hompes method - s3-eu-west-1.amazonaws.com
TRANSCRIPT

Hompes MethodLesson 27 –
Mineral Status Tests
© Health for the People Ltd – not for reuse without expressed permission

Mineral Analysis - Introduction
• The clinical assessment of mineral levels in nutrient status is not clear cut and carries similar challenges to the assessment of body burden, namely that a given tissue – hair, urine and blood (serum, whole blood and red blood cells) will tell you something different!

Mineral Analysis - Introduction
• When you throw in the concepts of metabolic individuality and metabolic typing things can get even trickier because different metabolic types might need nutrients that seem contradictory to lab test results. We’ll explore this in a moment.

Mineral Analysis - Introduction
• The need for testing is obvious – a frank deficiency in a single element can cause significant declines in metabolic function (just think of iron-deficiency anemia, for example).

Mineral Analysis - Introduction
“Across all demographic strata in industrialised nations, element deficiencies are recognised as being involved in the pathogenesis of many health conditions, including
hypertension, heart disease and cancer.”
“In the United States the recommended daily allowance is not met by most population groups for magnesium ,
calcium and potassium.”

Mineral Analysis - Introduction
“The causes of such widespread element
deficiencies vary within each element, but may be
categorized as those which decrease supply and
those that increase demand.”

Mineral Analysis - Introduction
• Factors contributing to mineral deficiencies:
– Diet
• Even whole food, non-organic will lack nutrients due to depleted soil
– Poor digestion and absorption
– Parasites stealing nutrients
– Toxicity increases demand
– Stress increases demand

Mineral Analysis - Introduction
• Key resources:
– Table 3.1, p.67• Summary of Essential
Element Assessment and Treatment
– Table 3.2, p.70• Summary of Essential
Element Deficiencies and Toxicities

Mineral Analysis - Introduction
• Pages 5-14 of the Elements Interpretive Guide, as well as Table One in this handout are of significant help.
Mineral Analysis - Introduction
• Emma Lane’s Guidelines to Supplement Use –Minerals – is also a very worthy resource.

Mineral Analysis - Introduction
• Blood:
– Whole blood or red blood cell (RBC) are the most broadly recognized specimens for assessing total body status of nutrient elements. Low levels of nutrient elements in blood can indicate low nutritional status and need for supplementation. High levels of nutrient elements are unusual but may be due to excessive supplementation or abnormal cellular homeostasis.

Mineral Analysis - Introduction
• Blood:
– Erythrocyte (RBC) essential element testing is a valuable assessment tool for evaluating long term element status. The average RBC population turnover is four months, so they represent average long-term elemental status. Erythrocyte levels tend to reflect elemental tissue levels.

Mineral Analysis - Introduction
• Hair:– Keratin, which is rich in sulfur-containing cysteine
residues, is the major component of hair. When elements circulating in blood reach the hair follicle, they bind with high affinity to keratin, becoming trapped in the extruded shaft of hair. High levels of nutrient elements found in hair may be due to supplementation or abnormal homeostasis. High levels of some nutrient elements, such as calcium and magnesium, can suggest bone resorption due to chronic negative element balance.

Mineral Analysis - Introduction
• Urine:– Urinary element excretion can vary with recent
dietary intake and exposure. Thus,for individuals whose day-to-day dietary intake is relatively constant, urine elements can be useful for detecting nutrient insufficiency. Normal levels of urinary zinc and chromium can reflect nutritional adequacy for these elements, since urine is the main route of excretion. On the other hand, for individuals with large daily variations in diet and exposure, urinary levels are more difficult to interpret.

Mineral Analysis - Introduction
• Urine:
– Low levels of nutrient elements in non-provoked urine points to possible dietary deficiency. However, this does not tell the clinician overall body status. High levels of nutrient elements are sometimes found in urine due to recent intake of foods or supplements rich in those elements.

Calcium
• The majority of the calcium in the body (98-99%) is stored in the bone and teeth, which act as a major functional store. The body will use this reservoir to maintain the calcium blood levels, which are tightly regulated within a narrow range.

Calcium
• There is a belief that calcium deficiency is common and that most folk would benefit from supplements. But a calcium need has more to do with an inability to absorb and utilize dietary calcium than a simple calcium deficiency. Calcium regulation in the body is determined by a number of co-factors that are necessary for adequate digestion, absorption and utilization of calcium.

Calcium
• Digestion• Vitamin D- increases blood calcium level• Essential Fatty Acid- increase tissue levels• Acid-Alkaline balance• Macro-minerals (phosphorous, potassium and
magnesium) • Trace minerals (manganese, boron, copper, zinc)• Hormones
– Calcitonin– Parathyroid hormone– Sex hormones (Progesterone, Testosterone , Estrogen)

Calcium
• Much of the serum calcium (as seen in a CBC) is bound to the albumin in the blood. Before drawing conclusions about Ca status, check the serum albumin level to make sure that a decrease in serum albumin is not the cause for a relative serum calcium decrease. Decreased albumin is the most common cause of decreased calcium level in a CBC.

Calcium
• Because calcium is high outside of the cell, calcium levels in RBCs are not a measurement of total body calcium status, but instead are a measure of cell membrane permeability. RBC calcium is a useful marker in patients with hypertension and arrhythmias, renal failure, and even pre-menstrual syndrome
Calcium
• Calcium accumulation in hair can reflect the end result of the process of chronic mobilization from bone. Thus, high levels are associated with calcium loss, which may indicate early signs of osteoporosis, especially in females in the age range of 30-50 yrs. High hair calcium in younger women may, by inference, indicate calcium loss that has not yet shown as bone density decrease.

Calcium
• Low hair calcium accompanied by other low element levels such as chromium, cobalt, magnesium, and manganese may suggest malabsorption. Hair treatments such as permanent solutions, bleach, or dyes may contain calcium and cause high hair calcium levels.
Calcium
• Low hair calcium does not correlate with intake.
• High hair calcium may indicate low dietary intake because the body in its wisdom will resorb bone to keep blood levels as constant as possible.
• Female Calcium levels in hair may be higher than males due to hormonal changes (oestrogen / progesterone levels, in particular).

Calcium
“Perhaps more than most elements, calcium balance evaluation requires multiple markers, both functional
and direct. Biochemical tests of calcium tell only circulating levels of calcium and not the status of
calcium in the body’s principal reservoir, the skeleton.”
Metametrix Lab Evaluations Manual, p.83.

Calcium
• Other tests that may be helpful when calcium is abnormal are:– Bone density analysis (DEXA, bone density scan, alkaline
phosphatase)
– Vitamin D (vitamin D is associated with higher calcium)
– Deoxypyridinoline (DPD)
– Albumin (around 50% calcium in blood is bound to albumin)
– Parathyroid hormone (PTH increases calcium levels)
– High phosphorus is antagonistic (e.g food intake)
– Low magnesium intake can increase calcium

Calcium
• Optimal supplemental forms are gluconate and citrate, or food forms:
– Egg shell calcium, as outlined by Ray Peat and some of his followers (Josh Rubin, Danny Roddy, et al.)
– Milk products (ensure digestion)
– Green leafy veg (well cooked)
– Broths
– Treatment for high intracellular calcium RBC) includes magnesium, antioxidants, and fatty acids (to improve the integrity of the cell membrane).

Magnesium
• Magnesium is mostly an intracellular nutrient and is involved (as Mg-ATP) in virtually every metabolic process occurring in the body. It’s thought to be involved in 350 or more enzymes. We can’t really underestimate the importance of having optimal MG levels, yet it’s one of the most frequently detected deficiencies.
Magnesium
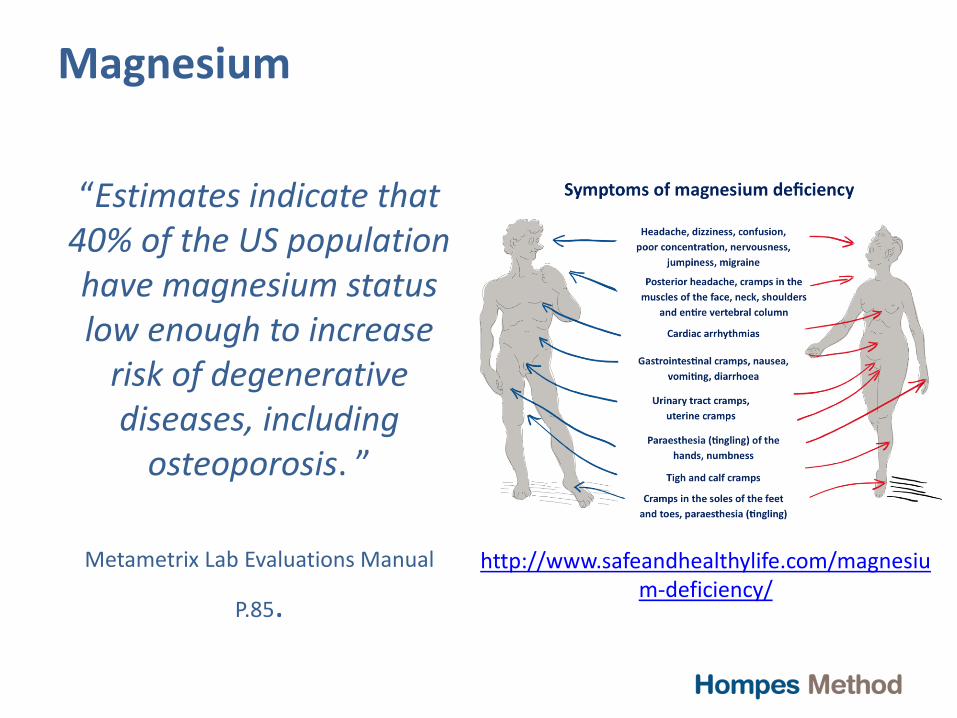
“Estimates indicate that 40% of the US population have magnesium status low enough to increase
risk of degenerative diseases, including
osteoporosis. ”
Metametrix Lab Evaluations Manual
P.85.
http://www.safeandhealthylife.com/magnesium-deficiency/

Magnesium
• It’s not so easy to assess magnesium status (shock!) Serum is most commonly used in the medical setting, but it’s not the best option. It’s an intracellular element/mineral, so it’s better to look at Mg on RBCs (see pages 84-86 of the Lab Evaluations Manual for details).
Magnesium
• High magnesium levels in hair may reflect increased magnesium loss due to high PTH levels, which is likely to result from dietary deficiency (PTH signals the release of Mg – and Ca – from bone: high Mg and Ca in hair may mean both are deficient). Low hair Mg may not be indicative of Mg deficiency.

Magnesium
• Other, indirect tests that may be useful include:
– Magnesium load retention test
– C-reactive protein
– Thromboxane B2
– Endothelin-1
– Na/K ATPase
• Other factors can influence these markers

Magnesium
• The restoration of magnesium level involves:
– Increase Mg intake in the diet through fresh fruit and veg, coffee, brewer’s yeast.
– You can replete with doses up to 750mg/day with supplementation
– Lactate, aspartate, glycinate and gluconate forms are well-absorbed.
– Epsom salt / magnesium flake baths are good, taking great care to manage blood sugar with OJ and salt.

Potassium
• Potassium (K) is the most abundant intracellular cation in the body, with an RDA of 5,000mg/day (need much more than that to be optimal). Deficiency symptoms are generally vague and unspecific. Diets high in processed food (sodium) and lacking in fresh produce will create mild deficiencies in many cases.

Potassium
• RBC potassium may be the best specimen for assessing intracellular K. Serum is not a good sample as K is an intracellular mineral. Urine assessment accurately reflects dietary intake on the same day (you can run it to see if your clients and patients are eating enough fruit and veg!)
Potassium
• The Laboratory Evaluations Manual doesn’t discuss hair potassium in any detail, but the Interpretive Guide says a few words. Hair potassium levels decrease after prolonged alcoholism, apparently showing chronic deprivation of hair follicles during their active growth phase. Low values are frequently found in highly trained athletes and may indicate proper intake and utilization of this element.

Potassium
• High hair potassium may suggest imbalanced whole body homeostasis of potassium, such as that seen in adrenocortical insufficiency. Abnormal potassium balance should be further investigated with blood and/or urine measurements of potassium. We’ll discuss hair potassium in more detail when we look at hair testing separately.

Potassium
• It’s pertinent to focus on foods more than supplements when replacing potassium, but supplements can be used:
– Food sources include mango, banana, corn on the cob, potatoes, tomatoes and fruit/veg generally.
– Most supplements are in citrate and chloride forms.

Sodium
• Sodium and chloride, along with calcium, are the extracellular electrolytes. According to the Lab Evaluations Manual, sodium deficiency is rare, but Ray Peat recommends adding pinches of high quality salt to things like orange juice to ensure adequate sodium supply (blood sugar and anti-stress). Sodium and chloride are included on a CBC. Sodium alone is included on a hair test.
Sodium
• High hair sodium indicates potential for impaired renal function. Electrolyte balance may be disturbed, causing excessive retention of sodium and accumulation in hair. Some evidence points to an association of chronic stress reaction with increased and decreased hair sodium and/or potassium, possibly due to adrenal hormones.

Sodium
• The body has many complex mechanisms for regulating plasma and extracellular sodium. One of the main mechanisms of control is the adrenal cortex via the mineralcorticoid aldosterone. Aldosterone allows the body to hold onto sodium by causing a decreased excretion of sodium from the urine. As such, sodium levels can be a marker for adrenal dysfunction.

Phosphorus
• P is the second most abundant mineral in the body after calcium. Most of it is in the bone, but it’s present in every cell of the body. It’s essential for DNA and RNA, as well as for ATP (energy) and phospholipids in cell membranes. A low serum Ca:Pratio in a CBC indicates bone loss but deficiencies are unlikely given high amounts of P even in poor quality food.
Zinc
• Zinc is a cofactor for more than three hundred known enzymes. Symptoms of mild and severe zinc deficiency include depressed growth, teratogenesis, poor carbohydrate metabolism, altered cognition, poor immune function, alopecia, impotence, eye and skin lesions, and diarrhea. Causes of zinc deficiency include: maldigestion and malabsorption, chelation, low dietary zinc, extensive use of diuretics, metallothionein dysfunction, high alcohol intake, surgery, and burns – it’s used up quickly under stress.
Zinc
“Accurate assessment of zinc status is difficult and studies are often contradictory.”

Zinc
• Levels in plasma, whole blood, blood cells and urine tend to fall with deficiencies. Erythrocyte zinc levels become low in zinc depletion. Erythrocyte zinc analysis is useful. Since red blood cells remain in the circulation for 110 to 120 days, RBC zinc levels reflect long-term zinc stores. RBCs contain about ten times more zinc than plasma.

Zinc
• Urinary zinc has also been shown to be a useful biomarker of zinc status, and correlates with plasma zinc levels. Low urinary zinc indicates zinc deficiency. Urinary zinc levels are high in muscle protein catabolism precipitated by starvation or trauma.

Zinc
• Nutritional zinc deficiency has been associated with low hair zinc levels. Elevations of hair zinc have been reported only during the special metabolic needs of pregnancy, where the high values were present together with evidence of zinc deficiency. Such a “false” high value in a tissue like hair is not indicative of systemic elevation, but possibly of the system depletion (in other words, high hair zinc is more likely to reveal zinc is being lost).

Zinc
• Remember, you also have the zinc tally test as an option. It’s inexpensive, simple to do and you may well derive useful information from it’s simplicity. The zinc tally liquid is placed in the mouth; a strong taste sensation means zinc status is ok, whereas no taste or a weak taste indicates deficiency.
Zinc
• Other indirect markers for zinc status include:
– A high LA to GLA ratio on a fatty acid test can indicate a functional zinc deficiency (Mg, niacin, B6 and vitamin C are also involved).
– Decreased alkaline phosphatase on a CBC may indicate zinc deficiency.
– High cadmium implies low zinc as they’re antagonistic.

Zinc
• When repleting zinc, care must be taken not to lower copper:
– High zinc foods include oysters and red meat (and whole grains – gluten free)
– The best forms are picolinate, sulphate, gluconate, acetate
– Supplements are best taken away from other minerals for optimal absorption

Copper
• Copper is required for over 30 metalloproteinsinvolved in oxidation-reduction reactions; neurotransmitter, energy, myelin, and bone or connective tissue production; immune function; and haematopoeisis. Levels need to be tightly maintained, as copper can be toxic.

Copper
• Refractory anemia is the major copper deficiency condition. More subtle deficiencies are harder to detect. Copper toxicity can cause the same symptoms as deficiency!

Copper
• RBC copper is a good marker for early and ongoing copper deficiency. Chronically elevated plasma copper may result in elevation of erythrocyte copper levels as well, although the two specimens represent different copper utilization.
Copper
• Low hair copper offers evidence that either dietary copper is low or other conditions have diminished tissue copper supply. Excess dietary copper can lead to elevated hair levels. However, in copper loading diseases, such as Wilson’s disease, high hair copper is not detected.

Copper
• Although urinary copper is occasionally used to assess body status, it is primarily useful for diagnosis of copper toxicity, such as in Wilson’s disease, where excretion is significantly elevated.

Copper
• Other tests for copper deficiency include:
– Elevated HVA:VMA ratio in organic acids (>4)
– CBC:• Low uric acid
• Low HCT
• Low HBG
• Low RBCs
– We’ll discuss specific markers in hair mineral analysis that may reveal hidden copper toxicity.

Copper
• Balancing copper requires skill and practice:
– Primary food sources include liver, cashews, black eyed peas, sunflower seeds
– Supplement forms include sulphate and aspartate.
– Taking too much copper may lower zinc.
Nutrient Pairs
• The following mineral pairs are antagonistic to each other. High dietary or supplement intake of one can bring the other down.
– Calcium and Magnesium
– Sodium and Potassium
– Zinc and Copper

Iron
• It’s estimated that at least 6% of the US population is in negative iron balance, with 1% having iron overload. 70% iron is carried in haemoglobin; plasma iron is bound to transport proteins – ferritin, transferrin, albumin.

Iron
• Causes of deficiency can be grouped into five categories – see the Metametrix Lab Evaluations Manual, pages 90-91:
– Dietary intake
– GI blood loss
– Poor absorption (e.g. low HCl)
– Inadequate B12, folic acid, vitamins, A, C and E
– Menstrual blood loss

Iron
“Due to the body’s complex homeostatic controls on elemental concentrations in body tissues and fluids,
testing of multiple specimens may be needed to accurately assess status. Iron provides a good
example.”

Iron
• Routine complete blood counts (CBC) can be very helpful:
– Hemoglobin (Hb)
– Hematocrit
– Mean corpuscular volume (MCV)
– Mean cell hemoglobin (MCH)
– Mean corpuscular hemoglobin concentration (MCHC)
– Erythroycte count

Iron
• Complete blood count markers, continued (note that many CBCs will only include ferritin; the other markers will need to be specially requested):
– Ferritin
– Transferrin saturation
– Serum iron
– Total iron-binding capacity

Iron
“Many physicians make the mistake of only ordering RBC and indices when investigating iron excess or iron deficiency anemia. Without the total serum iron and
other iron tests, such as ferritin, TIBC and % transferrin saturation the degree of iron deficiency anemia or iron excess cannot be appreciated. Also, ordering serum iron without a serum ferritin and TIBC has very little clinical
value.”
Weatherby & Ferguson – Blood Chemistry Analysis Course

Iron
• Decreased ferritin is a good early marker for iron depletion. Serum ferritin reflects iron stores as it’s the major iron storage protein. It appears to be the most sensitive test for identifying iron deficiency anemia.

Iron
• However it’s risky to rely on ferritin levels in patients with:
– Inflammation (it increases with inflam markers such as CRP and IL-10)
– Infection
– Cancer
– Liver disease
• Ferritin can increase in these situations even though a patient’s iron reserves may be low.

Iron
• Transferrin is the transport protein for iron (remember ferritin is the storage protein). Transferrin saturation percentage (Tsat) reveals how much transferrin is carrying iron and is a good indicator of iron availability to bone marrow. Fasting Tsat is the earliest indicator of hemochromatosis* (iron load).
• *Discussed later in this presentation.

Iron
• The total iron binding capacity (TIBC) is the maximum amount of iron that the serum proteins will hold/bind.
Iron
• Serum iron is a useful test for assessing iron deficiency anemia and monitoring its treatment. It can also be helpful in monitoring conditions of iron overload.

Iron
• Consider iron deficiency if you see:
– Decreased HCT (<0.37, <0.40) and/or HGB (<135, <140)
– Decreased MCV (<82), MCH (<28), and MCHC (32)
– Decreased serum iron (<8.96)
– Decreased ferritin (<10)
– Decreased % transferrin saturation
– Increased RDW (>13)
Weatherby & Ferguson – Blood Chemistry Analysis Course
Iron
• Iron deficiency anemia may be secondary to hypochlorhydria if:
– Serum phosphorous is decreased (<0.97)
– Serum globulin is increased (>28) or decreased (<24)
Weatherby & Ferguson – Blood Chemistry Analysis Course

Iron
• Hemochromatosis and hemosiderosis result from excess absorption of iron. Hemochromatosis is a hereditary iron storage disease, which leads to deposition of excess iron in the tissues, especially the liver. It’s different from hemosiderosis, which is the non-hereditary form of the disease.
Iron
• Laboratory changes seen in hemochromatosis include the following:
– An increased serum iron (>39.4)
– A decreased TIBC (<44.8)
– An increased % transferrin saturation (usually > 60%)
– An increased ferritin level (often >1000 μmol/L).
– SGOT/AST is usually elevated (>40)
Weatherby & Ferguson – Blood Chemistry Analysis Course

Iron
• If the serum iron is normal or increased (> 17.9)
– With a decreased RBC (<3.9, <4.2)
– HGB ( < 135, < 140)
– HCT ( < 0.37, <0.40), consider that there may be an inability of the body to convert inorganic iron (the type found in serum iron) into hemoglobin (organic iron).
• There may be a concomitant need for B12, folic acid, B6, and/or copper.
Weatherby & Ferguson – Blood Chemistry Analysis Course

Iron
• Replenishing iron involves optimizing dietary intake - iron in plants is non-heme and is less bioavailable than iron found in animal products (e.g. red meat).– Stomach acid levels and absorption must be considered and
optimised
– Loss of blood (GI or menstrual) should be considered and addressed.
– Check if/how frequently your client/patient gives blood.
– Supplementation should be done carefully – I’ve had good success using properly designed iron supplements at doses of up to 100mg/day.
– Vitamin C enhances iron absorption.

General Replenishment Guidelines
• General additions for improving mineral status:– Organic food.– Bone broth.– Mineral broth.– More fresh produce.– Cook green vegetables well and drink the water at the bottom
of the steamer/in the pan to make digestion easier and reduce phytotoxicity.
– Broad spectrum mineral supplement taken on empty stomach before bed can be helpful.
– Epsom salt / magnesium flake baths (sip OJ with a little salt to maintain blood sugar and keep stress hormones down).
– Stool test / organic acids for digestive function.

Sample Report 1

Sample Report 2

Sample Report 3 - Ben

Sample Report 3 - Ben
• I’ve chosen the third sample for a very specific reason. This was a very tricky client who had a lot of symptoms and had been feeling unwell for quite some time. He really wanted to hone in and focus on fine-tuning his nutrition, so we did a metabolic type analysis (advanced level).
Sample Report 3 - Ben
• He came out as a parasympathetic dominant metabolic type (with a fast oxidiser dominance). You don’t need to know the ins and outs of this, just the principle I am trying to get across. This is NOT taught in other programmes, to my knowledge.

Sample Report 3 - Ben

Sample Report 3 - Ben
Sample Report 3 - Ben
• I gave him potassium, magnesium and selenium, based on his lab result – why wouldn’t a practitioner do this? After all, his levels were very low. Well, he felt awful! I immediately switched to products that support the metabolic type imbalances and he progressed in leaps and bounds.

Mineral Balancing
• Why did I throw this case in? To show you that replenishing mineral levels requires a little skill and understanding that the tests are only guiding you –they’re not, and never will be – 100% correct. That’s why we go broad first with food, gut and general supplementation, then fine tune.

Thank You!
• Thanks a million for tuning in. I appreciate your time and I appreciate you choosing me as one of your teachers. In the next lesson we’ll look at hair mineral analysis, specifically.