hospice-palliative care chapter 17. class objectives: define both palliative & end-of-life care....
TRANSCRIPT
Hospice-Palliative Care
Chapter 17

Class Objectives: Define both palliative & end-of-life care. Discuss the legal & socio-cultural perspectives of
palliative care & end-of-life care. Describe the principles & philosophy that guide palliative
care. Reflect on your own experience with and attitudes about
death and dying. Discuss important communication skills when working
with terminally ill clients and their families. Provide culturally and spiritually sensitive care to
terminally ill clients and their families. Use the nursing process to provide and address the
physiologic responses to terminal illness

Please read End-of-life Care Chapter 17 in your text!! Especially Nutrition & Hydration at end-of -life
Canadian Hospice Palliative Care Associationhttp://www.chpca.net/Reading Effective Communication in Palliative Carehttp://palliative.info/teaching_material/
EffectiveCommunication.pdfVisit:

Please Read
Chapter 17: End of Life CarePay attention to Nutrition and Hydration at the End of Life p. 436-438.

Case Study 1 Mrs. Hills is a 45 year old woman of Arabic
descent. She has advanced ovarian cancer. Recent test results indicate that her cancer is progressing and end-of-life issues need to be discussed. Mrs. Hills immigrated to Canada 10 years ago with her husband and 3 children. Her understanding of English is limited. Her husband accompanies her to all appointments to translate for her. He often answers questions and makes decisions without communicating with her. Today Mrs. Hills appears withdrawn. She is very quiet and does not make eye contact. You are concerned about how she is coping.

Consider……… How would you approach this situation? What issues are important to consider
when caring for Mrs. Hills? What resources could be considered? What can you do as a nurse in this
situation?

Description: I have tried to show on my face the psychological tension cause by the
question, 'Has the cancer recurred?'

What is hospice-palliative care?

Of interest in Canada
Published by The Canadian Hospice Palliative Care Association (CHPCA), in 2002.
The Model is based on nationally accepted principles and norms of practiced that were established through a national consensus-building process between 1993 and 2001.
http://www.chpca.net/resource_doc_library/model_to_guide_hpc/A+Model+to+Guide+Hospice+Palliative+Care+2002-URLUpdate-August2005.pdf


Key Features of Hospice Palliative Care “Whole person” care Combines science, presence, openness,
compassion, mindful attention to detail, and teamwork
The patient & family are the unit of care Goal is quality of life & relief of suffering Includes care of the dying and bereavement
follow-up


Who is the hospice palliative care patient?
The patient facing a life-threatening illness (regardless of the type of illness or the stage, ranging from new diagnosis to terminal prognosis) in need of specialized care to promote physical, psychosocial, and spiritual comfort.

Needs of the Palliative Client To be pain free To conserve energy To obtain relief from physical symptoms To be secure To feel that they are being told the truth To trust those who care for them To be given an opportunity to voice fears To be with a caring person when dying To be loved & to share love

Needs of the Palliative Client To be listened to with understanding To talk To preserve identity To feel like a normal person, a part of life right
up to the end To maintain independence To maintain respect in the face of increasing
weakness To perceive meaning in death To share & come to terms with the unavoidable
future

What is end-of-life care? The care that patients and their
families receive when patients are near death or dying.
This can include palliative care, hospice care, and/or supportive care, although not all patients who receive supportive or palliative care are actually receiving end-of-life care (Kinzbrunner ,2005).
the founder of the modern hospice movement

Premises of End-of-Life Care The dying are not people for whom “nothing can
be done”
Everything will be done to
• Promote comfort• Promote dignity• Involve & support significant others

Goals of Hospice Palliative Care To achieve the best quality of life for
patients & families while maximizing comfort & maintaining dignity.
The patient and family’s wishes are respected
The patient and family feel a sense of control over the situation
The patient is comfortable

Hospice Palliative Care Nursing Provision of effective pain
and symptom management Addressing the psychosocial
and physical needs of the patient and family
Incorporating cultural values and attitudes into the plan of care
Supporting those who are experiencing loss and grief
Hospice Palliative Care Nursing (cont’d)
Promoting ethical and legal decision-making Advocating for personal wishes and preferences Using therapeutic communication skills Facilitating collaborative practice

The Importance of Personal Awareness Personal experiences with loss and grief
Attitudes and fears of death and vulnerability
What would I want and need if I were seriously ill or dying
Who’s needs am I meeting?
Were you aware In Nova Scotia

Where is hospice palliative care provided?
Hospice palliative care can be initiated through a number of referral systems and is provided in both community and institutional settings

Communication Active listening The four C’s
Collaboration Credibility Compassion Coordination

Collaboration Gathering and processing information Critiquing and evaluating data for veracity Filtering and communicating knowledge in
an accurate, concise, and timely manner Updating other team members with new
data Engaging in dialogue to solve problems
and participate in decision making
Collaboration Example: I noticed her particular style was really effective.
She had an itinerary of things she would hit on and she did it exactly the same way for each patient. She was very specific. She gave information quickly and without a lot of the gabby extra stuff. The other nurses responded by asking precise questions. The key stuff was hit right up front. You got the information in a timely manner.
Credibility Avoiding jargon or vague
terminology Adjusting communication
style for roles, personalities, and circumstances
Being assertive and confronting conflict directly and respectfully

Credibility Example:

Compassion Consideration of and
caring for others Advocacy Conveying respect in
verbal and non-verbal communication
Fostering positive emotions in others

Compassion Example:

Coordination Effective leadership Encouraging input from others Mentoring Acknowledging contributions of others Facilitating participation of others
Coordination Example:
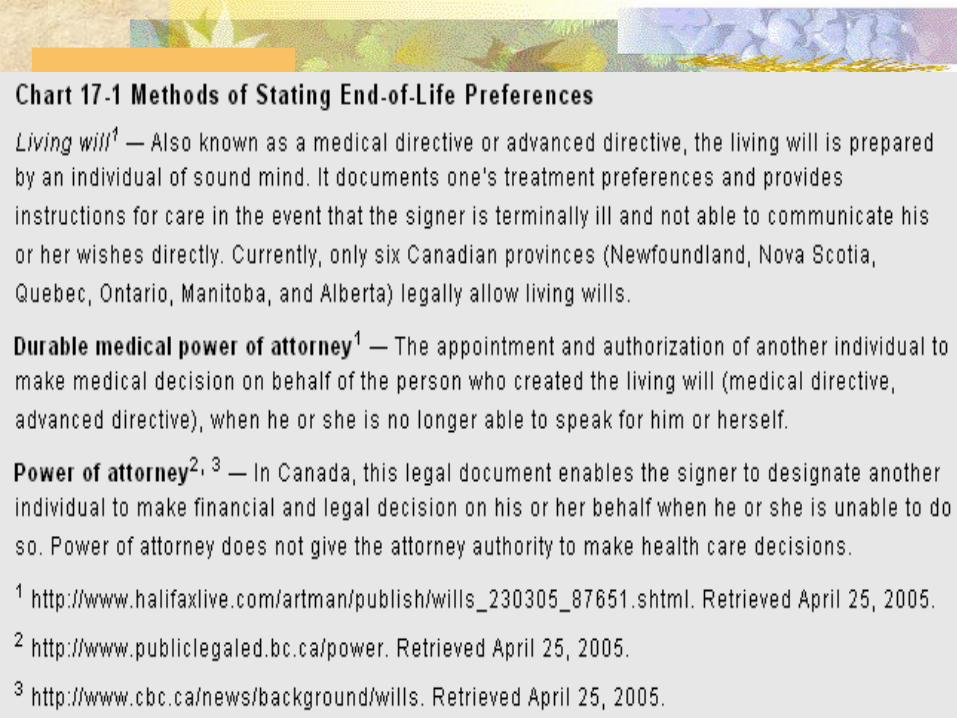
End-of-Life Decision Making

Common Issues
Which treatments to accept or decline and when
Arranging for allocation of worldly possessions
Possible organ donation
Designating care for children
Proxy decision-making Taking care of
“unfinished business”

Common Symptoms
Pain Nausea and
vomiting Fatigue Constipation Candidiasis Dyspnea
Anorexia/cachexia Depression Fever Urinary
incontinence Skin breakdown Confusion/delirium/
restlessness

Signs & Symptoms of Approaching Death Increasing physical
and emotional withdrawal
Reduced food and fluid intake
Confusion/agitation Change in breathing
patterns
Noisy respirations “terminal bubbling”
Incontinence of urine & stool
Changes in skin temperature and colour

Death is inevitable. Pain , distress & other symptoms do not have to be!

Nursing Interventions Providing comfort Ensuring safety Addressing physical and emotional needs Explaining what is happening to the patient and
family Supporting & sustaining patient/family
relationships Helping the patient/family to retain as much
control over the situation as possible Knowing and following patients' wishes for
end-of-life care



Nutrition & Hydration Artificial nutrition & hydration includes
tube feedings & IV therapy General consensus from the literature that
providing artificial hydration such as IV therapy does not improve the comfort level of dying clients, provided that the symptoms such as dry mouth & transitory thirst are addressed with good mouth care & oral fluids or ice chips (McCaulay, 2001; Tarrant, 2001)