hiv services for cross border migrants in the context of nepal, india and bangladesh by prabodh...
TRANSCRIPT

HIV Services for cross border migrants in the context of Nepal, India and
Bangladesh
By Prabodh Devkota
Senior Regional Project Director
CARE International

Cross border mobility contexts in South Asia(Nepal, India and Bangladesh)
Nepal and India share open border India and Bangladesh do not share open border Mobility with in South Asia remains as a historical fact
Enhancing Mobile Population’s Access to HIV Services, Information and Support (EMPHASIS) works in Nepal, India, Bangladesh with research partners in the UK
EMPHASIS experience offers learning from two different cross border contexts of South Asia

EMPHASIS Project Sites Source: Nepal· Achham and Kanchanpur Bangladesh · Jessore and Satkhira
Transit Nepal
· Gaddachauki, Nepal · Banbasa and Gaurifanta, India
Bangladesh · Border area of Sarsha, Sub-district of
Jessore · Border area of Debhata, Satkhira Sadar
& Kalaroa Sub-district, Satkhira
Destination Mumbai:· Thane, Bandra, Jogeshwari, Mulund, Malad, Borivalli, Andheri, Goregaon, Kalwa, Wadala, Mankhurd, Koper Kairne, Santacruz
Delhi : · Naraina, Ramesh Nager, Kirti Nager, Madipur, Kapashera, Gurgaon, Jhilmil, Kashmiri Gate, Nand Nagri
Kolkata ·Bongaon, Barasat, Machhalandpur, Cossipore, Rajabazar, Gardenreach, Madhyamgram
EMPHASIS
Research/Policy
advocacy
Safe Mobility
Women Empowerment
Social Mobilizatio
n
Cross border referral linkage
Health System
Strengthening
Capacity Building Referra
l &
Peer
Educatio
n
Collabora
tio
n
Remittance

Living Conditions of migrants
Female
sex
workers
Inje
ctin
g dru
g use
rs
Clients
of s
ex work
ers
MSW
s, tr
ansgender a
nd clie
nts
Oth
er MSM
who d
o not s
ell and/o
r buy
sex
Remain
ing m
ale P
opulatio
n
Male
labour m
igra
nts
Remain
ing fe
male
Popula
tion
0.05.0
10.015.020.025.030.0
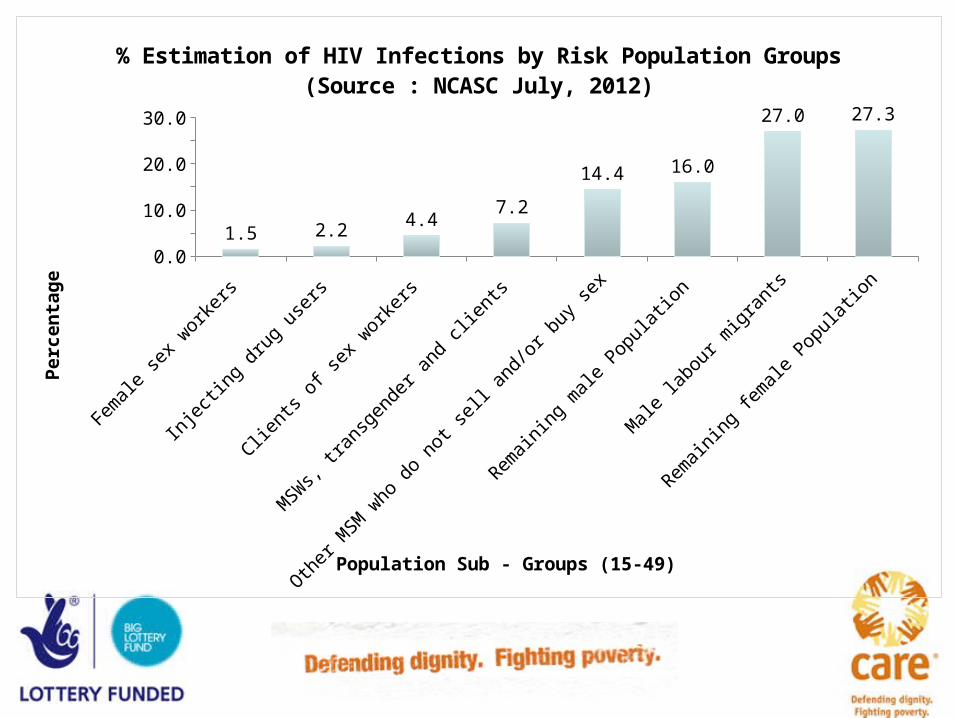
1.5 2.24.4
7.2
14.4 16.0
27.0 27.3
% Estimation of HIV Infections by Risk Population Groups(Source : NCASC July, 2012)
Population Sub - Groups (15-49)
Pe
rce
nta
ge

HIV and Migration: Bangladesh
According to the NASP Report of 2006, approximately 67 percent of identified HIV-positive cases in the country were returnee migrant workers and their spouses.
NASP on the World AIDS Day 2010 stated that 40 per cent of total new HIV cases reported were from external migrant workers and 34 per cent of total cases were female, of which 24 per cent were wives of HIV-positive men.
In 2011, out of the 445 new HIV infections, 138 (31%) are the external migrant workers and 21.1% are the housewives.
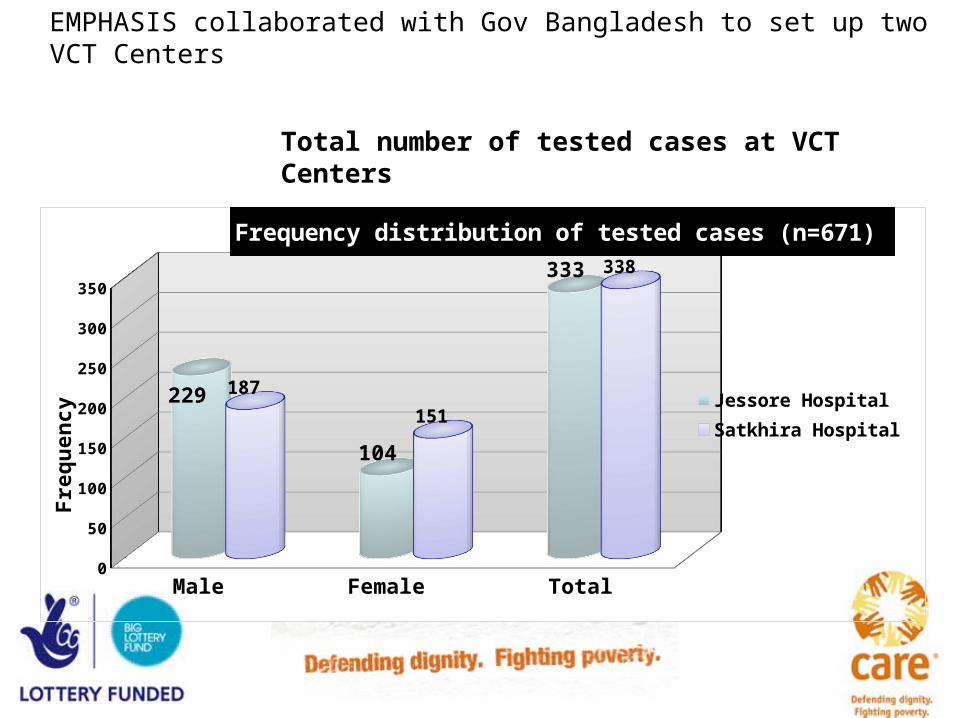
EMPHASIS collaborated with Gov Bangladesh to set up two VCT Centers
Male Female Total0
50
100
150
200
250
300
350
229
104
333
187
151
338
Frequency distribution of tested cases (n=671)
Jessore Hospital Satkhira Hospital
Fre
qu
en
cy
Total number of tested cases at VCT Centers
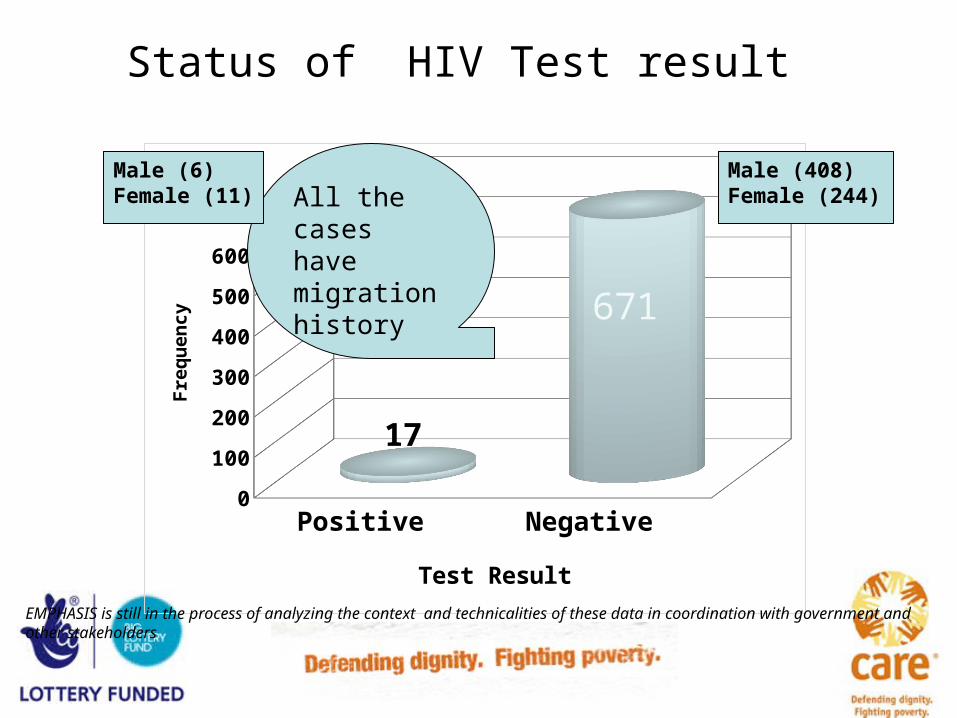
Status of HIV Test result
Positive Negative 0
100
200
300
400
500
600
700
17
671
Test Result
Fre
qu
en
cy
All the cases have migration history
Male (408)Female (244)
Male (6)Female (11)
EMPHASIS is still in the process of analyzing the context and technicalities of these data in coordination with government and other stakeholders

The process to receive ART in India requires the following documents:
Address proof (Ration card/electricity bill) OR Recommendation letter/undertaking from NGO or Recommendation from employer and
Employee ID card
Key Issues faced by PLHIV in the continuum of Mobility Lack of Information Lack of identity proof Long queue (some time 300-400 persons) for getting ART (Mumbai/Delhi) Inadequate time given by ART counsellor though efforts are made to make it easy Access to medicine other than ART Accessing services from different points within a hospital Travel cost-Poor financial status women and widows are on the hardest hit Language barrier

Opportunities
India operates under the principles of universal access to treatment services

EMPHASIS Efforts in Destination
Accessing services through regular referral system in India
Male Female Total
NMP 85 29 114
BSP 14 27 41
Total 99 56 155
People with HIV in EMPHASIS India Male Female Total
NMP 113 33 146
BSP 17 32 49
Total 130 65 195
Accessing services through cross-border referral: A Historic Achievement
Male Female Total
NMP 28 4 32
BSP 3 5 8
Total 31 9 40
ART TRANSFER FROM NEPAL TO INDIA
• Transfer Letter should mention the following:• Letter on hospital letter head with email & phone number of hospital• ART number• Current course of medicine• Date when started ART• Current status of CD4 count• Name of preferred ART centre (asked in Mumbai)
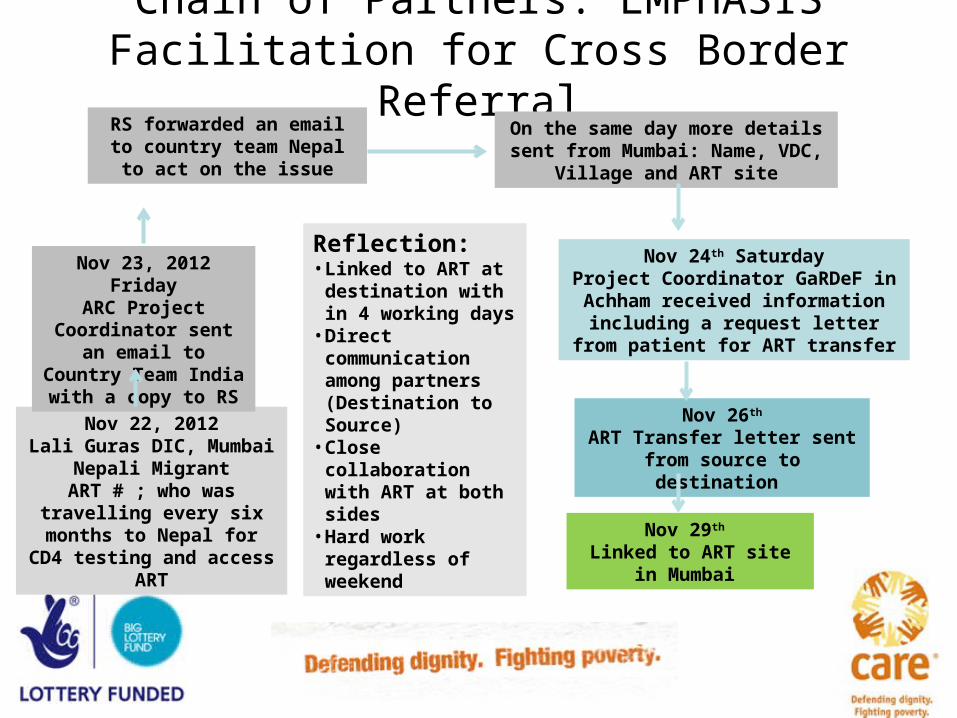
Chain of Partners: EMPHASIS Facilitation for Cross Border Referral
Nov 22, 2012Lali Guras DIC, Mumbai
Nepali MigrantART # ; who was travelling every six months to Nepal for CD4 testing and access
ART
Nov 23, 2012 FridayARC Project
Coordinator sent an email to Country Team India with a copy to RS
RS forwarded an email to country team Nepal to act on
the issue
On the same day more details sent from Mumbai: Name, VDC, Village
and ART site
Nov 24th SaturdayProject Coordinator GaRDeF in Achham received information including a request letter from
patient for ART transfer
Nov 26th
ART Transfer letter sent from source to destination
Nov 29th Linked to ART site in
Mumbai
Reflection: • Linked to ART at
destination with in 4 working days
• Direct communication among partners (Destination to Source)
• Close collaboration with ART at both sides
• Hard work regardless of weekend

Strategic significance of having a cross border program
EMPHASIS services were provided to 13828 migrants at destination in 15 months who were from 67 districts of Nepal at source. This proves the fact that for a cross border program it is important to have programs both at source and destination.
Key Learning
• Unless Migration is underscored as a key priority within National AIDS Response, reaching migrants will be more challenging
• Program at source and destination are strategic to reach the mobile population
• Governments, civil society and people’s network can make universal access possible
• A comprehensive migration program can make a difference

Thank you
www.care-emphasis.org