hepatocellular carcinoma and liver transplantation tts key opinion leaders meeting montreal, april...
TRANSCRIPT

Hepatocellular Hepatocellular Carcinoma and Liver Carcinoma and Liver TransplantationTransplantation
TTS Key Opinion Leaders TTS Key Opinion Leaders MeetingMeetingMontreal, April 2007Montreal, April 2007
Mazen Hassanain MBBS, FRCS(C)Mazen Hassanain MBBS, FRCS(C)Assistant Professor of SurgeryAssistant Professor of SurgeryMcGill University Health CentreMcGill University Health Centre


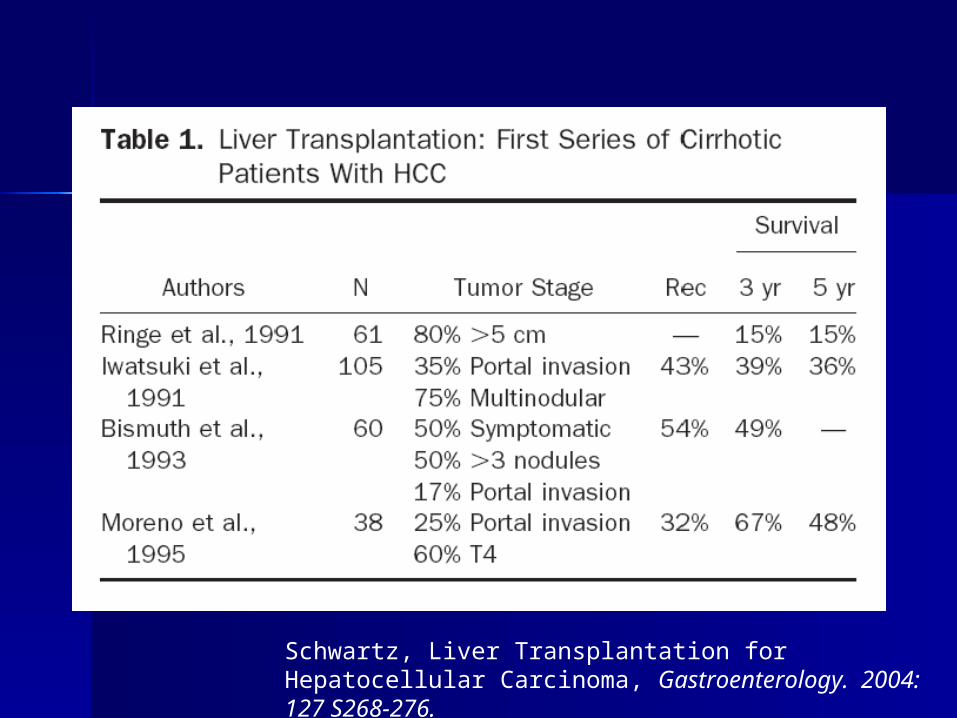
Schwartz, Liver Transplantation for Hepatocellular Carcinoma, Gastroenterology. 2004: 127 S268-276.

Schwartz, Liver Transplantation for Hepatocellular Carcinoma, Gastroenterology. 2004: 127 S268-276.

Improving survival Improving survival over timeover time
Yoo et al. Journal of Clinical Oncology. 2003: 21 4329-4335.

Milan CriteriaMilan Criteria
Mazzafero 1996Mazzafero 1996 Single tumour less than 5 cmSingle tumour less than 5 cm Up to three tumour nodules each Up to three tumour nodules each
3cm or less3cm or less
Mazzaferro, et.al. NEJM1996;334:693-699

Milan CriteriaMilan Criteria
Regalia et al. Liver Transplantation for small hepatocellular carcinoma in cirrhosis: analysis of our experience. Transplantation Proceedings, 33, 1442–1444 (2001)

UCSF CriteriaUCSF Criteria
Patients with HCC meeting the following criteria: – Solitary tumor < 6.5 cm, – or < 3 nodules with the largest
lesion < 4.5 cm – and total tumor diameter < 8 cm
Yao et al. Liver transplantation for hepatocellular carcinoma: expansion of the tumor size limits does not adversely impact survival. Hepatology. 2001 33:1394

UCSF criteriaUCSF criteria
Yao et al. Liver Transplantation. 2002: 8(9) 765-774

UCSF vs MilanUCSF vs Milan
Schwartz, Liver Transplantation for Hepatocellular Carcinoma, Gastroenterology. 2004: 127 S268-276.

Vascular InvasionVascular Invasion
Khakhar et al. Survival after Liver Transplantation for Hepatocellular Carcinoma. Transplantation Proceedings. 2003: 35 2438-2441

Vascular InvasionVascular Invasion
Hemming et al. Liver Transplantation for Hepatocellular Carcinoma. Annals of Surgery. 2001: 233(5) 652-659

Vascular InvasionVascular Invasion
Jonas et al. Vascular invasion and histologic grading determine outcome after liver transplantation for hepatocellular carcinoma in cirrhosis. Hepatology 2001;33:1080-1086.

Histologic GradeHistologic Grade
Jonas et al. Vascular invasion and histologic grading determine outcome after liver transplantation for hepatocellular carcinoma in cirrhosis. Hepatology 2001;33:1080-1086.
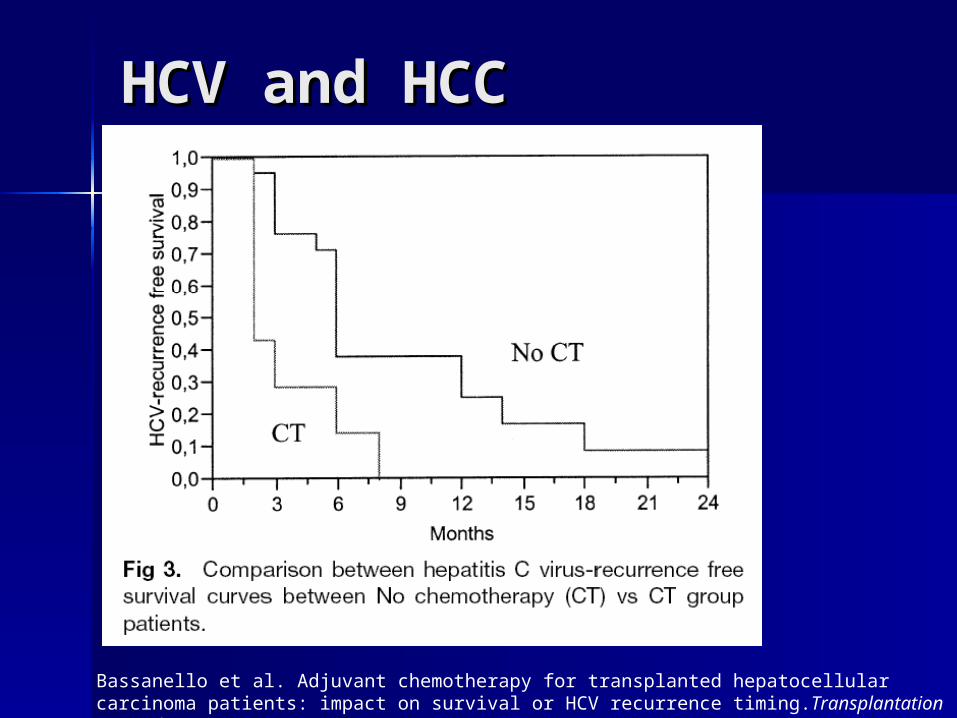
HCV and HCCHCV and HCC
Bassanello et al. Adjuvant chemotherapy for transplanted hepatocellular carcinoma patients: impact on survival or HCV recurrence timing.Transplantation Proceedings. 2003: 35 2991-2994

McGill ProtocolMcGill Protocol
Tumours exceeding Milan criteriaTumours exceeding Milan criteria Receive 3 TACE treatments at 6 Receive 3 TACE treatments at 6
week intervalsweek intervals Lipiodol,carboplatinum, gelfoamLipiodol,carboplatinum, gelfoam If patients respond (AFP decreases If patients respond (AFP decreases
or tumours shrink, then go on to or tumours shrink, then go on to Tx, otherwise continue care)Tx, otherwise continue care)

McGill ExperienceMcGill Experience
January 1992 to December 2005January 1992 to December 2005 496 OLTx496 OLTx 1/3 for HCV1/3 for HCV 99 for HCC99 for HCC 33 outside Milan criteria33 outside Milan criteria

McGill ExperienceMcGill Experience
0.00
0.25
0.50
0.75
1.00
0 1 2 3 4 5Time (years)
No HCC HCC
HCC vs No HCCOverall Patient Survival

McGill ExperienceMcGill Experience
0.00
0.25
0.50
0.75
1.00
0 1 2 3 4 5Time (years)
No HCC Milan HCC
No HCC vs Milan HCCSurvival of Patients with Milan HCC
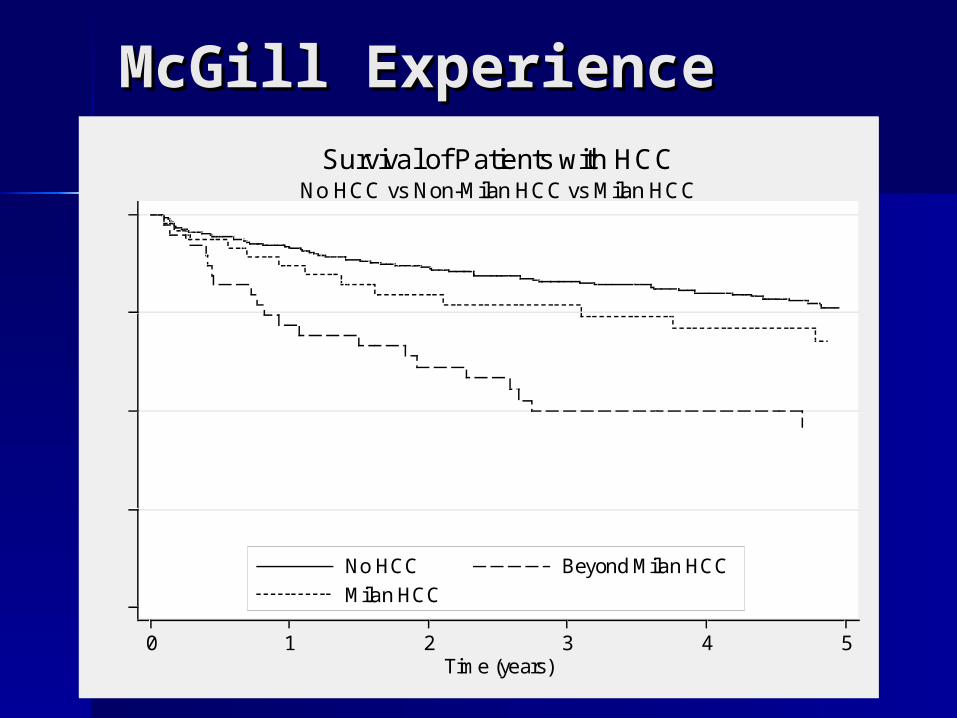
McGill ExperienceMcGill Experience
0.00
0.25
0.50
0.75
1.00
0 1 2 3 4 5Time (years)
No HCC Beyond Milan HCC
Milan HCC
No HCC vs Non-Milan HCC vs Milan HCCSurvival of Patients with HCC
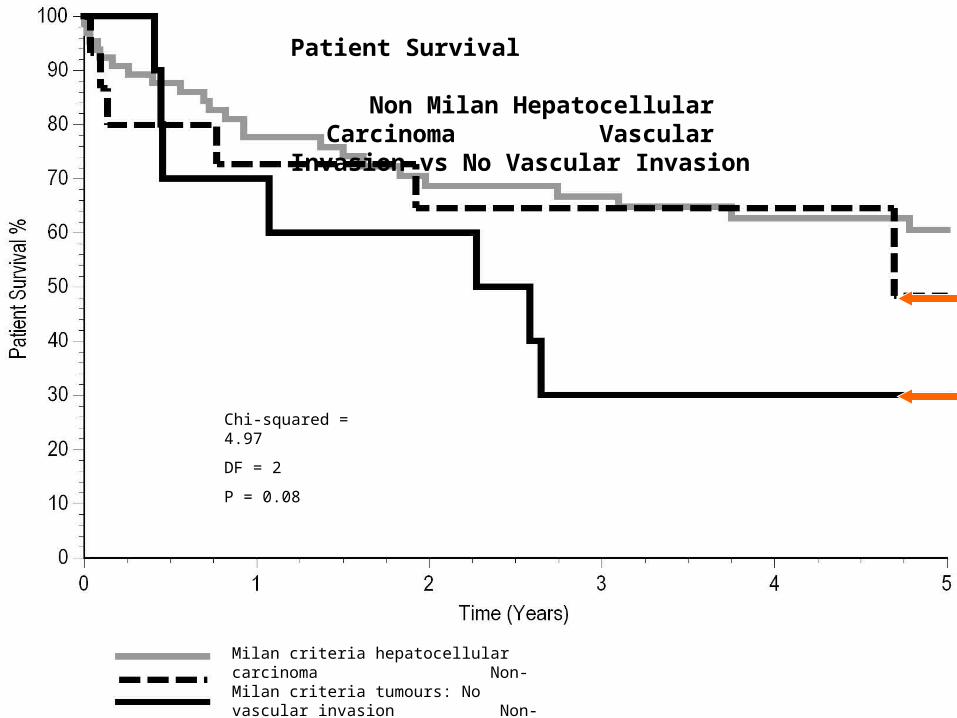
No hepatocellular carcinomaMilan criteria hepatocellular carcinoma Non-Milan criteria tumours: No vascular invasion Non-Milan criteria tumours: Vascular invasion
Chi-squared = 4.97
DF = 2
P = 0.08
Patient Survival Non Milan Hepatocellular
Carcinoma Vascular Invasion vs No Vascular Invasion

Dead with Recurrence
Alive with Recurrence
Rising Serum FP during TACE
Log scale of -FP values(ng/ml)
Initiation of TACE sessions
1
10
100
1000
10000
1 2 3 4 5 6 7
1
10
100
1000
10000
1 2 3 4 5 6 7 8 9 10
Log scale of-FP values(ng/ml)
Initiation of TACE sessions
Recurrence-free alive
Recurrence-free deadOLTOLT or
Drop-off
Declining Serum FP during TACE
A B
Duration of TACE Treatments Duration of TACE Treatments
Non Milan Hepatocellular Carcinoma

-10
-5
0
5
10
15
Pre-TACE αFP Post-TACE αFP Pre-TACE αFP Post-TACE αFP
No vascular invasion Vascular invasion
Slope -1
Non Milan Tumours receiving TACELinear regression based on 4 or more alpha fetoprotein levels
pre-transplantation
P = 0.008 (95%CI -9.1 to -1.6)
Linear regression slope
ConclusionsConclusions
Changes in AFP following TACE predicted who would have vascular invasion on explant histology and which patients would have recurrent disease post-transplantation.
AFP levels >64ng/ml pre-TACE were more likely to be associated with vascular invasion.
When the AFP level was > 10ng/ml pre-TACE, a positive AFP slope following TACE predicted vascular invasion (p<0.01).

Live donor liver Live donor liver transplant (LDLT)transplant (LDLT)
Initial experience in LDLT for HCC Initial experience in LDLT for HCC very promising.very promising.
Survival comparable to DDLTSurvival comparable to DDLT
Schwartz et al. Adult living donor liver transplantation for patients with hepatocellular carcinoma. Annals of Surgery2004:239(2) 142-9
Lo et al. The role and limitations of living donor liver transplantation for hepatocellular carcinoma. Liver Transplantation. 2004;10:440-7
Northwestern group experienceNorthwestern group experience– Stage for stage higher recurrence Stage for stage higher recurrence
rate after LDLTrate after LDLT
Live donor liver Live donor liver transplant (LDLT)transplant (LDLT)
Kulik and Abecassis. Living donor liver Kulik and Abecassis. Living donor liver transplantation for hepatocellular carcinoma. transplantation for hepatocellular carcinoma. Gastroenterology.Gastroenterology. 2004;127:S277. 2004;127:S277.
Axelrod et al. Living donor liver transplant for Axelrod et al. Living donor liver transplant for malignancy. malignancy. Transplantation. Transplantation. 2005;79(3):363-6 2005;79(3):363-6

A2ALL dataA2ALL data Confirms higher stage for stage Confirms higher stage for stage
recurrence rate.recurrence rate.
Higher recurrence rate recently also Higher recurrence rate recently also confirmed by Hong Kong groupconfirmed by Hong Kong group
Live donor liver Live donor liver transplant (LDLT)transplant (LDLT)
A2ALL Study Group. A comparison of adult iving donor A2ALL Study Group. A comparison of adult iving donor (LDLT) to deceased donor liver transplant (DDLT) for (LDLT) to deceased donor liver transplant (DDLT) for hepatocellular carcinoma: data from the A2ALL study. hepatocellular carcinoma: data from the A2ALL study. HepatologyHepatology. 2005;42(4) 199a (AASLD abstract). 2005;42(4) 199a (AASLD abstract)
A2ALL Study Group. Personal communication.A2ALL Study Group. Personal communication.
Wong et al. Living donor versus deceased donor liver transplantation for early irresectable hepatocellular carcinoma. British Journal of Surgery 1007; 94:78-86.
““Fast-tracking”Fast-tracking” RegenerationRegeneration Surgical techniqueSurgical technique
Live donor liver Live donor liver transplant (LDLT)transplant (LDLT)

1818FDG-PETFDG-PET
PET not widely used for HCC PET not widely used for HCC – AvailabilityAvailability– Relatively high false negative rateRelatively high false negative rate
Early data suggested that Early data suggested that visualization varied with degree visualization varied with degree of differentiation.of differentiation.

1818FDG-PETFDG-PET
Korean study of Korean study of 1818FDG-PET in HCCFDG-PET in HCC PET positive tumours significantly PET positive tumours significantly
moremore– Vascular invasionVascular invasion– Higher grade (II, IV)Higher grade (II, IV)– AFP >200ng/mLAFP >200ng/mL
No association with No association with – Size or number of tumoursSize or number of tumours
Yang et al. The role of 18-F FDG-PET Imaging for the Selection of Liver Transplantation candidates among Hepatocellular Carcinoma Patients. Liver Transplantation. 2006, 12 1655-1660.

1818FDG-PETFDG-PET
TACETACE
TACE improves survival of unresectable TACE improves survival of unresectable HCCHCC
– Llovet et al. Systematic review of randomized trials Llovet et al. Systematic review of randomized trials for unresectable hepatocellular carcinoma: for unresectable hepatocellular carcinoma: chemoembolization improves survival. chemoembolization improves survival. HepatlogyHepatlogy 2003; 37:429-4422003; 37:429-442
Improved long-term survival for T2-T3 Improved long-term survival for T2-T3 HCC when used pre-TxHCC when used pre-Tx
– Yao et al. The Impact of Pre-Operative Loco-Regional Yao et al. The Impact of Pre-Operative Loco-Regional Therapy on Outcome after Liver Transplantation for Therapy on Outcome after Liver Transplantation for Hepatocellular Carcinoma. Hepatocellular Carcinoma. American Journal of American Journal of Transplantation.Transplantation. 2005;5:795-804. 2005;5:795-804.

TACETACE
Despite widespread use of TACE Despite widespread use of TACE as a bridge to transplantation as a bridge to transplantation data is meagerdata is meager
Recent systematic review showed Recent systematic review showed no survival benefit and minimal no survival benefit and minimal wait list benefit.wait list benefit.
Clavien et al. Transarterial chemoembolization as a bridge to liver transplantation for hepatocellular ccarcinoma: an evidence-based analysis. American Journal of Transplantation. 2006: 6:2644

Future directionsFuture directions
Better patient selection!!Better patient selection!! Criteria that are more flexible Criteria that are more flexible
than Milan/UCSFthan Milan/UCSF Criteria that are better surrogates Criteria that are better surrogates
for vascular invasionfor vascular invasion– Potential role for pre-operative Potential role for pre-operative
biopsybiopsy Adjuvant treatment for HCVAdjuvant treatment for HCV

1818FDG-PET and histologic data FDG-PET and histologic data need prospective correlationneed prospective correlation
Role of LDLT and criteria for Role of LDLT and criteria for selection need to be definedselection need to be defined
Prospective definition/evaluation Prospective definition/evaluation of pre-transplant therapiesof pre-transplant therapies– TACE, RFA, Theraspheres and/or TACE, RFA, Theraspheres and/or
combinations of thesecombinations of these

AcknowledgementsAcknowledgements
Peter MetrakosPeter Metrakos Jeffery BarkunJeffery Barkun Jean TchervenkovJean Tchervenkov Steve ParaskevasSteve Paraskevas Michael AbecassisMichael Abecassis Laura KulikLaura Kulik Alan KoffronAlan Koffron Peter HortonPeter Horton John MartinieJohn Martinie George TzimasGeorge Tzimas
Myriam FernandezMyriam Fernandez MUHC Transplant MUHC Transplant
TeamTeam

Montreal Hepatoma Treatment AlgorithmMontreal Hepatoma Treatment Algorithm
Resection Transplant PEI/RFA/RTx TACE Therasphere New AgentsSymptomatic
Tx
HCC
Stage APST 0, CTP A, Okuda 1
Very earlySingle < 2 cm
Portal Press/Bili
Normal
3 nodules< 3 cm
Associated disease
increased
no yes
Stage B,C,DPST 0-2, CTP A-B, Okuda 1-2
Early stage BSingle < 5 cm, PST 0
Intermediate stage CMulti-nodules, PST 0
CTP A CTP B
Decreasing a-FP
Advanced Stage DPortal Vein invasion,N1,M1, PST 1-2
Portal vein invasion,N1, M1
No
Yes
Stage EPST>2,CTP C,Okuda 3
Terminal Stage D
