hepatitis b: impeding liver cancer through prevention and management hepatitis b: impeding liver...
Post on 18-Dec-2015
217 views
TRANSCRIPT
Hepatitis B: Impeding Liver Hepatitis B: Impeding Liver
Cancer through Prevention and Cancer through Prevention and ManagementManagement
Raymond S. Koff, M.D.Raymond S. Koff, M.D.Clinical Professor of MedicineClinical Professor of Medicine
University of Connecticut University of Connecticut Health Science CenterHealth Science Center
Farmington, ConnecticutFarmington, Connecticut
Raymond S. Koff, M.D.Raymond S. Koff, M.D.Clinical Professor of MedicineClinical Professor of Medicine
University of Connecticut University of Connecticut Health Science CenterHealth Science Center
Farmington, ConnecticutFarmington, Connecticut
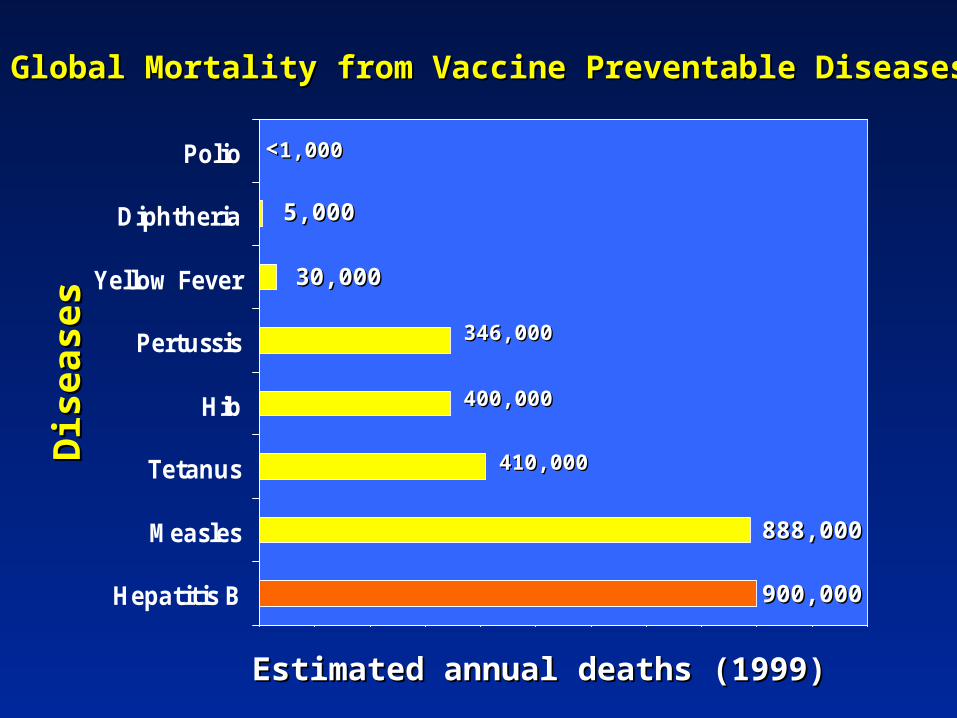
Hepatitis B
Measles
Tetanus
Hib
Pertussis
Yellow Fever
Diphtheria
Polio
900,000900,000
888,000888,000
410,000410,000
346,00346,0000
30,00030,000
400,00400,0000
5,005,0000
<<1,001,0000
Global Mortality from Vaccine Preventable DiseasesGlobal Mortality from Vaccine Preventable DiseasesD
i seases
Di s
eases
Estimated annual deaths (1999)Estimated annual deaths (1999)
Hepatocellular CarcinomaHepatocellular Carcinoma
● Among solid tumors, 5th highest incidence worldwide and 3rd most common cause of cancer deaths
● In the U.S. in 2007, 13th most common cancer and increasing faster than all others from 1995 to 2004; 8th most common cause of cancer deaths
● Despite advancing technology and available treatments, 5-year survival rates are generally less than 5%
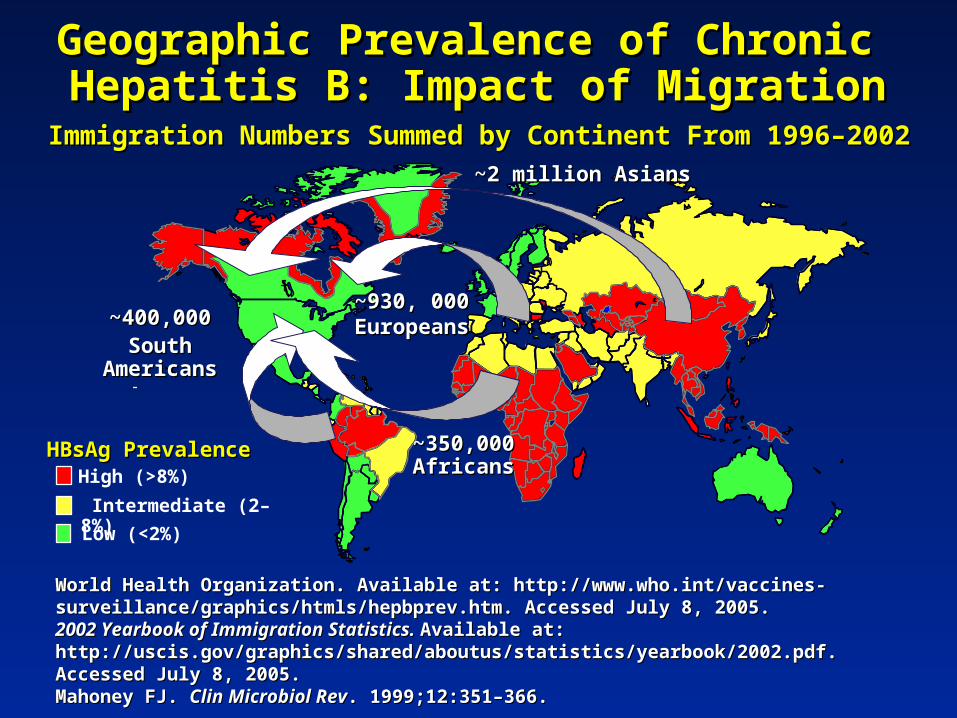
Geographic Prevalence of Chronic Geographic Prevalence of Chronic Hepatitis B: Impact of MigrationHepatitis B: Impact of Migration
World Health Organization. Available at: World Health Organization. Available at: http://www.who.int/vaccines-surveillance/graphics/htmls/hepbprev.htm. Accessed July 8, http://www.who.int/vaccines-surveillance/graphics/htmls/hepbprev.htm. Accessed July 8, 2005.2005.2002 Yearbook of Immigration Statistics. 2002 Yearbook of Immigration Statistics. Available at:Available at: http://uscis.gov/graphics/shared/aboutus/statistics/yearbook/2002.pdf. Accessed July 8, 2005.http://uscis.gov/graphics/shared/aboutus/statistics/yearbook/2002.pdf. Accessed July 8, 2005.Mahoney FJ. Mahoney FJ. Clin Microbiol RevClin Microbiol Rev. 1999;12:351–366.. 1999;12:351–366.
Immigration Numbers Summed by Continent From 1996–2002Immigration Numbers Summed by Continent From 1996–2002
HBsAg PrevalenceHBsAg PrevalenceHigh (>8%)
Intermediate (2–8%)
Low (<2%)
~2 million Asians~2 million Asians
~400,000~400,000South AmericansSouth Americans
~350,000 ~350,000 AfricansAfricans
~930, 000 ~930, 000 EuropeansEuropeans

Chronic Hepatitis Chronic Hepatitis B B
Morbidity and Mortality, U.S. Morbidity and Mortality, U.S.
Previously infected individuals: ~10 millionPreviously infected individuals: ~10 million
Actively infected individuals: ~1-1.25 millionActively infected individuals: ~1-1.25 million
Annual cirrhosis deaths: ~4,000Annual cirrhosis deaths: ~4,000
Annual HCC deaths: ~1,000-1,500Annual HCC deaths: ~1,000-1,500

HBV Disease Progression
1. Torresi J. 1. Torresi J. GastroenterologyGastroenterology. 2000;118(2 suppl 1):S83. 2000;118(2 suppl 1):S83–S–S103.103.2. Fattovich G. 2. Fattovich G. HepatologyHepatology. 1995;21:77–82.. 1995;21:77–82.3. Moyer LA. 3. Moyer LA. Am J Prev MedAm J Prev Med. 1994;10:45. 1994;10:45––55.55.4. Perrillo R. 4. Perrillo R. HepatologyHepatology. 2001;33:424–432.. 2001;33:424–432.
Acute Acute infectioninfection
ChronicChronic infectioninfection CirrhosisCirrhosis Death
55––10%10%1,31,3
Liver failure
30%30%11
25% in 5 years
Liver Liver Cancer Cancer (HCC)(HCC)
Chronic HBV is the Chronic HBV is the 66thth leading cause of leading cause of liver transplantation liver transplantation
in the USin the US44
Liver Liver transplant-transplant-ationation
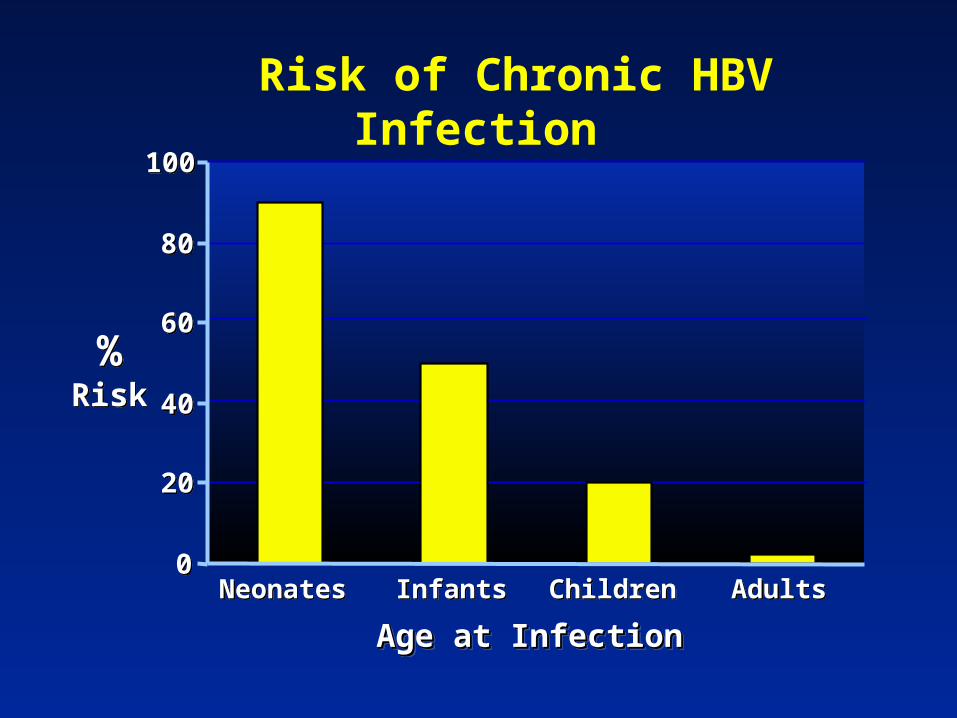
Age at InfectionAge at InfectionAge at InfectionAge at Infection
00
2020
4040
6060
8080
100100
NeonatesNeonates InfantsInfants ChildrenChildren AdultsAdults
%Risk%
Risk
Risk of Chronic HBV Infection

Chronic HBV InfectionChronic HBV Infection Chronic HBV InfectionChronic HBV Infection
Years after clinical presentationYears after clinical presentation
00
2020
4040
6060
8080
100100
00 11 22 33 44 55 66 77 88 991010
1111
1212
1313
% Probability
% Probability
Fattovich G, Gut 1991; 32:294Fattovich G, Gut 1991; 32:294
Overall Risk of Progression to Overall Risk of Progression to CirrhosisCirrhosis
Overall Risk of Progression to Overall Risk of Progression to CirrhosisCirrhosis
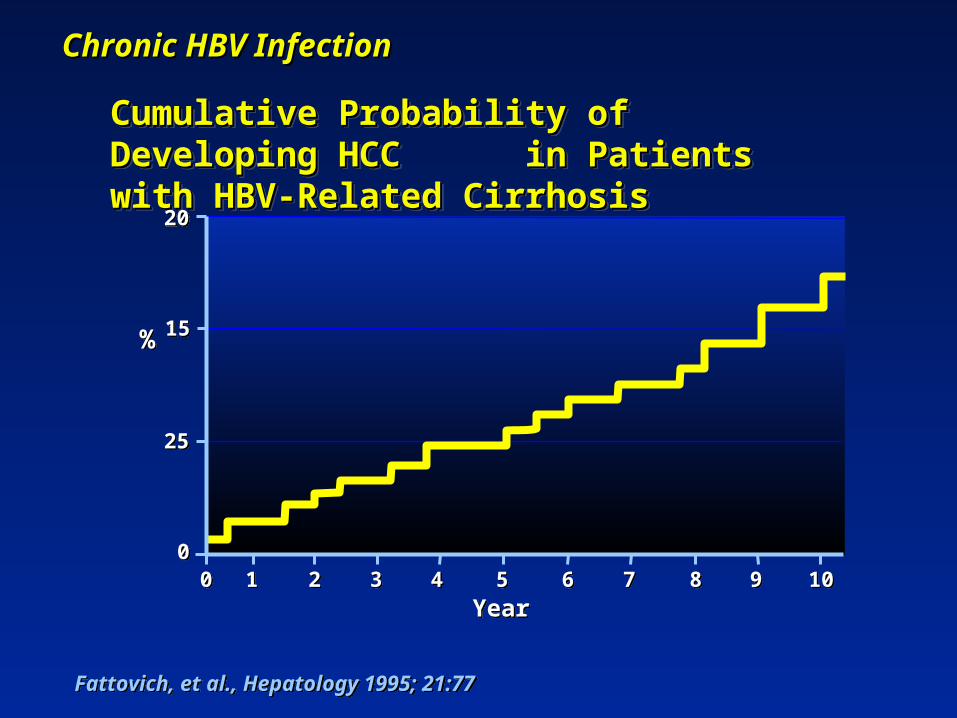
Fattovich, et al., Hepatology 1995; 21:77Fattovich, et al., Hepatology 1995; 21:77
Cumulative Probability of Developing Cumulative Probability of Developing HCC in Patients with HBV-Related HCC in Patients with HBV-Related CirrhosisCirrhosis
Cumulative Probability of Developing Cumulative Probability of Developing HCC in Patients with HBV-Related HCC in Patients with HBV-Related CirrhosisCirrhosis
00101000 998877665544332211
%%
YearYear
2020
2525
1515
Chronic HBV Chronic HBV InfectionInfection
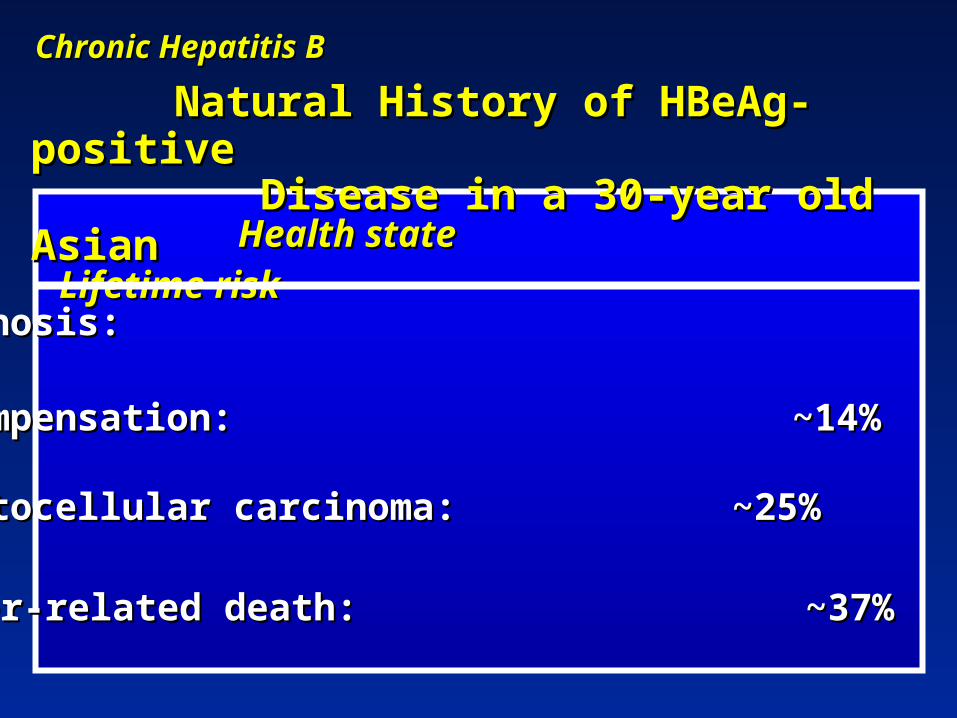
Natural History of HBeAg-positive Natural History of HBeAg-positive Disease in a 30-year old AsianDisease in a 30-year old Asian
Health stateHealth state Lifetime Lifetime riskrisk
• Cirrhosis: ~42%Cirrhosis: ~42%
• Decompensation: ~14%Decompensation: ~14%
• Hepatocellular carcinoma: Hepatocellular carcinoma: ~25% ~25%
• Liver-related death: ~37%Liver-related death: ~37%
Chronic Hepatitis BChronic Hepatitis B
Higher HBV DNA levels (>10Higher HBV DNA levels (>104 4
copies/mL)copies/mL)
HBeAg-positivityHBeAg-positivity
Persistent ALT elevationPersistent ALT elevation
HIV, alcohol, immunosuppressionHIV, alcohol, immunosuppression
Higher HBV DNA levels (>10Higher HBV DNA levels (>104 4
copies/mL)copies/mL)
HBeAg-positivityHBeAg-positivity
Persistent ALT elevationPersistent ALT elevation
HIV, alcohol, immunosuppressionHIV, alcohol, immunosuppression
Chronic Hepatitis B Chronic Hepatitis B
Factors Influencing Risk of Factors Influencing Risk of CirrhosisCirrhosis

Cumulative Incidence of Cirrhosis for Five HBV DNA
Categories (n=3,774)Multivariate adjusted HR
0
0.1
0.2
0.3
0.4
0 1 2 3 4 5 6 7 8 9 10 11 12 13
Year of Follow-up
Cu
mu
lati
ve In
cid
ence
of
Liv
er C
irrh
osi
s
≥ 1.0 x 101.0 - 9.9 x 101.0 - 9.9 x 10300 - 9.9 x 10< 300
Iloeje UH et al, Iloeje UH et al, Gastroenterology 2006;Gastroenterology 2006;130:678-86: The Taiwan Natural History Study130:678-86: The Taiwan Natural History Study
2.5 1.41.0
5.6
6.5
P value for log-rank test, <0.001
65
43

Serum HBV DNA Incidence Adj. Rel Risk Serum HBV DNA Incidence Adj. Rel Risk
pp(copies/mL) (per 100,000)(copies/mL) (per 100,000)
>>1.0 x 101.0 x 106 6 1150 11.6 1150 11.6 <.001<.001
>>1.0 x 101.0 x 1055 - <1.0 x 10 - <1.0 x 106 6 952 7.2 952 7.2
<.001<.001
>>1.0 x 101.0 x 1044 - <1.0 x 10 - <1.0 x 105 5 315 2.4315 2.4
<.008<.008
>300 - <1.0 x 10>300 - <1.0 x 104 4 112 0.9 112 0.9
NSNS
<300 145 1.0 <300 145 1.0
------
Serum HBV DNA Incidence Adj. Rel Risk Serum HBV DNA Incidence Adj. Rel Risk
pp(copies/mL) (per 100,000)(copies/mL) (per 100,000)
>>1.0 x 101.0 x 106 6 1150 11.6 1150 11.6 <.001<.001
>>1.0 x 101.0 x 1055 - <1.0 x 10 - <1.0 x 106 6 952 7.2 952 7.2
<.001<.001
>>1.0 x 101.0 x 1044 - <1.0 x 10 - <1.0 x 105 5 315 2.4315 2.4
<.008<.008
>300 - <1.0 x 10>300 - <1.0 x 104 4 112 0.9 112 0.9
NSNS
<300 145 1.0 <300 145 1.0
------
HBV DNA Levels and Risk of HBV DNA Levels and Risk of Hepatocellular Hepatocellular Carcinoma: The Taiwan Natural Carcinoma: The Taiwan Natural History History Study Study**
* Chen C-J et al. JAMA, 2006* Chen C-J et al. JAMA, 2006
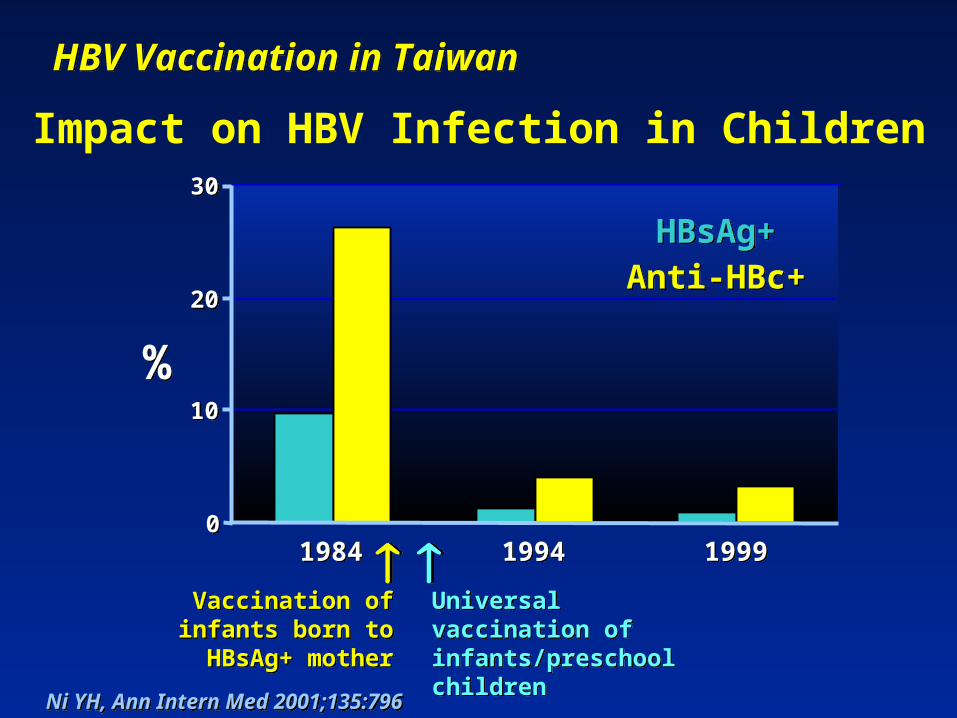
HBV Vaccination in TaiwanHBV Vaccination in Taiwan
%%
00
1010
2020
3030
19841984 19941994 19991999
Vaccination of infants born to
HBsAg+ mother
Vaccination of infants born to
HBsAg+ mother
HBsAg+HBsAg+Anti-HBc+Anti-HBc+
Universal vaccination of infants/preschool children
Universal vaccination of infants/preschool children
Ni YH, Ann Intern Med 2001;135:796 Ni YH, Ann Intern Med 2001;135:796
Impact on HBV Infection in Children
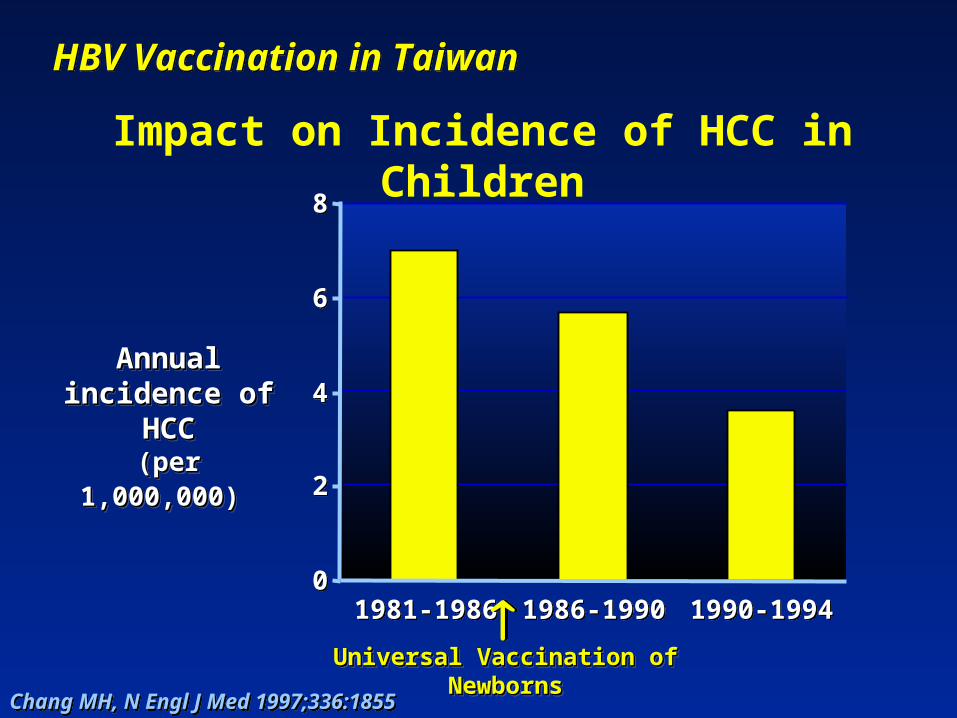
HBV Vaccination in TaiwanHBV Vaccination in Taiwan
00
22
44
66
88
1981-19861981-1986 1986-19901986-1990 1990-19941990-1994
Annual Annual incidence of incidence of
HCCHCC(per (per
1,000,000)1,000,000)
Annual Annual incidence of incidence of
HCCHCC(per (per
1,000,000)1,000,000)
Universal Vaccination of Universal Vaccination of
NewbornsNewbornsUniversal Vaccination of Universal Vaccination of
NewbornsNewbornsChang MH, N Engl J Med 1997;336:1855Chang MH, N Engl J Med 1997;336:1855
Impact on Incidence of HCC in Children
Epidemiology of HBV
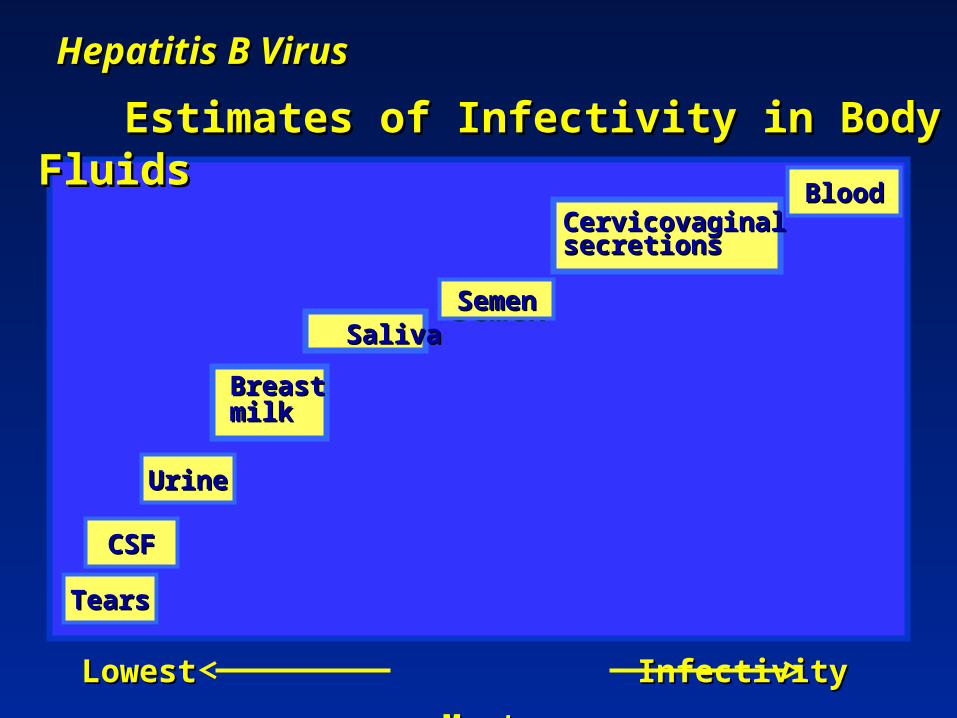
Hepatitis B VirusHepatitis B Virus
Estimates of Infectivity in Body Estimates of Infectivity in Body FluidsFluids
BloodBlood
SemenSemen
CSFCSF
SemenSemen
BloodBlood
Lowest Infectivity Lowest Infectivity
MostMost
UrineUrine
BreastBreastmilkmilk
SalivaSaliva
CervicovaginalCervicovaginalsecretionssecretions
TearsTears

Epidemiologic Characteristics of Epidemiologic Characteristics of Patients With Hepatitis B — US, Patients With Hepatitis B — US,
2005*2005*More than 70% of newly acquired infections in 2005 were
attributable to high-risk sexual activity or injection drug use
58%
15%10%
14%
32%
9%6% No risk factor identified
Injection drug use
Sexual contact withhepatitis B patient
Homosexual activity (male)
>1 sex partner
Surgery
Other
*Values total >100% because multiple risk factors could be reported for a single case.CDC. MMWR. 2007;56(SS-3):1-25.
Hepatitis BHepatitis B
Factors Associated with Sexual Factors Associated with Sexual TransmissionTransmission
• Multiple sexual partners, unprotected Multiple sexual partners, unprotected
sexsex
• Injecting drug user as sexual partnerInjecting drug user as sexual partner
• Duration of sexual activityDuration of sexual activity
• Male to female,male to male,female to Male to female,male to male,female to
malemale
• History or serologic evidence of otherHistory or serologic evidence of other sexually transmitted diseasessexually transmitted diseases

Prevention of Hepatitis B

Hepatitis B Prevention StrategiesHepatitis B Prevention Strategies
Reducing the Risk of InfectionReducing the Risk of Infection
• Decreasing exposure Decreasing exposure
opportunitiesopportunities
• Decreasing susceptibilityDecreasing susceptibility
- immunization with hepatitis B - immunization with hepatitis B
vaccinesvaccines
Non-vaccine Prevention of HBV
● Screening of blood donors for HBsAg, anti-Screening of blood donors for HBsAg, anti-HBc (future screening for HBV DNA)HBc (future screening for HBV DNA)
● Screening of organ and tissue donorsScreening of organ and tissue donors● Safe-sex practicesSafe-sex practices● Reduction in sharing equipment for IV drug Reduction in sharing equipment for IV drug
useuse● Needle-exchange programs and education Needle-exchange programs and education
about cleaning equipmentabout cleaning equipment● Avoidance of intranasal cocaine useAvoidance of intranasal cocaine use● Inspection of tattoo and body-piercing Inspection of tattoo and body-piercing
shopsshops● Sterilization of manicure/pedicure Sterilization of manicure/pedicure
equipment equipment ● Avoidance of multidose vial misuseAvoidance of multidose vial misuse
Vaccine-based Strategies for Vaccine-based Strategies for Eliminating HBV Transmission in the Eliminating HBV Transmission in the U.S.U.S.• Maternal screening for HBsAg:Maternal screening for HBsAg: providing providing
post-exposure prophylaxis to infants of post-exposure prophylaxis to infants of HBsAg-positive womenHBsAg-positive women
- HBIG within 12 hours of birth and first of - HBIG within 12 hours of birth and first of
3 3 doses of HBV vaccinedoses of HBV vaccine
• Routine vaccination of all newborn infantsRoutine vaccination of all newborn infants
• Catch-up vaccination:Catch-up vaccination: for children aged <19 for children aged <19
yrs yrs
• Targeting high risk:Targeting high risk: children, adolescents, children, adolescents,
adultsadults
• Screening and vaccination:Screening and vaccination: household and household and
family members of HBsAg-positive personsfamily members of HBsAg-positive persons
0
0.5
1
1.5
1990 1992 1994 1996 1998 2000 2002 2004
0
2
4
6
8
10
1990 1992 1994 1996 1998 2000 2002 2004
Year
Cas
es/1
00,0
00
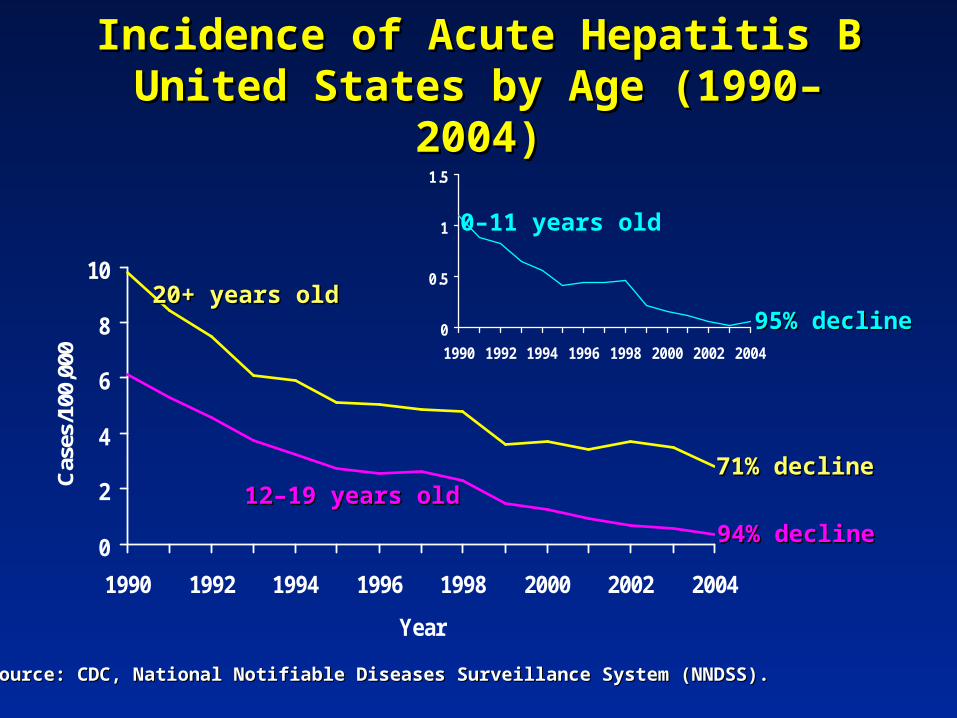
0–11 years old
95% decline95% decline
71% decline71% decline
94% decline94% decline
20+ years old20+ years old
12–19 years old12–19 years old
Source: CDC, National Notifiable Diseases Surveillance System (NNDSS).Source: CDC, National Notifiable Diseases Surveillance System (NNDSS).
Incidence of Acute Hepatitis B Incidence of Acute Hepatitis B United States by Age (1990–United States by Age (1990–
2004)2004)
2007 Vaccine-based Strategies to Eliminate Hepatitis B Transmission in the Young
● Establish standing orders for first dose of HBV vaccine at birth
● Improve identification of and immunization of infants born to HBsAg-positive mothers and those in whom the maternal HBsAg status is unknown
● Develop HBV vaccination record reviews of all children aged 11 to 12 years and for individuals <19 years of age born in endemic regions
● Make hepatitis B vaccination a requirement for school entry● Incorporate HBV vaccine delivery into adolescent care
services

2007 Vaccine-based Strategies to Eliminate Hepatitis B Transmission in Adults
● Vaccinate high-risk adults attending facilities for individuals with high risks for sexual or parenteral exposure
● Educate adults in primary or specialty care settings about risks of infection, benefits of vaccination, and current recommendations; vaccinate those who report risks
● Vaccinate any individual requesting protection● Establish standing orders by health-care workers to
identify those recommended for vaccination and to vaccinate as part of routine care
● Initiate vaccination in individuals who fail to Initiate vaccination in individuals who fail to acknowledge a risk factoracknowledge a risk factor
Treatment of Chronic Treatment of Chronic Hepatitis B Hepatitis B

Suppression of viral replicationSuppression of viral replication
Improvement in hepatic necroinflammatory Improvement in hepatic necroinflammatory diseasedisease
Reduction in long-term sequelae: HBV-Reduction in long-term sequelae: HBV-associated cirrhosis, hepatocellular associated cirrhosis, hepatocellular carcinomacarcinoma
Reduction of infectivityReduction of infectivity
Chronic Hepatitis B Management Chronic Hepatitis B Management GoalsGoals

Effect of Lamivudine on Incidence Effect of Lamivudine on Incidence of HCC in Chronic HBV with of HCC in Chronic HBV with
Advanced FibrosisAdvanced Fibrosis
Liaw YF, et al.Liaw YF, et al. N Engl J Med N Engl J Med 2004;351:1521–1531. 2004;351:1521–1531.
Length of Therapy (months)
Lamivudine
Placebo
Dia
gn
osi
s o
f H
CC
(%
)
0
10
60 12 18 24 30 36
P = 0.047
Chronic Hepatitis BChronic Hepatitis B
Patients with:Patients with:
Elevated or normal ALT levelsElevated or normal ALT levels andand::
HBeAg-positive and HBV DNA HBeAg-positive and HBV DNA ≥≥10104-54-5 copies/mL copies/mL
by PCRby PCR
HBeAg-negative and HBV DNA HBeAg-negative and HBV DNA ≥≥101044 copies/mL by PCRcopies/mL by PCR
+/- liver biopsy evidence of disease +/- liver biopsy evidence of disease
Cirrhosis with detectable HBV DNACirrhosis with detectable HBV DNA
Candidates for TreatmentCandidates for Treatment
HBV Treatment Options in 2008HBV Treatment Options in 2008
● Pegylated interferon alfa-2aPegylated interferon alfa-2a● Interferon alfa-2bInterferon alfa-2b
● Nucleoside analogsNucleoside analogs– EntecavirEntecavir– LamivudineLamivudine– TelbivudineTelbivudine
● Nucleotide analogsNucleotide analogs– AdefovirAdefovir– Tenofovir (likely to be FDA-approved Tenofovir (likely to be FDA-approved
soon)soon)
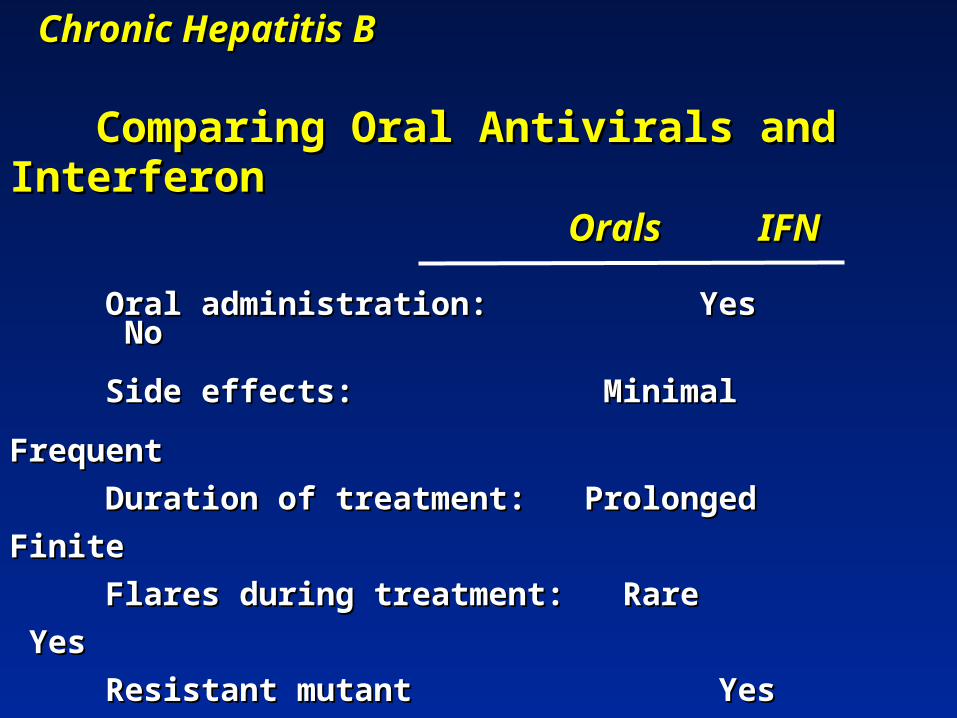
Chronic Hepatitis BChronic Hepatitis B
Comparing Oral Antivirals and Comparing Oral Antivirals and InterferonInterferon
Orals IFNOrals IFN Oral administration: Yes NoOral administration: Yes No
Side effects:Side effects: Minimal Frequent Minimal Frequent
Duration of treatment: Prolonged Finite Duration of treatment: Prolonged Finite
Flares during treatment: Rare YesFlares during treatment: Rare Yes
Resistant mutant Yes NoResistant mutant Yes No
Rate of HBsAg clearance: Low HigherRate of HBsAg clearance: Low Higher
Improved outcomes: Yes YesImproved outcomes: Yes Yes
Treatment of HBV Patients:Treatment of HBV Patients: Now Now and and
in the Futurein the Future
● Focus on HBV DNA suppressionFocus on HBV DNA suppression● Treatment decisions based on HBV DNA Treatment decisions based on HBV DNA
levels, disease severity, drug efficacy and levels, disease severity, drug efficacy and resistance patterns (for oral agents)resistance patterns (for oral agents)
● Combination oral therapy emergingCombination oral therapy emerging
● New agents with prolonged activity after New agents with prolonged activity after end-of-treatment, e.g. clevudineend-of-treatment, e.g. clevudine
Other Management Other Management StrategiesStrategies
● Immunization against HAV, other infectionsImmunization against HAV, other infections● Avoidance of alcohol, hepatotoxic herbalsAvoidance of alcohol, hepatotoxic herbals
● Screening for hepatocellular carcinomaScreening for hepatocellular carcinoma
- imaging studies, AFP, others- imaging studies, AFP, others
- appropriate timing- appropriate timing
● Case-finding (family, non-family contacts) Case-finding (family, non-family contacts) for for
vaccinationvaccination

Summary
● Hepatitis B is the major global cause of HCC
● Safe and effective vaccines: result in dramatic declines of HBV infection in children and HCC
● Many at-risk individuals remain unvaccinated; a large reservoir of infected persons exists
● Treatment should reduce HBV transmission and improves outcomes but is expensive and long-term for most patients
● Concomitantly with increasing vaccine coverage, education on reducing high-risk lifestyles must be a continuing focus