend to create an environment where turf battles emerge as professions seek to protect the status quo, adding, “This ‘turf battle’ mentality results in politically focused decision-making that marginalizes if not discounts the greater public interest and consumers’ need for access to quality care.”
In many states, CAC noted that artificial scope of practice restrictions prevent providers in rural areas from practicing to the full extent of their qualifications and training, affecting access to health care to rural residents, particularly the elderly. This white paper cites a 2009 University of Washington School of Medicine-WWAMI (Washington, Wyoming, Alaska, Montana, Idaho) Rural Health Research Center policy brief noting the shortage of primary care providers in rural communities, which also points out that these communities rely more heavily on non-physician providers.13
Six professions recommend states change their approach to scope of practice regulation. Building on work by Shimberg, a 2007 report by the national associations of boards regulating the nursing, medical, social worker, physical therapy, and pharmacy professions, plus the national
12 LeBuhn, Rebecca, Swankin, David, and Gulish, Artem. “Reforming Scopes of Practice, Empowering Non-Physician Providers to Meet the Health Care Needs of Consumers and Communities – A Tool Kit.” Citizen Advocacy Center, August 2010. 13 “The Crisis in Rural Primary Care.” University of Washington School of Medicine WWAMI Rural Health Research Center, April 2009.

Health Systems Quality Assurance Division HB 1103 Report 42 SECTION 1
certifying group for occupational therapists, recommended that states dramatically change the way they approach scope-of-practice disputes, based on the following assumptions:14
• The purpose of regulation, i.e., public protection, should have top priority in scope-of-practice decisions rather than professional self-interest.
• Changes in scope of practice are inherent in our healthcare system.
• Collaboration between the health professions should become the professional norm.
• Overlap among health professions is necessary.
• Practice acts should require licensees to demonstrate that they have the requisite training and competence to provide a service.
GAO: Inability of related agencies to coordinate common functions creates barriers to efficiency. A 2000 U.S. General Accounting Office report looked at the inability of military branches to integrate their common administrative and support services, including their medical departments, into a single coordinated agency. The report found, in part, that:15
• Decision makers and managers are finding that achieving results on public problems increasingly calls for effective interagency coordination
• Agencies encounter a range of barriers when they attempt such coordination • Implementation of …crosscutting programs is often characterized by numerous individual
agency efforts that are implemented with little apparent regard for the presence of efforts of related activities
• Missions that are not mutually reinforcing or that may even conflict, making reaching a consensus on strategies and priorities difficult
• A significant barrier is agencies' concerns about protecting jurisdiction over missions and control over resources
• Interagency coordination is often hindered by incompatible procedures, processes, data, and computer systems
Impact of licensing to the quality and cost of health care services. A 2003 Minnesota analysis of several studies found that higher levels of health profession licensing tended to increase net quality to consumers while also increasing the cost of health and earnings to practitioners.16
14 “Changes in Healthcare Professions’ Scope of Practice: Legislative Considerations,” NCSBN and Association of Social Work Boards (ASWB), Federation of State Boards of Physical Therapy (FSBPT), Federation of State Medical Boards (FSMB), National Board for Certification in Occupational Therapy (NBCOT),, and National Association of Boards of Pharmacy (NABP), February 2007
Quality for consumers is increased, they noted, because minimum qualifications or examination requirements allow only those individuals to practice who meet licensing standards. Conversely, the researchers found that higher licensing standards tend to raise the cost of health care (and practitioner earnings) because there are fewer practitioners to serve a population. The analysis also found that mobility in health care occupations into a state with tougher standards is significantly reduced.
15 “Managing for results: Barriers to Interagency Coordination.” United State General Accounting Office, Report to the Chairman, Committee on Governmental Affairs, U.S. Senate, March 2000. Publication GAO/GGD/00-106. 16 Kleiner, Morris M. “Occupational Licensing and Health Services – Who gains and who loses?” University of Minnesota and the National Bureau of Economic Research. Hearings before the Federal Trade Commission and Department of Justice, June 10, 2003.

Health Systems Quality Assurance Division HB 1103 Report 43 SECTION 1
Integrated “Family of Plans” recommended to encourage performance measure linkages. The U.S. General Accounting Office in 1999 studied 23 state and federal agencies that used performance management and measurement processes.17
Among the GAO’s findings was that successful organizations needing to coordinate performance efforts agency wide used an integrated “family of plans” linking strategic goals and measures to operational and support goals, measures and related activities. The report said these organizations found that “a family of plans (approach) helped prevent the occurrence of contradictory plans across the organization.” These organizations also developed a hierarchy of plans recognizing that different levels of the organization needed different performance information, and that goals, objectives and measures become more meaningful if they relate to the appropriate level of responsibility and control over outcomes.
Interstate task force recommends balancing public health and safety with free enterprise. A Council of State Governments taskforce studying dental practice acts in various states developed suggested scope of practice legislation in 1979 for the dentistry profession.18
• Protecting public health and safety of the consuming public was the foundation on which all state dental practice acts and other health regulatory legislation should be based
Its work was guided by two concepts:
• Public health and safety should be protected with a minimal amount of governmental interference with the free enterprise system of providing health care services.
The taskforce acknowledged the policy dilemma of balancing the risk to the public with a free economy. But rather than regulate certain aspects of a profession, such as mode or practice or numbers of auxiliary staff a practitioner employs, the task force suggested that adequate enforcement would be a more effective approach to these problems. The group also recommended that auxiliary staff have a scope of practice that would include all of the potential functions that they may perform based on education and training, with three degrees of supervision defined. The taskforce said that a practice should be allowed to incorporate general, specialty, and other related health care providers, and that ownership restrictions on health care practices should be removed. Colorado studies alternatives to primary health care delivery in rural and underserved areas; Recommends health data gathering by a central regulatory agency. The state of Colorado commissioned a 2008 study of the scopes of practice, research and other data regarding advanced practice nurses, physician assistants and dental hygienists to determine the potential impact to quality of care of these professional practicing independently in rural or underserved areas.19
17 “Managing for Results – Strengthening Regulatory Agencies Performance Management Practices.” U.S. General Accounting Office – Report for the Chairman, House of Representatives Committee on Banking and Financial Services, October 1999.
Among the study’s findings was that health care data gathering should be housed within a centralized regulatory agency and require health profession licensing boards to collect data on practice settings and practitioners. Deficits in data gathering impact policy making and monitoring, and result in suboptimal estimates of health care workforce supply and
18 “State Regulatory Policies – Dentistry and the Health Professions.” The Council of State Governments. February 1979 19 “Collaborative Scopes of Care Advisory Committee – Final Report on Findings.” Prepared by Colorado Health Institute for the SOC Advisory Committee. December 30, 2008.

Health Systems Quality Assurance Division HB 1103 Report 44 SECTION 1
distribution. The report said, “Effective and informed policymaking assumes the availability of objective and reliable data, both to frame policy actions and then to monitor the implementation of policies once enacted.”
Washington among 25 states that check national health profession databases, and among 33 states that do FBI background checks on new credential applications. In an informal survey of all 50 state credentialing agencies for physicians and physician assistants, osteopathic physicians, and podiatrists, HSQA found that half of the states, including Washington, check the federal government’s two health profession data bases for new applicants, the Healthcare Integrity and Protection Data Bank (HIPDB) or the National Practitioner Data Bank (NPDB). HSQA checks both databases for all applicants, as do 21 other states (MQAC also checks the American Medical Association profile for physician and PA applicants). HIPDB provides the following information:
• Credential actions, including revocation, reprimand, suspension (and duration), censure, probation, voluntary surrender, or other action resulting in loss of the credential or right to apply.
• Health care related civil judgments or criminal convictions • Exclusion from participating in federal or state health care programs • Other adjudication actions
NPDB collects the following information:
• Medical malpractice payments • Adverse licensing actions • Adverse clinical privilege actions • Adverse professional society membership actions • Medicare/Medicaid exclusions
Health profession regulatory agencies in 33 states conduct a finger-print based FBI background check. HSQA does an FBI background check for every applicant from outside Washington, and whenever a Washington State Patrol “WATCH” in-state criminal history check is not available for the applicant or the WATCH results are determined to be inadequate.