hiv testing among pregnant women in durban,south africa ali groves, suzanne maman, juliana thornton,...
TRANSCRIPT
HIV TESTING AMONG PREGNANT WOMEN IN DURBAN,SOUTH AFRICAAli Groves, Suzanne Maman, Juliana Thornton, Thandeka Nkosi, Zinhle Shazi, Daya Moodley
Intro: PMTCT in KwaZulu Natal, South Africa Women and children living in KZN continue to be hardest hit
by the epidemic in South Africa
In 2001, PMTCT programs were piloted in 9 provinces, including KZN
In KZN, it is estimated that 83% of births take place in clinics or hospitals and the average number of ANC visits is 4.31
HIV testing is provided by “lay counselors” who receive a ten day training course; in 2007/2008, there were 1,876 lay counselors in the province2
72% of all HIV-exposed infants received NVP21. Moodley D. Progress Report of PMTCT
Programme in Kwazulu Natal. (2002)2. KwaZulu Natal Department of Health Annual Report (2007/2008)

Intro: PMTCT Policy and Guidelines (2008)1
Provider-initiated and opt-in– Group information session
– Individual information session
– Written & verbal consent
– Post-test individual counseling for all
– Assurance of confidentiality & discussion of shared confidentiality within healthcare setting
1.South Africa National Department of Health; Policy and Guidelines for the Implementation of the PMTCT Programme(2008)
Intro: PMTCT Policy and Guidelines (cont’d)
• One of the guiding principles of the pregnancy-specific policy is that interventions are to be situated within a human rights paradigm
• Committed to provision of dual therapy for the pregnant mother (and HAART for those clinically indicated)
• Blood to be collected at initiation of ANC visit along
with all other routine blood draws for screening purposes – “the sample taken for HIV testing will not be processed if the pregnant woman objects to being tested for HIV”

Methodology
Research aims1. To understand experiences with HIV testing models from
the pregnant women’s perspective
2. To understand HIV testing implementation; barriers to women testing; and practices around consent and confidentiality from the health care providers perspective
Qualitative Research Methods In-depth interviews with 32 women at two ANC clinics In-depth interviews with all providers of HIV testing at two
ANC clinics Collection of contextual data on PMTCT services in
eThekwini district Data collection took place between June 15th and July 31st
of 2009

Methodology (cont’d)
Analytic strategy All in-depth interviews were audiotaped, transcribed,
translated, coded and computerized for analysis.
South Africa team met weekly to review findings and discuss emerging themes
Used Atlas.ti to assist with organization of data
Coded data using structural codes based on the IDI guide
Developed matrices organized by case; identified patterns in data

PRELIMINARY RESULTS

Results: PMTCT in eThekwini District (2008) 89% of all antenatal clinics provide PMTCT
(110/123)
94% of all ANC attendees tested for HIV
38.75% tested HIV+
81% received CD4 count testing

Results: Description of Clinics

Results: Demographic characteristics Mean age: 23 years
Mean years of education: 11
Majority of participants were in a relationship
Nearly all identified as Black South Africans whose first language was Zulu
50% of women interviewed were pregnant with their first child
80% had never been tested for HIV before the current pregnancy
Results: Pre-test counseling All women received an individual information session and most
felt that it met their needs A majority of the counselors reviewed the benefits of testing
Many women felt like they were able to ask questions“You talk to each other and she’d ask if you have any questions; you’d say yes if you have them and she’d let you ask them. You’d ask those questions and get answered, if you are not satisfied she’d try and explain to you until you are satisfied [deep breath] then when you are both on the “same page”, she’d then take your blood sample (31 years old, HIV+, Clinic 1)
In Clinic 2, at least a quarter of the sessions had more than one counselor in the pre-test session; this made a number of the women uncomfortable
In Clinic 1, one woman was asked if she would prefer to test first or to receive counseling first

Results: Post-test counseling Nearly all women felt that the content and length
of their post-test counseling session met their needs
Counselors did not consistently ask women to talk about their support networks
Counselors did support disclosure when women felt that it would be safe to do so
Results: Post-test counseling (cont’d) A few were dissatisfied or didn’t feel like the post-test
counseling session was sufficient
Two women felt rushed b/c they were the last patient to be seen and a few felt like they were not able to ask the questions they wanted to ask
Two women were interrupted by other clinic staff during their post-test counseling session
At least one woman returned for additional counseling with the same counselor; two sought counseling from other sources
A number of women were also told about supplemental HIV education classes they could attend at the clinic; however, only 1 woman actually attended these classes
Results: Confidentiality An overwhelming majority felt that their results would
be kept confidential
“I’d sometimes hear people saying that this clinic is better, there’s this other clinic where I used to live, you’ll hear people talking about things that shouldn’t have been leaked out of the counseling room. I’ve never heard of such a thing in this clinic that is why I have trust in this clinic.”
(21 year old, HIV - , Clinic 1)
Most women were comfortable with the fact that the nurses also knew their status and that the “sharecode” on the health card made their status not discernable to others
“before they [the nurses] do anything they look at the card if you tested [pause] I think they understand the way the cards are written maybe like if I were to leave it at home and someone picks it up, they won’t know what’s going on…” (29 year old, HIV+, Clinic 1)
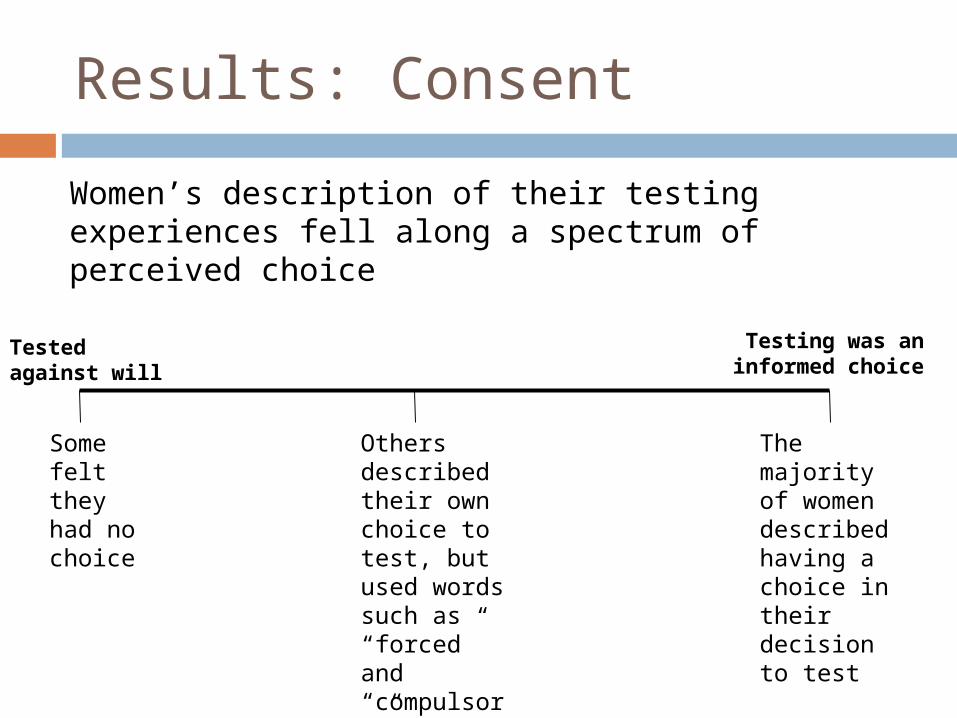
Results: Consent
Women’s description of their testing experiences fell along a spectrum of perceived choice
The majority of women described having a choice in their decision to test
Others described their own choice to test, but used words such as “forced” and “compulsory”
Tested against will
Testing was an informed choice
Some felt they had no choice

Results: Women’s experiences across the spectrum
Choice was clear “No one forced me to, I did by myself. He asked me if I would like to get tested, and I said yes. And he asked are you sure that you are fine with it, there is nowhere where you have a problem - how will you feel if the results say positive? And I told him that I do not have a problem with that I should not run away from it - if I run I am running away with the life of my baby. And he said ‘ok fine’ and he tested me. I did not have a problem” (22 years old, HIV+, Clinic 2)
Choice was less clear
“No, but I would think of refusing - but knowing that you get forced to do it, it’s a must to do it - and I too, knew that it’s a forcing situation, but in a good way because it’s another way of helping you anyway, it’s another way of helping you, I could see that they force you in a good way, I knew you are forced to do it.” (23 years old, HIV-, Clinic 1)
Did not have a choice
"Yes. But I had never anticipated testing on the day I was tested. They just said ‘today we are going to be testing bloods, no one’s going back without having their blood taken for testing.’ I was forced to test in that way. “ (21 years old, HIV-, Clinic 1)

Results: Ability to refuse testing A majority of the women felt that a woman could refuse
to get tested and that she would not face negative repercussions
“No nothing [negative] happens to her, because it’s her choice the nurses do not have a problem because they told you how things happen.”
(HIV+, age unknown, Clinic 1)
However, very few knew anyone who had actually declined testing
Interviewer: “What about those who refuse to test, what consequences do they suffer?”
Respondent: “I don’t know but you just don’t refuse, you don’t refuse.”
(18 years old, HIV+, clinic 2)

Conclusions
Most women felt really good about the care they received at these two clinics. Their positive experiences reflected a practice that is well aligned with policy.
There is need for deeper understanding of different perceptions of choice in consenting to test for HIV so that we don’t sacrifice autonomy in our efforts to maximize testing in antenatal clinics.

Acknowledgements
To the women and the providers who participated in this study and shared their experiences with us
Our research team in South Africa
Open Society Institute for funding this work