hormone replacement therapy: practical considerations marco gambacciani and nick panay
TRANSCRIPT
Hormone replacement therapy: Hormone replacement therapy: practical considerationspractical considerations
Marco Gambaccianiand Nick Panay
HRT HRT governing principlegoverning principle
• HRT should be part of an overall strategy including lifestyle recommendations regarding diet, exercise, smoking and alcohol for maintaining the health of postmenopausal women
IMS Updated Recommendations, February 2007
The emerging concepts in HRTThe emerging concepts in HRT
• Timing (window of opportunity)– Early start – Maintenance of estrogenic benefits
• Patient selection – Avoiding generalized prescribing
• Personalization– Tailoring dose to patient– Continuation and tapering the dose with age
17
48
10
25
0
10
20
30
40
50
60
Years since menopause
Pe
rce
nta
ge
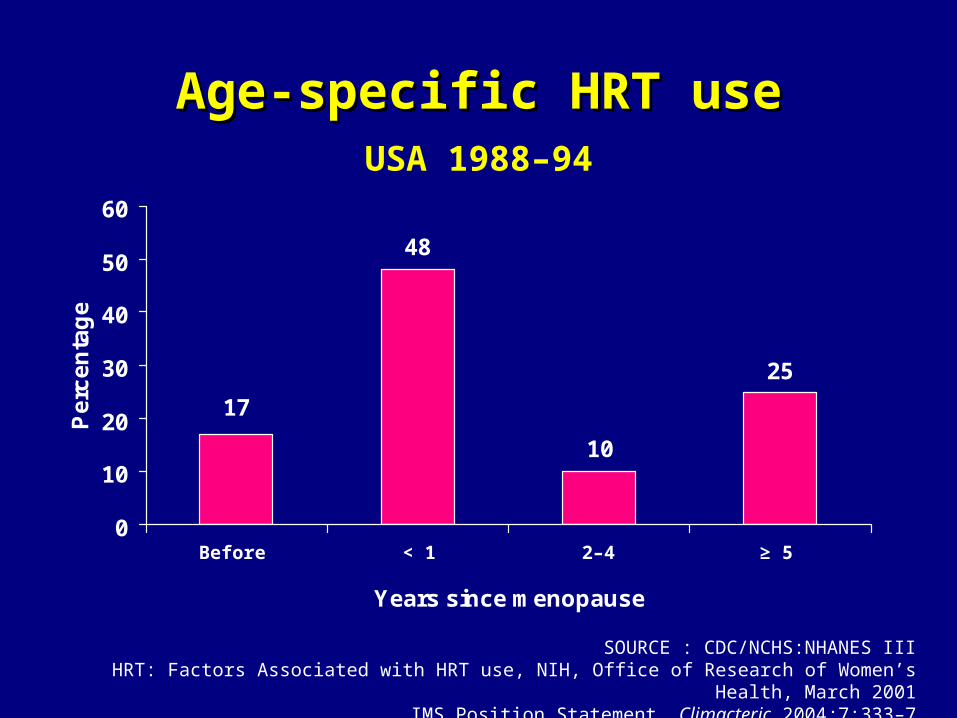
Age-specific HRT useAge-specific HRT useUSA 1988–94
SOURCE : CDC/NCHS:NHANES IIIHRT: Factors Associated with HRT use, NIH, Office of Research of Women’s Health, March 2001
IMS Position Statement, Climacteric 2004;7:333–7
Before < 1 2–4 ≥ 5
Percentage
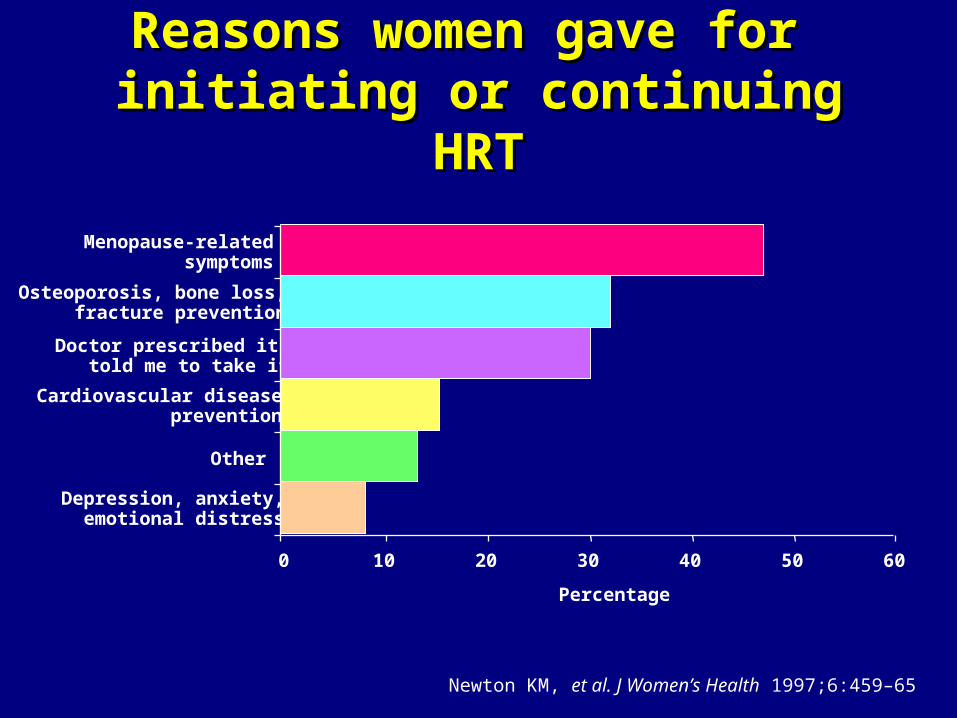
Menopause-relatedsymptoms
Osteoporosis, bone loss,fracture prevention
Doctor prescribed it,told me to take it
Cardiovascular diseaseprevention
Other
Depression, anxiety,emotional distress
0 10 20 30 40 50 60
Reasons women gave for Reasons women gave for initiating or continuing HRTinitiating or continuing HRT
Newton KM, et al. J Women’s Health 1997;6:459–65
Estrogen deprivation andEstrogen deprivation and symptomatic postmenopausal womensymptomatic postmenopausal women
• 75% of women report hot flushes (HF) around menopause
• 25% remain symptomatic for > 5 years
• Not all women will experience HF when they become menopausal
• HF are not just a symptom
• In postmenopausal women suffering from HF, the brain sensitivity to estrogen depletion is higher
The International Menopause SocietyHRT in climacteric and aging brain, Pisa 15–18 March, 2003
Estrogen deprivation andEstrogen deprivation andsymptomatic postmenopausal womensymptomatic postmenopausal women
• HRT:– Can cure HF and improve sleep, mood
and quality of life– May have the potential to prevent/delay
cognitive decline, Alzheimer’s disease, Parkinson’s disease, schizophrenia through multiple neuroprotective actions
The International Menopause SocietyHRT in climacteric and aging brain, Pisa 15–18 March, 2003
Emerging directions in HRTEmerging directions in HRT
• Early start
• Patient selection
• Personalization
• Lower HRT doses
Why lower HRT doses?Why lower HRT doses?
• Continued efficacy with fewer side-effects and possibly fewer risks
• Potential for greater acceptance by women
• Improved continuance to achieve potential long-term health benefits
• Efficacy in prevention of osteoporosis is not compromised
Estrogenic side-effectsEstrogenic side-effects
HRT: maximizing efficacy, minimizing problemsHRT: maximizing efficacy, minimizing problems
Estrogenic side-effectsEstrogenic side-effects
• Problems– Breast tenderness – especially in those
over 60– Fluid retention– Nausea– Heavy withdrawal bleeds– Breakthrough bleeding– Endometrial hyperplasia
HRT: maximizing efficacy, minimizing problems HRT: maximizing efficacy, minimizing problems
Estrogenic side-effectsEstrogenic side-effects• Management
– Start with low-dose estradiol in most cases– 1.0 mg p.o. (0.5 mg)/0.3 mg CEE/25–50 µg t.d./25
mg implant– Warn re possibility of side-effects initially and
reassure– Monitor E2 levels if poor response to therapy– Consider local use of estrogens for new/persistent
urogenital symptoms, e.g. vaginal dryness, even when systemic therapy has been initiated
Mammographic density: Mammographic density: comparative datacomparative data
• Marchesoni et al. Maturitas 2005– CEE 0.625 mg/MPA 5 mg, 45% had
increase in mammographic density– Tibolone 4%
• Christodoulakos et al. Maturitas 2006 – CEE 0.625 mg/MPA 5 mg
13.2% – E2 2 mg/NETA 1 mg
31.8%– E2 1 mg/NETA 0.5 mg
12.2%
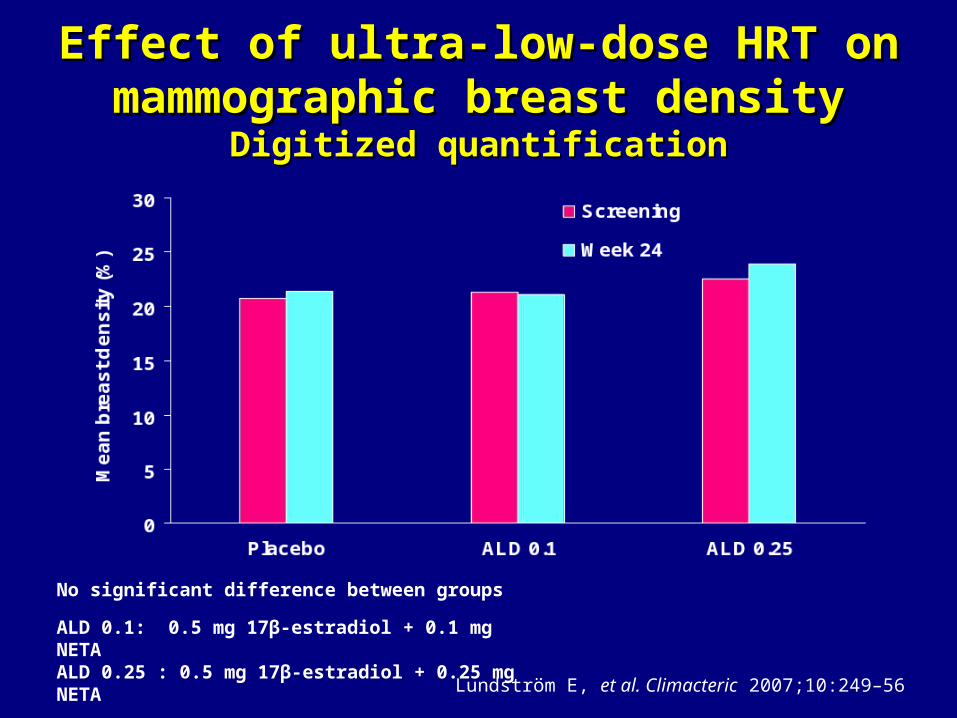
Effect of ultra-low-dose HRT onEffect of ultra-low-dose HRT onmammographic breast densitymammographic breast density
Digitized quantificationDigitized quantification
No significant difference between groups
ALD 0.1: 0.5 mg 17β-estradiol + 0.1 mg NETAALD 0.25 : 0.5 mg 17β-estradiol + 0.25 mg NETA
Lundström E, et al. Climacteric 2007;10:249–56

HRT: maximizing efficacy, minimizing problems HRT: maximizing efficacy, minimizing problems
Estrogenic side-effectsEstrogenic side-effects
• Exceptions to low starting dose of E2– Premature ovarian failure– Severe osteoporosis– Predominance of psychological
problems, e.g. climacteric depression
Maintaining benefitsMaintaining benefits
Low-dose HRT
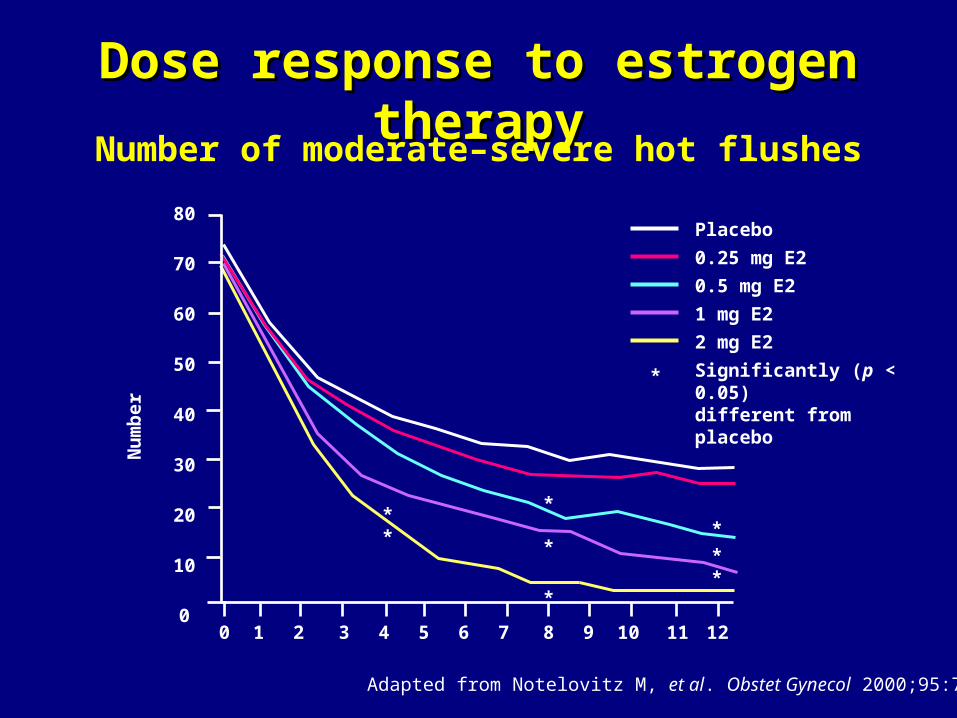
Dose response to estrogen therapyDose response to estrogen therapyNumber of moderate–severe hot flushes
Adapted from Notelovitz M, et al. Obstet Gynecol 2000;95:726–31
Nu
mb
e r
80
70
60
50
40
30
20
10
00 1 2 3 4 5 6 7 8 9 10 11 12
** *
**
*
*
*
Placebo
0.25 mg E2
0.5 mg E2
1 mg E2
2 mg E2
Significantly (p < 0.05)different from placebo
*
0
2
4
6
8
10
1 2 3 4 5 6 7 8 9 10 11 12 13Cycle
Ad
jus
ted
me
an
nu
mb
er*
0
2
4
6
8
10
1 2 3 4 5 6 7 8 9 10 11 12 13Cycle
Ad
jus
ted
me
an
nu
mb
er*
0.625
0.45
0.3
Placebo
0.625/2.50.45/2.50.45/1.50.3/1.5
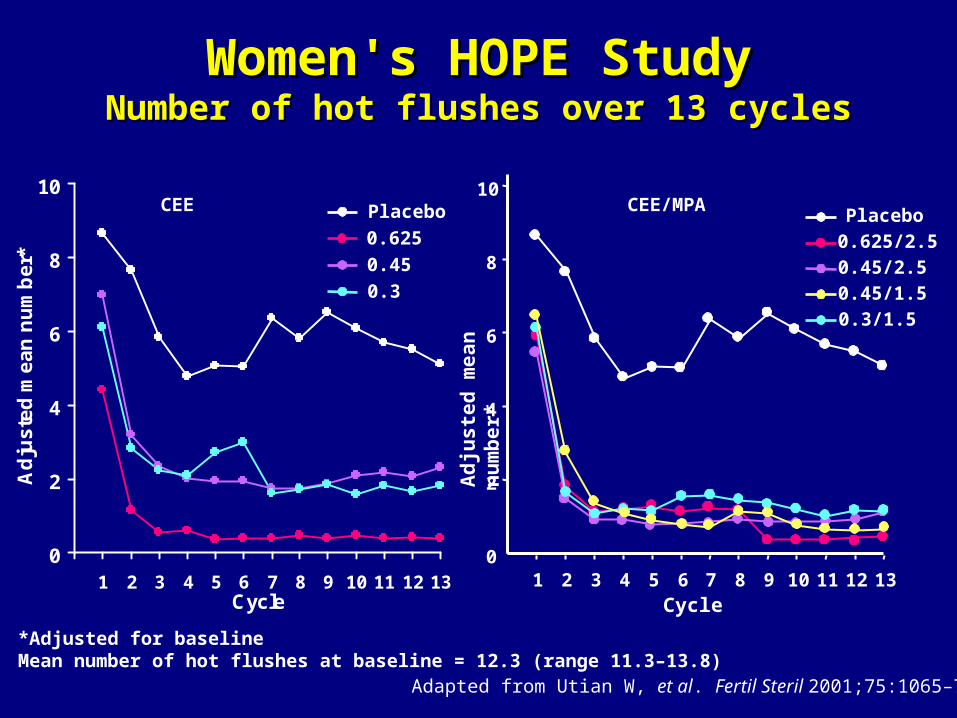
PlaceboCEE/MPACEE
Women's HOPE StudyWomen's HOPE StudyNumber of hot flushes over 13 cyclesNumber of hot flushes over 13 cycles
Adapted from Utian W, et al. Fertil Steril 2001;75:1065–79
*Adjusted for baselineMean number of hot flushes at baseline = 12.3 (range 11.3–13.8)
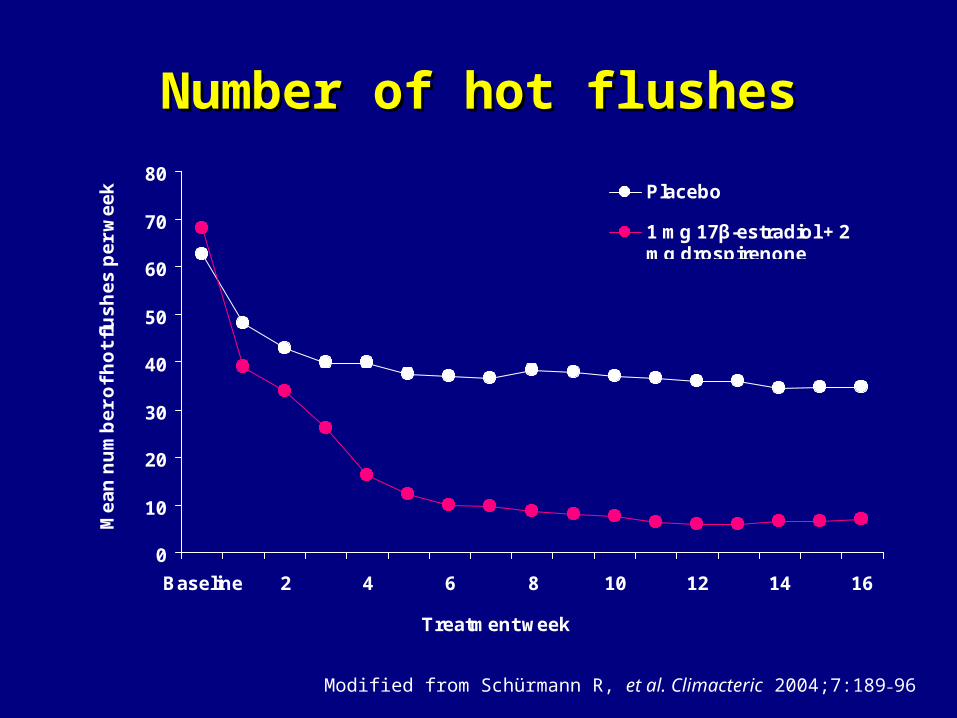
Number of hot flushesNumber of hot flushes
0
10
20
30
40
50
60
70
80
Baseline 2 4 6 8 10 12 14 16
Treatment week
Me
an
nu
mb
er
of
ho
t fl
us
he
s p
er
we
ek Placebo
1 mg 17β-estradiol + 2mg drospirenone
Modified from Schürmann R, et al. Climacteric 2004;7:189–96
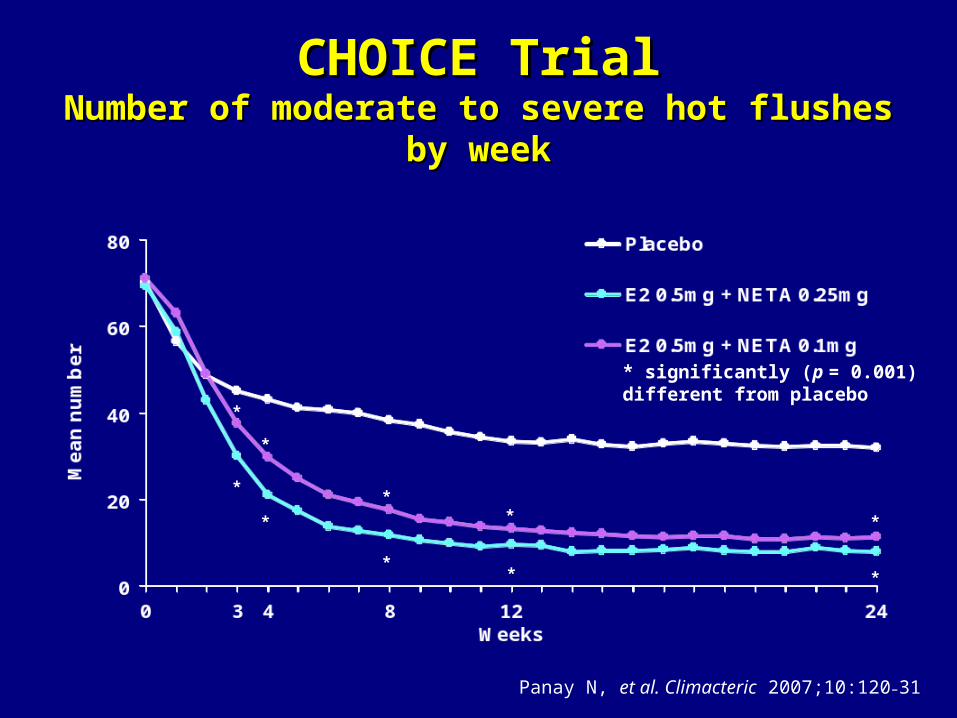
*
*
* significantly (p = 0.001)different from placebo
*
**
*
*
*
*
*
Panay N, et al. Climacteric 2007;10:120–31
CHOICE TrialCHOICE TrialNumber of moderate to severe hot flushes by weekNumber of moderate to severe hot flushes by week
-4
-3
-2
-1
0
1
2
3
4
Baseline 6 12 18 24
Months
Me
an
ch
an
ge
fro
m b
as
elin
e (
%)
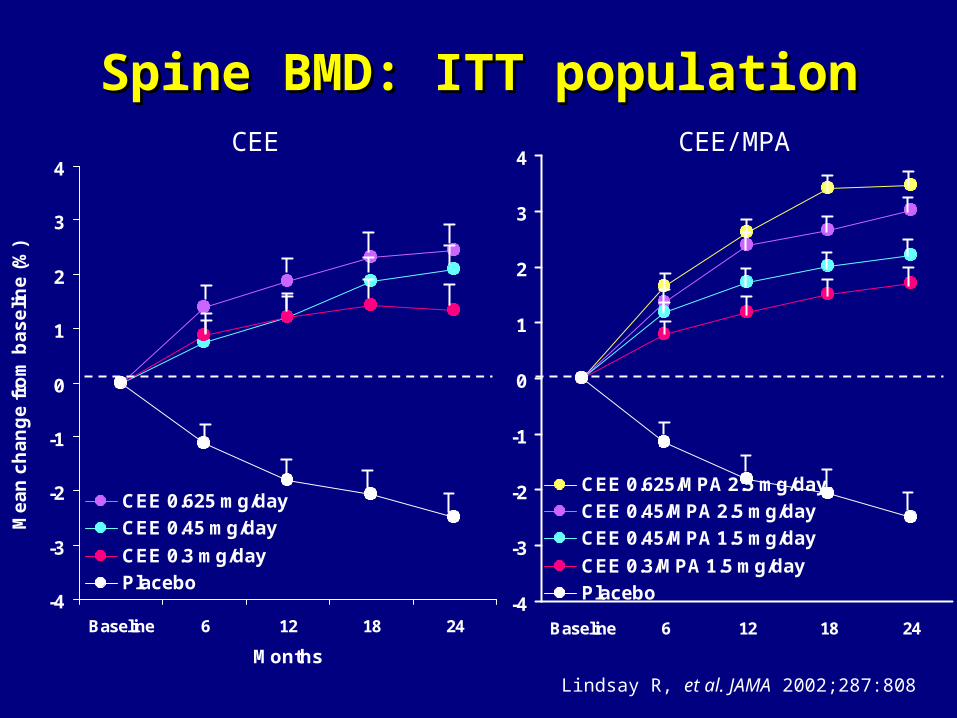
CEE 0.625 mg/day
CEE 0.45 mg/day
CEE 0.3 mg/day
Placebo-4
-3
-2
-1
0
1
2
3
4
Baseline 6 12 18 24
CEE 0.625/MPA 2.5 mg/day
CEE 0.45/MPA 2.5 mg/day
CEE 0.45/MPA 1.5 mg/day
CEE 0.3/MPA 1.5 mg/day
Placebo
CEE CEE/MPA
Spine BMD: ITT populationSpine BMD: ITT population
Lindsay R, et al. JAMA 2002;287:808
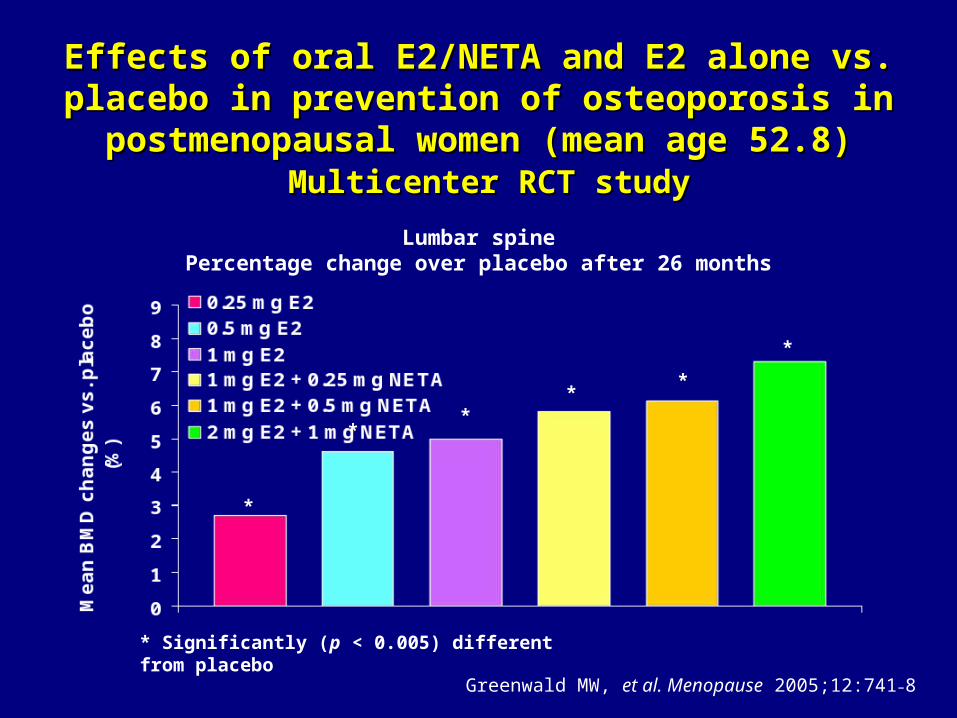
*
*
*
* Significantly (p < 0.005) different from placebo
*
*
*
Lumbar spinePercentage change over placebo after 26 months
Effects of oral E2/NETA and E2 alone vs. placebo Effects of oral E2/NETA and E2 alone vs. placebo in prevention of osteoporosis in postmenopausal in prevention of osteoporosis in postmenopausal
women (mean age 52.8)women (mean age 52.8) Multicenter RCT studyMulticenter RCT study
Greenwald MW, et al. Menopause 2005;12:741–8
Progestogenic side-effectsProgestogenic side-effects
Intolerance
HRT: maximizing efficacy, minimizing problems HRT: maximizing efficacy, minimizing problems
Progestogen intolerance: Progestogen intolerance: mineralocorticoid effectsmineralocorticoid effects
• Symptoms– Edema, weight gain, bloating, migraine
• Etiology– Competition for mineralocorticoid
receptors– Possible effect on renin-angiotensin-
aldosterone cascade
HRT: maximizing efficacy, minimizing problems HRT: maximizing efficacy, minimizing problems
Progestogen intolerance:Progestogen intolerance:mild androgenic effectsmild androgenic effects
• Symptoms– Acne, greasy skin, hirsutism, etc.
• Competition for androgen receptor – Especially C19 nortestosterone-
derived progestogens
HRT: maximizing efficacy, minimizing problems HRT: maximizing efficacy, minimizing problems
Progestogen intolerance: Progestogen intolerance: CNS effectsCNS effects
• Stimulation of progesterone receptors in CNS may lead to negative mood effects
• Mediation by neurotransmitter pathways– GABA receptors stimulated – Serotonin levels reduced– Increased monoamine turnover
Progestogen intolerance:Progestogen intolerance:minimizing progestogenicminimizing progestogenic
side-effectsside-effects
• Progestogenic side-effects may resolve after first few weeks
• Direct treatment– Mild diuretics – Linolenic acid for breast tenderness– ?Mifepristone (anti-progesterone)
HRT: maximizing efficacy, minimizing problems HRT: maximizing efficacy, minimizing problems
Minimizing progestogenicMinimizing progestogenicside-effectsside-effects
• Action– Change progestogen
• Drospirenone may offer additional benefits– Lower dose and duration (7–10 days)– Switch to: ccHRT, tibolone, intermittent
progestogen, LNG-IUS• Transvaginal ultrasonography ±
endometrial biopsy if bleeding problems
Minimizing side-effectsMinimizing side-effects
Bleeding
HRT: maximizing efficacy, HRT: maximizing efficacy, minimizing problems minimizing problems
• Heavy/prolonged bleeding
• Increase dose/duration of progestogen (13–21 days)
• Avoid bleeds altogether• Continuous combined HRT • Tibolone• LNG-IUS
Panay N, Studd J. Hum Reprod Update 1997;3:159
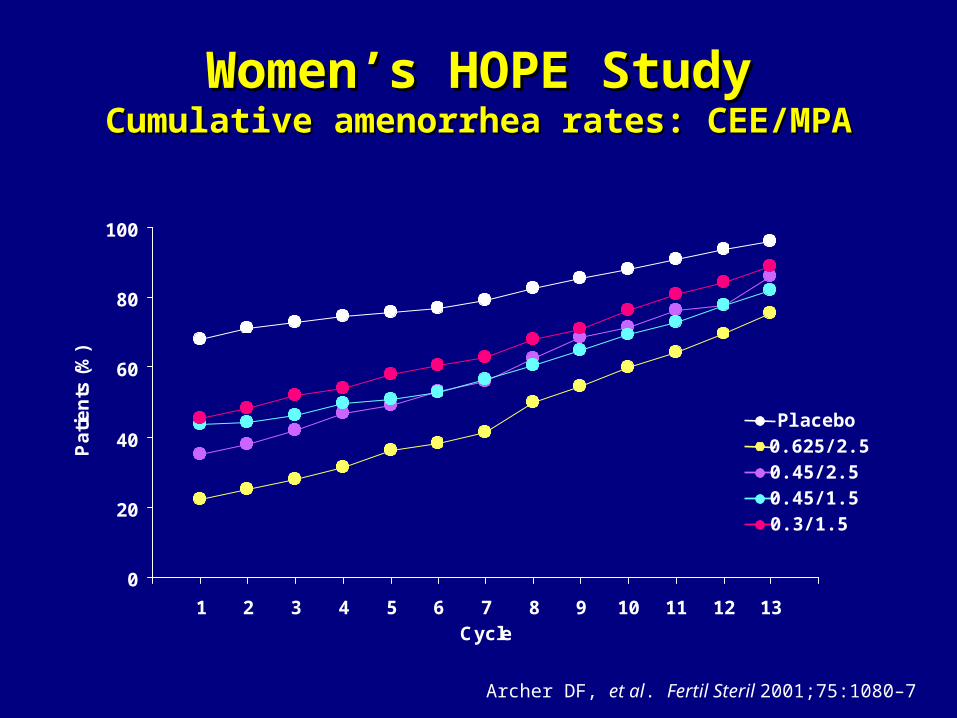
Women’s HOPE StudyWomen’s HOPE StudyCumulative amenorrhea rates: CEE/MPACumulative amenorrhea rates: CEE/MPA
0
20
40
60
80
100
1 2 3 4 5 6 7 8 9 10 11 12 13Cycle
Pa
tie
nts
(%
)
0.625/2.50.45/2.50.45/1.50.3/1.5
Placebo
Archer DF, et al. Fertil Steril 2001;75:1080–7
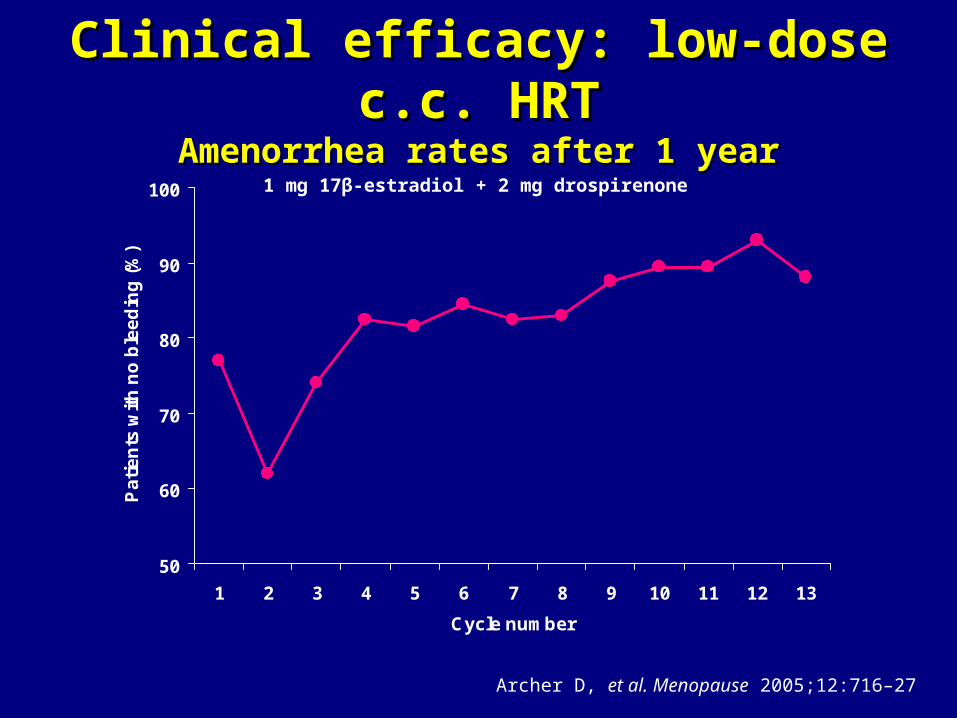
Clinical efficacy: low-dose c.c. HRTClinical efficacy: low-dose c.c. HRTAmenorrhea rates after 1 yearAmenorrhea rates after 1 year
50
60
70
80
90
100
1 2 3 4 5 6 7 8 9 10 11 12 13
Cycle number
Pa
tie
nts
wit
h n
o b
lee
din
g (
%)
1 mg 17β-estradiol + 2 mg drospirenone
Archer D, et al. Menopause 2005;12:716–27
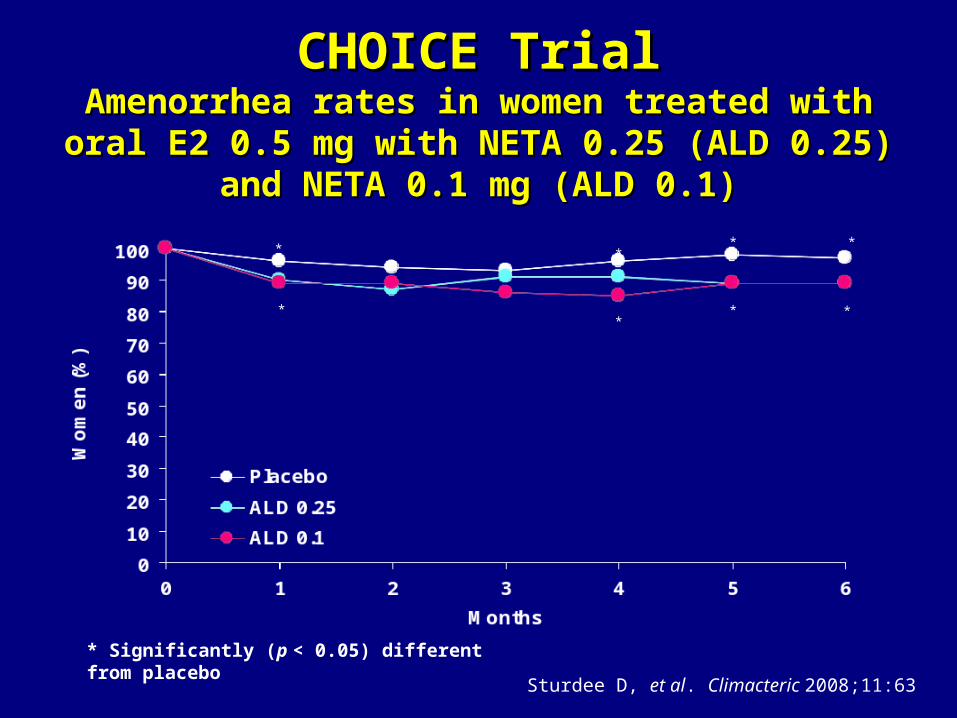
CHOICE TrialCHOICE TrialAmenorrhea rates in women treated withAmenorrhea rates in women treated with
oral E2 0.5 mg with NETA 0.25 (ALD 0.25) and oral E2 0.5 mg with NETA 0.25 (ALD 0.25) and NETA 0.1 mg (ALD 0.1)NETA 0.1 mg (ALD 0.1)
** **
* Significantly (p < 0.05) different from placebo
* ** *
Sturdee D, et al. Climacteric 2008;11:63
Unopposed ultra-low-dose Unopposed ultra-low-dose transdermal estradiol (14 µg/day)transdermal estradiol (14 µg/day)
Endometrial effects vs placebo:
• Proliferation 8.5% vs. 1.1% p = 0.6
• Bleeding 12.4% vs. 8.6% p = 0.3
• Atypical hyperplasia × 1
• Adenosarcoma × 1
Johnson SR, et al. Obstet Gynecol 2005;105:779–87
Conclusions:
“This therapy apparently causeslittle or no endometrial stimulation”
Management of breakthrough Management of breakthrough bleeding with c.c. HRT/tibolonebleeding with c.c. HRT/tibolone
• Usually in women – Recently menopausal – 1-year rule– Early menopause
• May be due to endogenous E2 production
• > 6 months breakthrough bleeding: investigate for pathology by ultrasonography (endometrial biopsy if endometrial thickness > 4 mm)
HRT indicationsHRT indications
• Vasomotor symptoms
• Urogenital symptoms
• Joint and muscle pains, mood swings, sleep disturbances and sexual dysfunction
• Prevention of osteoporosis and related fractures
• Prevention of atrophy – Epithelia– Skin– Connective tissue– Intervertebral disks
IMS Updated Recommendations, February 2007
HRT contraindications IHRT contraindications I(as specified by regulatory authorities)(as specified by regulatory authorities)
• Current, past or suspected breast cancer
• Known or suspected estrogen-dependent malignant tumors (e.g. endometrial cancer)
• Undiagnosed genital bleeding
• Untreated endometrial hyperplasia
• Previous idiopathic or current venous thromboembolism (deep venous thrombosis, pulmonary embolism)
Burger H, et al. Climacteric 2004;7:210–16
HRT contraindications IIHRT contraindications II(as specified by regulatory authorities)(as specified by regulatory authorities)
• Active or recent arterial thromboembolic disease (e.g. angina, myocardial infarction)
• Untreated hypertension
• Active liver disease
• Known hypersensitivity to the active substances or to any of the excipients
• Porphyria cutanea tarda (an absolute contraindication)
Burger H, et al. Climacteric 2004;7:210–16

HRT potential benefits IHRT potential benefits I
• CVD– HRT improves many aspects of the metabolic
syndrome and reduces the risk of diabetes– There is evidence that HT may be cardioprotective
if started around the time of menopause and continued long-term (often referred to as the ‘window of opportunity’ concept)
– In women less than 60 years old, recently menopausal, without prevalent cardiovascular disease, the initiation of HT does not cause early harm, and may reduce cardiovascular morbidity and mortality
IMS Updated Recommendations, February 2007
HRT potential benefits IIHRT potential benefits II
• CNS– HRT initiated around the time of menopause
or by younger postmenopausal women is associated with a reduced risk of Alzheimer’s disease
• Combined HRT may reduce the risk of colon cancer
IMS Updated Recommendations, February 2007
Principles of hormone treatmentPrinciples of hormone treatment
• HRT should not be recommended without there being a clear indication for its use
• Counselling should convey the benefits and risks of menopausal HT in simple terms, e.g. absolute numbers rather than as percentage changes from a baseline
• This allows a woman and her physician to make a well-informed decision about HRT
IMS Updated Recommendations, February 2007
Principles of hormone treatmentPrinciples of hormone treatment
• Women experiencing spontaneous or iatrogenic menopause before the age of 45, and particularly before the age of 40, are at higher risk for cardiovascular disease and osteoporosis
• They will benefit from hormone replacement, which should be given at least until the normal age of menopause
IMS Updated Recommendations, February 2007

Principles of hormone treatmentPrinciples of hormone treatment
• Women taking HRT should have at least an annual consultation for a physical examination, update of medical history, relevant laboratory and imaging investigations and a discussion on lifestyle
IMS Updated Recommendations, February 2007
Principles of hormone treatmentPrinciples of hormone treatment
• Whether or not to continue therapy should be decided at the discretion of the well-informed hormone user and her health professional, dependent upon the specific goals and an objective estimation of benefits and risks
• There are no reasons to place mandatory limitations on the length of treatment
IMS Updated Recommendations, February 2007