highlights from the bree collaborative guideline on prescribing opioids in dentistry ·...
TRANSCRIPT

Highlights from the Bree Collaborative Guideline on Prescribing Opioids in Dentistry
North Central Accountable Community of Health
May 3, 2019
Rolf Christensen, DDS, [email protected]
& some prescribing pearls
Rolf Christensen, DDS, MHA
Director, Dental Urgent Care ClinicDirector, Oral Medicine Clerkship
Dental Director, Mountain West AIDS Education Center

Whe
re w
e ar
e at

WA PMP North Central chronic opioid rx 2018-Q1
Similar to several WA accountable communities

WA PMP Chelan County chronic opioid rx 2018-Q1
Similar to several WA counties
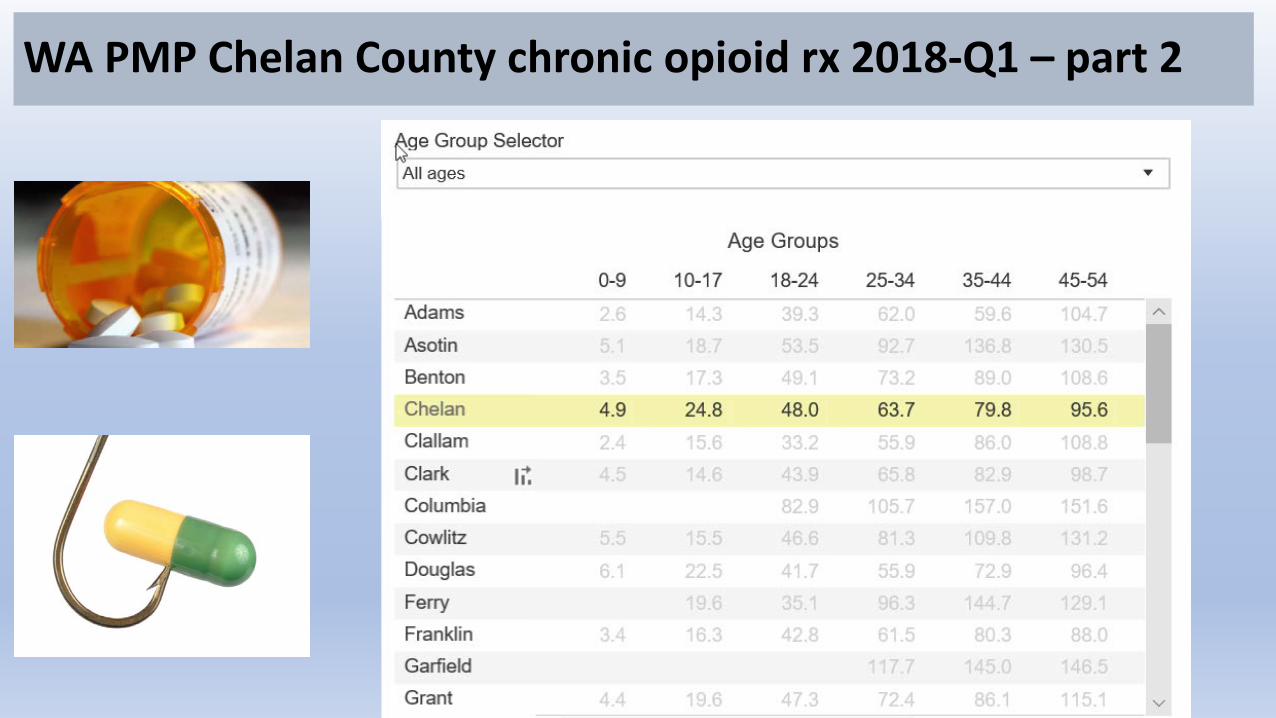
WA PMP Chelan County chronic opioid rx 2018-Q1 – part 2

WA State heroin deaths 2015-2017 (Ctr Health Statistics, DOH)
8

Objectives• Background on how we got to where we are, recent evidence and
emerging best practice
• Highlights of the Bree Collaborative Dental Guideline on Prescribing Opioids for Acute Pain Management (2017)
• Some prescribing pearls
• Compliance with new WA State Opioid Prescribing Rules
• Taking to ground level – panel discussions

RULES & BEST PRACTICES
ARE NOT THE SAME

Why use opioids
Pain is a common symptom in dentistry
• Opiates are efficacious analgesics w/ wide spread use• No anti-inflammatory effects• Respiratory depression, sedation• Constipation, urinary retention, nausea vomiting• Dependence, addiction & relapse risk
• Analgesia is dose dependent• Tolerance to respiratory depression is slower than tolerance to
analgesia – caution sleep disorders


Objectives
•Highlights of the Bree Collaborative Dental Guideline on Prescribing Opioids for Acute Pain Management (2017)

Where does this guideline come from?
• Dr. Robert Bree Collaborative
• Public & private stakeholders (~23), appointed by the governorPublic healthcare purchasers for WA state Private healthcare purchasers (employers, union trusts)Health plans Physicians & other healthcare providers HospitalsClinician organizations Quality Improvement organizations
• Collaborative members identify specific ways to improve health care quality, outcomes and affordability in Washington State (i.e. patient safety)

Bree Collaborative
historical activities
Hysterectomy 1/2018
Total knee and hip replacement bundle and warranty 10/2013
Dental guideline on prescribing opioids for acute pain 9/2017
Opioid prescribing metrics 7/2017
Opioid use disorder treatment 11/2017
Bariatric surgical bundle 11/2016
Oncology care 3/2016
Coronary artery bypass graft surgical bundle 9/2015
Addiction and dependence treatment 1/2015
End of life care 11/2014
Potentially avoidable Hospital readmissions 7/2014
Lumbar fusion surgical bundle and warranty 9/2014

Bree CONSENSUS BUILDING PROCESS for dental guideline
• Bree Collaborative provided opportunity and support
March 2017 summit convenedBroad invitation
Working grp, conf calls, email, meetings, written draft
Guideline approved by Bree Collaborative - Sept 2017
Dental Guideline on Prescribing Opioids for Pain Management – September 2017
In collaboration with broad advisory group(diverse representation, interests & practices)
Compare it to the CDC, ADA & other policies and guidelines
AMDG Guidelines
Be aware of externalities – your county, state and more
Dental Guideline on Prescribing Opioids for Pain Management – September 2017
Easy to use referenceSet of clinical guidelinesResources in the appendices
Helps align your opioid Rx practices with current evidence

Highlights of the
2017 Bree/AMDG Dental Guideline
on Prescribing Opioids for Pain
Rolf Christensen, DDS, [email protected]
Spokane, WA 4/19/2018
Seattle, WA 4/20/2018

Non-opioid analgesics as the FIRST line of pain control for dental procedures
1. Non-steroidal anti-inflammatory drugs (NSAIDs) & acetaminophen where pain anticipated – unless contraindications
2. If an opioid is warranted, follow the CDC recommendation – lowest effective dose… no longer than needed… (next slide)
• Prescribe opioids IN COMBINATION with first line therapy
• Avoid multiple acetaminophen preparations at same time

CDC guidelines:
“clinicians should prescribe the lowest effective dose of immediate-release opioids and should prescribe no greater quantity than needed for the expected duration of pain severe enough to require opioids. Three days or less will often be sufficient; more than seven days will rarely be needed”
If warranted, prescribe opioids for pain controlin combination with FIRST line non-opioids
Minor surgical procedures:
Adults – 3 days or less (rarely 7 days)
Adolescents & young adults to age 24 – limit opioids to 8 - 12 tablets
Bree Guideline clinical recommendations
= good practice
Skilled initial patient assessment -includes use of PMP
Individualized pain management strategies
Effective intervention
Re-assessment as necessary
Rare instances of chronic orofacial pain = AMDG Interagency Guideline on Rx Opioids for Pain
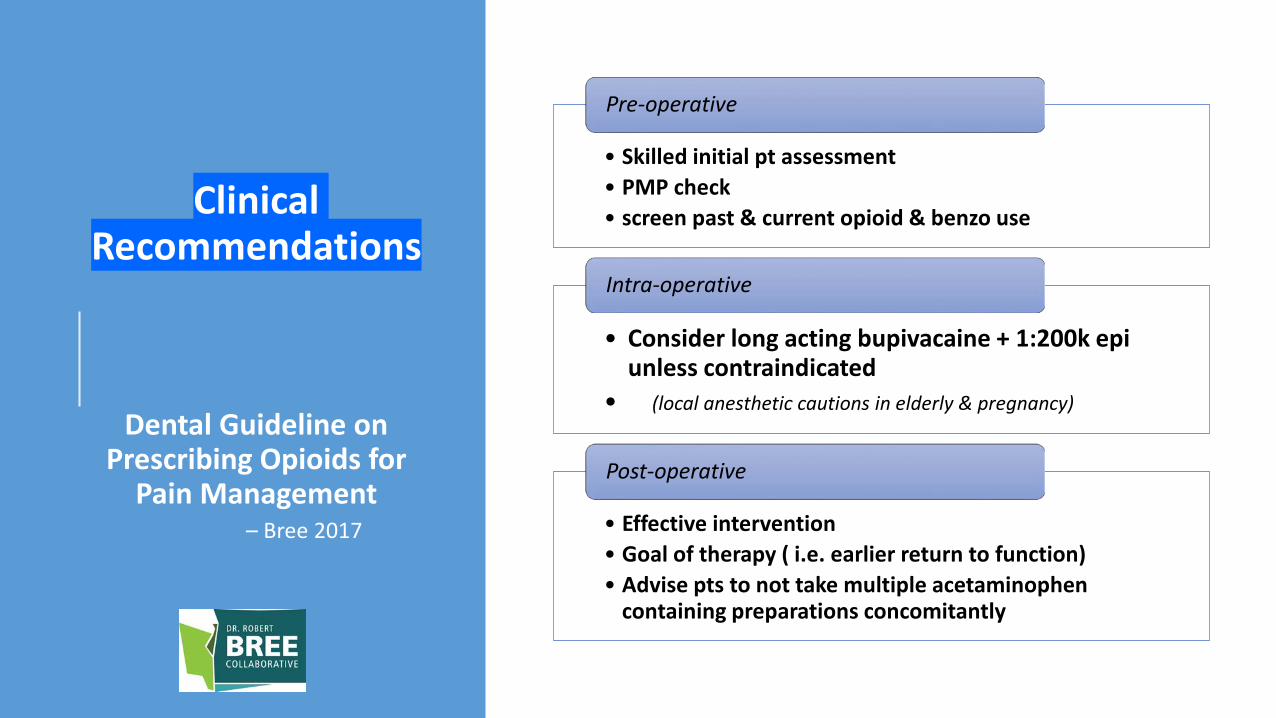
Clinical Recommendations
Dental Guideline on Prescribing Opioids for
Pain Management – Bree 2017
• Skilled initial pt assessment• PMP check• screen past & current opioid & benzo use
Pre-operative
• Consider long acting bupivacaine + 1:200k epi unless contraindicated
• (local anesthetic cautions in elderly & pregnancy)
Intra-operative
• Effective intervention• Goal of therapy ( i.e. earlier return to function)• Advise pts to not take multiple acetaminophen
containing preparations concomitantly
Post-operative

Non-opioid analgesics as the FIRST line of pain control for dental procedures
Non-steroidal anti-inflammatory drugs (NSAIDs) & acetaminophen where pain anticipated – unless contraindications
NSAID contraindications include hypersensitivity, hx gastrointestinal bleeding, aspirin sensitivity asthma
Acetaminophen contraindications include hypersensitivity, severe liver disease

Adjust dose or duration & monitor pts with
1) hepatic impairment (i.e. acetaminophen)
2) renal impairment (i.e. NSAIDs)
3) drug-to-drug interactions (use drug interaction app)
4) > 2 to 3 alcohol-containing drinks/day (ask, screen)
Consider cyclooxygenase-2 inhibitor (COX2, i.e. celecoxib) COX-2 inhibitor at moderate doses are noninferior to naproxen, ibuprofen for cardiovascular risk (PRECISION study), Cardiovascular Safety of Celecoxib, Naproxen, or Ibuprofen for Arthritis, NEJM 2016; 2516-2529

1) Appropriate use & duration2) Possible adverse effects, incl sensation of drug
craving3) Share info on drug disposal (next slide)
4) Avoid combining opioids with CNS depressants - benzodiazepines, sedative-hypnotics, anxiolytics
Educate patient & familyrisk / benefit

Community-based take back programs / DEA-approved
Unwanted meds in the home harm othersSafe disposalSelect areas
o Not all accept controlled rxo Pharmacies & police stations
http://www.takebackyourmeds.org/
WA state “Take back your meds” program

Know your tools
NSAIDs, acetaminophen,
drug interactions, contraindications

Treatment plan (peri- & post-procedure care)
• Rational plan / rational prescribing* (*if indicated)
• Physical methods ice packs, heat, massage
• Pharmacotherapy Therapeutics & analgesics / OTC & Rx
• Goal of therapy = pain relief, take the edge off - earlier return to function
• Discussion with pt

no rx↔ NSAIDs↔ acetaminophen ↔ opiates
• Mild to moderate, uncomplicated, nonpsychogenic pain• OTC analgesics = first line of therapy
• Simple analgesics – NSAIDs, acetaminophen
• Maximize non-opiate when possible
• Opiates as “rescue” meds
Pharmacotherapy plan - opiates
• Use a balanced approach• Risk / benefit analysis
• NSAID/acetaminophen backbone when indicated• Opiates as needed
• No need to start with less potent before attempting a more potent analgesic (i.e. opiate)

Pharmacotherapy plan – risk / benefitMatch the complete pain presentation to the appropriate agent & use a reasonable dose & duration
NSAID advantages• No respiratory depression, sedation• No constipation• Anti-inflammatory• No central nausea• No risk of habituation or addiction
NSAID disadvantages• GI irritation• Patient expectations not fulfilled• Drug interactions• Renal effects
Acetaminophen advantages• Little anti-platelet activity• Less potential GI irritation• Used in pregnancy• Small amount in breast milk
Acetaminophen disadvantages• Little anti-inflammatory action• Dose related adverse effects• Metabolites toxic & can accumulate• Dose adjust or avoid in hepatitis• Caution in alcoholics & fasting eating disorders

Pharmacotherapy plan - NSAID • NSAIDs both analgesic, anti-inflammatory & anti-pyretic
• Inhibits COX activity• Dose dependent analgesia & side effects• Ceiling effect analgesia (i.e. Ibuprofen 400mg)• No ceiling effect anti-inflammatory effect – (limited by side effects, bleeding, GI)
• Aspirin is unique = irreversibly inactivates COX • Suppresses prostaglandin & thromboxane production• (irreversibly acetylates serine 530 on COX-1 & a serine COX-2) • Antiplatelet effects (consider local factors)
• Platelet lifespan is 7-10 days

NSAID• Ibuprofen (proprionic class of NSAIDS)
• 400 or 600 mg every 6 hours• Side effects dose related – nausea, dyspepsia, gastric bleeding
• Naproxen (Naprosyn, Naprelan) 500mg initially, 250mg subsequently
• Naproxen sodium (Anaprox) 550mg initially, 275 subsequently (propionic acid class)
• Sulindac (Clinoril®) less effect on bleeding (salicylate salt)
• Ketorolac (Toradol® limit to 5 days) (pyrroacetic acid)
• Indomethacin (indoleacetic acid)

Opiate experienced patients
•Desensitized opiate receptors•Hyperalgesia
• Substance Abuse and Mental Health Services Administration (SAMSHA) recommends 1.5 x normal dosing
• SAMSHA is an agency within the US Dept of Health & Human Services
• Return to normal chronic opioid dose as soon as possible

Additional background on your tools

NSAID risks - Ibuprofen relatively fewer Adverse Events
• Renal adverse effects are well known• Normal renal function partially dependent of PG synthesis• PG maintain proper dilation of renal vasculature• Cause water & Na+ retention
• GI bleeding, ulcer (take w/ 8oz water, upright 20 minutes)
• Cardiac, hyperkalemia, heart failure, confusion, brochospam
• Drug interactions

Anticoagulants - NSAIDs adverse drug interactions
•AVOID the combination w/ NSAIDS• 2.4x risk of major bleed• Even for a few days ?
apixaban Eliquis®dabigatran Pradaxa®rivaroxaban Xarelto®warfarin Coumadin® & other names

anti-hypertensives - NSAIDs adverse drug interactions
•Caution with anti-hypertensives • (all anti-hypertensives except calcium channel
blockers = which are least affected)
• NSAIDS inhibit prostaglandin-mediated vasodilation
• NSAIDS promote salt & water retention• Can reverse effects of hypotensive drugs
= HYPERTENSION

anti-hypertensives - NSAIDs adverse drug interactions
• Ca++ channel blockers ~ok
• ACE inhibitors “pril” drugs
• ARB – angiotensin II receptor blockers
• β – blockers
• ~risk of hypertension
• ~risk of acute kidney injury• Typically not seen in normotensive pts & normal renal function• More often with kidney disease & blood pathologies
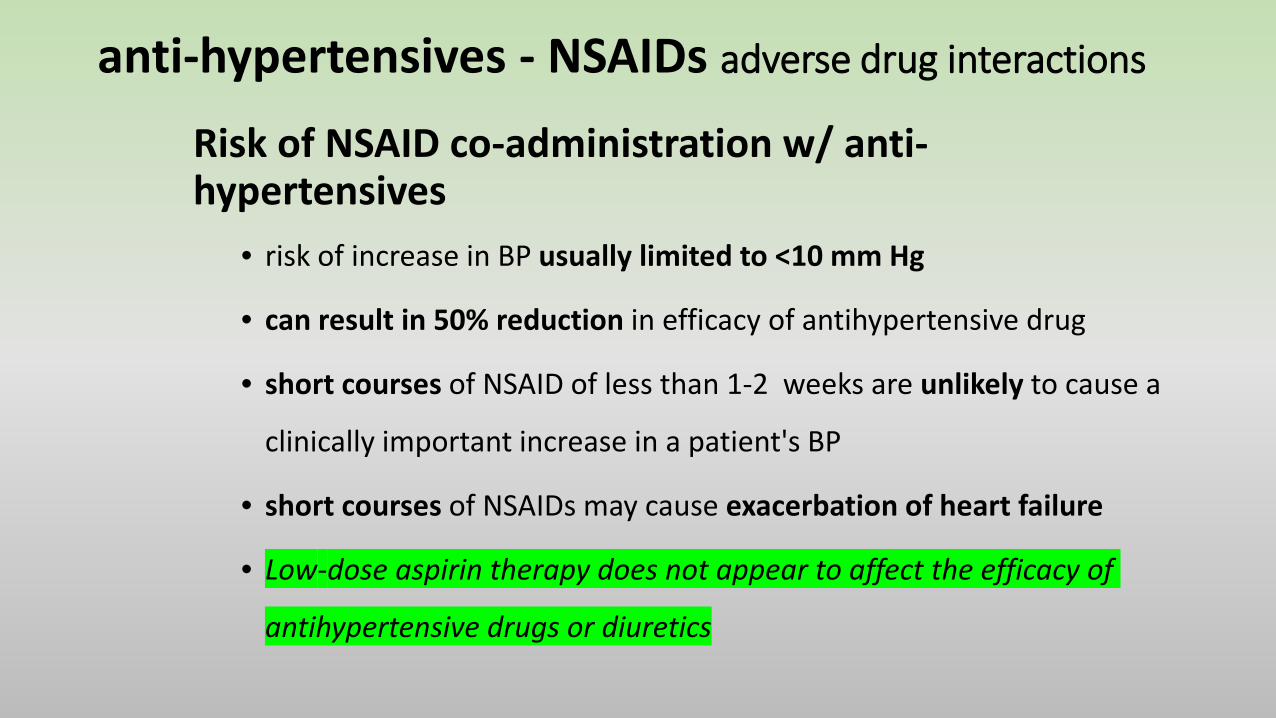
anti-hypertensives - NSAIDs adverse drug interactions
Risk of NSAID co-administration w/ anti-hypertensives
• risk of increase in BP usually limited to <10 mm Hg
• can result in 50% reduction in efficacy of antihypertensive drug
• short courses of NSAID of less than 1-2 weeks are unlikely to cause a
clinically important increase in a patient's BP
• short courses of NSAIDs may cause exacerbation of heart failure
• Low-dose aspirin therapy does not appear to affect the efficacy of
antihypertensive drugs or diuretics

anti-hypertensives - NSAIDs adverse drug interactions
• Diuretics • Na+ & water retention by NSAIDS• Suppression of plasma renin activity• risk of heart failure, edema
• Combination of ACE inhibitors, ARBs & diuretics“Double or triple whammy” thank you Karen Baker, MS (PNDC speaker 2017)
• 31% increase risk of acute kidney injury• kidney unable to use normal compensatory mechanisms• may suffer acute reduction in glomerular filtration• rising serum creatinine

other NSAIDs adverse drug interactions (not inclusive of all)
• Cyclosporin (immunosuppressant) Avoid if possible
• Lithium (increased lithium levels – use suldinac?)
• Cimetidine (Tagamet - +/- NSAID levels)
• Methotrexate (monitor for toxicities)
Use an online drug interaction checker !

NSAIDs
• Renal adverse effects
• NSAIDs
• Metabolized by liver
• Highly protein bound (avoid w/ warfarin)
• Old age no affect on elimination
• Renal impairment no effect on pharmacokinetics

Acetaminophen• Hepatic adverse effects of acetaminophen are well
known
• Acetaminophen• Careful about pt self-medicating• Essential a pt not exceed 4g acetaminophen in 24 hrs• June 2009 FDA recommended labeling 24 hours limit to less
than 4gm (= 3gm/24hr) – note this is self administered acetaminophen
• One metabolite is hepatotoxic & nephrotoxic• May accumulate in liver impairment• Caution in alcoholics & fasting eating disorders

Ibuprofen + acetaminophen
• Ibuprofen every 6 hours
• 400mg or 600mg for analgesia• 200mg to 800mg for anti-inflammatory
• Caution 800mg side effects for little anti-inflammatory• Side effects dose related – nausea, dyspepsia, gastric bleeding
• Acetaminophen every 6 hours
• 500mg or 650mg
• Tough spot = Ibuprofen 800mg + acetaminophen 1,000mg every 6 hours short duration, hepatic & renal risks

Review + more pearls
Rolf Christensen, DDS, MHA May 3, 2019

“Use opioids only when benefits are likely to outweigh risks”
“Start with the lowest effective dose of immediate-release opioids.
For acute pain, prescribe only the number of days that the pain is expected to be severe enough to require opioids.
Reassess benefits and risks if considering dose increases”
[CDC website: “Opioid Prescribing: where you live matters” last reviewed July 17, 2017; last checked January 28, 2019]

•nonopioid analgesics as 1st line of pain management
•
•multimodal pharmacologic & nonpharmacologic therapy
• If rx opioids = not be in a greater quantity than needed for the expected duration of pain severe enough to require opioids.

There is no substitute:
read the Washington
State Administrativ
e Code

If you rx opioids, you must register
Prescription Monitoring Program (PMP)
Diagnosis or reason on every opioid rxo Consider ICD-10 codes
Use the PMP helpline ! ! !
Remember & write down your initial registration information – address, etc.

Acute pain
Opioid prescription schedule & suggestions
0-6 weeks
Chronic painSubacute pain
6-12 weeks 12+ weeks
Prior to Rx opioids for non-operative pain
Prior to Rx opioids for subacute pain
When treating chronic pain patients with opioids
Alternative modalities
• Multi-modal pharmacologic & nonpharmacologic therapy for pain
• Rather than defaulting to opioids alone
• Where reasonable, evidence-based, clinically appropriate alternative exist

Co-prescribing & higher risk situations
1. Documentation in the pt record
2. Discussion of risks
3. Communication consultation with other prescribing practitioners

Co-prescribing – respiratory depressants = “high-risk”
–benzodiazepines
–barbiturates
–sedatives
–carisoprodol
–sleeping medications (also known as “Z drugs”)
Co-prescribing – “high-risk” co-morbidities
–COPD
–Respiratory disease
–Sleep apnea
–Significant psychiatric illness including major depression

Risks escalate with
–Polypharmacy
–Organic disease
–History of substance abuse disorder or abuse
–Aberrant behavior
Co-prescribing – “high-risk” medications
1. Documentation in the pt record
2. Discussion of risks
3. Consultation with other prescribing practitioners of other medications for patient care plan

Co-prescribing – “high-risk” co-morbidities = document
Co-prescribing opioid in combination with
–Organic disease, psychiatric illness, significant depression
–Any Central Nervous System depressant
–High dose opioid prescriptions >50 MME (milligram morphine equiv)
use MME opioid dose calculator as a guidenot for determining prescribing dosing
http://www.agencymeddirectors.wa.gov/opioiddosing.asp

Special requirement –if significant risk of overdose or oversedation =
Prescribe naloxone hcl or Narcan®
refer to Pharmacist for counseling, Rx access
https://www.ddap.pa.gov/Document%20Library/Naloxone%20for%20Opioid%20Safety-A%20Provider%27s%20Guide%20to%20Prescribing%20Naloxone%20to%20Patients%20Who%20Use%20Opioids.pdf
Naloxone for Opioid Safety; a
guide to prescribing naloxone it
patients who use opioids

High risk, high dose opioids, co-prescribing
Consider co-prescribing naloxone hcl (Narcan®)
OrRefer to pharmacist for
additional risk assessment & consultation

Naloxone co-prescribing
When co-prescribing opioid in combination with
–Caution with opioid prescriptions >50 MME (milligram morphine equiv)
–Consider co-prescribing naloxone (Narcan®) or
–Referral to pharmacy for naloxone counseling

Know your tools & use them
WA DOH handouts
Take the next steps …

Risks increase ++ above 50 MME
++++ above 90 MME

Patient & provider handouts
2019 WA State DOH Patient Handout Notification Acute Painhttps://www.doh.wa.gov/Portals/1/Documents/Pubs/631077-AcutePain.pdf
2019 WA State DOH Dental Prescriber Handouthttps://www.doh.wa.gov/Portals/1/Documents/630140-PrescriberHandout-Dental.pdf
Patient handout & provider resources
Opioid Dose Calculator (AMDG)http://www.agencymeddirectors.wa.gov/opioiddosing.asp
Disposing of unwanted medications (HCA)https://www.hca.wa.gov/disposing-safely-unwanted-medication
Thank you!
Rolf Christensen DDS rolfc@uw edu