hereditary colorectal cancer: an overview felice schnoll-sussman,md jay monahan center for...
TRANSCRIPT

Hereditary Colorectal Cancer: Hereditary Colorectal Cancer: An OverviewAn Overview
Felice Schnoll-Sussman,MDFelice Schnoll-Sussman,MDJay Monahan Center for Gastrointestinal HealthJay Monahan Center for Gastrointestinal Health
New York Hospital/ Weill Cornell Medical CollegeNew York Hospital/ Weill Cornell Medical College

U.S. Cancer Cases and Deaths - 2001U.S. Cancer Cases and Deaths - 2001
020,00040,00060,00080,000
100,000120,000140,000160,000180,000200,000
Prostate Breast Lung Colorectal
New CasesDeaths
CA Ca J Clin 2001

Colon Cancer, 2001Colon Cancer, 2001
• 135,400 cases, 56,700 deaths135,400 cases, 56,700 deaths
• 22ndnd most common cause of cancer most common cause of cancer deathdeath
• Lifetime risk 6%, about 1 in 17Lifetime risk 6%, about 1 in 17
• 93% of cases occur at >50 years 93% of cases occur at >50 years ageage
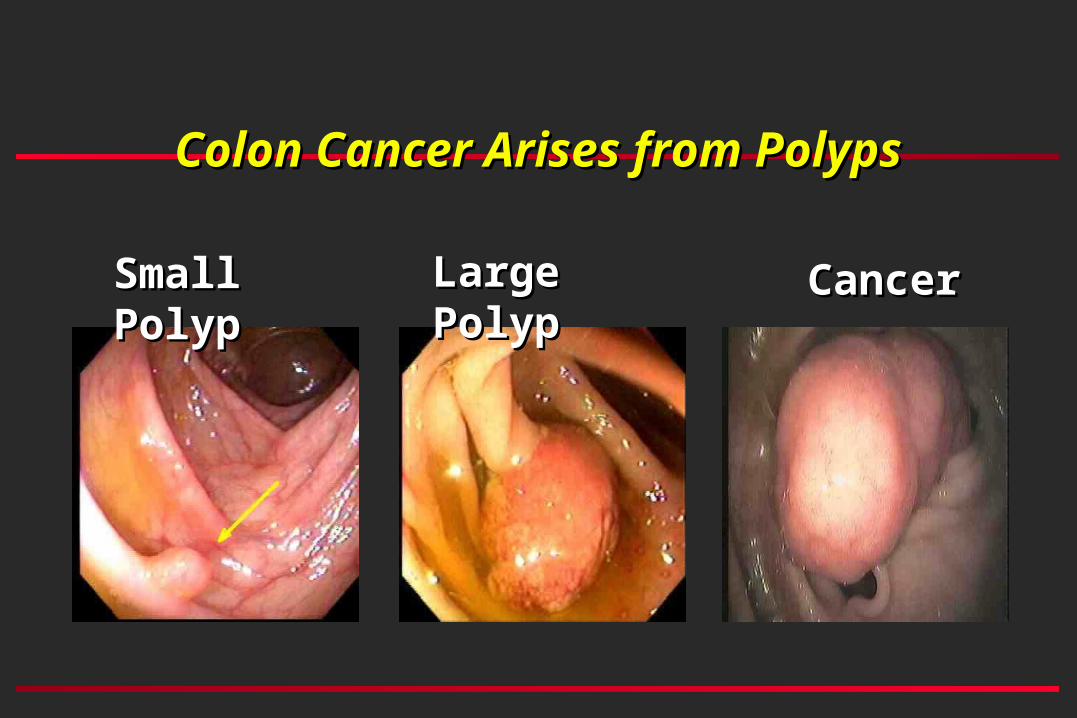
Colon Cancer Arises from PolypsColon Cancer Arises from Polyps
Small PolypSmall Polyp Large PolypLarge Polyp CancerCancer
Characteristics of Screening Tests for Characteristics of Screening Tests for CRCCRC
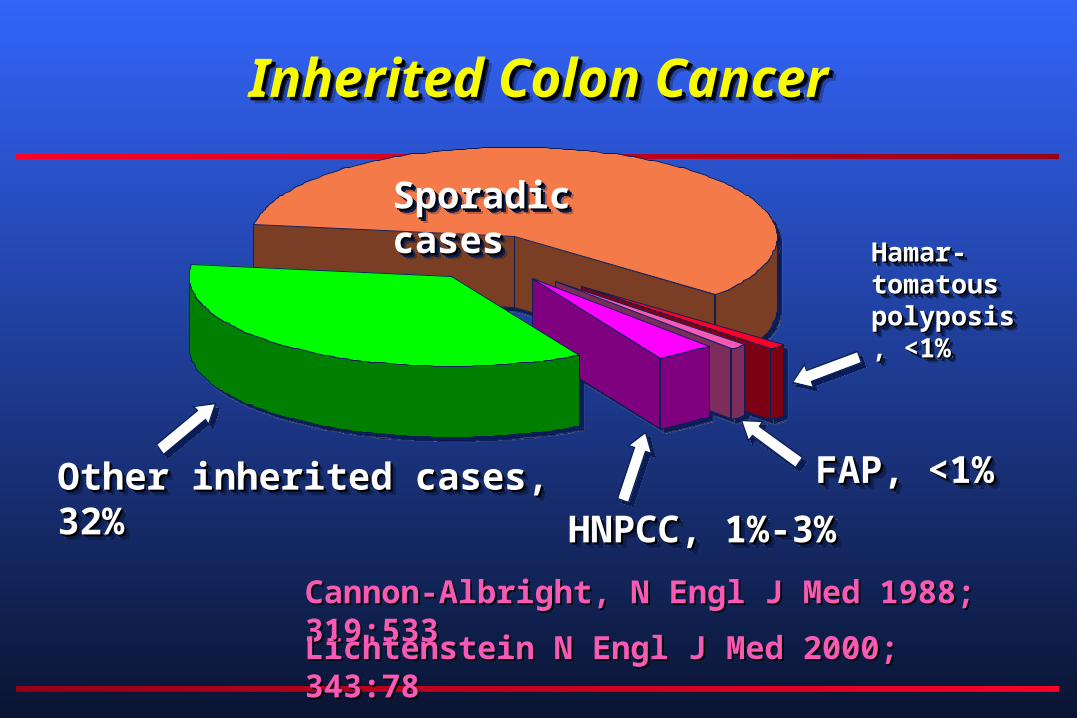
Sporadic casesSporadic casesSporadic casesSporadic cases
Other inherited cases, 32%Other inherited cases, 32%Other inherited cases, 32%Other inherited cases, 32%
Hamar-Hamar-tomatous tomatous polyposis, polyposis, <1%<1%
Hamar-Hamar-tomatous tomatous polyposis, polyposis, <1%<1%
FAP, <1%FAP, <1%FAP, <1%FAP, <1%
HNPCC, 1%-3%HNPCC, 1%-3%HNPCC, 1%-3%HNPCC, 1%-3%
Inherited Colon CancerInherited Colon CancerInherited Colon CancerInherited Colon Cancer
Cannon-Albright, N Engl J Med 1988; 319:533Cannon-Albright, N Engl J Med 1988; 319:533
Lichtenstein N Engl J Med 2000; 343:78Lichtenstein N Engl J Med 2000; 343:78

Syndromes GenesSyndromes Genes
SyndromeSyndrome GeneGeneFAPFAP APCAPCHNPCCHNPCC MMRMMRPeutz-JeghersPeutz-Jeghers STK11STK11Juvenile PolyposisJuvenile Polyposis SMAD4SMAD4Cowden SyndromeCowden Syndrome PTENPTEN

HereditaryHereditaryMother or Mother or FatherFather
1 damaged gene1 damaged gene1 normal gene1 normal gene
NonhereditaryNonhereditary
2 normal genes2 normal genes
Loss of normal geneLoss of normal gene
1 damaged gene1 damaged gene1 normal gene1 normal gene
Loss of normal geneLoss of normal gene
1 damaged gene1 damaged gene1 normal gene1 normal gene
The Development of Hereditary CancerThe Development of Hereditary Cancer
© 2001 Myriad Genetic Laboratories© 2001 Myriad Genetic Laboratories

Malignant Malignant transformationtransformationTCGATTCGAT
AGCTAAGCTA
HNPCC results from defective DNA repairHNPCC results from defective DNA repair
AGCTAAGCTATCGATTCGAT
AGCTAAGCTATCGATTCGAT
Cell Cell withwithDNA mismatch DNA mismatch repairrepair
AGAGTTTATATCTCAAATAT
Cell Cell without without DNA mismatch DNA mismatch repair (HNPCC)repair (HNPCC)
AGAGTTTATATCTCGGATAT

Genes That Give Rise to HNPCCGenes That Give Rise to HNPCC
HNPCC is associated with germline mutations in any HNPCC is associated with germline mutations in any one of five mismatch repair genesone of five mismatch repair genes
Chr 2Chr 2Chr 3Chr 3
Chr 7Chr 7
MSH2MSH2
PMS1PMS1
MLH1MLH1PMS2PMS2
MSH6MSH6
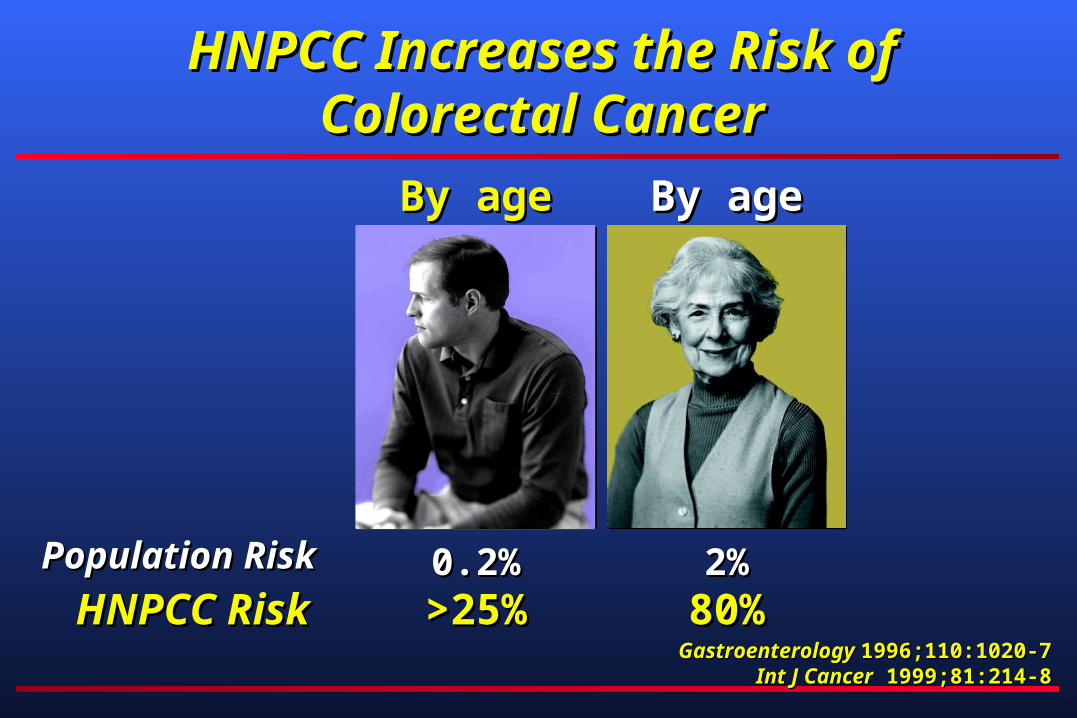
Population RiskPopulation Risk
By age 50By age 50
0.2%0.2%
By age 70By age 70
2%2%HNPCC RiskHNPCC Risk >25%>25% 80%80%
Gastroenterology Gastroenterology 1996;110:1020-71996;110:1020-7Int J CancerInt J Cancer 1999;81:214-8 1999;81:214-8
HNPCC Increases the Risk ofHNPCC Increases the Risk ofColorectal CancerColorectal Cancer

Population RiskPopulation Risk
By age 50By age 50
0.2%0.2%
By age 70By age 70
1.5%1.5%
HNPCC RiskHNPCC Risk 20%20% 60%60%Gastroenterology Gastroenterology 1996;110:1020-71996;110:1020-7
Int J CancerInt J Cancer 1999;81:214-8 1999;81:214-8
HNPCC Increases the Risk of HNPCC Increases the Risk of Endometrial CancerEndometrial Cancer

HNPCC Increases the Risks of HNPCC Increases the Risks of Other CancersOther Cancers
• OvaryOvary• 12% by age 7012% by age 70
• StomachStomach• 13% by age 7013% by age 70
• OtherOther• Urinary tract (4% by age 70)Urinary tract (4% by age 70)• Small intestine (100-fold relative risk, but < 5%)Small intestine (100-fold relative risk, but < 5%)• Biliary tract (2% by age 70)Biliary tract (2% by age 70)• Brain (~4% by age 70)Brain (~4% by age 70)
Gastroenterology Gastroenterology 1996;110: 1020-71996;110: 1020-7Int J CancerInt J Cancer 1999;81:214-8 1999;81:214-8

0%10%20%30%40%50%60%70%80%90%
100%
Percent diagnosed with a second
cancer
10 yrs after firstcancer
15 yrs after firstcancer
General Population HNPCC Cancer Cancer 1977;40:18491977;40:1849Dis Colon Rectum Dis Colon Rectum 1993;36:3881993;36:388
HNPCC Increases the Risk of a HNPCC Increases the Risk of a Second CancerSecond Cancer

Features of HNPCCFeatures of HNPCC
SporadicSporadic
• Personal or family history of colorectal Personal or family history of colorectal or endometrial cancer before age 50or endometrial cancer before age 50
• Multiple cancers in an individualMultiple cancers in an individual• Multiple generations affectedMultiple generations affected• Other tumors associated with HNPCC: Other tumors associated with HNPCC:
ovarian, upper GI, renal pelvis, brainovarian, upper GI, renal pelvis, brain
HereditaryHereditary
• Family history of colorectal Family history of colorectal cancer but not other cancers cancer but not other cancers associated with HNPCCassociated with HNPCC
• Later age of onsetLater age of onset• No clear pattern on one side of No clear pattern on one side of
the family or the otherthe family or the other
CRC, 47CRC, 47
CRC, 42 & 51CRC, 42 & 51
Endo, 46Endo, 46CRC, 53CRC, 53
CRC, 71CRC, 71
CRC, 63CRC, 63

Identifying patients with HNPCCIdentifying patients with HNPCC
• Before genetic testing was available, HNPCC Before genetic testing was available, HNPCC was identified through defined criteria was identified through defined criteria (“Amsterdam criteria”).(“Amsterdam criteria”).
• 3 relatives with HNPCC-associated cancer3 relatives with HNPCC-associated cancer• one relative is a 1one relative is a 1stst-degree relative of the other two-degree relative of the other two• at least two successive generationsat least two successive generations• at least one diagnosed < 50 yrsat least one diagnosed < 50 yrs
• Many people with mutation-proven HNPCC Many people with mutation-proven HNPCC do do notnot meet these criteria. meet these criteria.
J Med GenetJ Med Genet 2000;37:641-5 2000;37:641-5

Laboratory Testing for HNPCCLaboratory Testing for HNPCC
• Clinical laboratory testing is availableClinical laboratory testing is available• Complete sequence analysis of the Complete sequence analysis of the MLH1MLH1 and and
MSH2MSH2 genes (the “gold standard”) genes (the “gold standard”)• Turnaround time of 3 weeksTurnaround time of 3 weeks
• Testing is available through health care providersTesting is available through health care providers
• For more informationFor more information• 800-469-7423 (Myriad Genetic Laboratories)800-469-7423 (Myriad Genetic Laboratories)• www.colaris-hnpcc.comwww.colaris-hnpcc.com

Microsatellite Instability (MSI)Microsatellite Instability (MSI)is a Feature of HNPCCis a Feature of HNPCC
• MSI is a DNA abnormality present in >90% of HNPCC-associated MSI is a DNA abnormality present in >90% of HNPCC-associated colorectal cancerscolorectal cancers
• MSI indicates an increased likelihood of HNPCCMSI indicates an increased likelihood of HNPCC• MSI is not diagnostic of HNPCC; also seen in 15% of sporadic colorectal cancersMSI is not diagnostic of HNPCC; also seen in 15% of sporadic colorectal cancers
• MSI analysis requires access to slides of archival paraffin-embedded MSI analysis requires access to slides of archival paraffin-embedded colorectal cancerscolorectal cancers
Nat MedNat Med 1996;2:169-74 1996;2:169-74

Overall ApproachOverall Approach
• Go directly to mutation testing if:Go directly to mutation testing if:– Amsterdam criteria +Amsterdam criteria +– Patient has two HNPCC tumorsPatient has two HNPCC tumors– CRC patient has FDR with HNPCC tumor, and one of CRC patient has FDR with HNPCC tumor, and one of
them diagnosed at age them diagnosed at age 50 years50 years– CRC CRC 50 years50 years
• Start with MSI if:Start with MSI if:– CRC patient has any FDR with HNPCC tumorCRC patient has any FDR with HNPCC tumor

The Importance of Genetic DiagnosisThe Importance of Genetic Diagnosis
5050
Pro
bab
ility
of
can
cer
(%)
Pro
bab
ility
of
can
cer
(%)
100100
Age (Years)Age (Years)3030 5050 7070
Family HistoryFamily History(without testing)(without testing)
With mutationWith mutation
Without mutationWithout mutation
Adapted with permission fromAdapted with permission from Ponder B: Genetic Testing for Cancer Risk.Ponder B: Genetic Testing for Cancer Risk. Science Science 1997; 278:1050-4 1997; 278:1050-4..Copyright 1997 American Association for the Advancement of ScienceCopyright 1997 American Association for the Advancement of Science
Each child of a carrier has a 50-50 chance of being at increased risk (or Each child of a carrier has a 50-50 chance of being at increased risk (or notnot).).

Managing the Cancer Risk of HNPCCManaging the Cancer Risk of HNPCC
•SurveillanceSurveillance– Colonoscopy every 1-3 years beginning age 20-25, annually after age Colonoscopy every 1-3 years beginning age 20-25, annually after age
4040– Annual transvaginal ultrasound and endometrial aspiration beginning Annual transvaginal ultrasound and endometrial aspiration beginning
age 25-35age 25-35
•SurgerySurgery– Subtotal colectomy for colorectal cancer or advanced adenomasSubtotal colectomy for colorectal cancer or advanced adenomas– Consideration of hysterectomy/salpingo-oophorectomy, especially at Consideration of hysterectomy/salpingo-oophorectomy, especially at
time of surgery for diagnosed colorectal cancertime of surgery for diagnosed colorectal cancer
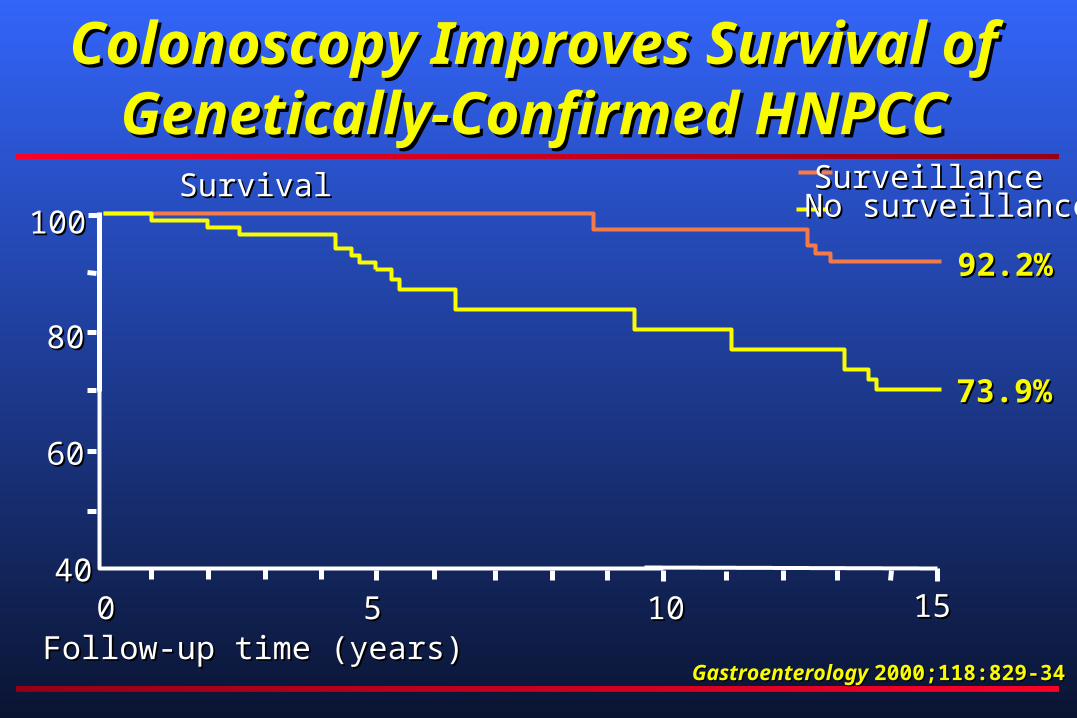
Colonoscopy Improves Survival of Colonoscopy Improves Survival of Genetically-Confirmed HNPCCGenetically-Confirmed HNPCC
Gastroenterology Gastroenterology 2000;118:829-342000;118:829-34
SurvivalSurvival
8080
6060
00 55 1010Follow-up time (years)Follow-up time (years)
4040
100100
1515
92.2%92.2%
SurveillanceSurveillance
73.9%73.9%
No surveillanceNo surveillance

Benefits and Limitations of Genetic Benefits and Limitations of Genetic Testing for HNPCCTesting for HNPCC
• BenefitsBenefits• Identification of HNPCC can lead to interventions that Identification of HNPCC can lead to interventions that
prevent cancer or detect it when it is still curable. prevent cancer or detect it when it is still curable. • Information for the health care of family membersInformation for the health care of family members• Results can alleviate uncertainty and anxietyResults can alleviate uncertainty and anxiety
• LimitationsLimitations• A negative result is most informative if there is a known A negative result is most informative if there is a known
mutation in the familymutation in the family• Some genetic variants are of unknown clinical significanceSome genetic variants are of unknown clinical significance

FAPFAP
•About 1 in 10,000 birthsAbout 1 in 10,000 births
•Autosomal dominantly inheritedAutosomal dominantly inherited
•100’s to 1000’s of colonic 100’s to 1000’s of colonic adenomatous polypsadenomatous polyps
•Average age of polyp occurrence, Average age of polyp occurrence, 16 years16 years



FAP, Colon CancerFAP, Colon Cancer
•Near 100% riskNear 100% risk
•Average age of diagnosis 39 yrsAverage age of diagnosis 39 yrs
•7% have colon cancer by age 21 7% have colon cancer by age 21
•93% have colon cancer by age 5093% have colon cancer by age 50
Other GI PolypsOther GI Polyps
• GastricGastric– At least 50% fundic gland polyps, rare cancerAt least 50% fundic gland polyps, rare cancer
• DuodenumDuodenum– >90% adenomatous polyps, 5%-10% cancer>90% adenomatous polyps, 5%-10% cancer
• Small bowelSmall bowel– About 50% adenomas, rare cancerAbout 50% adenomas, rare cancer

FAP, Extra-Colonic CancersFAP, Extra-Colonic Cancers
00.5
11.5
22.5
33.5
44.5
5
Per
i-am
pull
ary
Pan
crea
tic
Thy
roid
Gas
tric
CN
S
Hep
ato-
blas
tom
a
Life-time Life-time Risk(%)Risk(%)Life-time Life-time Risk(%)Risk(%)
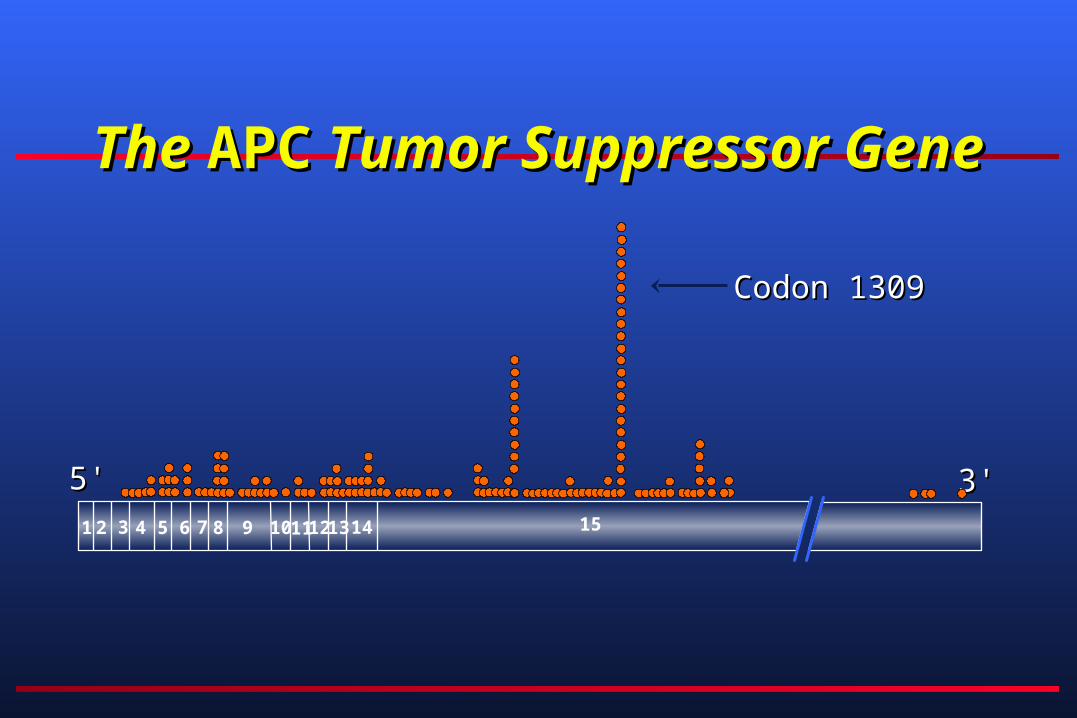
The The APCAPC Tumor Suppressor Gene Tumor Suppressor Gene
3'3'5'5'
Codon 1309Codon 1309
1 2 3 4 5 6 7 8 9 10111213 14 15
FAP, Genetic TestingFAP, Genetic Testing
• Methods used:Methods used:– Protein truncation testProtein truncation test– Sequencing, with SSCP or DGGESequencing, with SSCP or DGGE– LinkageLinkage
• Mutation finding is 80% to 90% Mutation finding is 80% to 90% successfulsuccessful
• Once mutation found, relatives tested Once mutation found, relatives tested with near 100% accuracywith near 100% accuracy

FAP, ManagementFAP, Management
•Genetic testingGenetic testing
•Colonic screeningColonic screening–Annual sigmoidoscopyAnnual sigmoidoscopy
–Start at age 10 to 12 yearsStart at age 10 to 12 years
–Colonoscopy for AAPCColonoscopy for AAPC
FAP, Extra-Colonic ScreeningFAP, Extra-Colonic Screening
• Duodenal: EGD every 1 to 3 yearsDuodenal: EGD every 1 to 3 years
• Pancreatic: ?Ultrasound, periodicPancreatic: ?Ultrasound, periodic
• Thyroid: Annual examThyroid: Annual exam
• Gastric: EGD every 1 to 3 yearsGastric: EGD every 1 to 3 years
• CNS: Annual H&PCNS: Annual H&P
• Liver: Ultrasound, AFP, annual <10 Liver: Ultrasound, AFP, annual <10 yearsyears

““Genetic Discrimination” in Health Genetic Discrimination” in Health Insurance is IllegalInsurance is Illegal
• Health Insurance Portability and Accountability Act Health Insurance Portability and Accountability Act (HIPAA)(HIPAA)– Prohibits group health insurance plans from discriminating on Prohibits group health insurance plans from discriminating on
the basis of genetic information.the basis of genetic information.
• Most states have enacted additional protectionsMost states have enacted additional protections
• Family members do not have to disclose whether Family members do not have to disclose whether a relative has undergone genetic testinga relative has undergone genetic testing
““Like so-called urban legends that are built on rumor rather than fact, the Like so-called urban legends that are built on rumor rather than fact, the perception of insurance company bias against patients who undergo predictive perception of insurance company bias against patients who undergo predictive genetic testing seems to be largely unsubstantiated.”- genetic testing seems to be largely unsubstantiated.”- JAMAJAMA 1999;282:2197-8, 1999;282:2197-8,