holy cross health update on ebola october 16, 2014
TRANSCRIPT
Holy Cross HealthUpdate on Ebola
October 16, 2014
Our Goals:• Provide staff with a basic understanding of Ebola
virus disease
• Communicate the state and federal role in testing for and communicating about Ebola
• Define the current Center for Disease Control (CDC) recommendations for personal protective equipment (PPE) and the Holy Cross Health plan
• Assure that staff understand what personal protective equipment (PPE) is needed and how to put on and take off safely

Ebola Virus Disease (EVD)-The Basics• First outbreak recognized in 1976 in Democratic
Republic Congo (DRC)
• Infection caused by a virus in the Filoviridae family (RNA)
• Is one of numerous viral hemorrhagic fevers• Many outbreaks in last decades confined to
West Africa have been contained by basic public health measures
• 2014 outbreak has been widespread
• Incubation period is 2 to 21 days after exposure• Symptoms are non-specific at first (flu-like) with
fever• Mortality rate > 50% in West Africa• Spread from human to human by unprotected
contact with body fluids• People are not contagious before the fever• Treatment is supportive—fluids, nutrition,
oxygen
Ebola Virus Disease (EVD)-The Basics

When should Ebola be considered?• Symptom onset within 21 days of return from affected countries in West Africa– Most affected--Senegal, Guinea, Sierra Leone, Liberia– See CDC website for most recent information – It is about travel history, not ethnicity
• Risk of exposure to Ebola when in affected area (see CDC risk categories)
• Close contact of individual with symptomatic Ebola virus disease (including healthcare workers)
• No other reason for illness—like malaria
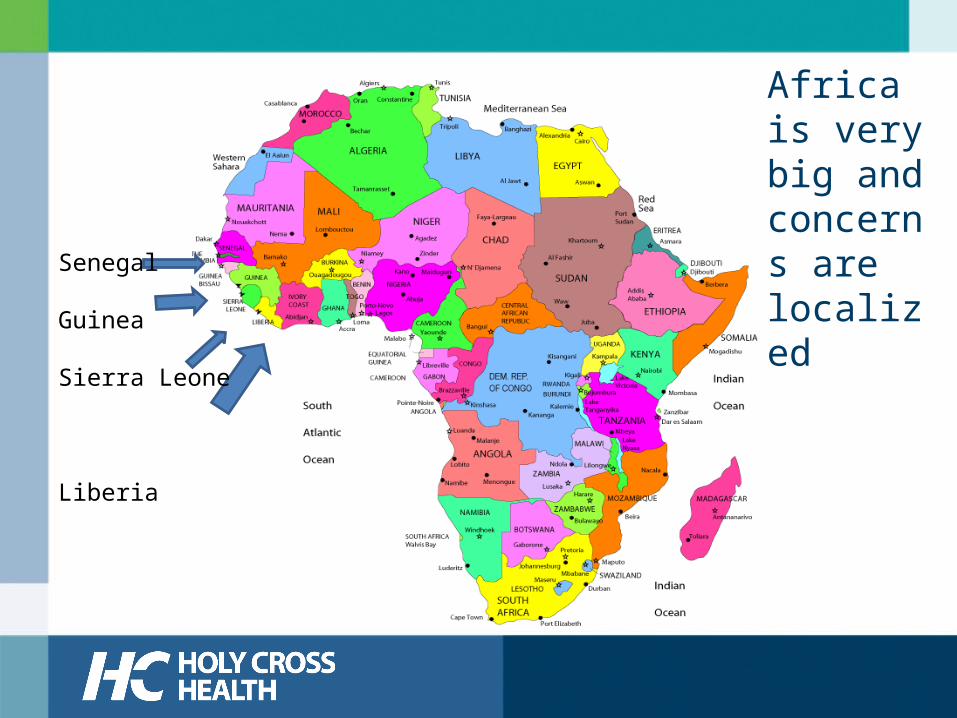
Africa is very big and concerns are localized
Senegal
Guinea
Sierra Leone
Liberia
CDC Ebola Virus Disease (EVD)Risk Categories• High Risk Activities:
– Direct care of EVD patient without PPEs
– Needle stick or mucus membrane contact with EVD blood/body fluids
– Lab worker processing EVD body fluids without PPEs
– Participation in funeral rites of EVD patient
– (Maryland Department of Health and Mental Hygiene also included eating bush meat)
• Low Risk Activities:– Household member or
other casual contact with EVD patient
– Providing patient care or casual contact without high-risk exposure to EVD patients in healthcare facilities in outbreak countries
• No Known Exposure– In affected countries– No high or low risk
exposure
Not all Travelers’ Fevers are Ebola• Febrile illnesses are very common• Ebola presents with flu-like symptoms• Common infections are more likely – Influenza– Sepsis from urinary tract, pneumonia, etc.
• Some infections are more common in West Africa– Malaria or Dengue fever
Testing for Ebola
• Montgomery County hospitals have already evaluated a number of patients, none of whom had Ebola
• When Ebola is a consideration in an ill patient—based primarily on travel history—physicians will consult with Maryland authorities and the CDC
• Only the state and CDC can run the Ebola test and they will approve testing only with strong suspicion
Talking about Ebola
• The Montgomery County Health Department has directed that no information be released about whether a patient is being evaluated for Ebola
• This respects the individual’s rights and minimizes public misinformation about the safety of the hospital
• Please be mindful of conversations with family and friends who might share protected information with others
• The state, CDC and involved hospital will jointly announce any confirmed case
• If you are contacted by members of the public or the press, please direct queries to Yolanda Gaskins, director, media relations (202-550-0454)
Protecting Caregivers from Ebola• It is transmitted by direct contact with
body fluids on mucous membranes or skin breaks
• Can’t transmit it before fever• Not transmitted through the air (like TB
or chickenpox)• Viral hemorrhagic patients have been
safely cared for in the U.S. since 1976, using Standard Precautions
Proper Use of PPE is Key• Study the recommended sequence and
technique for donning PPE1. Boot covers (if needed)2. Gown3. N-95 Mask4. Head cover (if needed)5. Face shield6. Gloves
• Practice with someone watching• Be observed by an assigned monitor or trained
“buddy” when caring for a patient
Protecting Caregivers from Ebola• As of October 15, CDC recommends contact
isolation with droplet precautions when body fluids may be aerosolized
• Holy Cross Health has simplified and standardized by designating a single higher level of protection for all patients
• Holy Cross Health will continue to monitor the latest recommendations for personal protection and will provide any necessary equipment and training
Holy Cross Health Will Provide a Uniform, Higher Level of Protection
CDC Recommendations• Contact isolation
– Gloves, fluid resistant gowns, face shield, shoe covers (for body fluids)
• Droplet isolation– Airborne isolation for
aerosolization procedures
• Private room-door closed– With bathroom– Negative pressure room
• For aerosolization procedures
Holy Cross Health Plan
• Contact isolation– Gloves, fluid resistant
gowns, face shield– boot covers and head
covers (for body fluids)– All Disposable
• Airborne isolation– N95 mask (disposable)
• Private Negative pressure room– Private room with toilet

Removing PPE Properly• Risk of healthcare worker exposure is greatest when
removing PPE, particularly if visibly soiled• Remove in proper sequence
1. Boot covers2. Gloves3. Face shield4. Head cover5. Gown6. N-95 mask
• Alcohol hand hygiene between each step after removing gloves
• Be observed by an assigned monitor or trained “buddy”• Ask for help if PPE is contaminated
– Helper must wear full PPE
• Practice with someone watching
First Steps
• An ill patient with a relevant travel and/or exposure history will be masked and moved as quickly as possible to an isolation room minimizing contact with other people
• Precautions will be instituted until the diagnosis is ruled out or confirmed
• Check with your unit manager for specifics for likely first contact areas—Emergency Department, Obstetrics, Health Centers
Patient Companions/Visitors• Companions of a suspected Ebola case will be
screened for evidence of active infection and triaged appropriately
• Visitors will not be allowed in the room with the patient
• Critical caregivers (parent-child) who remain with a suspected case must wear PPE under staff supervision
• Companions should be advised to return home after obtaining contact information
• Companions without evidence of infection who stay at the hospital should be directed to a private area until the patient’s disposition is determined
• If Ebola diagnosis is established, we will follow CDC visit guidelines and contacts will be followed by public health officials
Limiting Contact with Suspected Ebola• No visitors in the patient room• Nursing assignments will be 1:1• A monitor will be stationed outside the
isolation room to observe PPE use, limit access and maintain log of all entering room
• Blood draws will be minimized• Disposable equipment will be used where
possible
Disposing of Waste and Cleaning• All PPE and linens from an established
patient will be kept in sealed double red bag until transferred to a central site
• Clean hard surface or re-useable equipment with bleach wipes and allow to dry
• Solidify liquid spills with granules
Caring for Our Community• Many of our neighbors and colleagues come from West Africa
and many have family there and, consistent with our guiding behaviors, we need to be sensitive to their anxiety
• The Washington area has a large number of international travelers and some will have spent time in Ebola affected areas
• We can expect that Ebola will be a consideration in a few acutely ill patients in the days, weeks and months ahead. This has already occurred several times in Montgomery County hospitals including both Holy Cross Health hospitals. All cases had other explanations for their symptoms
• We need to be prepared to provide care for all who come to us and to provide that care in a way that keeps our colleagues safe
Recommendations Are Evolving• On October 15, we all learned of a second
healthcare worker in Texas who became infected with Ebola while caring for a dying patient
• The CDC and public health officials are evaluating the procedures and recommendations for protecting caregivers
• Holy Cross Health is monitoring the situation and will provide the equipment and training necessary to keep our staff and doctors safe

Next Steps
• Discuss this material with your manager• Review materials on HCnet and other credible
websites like CDC• Be alert to risk factors for Ebola in all clinical
settings• Practice using the PPE that is appropriate to your
unit and job• Participate in scenario-based training in your unit• Refer questions to Infection Control 301-754-7480
or 301-557-5969
Thank you for completing this course.
• Please return to your ‘My Learning’ page to complete a quiz.
• After completing the quiz, you will have an opportunity to submit questions or comments.