high risk cases in emergency medicine: part 2 · accidentally hit in eye with a small plastic...
TRANSCRIPT

High‐risk Cases in Emergency Medicine: Part 2
Kevin M. Klauer, DO, EJD, FACEPChief Medical Officer, EMP, Ltd.Medical Editor‐in‐Chief, ACEP NowSpeaker, ACEP CouncilAsst. Clinical Professor, MSU College of Osteopathic Medicine
The information provided in AHC Media Webinars does not, and is not intended to constitute medical or legal advice. Opinions, references and links provided by our speakers are provided for your convenience and do not represent our endorsement of such opinions, products or services.
Wednesday, November 12th, 2014

2
SpeakerDr. Kevin Klauer is the Director of the Center for Emergency Medical Education and the Chief Medical Officer for Emergency Medicine Physicians, Ltd., based in Canton, Ohio. He also is the Director of EMP’s Patient Safety Organization. He serves on the Board of Directors for Physicians Specialty Limited Risk Retention Group. He is an Assistant Clinical Professor at Michigan State University College of Osteopathic Medicine. He has received the EMRA Robert Dougherty ACEP/EMF Teaching Fellowship and also the ACEP's National Emergency Medicine Faculty Teaching Award. He was most recently recognized by the Ohio Chapter ACEP with the Bill Hall Award for service. Dr. Klauer is the co‐author of two risk management books: Emergency Medicine Bouncebacks: Medical and Legal and Risk Management and the Emergency Department: Executive Leadership for Protecting Patients and Hospitals.
22

3
1. Discuss strategies to identify high-risk features of clinical entities in emergency medicine.
2. Develop strategies to improve patient safety.
3. Review ways to reduce professional liability in the practice of emergency medicine.
Learning Objectives

High Risk Entities
Hyponatremia is expensiveSepsis is a chronic diseaseMethotrexateDon’t Forgot the Rhogam “Eye” Would Hate to Miss This One! “SEA” of Neuro Disasters

Hyponatremia


Clinical approach to hyponatremia shown as a flow diagram after initial presentation.
Tzamaloukas A et al. ahaoa 2013;2:-
©2013 by Lippincott Williams & Wilkins

Computed tomographic imaging brain slice from index patient showing myelinolysis in pons (white arrow).
Tzamaloukas A et al. ahaoa 2013;2:-
©2013 by Lippincott Williams & Wilkins

Medical Legal Case
• 42 y/o female• Found unresponsive by family (no trauma)
“Snoring loudly”• July 10, 2009: 23:00• Intermittent N & V for 1 week• PMHx: hypertension, pancreatitis, and anxiety • Meds: Lorazepam, Promethazine, and Benicar • Seizures: 1 upon EMS arrival and 2 in ED•

Medical Legal Case
• 124 P, 122/70 BP, 13 R, and 96 % O2 Sat • Exam: 23:55• GCS = 10• 0012: 60 second tonic/clonic seizure• Tx: Ativan 1mg IVP• Diagnostics: CT Neg

Medical Legal Case
• Treatment0100: 1st Liter of NS completed0145: BP 84/54: 2nd Liter bolus orderedCentral line initiated
• Consultation: Intensivist 0210Admit to ICU3% Hypertonic Saline at 80ml/hrK+ 60 meq over 6 hours

Medical Legal Case• Q 4 hr BMP order changed be intensivist to wait
for K+ to be completed• Next BMP 0945• Na+: 125• 24 hours later: Unresponsive• 8 days later: MRI: CPM• 10 days later: Trach and moved to long term care
facility
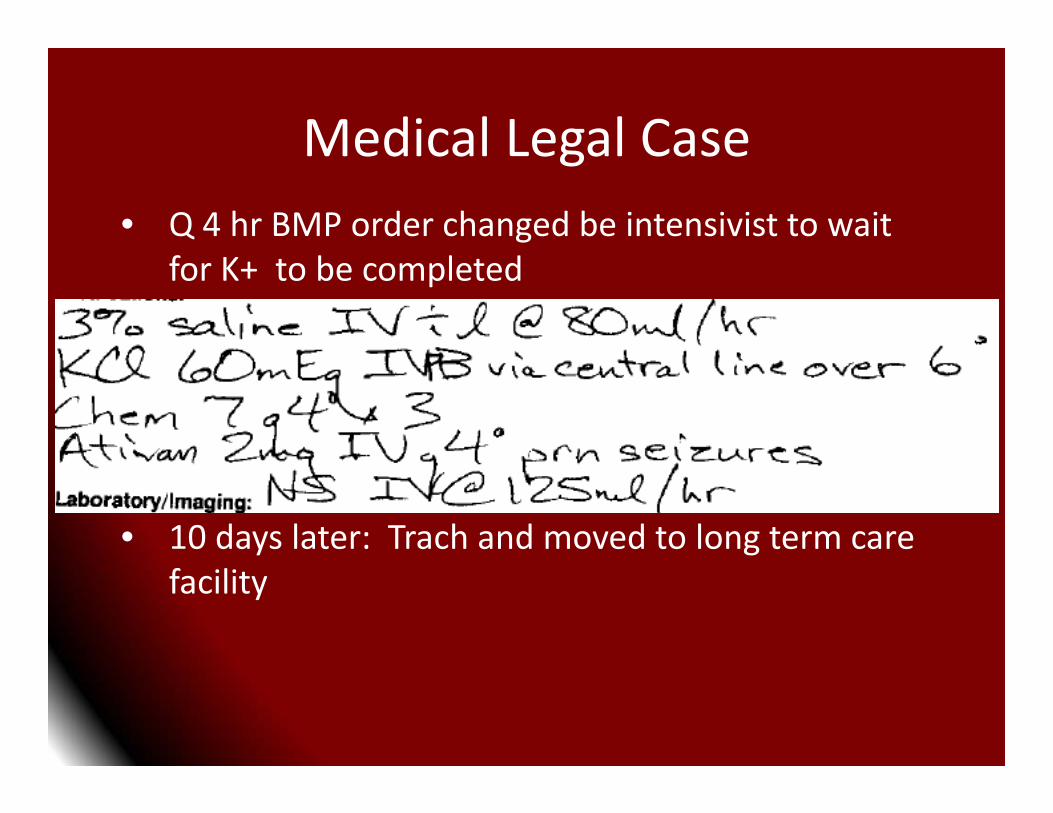
Medical Legal Case• Q 4 hr BMP order changed be intensivist to wait
for K+ to be completed• Next BMP 0945• Na+: 125• 24 hours later: Unresponsive• 8 days later: MRI: CPM• 10 days later: Trach and moved to long term care
facility

Medical Legal Case
Died August 22, 2009Lawsuit filed: September 23, 2012Mediation: Settlement1. Undisclosed for the Intensivist2. $60,000 for the EP

Take Home
• Slow Correction• Hypertonic Saline in Consultation• Frequent rechecks• 10‐15 mEq/L/24 hours and less than 18 mEq/L/48 hours
• CPM may occur on either side of the equation

Sepsis

Sepsis
Winters BD, et al. Long‐term mortality and quality of life in sepsis: a systematic review. Crit Care Med. 2010 May;38(5):1276‐83.• Ongoing Mortality up to 2 Yrs


975 with SepsisMortality Rates
Hospital: 8.9%1 yr: 23% v. 1%2 yr: 28.8% v. 2.6%5 yr: 43.8% v. 8.3%
750,000 Hospitalizations570,000 ED visits200,000 Deaths$16.7 Billion

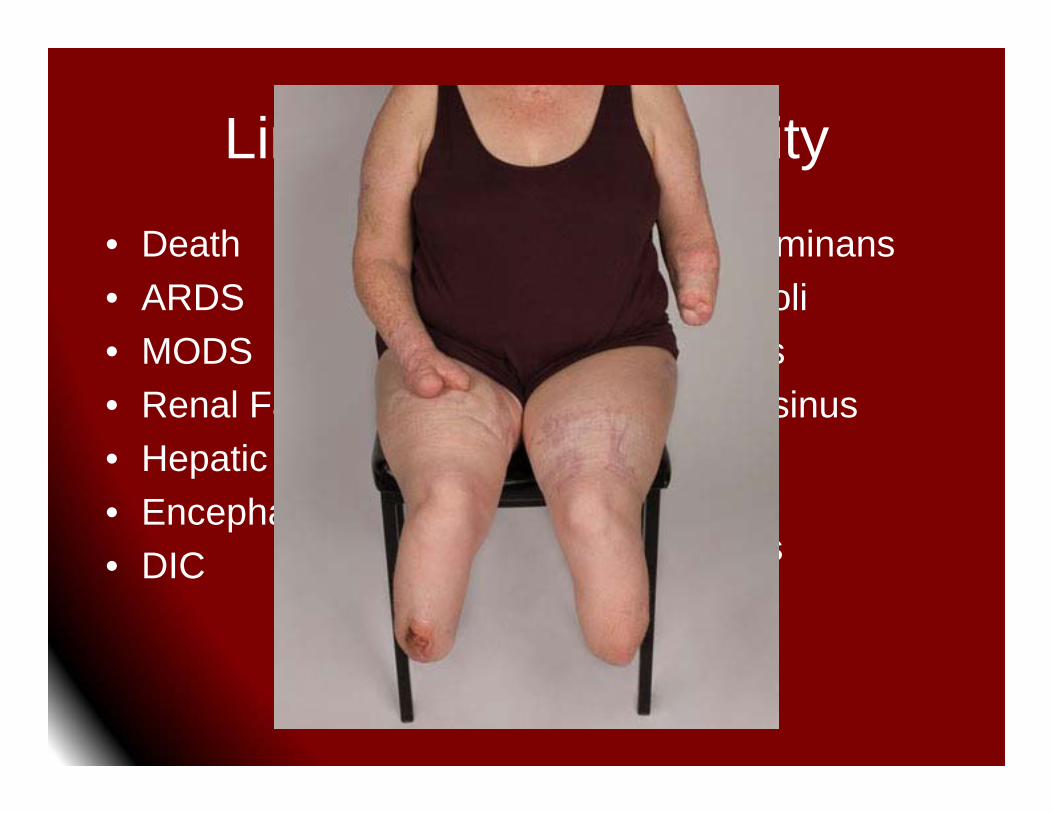
Limitations and Liability
• Death• ARDS• MODS• Renal Failure• Hepatic failure• Encephalopathy• DIC
• Purpura Fulminans• Septic Emboli• Endocarditis• Cavernous sinus
thrombosis• Limb/Digital
amputations
Limitations and Liability
• Death• ARDS• MODS• Renal Failure• Hepatic failure• Encephalopathy• DIC
• Purpura Fulminans• Septic Emboli• Endocarditis• Cavernous sinus
thrombosis• Limb/Digital
amputations


Outrage!

Outrage!

Daniels R. Surviving the first hours in sepsis: getting the basics right
(an intensivist’s perspective); J Antimicrob Chemother 2011; 66 Suppl 2: ii11–ii23 (US
National Library of Medicine)

Sankoff JD. Validation of the Mortality in Emergency Department Sepsis (MEDS) score in patients with the systemic inflammatory response syndrome
(SIRS). Crit Care Med. 2008 Feb;36(2):421-6.
• MEDS Score predicts 28 day mortality in admitted Pts with SIRS
• Terminal illness, Tachypnea or Hypoxemia, Septic shock, PLT < 150K, Bands > 5%, Age > 65 yrs, pneumonia, Nursing home, AMS
• very low (0.6%), low (5%), moderate (19%), high (32%), and very high (40%)


Carpenter C. J Emerg Med. 2009 Oct;37(3):319-27. Epub 2009 May 8.Valid: Less accurate in severe sepsis

Surviving Sepsis Campaign: InternationalGuidelines for Management of Severe Sepsis
and Septic Shock: 2012“A strong recommendation does not automatically implystandard of care. For example, the strong recommendationfor administering antibiotics within 1 hr of the diagnosisof severe sepsis, as well as the recommendation for achieving a central venous pressure (CVP) of 8 mm Hg and a central venous oxygen saturation (Scvo2) of 70% in the first 6 hrs of resuscitation of sepsis‐induced tissue hypoperfusion, although deemed desirable, are not yet standards of care as verified by practice data.”

• 31 U.S. EDs• 2 or more SIRS + Refractory HYN or Lactate >4
• 3 Groups for 6 hours of resuscitationEGDT, Sepsis Protocol, Usual
• 1,341 Pts (well matched at baseline)
Systemic Inflammatory Response Syndrome
At least 2 of the following:A temperature over 38.3C or less than 36.0CA heart rate over 90A respiratory rate over 20A WBC count less than 4,000 or over 12,000Acutely alerted mental statusHyperglycemia in non‐diabetic patients

• 31 U.S. EDs• 2 or more SIRS + Refractory HYN or Lactate >4
• 3 Groups for 6 hours of resuscitationEGDT, Sepsis Protocol, Usual
• 1,341 Pts (well matched at baseline)



Mortality20.1%18.2%18.9%No diff:90 Day/1 Yr Organ Support

Medical Legal Case
• 3 y/o female presented at 13:00• CC: Cough, earache, bruising and fever
Ill for 2 daysRash started today
• Initial Eval (PA) in FT: 16:10• Transferred to ED & EP: 18:02

Medical Legal Case
• Exam• Physician findings
“Slight Jaundice”“Purpura cheeks, earlobes, buttocks, thorax and lower extremities”“Crying but easily consolable”

Medical Legal Case
• Exam• Physician findings
“Slight Jaundice”“Purpura cheeks, earlobes, buttocks, thorax and lower extremities”“Crying but easily consolable”

Medical Legal Case
• DiagnosticsWBC: 3.1; PLT 50K; INR: 4.8; LFTs IVFAcetaminophenCeftriaxone 1 gm: 18:52
• DDX: ITP, HSP, EB ….
• Disposition: Transfer to Tertiary Referral Center: 2102 report; 2238 OTD

Medical Legal Case
• Outcome• Streptococcus A sepsis• 4 limb amputation• Multimillion $ settlement

Sepsis Solutions
1. Early Identification2. Early Patient Education (natural course)3. Document the consideration and discussion4. Discussion about outcomes5. Consent for vasopressors

Methotrexate

Kurt T. Barnhart. Ectopic Pregnancy. N Engl J Med 2009; 361:379‐387July 23, 2009
• Heterotopic pregnancy1 in 4,0001 in 100 with in vitro fertilization

Surgical Management of Ectopic PregnancyA Jazayeri. eMedicine, Jan 7, 2008
• 1. No evidence of rupture or hemoperitoneum• 2. Hemodynamically stable• 3. < 8 weeks gestation• 4. B-HCG <5,000 (3000 –15,000 reported in
various sources)• 5. Adnexal mass < 4 cm (2 cm –5 cm reported in
various sources)• 6. No fetal cardiac activity• 7. Confirmed ectopic, not requiring surgical
confirmation
Methotrexate

Case History
• 30 y.o. female • 7 weeks with vag bleeding and cramping.• BHCG: 9,500 • US: Small amt of non specific endometrial
fluid. • OB consulted, saw patient, and gave
methotrexate.

Follow Up
• Two days later patient seen at another facility
• US showed ~ 6 week IUP with fetal pole.• Next US, three days later showed fetal HR
around 70/min. • 1 week: HCG declining, Fetal demise and
D&C performed.• Lawsuit Filed: Numerous defendants

Rh Isoimmunization
• Walker v. Rinck, 604 N.E.2d 591 (Ind. 1992).“physician owes a duty to future children of an Rh‐negative woman who gives birth to an Rh‐positive child.”

RhoGAM• RhoGAM = IgG anti-D antibodies• Destroy Rh+ fetal red cells in the maternal
circulation• If RhoGAM not given, mother develops
antibodies to Rh+ fetal blood which cross the placenta and cause a hemolytic anemia in the fetus, splenomegaly, erythroblastosis, death
• Indications: Rh- and abortion (any type), abruption, ectopic, antepartum hemorrhage, trauma (even relatively minor)
• Dose: 50 mcg if <12 weeks, 300 mcg if >12 weeks

Anti-D administration after spontaneous miscarriage for preventing Rhesus alloimmunisation.
Cochrane Database Syst Rev. 2013 Mar 28;3:CD009617
• Rh-neg: Following spont AB• 1 RCT: 48 women• 8-24 weeks• 19/29• Small sample size• No difference
Maternal sensitizationRh alloimmunization in subsequent pregnancies

Medical Legal Case
• CC: “Vaginal bleeding”• HPI: 8 weeks pregnant; 2 days; No clots• PE: BP 112/70, pulse 72
25 y/oNo CVAT or LBPPelvic: Os Closed, Mod amount of BRB, No CMT
• No Tissue
Medical Legal Case
• DiagnosticsHgb: 13.7Quant: 28,543Pelvic US: 8 wk viable twin!
• ConsultPhone with the Ob/Gyn
• Clinical Impression: “Threatened miscarriage”• Disposition: Discharge

Outcome
• Twin GirlsTwin 1 diedTwin 2: Hydrops fetalis, Anemia, Kernicterus, Hearing impaired and learning disabilities(?)
• Claims: Rh IsoimmunizationWrongful deathInjury of twin 2Mother’s concerns about future pregnanciesFather’s loss of consortium
Outcome
• Demand $800,000• Settlement for $425,000
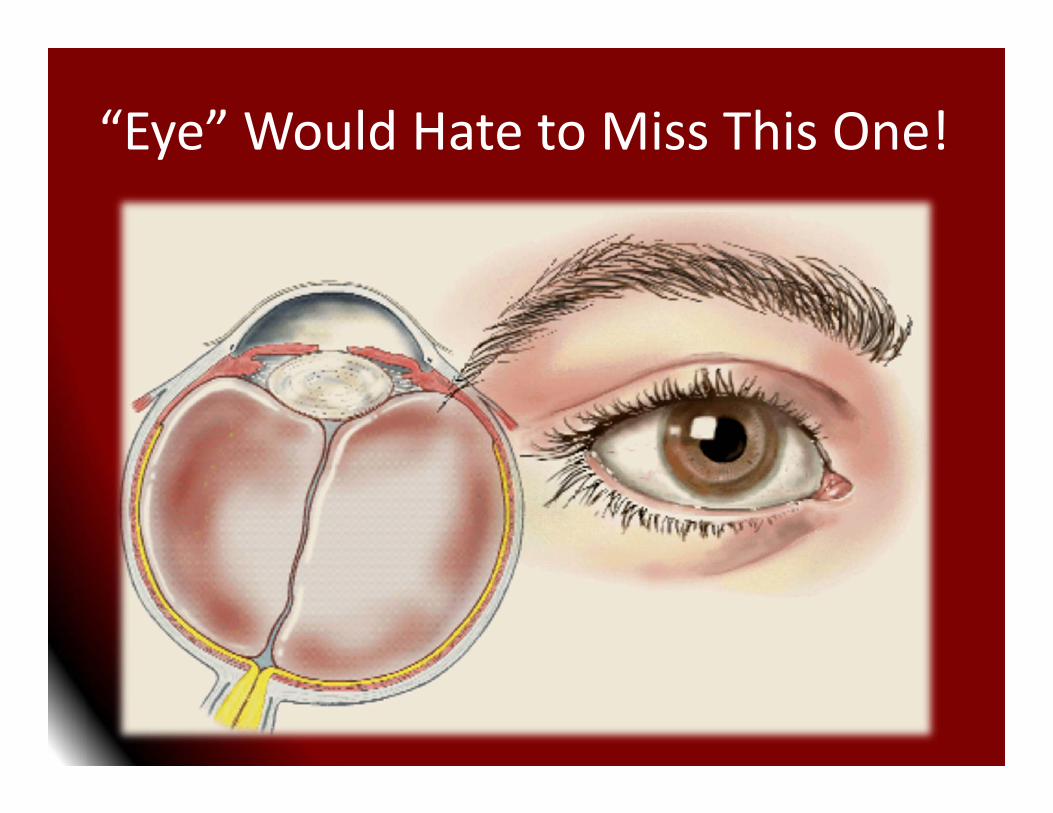
“Eye” Would Hate to Miss This One!

Medical Legal Case• CC: “Hit in the left eye with a piece of plastic”• HPI: 21 y/o male patient
Accidentally hit in eye with a small plastic object2 hours prior to arrivalBlurred vision after rubbing his eye since the injury
• PE: Vital signs NLInjected and swollen“Pupils, equal, round and reactive to light”Fundoscopic exam NLVA: NL in right eye; unable to decipher anything on the chart due to rubbing the eye

Medical Legal Case
• DiagnosticsSlit Lamp Exam
• 2mm corneal abrasion near the left pupil• Clinical Impression: Corneal Abrasion• Disposition: Discharge with 3 day follow up• Gentamicin drops

Outcome
• RN triage note“Working on his car when foreign material (metal or plastic) shot into his eye.”
• Follow up 3 days later• Dx: Globe perforation and Retinal detachment
• Permanent visual loss

Outcome
• A case for excess limits?• Settlement: $800,000

Corneal Lacerations• Anterior chamber perforation
• Teardrop shaped pupil
• Flat anterior chamber
• Black iris pigment may be at the wound edge• Seidel test: fluorescein on eye is washed away by
leaking aqueous humor = corneal perforation • Tonometry contraindicated / No patch (but put eye
shield on / Avoid eye movements) may extrude vitreous with eye muscle contractions
• Urgent referral / consultation

Corneal Lacerations

Corneal Laceration

Corneal Laceration
Med‐Challenger • EM

Globe Rupture• Most have associated hyphemas
• “Tear drop” pupil points to rupture site
• Flat anterior chamber (due to lowered
pressure)
• No pressure on eye - use shield
• No contact tonometry
• IV antibiotics / analgesia / tetanus / CT-MRI

Globe RupturePathology

“SEA” of Neuro Disasters

Medical Legal Case
• CC: Back pain, numbness and abdominal pain• 26 y/o Male • Rt lower back pain for 1wk• Seen at different ED twice in past 24 hours
Dx: “Sciatica”
• Numbness from knees down4 hours prior to arrival• PMHx: IDDM, Schizophrenia, ADD

Medical Legal Case
• Physical Examination• VS: T 101.6, HR 105, RR 20, BP 136/80• Abdomen: Soft and Non tender• T8‐L1 paraspinal tenderness near ML• Distal sensation NL• “Can’t move legs secondary to severe pain”

Medical Legal Case• Diagnostics• WBC: 13.9 with 11% bands• UA Neg• Abd CT: Paravertebral ST swelling T7‐L2 (no discitis)• Chest XR: NAD• Antibiotics: Vanco & Nafcillin• Consult: NSGY: Stop antibiotics due to Cxs

Medical Legal Case• Patient to be transferred• Dx: Acute discitis• “The patient is schizophrenic, not convinced that the patient can’t move his legs.”
• Transferred at 0010 (original arrival 1645)• T‐L MRI ordered: Canceled by radiology
Needs Plain Skull, Abd and Chest XR• Performed at 0445• 1247: Negative (but Thoracic portion not performed)• Reordered: 1300• Results: Posterior Epidural Collection T4‐T12• Taken to OR

Medical Legal Case
• OutcomeParaplegicDischarged to skilled nursing/rehabilitation
• Hospital Settlement (undisclosed)• Initial EP

Medical Legal Case
• OutcomeParaplegicDischarged to skilled nursing/rehabilitation
• Hospital Settlement (undisclosed)• Initial EP
$900,000

Davis DP. Prospective evaluation of a clinical decision guideline to diagnose spinal epidural abscess in patients who present to the emergency department with spine pain.J Neurosurg Spine. 2011 Jun;14(6):765‐70. Epub 2011 Mar 18.
• Risk factor assessment• ESR v. CRP
ESR outperformed CRP: 100%/67%
• Imaging• Control period v. Study period
Delays 83.6% v. 9.7%Deficits 81.8% v. 19.4%

Davis DP. Prospective evaluation of a clinical decision guideline to diagnose spinal epidural abscess in patients who present to the emergency department with spine pain.J Neurosurg Spine. 2011 Jun;14(6):765‐70. Epub 2011 Mar 18.
• Risk factor assessment• ESR v. CRP
ESR outperformed CRP: 100%/67%
• Imaging• Control period v. Study period
Delays 83.6% v. 9.7%Deficits 81.8% v. 19.4%
Recommendations1. Sodium correction: 10‐15 mEq/L/24 hours and less
than 18 mEq/L/48 hours.2. Alert patients about the dangers of vasopressors and
obtain informed consent.3. Methotrexate can be dangerous. Follow the
inclusion/exclusion criteria and consult Ob/Gyn.4. 24 hour follow for all eye injuries.5. Don’t forget the RhoGam!6. Consider SEA in all patients with new back pain and
new neuro deficits or risk factors with a positive ESR.

74
This presentation is intended solely to provide general information and does not constitute legal advice. Attendance at the presentation or later review of these printed materials does not create an attorney‐client relationship with the presenter(s). You should not take any
action based upon any information in this presentation without first consulting legal counsel familiar with your particular circumstances.

Thank you for attending!Questions?