hepatology referral pathways for gps - wordpress.com
TRANSCRIPT

Hepatology
Division C
Cambridge University Hospitals NHS Foundation Trust Page 1 of 11
Hepatology referral pathways for GPs Version 14; Approved November 2020
Hepatology referral pathways for GPs
1 Scope
For use within hepatology
Contents 2. Liver blood tests and what they mean p2
Acute and chronic liver screen p2
3. Hepatology A&G FAQs p3
Common reasons for referral
4. Raised ALT +/- GGT p4
5. Non alcoholic fatty liver disease (NAFLD) pathway p5
6. Alcohol-related liver disease (ArLD) pathway p6
7. Isolated asymptomatic raised bilirubin p7
8. Raised ALP and normal ALT p7
9. Combination of LFT abnormalities p8
10. Raised ferritin p8
11. Abnormal liver imaging p9
12. Hepatitis B p10
13. Hepatitis C p10
14. Referral pathways p11

Hepatology
Division C
Cambridge University Hospitals NHS Foundation Trust Page 2 of 11
Hepatology referral pathways for GPs Version 14; Approved November 2020
2 Liver blood tests and what they mean
Test Normal range
What does it mean? Actions if abnormal
ALT 7-40 Hepatocellular injury
Raised ALT
Bilirubin isolated raised Bilirubin with abnormal LFT
<21 Gilberts Haemolysis Liver or biliary pathology
Isolated asymptomatic raised bilirubin Refer (routine vs urgent acc to values)
Alkaline Phosphatase (ALP)
30-130 Biliary disease (if raised GGT) Bone disease Pregnancy (placenta) Acute phase response
Raised ALP and normal ALT
Gamma glutamyl transferase (GGT)
Male 0-73 Female 0-38
Non-specific – can reflect alcohol intake, non-alcoholic fatty liver or biliary disease if associated with raised ALP
Follow relevant pathway
Prothrombin time (PT) Elevated with impaired synthetic function or biliary obstruction
Refer if could be liver related
Albumin 35-50 Non-specific, but may represent impaired synthetic function if low
Refer if could be liver related
Ferritin Not necessarily iron overload Raised ferritin
Reduced platelets Can be a feature of cirrhosis with portal hypertension
Refer if could be liver related
Chronic liver screen U/E, LFT, FBC, PT, FIB-4 if suspected NAFLD Hepatitis B & C serology Liver autoantibodies Serum immunoglobulins Ferritin Alpha-1 antitrypsin level Random glucose, HBA1c, lipids if ?NAFLD If under 50 caeruloplasmin
Acute liver screen LFT, FBC, PT Hepatitis A, hepatitis B and hepatitis E serology (IgM & IgG), EBV and CMV Liver autoantibodies Serum immunoglobulins If under 50 caeruloplasmin
Hepatitis B screen Chronic liver screen plus: HBV DNA Hepatitis A IgG HIV screen
Hepatitis C screen Chronic liver screen plus: HCV RNA and genotype Hepatitis A IgG HIV screen

Hepatology
Division C
Cambridge University Hospitals NHS Foundation Trust Page 3 of 11
Hepatology referral pathways for GPs Version 14; Approved November 2020
3 Hepatology A&G FAQs
Result What it means
BLOOD
ALP raised with normal GGT
Not likely to relate to liver, more likely bony origin
Bilirubin (isolated raised ) Likely Gilbert’s if nil else to suggest liver disease, normal Hb, ‘split’ bilirubin predominantly unconjugated. NB may have family history
Caeruloplasmin 0.17-2.0 Unlikely to be significant if no other pointers to Wilson’s disease
Ferritin raised/normal tf sat
Common in NAFLD, Alcohol-related liver disease (ArLD)
FIB4 <1.3 (<2.0 over age 65)
Can be requested on T-Quest. Use for NAFLD assessment only. Means low risk of significant fibrosis. Not valid < age 35 or > age 75
FibroScan < 7 kPa (NAFLD)
Means low risk of significant fibrosis in NAFLD
FibroScan < 8 kPa (Alcohol)
Means low risk of significant fibrosis in Alcohol-related liver disease
Hepatitis C Ab positive Past exposure - requires HCV RNA to assess for active infection
HepBcAb +ve /HepBsAg –ve
Previous exposure, natural immunity, not chronic infection
IgA raised Common in NAFLD, ArLD – not concerning in itself
SmA/ANA Weak positive This will always be non-specific, common in NAFLD. Not a concern if IgG normal.
IMAGING
Focal lesion on US If likely benign but report not definitive – repeat at CUH if done elsewhere otherwise A&G
Gallbladder polyps Refer to ‘HPB surgery’ for advice/ follow their guidance

Hepatology
Division C
Cambridge University Hospitals NHS Foundation Trust Page 4 of 11
Hepatology referral pathways for GPs Version 14; Approved November 2020
4 Isolated raised ALT (+/- GGT)
Reinforce lifestyle advice/ monitor
Alcohol related liver disease pathway
YES
NO
ALT <150
ALT >300 at any stage Acute liver screen , urgent CUH USS
ALT normal
ALT >150
Repeat 2/52
ALT <150 Repeat
4/52
ALT remains >150 USS and Chronic liver screen
USS and Chronic liver screen
Do all the features below apply?
NO hepatomegaly/splenomegaly NO cirrhosis/portal hypertension
Normal chronic liver screen
Routine referral
Features of significant liver disease at any stage (eg possible cirrhotic appearance, splenomegaly, raised
bilirubin/PT, low platelets)
Routine referral
THINK about and address Risk Factors
• Metabolic syndrome • Diabetes • Alcohol • Risks for viral hepatitis (ethnicity, IV drug use) • Medication • Vigorous exercise (check CK)
> 14 units alcohol per week NAFLD pathway
NO
YES
Routine referral
Urgent referral

Hepatology
Division C
Cambridge University Hospitals NHS Foundation Trust Page 5 of 11
Hepatology referral pathways for GPs Version 14; Approved November 2020
5 Non Alcoholic Fatty liver Disease (NAFLD) pathway
From Pathway 4 (raised ALT +/- GGT) OR Type 2 diabetic or morbid obesity with BMI >35 kg/m2 (often with isolated elevated
GGT)
Age <35 or >75 with no significant comorbidities
Age 35 to 75
Intermediate Risk Intermediate values
High Risk > 2.67
RISK Stratification with FIB-4 to assess risk of significant fibrosis (available on T-QUEST)
Low Risk < 1.3 (age 35-64) < 2.0 (age ≥65)
Lifestyle advice Re-stratify in 2 years
FIBROSCAN REFERRAL
Unless BMI >40 when
for ROUTINE REFERRAL
If BMI <40 otherwise routine referral
NO
Hepatology will arrange a clinic
appointment
YES
Score ≥ 8 kPa

Hepatology
Division C
Cambridge University Hospitals NHS Foundation Trust Page 6 of 11
Hepatology referral pathways for GPs Version 14; Approved November 2020
6 Alcohol-related Liver Disease (ArLD) pathway
Reinforce lifestyle advice for
heavy alcohol intake
metabolic syndrome
Score ≥ 8 kPa:
Lifestyle advice for heavy alcohol intake and metabolic syndrome
Dependent drinkers should seek advice from CGL FIBROSCAN REFERRAL
From Pathway 4 (raised ALT +/- GGT)
Repeat FibroScan 3-5 years according to lifestyle success/LFTs
Repeat fibroscan 3-5 years according to lifestyle success/LFTs
Repeat fibroscan 3-5 years according to lifestyle success/LFTs
Repeat fibroscan 3-5 years according to lifestyle success/LFTs
Score < 8 kPa:
Hepatology will arrange a clinic
appointment

Hepatology
Division C
Cambridge University Hospitals NHS Foundation Trust Page 7 of 11
Hepatology referral pathways for GPs Version 14; Approved November 2020
7 Isolated asymptomatic raised bilirubin
8 Raised ALP and normal ALT
Ultrasound
Chronic liver screen
ROUTINE REFERRAL
YES
YES
Haemolysis screen: reticulocytes
lactate dehydrogenase (LDH) haptoglobin level
Direct Antiglobulin Test (DAT)
Blood film
+/- refer haematology
NO
YES
NO
NO
YES
NO Predominantly unconjugated hyperbilirubinemia,
normal albumin and platelet count
Anaemia?
Likely Gilbert’s syndrome (inherited defect in ability to conjugate bilirubin that is benign and requires reassurance and no
follow up)
Split bilirubin and FBC
Bilirubin > 2x ULN URGENT/2WW
REFERRAL
Check GGT Is it raised? ROUTINE
REFERRAL
Tests for bone pathologies Consider bone profile, vitamin D, ESR/CRP
PSA, PTH, myeloma screen
Ultrasound
Chronic liver screen

Hepatology
Division C
Cambridge University Hospitals NHS Foundation Trust Page 8 of 11
Hepatology referral pathways for GPs Version 14; Approved November 2020
9 Combination of LFT abnormalities
10 Raised ferritin
Bilirubin > 2x upper limit normal
(not isolated)
URGENT/2WW
REFERRAL
ALT >300 and/or ALP > 500 URGENT REFERRAL
Other USS
Chronic Liver screen ROUTINE
REFERRAL
If CRP elevated – exclude inflammatory cause / repeat after interval. Exclude anaemia (haem ref)
Check fasting transferrin saturation (tf sat) and LFTs / family history
Low/normal tf sat +/- raised ALT Borderline/raised tf sat or family history
HFE genotyping (EDTA to Molecular Genetics for simple
HFE1 genotype – see form at end of document or click here)
Consider: NAFLD pathway ArLD pathway
Lifestyle advice
Refer if not improving or
>1000 mcg/l
Refer to Bill Griffiths, Consultant Hepatologist
through CAS

Hepatology
Division C
Cambridge University Hospitals NHS Foundation Trust Page 9 of 11
Hepatology referral pathways for GPs Version 14; Approved November 2020
11 Abnormal liver imaging
Hepatomegaly Chronic liver screen ROUTINE REFERRAL
Cyst/s
Simple cyst/s No referral required unless >10
(?polycystic liver disease)
Complicated cysts thick-walled /septated
US CUH → A&G referral US not CUH → rpt US CUH
Suspected haemangioma
Small (< 2cm) incidental haemangioma No referral required
Large (> 2 cm)/complex/complicated
US CUH → A&G referral US not CUH → rpt US CUH
Focal fat sparing on background of “fatty liver” NAFLD/fibroscan pathways
Suspected cancer 2WW referral
Ultrasound scan shows gall bladder polyp(s)
Referral to HPB surgery

Hepatology
Division C
Cambridge University Hospitals NHS Foundation Trust Page 10 of 11
Hepatology referral pathways for GPs Version 14; Approved November 2020
12 Hepatitis B
13 Hepatitis C
* Pre-clinic workup: (see T-Quest Groups) For HBV and HCV: Chronic liver screen plus HIV and hepatitis A immunity serology For HCV: HCV RNA and genotype (large EDTA tube) For HBV: HBV DNA (large EDTA tube)
Refer to hepatitis clinic for assessment of the need for treatment, contact tracing and
cancer surveillance *
Exposed to and cleared hepatitis B. Contact tracing with GP.
Referral only required if patient takes immunosuppression or chemotherapy (or
does so in the future)
Hepatitis B surface antigen (HBsAg) positive
Hepatitis B core antibody (anti-HBcAb) positive
Hepatitis B surface antigen (HBsAg) negative
Hepatitis C antibody positive
+ve -ve
Exposure and clearance Contact tracing
Confirm with repeat HCV RNA and if negative no further action required.
Refer to hepatitis clinic for highly effective treatment, contact tracing and
cancer surveillance *
HCV RNA test (large EDTA)
Hepatology
Division C
Cambridge University Hospitals NHS Foundation Trust Page 11 of 11
Hepatology referral pathways for GPs Version 14; Approved November 2020
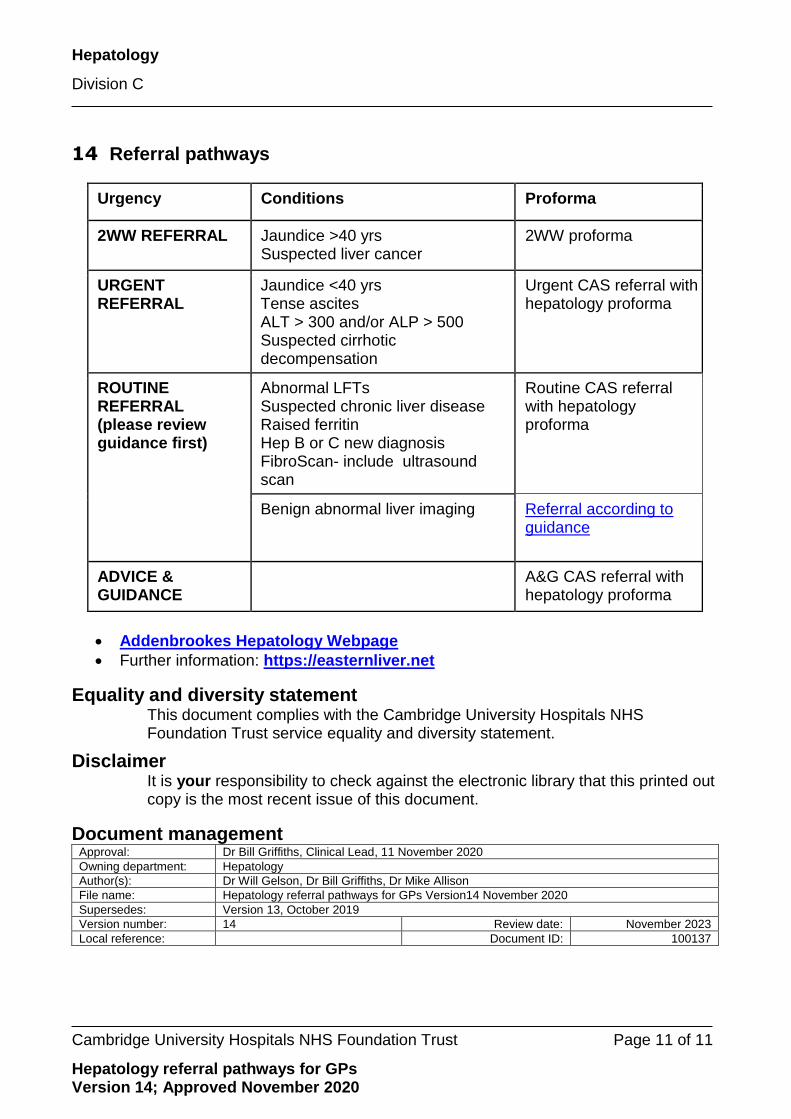
14 Referral pathways
Urgency Conditions Proforma
2WW REFERRAL
Jaundice >40 yrs Suspected liver cancer
2WW proforma
URGENT REFERRAL
Jaundice <40 yrs Tense ascites ALT > 300 and/or ALP > 500 Suspected cirrhotic decompensation
Urgent CAS referral with hepatology proforma
ROUTINE REFERRAL (please review guidance first)
Abnormal LFTs Suspected chronic liver disease Raised ferritin Hep B or C new diagnosis FibroScan- include ultrasound scan
Routine CAS referral with hepatology proforma
Benign abnormal liver imaging Referral according to guidance
ADVICE & GUIDANCE
A&G CAS referral with hepatology proforma
Addenbrookes Hepatology Webpage
Further information: https://easternliver.net
Equality and diversity statement This document complies with the Cambridge University Hospitals NHS Foundation Trust service equality and diversity statement.
Disclaimer It is your responsibility to check against the electronic library that this printed out copy is the most recent issue of this document.
Document management Approval: Dr Bill Griffiths, Clinical Lead, 11 November 2020
Owning department: Hepatology
Author(s): Dr Will Gelson, Dr Bill Griffiths, Dr Mike Allison
File name: Hepatology referral pathways for GPs Version14 November 2020
Supersedes: Version 13, October 2019
Version number: 14 Review date: November 2023
Local reference: Document ID: 100137

REGIONAL GENETICS LABORATORIES TEST REQUEST All tests requested will be reviewed against departmental criteria. If testing is not arranged, the samples will be stored and the referring clinicians informed. After testing, samples may be used anonymously for the development of new tests and for quality monitoring.
Venous blood samples: Adult: 5ml; Children: 1-5ml
☐ DNA test: EDTA tube
☐ Chromosomes: Lithium Heparin tube
☐ Microarray: Lithium Heparin and EDTA tubes
Other samples:
☐ Cord/Placenta/insertion site/skin
☐ Products of Conception (whole specimen in sterile pot)
☐ Amniotic Fluid
☐ CVS
☐ Other (please contact the laboratory)
Sample obtained by (Signature)……………………………
Printed Name ……………………………………………..
Date………………………………………………………….
Clinical Synopsis Please provide clinical synopsis and pedigree with relevant family history to help the team generate a laboratory
report Tests Required:
Storage Only (no testing at this time): ☐
Gestation in weeks (If pregnant): Partners Name and DOB: Index Case (if not this patient):
The Laboratory does NOT report results via the telephone
Surname Date of Birth Age at Presentation
First Names Sex
NHS Number
Ethnicity
Hospital Number Family Number
Home Address Postcode Patient email address
GP Name (Printed) GP Address Postcode GP email address (nhs.net preferred)
Consultant (PRINT) Hospital
Speciality/Dept/Ward Contact telephone number Email address (nhs.net preferred)
Results to (if different from above) inc email address (nhs.net preferred)
Billing to:
Private Patient: ☐
In Submitting this sample, the clinician confirms that consent has been obtained for:
a) Testing and Storage
☐ Yes ☐No
b) The use of this sample and the information generated from it to be shared with members of the patient’s family and their health professionals (if appropriate)
☐Yes ☐No

All samples MUST be labelled with FULL name, date of birth and NHS number Processing of samples will be delayed if information is incomplete
Send samples at room temperature by 1st
class post or courier to:
East Anglian Medical Genetics Service, Genetics Laboratories, Box 143
ATC Level 6, Addenbrooke’s Hospital, Hills Road, Cambridge, CB2 0QQ
CUH Laboratory Use Only:
Receipt date and time:
Tube type: Volume:
No of tubes:
Shire Only ☐
Patient Demographics Checked:
Other Information:
Send out approved by:………………………………….. Signature:…………………………………………………
Date:……………………………………………………
Laboratory opening hours: 8.30am - 5.30pm Monday to Friday
Telephone: 01223 348866 Fax: 01223 348712
E-mail: [email protected]
For further information about sample requirements and tests available see: www.cuh.org.uk/genetics-labs Indication for Genetic Testing:
1. To establish a diagnosis ☐
2. Guide clinical management ☐
3. Information regarding prognosis/recurrence risk ☐
4. Predictive testing ☐
5. PGD/Prenatal diagnosis ☐
Has the test been discussed at a clinical meeting? If so, please provide information on clinical meeting (I.e.: Neurology meeting, cancer meeting)
☐
Is the test urgent? (i.e. pregnant or will alter management)
☐
Please confirm that your department will fund the test* Has the test been approved by patient’s consultant
☐
☐
* Please see UKGTN website (http://ukgtn.nhs.uk/) for approximate cost or contact the duty scientist (tel: 01223 348866)