high resolution spect before after - journal of neurology...
TRANSCRIPT

J7ournal ofNeurology, Neurosurgery, and Psychiatry 1993;56:655-664
High resolution SPECT with [99mTc]-d,l-HMPAOin normal pressure hydrocephalus before and aftershunt operation
Gunhild Waldemar, Jes F Schmidt, Florence Delecluse, Allan R Andersen,Flemming Gjerris, Olaf B Paulson
AbstractCranial CT and high resolution mea-surements of regional cerebral bloodflow (rCBF) with brain dedicated singlephoton emission computer tomography(SPECT) and ["'-Tc]-d,l-hexamethyl-propyleneamine oxime ([99'Tc]-d,l-HMPAO) were performed before andafter shunt operation in 14 consecutivepatients with dementia and normal pres-sure hydrocephalus (NPH). When com-pared with a control group of 14 agematched healthy volunteers, the group ofNPH patients was characterised by anenlarged subcortical low-flow region,significantly reduced rCBF andenhanced side-to-side asymmetry ofrCBF in the central white matter, andenhanced side-to-side asymmetry in theinferior and mid-temporal cortex. GlobalCBF was normal. Shunt operationreduced the mean area of the ventricleson CT and of the subcortical low-flowregion on SPECT. Global CBF wasunchanged. All 14 patients had an abnor-mal pre-shunt rCBF pattern withenlargement of the subcortical low flowregion, focal cortical blood flow deficits,or both. Shunt operation improved theclinical status in 11 patients, and the areaof the subcortical low flow region cor-rectly classified 3/3 unimproved and 10/11improved patients. Shunt operation nor-malised or reduced the area of the sub-cortical low flow region in nine of 10patients. It is concluded that SPECTwith ["-"Tc]-d,l-HMPAO is a useful sup-plement in the diagnosis of NPH versusnormal ageing, and that SPECT mayhelp to identify patients not likely to ben-efit clinically from surgery.
(7 Neurol Neurosurg Psychiatry 1993;56:655-664)
Normal pressure hydrocephalus (NPH) is arare, but potentially treatable cause ofdementia. It was described in 1965 by Hakimand Adams' and Adams et al'2as a syndromeinvolving: 1) progressive dementia charac-terised by memory impairment and psy-chomotor retardation; 2) disturbance ofbalance and gait with rigidity or spasticity oflower limbs, and 3) impaired control ofsphincters, in patients with enlarged ventri-cles and normal CSF pressure. Permanentdrainage of the CSF was proposed as a treat-ment.' 2 Intensive research has aimed at
improving the clinical, radiographic, andhydrodynamic criteria used as indications forshunt operation. On the assumption that thepathogenesis of NPH involves impairedabsorption capacity of the CSF system andthus a reduced conductance to outflow ofCSF (CO.,), B0rgesen et aP described amethod for its determination. They con-cluded that only patients with Cout < 0-08ml-mm Hg-' min-' (or resistance to outflow,R.Ut > 12 mm Hg.min.ml-') might benefitfrom shunt operation.4
As reviewed by Turner and McGeachie,5the percentage of selected patients whoimproved after CSF shunting has beenreported to be in the range 25-80%. Thisresponse rate must be reviewed in the contextof a 30-40% postoperative complication rate,including anaesthetic complications, infec-tions, intracranial haematomas, and shuntmalfunctions.5 The clinical differentiation ofmild NPH from normal ageing, benign senileforgetfulness, Alzheimer's disease, or otherdegenerative dementia disorders, which maybe associated with enlarged ventricles andperhaps similar symptoms, is difficult. Betterdiagnostic studies might improve the predic-tive power of clinical improvement.The aim of this study was to investigate the
value of high resolution single photon emis-sion computer tomography (SPECT) ofregional cerebral blood flow (rCBF) using[99mTc] -d,l-hexamethyl-propyleneamineoxime ([9'9Tc]-d,l-HMPAO) in the diagnosisof NPH versus normal ageing and in the pre-diction of the clinical outcome after shuntoperation in NPH. Furthermore, the effect ofshunt operation on cortical and subcorticalrCBF was analysed.
Patients and methodsPatientsFourteen patients (four women, 10 men)with NPH were included in the study. Theirmedian age was 64 years (range: 24-84).Their clinical and hydrodynamic data are pre-sented in table 1. The patients were consecu-tively admitted to the Department ofNeurosurgery and selected for shunt opera-tion. In two patients the NPH condition haddeveloped secondary to a subarachnoidhaemorrhage (SAH), in two other patientspossibly to a previous head trauma, and inone patient to an arterial aneurysm. In theremaining nine patients the aetiology wasunknown. The median duration of symptomswas 18 months (range: 1-36). All patients
Rigshospitalet,Copenhagen,DenmarkDepartment ofNeurologyG WaldemarA R AndersenO B PaulsonDepartment ofNeurosurgeryJ F SchmidtF GjerrisHospital Erasme,Brussels, BelgiumDepartment ofNeurologyF DelecluseCorrespondence to:Dr Waldemar, Departnentof Neurology,Rigshospitalet, 9,Blegdamsvej, DK-2 100Copenhagen, Denmark.Received 11 November1991 and in final revisedform 16 June 1992.Accepted 7 July 1992
655 on 6 July 2018 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.56.6.655 on 1 June 1993. D
ownloaded from
Waldemar, Schmidt, Delecluse, Andersen, Gjerris, Paulson
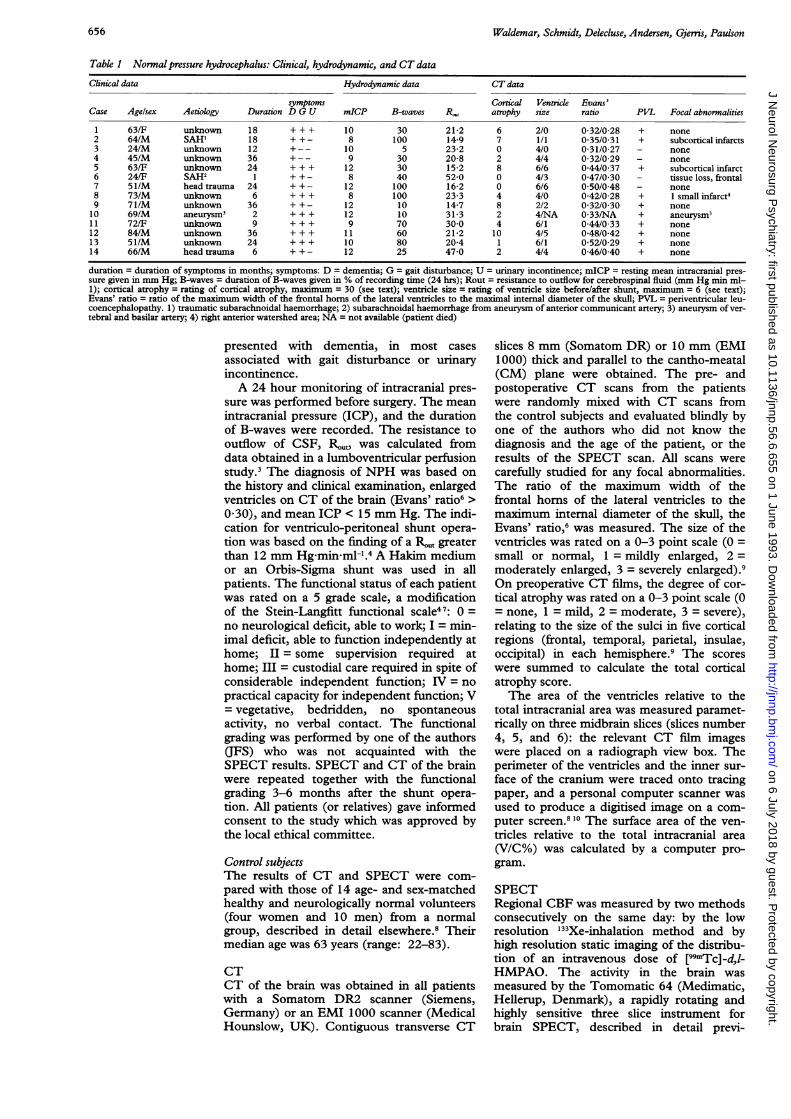
Table 1 Normal pressure hydrocephalus: Clinical, hydrodynamic, and CT data
Clinical data Hydrodynamic data CT data
symptoms Cortical Ventricle Evans'Case Age/sex Aetiology Duration D G U mICP B-waves R,, atrophy size ratio PVL Focal abnormalities
1 63/F unknown 18 + + + 10 30 21-2 6 2/0 0 32/0 28 + none2 64/M SAH' 18 + +- 8 100 14-9 7 1/1 0-35/0-31 + subcortical infarcts3 24/M unknown 12 +-- 10 5 23-2 0 4/0 0-31/0-27 - none4 45/M unknown 36 +-- 9 30 20-8 2 4/4 0-32/0 29 - none5 63/F unknown 24 + + + 12 30 15-2 8 6/6 0 44/0 37 + subcortical infarct6 24/F SAH2 1 + + - 8 40 52-0 0 4/3 0-47/0 30 - tissue loss, frontal7 51/M head trauma 24 + +- 12 100 16-2 0 6/6 0-50/0-48 - none8 73/M unknown 6 + + + 8 100 23-3 4 4/0 0 42/0-28 + 1 small infarct49 71/M unknown 36 + +- 12 10 14-7 8 2/2 0 32/0 30 + none10 69/M aneurysm3 2 + + + 12 10 31-3 2 4/NA 0-33/NA + aneurysm311 72/F unknown 9 + + + 9 70 30 0 4 6/1 0 44/0 33 + none12 84/M unknown 36 + + + 11 60 21-2 10 4/5 0 48/0-42 + none13 51/M unknown 24 + + + 10 80 20-4 1 6/1 0 52/0-29 + none14 66/M head trauma 6 + +- 12 25 47 0 2 4/4 0 46/0 40 + none
duration = duration of symptoms in months; symptoms: D = dementia; G = gait disturbance; U = urinary incontinence; mICP = resting mean intracranial pres-sure given in mm Hg; B-waves = duration of B-waves given in % of recording time (24 hrs); Rout = resistance to outflow for cerebrospinal fluid (mm Hg min ml-1); cortical atrophy = rating of cortical atrophy, maximum = 30 (see text); ventricle size = rating of ventricle size before/after shunt, maximum = 6 (see text);Evans' ratio = ratio of the maximum width of the frontal horns of the lateral ventricles to the maximal internal diameter of the skull; PVL = periventricular leu-coencephalopathy. 1) traumatic subarachnoidal haemorrhage; 2) subarachnoidal haemorrhage from aneurysm of anterior communicant artery; 3) aneurysm of ver-tebral and basilar artery; 4) right anterior watershed area; NA = not available (patient died)
presented with dementia, in most casesassociated with gait disturbance or urinaryincontinence.A 24 hour monitoring of intracranial pres-
sure was performed before surgery. The meanintracranial pressure (ICP), and the durationof B-waves were recorded. The resistance tooutflow of CSF, R,,,,,,t was calculated fromdata obtained in a lumboventricular perfusionstudy.3 The diagnosis of NPH was based onthe history and clinical examination, enlargedventricles on CT of the brain (Evans' ratio6 >0 30), and mean ICP < 15 mm Hg. The indi-cation for ventriculo-peritoneal shunt opera-tion was based on the finding of a R,,,t greaterthan 12 mm Hg minml-[.4 A Hakim mediumor an Orbis-Sigma shunt was used in allpatients. The functional status of each patientwas rated on a 5 grade scale, a modificationof the Stein-Langfitt functional scale47: 0 =no neurological deficit, able to work; I = min-imal deficit, able to function independently athome; II = some supervision required athome; III = custodial care required in spite ofconsiderable independent function; IV = nopractical capacity for independent function; V= vegetative, bedridden, no spontaneousactivity, no verbal contact. The functionalgrading was performed by one of the authors(JFS) who was not acquainted with theSPECT results. SPECT and CT of the brainwere repeated together with the functionalgrading 3-6 months after the shunt opera-tion. All patients (or relatives) gave informedconsent to the study which was approved bythe local ethical committee.
Control subjectsThe results of CT and SPECT were com-pared with those of 14 age- and sex-matchedhealthy and neurologically normal volunteers(four women and 10 men) from a normalgroup, described in detail elsewhere.8 Theirmedian age was 63 years (range: 22-83).
CTCT of the brain was obtained in all patientswith a Somatom DR2 scanner (Siemens,Germany) or an EMI 1000 scanner (MedicalHounslow, UK). Contiguous transverse CT
slices 8 mm (Somatom DR) or 10 mm (EMI1000) thick and parallel to the cantho-meatal(CM) plane were obtained. The pre- andpostoperative CT scans from the patientswere randomly mixed with CT scans fromthe control subjects and evaluated blindly byone of the authors who did not know thediagnosis and the age of the patient, or theresults of the SPECT scan. All scans werecarefully studied for any focal abnormalities.The ratio of the maximum width of thefrontal horns of the lateral ventricles to themaximum internal diameter of the skull, theEvans' ratio,6 was measured. The size of theventricles was rated on a 0-3 point scale (0 =small or normal, 1 = mildly enlarged, 2 =moderately enlarged, 3 = severely enlarged).9On preoperative CT films, the degree of cor-tical atrophy was rated on a 0-3 point scale (0= none, 1 = mild, 2 = moderate, 3 = severe),relating to the size of the sulci in five corticalregions (frontal, temporal, parietal, insulae,occipital) in each hemisphere.9 The scoreswere summed to calculate the total corticalatrophy score.The area of the ventricles relative to the
total intracranial area was measured paramet-rically on three midbrain slices (slices number4, 5, and 6): the relevant CT film imageswere placed on a radiograph view box. Theperimeter of the ventricles and the inner sur-face of the cranium were traced onto tracingpaper, and a personal computer scanner wasused to produce a digitised image on a com-puter screen.810 The surface area of the ven-tricles relative to the total intracranial area(V/C%) was calculated by a computer pro-gram.
SPECTRegional CBF was measured by two methodsconsecutively on the same day: by the lowresolution "33Xe-inhalation method and byhigh resolution static imaging of the distribu-tion of an intravenous dose of [99I"Tc]-d,l-HMPAO. The activity in the brain wasmeasured by the Tomomatic 64 (Medimatic,Hellerup, Denmark), a rapidly rotating andhighly sensitive three slice instrument forbrain SPECT, described in detail previ-
656 on 6 July 2018 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.56.6.655 on 1 June 1993. D
ownloaded from
SPECT with xw9 Tc]-d, l-HMPAO in NPH
ously." All scans were obtained in parallel tothe CM plane, and the patients were studiedin the supine position during rest with eyesclosed and with ears unplugged in quiet sur-roundings.The '33Xe-inhalation study lasted 4-5 min-
utes and was performed to obtain quantitativerCBF data. With this technique the in-planeresolution is 17-20 mm (full width at halfmaximum, FWHM) and the slice thickness20 mm. The calculation of CBF from asequence of 4 time activity pictures was basedon a combination of the isotope clearanceprinciple and the bolus distributionprinciple.'2 At the end of the study theend-expiratory CO2-fraction (FECO2) wasmeasured using a capnograph (CDA-1 CO2-analyser, Novo Diagnostic Systems, DK).Two patients were unable to cooperate in theinhalation procedure.
Before the [99mTc]-d,l-HMPAO study,99mTc pertechnetate was eluated from a Mo-Tc generator and mixed with d,l-HMPAO(Exametazime, CeretecR, Amersham, UK). Abolus containing 1-1 GBq [99mTc]-d,l-HMPAO was injected intravenously. Theacquisition time was approximately 25 min-utes yielding at least 3-106 counts per slice. Inas many patients as possible, data acquisitionwas performed in three different positions toobtain nine contiguous image slices coveringthe whole brain. In three cases, however, itwas not possible to obtain more than onedata set with three slices due to poor patientcooperation. Following reconstruction, thedata were normalised to the cerebellum andcorrected to adjust for incomplete retention
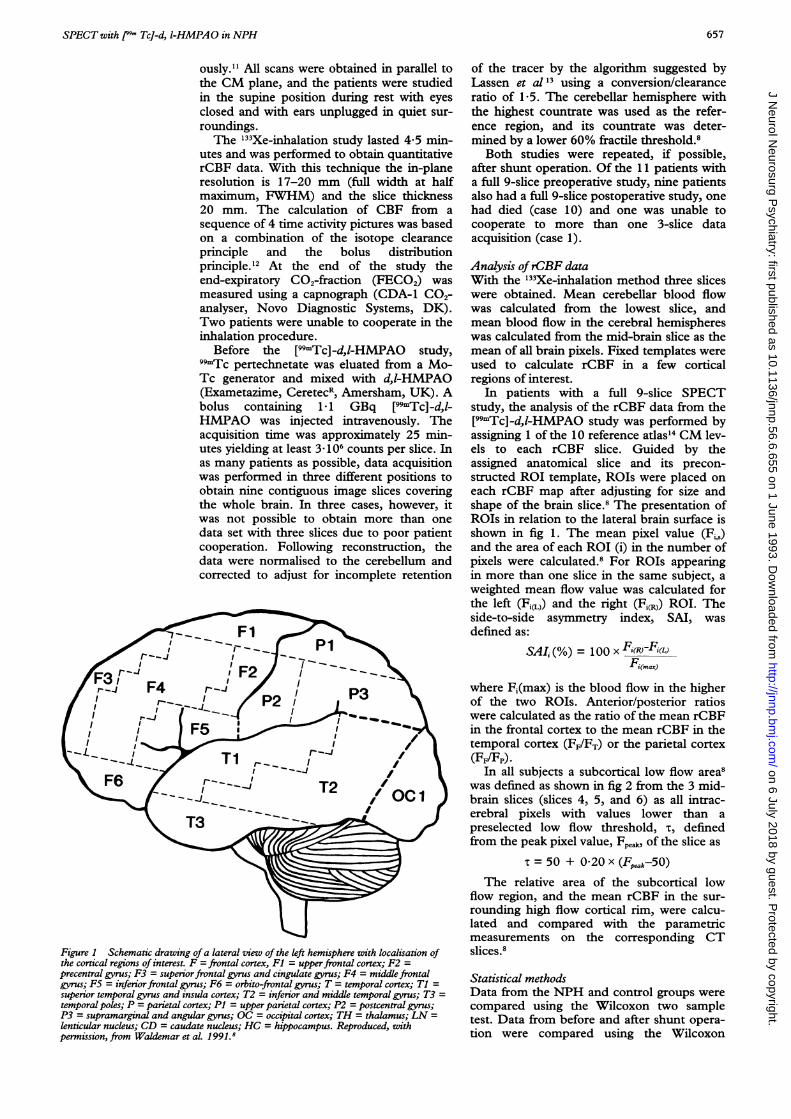
Figure I Schematic drawing of a lateral view of the left hemisphere with localisation ofthe cortical regions of interest. F = frontal cortex, Fl = upperfrontal cortex; F2 =
precentral gyrus; F3 = superiorfrontal gyrus and cingulate gyrus; F4 = middle frontalgyrus; F5 = inferior frontal gyrus; F6 = orbito-frontal gyrus; T = temporal cortex; Tl =
superior temporal gyrus and insula cortex; T2 = inferior and middle temporal gyrus; T3 =
temporal poles; P = parietal cortex; Pl = upper parietal cortex; P2 = postcentral gyrus;P3 = supramarginal and angular gyrus; OC = occipital cortex; TH = thalamus; LN =
lenticular nucleus; CD = caudate nucleus; HC = hippocampus. Reproduced, withpermission, from Waldemar et al. 1991.8
of the tracer by the algorithm suggested byLassen et al '3 using a conversion/clearanceratio of 1-5. The cerebellar hemisphere withthe highest countrate was used as the refer-ence region, and its countrate was deter-mined by a lower 60% fractile threshold.8
Both studies were repeated, if possible,after shunt operation. Of the 11 patients witha full 9-slice preoperative study, nine patientsalso had a full 9-slice postoperative study, onehad died (case 10) and one was unable tocooperate to more than one 3-slice dataacquisition (case 1).
Analysis ofrCBF dataWith the '33Xe-inhalation method three sliceswere obtained. Mean cerebellar blood flowwas calculated from the lowest slice, andmean blood flow in the cerebral hemisphereswas calculated from the mid-brain slice as themean of all brain pixels. Fixed templates wereused to calculate rCBF in a few corticalregions of interest.
In patients with a full 9-slice SPECTstudy, the analysis of the rCBF data from the[99mTc]-d,l-HMPAO study was performed byassigning 1 of the 10 reference atlas'4 CM lev-els to each rCBF slice. Guided by theassigned anatomical slice and its precon-structed ROI template, ROIs were placed oneach rCBF map after adjusting for size andshape of the brain slice.8 The presentation ofROIs in relation to the lateral brain surface isshown in fig 1. The mean pixel value (Fi,)and the area of each ROI (i) in the number ofpixels were calculated.8 For ROIs appearingin more than one slice in the same subject, aweighted mean flow value was calculated forthe left (Fi,L,) and the right (Fi,R)) ROI. Theside-to-side asymmetry index, SAI, wasdefined as:
SAI,(%) = OxF(R)-F,(L)Fi(ma)
where Fi(max) is the blood flow in the higherof the two ROIs. Anterior/posterior ratioswere calculated as the ratio of the mean rCBFin the frontal cortex to the mean rCBF in thetemporal cortex (FF/FT) or the parietal cortex(FF/Fp).
In all subjects a subcortical low flow area8was defined as shown in fig 2 from the 3 mid-brain slices (slices 4, 5, and 6) as all intrac-erebral pixels with values lower than apreselected low flow threshold, t, definedfrom the peak pixel value, Fp, of the slice as
= 50 + 0-20 x (Fp, -50)
The relative area of the subcortical lowflow region, and the mean rCBF in the sur-rounding high flow cortical rim, were calcu-lated and compared with the parametricmeasurements on the corresponding CTslices.8
Statistical methodsData from the NPH and control groups werecompared using the Wilcoxon two sampletest. Data from before and after shunt opera-tion were compared using the Wilcoxon
657
on 6 July 2018 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.56.6.655 on 1 June 1993. Dow
nloaded from

Waldemar, Schmidt, Delecluse, Andersen, Gjerris, Paulson
Figure 2 SPECT with /99Tc]-d,l-HMPAO (slice 6) in a 51 year old healthy male.The left hemisphere is shown to the left. The colour scale indicates rdative regional cerebralbloodflow (F(%)) values (from 0 to 140%) calculatedfrom corrected relative countratesnormalised to the cerebellum. The peak pixel value of this slice was 136% and the lowflowthreshold 67%. As shown to the right this threshold defined a subcortical low flow region(black), including the ventrides and periventricular tissue, and a surrounding cortical highflow region. The relative area and the mean rCBF of each region was calculated by thecomputer.
paired test. The level of statistical significancewas set at p = 0-05. To adjust for the effect ofmultiple comparisons, a Bonferroni correc-tion was applied to the statistical p values fordifferences in rCBF and SAI (NPH versuscontrol, and post-shunt versus pre-shunt) inthe 17 cortical subregions shown in fig 1.
In the analysis of rCBF patterns in individ-ual patients, CBF parameters (SAI valuesfrom large cortical ROIs (F, T, P, and OC),anterior-posterior ratios, and parameters fromthe subcortical low flow region) were charac-terised as significantly abnormal if they devi-ated by at least 2 SD from control mean. Thediagnostic sensitivity and specificity of a givenparameter in determining surgical outcome
was defined as the predictive value of a nor-mal and a significantly abnormal result (thatis, deviation more than 2 SD from controlmean), respectively.
ResultsClinical outcomeThere were three patients with grade I, fourwith grade II, five with grade III, and twowith a grade IV functional status (table 2).One patient (case 10) died before the postop-erative study. Eleven of the remaining 13patients improved (85%). Seven had a goodclinical outcome (functional grade reduced to0 or by at least two steps), and four patientshad a moderate effect (functional gradereduced by one step) of the operation. Twopatients had a poor clinical outcome (func-tional grade increased) after the operation,despite a well functioning shunt. The aetiol-ogy of NPH in these two patients wasunknown. Two patients needed re-operationbecause of shunt malfunction (case 7) orinfection (case 5). All seven patients withmore than 30% B-waves improved aftershunt operation.
Cranial CTCT data for individual patients are shown intable 1. Ten of 14 patients had periventricu-lar white matter abnormalities (lining, "halo"or irregular periventricular leuco-encephalo-pathy), in two it was associated with smallsubcortical infarcts.As already determined in the selection of
patients, the ventricles were significantlyenlarged in the patients with NPH. Themedian rating score was 4 (range 1-6) ascompared with 0 (range 0-4) in the controlsubjects (p < 0-01). The Evans' ratio was alsosignificantly (p < 0-01) higher in the NPHgroup, median 0-43 (range 0-31-0-52), thanin the control subjects, median 0-29 (range0-24-0-33). When an Evans' ratio at or abovecontrol mean + 2 SD ( = 0-35) was taken asabnormal, the diagnostic sensitivity and
Table 2 Clinicalfunction and regional SPECT abnormalities' in patients with NPH before and after shunt operationSubcortical lowflow region on SPECT
Clinicalfunction2 Corical rCBF deficitse and ventricles on C7
AIP ratio abnormnal SAP Before AfterCase Before After Effect Before Before After SC/C V/C SC/C V/C
1 II III no F/P frontal (NA) + 0 5 + 3-4 -03 + 4-42 II I moderate F/P 4 frontal, parietal, no change + 1*6 + 2-9 + 1*3 + 2-5
and temporal3 I 0 good (NA) (NA) (NA) + 2-3 + 2-4 + 1-3 + 0 94 I 0 good (NA) (NA) (NA) + 2-2 + 4-4 + 2-1 + 3-15 III U moderate F/P t occipital normal + 3-8 + 12-5 + 3-0 + 9 46 IV II good (NA) (NA) (NA) + 5-1 + 3-8 + 01 + 3-87 I 0 good normal none normal + 3-2 + 10-2 + 2-9 + 9-48 i II moderate F/P 1 frontal no change + 2-3 + 8-7 + 2-4 + 2-79 III v no FIT t temporal no change + 1-7 + 7-8 + 0.1 + 4-010 IV (NA) no F/P I none (NA) + 0-2 + 4-1 (NA) (NA)II m I good normal frontal, temporal normal + 5-4 + 11-6 + 2-6 + 2-612 m I good normal frontal, occipital no change + 3-2 + 10-3 + 1.8 + 6-713 II 0 good normal none normal + 4-4 + 12-0 + 1-0 + 3-214 II I moderate F/T T none normal + 3-0 + 10-3 + 1-9 + 5-1
1) abnormal = deviating more than 2 SD from control mean;2) clinical function = functional grading before and after shunt operation (see text);3) cortical rCBF parameters from 9-slice SPECT studies, not available in 3 patients;4) A/P ratio = significantly increased (t) or reduced (1) anterior-posterior ratio of rCBF (F/P, FIT = fronto-parietal, fronto-temporal ratio);5) cortical regions with significantly increased side-to-side asymmetry (SAI) ofrCBF;6) relative area of subcortical low flow region on SPECT (SC/C) and ventricles on CT (V/C), given in z-scores (deviation from control mean in number of SDs)for the mid-brain slice (slice 4, 5, or 6) with the most abnormal enlargement of ventricles. Normal z-scores (below 2 0) given in bold text.(NA) = not available
658 on 6 July 2018 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.56.6.655 on 1 June 1993. D
ownloaded from

SPECT with [99- TcJ-d, I-HMPAO in NPH
Table 3 Regional cerebral bloodflow (rCBF) and side-to-side asymmetry (SAI) of regional cerebral bloodflow valuesmeasured with SPECT and -TcJ-d,l-HMPAO in healthy control subjects and in patients with NPH before and aftershunt operation.
Control (N 14) NPH before (N =11) NPH after (N =9)ROIs: rCBF rCBF rCBF
Cerebral Hemisphere 86-3 (6-6) 80-8 (6-8) 84-4 (9 0)Frontal Cortex (F) 85-5 (6-3) 85-1 (5-6) 84-5 (7-3)Temporal Cortex (T) 89-3 (6-3) 89-0 (4 0) 92-0 (9-5)Superior temporal gyrusand insula cortex (T1) 93-5 (8 5) 97-7 (8 7) 98-9 (11-7)Inferior and middletemporal gyrus (T2) 89-1 (6-6) 85-6 (6-7) 90 4 (11-1)Temporal poles (T3) 78-1 (7-0) 74-2 (6-6) 75-8 (7 3)Parietal Cortex (P) 89-1 (7 3) 93-7 (10-7) 90 4 (11-2)Occipital cortex (OC) 103-1 (10-8) 109-9 (11-3) 105-6 (12-3)Hippocampus (HC) 83-0 (6 3) 77-0 (11-4) 77-2 (7-7)
ROIs: SAI m I SAI I SAI mISAII SAI mISAIICerebral Hemisphere 0-8 (2-0) 1-7 0-5 (7-4) 4-9 -2-3 (5 8) 3-9Frontal Cortex (F) 0-8 (2-8) 2-2 -2-3 (8-1) 5-9 -4-6 (6 5) 5-1Temporal Cortex (T) 1-8 (3-9) 3-4 1-4 (9 3) 6-8 -0-7 (6-0) 4-8Superior temporal gyrusandinsula cortex (Tl) 3-1 (5-1) 5-2 1-0 (7 8) 5-5 0-1 (6-8) 5-3Inferior and middletemporal gyrus (T2) 1-0 (4-1) 3-3 2-4 (13-4) 10-5* -1-0 (7-4) 5-8Temporalpoles (T3) 1 1 (6-1) 4-5 0-9 (11-7) 8-5 -1-7 (5 4) 4-7Parietal Cortex (P) 1-7 (3-3) 2-9 1-2 (5 5) 4-5 0-2 (5-9) 4-2Occipital cortex (OC) -0 9 (3 7) 3-1 1-1 (5-3) 4-1 -2-0 (7-1) 4.9Hippocampus (HC) -2-3 (6 0) 5-1 -1-5 (11-0) 8-0 -5 7 (7 8) 6-9
The results are presented as mean (SD) for all subjects with a full 9 slice SPECT study. rCBF = regional cerebral blood flow rel-ative to cerebellar blood glow given in %. SAI = side-to-side asymmetry index given in % (see text). A negative value indicatesthat left rCBF > right rCBF. m SA = mean numerical SAI. Data from the 9 frontal and parietal subregions are not shown, butthey were included in the statistical analysis. Data in the NPH group were compared with data from the control group usingWilcoxon two-sample tests (* = p < 0-002), and data from before and after shunt operation were compared using Wilcoxonmatched-pairs tests. After Bonferroni correction to adjust for multiple comparisons, there were no other significant differences(effective significance level 0-003).
specificity of the Evans' ratio for predictingclinical outcome after shunt operation was50% and 100%, respectively. There was nosignificant difference in the cortical atrophyratings, between the control subjects (median0, range 0-20) and the NPH patients(median 3, range 0-10). There was a signifi-cant reduction, although not complete nor-malisation, of ventricle size (p < 0 05) andEvans' ratio (p < 0.01) after shunt operation(table 1).
Global, cortical and subcortical rCBF in patientswith NPH vs control subjectsResults are presented as mean (SD) values.Global CBF, as measured with the 133Xeinhalation method, was 62-5 (8 9)ml/(100g min) and 58-9 (7'7) ml/100g-min)in the NPH and the control groups, respec-tively (non-significant). No significant differ-ences were seen in the regional CBF data.FECO, was significantly higher in the NPHgroup (4-6 (0 6) %) than in the control group[3-9 (0-6) %]-
Table 4 Regional cerebral bloodflow measured with SPECTand /9Tc]-d,l-HMPAOin healthy control subjects and in patients with NPH: subcortical low flow region.
Control (N = 14) NPH before (N = 14) NPH after (N = 13)Mean (SD) Mean (SD) Mean (SD)
Relative area of ventricleson CT (V/C %)slice 4 31 (3-1) 264 (10.9)** 17-1 (49) +slice 5 5-1 (2-9) 28-1 (9.9)** 18-6 (8-5) + +slice 6 6-2 (3 5) 22-2 (6.6)** 16-7 (7 4)Relative area ofcentral low flow region (%)slice 4 23-2 (6 5) 42-2 (12.2)** 31-0 (7-7) +slice 5 23 2 (7 6) 44 6 (11l5)** 34 0 (11 2) +slice 6 17 4 (4 4) 38-8 (12-8)** 26-7 (11 1) +
The results are presented as mean (SD). ** = p < 0-01 for comparison of NPH vs. controlgroup, Wilcoxon two-sample test. +, + + = p < 0 05, p < 0-01 for comparison of data beforeand after shunt operation, Wilcoxon matched-pairs test. The total SPECT slice area measuredin number of pixels was 1387 (112), 1563 (98), and 1591 (124) in slice 4, 5, and 6 respectively.There was no significant differences in these figures between NPH and control and betweenpre- and post-shunt images.
Mean CBF data obtained with the [99mTc]-d,l-HMPAO technique are presented intables 3 and 4. As in the '33Xe study, therewas no significant difference in global CBF orin the regional CBF data. The fronto-parietalratio of rCBF, however, was significantlylower (p < 0 05) in NPH patients (0-92(0 09)) than in control subjects [0-96 (0-04)],while there was no significant difference inthe fronto-temporal ratio. Generally, themean numerical SAI values were highest inthe NPH group (ranging from 4- 1% to 1 -4%in different ROIs) compared with the controlgroup (ranging from 2-2% to 5-3%). AfterBonferroni correction, only the inferior andmid-temporal cortex had a significantlyenhanced SAI (table 3).The mean rCBF of the central white
matter (centrum semiovale) was slightlyreduced (p < 0-05): 51-6 (12-7) % in NPHversus 63-0 (7-5) % in control subjects. TheSAI of the central white matter was signifi-cantly (p < 0-05) higher in NPH (+6-0(13-0)] %, mean numerical value 11*4%)than in control subjects (-2-3 (5 5) %, meannumerical value 4-9 %). The analysis of thesubcortical low flow region is presented intable 4. In slice 4, the mean area of the sub-cortical low flow region, relative to the totalSPECT slice area, was 42-2 (12-2) % in NPHpatients and 23-2 (6-5) % in control subjects(p < 0-01). Computerised measurement ofthe area of ventricles on the equivalent CTslice showed that the ventricles occupied inmean 26-4 (10-9) % of the total slice area asopposed to 3-1 (3 1) % in control subjects(p < 0-01). Accordingly, NPH was associatedwith enlarged ventricles, an enlarged subcor-tical low flow region, and a reduction of thearea of the cortical high flow region. Similarresults were obtained in slices 5 and 6(table 4).
659 on 6 July 2018 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.56.6.655 on 1 June 1993. D
ownloaded from
Waldemar, Schmidt, Delecluse, Andersen, G6erris, Paulson
The effect ofshunt-operation on rCBFIn the NPH group as a whole, no significantpost-shunt changes were observed in globalor regional cortical CBF. The size of the sub-cortical low flow region as well as the area ofthe ventricles were reduced significantly aftershunt-operation, although still abnormal(table 4).
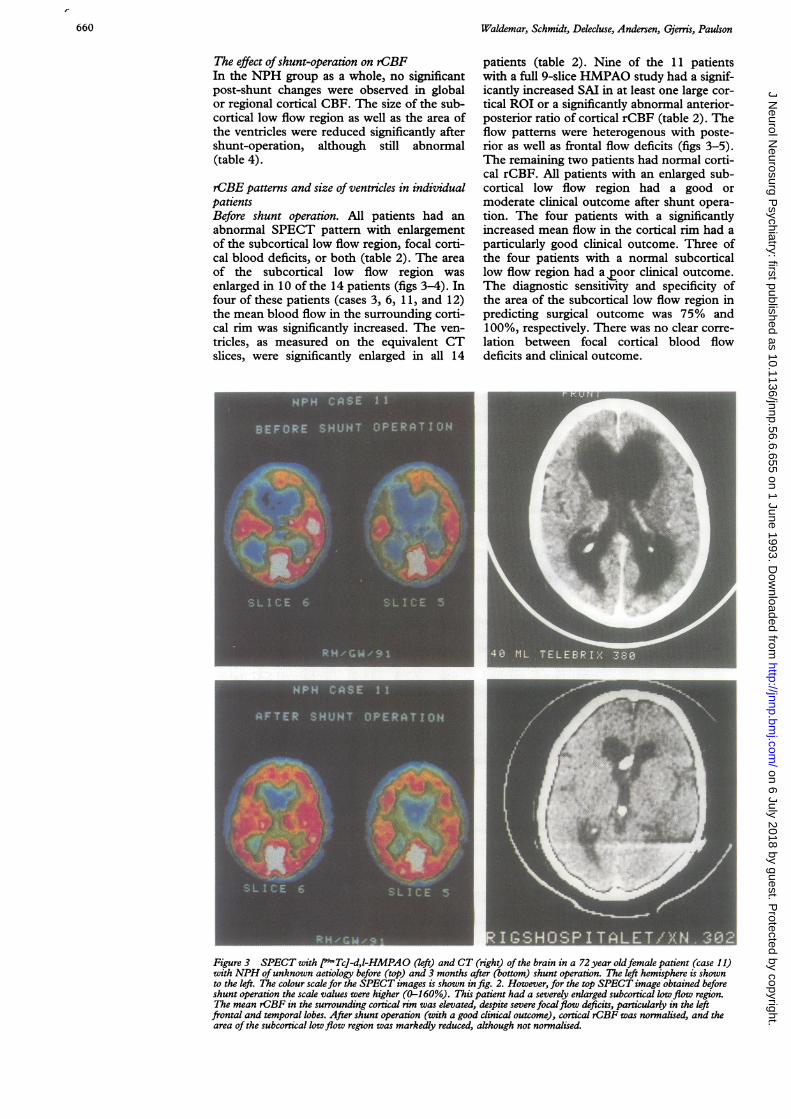
rCBE patterns and size of ventricles in individualpatientsBefore shunt operation. All patients had anabnormal SPECT pattern with enlargementof the subcortical low flow region, focal corti-cal blood deficits, or both (table 2). The areaof the subcortical low flow region wasenlarged in 10 of the 14 patients (figs 3-4). Infour of these patients (cases 3, 6, 1 1, and 12)the mean blood flow in the surrounding corti-cal rim was significantly increased. The ven-tricles, as measured on the equivalent CTslices, were significantly enlarged in all 14
patients (table 2). Nine of the 11 patientswith a full 9-slice HMPAO study had a signif-icantly increased SAI in at least one large cor-tical ROI or a significantly abnormal anterior-posterior ratio of cortical rCBF (table 2). Theflow patterns were heterogenous with poste-rior as well as frontal flow deficits (figs 3-5).The remaining two patients had normal corti-cal rCBF. All patients with an enlarged sub-cortical low flow region had a good ormoderate clinical outcome after shunt opera-tion. The four patients with a significantlyincreased mean flow in the cortical rim had aparticularly good clinical outcome. Three ofthe four patients with a normal subcorticallow flow region had a 2oor clinical outcome.The diagnostic sensitivity and specificity ofthe area of the subcortical low flow region inpredicting surgical outcome was 75% and100%, respectively. There was no clear corre-lation between focal cortical blood flowdeficits and clinical outcome.
Figure 3 SPECT with /99,Tc]-d,l-HMPAO (left) and CT (right) of the brain in a 72year oldfemale patient (case 11)with NPH ofunknown aetiology before (top) and 3 months after (bottom) shunt operation. The left hemisphere is shownto the left. The colour scale for the SPECT images is shown in fig. 2. However, for the top SPECT image obtained beforeshunt operation the scale values were higher (0-160%). This patient had a severely enlarged subcortical lowflow region.The mean rCBF in the surrounding cortical rim was elevated, despite severe focalflow deficits, particularly in the leftfrontal and temporal lobes. After shunt operation (with a good clinical outcome), cortical rCBF was normalised, and thearea of the subcortical lowflow region was markedly reduced, although not normalised.
660 on 6 July 2018 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.56.6.655 on 1 June 1993. D
ownloaded from

SPECT with [ 99m Tc]-d, l-HMPAO in NPH
Figure 4 SPECTwith r"Tc]-d,l-HMPAO (left) and CT (right) in a 66year old male patient (case 14) with NPH,secondary to a head trauma, before (top) and 6 months after (bottom) shunt operation. The left hemisphere is shown tothe left. The colour scale for the SPECT images is shown in fig 2. This patient had an enlarged subcortical low flow regionandfocal cortical bloodflow deficits in the temporal cortex. After shunt operation (with a moderate clinical outcome) therCBF pattern seen on SPECT was normalised.
Figure 5 SPECT withp9-Tc]-d,l-HMPAO in a71 year old male patient(case 9) with NPH ofunknown origin before(left) and 4 months after(right) shunt operation.The left hemisphere isshown to the left. Thecolour scale is shown infig. 2. This patient had alarge, but normal,subcortical lowflow regionandfocal cortical bloodflow deficits particularly inthe left hemisphere. Despitefulfilling the clinical andhydrodynamic criteria forNPH, this patient had no
effect of the operation anddeterioratedfurther.Regional CBF wasunchanged.
After shunt operation. In five patients thesize of the enlarged subcortical low flowregion was normalised (fig 4), in a furtherfour patients it was reduced (fig 3), and inone patient unchanged or slightly greater(table 2). Increased mean cortical blood flowwas reduced after shunt in all cases. The mid-brain area of the ventricles on CT was nor-malised in one patient, reduced in 10patients, unchanged in one patient, andincreased in one patient. Cortical blood flowdeficits were normalised in three patients andunchanged in four patients. In one of the lat-ter patients (case 8) the frontal flow deficitwas related to a small infarct (table 1).
DiscussionRegional cerebral bloodflow in NPHTo our knowledge this study is the first to use[99mTc]-d,l-HMPAO with high resolutionSPECT in NPH to measure the area of thesubcortical low flow region, a region of pri-mary interest in NPH. Although NPH should
661 on 6 July 2018 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.56.6.655 on 1 June 1993. D
ownloaded from

Waldemar, Schmidt, Delecluse, Andersen, Gjerris, Paulson
be defined from clinical, CT, and hydrody-namic criteria, SPECT may serve a separateand important role in the differential diagno-sis. Clinically NPH may resemble normalageing, benign senile forgetfulness,Alzheimer's disease, or other degenerativedementia disorders, which may be associatedwith enlarged ventricles and similar symp-toms. The ventricles are larger in NPH thanin elderly control subjects, but there is noobjective way to absolutely differentiatehydrocephalus from central atrophy.Periventricular white matter hypodensities onCT or hyperintensities on MRI are frequentlyseen in elderly patients, and also in patientswithout evidence of dementia.'5 The relativeoccurrence in NPH and the significance inrelation to CSF shunting is questionable.'5-'7Although it has been shown that increasedR.Ut is significantly associated with surgicaloutcome,418 the reported response rates aftershunt operation are highly variable, evenwhen taking hydrodynamic criteria intoaccount. The response rate in our study wasabout the same as in previous studies.'8SPECT might help identify patients withdegenerative dementia disorders, not likely tobenefit from surgery. However, it is still anopen question, whether Alzheimer's diseaseor other degenerative diseases could be asso-ciated with a partial and reversible CSFabsorption defect.
In this study SPECT correctly classifiedpatients from control subjects, in that allpatients had an abnormal rCBF pattern. Theindividual rCBF patterns were heterogeneouswith cortical as well as subcortical flowabnormalities. The most frequent pattern wasthat with an enlargement of the subcorticallow flow region associated with focal corticalblood flow deficits. Patients with a normalsubcortical low flow region were unlikely torespond clinically to shunt operation.
There are at least three studies of tomo-graphic rCBF using SPECT in NPH. 19-21Vorstrup et a!'9 in a study using the "'3Xenoninhalation method and SPECT found abnor-mal preoperative SPECT scans in all 17patients with either an abnormal large centrallow flow area or a reduced flow bilaterally inthe occipital and contiguous temporo-parietalregions. Postoperative improvement of rCBFwas seen in six of the 17 patients. Moretti etaP'0 used 123I-IAMP with SPECT to study 23patients with NPH. They found a frontal andparietal hypoactive pattern which improvedafter shunting in patients with a good clinicaloutcome. Graff-Radford et aP" studied 22NPH patients with the "33Xe-inhalationmethod and found a reduction of globalCBF, preferentially affecting the frontal lobe.An anterior/posterior ratio of 1 05, togetherwith the relative duration of B-waves, theduration of dementia, and gait abnormalitypreceding dementia, correctly classified surgi-cal outcome in a majority of patients.22 In ourpatients the anterior/posterior ratio did notdetermine surgical outcome. As in this study,post-shunt changes in CBF did not accom-pany improvement in the functional state in
all patients.Brooks et al 23 studied regional cerebral
oxygen extraction, oxygen metabolism, andCBF, with positron emission tomography inseven patients with NPH, three of whom hadidiopathic NPH. The oxygen extraction wasnormal. The rCBF matched the reducedregional oxygen metabolism. No improve-ment of rCBF was seen after shunt operation.Jagust et al 24 studied regional glucose metab-olism with positron emission tomography in 3patients and found a global reduction ofmetabolism.Thus most studies found a global reduc-
tion of flow and metabolism, while in ourstudy global CBF, measured with two differ-ent methods, was normal. It is likely that withour individualised ROI templates the braintissue was better delineated from extracere-bral structures. Some of the previous studiesfound focal cortical flow deficits, but therehas been disagreement as to their typical loca-tion. In this study the analysis of the fronto-parietal ratio and the side-to-side asymmetryratio of rCBF pointed to a fronto-temporalpredilection. In the individual analysis ofrCBF, however, it became clear that therCBF patterns were heterogenous. Theobserved rCBF patterns differed from therCBF patterns in other dementia disorders:in Alzheimer's disease a global CBF reduc-tion is seen, but with a disproportionatereduction of rCBF in posterior brain regions.The rCBF patterns are heterogenous andalways abnormal, often with severe focalrCBF reductions in fronto-parietal associa-tion areas. Severe enlargement of the subcor-tical low flow area is uncommon.25 Althoughno direct comparisons were made, the rCBFpattern in at least one of the patients with noclinical improvement after shunt operationresembled Alzheimer' disease. In frontal lobedementia26 and in Huntington's chorea27rCBF is reduced primarily in fronto-temporalbrain regions. Except for a reduction of rCBFin the caudate nuclei in the latter disease,subcortical blood flow has not been describedas abnormal.The enlargement of the subcortical low
flow region which was observed in this studywas due primarily to the enlarged ventricles.However, the area of the subcortical low flowregion was normal in some of the patientswith considerably enlarged ventricles.Furthermore, the subcortical low flow regionwas normalised after shunt operation even inpatients with still very large ventricles.Finally, in the group of NPH patients as awhole there was a reduction of rCBF in thecentral white matter, probably contributing tothe enlargement of the subcortical low flowregion. Thus the area of this region onSPECT contained information that was dif-ferent, and in some ways superior, to that ofthe size of ventricles on CT. We speculatethat enlargement of the ventricles due toNPH leads to a significant, and partlyreversible, enlargement of the subcortical lowflow region on SPECT. In contrast, enlarge-ment of the ventricles due to central atrophy
662 on 6 July 2018 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.56.6.655 on 1 June 1993. D
ownloaded from
SPECT with [99m Tc]-d, l-HMPAO in NPH
may only slightly, or not at all, increase thearea of the subcortical low flow region.Cortical blood flow deficits were improvedafter shunt operation in only a few patients.Probably, the NPH condition had alreadycaused irreversible structural changes withtissue degeneration, or some patients mayhave had a primary degenerative dementiadisorder. Although the Evans' ratio was alsoassociated with surgical outcome, CT datawere less successful than SPECT in predict-ing clinical outcome. However, both CT andSPECT are important tools for defining dis-eases other than NPH, which could havecaused dementia, before the final decisionabout surgery is made.
Methodological considerations[99mTc]-d,l-HNIPAO is a lipophilic tracercompound for measurements of rCBF withSPECT. The regional distribution in thebrain is proportional to rCBF,'8 although alinearisation correction is preferable to cor-rect for a preferential back-diffusion fromhigh flow regions. 13 The HMPAO methodhas already proved to be a valuable tool in thefocal diagnosis of epilepsy,29 and in the studyof normal ageing8 and degenerative neuropsy-chiatric diseases.2527 30 Frontal and subcorticalregions are visualised particularly well incomparison with the "33Xe inhalation method.The [99mTc]-d,l-HMPAO method, however,does not easily offer quantitative data, as doesthe "'Xe inhalation method.828 Data obtainedwith the [99mTc]-d,l-HMPAO method aretherefore usually expressed as regional count-rates relative to the mean count-rate of a ref-erence region, in our study, the cerebellum.8The cerebellum was chosen as referenceregion in NPH, because mean rCBF in thecerebellum measured with the "33Xe method,was not different from the control group, andbecause NPH is not known to be associatedwith structural abnormalities in the cerebel-lum. We used the cerebellar hemisphere withthe highest blood flow as reference region toavoid cerebellar tissue influenced by anycrossed cerebellar diaschisis. However, signif-icant side-to-side asymmetry was not seen inany patient. It is unlikely therefore that globalCBF was artefactually raised because of lowflow in the cerebellum. The higher FECO2during the "33Xe study in patients with NPH,compared with healthy control subjects, mayhave been caused by differences in the degreeof hyperventilation during the inhalation pro-cedure. Although this may have added to dif-ferences in CBF as measured with the "33Xemethod, it could not have significantlyaffected CBF measured in the [99mTc]-d,l-HMPAO study. The cortical ROIs shown infig 1 were defined in recognition of the in-plane and axial resolution of the method.They were partly arbitrary and partly basedon anatomical landmarks, such as large sulci,easily recognisable on most SPECT images,even in NPH. Because of the disturbedanatomy of the NPH brain and the interindi-vidual variability, the definition of most ROIscould not be based on a stereotactic atlas.
Pathophysiology ofNPHTheoretically, the different abnormal rCBFpatterns seen in NPH could reflect severalstages of the disease: Initially a progressiveresistance to outflow of CSF leads to enlargedventricles.'4 As a result, the area of the sub-cortical low flow region increases. Later,compromised white matter rCBF and persis-tent brain dysfunction is caused by continuedtension against the brain tissue across theependymal surface of the ventricles. There isa further increase in the area of the subcorti-cal low flow region, and mean rCBF in thethinned cortical rim increases. After sometime, due to deafferentation from the suffer-ing white matter, focal cortical blood flowdeficits appear, leaving the mean corticalblood flow subnormal. With further progres-sion of the disease the subcortical low flowregion may be extremely large, and severecortical blood flow deficits appear (fig 3).Even at this point, the SPECT abnormalitiesmay still be reversible after shunt operation.The relative increase of mean rCBF in the
thin cortical rim in some patients was proba-bly caused by a higher proportion of greymatter tissue relative to white matter tissueand a higher neuron density, than in thebroader cortical rim of the control subjects.Alternatively, the rise in cortical rCBF couldbe artefactual and caused by a reduced bloodflow in the cerebellum. This is unlikely, as thefour patients all had a normal rCBF in thecentral white matter (relative to the cerebel-lum). Furthermore, their mean blood flow inthe cerebellum measured with the "33Xe tech-nique was within the normal range (in 3 ofthem even high in the normal range).The heterogeneity of rCBF patterns could
reflect different underlying degenerative orvascular dementia disorders, as already dis-cussed. Patients with a poor or a missingresponse to shunt operation and periventricu-lar hypodensities on CT could also have suf-fered from subcortical arterioscleroticencephalopathy."7 Only studies with post-mortem analysis or biopsy would clarify thisimportant question.
In conclusion, NPH is associated with anenlargement of the subcortical low flowregion, a relative reduction of blood flow inthe frontal cortex, and an asymmetricalreduction of rCBF in the inferior and mid-temporal cortex, and in the central whitematter. In this study individual rCBF pat-terns on SPECT were all abnormal, but het-erogenous, with the most frequent patternbeing an enlarged subcortical low flow region,in some cases associated with focal corticalblood flow deficits. Shunt operation nor-malised or improved the rCBF pattern inmost patients, and improved the clinical sta-tus of 11 patients, 10 of whom had a signifi-cantly enlarged subcortical low flow region.Three (of 14) patients, all having focal corti-cal rCBF deficits together with a normal sub-cortical low flow region, did not improveclinically after shunt operation. We thereforesuggest that SPECT may help to identify
663 on 6 July 2018 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.56.6.655 on 1 June 1993. D
ownloaded from

Waldemar, Schmidt, Delecluse, Andersen, Gierris, Paulson
patients not likely to benefit from shunt oper-ation, a hypothesis to be tested in a largersample of patients with more detailed longitu-dinal neuropsychological evaluation.
This study was supported by grants from the Danish MedicalResearch Council, the Lundbeck Foundation, and the DanishHospital Foundation for Medical Research. Region ofCopenhagen, The Faroe Islands, and Greenland. GlennaSkouboe, and Gerda Thomsen are thanked for their excellenttechnical assistance.
1 Hakim S, Adams RD. The special clinical problem ofsymptomatic hydrocephalus with normal cerebrospinal-fluid pressure. Observations on cerebrospinal fluidhydrodynamics. J Neurol Sci 1965;2:307-77.
2 Adams RD, Fischer CM, Hakim S, Ojemann RG, SweetWH. Symptomatic occult hydrocephalus with "normal"cerebrospinal fluid pressure. New Engl Y Med 1965;273:117-26.
3 Borgesen SE, Gjerris F, S0rensen SC. Intracranial pres-sure and conductance to outflow of cerebrospinal fluidin normal pressure hydrocephalus. J Neurosurg 1979;50:489-93.
4 Borgesen SE, Gjerris F. The predictive value of conduc-tance to outflow of CSF in normal pressure hydro-cephalus. Brain 1982;105:65-86.
5 Turner DA, McGeachie RE. Normal pressure hydro-cephalus and dementia-Evaluation and treatment.Clinics in Geriatric Medicine 1988;4:815-30.
6 Evans WA. An encephalographic ratio for estimating ven-tricular enlargement and cerebral atrophy. Arch Neurol1942;47:931-7.
7 Stein SC, Langfitt TW. Normal-pressure hydrocephalus.Predicting the results of cerebrospinal fluid shunting.J Neurosurg 1974;41:463-70.
8 Waldemar G, Hasselbalch SG, Andersen AR, et al.99-Tc-d,l-HMPAO and SPECT of the brain in normalaging. J Cereb Blood Flow Metab 1991;11:508-21.
9 Jacoby RJ, Levy R, Dawson JM. Computed tomographyin the elederly: I. The normal population. Br JPsychiatry 1980;136:249-55.
10 Turkheimer E, Cullum CM, Hubler DW, Paver SW, YeoRA, Bigler ED. Quantifying cortical atrophy. J NeurolNeurosurg Psychiatry 1984;47: 1314-18.
11 Stokely EM, Sveinsdottir E, Lassen NA, Rommer P. Asingle photon dynamic computer assisted tomograph(DCAT) for imaging brain function in multiple crosssections. J Comput Assist Tomogr 1980;4:230-40.
12 Celsis P, Goldman T, Henriksen L, Lassen NA. Amethod for calculating regional cerebral blood flowfrom emission computed tomography of inert gas con-centrations. J ComputAssist Tomogr 1981;5:641-5.
13 Lassen NA, Andersen AR, Friberg L, Paulson OB. Theretention of [99mTc]-d,l-HMPAO in the human brainafter intracarotid bolus injection. A kinetic analysis.Y Cereb Blood Flow Metab 1988;8:S13-22.
14 Aquilonius S-M, Eckernas S-A. A colour adas of the humanbrain. Adapted to computed tomography. Stockholm:Esselte Studium, 1980.
15 Zimmerman RD, Fleming CA, Lee BCP, Saint-Louis LA,Deck MDF. Periventricular hyperintensity as seen by
magnetic resonance: Prevalence and significance. AJNR1986;7:13-20.
16 Jack CR, Mokri B, Laws ER, Houser OW, Baker HL,Petersen RC. MR findings in normal-pressure hydro-cephalus: significance and comparison with other formsof dementia. J Comput Assist Tomogr 1987;11:923-3 1.
17 Kinkel WR, Jacobs L, Polachini I, Bates V, Heffner RR.Subcortical arteriosclerotic encephalopathy (Bins-wanger's disease). Computed tomographic, nuclearmagnetic resonance, and clinical correlations. ArchNeurol 1985;42:951-9.
18 Gjerris F, B0rgesen SE. Pathophysiology of the CSF cir-culation. In: Crockard A, Hayward R, Hoff JT, eds.Neurosurgery. The scientific basis of clinical practice, vol 1,2nd ed. Oxford: Blackwell Scientific, 1992.
19 Vorstrup S, Christensen J, Gjerris F, Sorensen PS,Thomsen AM, Paulson OB. Cerebral blood flow inpatients with normal-pressure hydrocephalus before andafter shunting. J Neurosurg 1987;66:379-87.
20 Moretti J-L, Sergent A, Louarn F, et al. Cortical perfusionassessment with 123I-isopropyl amphetamine (12"I-IAMP)in normal pressure hydrocephalus (NPH). Eur J NuclMed 1988;14:73-79.
21 Graff-Radford NR, Rezai K, Godersky JC, Eslinger P,Damasio H, Kirchner PT. Regional cerebral blood flowin normal pressure hydrocephalus. J Neurol NeurosurgPsychiatry 1987;50: 1589-96.
22 Graff-Radford NR, Godersky JC, Jones MP. Variablespredicting surgical outcome in symptomatic hydro-cephalus in the elderly. Neurology 1989;39: 1601-4.
23 Brooks DJ, Beaney RP, Powell M, et al. Studies on cere-bral oxygen metabolism, blood flow, and blood volume,in patients with hydrocephalus before and after surgicaldecompression, using positron emission tomography.Brain 1986;109:613-28.
24 Jagust WJ, Friedland RP, Budinger TF. Positron emissiontomography with ['8F]Fluorodeoxyglucose differentiatesnormal pressure hydrocephalus from Alzheimer-typedementia. J Neurol Neurosurg Psychiatry 1985;48:1091-6.
25 Paulson OB, Andersen AR, Waldemar G. Utility of theretained tracer-complex [99mTc]-HMPAO for measure-ments of regional cerebral blood flow in epilepsy anddementia. In: Lassen NA, Ingvar DH, Raichle ME,Friberg L, eds. Brain work and mental activity.Copenhagen: Munksgaard 1991:363-73.
26 Neary D, Snowden JS, Northen B, Goulding P. Dementiaof frontal lobe type. J Neurol Neurosurg Psychiatry1988;51;353-61.
27 Hasselbalch SG, 0berg G, S0rensen SA, et al. Reducedregional cerebral blood flow in Huntington's diseasestudied by SPECT. J Neurol Neurosurg Psychiatry 1992;55:1018-23.
28 Andersen AR, Friberg HH, Schmidt JF, Hasselbalch SG.Quantitative measurements of cerebral blood flow usingSPECT and ["mTc]-d,l-HMPAO compared to xenon-133. J Cereb Blood Flow Metab 1988;8:S69-81.
29 Andersen AR, Waldemar G, Dam M, Fugisang-Frederiksen A, Herning M, Kruse-Larsen C. SPECT inthe presurgical evaluation of patients with temporal lobeepilepsy-a preliminary report. Acta Neurochir1990;Suppl 50:80-83.
30 Waldemar G, Vorstrup S, Jensen TS, Johnsen A, BoysenG. Focal reductions of cerebral blood flow in amy-otrophic lateral sclerosis: A [99mTc]-d,l-HMPAO study.JrNeurol Sci 1992;107:19-28.
664 on 6 July 2018 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.56.6.655 on 1 June 1993. D
ownloaded from