histiocytic and dendritic cell...
TRANSCRIPT

Histiocytic and Dendritic Cell Lesions
L. Jeffrey Medeiros, MD
MD Anderson Cancer Center

Outline
2016 classification of Histiocyte Society
Langerhans cell histiocytosis / sarcoma
Erdheim-Chester disease
Juvenile xanthogranuloma
Malignant histiocytosis
Histiocytic sarcoma
Interdigitating dendritic cell sarcoma
Follicular dendritic cell sarcoma
Rosai-Dorfman disease
Hemophagocytic lymphohistiocytosis

Writing Group of the Histiocyte Society

Group Name
L Langerhans-related
C Cutaneous and mucocutaneous
M Malignant histiocytosis
R Rosai-Dorfman disease
H Hemophagocytic lymphohistiocytosis
Major Groups of Histiocytic Lesions
Blood 127: 2672, 2016

L GroupLangerhans cell histiocytosisIndeterminate cell tumorErdheim-Chester disease
S100
Normal Langerhans cells

Langerhans Cell Histiocytosis“Old” Terminology
Eosinophilic granulomaSingle lesion of bone, LN, or skin
Hand-Schuller-Christian diseaseLytic lesions of skull, exopthalmos, and
diabetes insipidus
Letterer-Siwe diseaseWidespread visceral disease involving liver,
spleen, bone marrow, and other sites
Histiocytosis XTerm suggested by S. Farber and proposed by
L. Lichtenstein in 1953 Louis Lichtenstein1906-1977
Sidney Farber1903-1973

Langerhans Cell HistiocytosisIncidence and Disease Distribution
Incidence
Children: 5-9 x 106
Adults: 1 x 106
Sites of Disease
Bones 80%Skin 30%Pituitary gland 25%Liver 15%Spleen 15%Bone Marrow 15%Lymph nodes 10%CNS <5%
Poor Prognosis
LiverSpleen
Bone marrow
High-risk organs
Blood 127: 2672, 2016N Engl J Med 379: 856, 2018

Langerhans Cell HistiocytosisSolitary lesion of bone
CD1a
Eosinophilic Granuloma

Langerhans Cell HistiocytosisLymph Nodes
CD1a
LNs can be localized or a part of disseminated disease
This patient had generalized LNsand BRAF V600E mutation

Arch Pathol Lab Med 107: 59, 1983
Langerhans Cell HistiocytosisMorphologic Features
Frequency Feature
100% Langerhans cells (<5-75%)
92% Eosinophils
84% Multinucleated giant cells
75% Small lymphocytes
61% Necrosis
49% Neutrophils
29% Foamy histiocytes
Mild atypia (reactive type) in ~50% of cases
Mitotic rate: 0-23/10 high power fields

Langerhans Cell HistiocytosisImmunophenotype
Immunophenotype
S100+, CD1a+, CD207/langerin+
Cyclin D1 is usually +
+/- CD4, CD11c, CD45/LCA, CD68, lysozyme+
Note: S100, CD1a, and CD207/langerin are not restricted to Langerhans cells

Langerhans Cell HistiocytosisBirbeck Granules
Michael S. C. Birbeck, PhD1925-2005
Also known as Langerhans bodies
Birbeck granules are characteristic (but not unique to) Langerhans cells
Presence is a reflection of membrane activity; function debated
Contain langerin = a type II transmembrane lectin receptor
J Invest Dermatol 37: 51, 1961CR Acad Sci (Paris) 261:5719, 1965
Francoise Basset, PhD

Blood 124: 1655, 2014
Blood 116: 1919, 2010
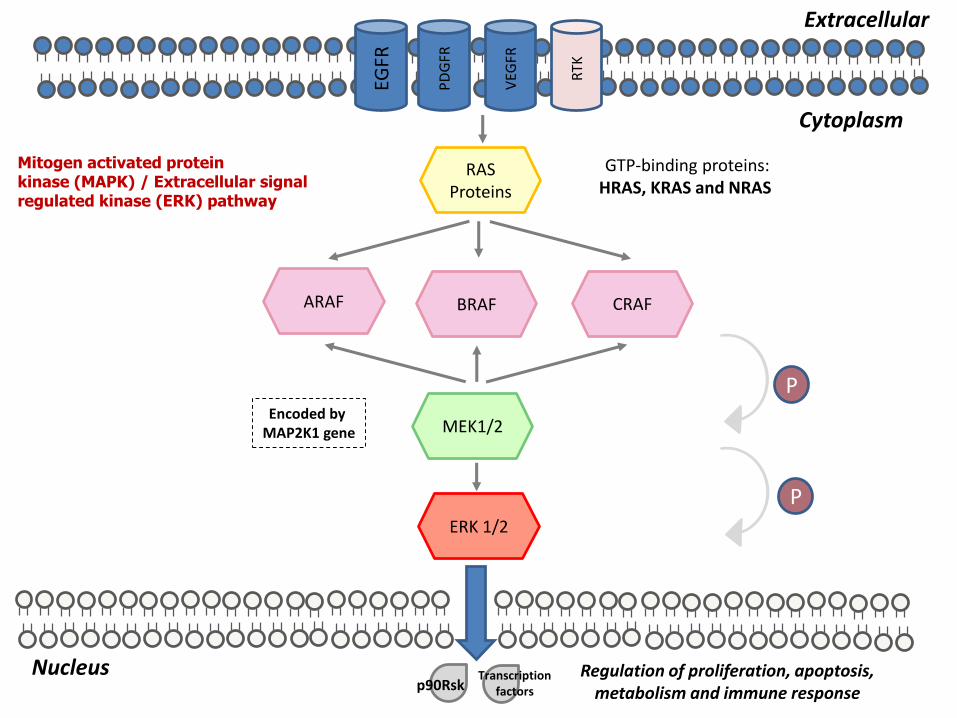
Langerhans Cell HistiocytosisMutations in BRAF/MAP2K1 Are Common
BRAF V600E 18/40 (45%)MAP2K1 11/40 (27.5%)

Blood 128: 2533, 2016
85% of LCH cases have genetic abnormalities of the MAPK pathway
They likely all do
PD
GFR
VEG
FR
RTK
EGFR
Cytoplasm
Extracellular
RAS Proteins
GTP-binding proteins:HRAS, KRAS and NRAS
ARAF BRAF CRAF
MEK1/2
ERK 1/2
Nucleus Regulation of proliferation, apoptosis, metabolism and immune response
Encoded by MAP2K1 gene
p90RskTranscription
factors
P
P
Mitogen activated protein kinase (MAPK) / Extracellular signal regulated kinase (ERK) pathway
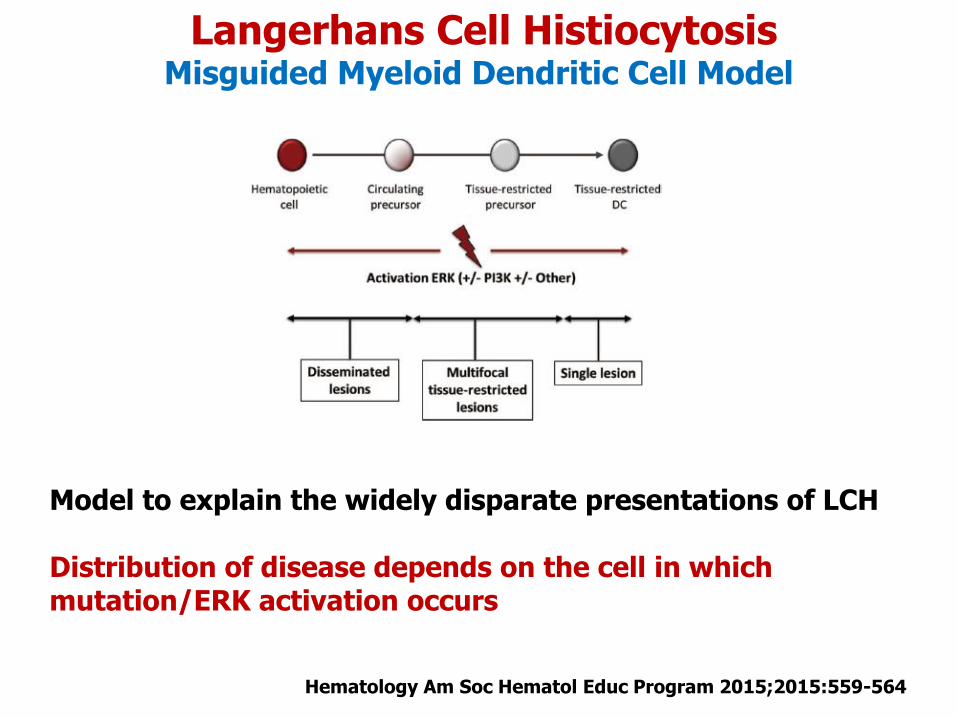
Langerhans Cell HistiocytosisMisguided Myeloid Dendritic Cell Model
Model to explain the widely disparate presentations of LCH
Distribution of disease depends on the cell in which mutation/ERK activation occurs
Hematology Am Soc Hematol Educ Program 2015;2015:559-564

Immunity 44: 439, 2016

Arch Pathol Lab Med 107: 59, 1983
“Histiocytosis X (HX) has the advantage of widespread use, although it has been applied to other types of histiocytosis. The generally recognized Langerhans cell derivation of HX makes Langerhans cell histiocytosis an attractive alternative.”

Br J Hematol 169: 3-13,2015

Langerhans Cell HistiocytosisLungs
CD207BRAF V600E
Associated with smoking

Langerhans Cell HistiocytosisDifferential Diagnosis
Indeterminate dendritic cell tumor
Langerhans cell sarcoma

Indeterminate Dendritic cell Tumor
Thought to be derived from normal precursors of Langerhans cells (so-called indeterminate cells)
Patients present with > nodules, papules or plaques on skin
Dermis-based disease that can extend into subcutaneous fat
Histologically looks like Langerhans cells histiocytosis
But often no eosinophils
Immunophenotype: CD1a+, S100+, CD207-
Electron microscopy: No Birbeck granules
Genetics: ETV3-NCOA2/t(1;8)(q23.1;8q13.3) reported in 3 cases
Highly variable clinical course: Spontaneous regression or progression

Indeterminate Dendritic Cell Tumor
CD1a
CD207A negative langerin/CD207 is required to make this diagnosis

Langerhans Cell Sarcoma
History Rarely preceded by typical LCH (in my experience)
Age and Sites of DiseaseMedian 41 yrs (10-72yrs)Extranodal ~ 80% (most often skin); nodal ~ 20%
Ancillary Support for DiagnosisImmunohistochemistry: S-100+, CD1a+, CD207/langerin+Electron microscopy: Birbeck granules
GeneticsRare cases with monoclonal IGH rearrangements
Prognosis ~50% mortality as a result of progressive disease
DefinitionA high-grade neoplasm with overt malignant cytologic features and Langerhans cell phenotype

Langerhans Cell Sarcoma
CD207

Erdheim-Chester DiseaseDefinition
Jacob Erdheim, MD William Chester, MD
Described by W. Chester in single author paper in German in 1930.
J. Erdheim was mentor
Renamed Erdheim-Chester disease in 1972
“A clonal, systemic proliferation of histiocytes, commonly having a foamy (xanthomatous) component and containing Touton giants cells.”
2017 WHO book p. 481

Erdheim-Chester DiseaseClinicopathologic Features
Age and Sex RatioMedian 53 years (range, 20-74)Sex ratio: 3 to 1 male predominance
SymptomsCan be asymptomatic or aggressive; related to sitesDull and deep bone pain common (especially knees)
Histologic featuresBland histiocytes infiltrate tissues
Foamy or eosinophilic cytoplasm; Touton giant cellsFibrosis is common; +/- lymphocytes, plasma cells, eosNo mitoses, necrosis, granulomas, emperipolesis
ImagingBilateral, symmetric cortical osteosclerosis of long bonesSurrounds aorta (“coated”) or kidney (“hairy kidney”)
GeneticsBRAF V600E mutations in ~50%, ~4% NRAS, ~10% PI3KA
Blood Advances 1:357, 2017

Erdheim-Chester Disease
CD68 CD1a
PositiveCD14CD68CD163FascinFactor XIIIa
NegativeCD1aCD207

Erdheim-Chester DiseaseRadiologic Images
Case courtesy of Dr Andrew Dixon, Radiopaedia.org, rID: 9351
Case courtesy of Dr Andrew LawsonRadiopaedia.org, rID: 29803

Blood 124:1119, 2014
23 patients with both LCH and ECD
BRAF V600E in 11/16 (69%) LCH and 9/11 (82%) ECD
LCH ECD

C Group
Many different lesions
Can subdivide into 2 broad groupsXanthogranulomaNon-xanthogranuloma

Juvenile Xanthogranuloma
Affects children >> adults
Rare: < 1% of all pediatric tumors
Single, few, or multiple lesions on skin: yellow papules 0.5-1 cmOften regress spontaneously
Long bones are not involved
Rarely patients have visceral involvement or disseminated diseaseCan cause symptoms or death due to local invasion
GeneticsLocalized
CGH: chromosomal abnormalities uncommon (~5%)
Disseminated CGH: nonspecific chromosomal abnormalities described
BRAF V600E and MAPK1 mutations reported (few cases) (Oncotarget 8: 46065, 2017; Hum Pathol 69: 118, 2017)
Mod Pathol 30:1234, 2017

Juvenile Xanthogranuloma
Immunophenotype
CD14+ CD68+ CD163+
Factor XIIIa +/-
S-100+ ~20% Fascin+ ~20%
CD1a- CD207/langerin -

MAPK Pathway Mutations in Histiocytic Lesions A Unifying Feature in Pathogenesis
Hematology Am Soc Hematol Educ Program 2015; 2015:559-564
LCH = Langerhans cell histiocytosisJXG = Juvenile xanthogranulomaECD = Erdheim-Chester disease

M GroupHistiocytic sarcoma
Interdigitating dendritic cell sarcoma
Langerhans cell sarcoma
“…we recommend reusing the old-term malignant histiocytosis, and refer to the phenotype as a subtype.”
Blood 127: 2672, 2016

Histiocytic SarcomaDefinition and Clinicopathologic Features
DefinitionA malignant proliferation of cells with morphologic and immunophenotypic features of mature tissue histiocytes
EpidemiologyMedian age = 52 y; males = femalesSubset associated with B-cell lymphoma (transdifferentiation) Rare pts with mediastinal germ cell tumor and isochromosome 12p
PresentationOften extranodal (GI tract, skin, soft tissues) Can be nodal or disseminated (“malignant histiocytosis”)
GeneticsSubset of cases with monoclonal Ig rearrangements
OutcomeClinically aggressive; poor response to therapy60-80% of patients die of disease
2017 WHO book p. 468-470

Transdifferentiation
Stoecker and Wang. Arch Pathol Lab Med 137: 865, 2013

Histiocytic SarcomaCD11c
CD163

Histiocytic SarcomaImmunophenotype
Positive VimentinS100 (weak or focal), Ki-67 10-20%ZBTZ46 (Mod Pathol 31:1479, 2018)
Variably PositiveFascin
Weakly and variably positiveCD45/LCA, CD68, lysozyme
NegativeCD1a, CD207/langerin
CD21, CD23, CD35, clusterin
CD34, myeloperoxidase
EMA, keratins, melanoma-associated antigens
B-cell and T-cell antigens 2017 WHO book p. 475

Mod Pathol 2019 (Epub)
Methods
28 cases of histiocytic sarcoma
NGS, hybrid capture, 447 gene panel
Copy number analysis
Results
16 (57%) with mutations in RAS-MAPK pathway
MAP2K1 most common
6 (21%) with mutations of PI3K-AKT-MTOR pathway
13 (48%) loss of CDKN2A / p16
7 (25%) with aberrant somatic mutation signature
Suggests possible B-cell origin
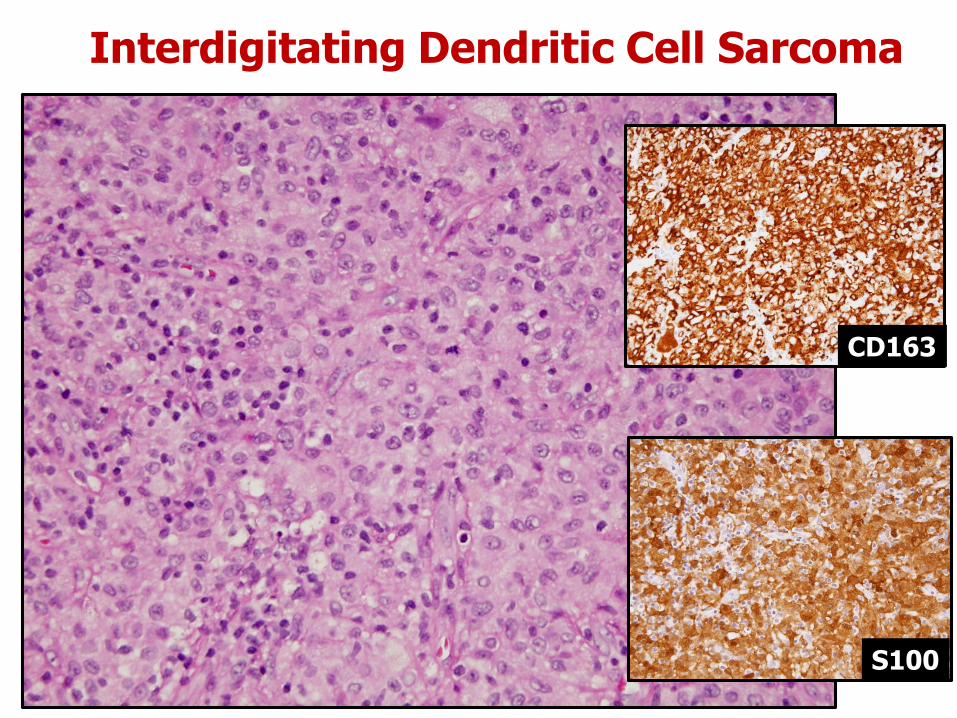
Interdigitating Dendritic Cell Sarcoma
S100
CD163

Interdigitating Dendritic Cell SarcomaDefinition and Clinicopathologic Features
DefinitionA neoplastic proliferation of spindle to ovoid cells with phenotypic features similar to those of interdigitating dendritic cells
EpidemiologyRare Usually adults; males > females
PresentationSolitary lymph node involvement most commonCan be extranodal or widely disseminated
GeneticsSubset of cases with monoclonal IGH rearrangementsRare cases reported with BRAF V600E mutation
OutcomeClinically aggressive50% of patients die of disease
2017 WHO book p. 476

Interdigitating Dendritic Cell SarcomaImmunophenotype
Positive S100 (diffuse and intense), vimentinKi-67 10-20%
Variably PositiveFascin
Weakly and variably positiveCD45/LCA, CD68, lysozyme
NegativeCD1a, CD207/langerin
CD21, CD23, CD35, clusterin
CD34, myeloperoxidase
EMA, keratins, melanoma-associated antigens
B-cell and T-cell antigens
2017 WHO book p. 476
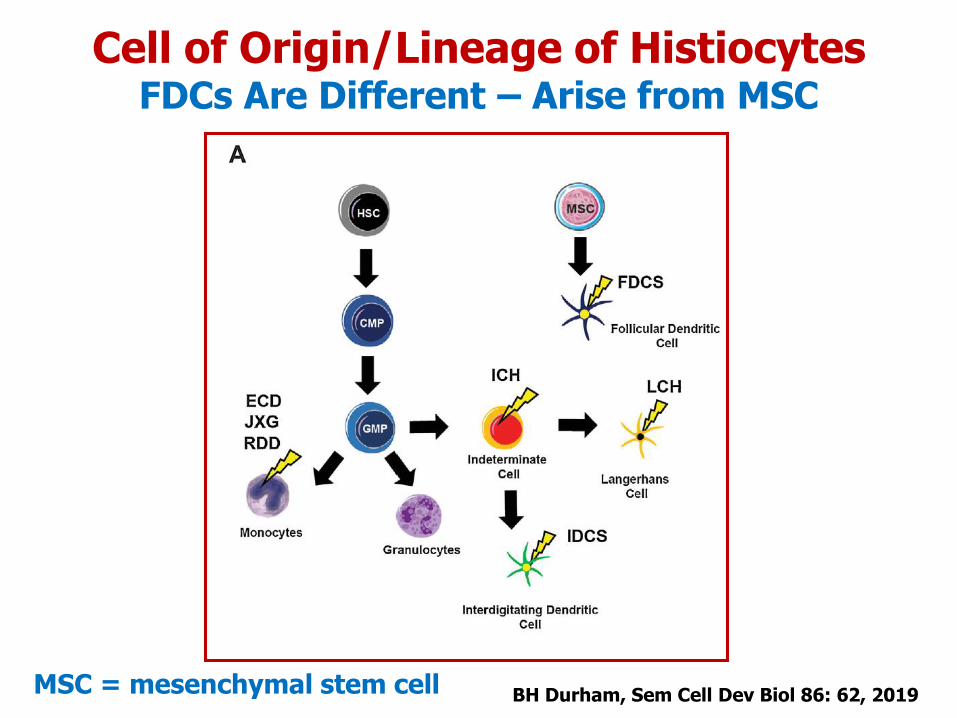
BH Durham, Sem Cell Dev Biol 86: 62, 2019
Cell of Origin/Lineage of HistiocytesFDCs Are Different – Arise from MSC
MSC = mesenchymal stem cell

Follicular Dendritic Cell SarcomaDefinition and Clinicopathologic Features
DefinitionA neoplasm with morphologic and immunophenotypic features of follicular dendritic cells
EpidemiologyUsually adults; males = femalesSmall subset arises in hyaline-vascular Castleman disease
PresentationExtranodal 58%, Nodal 31%, both 11%
GeneticsSubset of cases with monoclonal IGH rearrangementsComplex karyotypeMutations in genes that regulate NF-kB pathway0-20% of cases reported with BRAF V600E mutation
OutcomeNeed to resect completely; +/- XRT or chemotherapy~1/3 of pts recur locally; ~1/3 distant metastases
2017 WHO book p. 476-479

Follicular Dendritic Cell SarcomaImmunophenotype and Electron Microscopy
Positive (often variable/focal)VimentinCD21, CD23, CD35 CXCL13, clusterin, D2-40, EGFR, fascinKi-67: 5-25%
Weakly and variably positiveCD68, EMA, S100 (focal), HLA-DR
NegativeCD1a, CD207/langerin
CD34, myeloperoxidase
Keratins, melanoma-associated antigens
B-cell and T-cell antigens
Electron microscopy
Long cytoplasmic processes; desmosomes 2017 WHO book p. 475-476

Follicular Dendritic Cell SarcomaSpindled
CD35

Follicular Dendritic Cell SarcomaEpithelioid
CD21

R Group
Rosai-Dorfman disease

Rosai-Dorfman DiseaseHistory
Juan Rosai, MD Ronald F. Dorfman, MD
Described in detail by Rosai and Dorfman in 1969
Designated as sinus histiocytosis with massive lymphadenopathyArch Pathol Lab Med 87: 63, 1969
First described in French in 1965 by Destombes
Reported as adenitis with lipid excessBull Soc Pathol Exot Filiales 58: 1169, 1965
Pierre-Paul Destombes, MD

Azoury FJ, Reed RJ. N Eng J Med 274:928-930, 1966
Rosai-Dorfman Disease A Case Report
Richard J. Reed, MD

Rosai-Dorfman DiseaseClinicopathologic Features
Most cases are sporadic
Rare familial forms
H (Faisalabad) syndrome
SLC29A3 mutation
Autoimmune lymphoproliferative syndrome
TNFRSF6 mutation
Presentation
~60% Lymphadenopathy
Bilateral large, painless cervical LNs
Other lymph node groups can be involved
+/- fever, night sweats, weight loss, fatigue
~40% Extranodal sites of disease Sem Diagn Pathol 33:244, 2016

Rosai-Dorfman DiseaseBilateral Cervical Lymphadenopathy is Common
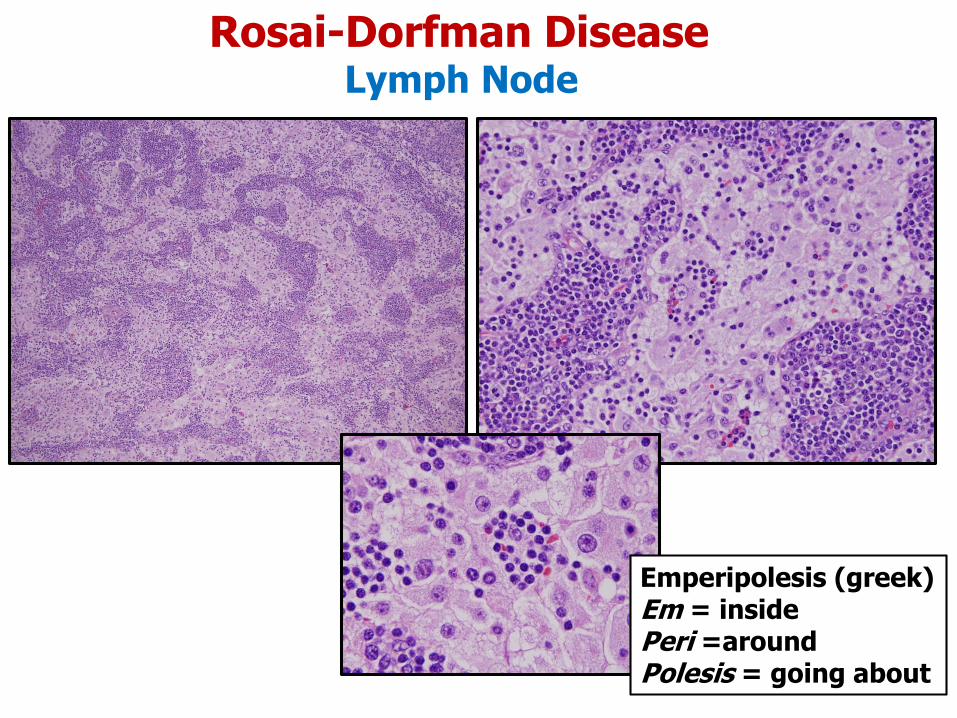
Rosai-Dorfman DiseaseLymph Node
Emperipolesis (greek)Em = insidePeri =aroundPolesis = going about

Anatomic Site Frequency
Nasal cavity and paranasal sinuses 11.3%
Soft tissue 8.9%
Orbit/eyelid 8.5%
Bones 7.8%
Skin 6.8%
Genitourinary system 6.4%
Major salivary glands 5.2%
Central nervous system 4.7%
Oral cavity 2.6%
Lungs, larynx, liver, tonsil, breast,
GI tract, thyroid, heart
Each < 2%
Extranodal Sites Involved by RDD
E. Foucar et al. Semin Diagn Pathol 7:19, 1990

Rosai-Dorfman DiseaseSoft Tissue
S-100
Emperipolesis is less in RDD at extranodal sites

Rosai-Dorfman DiseaseImmunophenotype
S100
Positive
S100 protein
CD68
CD163
Fascin
HLA-DR
Negative
CD1a
CD207/langerin
CD3, CD20
Beware
IgG4 plasma cells can be numerous in RDD

Mod Pathol 30: 1367, 2017MAP2K1 c.157 T>G p.F53V
7/21 (33%) cases with KRASor MAP2K1 mutation
All point mutations
KRAS exon 2 (n=2) or exon 4 (n=2)MAP3K1 exon 1 (n=1) or exon 3 (n=2)
VAF ~ 5%
Mutations correlated with
Head and neck site
Younger ageMultifocal disease
No correlation with outcome
Sofia Garces, MD

N Engl J Med 377: 2398, 2017
Before After
H Group
Hemophagocytic lymphohistiocytosis
Hemophagocytic lymphohistiocytosis (HLH)Definition and Classification
Definition
A syndrome of severe immune activation and dysregulation characterized by hyperactive macrophages and lymphocytes, proinflammatory cytokine hypersecretion, tissue infiltration, hemophagocytosis, and organ damage.
Types of HLH
Primary (familial)Genetic defects that impair cytotoxic immune function
Secondary
Malignant neoplasms
Non-malignantInfectionAutoimmune diseaseFollowing organ transplantationIatrogenic immune suppression Cancer 123:3229, 2017

Hemophagocytic lymphohistiocytosisPrimary
Epidemiology
Most patients are young childrenIncidence is 1 in 50,000-100,000 live births
Genetics
Biallelic mutations in genes that encode for molecules involved in cytotoxic granule activation, fusion, function, etc.
Examples: PRF1 (perforin), STX11 (syntaxin 11), SH2D1A
Mendelian inheritance for many of these genes
Survival
Median = 2 months without treatment
Therapy
Etoposide, dexamethasone, and intrathecal methotrexateAllogeneic stem cell transplantation

Hemophagocytic lymphohistiocytosisSecondary
Epidemiology
Most patients are adultsMalignant neoplasms are usually hematologic
Lymphomas, acute leukemias, MDS, T/NK-cell neoplasms
InfectionEBV, CMV, bacteria, fungi, protozoa
Autoimmune (AKA macrophage activation syndrome)Systemic lupus erythematosus, juvenile RA, polymyositis
Organ TransplantationStem cell or solid organ
Mortality Rate
80%
Therapy
Treat the neoplasmSuppress immune activation

Hemophagocytic lymphohistiocytosisCriteria for Diagnosis
1. Fever2. Splenomegaly3. Cytopenias affecting >2 cell lineages 4. Elevated triglycerides and/or hypofibrinogenemia5. Hemophagocytosis in bone marrow, spleen, or lymph nodes6. Low or absent NK-cell activity7. Elevated serum ferritin8. High levels of soluble IL-2 receptor alpha
5 of 8 criteria are required to establish diagnosis of HLHGenetic testing, if positive, trumps
Pediatr Blood Cancer 48:124, 2007
One can establish a diagnosis of HLH without morphologic evidence

Hemophagocytic lymphohistiocytosisSecondary to EBV Infection
Patient with mantle cell lymphoma who died of HLH
EBER
LN
BM smear

Paul LangerhansCirca 1867
Paul Langerhans1847-1888
Paul and Margarethe Langerhans1885
Grave site on Madeira Island