hours worked by general practitioners (gps) and waiting times ... - business &...
TRANSCRIPT

Hours worked by General Practitioners (GPs) and waiting
times for primary care 1
Megha Swamia 2, Hugh Gravelleb, Anthony Scottc, Jenny Williamsd
aMelbourne Institute of Applied Economic and Social Research and Department of Economics,
University of Melbourne
bCentre for Health Economics, University of York, UK
cMelbourne Institute of Applied Economic and Social Research, University of Melbourne
dDepartment of Economics, University of Melbourne
Abstract:Waiting times are an important measure of access to health services. Delay in
receiving primary care can affect patient health and increase use of hospitals. One of the key
factors contributing to the rising concern about accessibility to primary care are the changing
workload patterns and labour supply of General Practitioners (GPs) with increasing proportions
of GPs working shorter hours. Examining the effect on access to primary care of labour supply
at the intensive margin (hours of work) is important since GP supply at the extensive margin is
inflexible in short to medium run. We investigate the effect of hours worked by general practi-
tioners (GPs) on waiting times for GP appointments using panel data on 3,561 GPs from first
seven waves (2008-2014) of the Medicine in Australia: Balancing Employment and Life (MA-
BEL) survey of Australian doctors. We use both GP fixed effects and instrumental variables to
allow for the possible endogeneity of hours worked due to both time-invariant and time-varying
unobserved factors that might be correlated with GPs labour supply and waiting times. We also
1The authors would like to thank Tamara Taylor, the MABEL Data Manager, for assistancewith the Survey data. This study used data from the MABEL longitudinal survey of doctorsconducted by the University of Melbourne and Monash University (the MABEL research team).Funding for MABEL comes from the National Health and Medical Research Council (HealthServices Research Grant: 2008-2011; and Centre for Research Excellence in Medical WorkforceDynamics: 2012-2016) with additional support from the Department of Health (in 2008) andHealth Workforce Australia (in 2013).The MABEL research team bears no responsibility forhow the data has been analysed, used or summarised in this study.
2Correspondence to: Faculty of Business and Economics (FBE), University of Melbourne, 111Barry Street, Carlton VIC 3053, Australia. E-mail: [email protected]

control for a rich set of individual GP characteristics, practice features and characteristics of the
practice location. Our results suggest that waiting times do respond to changes in hours worked
by GPs. An increase in the average hours worked by 10 percent would reduce average waiting
time for a patient by about 12 percent. These results are largely driven by female GPs, who
work much fewer hours than male GPs due to a significant negative effect of childbearing on
women labour supply. We also find that quality indicators such as qualifications and experience
are associated with higher waiting times, and GPs working in relatively affluent areas and those
in areas with higher GP density have lower waiting times.
Keywords: waiting times; primary care; labour supply; fixed-effects; Instrumental
Variable model; MABEL Survey
2

1 Background and Motivation
Health care services play an important role in the welfare of the population in a
country and hence timely access to health care is vital for welfare. In markets
for most goods and services, the money price acts as a rationing mechanism to
equilibrate demand and supply. However, in health care markets public or private
insurance means that consumers either face a zero or below market clearing price
and rationing occurs through waiting times (Martin and Smith, 1999). Therefore,
waiting times are an important measure of access to health care.
Primary health care is typically the first point of contact with the health care
system and plays an important role in the diagnosis and management of patients’
health problems. However, concerns about access to primary health care services
has been growing in many countries (Sarma et al., 2011). On one hand, demand
for primary health services is increasing due to changing health needs, increased
prevalence of chronic diseases and ageing populations. On the other hand, changes
in the workload patterns and supply of General Practitioners (GPs) have become
an important issue in many countries including Australia, Canada and United
States (Crossley et al., 2009; Kirch and Vernon, 2008; Sarma et al., 2011). Research
indicates that young doctors are working less than their predecessors (Sarma et al.,
2011) and there has been an overall decline in the hours of direct patient care
(Crossley et al., 2009). In Australia too, there has been a significant decline in the
proportion of GPs working more than 40 hours in direct patient care from 41.8%
in 2003-04 to 30.6% in 2013-14 (Britt et al., 2013). These reductions in hours
worked by doctors are primarily attributed to the increasing proportion of female
doctors, ageing of the medical workforce and a shift of preferences towards greater
work-life balance (Crossley et al., 2009; Joyce et al., 2006; Kirch and Vernon, 2008;
Shrestha and Joyce, 2011). However, there is currently very little understanding of
how these changes in the labour supply of doctors influence access to health services
1

in general and in particular, waiting times in primary care. This is important since
medical training is a lengthy and costly process, and there are licensing restrictions
on entry into the medical profession. This makes supply at the extensive margin
inflexible in the short to medium run. As a result, a decline in the hours worked
by GPs could reduce the supply of ‘effective full-time practitioners’ 3 (Joyce et al.,
2006). Hence, changes in hours of work can have important implications for access
to primary care services.
In this study, we investigate the extent to which GP hours worked affect
waiting times for appointments with GPs. We perform the analysis separately
for female and male GPs since within-gender analysis controls for unobservable
gender-differences in productivity and practice styles which might affect demand
for consultations and waiting times. Further, as in other labour markets, research
on medical workforce suggests that female doctors on average work fewer hours
than their male counterparts (Gravelle and Hole, 2007; Kalb et al., 2015).
To answer our research questions, we first provide a simple theoretical frame-
work. The empirical analyses use the Medicine in Australia: Balancing Employ-
ment and Life (MABEL) panel survey of Australian doctors. The MABEL survey
provides the opportunity to study the impact of hours worked on waiting times as
it has unique information on the workload - both waiting times and hours worked,
of individual doctors. It also has rich data on doctors’ personal characteristics,
postgraduate qualifications, location, practice settings and style, which are likely
to affect demand and hence waiting times (Campbell et al., 2005; Cheraghi-Sohi
et al., 2008; Gandhi et al., 1997; Gerard et al., 2008; Scott, 2000; Scott and Vick,
1999; Scott et al., 2003; Turner et al., 2007).
We use panel data methods to control for unobserved heterogeneity at the indi-
vidual level. This mitigates the risk of omitted variable bias due to time-invariant
3It refers to a modified count of doctors, equivalent to FTE (Full Time Equivalent) practi-tioners. (http://www.phcris.org.au/fastfacts/fact.php?id=4833)
2

unobserved GP characteristics that might be correlated with both labour supply
decisions of the GPs and the waiting times, for example a GP’s intrinsic moti-
vation and passion towards his/her work. We also employ instrumental variables
(IV) to account for any time-varying unobserved factors correlated with both hours
worked and waiting times, for example, changing complexity of patients. The IV
approach will also address the concern about possible reverse causality between
hours worked and waiting times, which could arise if GPs respond to high waiting
times by increasing the hours worked. Regressing waiting times on hours worked
without taking into account these potential sources of endogeneity, we would ex-
pect to find a positive correlation between hours worked and the error term, which
would bias the expected negative estimated effect of hours worked on waiting times
upwards towards zero.
We find that waiting times for appointments respond to hours worked by GPs:
an increase in the average hours worked by a GP of 10 percent would reduce
the average waiting time by about 12 percent. This is largely driven by female
GPs who work much fewer hours than their male counterparts. We also find that
waiting times are affected by demand side factors including GP’s quality attributes
such as education and experience, and the socioeconomic status of the area and
GP density.
The study makes several contributions to the existing literature. It is the
first study to directly examine the impact of doctors’ labour supply decisions
on waiting times in primary care, using rich MABEL survey which has unique
information on waiting times for individual doctors and their labour supply. We
use instrumental variable methods to address the issue of time-varying omitted
variables and potential reverse causality between waiting times and labour supply,
in addition to exploiting panel data techniques to control for endogeneity due to
unobserved heterogeneity at individual level and unobserved time-invariant factors.
3

Moreover, we study waiting time for the preferred doctor and hence take into
account the patient-doctor relationship and the availability of continuous care.
This is important because patients generally prefer to see the same or a familiar
GP overtime (Guthrie and Wyke, 2006; Nutting et al., 2003; Rubin et al., 2006;
Schers et al., 2002) and there is evidence that patients are willing to wait longer
to see their preferred doctor (Rubin et al., 2006; Turner et al., 2007).
Delays in receiving primary care are costly not only in terms of risk of dete-
rioration of patients’ health condition, but also in terms of increased hospital or
emergency department use. Given that countries like Australia and U.K. are im-
plementing programs to encourage general practices to extend the working hours
(Department of Health and Ageing - Medicare Australia, 11; Department of Hu-
man Services, 2015b; Department of Health and Prime Minister’s Office U.K.,
2013), and Spain is implementing policies to extend the working hours of its Na-
tional Health System (NHS) personnel (Luigi et al., 2013), our study provides
insights about the extent to which such policy interventions could be helpful in
combating waiting times and improving access to primary care.
1.1 Empirical evidence on waiting time elasticities
There is a considerable body of research on waiting times in the health economics
literature which recognises that waiting times are determined by the interaction of
demand for and supply of health services when money prices cannot adjust to clear
the market. The bulk of literature focuses on hospital (non-emergency elective)
waiting times (Cullis and Jones, 1986; Goddard et al., 1995; Gravelle et al., 2003;
Iversen, 1993; Lindsay and Feigenbaum, 1984; Martin and Smith, 1999), with the
majority of studies outlining models to examine the responsiveness of demand for
and supply of hospital care to waiting times or waiting lists, using both cross-
sectional and longitudinal data (Gravelle et al., 2003; Martin et al., 2003). These
4

studies suggests that demand for hospital care is negatively associated with waiting
times (although relatively inelastic with elasticity estimates less than -0.5 in most
studies) and the supply is positively associated with waiting times. However, in
most of the studies the supply side is modeled relatively simply and lacks important
supply side features, such as availability of health personnel - doctors and allied
health professionals, which are central to supply capacity. This is primarily due
to the lack of available information on resources used by health providers.
Waiting times for primary care are a policy concern in several OECD countries
including Australia, Canada, U.K. and Sweden (Siciliani et al., 2013) but much
less studied by economists. The existing literature on accessibility to primary care
does not focus on waiting times as a measure of accessibility and is primarily based
on patient surveys. The majority of these studies focus on variation in reported
access by patients’ demographic characteristics such as age, gender, location and
self-reported health (Kontopantelis et al., 2010; Muggah et al., 2014; Young et al.,
2000) and find that being female, older in age, living in urban areas and having
better self-reported health is positively associated with better access to primary
care. Very few studies have looked at waiting times in primary care and those that
do, find that income and private insurance lead to faster access to GP care (Roll
et al., 2012). However, all of these studies provide information only about the
demand side of the market and they are mostly cross-sectional in nature. Hence,
results only suggests associations.
Therefore, there is a paucity of research on how waiting times in primary care
are affected by supply side factors. This is crucial in designing policies necessary
to ensure timely access to GP services in the face of rising demand for primary
health care.
Section 2 describes the institutional background to Australian health care.
Section 3 sets out the conceptual framework used for empirical analyses, section 4
5

describes the data and section 5 the empirical analyses including the econometric
method and results. The study concludes with a discussion of the results.
2 Institutional Context: General Practitioners
in Australia
GPs are the most commonly accessed primary health service in Australia and act
as gatekeepers to specialist care. Eighty two percent of Australians consulted a
GP at least once in previous 12 months in 2013-14 and the figure was eighty one
percent in 2012-13 (ABS, 2014). GPs primarily work in private practices with
various ownership arrangements and operate on a fee-for-service basis. Medicare
Australia sets out fixed subsidies or rebates for a range of GP services in the
Medicare Benefit Schedule (MBS) and GPs are free to set the level of their fees at
or above the MBS rebate, which acts as a floor price. However, Medicare provides
financial incentives to GPs to charge equal to the rebate amount i.e. bulk-bill,
for Commonwealth Concession Card holders and children under 16 years of age
(Department of Human Services, 2015a) with higher incentives in regional, rural
and remote areas (Rural and Regional Health Australia, Department of Health,
2015), and in this case patients pay no out-of-pocket costs.
Overall, around eighty percent of GP services are bulk-billed in Australia
(MBS, 2014). However, practices have distinct business models and practice styles.
For example, large corporate practices usually have a high volume-low price busi-
ness model where they bulk-bill all or most of their patients and see a high volume
of patients with short consultations. This usually occurs in areas of low socio-
economic status where price elasticities are relatively higher. On the other hand,
practices may bulk-bill only a small proportion of their patients and see a lower
number of patients, usually in more affluent areas (Gravelle et al., 2013). Patients
6

are free to choose any general practice and can visit any GP of their choice as
there is no compulsory patient list or registration system.
There has been a steady decline in the number of general practices in Australia,
from 8,309 practices in 2000-01 to 7,035 in 2010-11, owing to increases in practice
sizes (Carne, 2013). As a result, more than 90% of GPs are now working in group
practices and the majority of practices are located in metro areas (Britt et al.,
2013). General practices are characterized by group practice comprising GPs,
practice nurses and allied health professionals, and most general practices provide
prevention and early intervention services like immunization, and diabetes and
mental health programs.
3 Conceptual Framework: A simple model of
waiting time and hours worked for a GP
To explain how labour supply decisions of a GP might affect waiting times we use
a simple demand and supply framework. The demand for consultations with a GP
can be written as4:
D = D(w, q;xd, εd) (1)
where w is the waiting time, q is a measure of GP’s quality, xd is a vector of
exogenous demand shifters - socioeconomic characteristics such as income, educa-
tion, health status, age-distribution, etc., of local population and it also includes
other exogenous factors such as availability of substitutes and measure of compe-
tition. εd is the unobserved error which captures the effect of unmeasured factors
4See Cheraghi-Sohi et al. (2008); Gandhi et al. (1997); Gerard et al. (2008); Gravelle et al.(2003); Martin et al. (2003); Scott (2000); Scott and Vick (1999); Scott et al. (2003); Turneret al. (2007) for related literature and theoretical models.
7

shifting demand.
The model assumes that the GP bulk-bills all patients who therefore face a
zero price. We believe that this assumption is reasonable, given the institutional
context of Australia and the fact that most (80.3 % in 2013-2014) GP services are
bulk-billed in Australia (MBS, 2014).
On the supply side we assume that all consultations with a GP have the same
length (exogenously determined) t. Hours worked per week by the GP is denoted
h and n is the number of consultations per week with the GP. The number of
hours worked is h = nt, assuming that GPs spend all their time in direct patient
care.
The waiting time is determined by the market clearing condition that demand
for consultations D(.) equals the number of consultations supplied by the GP n:
D(w, q;xd, εd) − n = 0, Dw < 0, Dq > 0 (2)
The equilibrium waiting time is thus
w = w(q, n;xd, εd) (3)
which is very similar to the waiting time equation specified in Gravelle et al.
(2003) and Martin et al. (2003). Waiting time will decrease with the number of
consultations and hence hours worked, and will increase with higher quality:
wn = −−1
Dw
=1
Dw
< 0 (4)
8

and
wq = −Dq
Dw
> 0 (5)
Assuming that the GP bulk-bills all patients and so gets a fixed Medicare rebate
m per patient, the GP’s revenue will depend on the number of consultations she
has. She incurs financial costs of practicing which is given by c(n, q;xc, εc) where xc
are observed factors such as wage rates for allied health and administrative staff
and εc is the unobserved component that affects costs. The GP has exogenous
non-work income y0. The GP utility is
u = u(y, h, xg, εg) (6)
where y = y0 +mn− c(n, q;xc, εc), xg denote GP’s personal characteristics such as
age, gender, children, etc., and εg is an unobserved preference shifter. GP chooses
her hours h = nt of work to satisfy
uh + uy[m
t− cn
1
t] = 0 (7)
or
uht+ uy[m− cn] = 0 (8)
and so the number of hours of work is:
h = h∗(m, t, q, xc, xq, εc, εg) (9)
9
The supply of consultations is:
n = h∗(m, t, q, xc, xg, εc, εg)/t = n∗(m, t, q, xc, xg, εc, εg) (10)
From (3) and (10), the equilibrium waiting time is given by:
w = w∗(q, n∗(m, t, q, xc, xg, εc, εg), xd, εd) = w∗(q, h∗(m, t, q, xc, xg, εc, εg)/t, xd, εd)
(11)
We want to estimate the effect of hours worked on waiting times and so es-
timate (11), rather than reduced form w0(q,m, t, xc, xg, xd, εc, εg, εd). Section 5.2
discusses the issues in estimating (11) and how we address them in our empirical
analysis.
The above model considers consultation length as exogenous. This means that
we assume that a GP does not change the length of her consultations in response
to changes in waiting times, that is, it is not a choice variable in our waiting
time model. We argue that this is a reasonable assumption because of two main
reasons. First, research from Australia as well as United States and European
countries indicates that consultation length is determined to a large extent by the
nature of the problems managed during the consultation, the characteristics of
the patients such as age and gender (Britt et al., 2005; Deveugele et al., 2002;
Sayer et al., 2000) which are exogenous; and GP characteristics such as GP’s age,
gender, type of medical training (which is specific to the country and health care
system). These GP characteristics are likely to be time-invariant and hence length
of standard consultation can be thought as a measure of exogenous practice style
(Schurer et al., 2015). Practice-related factors such as practice type and location
are also found to be associated with consultation length (Bensing et al., 2003; Britt
10

et al., 2005; Deveugele et al., 2002). Our model incorporates all these factors.
Second, in Australia most general practices follow a fixed appointment scheduling
system where patients can book only 15-20 minutes’ appointments with the GPs
for a standard level B consultation5 6. In section 5, we test this assumption
empirically by using the number of patients (visits) seen (n in the model) instead
of hours worked as the main independent variable. n combines hours worked h
and consultation length t as per the theoretical model and we test whether using
n makes any qualitative difference to the results.
The model is a simple representation of the relationship between a GP’s hours
worked and waiting time and emphasizes the effect of GP’s labour supply decisions
on waiting time for consultation with her. Under reasonable assumptions the
model provides a framework for empirical examination of the effect of hours worked
on waiting times.
4 Data
We use data from the first seven waves (2008 to 2014) of the Medicine in Australia:
Balancing Employment and Life (MABEL) panel survey of Australian doctors.
The MABEL survey is tailored to four groups of clinicians - General Practitioners
(GPs), specialists, specialists in training and hospital non-specialists and provides
exceptionally rich data on these doctors’ workload, place of work, qualifications,
personal characteristics and family circumstances. The baseline 2008 cohort in-
cludes 10,498 Australian doctors including 3,906 GPs, 4,596 specialists, 1,072 spe-
cialists in training and 924 hospital non-specialists. The cohort was found to
5Level B consultation is defined as - Professional attendance involving taking a selectivehistory, examination of the patient with implementation of a management plan in relation to oneor more problems OR a professional attendance of less than 20 minutes duration (Britt et al.,2004)
6For evidence see: https://healthengine.com.au/
11

be nationally representative with respect to age, gender, geographic location and
hours worked. In the subsequent waves a new cohort of doctors was invited to par-
ticipate each year as a top-up sample. The methods of study and characteristics
of the baseline cohort are discussed in more detail in Joyce et al. (2010).
4.1 Waiting times and hours worked
Our dependent variable is the waiting time for an appointment with the GP in
the practice, in days. Each wave of the MABEL survey asks GPs to report on
three types of waiting times in their practice: ‘Excluding emergencies or urgent
needs, for how many days does a patient typically have to wait for (i) ’you’ their
preferred doctor in the practice (ii) any doctor in the practice, and (iii) waiting
time for a new patient in the practice? (please write average number of days)’.
For the analysis we use the responses to question (i) i.e. waiting time for ‘you’ the
preferred GP in the practice, since we are interested in examining the impact of a
GP’s labour supply decisions on his/her waiting time.
MABEL provides detailed information on the labour supply of doctors. In
addition to total hours worked, the doctors are asked to report the number of
hours worked in their most recent usual week at work in direct patient care, in-
direct patient care, educational activities, management and administration; and
also by various public and private settings - private medical practitioner’s rooms
or surgery, community health centre or other state-run primary care organization,
public and private hospital, residential/aged care health facility, aboriginal health
service, government department, tertiary education institution and others. Doc-
tors are also asked to report the number of patients they provided care in the most
recent usual week at work. On average GPs report spending most of their working
hours in private practice and in direct patient care (more than 80% of total hours
worked).
12

We use total hours worked as our measure of labour supply and use the infor-
mation on working hours from other questions to check for any reporting inconsis-
tencies (discussed in section 4.3). We believe that total hours is a better measure
of labour supply choice and is less likely to be measured with error. This is impor-
tant because we instrument for hours worked in our analysis using a set of family
characteristics and such instruments are likely to better explain the decision on
total hours. In a robustness check, we conduct our analysis using hours worked in
direct patient care per week to test whether it makes any qualitative difference to
the results.
4.2 Covariates
4.2.1 Personal characteristics
We use individual GP characteristics to control for factors that might influence
demand for consultations with the GP in the practice and hence waiting times.
We include GP’s standard consultation length (minutes per patient) as a proxy
for practice style. In the analysis with all GPs, we include GP gender as this
may affect the demand for their consultations, for example female patients might
prefer to see a female GP. Moreover, gender is also found to be associated with
labour supply decisions of doctors (Gravelle and Hole, 2007; Kalb et al., 2015).
We proxy for GP’s quality attributes using several variables. First, we include age
group, measured in five year bands, as a measure for GP’s experience 7. Second,
we include whether the GP is an Australian medical graduate, since graduating
from an Australian medical school (as opposed to an overseas school) may be
perceived by patients as higher quality. Third, we include whether the GP has a
7We also have information on ‘Years since graduation’ for each GP but it is not used becauseit will be perfectly collinear with year fixed effects for those GPs on which we have observationsfor consecutive years.
13
post graduate qualification or Fellowship with a college.
We use a set of dummy variables capturing family characteristics as instruments
for hours worked in the Instrumental Variable (IV) model of waiting times (see
section 5.2). The set of binary instruments are: 1) Single GP (reference category),
2) GP with no dependent child and a partner who does not work or works part
time 3) GP with no dependent child and a partner who works full time, 4) GP
with a dependent child aged 5 years or under and a partner who doesn’t work,
5) GP with a dependent child aged 5 years or under and a partner who works
part time, 6) GP with a dependent child aged 5 years or under and a partner who
works full time, 7) GP with a dependent child aged over 5 years and a partner
who doesn’t work or works part time, 8) GP with a dependent child aged over 5
years and a partner who works full time, 9) Single GP with a dependent child.
These family characteristics are likely to be strongly correlated with labour supply
decisions (relevance), but seems unlikely to directly influence waiting times and
hence likely to be uncorrelated with the error term (validity).
4.2.2 Practice related characteristics
We control for GP tenure in current practice (in years) which might influence de-
mand. For this we use information from responses to the following question in
the Survey - ‘When did you start working at this practice (year)?’ asked to new
doctors in each wave. We also use information on the distance the GP has moved
practice since she last completed MABEL. We include the proportion of patients
bulk-billed by the GP and GP’s contract or employment type - principal/partner,
associate, contracted/salaried employee or locum/others. GP’s who are partners
or associates (self-employed) have more control over their hours and salary which
is likely to affect their productivity and earnings (Schurer et al., 2015) which might
influence labour supply decisions. Their contract may also affect their financial
14

incentives and hence influence prices (Gravelle et al., 2013) and patient volume.
Further, being a principal/partner might also be associated by patients with se-
niority and higher quality. These are likely to affect the demand for GP in the
practice, and hence waiting times.
To allow for the effect of economies scale on practice costs and hence GP
productivity and efficiency (Damiani et al., 2013; Olsen et al., 2013; Reinhardt,
1972), we also control for size of the practice, measured by the total number of GPs
in the practice and also control for number of nurses, allied health professionals
and administrative staff in the practice.
4.2.3 Area measures
We include several GP practice postcode area level measures to capture factors
which may affect demand for primary care which is likely to be correlated with
both waiting times and hours worked. We control for the location of GP’s practice,
distinguishing between three categories based on Australian Standard Geographic
Classification (ASGC) of rurality: major city, regional (outer and inner) and re-
mote.
Patients’ socioeconomic status has been found to be negatively associated with
demand for primary care (Van Doorslaer et al., 2008; Van Doorslaer and Masse-
ria, 2004) and waiting times (Roll et al., 2012). It is also likely to affect price
elasticity of demand (Gravelle et al., 2013; Johar, 2012; Johar et al., 2014) and
this might influence practice’s choice of business model. We use Socio-Economic
Index for Areas (SEIFA) of Relative Socio-Economic Advantage and Disadvantage
constructed by Australian Bureau of Statistics census. It is based on measures of
income, education, occupational structure and employment status in a small area,
where higher values correspond to greater advantage. We match these to GPs on
the basis of their practice’s postcode.
15

We control for age distribution of the population in each postcode: the percent-
age of the population under 5 years of age and above 65 years of age, and distance
to nearest emergency department (in kilometers) as a measure of availability of
substitutes. We also include the number of GPs per 1000 population, at postcode
level8, as a measure of competition for GPs.
4.3 Analysis sample
The initial sample size of the unbalanced panel from seven waves of the Survey
for GPs is 24,609 observations on 6,707 GPs. Sample restrictions are used to take
into account inconsistencies and outliers. First, observations are excluded if the
difference between reported number of working hours across different questions in
the survey and total hours worked is greater than or equal to 5 hours9. Secondly,
to drop the outliers from the analysis, observations were not included if total hours
worked per week were less than 4 hours or greater than 75 hours a week10 or if
the waiting time for an appointment with the GP was reported to be greater than
30 days11. Similarly, other variables such as number of patients seen, standard
consultation length, number of GPs, nurses, allied health professionals and admin-
istrative staff, were checked for outliers and were coded missing correspondingly12.
The sample size with non-missing data on all variables of interest is 16,140 obser-
vations on 5,126 GPs. For the analysis, the sample was restricted to GPs with
8This data is based on Australian Medical Publishing Company (AMPCo) and 2011 Censusdata
9This was true in 1,058 cases or 4.5% of non-missing data on hours worked (23,612 observa-tions). This leaves 22,554 non-missing observations on hours worked.
10This was true in 1,011 cases or 4.48% of 22,554 observations.11This was true in 355 cases or 1.6% of 22,301 non-missing observations on waiting time.12‘Number of patients seen’ was coded missing if it was reported to be less than 10 or greater
than 300 per week; length of standard private consultation was coded missing if it was reportedto be less than 5 minutes or greater than 30 minutes; number of GPs was coded missing ifreported more than 30 GPs in practice; number of nurses, allied and administrative staff werecoded missing if reported greater than 30, 10 and 10 respectively.
16

at least two observations across seven waves, leaving 14,589 observations on 3,575
GPs in the estimation sample. Out of the 3,575 individual GP observations, 11%
are present in all seven waves, 15% each in six, five and four waves, 18% in three
waves and 26% in two waves.
5 Empirical Analysis
5.1 Descriptive analysis
Table 1 and 2 present the summary statistics of all variables for the analysis
sample. Half of GPs in the sample are females and aged 50 years or over. The
average waiting time for appointment with a GP is around 4 days, with female
GPs having higher average waiting time of 4.28 days compared to 3.76 days for
male GPs. Male GPs work 43.35 hours per week and female GPs works 31.64
hours per week on average, or about 73% of male weekly hours. Figures 1 and 2
show the distribution of waiting times and total hours worked. Most GPs have
waiting time less than 5 days, where male GPs have higher relative frequency of
zero waiting times (in days) as compared to their female counterparts (Figure 1).
Figure 2 reveals that female GPs work fewer hours than male GPs, with female GPs
working mostly work between 20 to 40 hours per week, while male GPs mostly
work between 35 to 55 hours per week. Moreover, the observed distribution of
hours worked indicates that for both part-time (less than 35 hours a week) and
full-time hours, ranges are fairly well covered.
On average female GPs have standard consultation length of 16.89 minutes,
about 14% longer than male GPs (14.76 minutes). Figure 3 shows the distribution
of consultation length. For both female and male GPs, the distribution is tight and
centered around 15 minutes, suggesting that most GPs spend around 15 minutes
per patient for a level B consultation.
17

Overall 74% of GPs are Australian medical graduates with 61% having post-
graduate degree or Fellowship of a college and mostly (67%) located in cities. Male
GPs bulk-bill a higher proportion of their patients, about 65%, as opposed to fe-
male GPs who bulk-bill about 56% of their patients13. Female GPs are more likely
to work in larger practices and as salaried/contracted employee. They are also
more likely work in areas with higher socio-economic status and GP density. Male
GPs are more likely to have a partner who is not working or working part time
and less likely to have dependent children aged under 5 years.
The standard deviations between GPs and within each GP over time indicates
the extent of variation in the sample. Overall the variation between different GPs
is larger than within a GP overtime, but there is still sufficient within variation
in waiting times and labour supply variables (columns 5-6 in Table 1 and columns
3-4 and 7-8 in Table 2). There is not much variation in consultation length, both
between and within GPs, with length of standard consultation varying less than 4
minutes between different GPs and less than 2 minutes for a GP over time (as also
suggested by the distribution of consultation length in Figure 3). This indicates
that our assumption of exogeneity of consultation length in the theoretical model
is reasonable, where most GPs have standard consultation length between 15-20
minutes for a standard level B consultation and a GP on average doesn’t change
his/her consultation length much over time.
For area level measures, the between variation is much larger than within vari-
ation, which is not surprising because area level measures are based on 2011 census
data and hence do not change overtime for an area (post code). Therefore, within
GP variation only results when a GP changes his workplace location (post code).
The between variation in family characteristics (instruments) is larger than
13It should be noted that the survey asks GPs to report proportion of patients bulk-billed,while the figure of 80% reported by (?) is based on the proportion of GP services (not patients)bulk-billed. A GP might to choose to bulk-bill some services and not bulk-bill others from thesame patient and hence the bulk-billing proportions reported in the survey are likely to be lower.
18

within variation, but there is still sufficient within variation. Figures 4 and 5
present the average hours worked for different family types for female and male
GPs. Overall, single GPs are not much different in their hours worked (both
total and direct patient care) from those having a partner but no dependent child,
irrespective of the employment status of the partner. For female GPs, having a
dependent child aged under 5 years and a partner who works seems to be associated
with significant reduction the average hours worked, with the reduction being
higher if partner works full time. Also, even if the dependent child is more than
5 years old, having a partner who works full time is associated with lower hours
worked. This indicates that, both having a young dependent child and employment
status of the partner are likely to play important role in labour supply decisions of
female GPs. For male GPs, there seems to be no significant relationship between
having a dependent child and employment status of the partner, and hours worked.
This suggests that our instruments are likely to work relatively better for female
GPs than for male GPs.
5.2 Econometric analysis
Based on the conceptual framework our baseline regression model is given by:
Wit = β0 + β1hit + β2Xit + λt + εit (12)
where Wit is the waiting time for GP i in year t, hit is the total hours worked; Xit
is a vector of control variables - GP characteristics, practice characteristics and
area level measures discussed in the section 4.2. λt is the year effect which controls
for shocks that affect waiting times for all GPs (cross-sectional dependence) such
as episodes of seasonal infections or an outbreak of some illness such as flu. We
19

estimate (12) for all GPs and separately by gender, using two types of models -
GP fixed effects and Instrumental Variable (IV), in addition to simple Ordinary
Least Squares (OLS) model.
5.2.1 GP fixed effects
The GP fixed effects model exploits the within-individual variation in both waiting
times and hours worked over the panel, mitigating endogeneity resulting from
the confounding effects of unobserved individual GP heterogeneity that might be
correlated with both waiting times and total hours worked. For example, a GP’s
intrinsic motivation and passion towards her work is likely to affect her choice of
hours and at the same time the demand for her consultations and hence waiting
times. This would result in endogeneity due to positive correlation between hit
and εit, biasing the estimates upwards (towards zero).
5.2.2 Instrumental Variables
As long as the omitted factors are time-invariant, such as GP’s interpersonal skills
and professional ethics which might affect quality and hence demand, GP fixed
effects model will remove the potential bias. However, if there are unobserved
omitted variables that are time-varying such as complexity of patients, then the
potential bias will not be removed by inclusion of GP fixed effects. We therefore
an employ instrumental variable approach to test and correct for this potential
endogeneity, using a set of binary variables capturing different family types to
instrument for hours worked. The IV approach will also address the potential
issue of reverse-causality between waiting times and hours worked which could
arise if GP’s change their hours in response to changes in waiting times.
We also estimate IV with GP fixed effects (FEIV) model. Although this model
will provide the most robust estimates since it mitigates the potential bias from
20
both unobserved time-invariant as well as time-varying omitted factors and can
be interpreted as causal, it is quite demanding since it requires sufficient within
variation in instruments, in addition to the dependent and main explanatory vari-
ables. As Tables 1 and 2 indicate, between GP variation is larger than within-GP
variation in the data. However, there is still sufficient within variation even when
we slice the sample by gender.
The IV/FEIV method will be inefficient in the presence of heteroscedasticity
and so this is tested using the Pagan and Hall statistic (Baum et al., 2007). If the
null hypothesis of homoscedasticity is rejected, then two-step Generalised Method
of Moments (GMM) is used which is robust to heteroscedasticity of unknown form
and thus more efficient than the standard IV estimator (Hayashi, 2000). Further,
we use C or GMM distance test to test for endogeneity of total hours worked14.
Unlike Durbin-Wu-Hausman test of endogeneity, this test is robust to various
violations of conditional homoscedasticity.
We first ran IV models for all GPs and then separately for male and female
GPs. The F statistic on the (excluded) instruments and partial R-squared in
the first stage GP total hours worked model was used to test for weak identifi-
cation. Kleibergen-Paap rk LM statistic was used to test for under-identification
and Hansen J statistic was used for testing the over-identifying restrictions (Baum
et al., 2007). As expected, the instruments were unsatisfactory for male GPs’ hours
and we were unable to find any other instruments for male hours. We therefore
report estimates only from OLS and GP fixed models for male GPs.
All Models were estimated with heteroscedastic robust standard errors and
clustering by individual GP to allow for within-GP error correlation.
14Conducted using endog option in STATA’s ivreg2 command. Under conditional homoscedas-ticity, this endogeneity test is numerically equivalent to a Hausman test.
21

5.3 Estimation results
5.3.1 Results for all GPs
Table 3 reports results from OLS, GP fixed effects, IV and FEIV models for all GPs.
The first column reports the OLS results. The coefficient on total hours worked
is positive and significant, indicating that higher hours worked is associated with
longer waiting times. As argued before, this is likely to be the result of strong
endogeneity of hours worked15. Once we control for GP fixed effects in column 2,
the coefficient becomes statistically insignificant16. However, the inclusion of GP
fixed effects corrects only for that part of the endogeneity problem that arises from
time-invariant individual GP heterogeneity. As discussed earlier, the total hours
worked is likely to be positively correlated with the error term due to time-varying
unobserved confounding factors and possible reverse-causality between total hours
worked and waiting times and this will bias the coefficient on hours towards zero.
To address these issues, we instrument for hours worked with a set eight binary
variables capturing different family types using single GP as the reference category
in columns 3 and 4. Once instrumented for, the effect of total hours worked
increases in magnitude and becomes negative. The IV model (column 3) exploits
the between-GP variation and results in a coefficient of -0.066 on total hours
worked, suggesting that an hour increase in total hours worked per week by a
GP is associated with a reduction in waiting times of about 32 minutes for an
appointment with the GP 17. The FEIV model exploits within-GP variation and
leads to a larger in magnitude effect with coefficient of -0.125 on total hours worked,
15This was tested using Durbin-Wu-Hausman test and it confirmed the endogeneity of hoursworked.
16The Hausman-Wu was applied and it rejected random effects in favour of the fixed effectsmodel with a p-value of 0.000, indicating a significant correlation between time-invariant omittedvariables and observed variables.
17We interpret the coefficients assuming 8 hours working day. So coefficient of -0.066 means areduction of 0.066 x 8 hours x 60 minutes = 31.68 minutes.
22

suggesting that an hour increase in total hours worked per week would reduce
waiting time for appointment with the GP by about 60 minutes. In terms of
elasticity, the FEIV model suggests that a 10 percent increase in average hours
worked by a GP would reduce the average waiting time by 11.7 percent.
The instruments work better in case of the IV model (F statistic = 41.09
(p < 0.000), partial R2 = 0.048), as compared to FEIV model (F statistic = 17.16
(p < 0.000), partial R2 = 0.018) given the larger between than within variation
in data, but they are still sufficiently strong in case of FEIV. Both IV and FEIV
models pass the under-identification and over-identifying restrictions tests18. The
C or GMM distance test of endogeneity confirmed the endogeneity of total hours
worked in both IV and FEIV models, with null hypothesis of exogeneity strongly
rejected at 1% level of significance. Table A1 in the appendix presents the results
of the first stage regression19. As expected, having a dependent child aged under
5 years is associated with a significant reduction in total hours worked, and this
negative effect is heightened by the presence of a partner who works full time.
Comparing results from OLS to GP fixed effects and IV models allows us to
identify the main source of endogeneity. When we move from OLS (column 1)
to IV (column 3) we eliminate the endogeneity bias resulting from time-varying
omitted factors and potential reverse-causality between total hours worked and
waiting times, and by doing so the hours worked coefficient becomes significantly
negative from significantly positive. On the other hand, when we only eliminate
bias caused by individual GP heterogeneity by using GP fixed effects (column 2),
the coefficient on hours worked becomes insignificant but remains positive. This
18The null hypothesis for Kleibergen-Paap rk LM test of under-identification is that equationis under-identified, which is rejected in our case with p < 0.000. For Hansen J test of over-identifying restrictions which is a test of validity of instruments, the null hypothesis is thatinstruments are valid and it is not rejected with p < 0.402 in case of IV and p < 0.376 in case ofFEIV.
19All appendix tables are available on request.
23

suggests that most of the endogeneity (positive correlation between total hours
worked and the error term) is resulting from time-varying unobserved confounding
factors and possible reverse-causality.
5.3.2 Results for Female GPs
Table 4 reports the results from OLS, GP fixed effects, IV and FEIV models for
female GPs. As expected, the instruments work well for female GPs. They are
stronger in case of IV model (F = 42.85, Partial R2 = 0.100) than in FEIV model
(F = 14.74, Partial R2 = 0.038), but are still satisfactory in FEIV model. Total
hours worked are found to be endogenous using both the C or GMM distance
test (P-values reported in Table 8) and Durbin-Wu-Hausman test (p < 0.000).
The hours worked get a negative coefficient of -0.042 in the IV model but not
statistically significant. The FEIV model results in a larger in magnitude and
significantly negative effect of total hours worked on waiting times (coefficient of
-0.096), with estimate suggesting that an hour increase in total hours worked per
week would reduce waiting time for an appointment by about 46 minutes, or in
terms of elasticity, a 10 percent increase in average hours worked would reduce the
average waiting time by 7.1 percent. Table A2 in the appendix presents the results
of the first stage regression and it confirms that the negative effects of having a
dependent child on hours worked are primarily driven by female GPs. Having a
dependent child aged under 5 years and a partner who works full time is associated
with a reduction in female GP labour supply of about 13 hours a week as compared
to a single female GP without a young dependent child (column 1).
5.3.3 Results for Male GPs
For male GPs we do not find any significant negative effects of hours worked
on waiting times in GP fixed effects model (Table 5). Due to instruments be-
24
ing unsatisfactory for male GPs we could not test and correct for endogeneity of
hours worked resulting from time-varying unobserved factors and potential reverse-
causality between waiting times and hours. Hence, unable to identify any effects.
5.3.4 Effect of covariates
The effect of personal and practice characteristics, and area measures are consistent
across the models for all GPs and separately for female and male GPs. Female
GPs have higher waiting times. This is perhaps because females GPs are perceived
to have better interpersonal skills or because female patients may prefer to consult
a female GP.
GPs who spend more time per patient, who graduated from an Australian
medical school or have a post graduate qualification or Fellowship of a college,
have higher waiting times. This suggests that these characteristics are associated
by patients with higher quality. GP’s age (a proxy for experience) has a non-linear
effect on waiting time. Waiting time increases with age till the GP is aged between
55 to 59 years, but then age is found to have no effect or negative effect on waiting
times, suggesting that patients prefer to consult GPs who are neither too young
nor too old.
Tenure in the practice is also found to be positively associated with waiting
times, with waiting times increasing with tenure but at a decreasing rate. This
indicates that patients prefer to consult GPs who have been in the practice for
longer, suggesting preference for continuity of care. There is no strong evidence
that percentage of patients bulk-billed is associated with waiting times, suggesting
that prices charged are unlikely to be associated with waiting times.
Employed GPs (contracted/salaried or working as locum) have lower waiting
times compared to GPs who are principals or partners in the practice. One expla-
nation for longer waiting times for principals/partners in a practice is that these
25

GPs are considered as having higher quality and hence patients are willing to wait
more for such GPs. The coefficient on number of nurses is positive and signifi-
cant in several models, suggesting that practices with high waiting times might be
employing more nurses20.
Regional (for both female and male GPs) and remote (for female GPs) areas
have higher waiting times as compared to major cities. GPs in higher socioe-
conomic areas have lower waiting times which is consistent with what has been
found in the waiting time literature (Cooper et al., 2009; Laudicella et al., 2012;
Roll et al., 2012; Sharma et al., 2013; Siciliani and Verzulli, 2009; Sudano and
Baker, 2006). GPs in areas with higher proportion of elderly people have higher
waiting times, particularly female GPs, reflecting that elderly have higher demand
for primary health care. Waiting times are lower in areas with higher GP density,
suggesting a negative effect of competition on waiting times.
5.3.5 Sensitivity analyses
We carry out a number of sensitivity tests to investigate the robustness of the
results to alternative measures of GP’s labour supply and sample restrictions.
5.3.6 Alternative measure of labour supply
We estimated models with two separate measures of GP labour supply. First,
we use hours worked in direct patient care as the measure of labour supply to
test if that makes any qualitative difference to our results. Moreover, it allows us
to understand whether increase in hours spent in direct patient care and corre-
sponding decrease in hours spent in administrative and other activities can serve
as a means to lower waiting times without changing total hours worked. Second,
20This means that number of nurses are endogenous, but since it is a control variable in ourmodel and not our main independent variable, this does not affect our model and estimationstrategy.
26

to test the sensitivity of results to the assumption of exogeneity of consultation
length, we estimate models using number of patients (visits) seen per week as
the main explanatory variable. As per the theoretical model, number of patients
combines hours worked and consultation length into one variable and can be used
as an alternative measure of GP labour supply. If the assumption of exogenous
consultation length is reasonable then we should get qualitatively similar results21.
The results are reported in Table 6 and for brevity, only coefficient on hours
worked in direct patient care per week, and on number of patients seen per week
are reported. GP fixed effects model (column 2) results in negative and significant
(at 10% level) effect of hours worked in direct patient care for all GPs overall and
female GPs. The results of IV and FEIV models, however, remain qualitatively
similar for both all GPs and female GPs. The instruments are relatively weaker
for direct patient hours, particularly in FEIV model. As discussed before, this is
because our instruments capture family characteristics which are likely to explain
the choice of total hours worked relatively better than the hours spent in direct pa-
tient care, which might also be affected by other factors in the practice22. In case of
the IV model, the results indicate that hours spent in direct patient care are likely
to be associated with a relatively greater reduction in waiting times. It suggests
that spending more time in direct patient care and less time on administrative and
other work, can help reduce waiting times.
When we use ‘number of patients (visits) seen per week’ as the main explana-
tory variable in place of hours worked and consultation length, the instruments are
21We could not find any instrument for consultation length and hence could not formallytest for endogeneity. In this case, using number of patients seen as main explanatory variableprovides an alternative way to test the robustness of the results to the assumption of exogeneityof consultation length
22Both the C or GMM distance test and Durbin-Wu-Hausman test indicated that hours workedin direct patient care are endogenous at 5% level in case of all and female GPs, however, theP-values of both the test statistics were slightly larger as compared to those in case of total hoursworked.
27

satisfactory in case of IV model and we do get negative and significant coefficients
on number of patients seen. The estimates suggest that an extra patient seen per
week would be associated with reduction in waiting time of about 13 minutes for
all GPs overall and about 8 minutes for female GPs (column 3). Moreover, the fact
that our instruments based on family characteristics are satisfactorily explaining
number of patients seen by a GP (in IV model), indicates that consultation length
reflects practice style, i.e. longer versus shorter consultations, and hence the num-
ber of patients seen by a GP is likely to be proportional to hours worked. This
further shows that it is reasonable to assume consultation length to be exogenous
in our model.
5.3.7 Sample restrictions
In our theory model, we assumed that GP bulk-bills all patients. We therefore con-
duct our analysis only on GPs who bulk-bill 80 or more percent of their patients23.
The results are reported in Table 7 and for brevity, only coefficient on total hours
worked per week is reported. We still find negative and significant effect of total
hours worked on waiting times in case of IV model for all GPs and in addition,
find significantly negative (at 10% level) effect for female GPs. The magnitude of
the effects, however, is relatively large. In case of FEIV model, the instruments
become weak due to smaller sample size which reduces within variation in the data
and hence the estimates become imprecise.
Next, in order to test whether the results are not driven by GPs who are
principals/partners or associates in the practice who have greater control over
hours worked, we carry out the analysis separately for employed and self-employed
(principals/partners or associates) GPs. These results are also reported in Table
7. Overall the results remain qualitatively similar. However, as expected, the
23We did not use GPs who bulk-bill 100 percent of their patients because of very small samplesize to perform analysis.
28

estimates suggest that most of the endogeneity is driven by self-employed GPs.
This is possibly because GPs who are self-employed have much more control over
the hours they work and hence could alter their hours in response to unobserved
factors such as changing complexity of patients (which might also affect waiting
times). In case of all employed GPs, we still observe a negative and significant
effect of total hours worked on waiting times, although the magnitude of the effect
is slightly smaller. Due to small sample size of self-employed GPs, the instruments
become weak and hence the estimates becomes insignificant (in IV model) or less
significant (in FEIV model) due to loss of precision.
In case of female GPs, for those who are employed the negative effect of total
hours worked becomes statistically significant and increase in magnitude in IV
model. One possible explanation for finding stronger effect among employed female
GPs is that these female GPs have less control over their hours which prevents them
from flexibly adjusting their working hours to changes in exogenous circumstances
such as having a dependent child or spouse’s employment status and hence they are
more likely to reduce the hours worked in response to such external shocks. The
IV model is therefore able to identify the effects better for these employed female
GPs. In FEIV model, the coefficient remains negative but becomes insignificant
and the endogeneity test could not reject the null of exogeneity (P-value=0.140).
Hence, IV estimates are preferred. For self-employed female GPs, the sample size
is much smaller and hence most of the estimates are insignificant.
6 Discussion and conclusions
The labour supply of GPs is crucial to addressing the concerns about accessibility
to primary care services. This study examines the extent to which increasing the
labour supply at the intensive margin can reduce waiting times for appointments
29

with GPs using data from a unique Australian longitudinal survey of doctors. The
results suggest that, taking into account important demand side factors, waiting
times do respond negatively to hours worked by GPs: an increase in the average
hours worked by a GP by 10 percent would reduce average waiting time for a
patient by about 12 percent. These results are largely driven by female GPs where
our instruments are stronger.
Female GPs have longer waiting times, work shorter hours (31.64 per week
against male hours of 43.35 per week) and having dependent children significantly
reduces their labour supply at the intensive margin. On the other hand, male GPs
already work long hours and research indicates that male GPs have higher incomes
and negative wage elasticities of labour supply (Gravelle et al., 2011; Kalb et al.,
2015). Hence, it hard to provide incentives to male GPs to increase their hours
worked. Moreover, a recent study on Australian GPs found that male GPs do
not significantly alter their labour supply in response to having children (Schurer
et al., 2015). And this is the reason that we also find that family characteristics
could not satisfactorily serve as instruments for male GPs. Therefore, we are not
able to identify any significant effect of total hours worked on waiting times for
male GPs.
We find important evidence that waiting times for GPs are positively associated
with his/her quality attributes such being Australian trained, having post-graduate
qualification or Fellowship and experience, and by GP’s tenure in the practice and
employment status (principal/partner versus contracted/salaried employee). This
suggests that patients are willing to wait longer for a GP they perceive as a better
quality doctor. We also find that waiting times are lower in more affluent areas
and in areas with more competition as measured by GP density.
From policy perspective the findings of this study are important. With an
increased proportion of women in the medical workforce - the proportion of GPs
30

who are women increased from 36.5% in 2004 to 41.0% in 2014 (AIWH, 2015),
reduced labour supply by female GPs is likely to negatively affect the accessibility
to primary care services. Therefore, policy responses aimed at reducing average
waiting times in short to medium run by focusing on the intensive margin should
acknowledge the important role of female GPs and address ways of reducing the
negative effect of child-bearing on female GP labour supply. For example, by
improving child care policies and facilities for female doctors which provide them
with more flexibility in the hours they have to work enabling them to achieve
better work-life balance.
31

Table 1: Summary statistics of main variables and instruments for All GPs (N=14,544,n=3,561)
Overall S D S D
Variable Mean S D Min Max Between Within(1) (2) (3) (4) (5) (6)
Waiting time for you in practice 4.02 5.60 0 30 4.99 2.72Total hours worked per week 37.54 13.60 4 75 12.53 5.26Hours worked in direct patient care per week 31.18 12.18 4 75 11.24 4.93No. of patients (visits) seen per week 110.50 57.02 10 300 52.74 23.01
Personal characteristicsFemale 0.50 0.50 0 1 0.50 0.00Age: Under 35 0.09 0.28 0 1 0.30 0.12Age: 35-39 0.11 0.31 0 1 0.27 0.18Age: 40-44 0.12 0.33 0 1 0.26 0.21Age: 45-49 0.16 0.36 0 1 0.28 0.24Age: 50-54 0.18 0.38 0 1 0.29 0.26Age: 55-59 0.16 0.36 0 1 0.27 0.24Age: 60-64 0.10 0.30 0 1 0.23 0.20Age: 65 or over 0.09 0.29 0 1 0.27 0.12Length of std. private consultation 15.82 3.99 5 30 3.61 1.88Australian medical graduate 0.74 0.44 0 1 0.45 0.00Have post graduate qualification/Fellowship 0.61 0.49 0 1 0.46 0.16
Practice characteristicsTenure in practice (years) 9.00 9.81 0 61 9.16 3.21Total no. of GPs in the practice 7.76 4.17 1 25 3.82 1.92% of patients bulk-billed 60.56 30.15 0 100 27.78 12.29No. of nurses in the practice 2.39 1.90 0 10 1.70 0.92No. of allied health prof. & administrative staff in practice 6.18 4.20 0 30 3.59 2.38Employment type: Principal or partner 0.28 0.45 0 1 0.41 0.18Employment type: Associate 0.11 0.31 0 1 0.24 0.19Employment type: Salaried or Contracted employee 0.57 0.50 0 1 0.44 0.23Employment type: Locum or other 0.04 0.20 0 1 0.15 0.13
Area characteristicsLocation (ASGC): City 0.67 0.47 0 1 0.46 0.13Location (ASGC): Regional 0.31 0.46 0 1 0.45 0.13Location (ASGC): Remote 0.03 0.17 0 1 0.16 0.05SEIFA Index 1016.09 74.44 669.50 1213.92 70.92 23.26Percent of population under 5 yrs of age 6.03 1.40 0.43 13.34 1.32 0.52Percent of population above 65 yrs of age 13.89 4.96 0.18 43.37 4.71 1.67Min. distance to emergency department 4.62 3.53 1 19 3.29 1.29Ratio of GPs to population (per 1,000) 1.40 0.83 0.07 10.10 0.72 0.39
InstrumentsSingle 0.08 0.28 0 1 0.24 0.14No dep. child, partner doesn’t work or works part time 0.19 0.39 0 1 0.34 0.19No dep. child, partner works full time 0.11 0.32 0 1 0.28 0.18Dep. child ≤ 5 yrs, partner doesn’t work 0.03 0.16 0 1 0.13 0.10Dep. child ≤ 5 yrs, partner works part time 0.03 0.16 0 1 0.12 0.11Dep. child ≤ 5 yrs, partner works full time 0.05 0.21 0 1 0.17 0.12Dep. child > 5 yrs, partner doesn’t work or works part time 0.25 0.43 0 1 0.37 0.24Dep. child > 5 yrs, partner works full time 0.22 0.42 0 1 0.36 0.23Single, Dep. child 0.04 0.19 0 1 0.16 0.10
32

Table 2: Summary statistics of main variables and instruments by gender
Female GPs Male GPs(N=7,211, n=1,786) (N=7,333, n=1,775)
Variable Mean S D S D S D Mean S D S D S DOverall Between Within Overall Between Within
(1) (2) (3) (4) (5) (6) (7) (8)
Waiting time for you in practice 4.28 5.55 4.80 2.83 3.76*** 5.64 5.16 2.61Total hours worked per week 31.64 12.20 11.18 5.11 43.35*** 12.35 11.21 5.40Hours worked in direct patient care per week 25.79 10.63 9.76 4.54 36.47*** 11.26 10.21 5.29No. of patients (visits) seen per week 85.38 45.41 41.13 20.37 135.21*** 56.47 51.95 25.33
Personal characteristicsAge: Under 35 0.12 0.33 0.34 0.14 0.05*** 0.22 0.23 0.10Age: 35-39 0.14 0.34 0.29 0.21 0.08*** 0.26 0.23 0.15Age: 40-44 0.15 0.36 0.28 0.23 0.10*** 0.29 0.24 0.19Age: 45-49 0.17 0.38 0.29 0.25 0.14*** 0.35 0.27 0.23Age: 50-54 0.18 0.38 0.28 0.26 0.18 0.39 0.29 0.26Age: 55-59 0.13 0.34 0.25 0.22 0.18*** 0.39 0.29 0.26Age: 60-64 0.08 0.26 0.20 0.17 0.13*** 0.33 0.25 0.22Age: 65 or over 0.03 0.18 0.16 0.09 0.14*** 0.35 0.33 0.14Length of std. private consultation 16.89 4.16 3.70 2.05 14.76*** 3.52 3.19 1.70Australian medical graduate 0.78 0.42 0.44 0.00 0.71*** 0.45 0.47 0.00Have post graduate qualification/Fellowship 0.64 0.48 0.45 0.18 0.58*** 0.49 0.47 0.15
Practice characteristicsTenure in practice (years) 7.02 7.82 7.17 2.73 10.94*** 11.09 10.46 3.62Total no. of GPs in the practice 7.99 4.02 3.69 1.86 7.53*** 4.30 3.94 1.97% of patients bulk-billed 56.10 30.51 27.84 12.89 64.94*** 29.15 27.12 11.67No. of nurses in the practice 2.34 1.86 1.65 0.93 2.45*** 1.94 1.76 0.90No. of allied health prof. & administrative staff in practice 6.26 4.10 3.45 2.36 6.09** 4.30 3.71 2.39Employment type: Principal or partner 0.16 0.36 0.33 0.15 0.41*** 0.49 0.44 0.21Employment type: Associate 0.09 0.29 0.22 0.18 0.12*** 0.32 0.26 0.19Employment type: Salaried or Contracted employee 0.71 0.45 0.39 0.23 0.43*** 0.50 0.45 0.23Employment type: Locum or other 0.04 0.19 0.14 0.14 0.04 0.20 0.17 0.12
Area characteristicsLocation: City 0.71 0.45 0.44 0.14 0.62*** 0.49 0.47 0.13Location: Regional 0.27 0.44 0.43 0.14 0.35*** 0.48 0.46 0.13Location: Remote 0.02 0.15 0.15 0.06 0.03*** 0.18 0.18 0.05SEIFA Index 1028.62 74.51 71.01 25.19 1003.77 72.29 68.86 21.19Percent of population under 5 yrs of age 5.98 1.42 1.34 0.56 6.08*** 1.37 1.29 0.48Percent of population above 65 yrs of age 13.52 4.78 4.47 1.78 14.26*** 5.10 4.90 1.55Min. distance to emergency department 4.62 3.44 3.16 1.37 4.62 3.62 3.41 1.19Ratio of GPs to population (per 1,000) 1.47 0.89 0.76 0.41 1.32*** 0.77 0.67 0.37
InstrumentsSingle 0.10 0.30 0.27 0.15 0.07*** 0.25 0.22 0.14No dep. child, partner doesn’t work or works part time 0.10 0.30 0.26 0.15 0.28*** 0.45 0.39 0.22No dep. child, partner works full time 0.14 0.35 0.31 0.20 0.08*** 0.28 0.23 0.17Dep. child ≤ 5 yrs, partner doesn’t work 0.02 0.12 0.09 0.08 0.04*** 0.19 0.16 0.12Dep. child ≤ 5 yrs, partner works part time 0.02 0.13 0.09 0.09 0.03*** 0.18 0.14 0.12Dep. child ≤ 5 yrs, partner works full time 0.08 0.28 0.23 0.16 0.01*** 0.10 0.07 0.07Dep. child > 5 yrs, partner doesn’t work or works part time 0.13 0.34 0.28 0.20 0.37*** 0.48 0.41 0.26Dep. child > 5 yrs, partner works full time 0.35 0.48 0.40 0.26 0.10*** 0.30 0.25 0.18Single, Dep. child 0.06 0.23 0.20 0.11 0.02*** 0.14 0.11 0.09
Notes: The Asterisks denote significant difference in means for male GPs as compared to female GPs based on t-test of equality of means. ***, **, *significant at 1%, 5% and 10% respectively.
33

Figure 1
Figure 2
Figure 3
34

Figure 4
Figure 5
35

Table 3: Regression results for all GPs
Dependent variable: Waiting time for ’you’ in practice (days)
(1) (2) (3) (4)Independent Variables OLS GP fixed effects IV FEIV
Total hours worked per week 0.012** 0.006 -0.066** -0.125***(0.005) (0.006) (0.026) (0.043)
Personal characteristicsFemale 0.872*** - 0.217 -
(0.172) (0.299)Age: 35-39 [Excl: Under 35 years] 0.618*** 0.293 0.499** 0.162
(0.202) (0.278) (0.228) (0.280)Age: 40-44 0.897*** 0.297 0.741*** 0.372
(0.232) (0.388) (0.267) (0.389)Age: 45-49 0.969*** 0.233 0.998*** 0.637
(0.226) (0.453) (0.246) (0.469)Age: 50-54 0.963*** 0.163 1.134*** 0.709
(0.225) (0.496) (0.246) (0.527)Age: 55-59 0.567** -0.293 0.751*** 0.319
(0.233) (0.547) (0.248) (0.588)Age: 60-64 0.427* -0.466 0.410 -0.106
(0.246) (0.602) (0.280) (0.628)Age: 65 or over 0.024 -0.783 -0.662 -0.900
(0.288) (0.695) (0.415) (0.711)Practice style: Length of std. private consultation (min) 0.153*** 0.096*** 0.253*** 0.081***
(0.015) (0.018) (0.020) (0.019)Australian medical graduate 1.176*** - 0.740*** -
(0.156) (0.171)Have post graduate qualification/Fellowship 0.716*** 0.557*** 0.698*** 0.454**
(0.128) (0.192) (0.162) (0.204)
Practice characteristicsTenure in practice (years) 0.158*** 0.136*** 0.180*** 0.149***
(0.017) (0.023) (0.021) (0.024)Tenure in practice (years) squared -0.003*** -0.003*** -0.004*** -0.003***
(0.001) (0.001) (0.001) (0.001)Total no. of GPs in the practice 0.036** 0.005 0.063** -0.004
(0.017) (0.020) (0.024) (0.021)% of patients bulk-billed 0.001 0.004 0.000 0.003
(0.002) (0.003) (0.003) (0.003)No. of nurses in the practice 0.164*** 0.115*** 0.226*** 0.117***
(0.037) (0.043) (0.054) (0.044)No. of allied health prof. & admin. staff in practice 0.003 -0.011 0.055*** -0.013
(0.012) (0.013) (0.021) (0.013)Business relationship: Associate [Excl: Principal or partner] -0.200 -0.120 -0.684** -0.403*
(0.183) (0.205) (0.333) (0.234)Business relationship: Salaried or Contracted employee -0.733*** -0.446** -1.706*** -0.866***
(0.162) (0.208) (0.304) (0.260)Business relationship: Locum or other -0.877*** -0.585** -2.102*** -1.024***
(0.208) (0.247) (0.390) (0.302)
Area level characteristicsLocation (ASGC): Regional [Excl: City] 1.800*** 1.623*** 1.937*** 1.730***
(0.174) (0.287) (0.215) (0.299)Location (ASGC): Remote 1.558*** 1.123** 2.188*** 1.516**
(0.423) (0.514) (0.647) (0.607)SEIFA Index -0.006*** -0.002 -0.010*** -0.003*
(0.001) (0.001) (0.001) (0.002)Percent of population under 5 yrs of age -0.053 -0.044 -0.037 -0.039
(0.047) (0.062) (0.063) (0.066)Percent of population above 65 yrs of age 0.058*** 0.047** 0.060*** 0.049**
(0.015) (0.024) (0.016) (0.025)Min. distance to emergency department -0.056*** -0.043* -0.088*** -0.057**
(0.018) (0.025) (0.024) (0.028)Ratio of GPs to population (per 1,000) -0.179** -0.111 -0.341*** -0.082
(0.070) (0.086) (0.091) (0.087)
Year fixed effects Yes Yes Yes YesGP fixed effects No Yes No Yes
Observations 14,544 14,544 14,544 14,544R-squared 0.185 0.031 0.164 -Number of GPs 3,561 3,561 3,561 3,561
First Stage statisticsF-stat of excluded instruments [P-value] 41.09 [0.000] 17.16 [0.000]Partial R-squared of excluded instruments 0.048 0.018Underidentification test P-value 0.000 0.000Hansen J overidentification test P-value 0.402 0.376Endogeneity test P-value 0.000 0.001
Notes: Robust and clustered (at individual level) standard errors in the parenthesis. Coefficients for year fixed effectsand constant are omitted. ***, **, * significant at 1%, 5% and 10% respectively.
36

Table 4: Regression results for female GPs
Dependent variable: Waiting time for ’you’ in practice (days)
(1) (2) (3) (4)Independent Variables OLS GP fixed effects IV FEIV
Total hours worked per week 0.015** 0.005 -0.042 -0.096**(0.007) (0.009) (0.026) (0.041)
Personal characteristicsAge: 35-39 [Excl: Under 35 years] 0.902*** 0.501 0.619** 0.284
(0.250) (0.356) (0.288) (0.358)Age: 40-44 0.964*** 0.245 0.593* 0.075
(0.286) (0.518) (0.337) (0.505)Age: 45-49 0.950*** -0.012 0.778** 0.049
(0.278) (0.614) (0.308) (0.611)Age: 50-54 0.977*** -0.168 0.877*** 0.015
(0.280) (0.686) (0.319) (0.697)Age: 55-59 0.663** -0.700 0.768** -0.409
(0.305) (0.766) (0.348) (0.785)Age: 60-64 0.425 -1.177 0.494 -1.116
(0.334) (0.858) (0.400) (0.867)Age: 65 or over 0.397 -1.142 -0.428 -1.463
(0.492) (1.036) (0.559) (1.022)Practice style: Length of std. private consultation (min) 0.195*** 0.130*** 0.294*** 0.124***
(0.020) (0.024) (0.027) (0.024)Australian medical graduate 1.157*** - 0.764*** -
(0.219) (0.232)Have post graduate qualification/Fellowship 0.875*** 0.863*** 0.819*** 0.662**
(0.172) (0.248) (0.223) (0.264)
Practice characteristicsTenure in practice (years) 0.227*** 0.187*** 0.246*** 0.184***
(0.027) (0.034) (0.037) (0.034)Tenure in practice (years) squared -0.005*** -0.005*** -0.005*** -0.005***
(0.001) (0.001) (0.001) (0.001)Total no. of GPs in the practice 0.029 -0.001 0.049 -0.010
(0.023) (0.027) (0.031) (0.028)% of patients bulk-billed 0.002 0.005 0.004 0.003
(0.003) (0.004) (0.004) (0.004)No. of nurses in the practice 0.169*** 0.144** 0.204*** 0.149**
(0.056) (0.066) (0.075) (0.066)No. of allied health prof. & admin. staff in practice 0.005 -0.011 0.063** -0.017
(0.018) (0.019) (0.028) (0.019)Business relationship: Associate [Excl: Principal or partner] -0.188 -0.150 -0.835 -0.336
(0.329) (0.368) (0.521) (0.387)Business relationship: Salaried or Contracted employee -0.789*** -0.581* -1.677*** -0.877**
(0.265) (0.329) (0.446) (0.367)Business relationship: Locum or other -1.192*** -1.010*** -2.119*** -1.332***
(0.321) (0.385) (0.561) (0.430)
Area level characteristicsLocation (ASGC): Regional [Excl: City] 1.660*** 1.576*** 1.773*** 1.694***
(0.251) (0.413) (0.297) (0.421)Location (ASGC): Remote 2.123*** 2.360*** 2.315*** 2.914***
(0.639) (0.719) (0.868) (0.755)SEIFA Index -0.007*** -0.002 -0.010*** -0.003
(0.001) (0.002) (0.002) (0.002)Percent of population under 5 yrs of age -0.031 -0.013 -0.019 -0.026
(0.063) (0.080) (0.092) (0.084)Percent of population above 65 yrs of age 0.070*** 0.062* 0.073*** 0.045
(0.022) (0.036) (0.023) (0.036)Min. distance to emergency department -0.034 -0.033 -0.040 -0.042
(0.027) (0.037) (0.034) (0.040)Ratio of GPs to population (per 1,000) -0.149 -0.048 -0.302** -0.053
(0.101) (0.128) (0.120) (0.129)
Year fixed effects Yes Yes Yes YesGP fixed effects No Yes No Yes
Observations 7,211 7,211 7,211 7,211R-squared 0.198 0.043 0.189 -Number of GPs 1,786 1,786 1,786 1,786
First Stage statisticsF-stat of excluded instruments [P-value] 42.85 [0.000] 14.74 [0.000]Partial R-squared of excluded instruments 0.100 0.038Underidentification test P-value 0.000 0.000Hansen J overidentification test P-value 0.416 0.393Endogeneity test P-value 0.007 0.009
Notes: Robust and clustered (at individual level) standard errors in the parenthesis. Coefficients for year fixedeffects and constant are omitted. ***, **, * significant at 1%, 5% and 10% respectively.
37
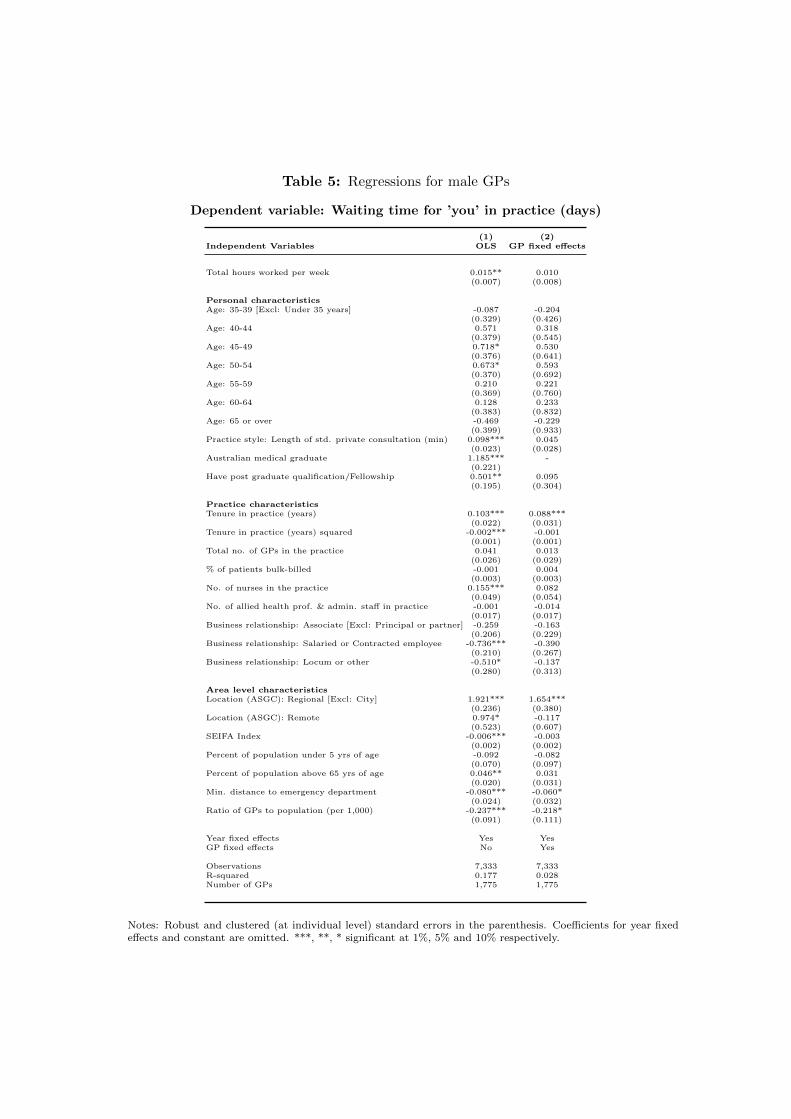
Table 5: Regressions for male GPs
Dependent variable: Waiting time for ’you’ in practice (days)
(1) (2)Independent Variables OLS GP fixed effects
Total hours worked per week 0.015** 0.010(0.007) (0.008)
Personal characteristicsAge: 35-39 [Excl: Under 35 years] -0.087 -0.204
(0.329) (0.426)Age: 40-44 0.571 0.318
(0.379) (0.545)Age: 45-49 0.718* 0.530
(0.376) (0.641)Age: 50-54 0.673* 0.593
(0.370) (0.692)Age: 55-59 0.210 0.221
(0.369) (0.760)Age: 60-64 0.128 0.233
(0.383) (0.832)Age: 65 or over -0.469 -0.229
(0.399) (0.933)Practice style: Length of std. private consultation (min) 0.098*** 0.045
(0.023) (0.028)Australian medical graduate 1.185*** -
(0.221)Have post graduate qualification/Fellowship 0.501** 0.095
(0.195) (0.304)
Practice characteristicsTenure in practice (years) 0.103*** 0.088***
(0.022) (0.031)Tenure in practice (years) squared -0.002*** -0.001
(0.001) (0.001)Total no. of GPs in the practice 0.041 0.013
(0.026) (0.029)% of patients bulk-billed -0.001 0.004
(0.003) (0.003)No. of nurses in the practice 0.155*** 0.082
(0.049) (0.054)No. of allied health prof. & admin. staff in practice -0.001 -0.014
(0.017) (0.017)Business relationship: Associate [Excl: Principal or partner] -0.259 -0.163
(0.206) (0.229)Business relationship: Salaried or Contracted employee -0.736*** -0.390
(0.210) (0.267)Business relationship: Locum or other -0.510* -0.137
(0.280) (0.313)
Area level characteristicsLocation (ASGC): Regional [Excl: City] 1.921*** 1.654***
(0.236) (0.380)Location (ASGC): Remote 0.974* -0.117
(0.523) (0.607)SEIFA Index -0.006*** -0.003
(0.002) (0.002)Percent of population under 5 yrs of age -0.092 -0.082
(0.070) (0.097)Percent of population above 65 yrs of age 0.046** 0.031
(0.020) (0.031)Min. distance to emergency department -0.080*** -0.060*
(0.024) (0.032)Ratio of GPs to population (per 1,000) -0.237*** -0.218*
(0.091) (0.111)
Year fixed effects Yes YesGP fixed effects No Yes
Observations 7,333 7,333R-squared 0.177 0.028Number of GPs 1,775 1,775
Notes: Robust and clustered (at individual level) standard errors in the parenthesis. Coefficients for year fixedeffects and constant are omitted. ***, **, * significant at 1%, 5% and 10% respectively.
38

Table 6: Results using ‘Hours worked in direct patient care per week’ and ‘No. ofpatients seen’ as measures of labour supply
Dependent variable: Waiting time for ’you’ in practice (days)
(1) (2) (3) (4)Main explanatory variable OLS GP fixed effects IV FEIV
ALL GPsHours worked in direct patient care per week -0.010* -0.011* -0.078** -0.196***
(0.005) (0.006) (0.032) (0.062)[F = 34.47] [F = 9.441]
No. of patients (visits) seen per week -0.005*** -0.001 -0.028*** -0.045**(0.001) (0.001) (0.010) (0.018)
[F = 15.44] [F = 6.428]
FEMALE GPsHours worked in direct patient care per week -0.010 -0.018* -0.046 -0.132**
(0.008) (0.010) (0.031) (0.054)[F = 40.61] [F = 11.43]
No. of patients (visits) seen per week -0.009*** -0.005** -0.017* -0.036**(0.002) (0.002) (0.010) (0.016)
[F = 23.91] [F= 8.104]
MALE GPsHours worked in direct patient care per week -0.006 -0.004 - -
(0.007) (0.008)
No. of patients (visits) seen per week -0.002 0.002 - -(0.001) (0.002)
Notes: The table only presents the coefficient on ‘hours worked in direct patient care per week’ and ‘no. ofpatients seen’ for the models for brevity. Complete tables are provided in the appendix. ***, **, * significantat 1%, 5% and 10% respectively.
39
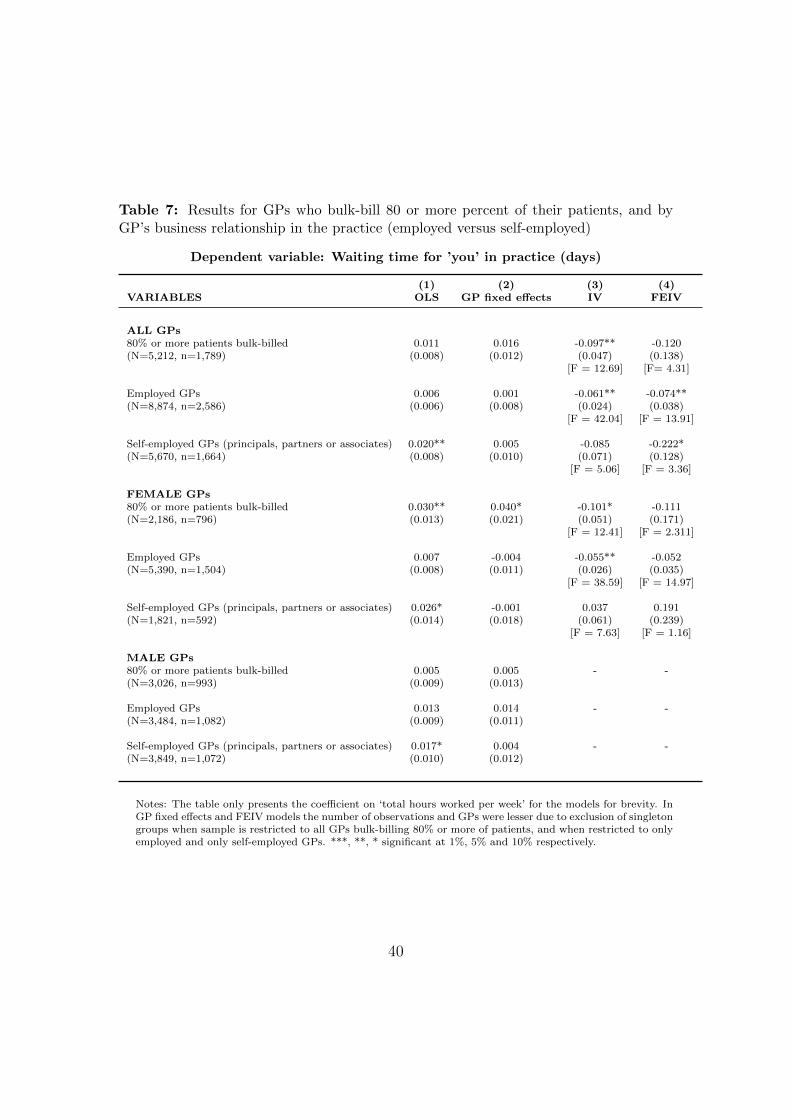
Table 7: Results for GPs who bulk-bill 80 or more percent of their patients, and byGP’s business relationship in the practice (employed versus self-employed)
Dependent variable: Waiting time for ’you’ in practice (days)
(1) (2) (3) (4)VARIABLES OLS GP fixed effects IV FEIV
ALL GPs80% or more patients bulk-billed 0.011 0.016 -0.097** -0.120(N=5,212, n=1,789) (0.008) (0.012) (0.047) (0.138)
[F = 12.69] [F= 4.31]
Employed GPs 0.006 0.001 -0.061** -0.074**(N=8,874, n=2,586) (0.006) (0.008) (0.024) (0.038)
[F = 42.04] [F = 13.91]
Self-employed GPs (principals, partners or associates) 0.020** 0.005 -0.085 -0.222*(N=5,670, n=1,664) (0.008) (0.010) (0.071) (0.128)
[F = 5.06] [F = 3.36]
FEMALE GPs80% or more patients bulk-billed 0.030** 0.040* -0.101* -0.111(N=2,186, n=796) (0.013) (0.021) (0.051) (0.171)
[F = 12.41] [F = 2.311]
Employed GPs 0.007 -0.004 -0.055** -0.052(N=5,390, n=1,504) (0.008) (0.011) (0.026) (0.035)
[F = 38.59] [F = 14.97]
Self-employed GPs (principals, partners or associates) 0.026* -0.001 0.037 0.191(N=1,821, n=592) (0.014) (0.018) (0.061) (0.239)
[F = 7.63] [F = 1.16]
MALE GPs80% or more patients bulk-billed 0.005 0.005 - -(N=3,026, n=993) (0.009) (0.013)
Employed GPs 0.013 0.014 - -(N=3,484, n=1,082) (0.009) (0.011)
Self-employed GPs (principals, partners or associates) 0.017* 0.004 - -(N=3,849, n=1,072) (0.010) (0.012)
Notes: The table only presents the coefficient on ‘total hours worked per week’ for the models for brevity. InGP fixed effects and FEIV models the number of observations and GPs were lesser due to exclusion of singletongroups when sample is restricted to all GPs bulk-billing 80% or more of patients, and when restricted to onlyemployed and only self-employed GPs. ***, **, * significant at 1%, 5% and 10% respectively.
40
References
ABS (2014). Patient Experiences in Australia: Summary of Findings, 2013
-14. http://www.abs.gov.au/ausstats/[email protected]/Lookup/by%20Subject/
4839.0~2013-14~Main%20Features~General%20practitioners~2.
AIWH (2015). Medical Practitioner workforce. Australian Institute of
Health and Welfare. http://www.aihw.gov.au/workforce/medical/
types-of-medical-practitioners/.
Baum, C. F., Schaffer, M. E., and Stillman, S. (2007). Enhanced routines for
instrumental variables/GMM estimation and testing. Stata Journal, 7(4):465 –
506.
Bensing, J. M., Roter, D. L., and Hulsman, R. L. (2003). Communication patterns
of primary care physicians in the United States and the Netherlands. Journal
of general internal medicine, 18(5):335 – 342.
Britt, H., Miller, G. C., Henderson, J., Bayram, C., Valenti, L., Harrison, C.,
Charles, J., Pan, Y., Zhang, C., and Pollack, A. (2013). A decade of Australian
general practice activity 2003-04 to 2012-13: General practice series no. 34,
volume 34. Sydney University Press.
Britt, H., Valenti, L., Miller, G. C., and Farmer, J. (2004). Determinants of GP
billing in Australia: content and time. Medical Journal of Australia, 181:100–
105.
Britt, H. C., Valenti, L., and Miller, G. C. (2005). Determinants of consultation
length in Australian general practice. Medical Journal of Australia, 183(2):68.
Campbell, J. L., Ramsay, J., Green, J., and Harvey, K. (2005). Forty-eight hour
41

access to primary care: practice factors predicting patients’ perceptions. Family
practice, 22(3):266–268.
Carne, A. (2013). Summary data report of the 2011-2012 annual survey of di-
visions of general practice. Report, Adelaide: Primary Health Care Research
& Information Service, Discipline of General Practice, Flinders University, and
Australian Government Department of Health and Ageing.
Cheraghi-Sohi, S., Hole, A. R., Mead, N., McDonald, R., Whalley, D., Bower, P.,
and Roland, M. (2008). What patients want from primary care consultations: a
discrete choice experiment to identify patients’ priorities. The Annals of Family
Medicine, 6(2):107–115.
Cooper, Z. N., McGuire, A., Jones, S., Le Grand, J., et al. (2009). Equity, waiting
times, and NHS reforms: retrospective study. British Medical Journal, 339.
Crossley, T. F., Hurley, J., and Jeon, S.-H. (2009). Physician labour supply in
Canada: a cohort analysis. Health economics, 18(4):437–456.
Cullis, J. G. and Jones, P. R. (1986). Rationing by waiting lists: an implication.
The American Economic Review, pages 250–256.
Damiani, G., Silvestrini, G., Federico, B., Cosentino, M., Marvulli, M., Tirabassi,
F., and Ricciardi, W. (2013). A systematic review on the effectiveness of group
versus single-handed practice. Health policy, 113(1):180–187.
Department of Health and Ageing - Medicare Australia (2010 - 11). Practice
Incentives Program: The Auditor General Audit Report - Performance Au-
dit. http://anao.gov.au/~/media/Uploads/Documents/2010%2011_audit_
report_no5.pdf.
42

Department of Health and Prime Minister’s Office U.K. (2013). Seven day, 8am -
8pm, GP access for hard working people. Press release.
Department of Human Services (2015a). Incentive payments to GPs who bulk bill
concessional patients and children aged under 16 years.
Department of Human Services (2015b). Practice Incentive Program - After Hours
Incentive.
Deveugele, M., Derese, A., van den Brink-Muinen, A., Bensing, J., and De Mae-
seneer, J. (2002). Consultation length in general practice: cross sectional study
in six European countries. British Medical Journal, 325(7362):472.
Gandhi, I., Parle, J., Greenfield, S., and Gould, S. (1997). A qualitative investi-
gation into why patients change their GPs. Family practice, 14(1):49–57.
Gerard, K., Salisbury, C., Street, D., Pope, C., and Baxter, H. (2008). Is fast
access to general practice all that should matter? A discrete choice experiment
of patients’ preferences. Journal of Health Services Research and Policy, 13(2):3
– 10.
Goddard, J., Malek, M., and Tavakoli, M. (1995). An economic model of the
market for hospital treatment for non-urgent conditions. Health Economics,
4(1):41–55.
Gravelle, H. and Hole, A. R. (2007). The work hours of GPs: survey of English
GPs. British journal of general practice, 57(535):96 – 100.
Gravelle, H., Hole, A. R., and Santos, R. (2011). Measuring and testing for gen-
der discrimination in physician pay: English family doctors. Journal of Health
Economics, 30(4):660–674.
43

Gravelle, H., Scott, A., Sivey, P. M., and Yong, J. (2013). Competition, prices and
quality in the market for physician consultations. Melbourne Institute Working
Paper No. 23/13.
Gravelle, H., Smith, P., and Xavier, A. (2003). Performance signals in the public
sector: the case of health care. Oxford Economic Papers, 55(1):81–103.
Guthrie, B. and Wyke, S. (2006). Personal continuity and access in UK general
practice: a qualitative study of general practitioners’ and patients’ perceptions
of when and how they matter. BMC Family Practice, 7(1):11.
Hayashi, F. (2000). Econometrics. 2000. Princeton University Press. Section,
1:60–69.
Iversen, T. (1993). A theory of hospital waiting lists. Journal of Health Economics,
12(1):55–71.
Johar, M. (2012). Do doctors charge high income patients more? Economics
Letters, 117(3):596–599.
Johar, M., Jones, G., and Savage, E. (2014). What explains the quality and price
of GP services? An investigation using linked survey and administrative data.
Health Economics, 23(9):1115 – 1133.
Joyce, C. M., McNeil, J. J., and Stoelwinder, J. U. (2006). More doctors, but
not enough: Australian medical workforce supply 2001-2012. Medical Journal
of Australia, 184(9):441.
Joyce, C. M., Scott, A., Jeon, S.-H., Humphreys, J., Kalb, G., Witt, J., and
Leahy, A. (2010). The ”Medicine in Australia: Balancing Employment and
Life (MABEL)” longitudinal survey-Protocol and baseline data for a prospective
44

cohort study of Australian doctors’ workforce participation. BMC health services
research, 10(50):1 – 10.
Kalb, G., Kuehnle, D., Scott, A., Cheng, T. C., and Jeon, S.-H. (2015). What Fac-
tors Affect Doctors’ Hours Decisions: Comparing Structural Discrete Choice and
Reduced-Form Approaches. Report, Melbourne Institute of Applied Economic
and Social Research, The University of Melbourne.
Kirch, D. G. and Vernon, D. J. (2008). Confronting the complexity of the physician
workforce equation. JAMA, 299(22):2680–2682. 10.1001/jama.299.22.2680.
Kontopantelis, E., Roland, M., and Reeves, D. (2010). Patient experience of access
to primary care: identification of predictors in a national patient survey. BMC
family practice, 11(1):61.
Laudicella, M., Siciliani, L., and Cookson, R. (2012). Waiting times and socioeco-
nomic status: evidence from England. Social Science & Medicine, 74(9):1331 –
1341.
Lindsay, C. M. and Feigenbaum, B. (1984). Rationing by waiting lists. The
American Economic Review, pages 404 – 417.
Luigi, S., Michael, B., and Valerie, M. (2013). OECD Health Policy Studies Wait-
ing Time Policies in the Health Sector: What Works? OECD Publishing.
Martin, S., Jacobs, R., Rice, N., and Smith, P. (2003). Waiting times for elective
surgery: A hospital based approach. Report, University of York, York.
Martin, S. and Smith, P. C. (1999). Rationing by waiting lists: an empirical
investigation. Journal of Public Economics, 71(1):141 – 164.
MBS (2014). Medicare Benefits Schedule-Medicare Statistics. https:
//www.health.gov.au/internet/main/publishing.nsf/Content/
45

34A89144DB4185EDCA257BF0001AFE29/$File/MBS%20Statistics%
20Financial%20Year%202013-14%20external%2020140718.pdf.
Muggah, E., Hogg, W., Dahrouge, S., Russell, G., Kristjansson, E., Muldoon, L.,
and Devlin, R. A. (2014). Patient-reported access to primary care in Ontario:
Effect of organizational characteristics. Canadian Family Physician, 60(1):e24
– e31.
Nutting, P. A., Goodwin, M. A., Flocke, S. A., Zyzanski, S. J., and Stange, K. C.
(2003). Continuity of primary care: to whom does it matter and when? The
Annals of Family Medicine, 1(3):149 – 155.
Olsen, K. R., Gyrd-Hansen, D., S Arensen, T. H. t. j., Kristensen, T., Vedsted, P.,
and Street, A. (2013). Organisational determinants of production and efficiency
in general practice: a population-based study. The European Journal of Health
Economics, 14(2):267 – 276.
Reinhardt, U. (1972). A production function for physician services. The Review
of Economics and Statistics, pages 55 – 66.
Roll, K., Stargardt, T., and Schreyogg, J. (2012). Effect of type of insurance and
income on waiting time for outpatient care. The Geneva Papers on Risk and
Insurance-Issues and Practice, 37(4):609 – 632.
Rubin, G., Bate, A., George, A., Shackley, P., and Hall, N. (2006). Preferences
for access to the GP: a discrete choice experiment. British Journal of General
Practice, 56(531):743 – 748.
Rural and Regional Health Australia, Department of Health (2015).
Higher Bulk Bill Incentives in Regional, Rural and Remote Areas.
http://www.ruralhealthaustralia.gov.au/internet/rha/publishing.
46

nsf/Content/Higher_Bulk_Bill_Incentives_in_Regional_Rural_and_
Remote_Areas-Tasmania_and_Metropolitan_Areas.
Sarma, S., Thind, A., and Chu, M.-K. (2011). Do new cohorts of family physicians
work less compared to their older predecessors? The evidence from Canada.
Social Science & Medicine, 72(12):2049 – 2058.
Sayer, G., Britt, H., Horn, F., Bhasale, A., McGeechan, K., Charles, J., Miller,
G., Hull, B., and Scahill, S. (2000). Measures of health and health care delivery
in general practice in Australia. General Practice Series 3. Cat. no. GEP 3.
Canberra: AIHW.
Schers, H., Webster, S., van den Hoogen, H., Avery, A., Grol, R., and van den
Bosch, W. (2002). Continuity of care in general practice: a survey of patients’
views. British Journal of General Practice, 52(479):459 – 462.
Schurer, S., Kuehnle, D., Scott, A., and Cheng, T. C. (2015). A man’s blessing
or a woman’s Curse? The family-earnings gap of doctors. Melbourne Institute
Working Paper.
Scott, A. (2000). Economics of general practice. Handbook of health economics,
1:1175 – 1200.
Scott, A. and Vick, S. (1999). Patients, Doctors and Contracts: An Application
of Principal-Agent Theory to the Doctor-Patient Relationship. Scottish journal
of political economy, 46(2):111 – 134.
Scott, A., Watson, M. S., and Ross, S. (2003). Eliciting preferences of the commu-
nity for out of hours care provided by general practitioners: a stated preference
discrete choice experiment. Social science and medicine, 56(4):803 – 814.
47

Sharma, A., Siciliani, L., and Harris, A. (2013). Waiting times and socioeconomic
status: Does sample selection matter? Economic Modelling, 33:659 – 667.
Shrestha, D. and Joyce, C. M. (2011). Aspects of work-life balance of Australian
general practitioners: determinants and possible consequences. Australian jour-
nal of primary health, 17(1):40 – 47.
Siciliani, L., Borowitz, M., and Moran, V. (2013). Waiting Time Policies in the
Health Sector: What Works? OECD Health Policy Studies. OECD Publishing.
Siciliani, L. and Verzulli, R. (2009). Waiting times and socioeconomic status among
elderly Europeans: evidence from SHARE. Health Economics, 18(11):1295 –
1306.
Sudano, J. J. and Baker, D. W. (2006). Explaining US racial/ethnic disparities in
health declines and mortality in late middle age: the roles of socioeconomic
status, health behaviors, and health insurance. Social Science & Medicine,
62(4):909 – 922.
Turner, D., Tarrant, C., Windridge, K., Bryan, S., Boulton, M., Freeman, G.,
and Baker, R. (2007). Do patients value continuity of care in general practice?
An investigation using stated preference discrete choice experiments. Journal of
Health Services Research and Policy, 12(3):132 – 137.
Van Doorslaer, E., Clarke, P., Savage, E., and Hall, J. (2008). Horizontal inequities
in Australia’s mixed public/private health care system. Health Policy, 86(1):97
– 108.
Van Doorslaer, E. and Masseria, C. (2004). Income-related inequality in the use of
medical care in 21 OECD countries. OECD Paris.
48

Young, A. F., Dobson, A. J., and Byles, J. E. (2000). Access and equity in the
provision of general practitioner services for women in Australia. Australian and
New Zealand Journal of Public Health, 24(5):474 – 480.
49