hiv pregnancy
TRANSCRIPT

2012;14:17–24DOI: 10.1111/j.1744-4667.2011.00076.x
The Obstetrician & Gynaecologist
http://onlinetog.org
Review
HIV in pregnancy: an international perspectiveLaura Byrne MRCP,a,∗ Ade Fakoya FRCP,b Kate Harding FRCOGc
aSpecialty Registrar in Genitourinary & HIV Medicine, Ambrose King Centre, The Royal London Hospital, Turner Street, London E1 1BB, UKbHonorary Senior Research Fellow, Primary Care & Population Health, Faculty of Population Health Sciences, University College London, GowerStreet, London WC1E 6BT, UKcConsultant Obstetrician, Department of Obstetrics, St Thomas’ Hospital, Westminster Bridge Road, London SE1 7EH, UK∗Correspondence: Laura Byrne. Email: [email protected]
Key content:� The HIV epidemic continues to be a major challenge to globalhealth.
� Mother to child transmission accounts for 90% of HIV infectionsin childhood.
� Transmission of HIV from mother to child is largely preventable.� The implementation of interventions to prevent mother to childtransmission of HIV has been successful in the developed world.
� Prevention of mother to child transmission of HIV in thedeveloping world is limited by resources, lack of infrastructure andstigma.
Objectives:� To outline the interventions that have been shown to reducemother to child transmission of HIV in both the developed anddeveloping worlds.
� To discuss the challenges in the prevention of mother to childtransmission faced by the international community.
Ethical issues:� Should we take cost into account when writing guidelines forpreventing mother to child transmission of HIV in resource-poorsettings?
Keywords highly active antiretroviral therapy / HIV testing / infantfeeding / mother to child transmission / short-term antiretroviraltherapy
Please cite this paper as: Byrne L, Fakoya A, Harding K. HIV in pregnancy: an international perspective. The Obstetrician & Gynaecologist 2012;14:17–24.
Introduction
The HIV epidemic continues to be a major challenge forglobal health. The latest figures published by the World HealthOrganization (WHO)1 show that there are 34 million peopleliving with HIV and 2.02 million of these are children underthe age of 15 who require antiretroviral therapy. In 2010 therewere 390 000 new HIV infections in children and over 90% ofthese were acquired by mother to child transmission.1 The HIVepidemic has also had a negative impact on maternal mortalityrates, especially in Eastern and Southern Africa.2 Globally,HIV/AIDS is now the leading cause of mortality among womenof reproductive age and in several high-prevalence countries,such as South Africa and Zimbabwe, HIV is the leading causeof maternal mortality.3
The challenges in the prevention of mother to childtransmission centre on scaling up services to meet the currentrecommendations of universal antenatal testing in areas ofhigh HIV prevalence and antiretroviral therapy for all HIV-positive pregnant women. Access to antenatal care is variablein resource-limited countries. While 98% of pregnant womenin high-income countries report at least one antenatal visitwith a skilled health worker, this figure is at most 68% inthe developing world (range 28–100%).4 In resource-limited
settings only 35% of pregnant women receive an HIV testand 48% of HIV-positive pregnant women receive effectiveantiretroviral therapy to prevent mother to child transmission,although this is a significant improvement on the 10% in2004.1, 5 In resource-rich countries, the implementation ofmultiple evidence-based interventions has reduced mother tochild transmission of HIV to very low levels. The mother tochild transmission rate in the UK is 1.2% overall and 0.8% inwomen who have been on antiretroviral therapy for at least thelast 2 weeks of their pregnancy.6
To reduce the number of children infected or affectedby HIV, the WHO and Joint United Nations Programmeon HIV/AIDS (UNAIDS) have proposed a comprehensiveapproach consisting of four main strategies:5
1 Primary prevention of HIV among women of childbearingage
2 Preventing unintended pregnancies among women livingwith HIV
3 Preventing HIV transmission from women living with HIVto their infants
4 Providing appropriate treatment, care and support tomothers living with HIV and their children and families.
C© 2012 Royal College of Obstetricians and Gynaecologists 17
HIV in pregnancy: an international perspective
This article focuses on the interventions that are effective inaddressing the third strategy:
� antenatal HIV testing� antiretroviral therapy during pregnancy, labour and the
postnatal period� optimal management of labour and delivery� support of infant feeding choice.
We review both the guidance in the UK and guidancefrom WHO, which is intended primarily for resource-limitedcountries.
Timing and factors affecting mother tochild transmission of HIV
Transmission rates in untreated non-breastfeeding populationsin resource-rich countries range from 14–32%, comparedwith 25–48% among breastfeeding populations in resource-poor settings.7 HIV transmission from mother to child canoccur antenatally (in utero), during the intrapartum periodand postnatally (through breastfeeding). The absolute risk ofthese modes of transmission has been estimated at 5–10%,10–20% and 5–30%, respectively.8 It is important todifferentiate between modes of transmission, as these informprevention strategies. Please see Table 1 for a summary ofestimated risks of transmission by population and intervention.
All infants born to HIV-positive mothers have serum HIVantibodies because of passive placental transfer, which persistup to 18 months of age; this does not indicate infection withthe virus. A positive HIV DNA on polymerase chain reactiontesting from the infant before 7 days of age indicates in uterotransmission; if positive at 1 month this indicates intrapartumtransmission, although the cut-offs are not absolute.9
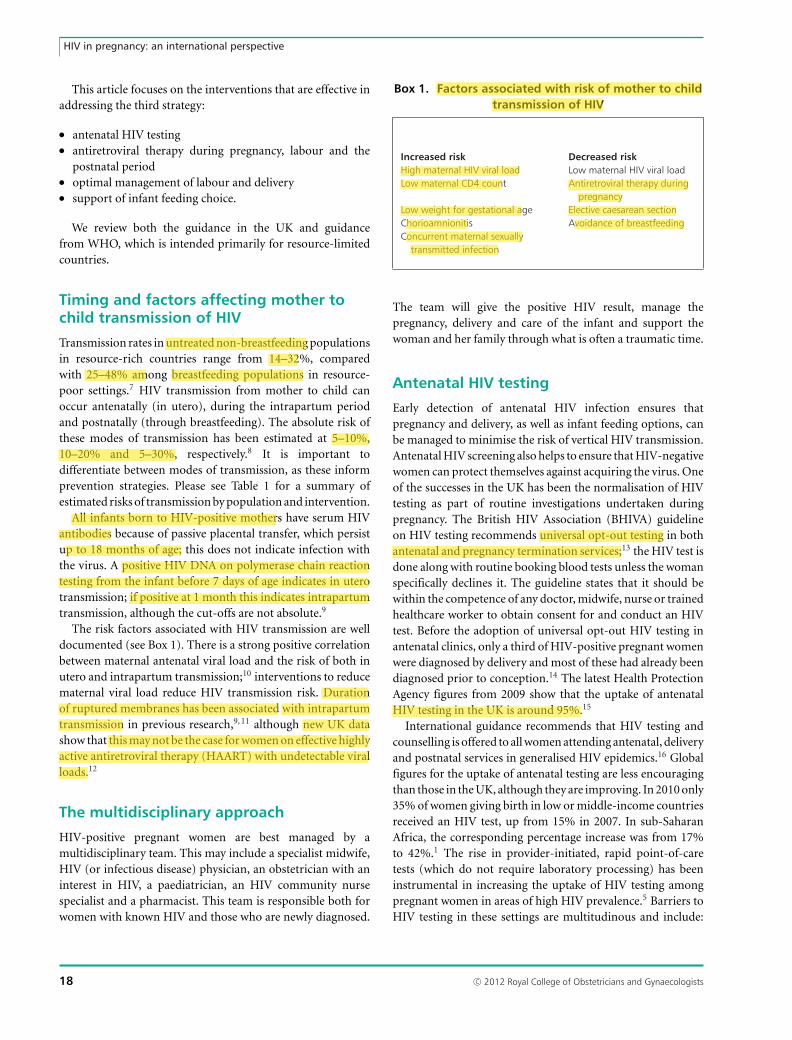
The risk factors associated with HIV transmission are welldocumented (see Box 1). There is a strong positive correlationbetween maternal antenatal viral load and the risk of both inutero and intrapartum transmission;10 interventions to reducematernal viral load reduce HIV transmission risk. Durationof ruptured membranes has been associated with intrapartumtransmission in previous research,9, 11 although new UK datashow that this may not be the case for women on effective highlyactive antiretroviral therapy (HAART) with undetectable viralloads.12
The multidisciplinary approach
HIV-positive pregnant women are best managed by amultidisciplinary team. This may include a specialist midwife,HIV (or infectious disease) physician, an obstetrician with aninterest in HIV, a paediatrician, an HIV community nursespecialist and a pharmacist. This team is responsible both forwomen with known HIV and those who are newly diagnosed.
Box 1. Factors associated with risk of mother to childtransmission of HIV
Increased risk Decreased riskHigh maternal HIV viral load Low maternal HIV viral loadLow maternal CD4 count Antiretroviral therapy during
pregnancyLow weight for gestational age Elective caesarean sectionChorioamnionitis Avoidance of breastfeedingConcurrent maternal sexually
transmitted infection
The team will give the positive HIV result, manage thepregnancy, delivery and care of the infant and support thewoman and her family through what is often a traumatic time.
Antenatal HIV testing
Early detection of antenatal HIV infection ensures thatpregnancy and delivery, as well as infant feeding options, canbe managed to minimise the risk of vertical HIV transmission.Antenatal HIV screening also helps to ensure that HIV-negativewomen can protect themselves against acquiring the virus. Oneof the successes in the UK has been the normalisation of HIVtesting as part of routine investigations undertaken duringpregnancy. The British HIV Association (BHIVA) guidelineon HIV testing recommends universal opt-out testing in bothantenatal and pregnancy termination services;13 the HIV test isdone along with routine booking blood tests unless the womanspecifically declines it. The guideline states that it should bewithin the competence of any doctor, midwife, nurse or trainedhealthcare worker to obtain consent for and conduct an HIVtest. Before the adoption of universal opt-out HIV testing inantenatal clinics, only a third of HIV-positive pregnant womenwere diagnosed by delivery and most of these had already beendiagnosed prior to conception.14 The latest Health ProtectionAgency figures from 2009 show that the uptake of antenatalHIV testing in the UK is around 95%.15
International guidance recommends that HIV testing andcounselling is offered to all women attending antenatal, deliveryand postnatal services in generalised HIV epidemics.16 Globalfigures for the uptake of antenatal testing are less encouragingthan those in the UK, although they are improving. In 2010 only35% of women giving birth in low or middle-income countriesreceived an HIV test, up from 15% in 2007. In sub-SaharanAfrica, the corresponding percentage increase was from 17%to 42%.1 The rise in provider-initiated, rapid point-of-caretests (which do not require laboratory processing) has beeninstrumental in increasing the uptake of HIV testing amongpregnant women in areas of high HIV prevalence.5 Barriers toHIV testing in these settings are multitudinous and include:
18 C© 2012 Royal College of Obstetricians and Gynaecologists

Byrne et al.
Table 1. Estimated risk of vertical HIV transmission by population and intervention6,8,22,23,30,36–45,50,51
Estimated risk of verticalPopulation Intervention vertical transmission (%)∗
Resource-poor, breastfeeding None 20–45Resource-poor, non-breastfeeding None 15–30Resource-rich, non-breastfeeding Elective caesarean section 6.4–8.2Resource-poor, breastfeeding Daily AZT 12.2–18Resource-poor, non-breastfeeding Daily AZT 4.1–9.4Resource-poor, breastfeeding Maternal HAART to 6 months postnatal +/- infant prophylaxis 0.5–6Resource-rich, non-breastfeeding HAART 1Resource-rich, non-breastfeeding HAART 0.1
Maternal viral load <50 copies/ml at 36 weeks
∗These figures are a guide only, based on a review of the relevant literature.AZT = zidovudine; HAART = highly active antiretroviral therapy
lack of health system infrastructure; financial impediments;and social and cultural barriers, including the persistent stigmastill attached to the diagnosis of HIV.17
In high-prevalence areas women are more at risk of acquiringprimary HIV infection during pregnancy.18 Primary HIVinfection is associated with high plasma HIV RNA levels,which increases the risk of mother to child transmission. Somecountries, such as South Africa, therefore, have adopted apolicy of re-testing pregnant women in the third trimester.19
Serodiscordant couples (in which one partner is initially HIV-negative and the other positive) may account for upwards of60% of HIV infections in high-prevalence settings in Africa.20
Voluntary testing and counselling of cohabiting couplesincreases safer sex practices and disclosure of HIV status.21
Testing in the antenatal setting provides an opportunity tooffer testing to male partners and for safe sex promotion forserodiscordant couples, in both resource-poor and resource-rich countries.
Antiretroviral therapy
HAART has revolutionised the management of HIV and isthe single most important intervention in reducing motherto child transmission in pregnant women. Suppression ofmaternal HIV viral load improves maternal health outcomesand prevents both in utero, intrapartum and postnataltransmission. Most pregnant HIV-positive women requiretriple drug therapy, whether initiated for their own healthand continued for the rest of their life, or given as a shortcourse to prevent mother to child transmission during theantenatal and postnatal periods. Decisions about maternalantiretroviral therapy and mode of delivery in the UK arebased on maternal viral load, but this is often unavailable inresource-poor countries. The BHIVA and the WHO guidelinesdifferentiate pregnant women into those who require HAARTfor their own health and those who do not.22, 23 The threshold
Table 2. Maternal drug strategies for prevention of mother to childtransmission of HIV in the UK (adapted from BHIVA guidelines, 200823)
Maternal CD4 count (cells/μl)
<350 >350
Maternal viral load HAART START<6000–10 000 copies/ml or
zidovudine monotherapy+ elective caesarean section
Maternal viral load HAART START>10 000 copies/ml
HAART = highly active antiretroviral therapy; START = short-termantiretroviral therapy
for starting lifelong HAART has been revised to a CD4 count<350 cells/μl. Different treatment strategies are summarisedin Table 2 and Table 3.
In women who require HAART for their own health,BHIVA recommends that they are treated with a nucleosidereverse transcriptase inhibitor (NRTI) backbone of zidovudineand lamivudine, together with a non-nucleoside reversetranscriptase inhibitor (NNRTI) or a protease inhibitor,because this combination has been used most widely inpregnant women.23 However, non-zidovudine-based HAARTis increasingly being used in women pre and post-conceptionand so far there is no evidence of increased risk of maternalHIV viral load at delivery, congenital abnormality or motherto child transmission.24 The WHO guideline also recommendszidovudine and lamivudine as the NRTI backbone, but withnevirapine or efavirenz22 (protease inhibitors are considerablymore expensive than NNRTIs and are not widely available inresource-limited countries).
In the UK, women who do not require HAART for theirown health have two options. Short-term antiretroviral therapy
C© 2012 Royal College of Obstetricians and Gynaecologists 19
HIV in pregnancy: an international perspective
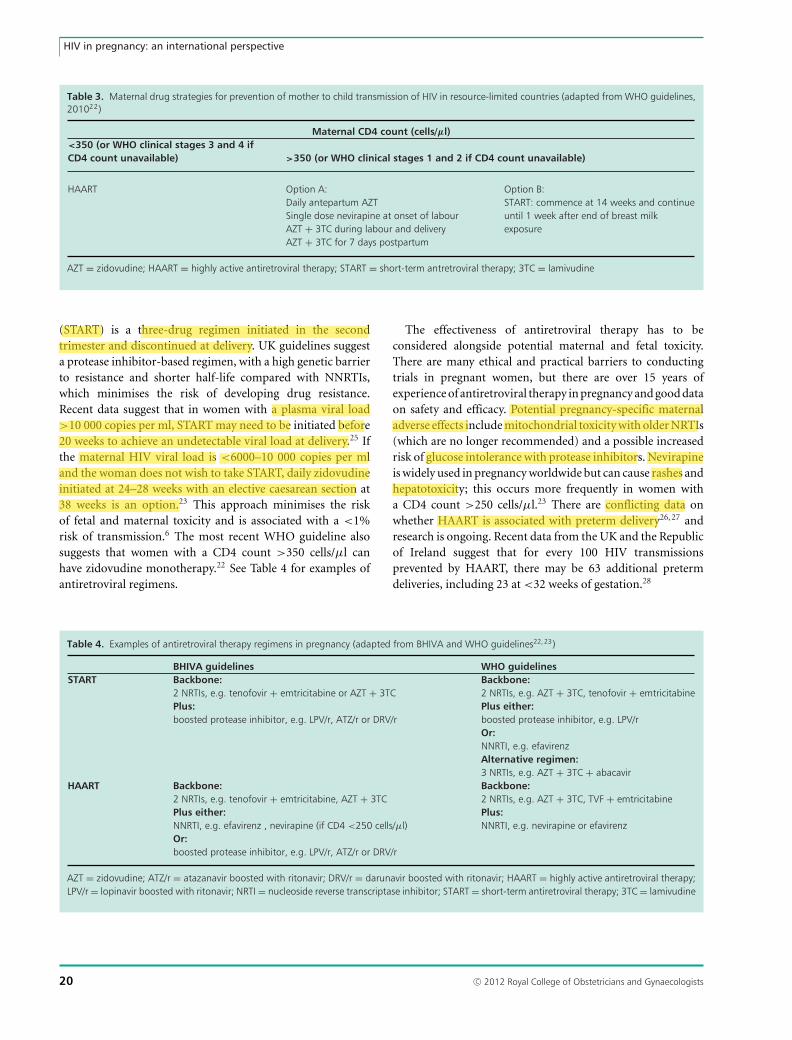
Table 3. Maternal drug strategies for prevention of mother to child transmission of HIV in resource-limited countries (adapted from WHO guidelines,201022)
Maternal CD4 count (cells/μl)<350 (or WHO clinical stages 3 and 4 ifCD4 count unavailable) >350 (or WHO clinical stages 1 and 2 if CD4 count unavailable)
HAART Option A: Option B:Daily antepartum AZT START: commence at 14 weeks and continue
until 1 week after end of breast milkexposure
Single dose nevirapine at onset of labourAZT + 3TC during labour and deliveryAZT + 3TC for 7 days postpartum
AZT = zidovudine; HAART = highly active antiretroviral therapy; START = short-term antretroviral therapy; 3TC = lamivudine
(START) is a three-drug regimen initiated in the secondtrimester and discontinued at delivery. UK guidelines suggesta protease inhibitor-based regimen, with a high genetic barrierto resistance and shorter half-life compared with NNRTIs,which minimises the risk of developing drug resistance.Recent data suggest that in women with a plasma viral load>10 000 copies per ml, START may need to be initiated before20 weeks to achieve an undetectable viral load at delivery.25 Ifthe maternal HIV viral load is <6000–10 000 copies per mland the woman does not wish to take START, daily zidovudineinitiated at 24–28 weeks with an elective caesarean section at38 weeks is an option.23 This approach minimises the riskof fetal and maternal toxicity and is associated with a <1%risk of transmission.6 The most recent WHO guideline alsosuggests that women with a CD4 count >350 cells/μl canhave zidovudine monotherapy.22 See Table 4 for examples ofantiretroviral regimens.
The effectiveness of antiretroviral therapy has to beconsidered alongside potential maternal and fetal toxicity.There are many ethical and practical barriers to conductingtrials in pregnant women, but there are over 15 years ofexperience of antiretroviral therapy in pregnancy and good dataon safety and efficacy. Potential pregnancy-specific maternaladverse effects include mitochondrial toxicity with older NRTIs(which are no longer recommended) and a possible increasedrisk of glucose intolerance with protease inhibitors. Nevirapineis widely used in pregnancy worldwide but can cause rashes andhepatotoxicity; this occurs more frequently in women witha CD4 count >250 cells/μl.23 There are conflicting data onwhether HAART is associated with preterm delivery26, 27 andresearch is ongoing. Recent data from the UK and the Republicof Ireland suggest that for every 100 HIV transmissionsprevented by HAART, there may be 63 additional pretermdeliveries, including 23 at <32 weeks of gestation.28
Table 4. Examples of antiretroviral therapy regimens in pregnancy (adapted from BHIVA and WHO guidelines22,23)
BHIVA guidelines WHO guidelinesSTART Backbone: Backbone:
2 NRTIs, e.g. tenofovir + emtricitabine or AZT + 3TC 2 NRTIs, e.g. AZT + 3TC, tenofovir + emtricitabinePlus: Plus either:boosted protease inhibitor, e.g. LPV/r, ATZ/r or DRV/r boosted protease inhibitor, e.g. LPV/r
Or:NNRTI, e.g. efavirenzAlternative regimen:3 NRTIs, e.g. AZT + 3TC + abacavir
HAART Backbone: Backbone:2 NRTIs, e.g. tenofovir + emtricitabine, AZT + 3TC 2 NRTIs, e.g. AZT + 3TC, TVF + emtricitabinePlus either: Plus:NNRTI, e.g. efavirenz , nevirapine (if CD4 <250 cells/μl) NNRTI, e.g. nevirapine or efavirenzOr:boosted protease inhibitor, e.g. LPV/r, ATZ/r or DRV/r
AZT = zidovudine; ATZ/r = atazanavir boosted with ritonavir; DRV/r = darunavir boosted with ritonavir; HAART = highly active antiretroviral therapy;LPV/r = lopinavir boosted with ritonavir; NRTI = nucleoside reverse transcriptase inhibitor; START = short-term antiretroviral therapy; 3TC = lamivudine
20 C© 2012 Royal College of Obstetricians and Gynaecologists
Byrne et al.
There is a theoretical concern that NRTIs could causemitochondrial toxicity in infants exposed perinatally, but thereis limited evidence and further research in this area is required.The Antiretroviral Pregnancy Registry has found no increase inoverall risk of birth defects in infants exposed to antiretroviraltherapy, including efavirenz, in the first trimester,29 althoughadditional prospective data is required to confirm this.
Management of labour and delivery
In women with HIV this has evolved as understanding ofthe risks of intrapartum transmission has improved. In the1990s, prior to the advent of HAART, elective caesareansection was found to reduce intrapartum mother to childtransmission of HIV.30 In the UK the rate of mother to childtransmission of HIV in women on HAART is 0.7% with bothelective caesarean section and vaginal delivery.6 The potentiallydecreased risk of mother to child transmission by electivecaesarean section in women with higher viral loads, may beoutweighed by the increased risk of complications to bothmother and infant. The risks associated with vaginal birth aftercaesarean section also need to be considered, if the womanis likely to have subsequent children. If the maternal viralload is undetectable at 36 weeks, therefore, a vaginal deliverycan be planned. Women on zidovudine monotherapy andthose on HAART (or START) with a detectable viral load at36 weeks (>400 copies per ml) are recommended to haveelective caesarean section at 38 weeks. A caesarean sectionshould be considered in those with a viral load 50–400 copiesper ml.31
Prelabour rupture of membranes is associated with increasedrisk of HIV transmission, so delivery should be expedited if thewoman is more than 34 weeks pregnant. Prior to 34 weeks,obstetric management should take into account the risk ofneonatal morbidity and mortality associated with prematurity,as well as other factors such as maternal HAART, viral loadand the presence of comorbidities.23 The decision to delivershould include the paediatrician, HIV-specialist physician andthe obstetrician.
In many low and middle-income countries, electivecaesarean section is often not a feasible option. In the lessand least developed areas of the world, the proportion ofbirths attended by a skilled health worker is 62% and 35%,respectively. The rate of caesarean section in sub-Saharan Africais thought to be 3.6–6.5%,32 compared with 24.8% in 2009 inEngland and Wales.33
Invasive procedures that could theoretically increase the riskof transmission during labour, such as fetal blood sampling,should be avoided if possible. There is no evidence that washingthe infant in chlorhexidine after delivery reduces transmission;the infant should be wiped clean and only washed once warm.
Infant feeding
Postnatal transmission of HIV occurs due to breastfeeding.Breast milk from HIV-infected mothers contains cell-freeHIV RNA and intracellular HIV DNA and both are thoughtto contribute to transmission.34 The breast milk viral loadcorrelates with the plasma viral load.35 In breastfeedingpopulations, 24–44% of all mother to child transmission ofHIV is due to breastfeeding and the cumulative probability ofHIV transmission is fairly constant over time and so correlateswith duration of breastfeeding.36, 37 Transmission risk is highestwith mixed feeding compared with exclusive breast or bottlefeeding36, 38 and complete replacement of infant feeding withformula reduces postnatal transmission.
Several studies in the developing world show that maternalHAART (or START continued through the breastfeedingperiod) to suppress maternal viral load and for infantprophylaxis significantly reduces the rate of postnataltransmission of HIV.39–45 The estimated cumulative probabilityof postnatal transmission of HIV in these cohorts is 0.5–3% at6–9 months of age.39, 42–44
Breastfeeding reduces infant morbidity and mortality,protects against childhood infections and promotes childspacing. In resource-poor countries mothers often have noaccess to clean water or formula for safe replacement feeding.Moreover, there can be a stigma attached to replacementfeeding, as it can be seen as an indication of HIV infectionin both resource-poor and resource-rich countries.41 WHOonly advocates replacement feeding if it is acceptable, feasible,affordable, safe and sustainable and recommends that, wherethis is not the case, women who are HIV-positive breastfeedtheir infant exclusively until the age of 6 months, then introducecomplementary foods and continue breastfeeding until the ageof 12 months.46 Mothers who are not eligible for HAARTshould continue START until all breastfeeding has ceased ifresources allow and antiretroviral prophylaxis is recommendedfor the infant depending on the maternal treatment strategy.22
In the UK exclusive replacement feeding is possible becausewomen have access to formula, clean water, sterilisingequipment, counselling and support from postnatal services.There is concern about the unknown risk of exposinguninfected breastfeeding infants to antiretroviral therapy,either through maternal HAART or infant prophylaxis, and thepotential for development of viral resistance in HIV-infectedinfants exposed to antiretroviral therapy who have yet to bediagnosed. This may be a priority in countries where supportfor formula feeding is readily available. The under-reportingof mixed feeding practices in those encouraged to formulafeed is also a concern, as there is no evidence on the risk oftransmission with mixed feeding from mothers on HAART.BHIVA and the Children’s HIV Association recently issuedguidance, in which they continue to recommend that mothers
C© 2012 Royal College of Obstetricians and Gynaecologists 21

HIV in pregnancy: an international perspective
known to be HIV-positive refrain from breastfeeding frombirth.47
Conclusion
At the United Nations Millennium Summit in 2000, 189 worldleaders agreed to meet the Millennium Development Goals.These include: halting the spread of HIV/AIDS, achievinguniversal access to treatment of HIV/AIDS to those who needit, reducing the under-5s mortality rate by two-thirds andreducing the maternal mortality ratio by two-thirds, by 2015.In June 2011, the ‘Countdown to Zero: Global Plan Towards theElimination of New HIV Infections in Children by 2015 andKeeping their Mothers Alive’ set ambitious goals to reduce newchildhood infections by 90%, and HIV-related maternal deathsby 50%.48 There has been considerable success in some areas:the coverage of antiretroviral treatment in poorer countrieshas increased four-fold over 5 years, there has been the firstdecline in the death rate from AIDS and there has been asignificant increase in the proportion of pregnant HIV-positivewomen getting antiretroviral therapy to prevent mother tochild transmission.5, 49 Nevertheless, we are still falling wellshort of the targets and the HIV/AIDS epidemic remains aglobal health emergency, with a significant impact on maternaland child mortality and morbidity.
Experience in the UK and other resource-rich countries hasshown that a universal antenatal HIV screening programme,with appropriate and timely interventions for HIV-positivewomen, can reduce the risk of mother to child transmissionof HIV to very low levels. The challenge of implementingthis strategy worldwide is considerable: without access tospecialist antenatal care, low-cost drugs and support forexclusive breast or formula feeding, HIV-positive women in thedeveloping world will continue to transmit the virus to theirchildren.
References1 Joint United Nations Programme on HIV/AIDS (UNAIDS) and
World Health Organization (WHO). Global HIV/AIDS Response:Epidemic Update and Health Sector Progress Towards UniversalAccess 2011. Geneva: WHO, 2011 [whqlibdoc.who.int/publications/2011/9789241502986_eng.pdf].
2 Hogan MC, Foreman KJ, Naghavi M, Ahn SY, Wang M, et al.Maternal mortality for 181 countries, 1980–2008: a systematicanalysis of progress towards Millennium Development Goal 5. Lancet2010;375:1609–23 [http://dx.doi.org/10.1016/S0140-6736(10)60518-1].
3 World Health Organization. PMTCT Strategic Vision 2010–2015:Preventing Mother-to-Child Transmission of HIV to Reach theUNGASS and Millennium Development Goals. Geneva: WHO; 2010[www.who.int/hiv/pub/mtct/strategic_vision.pdf].
4 World Health Organization. Antenatal Care in Developing Countries:Promises, Achievements and Missed Opportunities. An Analysis ofTrends, Levels and Differentials 1990–2001. Geneva: WHO; 2003[http://whqlibdoc.who.int/publications/2003/9241590947.pdf].
5 World Health Organization. Towards Universal Access: Scalingup Priority HIV/AIDS Interventions in the Health Sector. ProgressReport 2010. Geneva: WHO; 2010 [www.unicef.org/eapro/Towards_Universal_Access_on_HIVAIDS.pdf].
6 Townsend CL, Cortina-Borja M, Peckham CS, de Ruiter A, LyallH, et al. Low rates of mother-to-child transmission of HIVfollowing effective pregnancy interventions in the United Kingdomand Ireland, 2000–2006. AIDS 2008;22:973–81 [http://dx.doi.org/10.1097/QAD.0b013e3282f9b67a].
7 Wiktor SZ, Ekpini E, Nduati RW. Prevention of mother-to-childtransmission of HIV-1 in Africa. AIDS 1997;11 (Suppl B):S79–87.
8 De Cock KM, Fowler MG, Mercier E, de Vincenzi I, Saba J,et al. Prevention of mother-to-child HIV transmission in resource-poor countries: translating research into policy and practice. JAMA2000;283:1175–82 [http://dx.doi.org/10.1001/jama.283.9.1175].
9 Magder LS, Mofenson L, Paul ME, Zorrilla CD, BlattnerWA, et al. Risk factors for in utero and intrapartumtransmission of HIV. J Acquir Immune Defic Syndr 2005;38:87–95[http://dx.doi.org/10.1097/00126334-200501010-00016].
10 Garcia PM, Kalish LA, Pitt J, Minkoff H, Quinn TC, et al. Maternallevels of plasma human immunodeficiency virus type 1 RNA andthe risk of perinatal transmission. N Engl J Med 1999;341:394–402[http://dx.doi.org/10.1056/NEJM199908053410602].
11 International Perinatal HIV Group. Duration of rupturedmembranes and vertical transmission of HIV-1: a meta-analysisfrom 15 prospective cohort studies. AIDS 2001;15:357–68[http://dx.doi.org/10.1097/00002030-200102160-00009].
12 Haile-Selassie H, Tookey P, de Ruiter A. Duration of rupturedmembranes and vertical transmission of HIV: data from nationalsurveillance in the UK and Ireland. Second Joint Conference ofthe British HIV Association and the British Association for SexualHealth and HIV. Manchester, 2010. Abstract 02. HIV Medicine2010;11(Suppl 1):1–119 [www.bhiva.org/documents/Conferences/Manchester2010/Abstracts10Entire.pdf].
13 British HIV Association, British Association of Sexual Health and HIV,British Infection Society. UK National Guidelines for HIV Testing 2008.London: BHIVA; 2008.
14 Royal College of Paediatrics and Child Health. Reducing Mother toChild Transmission of HIV Infection in the United Kingdom. UpdateReport of an Intercollegiate Working Party. London: RCPCH; 2006[www.hpa.org.uk/webc/HPAwebFile/HPAweb_C/1197382224430].
15 Health Protection Agency. HIV in the United Kingdom:2009 Report. London: HPA; 2009 [www.hpa.org.uk/webc/HPAwebFile/HPAweb_C/1259151891830].
16 World Health Organization, UNAIDS. Guidance on Provider-initiatedHIV Testing and Counselling in Health Facilities. Geneva: WHO; 2007[www.who.int/hiv/pub/guidelines/9789241595568_en.pdf].
17 Sambisa W, Curtis S, Mishra V. AIDS stigma as an obstacleto uptake of HIV testing: evidence from a Zimbabweannational population-based survey. AIDS Care 2010;22:170–86[http://dx.doi.org/10.1080/09540120903038374].
18 Moodley D, Esterhuizen TM, Pather T, Chetty V, NgalekaL. High HIV incidence during pregnancy: compelling reasonfor repeat HIV testing. AIDS 2009;23:1255–9 [http://dx.doi.org/10.1097/QAD.0b013e32832a5934].
19 Soorapanth S, Sansom S, Bulterys M, Besser M, Theron G, FowlerMG. Cost-effectiveness of HIV rescreening during late pregnancy toprevent mother-to-child HIV transmission in South Africa and otherresource-limited settings. J Acquir Immune Defic Syndr 2006;42:213–21 [http://dx.doi.org/10.1097/01.qai.0000214812.72916.bc].
20 Bishop M, Foreit K. Serodiscordant Couples in Sub-SaharanAfrica: What Do Survey Data Tell Us? Washington DC: FuturesGroup, Health Policy Initiative, Task Order 1; 2010 [www.healthpolicyinitiative.com/Publications/Documents/1070_1_Serodiscordant_Couples_FINAL_3_04_10_acc.pdf].
22 C© 2012 Royal College of Obstetricians and Gynaecologists

Byrne et al.
21 Dunkle KL, Stephenson R, Karita E, Chomba E, KayitenkoreK, et al. New heterosexually transmitted HIV infections inmarried or cohabiting couples in urban Zambia and Rwanda: ananalysis of survey and clinical data. Lancet 2008;371:2183–91[http://dx.doi.org/10.1016/S0140-6736(08)60953-8].
22 World Health Organization. Antiretroviral Drugs for TreatingPregnant Women and Preventing HIV Infection in Infants:Recommendations for a Public Health Approach. Geneva: WHO; 2010[http://whqlibdoc.who.int/publications/2010/9789241599818_eng.pdf].
23 de Ruiter A, Mercey D, Anderson J, Chakraborty R, ClaydenP, et al. British HIV Association and Children’s HIV Associationguidelines for the management of HIV infection in pregnant women2008. HIV Med 2008;9:452–502 [http://dx.doi.org/10.1111/j.1468-1293.2008.00619.x].
24 Tariq S, Townsend CL, Cortina-Borja M, Duong T, Elford J, ThorneC, et al; European Collaborative Study; National Study of HIVin Pregnancy Childhood. Use of zidovudine-sparing HAART inpregnant HIV-infected women in Europe: 2000–2009. J AcquirImmune Defic Syndr 2011;57:326–33 [http://dx.doi.org/10.1097/QAI.0b013e31821d34d0].
25 Read PJ, Khan P, Mandalia S, Naftalin C, Harrisson U,et al. When should HAART be initiated in pregnancy toachieve an undetectable viral load? [Poster.] 17th Conference onRetroviruses and Opportunistic Infections. San Francisco, 2010[www.retroconference.org/2010/PDFs/896.pdf].
26 European Collaborative Study. HIV-infected pregnant women andvertical transmission in Europe since 1986. AIDS 2001;15:761–70[http://dx.doi.org/10.1097/00002030-200104130-00012].
27 Patel K, Shapiro DE, Brogly SB, Livingston EG, Stek AM, et al;P1025 team of the International Maternal Pediatric AdolescentAIDS Clinical Trials Group.Prenatal protease inhibitor use andrisk of preterm birth among HIV-infected women initiatingantiretroviral drugs during pregnancy. J Infect Dis 2010;201:1035–44 [http://dx.doi.org/10.1086/651232].
28 Townsend CL, Tookey PA, Newell ML, Cortina-Borja M. Antiretroviraltherapy in pregnancy: balancing the risk of preterm deliverywith prevention of mother-to-child HIV transmission. Antivir Ther2010;15:775–83 [http://dx.doi.org/10.3851/IMP1613].
29 Antiretroviral Pregnancy Registry Steering Committee. AntiretroviralPregnancy Registry International Interim Report for 1 January 1989through 31 January 2011. Wilmington, NC: Registry CoordinatingCenter; 2011 [www.apregistry.com/forms/interim_report.pdf].
30 Read JS, Newell MK. Efficacy and safety of cesarean delivery forprevention of mother-to-child transmission of HIV-1. CochraneDatabase Syst Rev 2005;(4):CD005479.
31 National Institute for Health and Clinical Excellence. NICEGuidance on Caesarean Section. London: National Institute forHealth and Clinical Excellence; 2011 [www.nice.org.uk/nicemedia/live/13620/57163/57163.pdf].
32 Dumont A, de Bernis L, Bouvier-olle M, Breart G; MOMA StudyGroup. Caesarean section rate for maternal indication in sub-Saharan Africa: a systematic review. Lancet 2001;358:1328–33[http://dx.doi.org/10.1016/S0140-6736(01)06414-5].
33 HES Online Hospital Episode Statistics. Maternity Data.NHS Maternity Statistics, 2009–10 [www.hesonline.nhs.uk/Ease/servlet/ContentServer?siteID = 1937&categoryID = 1475].
34 Lehman DA, Chung MH, John-Stewart GC, Richardson BA, Kiarie J,et al. HIV-1 persists in breast milk cells despite antiretroviral treatmentto prevent mother-to-child transmission. AIDS 2008;22:1475–85[http://dx.doi.org/10.1097/QAD.0b013e328302cc11].
35 Pillay K, Coutsoudis A, York D, Kuhn L, Coovadia HM. Cell-free virusin breast milk of HIV-1-seropositive women. J Acquir Immune DeficSyndr 2000;24:330–6.
36 Nduati R, John G, Mbori-Ngacha D, Richardson B, Overbaugh J,
et al. Effect of breastfeeding and formula feeding on transmissionof HIV-1: a randomized clinical trial. JAMA 2000;283:1167–74[http://dx.doi.org/10.1001/jama.283.9.1167].
37 Coutsoudis A, Dabis F, Fawzi W, Gaillard P, Haverkamp G,et al. Late postnatal transmission of HIV-1 in breast-fed children: anindividual patient data meta-analysis. J Infect Dis 2004;189:2154–66[http://dx.doi.org/10.1086/420834].
38 Coovadia HM, Rollins NC, Bland RM, Little K, CoutsoudisA, et al. Mother-to-child transmission of HIV-1 infectionduring exclusive breastfeeding in the first 6 months oflife: an intervention cohort study. Lancet 2007;369:1107–16[http://dx.doi.org/10.1016/S0140-6736(07)60283-9].
39 Peltier CA, Ndayisaba GF, Lepage P, van Griensven J, Leroy V, et al.Breastfeeding with maternal antiretroviral therapy or formula feedingto prevent HIV postnatal mother-to-child transmission in Rwanda.AIDS 2009;23:2415–23.
40 Marazzi MC, Nielsen-Saines K, Buonomo E, Scarcella P, GermanoP, et al. Increased infant human immunodeficiency virus-type onefree survival at one year of age in sub-Saharan Africa with maternaluse of highly active antiretroviral therapy during breast-feeding.Pediatric Infect Dis J 2009;28:483–7 [http://dx.doi.org/10.1097/INF.0b013e3181950c56].
41 Horvath T, Madi BC, Iuppa IM, Kennedy GE, Rutherford G,et al. Interventions for preventing late postnatal mother-to-childtransmission of HIV. Cochrane Database Syst Rev 2009;(1):CD006734[http://dx.doi.org/10.1097/QAI.0b013e3181b323ff].
42 Shapiro R. A randomized trial comparing highly active antiretroviraltherapy regimens for virologic efficacy and the prevention ofmother-to-child HIV transmission among breastfeeding women inBotswana (The Mma Bana Study). [Abstract.] 5th IAS Conferenceon HIV Pathogenesis, Treatment and Prevention, 19–22 July 2009,Cape Town, South Africa [www.ias2009.org/pag/Abstracts.aspx?SID=2435&AID=3821].
43 Kilewo C, Karlsson K, Ngarina M, Massawe A, Lyamuya E,et al. Prevention of mother-to-child transmission of HIV-1 throughbreastfeeding by treating mothers with triple antiretroviral therapy inDar es Salaam, Tanzania: the Mitra Plus study. J Acquir Immune DeficSyndr 2009;52:406–16.
44 Chasela C, Hudgens M, Jamieson D, Kayira D, Hosseinipour M, et al.Both maternal HAART and daily infant nevirapine (NVP) are effectivein reducing HIV-1 transmission during breastfeeding in a randomizedtrial in Malawi: 28 week results of the Breastfeeding, Antiretroviraland Nutrition (BAN) Study. 5th IAS Conference on HIV Pathogenesis,Treatment and Prevention, 19–22 July 2009, Cape Town, South Africa.Abstract no. WELBC103 [www.iasociety.org/Default.aspx?pageId =11&abstractId = 200722774%20].
45 Kesho Bora Study Group, de Vincenzi L. Triple antiretroviralcompared with zidovudine and single-dose nevirapine prophylaxisduring pregnancy and breastfeeding for prevention ofmother-to-child transmission of HIV-1 (Kesho Bora study): arandomised controlled trial. Lancet Infect Dis 2011;11:171–80[http://dx.doi.org/10.1016/S1473-3099(10)70288-7].
46 World Health Organization. Guidelines on HIV and Infant Feeding.2010. Principles and Recommendations for Infant Feeding inthe Context of HIV and a Summary of Evidence. Geneva: WHO;2010 [www.who.int/child_adolescent_health/documents/9789241599535/en/].
47 British HIV Association and Children’s HIV Association. PositionStatement on HIV and Infant Feeding in the UK. London: BHIVA;2010 [www.bhiva.org/BHIVA-CHIVA-PositionStatement.aspx].
48 UNAIDS. Countdown to Zero: Global Plan Towards the Elimination ofNew HIV Infections in Children by 2015 and Keeping their MothersAlive. Geneva: UNAIDS; 2011 [www.unaids.org/en/media/unaids/contentassets/documents/unaidspublication/2011/20110609_JC2137_Global-Plan-Elimination-HIV-Children_en.pdf].
C© 2012 Royal College of Obstetricians and Gynaecologists 23

HIV in pregnancy: an international perspective
49 United Nations. The Millennium Development Goals Report, 2011.New York: United Nations; 2011 [www.un.org/millenniumgoals/pdf/(2011_E)%20MDG%20Report%202011_Book%20LR.pdf].
50 International Perinatal HIV Group. The mode of delivery and therisk of vertical transmission of human immunodeficiency virustype 1 – a meta-analysis of 15 prospective cohort studies.
New Engl J Med 1999;340:977–87 [http://dx.doi.org/10.1056/NEJM199904013401301].
51 European Mode of Delivery Study Group. Elective caesarean-section versus vaginal delivery in prevention of vertical HIV-1transmission: a randomised clinical trial. Lancet 1999;353:1035–9[http://dx.doi.org/10.1016/S0140-6736(98)08084-2].
24 C© 2012 Royal College of Obstetricians and Gynaecologists