hepatic stellate cell immunodetection and cirrhotic evolution of viral hepatitis in liver allografts
TRANSCRIPT
Hepatic Stellate Cell Immunodetection and Cirrhotic Evolution ofViral Hepatitis in Liver Allografts
MARIA GUIDO,1 MASSIMO RUGGE,1 GIOACCHINO LEANDRO,2 ISABEL M. FIEL,3 AND SWAN N. THUNG3
Infections with hepatitis B and hepatitis C viruses are thePatients with chronic viral hepatitis are at high risk ofmost common cause of chronic hepatitis with a high preva-developing cirrhosis, but the outcome of the disease in alence of evolution to cirrhosis. It would be of great clinicalgiven patient is unpredictable. Hepatic stellate cells have beenvalue to identify patients at a high risk of developing cirrhosisdemonstrated to be the most important cell type involved inbecause only 20% to 30% of cases benefit from interferonhepatic fibrogenesis, regardless of the cause of the liver injury.therapy,1-3 which is also a rather expensive treatment and isThe alpha isotype of actin (a phenotypic marker of smoothassociated with various side effects. Efforts have been mademuscle cells) may be expressed by hepatic stellate cells, re-to identify morphological lesions that may predict a cirrhoticflecting their ‘‘activation’’ to myofibroblast-like cells. The pres-evolution.ent study aimed to analyze the expression of a-smooth muscle
Piecemeal necrosis, intralobular necrosis, and particularlyactin-positive hepatic stellate cells in liver allografts with re-portal-central bridging necrosis,4 have been considered im-current viral hepatitis, and to evaluate whether and how suchportant features in the morphogenesis of cirrhosis, but whichexpression may be related to the outcome of the disease.patients will develop cirrhosis is still unpredictable. OurUsing immunohistochemistry and a semi-quantitative scoringknowledge of fibrogenesis, which is a necessary step in cir-system, the expression of a-smooth muscle actin in hepaticrhosis, has dramatically increased in recent years. Hepaticstellate cells was analyzed in liver allografts of 17 patientsfibrogenesis is a highly complex process involving severalwith recurrent viral hepatitis. They included nine patientstypes of cells.5 In this context, a key role played by hepaticwho developed cirrhosis at the end of follow-up (mean timestellate cells (HSC), which change into myofibroblast-like23.6 months), and eight patients with no cirrhosis at the endcells and produce extracellular matrix (HSC activation), isof a comparable follow-up time (mean 30.1 months). In alllargely accepted as the central event of hepatic fibrogenesis.patients, liver biopsy specimens were obtained between 3Most of the data have been collected by means of experimen-and 6 months (t1) and between 10 and 15 months (t2) aftertal studies, however, and the mechanisms of fibrogenesis intransplantation. Preperfusion biopsy specimens of donor liv-human chronic liver disease are still under investigation.ers served as a baseline (t0). By comparison with the baselineHuman HSCs may express alpha-smooth muscle specific ac-biopsy, an increased number of a-smooth muscle actin-ex-tin (a-SMA),6 which are then considered as ‘‘activated’’ myo-pressing hepatic stellate cells was observed in all cases in t1fibroblast-like HSCs.7,8 An increased number of a-SMA ex-biopsies. An increase in the amount of a-smooth muscle actin-pressing HSCs has been documented in several pathologicalpositive hepatic stellate cells in zone 1 at t1 was significantlyconditions associated with fibrosis6,8-10; on the other hand,(P õ .006) related to subsequent cirrhotic evolution. In con-a decreasing number of HSCs has been documented afterclusion, in liver allografts with recurrent viral hepatitis, theinterferon therapy associated with an improvement in theactivation of hepatic stellate cells is an early event. An in-necroinflammatory lesions.11 In the present study, we focuscreased number of a-smooth muscle actin-positive hepaticon the possible relationship between the immunodetectionstellate cells in zone 1 may represent an unfavorable eventof a-SMA–expressing HSCs and the development of cirrhosisrelated to cirrhotic evolution. (HEPATOLOGY 1997;26:310-in liver allografts with viral hepatitis.314.)
PATIENTS AND METHODS
Seventeen patients were studied. They included 9 consecutivesubjects (4 females and 5 males) who underwent orthotopic liver
Abbreviations: HSC, hepatic stellate cell; a-SMA, alpha-smooth muscle specifictransplantation (OLT) for cirrhosis related to chronic hepatitis B
actin; OLT, orthotopic liver transplantation.(1 case) and C (8 cases) at the Mount Sinai Medical Center, andFrom 1Cattedra di Istochimica ed Immunoistochimica Patologica, Universita diwho developed cirrhosis again in a mean follow-up of 23.6 monthsPadova-Servizio di Anatomia Patologica ULSS 15, Ospedale di Cittadella, Padova, Italy;(range 14-45 mo) after OLT (group I); a control group (group II)2Ente Specializzato in Gastroenterologia ‘‘Saverio de Bellis,’’ Castellana Grotte Bari,
Italy; and 3The Lillian and Henry M. Stratton, Hans Popper Department of Pathology, was composed of 8 consecutive patients (3 females and 5 males)the Mount Sinai Medical Center of the City University of New York, New York, NY. who underwent OLT for viral hepatitis-induced cirrhosis (hepatitis
Received August 29, 1996; accepted March 26, 1997. B virus in 2 cases, hepatitis C virus in 5), but who had not developedThe statistical analysis was performed by G. Leandro, M.D., biostatistician. cirrhosis at the end of a comparable follow-up time (mean 30.1Supported in part by a grant from the ‘‘CCC’’ Association Against Cancer, Cittadella, months, range 21-42).
Italy; and by a grant from the Italian Ministry for the University, Rome, Italy (MURST,Groups I and II showed no significant difference in age (group
60%).I: mean age 38.5 years, range 16-58; group II mean age 44 years,Address reprint requests to: Massimo Rugge, M.D., Istituto di Anatomia Patologica,range 16-63). The general transplantation data, including surgery,Via Gabelli 61, I-35121, Padova, Italy. Fax: 39-49-942-4981.postoperative monitoring, and type of immunosuppressant therapy,Copyright q 1997 by the American Association for the Study of Liver Diseases.
0270-9139/97/2602-0010$3.00/0 were similar in the two groups. No statistical differences were noted
310
AID Hepa 0017 / 5p24$$$321 07-10-97 12:24:13 hepa WBS: Hepatology

HEPATOLOGY Vol. 26, No. 2, 1997 GUIDO ET AL. 311
TABLE 1. Necroinflammatory Lesions in Liver Biopsy Specimens of serum. The presence of a-SMA reactive HSCs was semiquantita-tively scored as described by Schmitt-Graff et al.6 as 0 Å no stainingGroup I and II Patients Obtained Between 3 and 6 Months
After OLT (t1) or very rare staining, 1 Å few cells stained (Å staining of HSCsoccupying approximately 1% to 10% of the sinusoidal liver cell
Group I Group IIsurface), 2 Å more cells stained (Å staining of HSCs occupying
N % N % approximately 10% to 30% of the sinusoidal liver cell surface), 3Å large number of cells stained (Å staining of HSCs occupying
Periportal Necrosis approximately 30% to 70% of sinusoidal liver cell surface), and 4Absent 5 55 6 75 Å diffuse staining of more than 70% of sinusoidal liver cell surface.Low grade 1 11 1 12 For statistical purposes, scores of 3 and 4 were combined as high-High grade 3 34 1 12 grade a-SMA-HSC expression and scores of 1 and 2 were combined
Lobular Necrosis as low-grade a-SMA-HSC expression. In addition, a-SMA-positiveAbsent 0 0 3 37 HSCs were scored separately in periportal, intermediate, and peri-Low grade 2 22 1 12 venular zones. No less than five liver acini were evaluated in eachHigh grade 7 78 4 50 sample. The final score assigned to each zone was defined according
Sinusoidal Cell Hyperplasia* to the highest value observed.Absent 0 0 4 50 Both histological and immunohistochemical studies were blindlyLow grade 7 78 1 12 evaluated. Intraobserver agreement resulted higher than 85%.High grade 2 23 3 38 Statistical Study. The statistical analysis of the results was made
by means of the x2 test to assess the independence of the variables* Difference between group I and II was significant (P õ .01).evaluated in the two groups. McNemar’s x2 test was used to evaluatevariations in the paired variables.
between groups I and II in the number of episodes of rejection.RESULTS
The mean value of serum alanine aminotransferase at t1 was 605.56UI/L in group I (range, 350-1,000) and 547.5 UI/L in Group II Histological Study. Preperfusion biopsy specimens of donor(range, 280-900). At t2 the values were respectively 321.43 UI/L in livers (t0) showed no abnormalities, or mild, nonspecificgroup I (range, 200-600) and 262 UI/L in group II (range, 60-400). lesions including mild steatosis, mild sinusoidal cell hyper-At both t1 and t2 the difference was not significant. plasia, and mild portal fibrosis. No differences were detected
All patients in both groups had a recurrence of the same type of in t0 biopsy specimens between patients with and withoutpre-OLT viral infection. In all cases, the infection was serologically subsequent cirrhotic evolution.shown between 2 and 6 months after transplantation by means of
As for the histology of t1 biopsies, high-grade portal inflam-serologic viral markers and/or by the detection of the viral genomemation, piecemeal necrosis, and lobular necrosis were moreby the polymerase chain reaction method. No quantitative data onfrequently observed in group I than in group II, but thehepatitis C virus-RNA levels were available.differences were not statistically significant. A significant as-The preperfusion biopsy specimen of donor livers served as a
baseline biopsy (t0). All patients had at least one liver biopsy per- sociation (P õ .01) was observed at t1 between the absenceformed between 3 and 6 months (t1) and 14 patients had at least of sinusoidal cell hyperplasia and no cirrhotic evolution (Ta-one liver biopsy performed between 10 and 15 months (t2) after ble 1). No differences were detected in the presence andOLT. Of the three patients with no liver biopsy specimens available zonal distribution of all the other lesions considered.at t2 , two had already developed cirrhosis at the 15th month after Similar findings were observed in the biopsies taken atOLT. In the last one, the liver biopsy performed 25 months after t2 , except that the significant difference in sinusoidal cellOLT showed a stage 2 fibrosis (hence the inclusion of this case in
hyperplasia between the two groups was lost.the control group).As for the conclusive diagnosis, differences were not signif-The diagnosis or exclusion of cirrhosis at the end of follow-up
icant, though acute hepatitis was more frequently observedwas histologically confirmed in all patients.at t1 in the biopsy specimens of patients developing cirrhosisHistological Study. Liver biopsy specimens were formalin-fixed,
paraffin-embedded, and stained with hematoxylin and eosin, peri- than in the other group (Table 2). No cases of fibrosingodic acid–Schiff before and after diastase digestion, reticulin for cholestatic hepatitis were seen.collagen fibers, and Perls’ method for iron. Immunohistochemical Study. A strong a-SMA immunoreac-
The following lesions were semi-quantitatively graded as absent, tivity was observed in the vessel walls in all cases, whereaslow- (mild), and high- (moderate or severe) grade: portal inflamma- no positivity was detected in the negative controls.tion, piecemeal necrosis, lobular necrosis, sinusoidal (Kupffer andendothelial) cell hyperplasia, intrasinusoidal inflammation, chole-stasis, steatosis. Lobular lesions were also separately assessed in the
TABLE 2. Histological Diagnosis in Groups I and II at t1 and t2three acinar zones. Using accepted criteria,12 fibrosis was graded as0 Å absent, 1 Å portal, 2 Å septal with no architectural distortion,
t1 t23Å incomplete cirrhosis, and 4Å cirrhosis. Only cases with a score
Group I Group II Group I Group IIof 4 were included in the cirrhosis group, and scores of 0 to 2 wereincluded in the noncirrhotic group. One biopsy showing stage 3
Diagnosis N % N % N % N %fibrosis was excluded (see above). Rejection was graded as absent,mild, moderate or severe, using current methods.13
Normal liver 0 0 0 0 0 0 1 14Each biopsy was labeled with one or more of the following con- Rejection 1 11 1 12 1 14 0 0
clusive diagnoses: acute hepatitis, chronic hepatitis, rejection, and/ Acute hepatitis 6 67 3 37 1 14 0 0or other types of lesions (e.g., consistent with large bile duct dam- Chronic hepatitis 1 11 2 25 5 71 5 71age). Others 1 11 2 25 0 0 1 14
Immunohistochemical Study. HSCs were detected using antibody toa-SMA as described elsewhere11 and using vascular smooth muscle NOTE. t1 , Liver biopsies taken between 3 and 6 months after OLT; t2 ,
liver biopsies taken between 10 and 15 months after OLT (see Patients andcell immunoreactivity as an internal positive control. As a negativecontrol, the primary antibody was replaced with normal mouse Methods).
AID Hepa 0017 / 5p24$$$321 07-10-97 12:24:13 hepa WBS: Hepatology
312 GUIDO ET AL. HEPATOLOGY August 1997
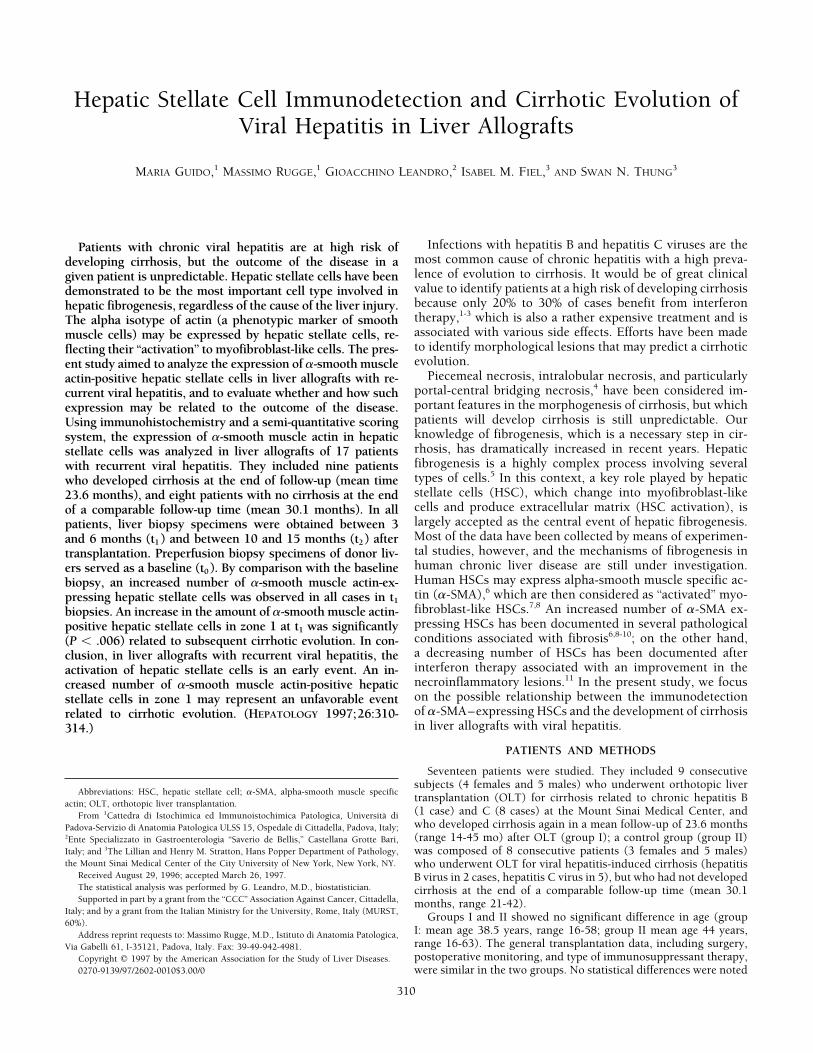
FIG. 1. Liver biopsy taken at t0 :In the portal tract (left corner) thevessel walls are strongly positive fora-SMA. Low grade a-SMA expres-sion (score 1) in sinusoidal hepaticstellate cells (arrow heads). (Avidin-biotin complex method; originalmagnification 1250.)
At t0 most cases showed absent or low-grade (Fig. 1) a-SMA immunoreactivity in zones 1 and 2 was more fre-quently detected in group I than in group II (Table 3). Proba-a-SMA expression (Table 3). The amount of immunoreactive
cells varied through the three acinar zones and an increasing bly because of the small number of cases, the difference wasnot significant. However, the increase in the number of a-gradient from zone 1 to 2 to 3 was observed. No significant
differences were observed at this time, however, between SMA–reactive HSCs in zone 1 at t1 was significantly related tocirrhotic evolution (Põ .006). The sensitivity and specificitypatients in groups I and II.
In liver biopsies performed at t1 , the amount of a-SMA- were 88.9% and 87.5%, respectively. Because of the decreas-ing number of a-SMA–reacting cells from the t1 to the t2 liverpositive HSCs increased in both groups. Positivity was fre-
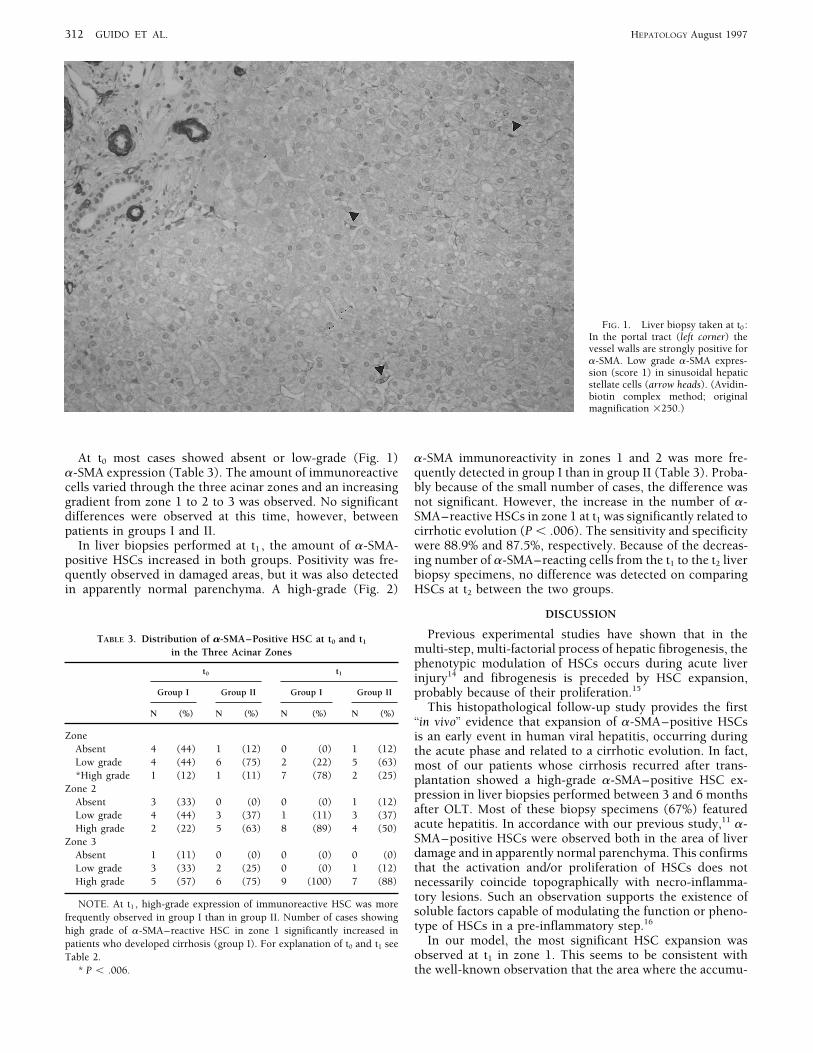
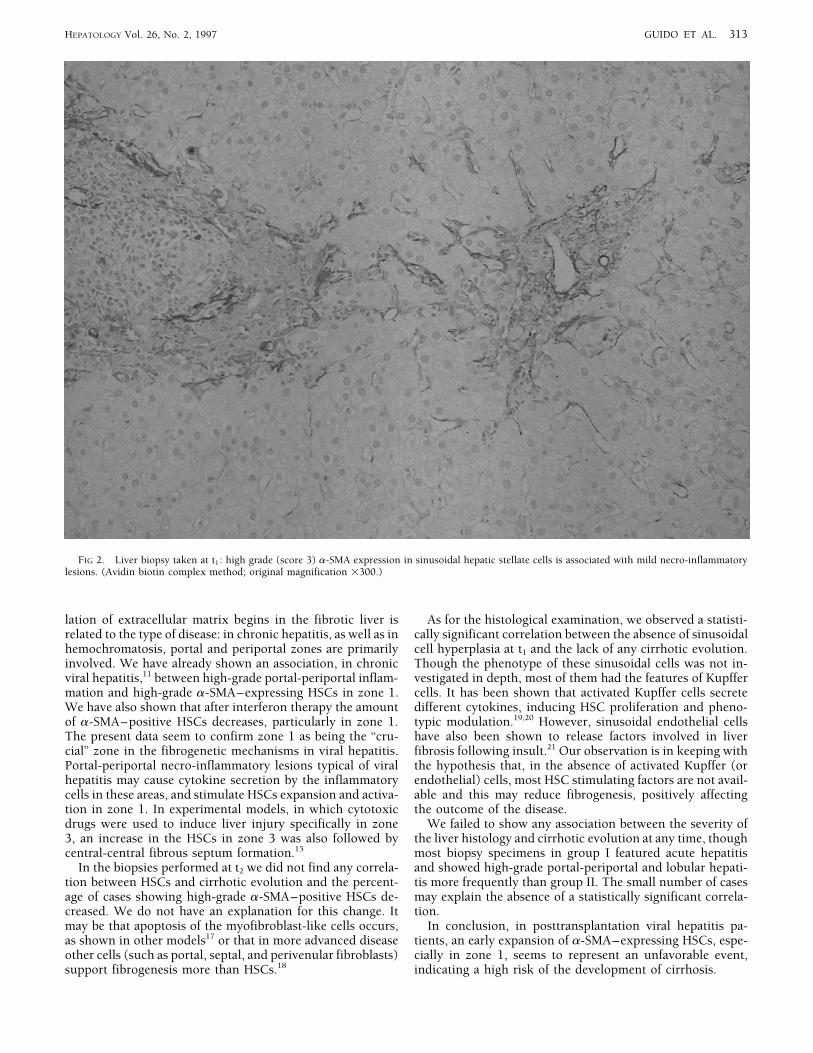
quently observed in damaged areas, but it was also detected biopsy specimens, no difference was detected on comparingHSCs at t2 between the two groups.in apparently normal parenchyma. A high-grade (Fig. 2)
DISCUSSION
Previous experimental studies have shown that in theTABLE 3. Distribution of a-SMA–Positive HSC at t0 and t1
multi-step, multi-factorial process of hepatic fibrogenesis, thein the Three Acinar Zonesphenotypic modulation of HSCs occurs during acute liver
t0 t1 injury14 and fibrogenesis is preceded by HSC expansion,Group I Group II Group I Group II probably because of their proliferation.15
This histopathological follow-up study provides the firstN (%) N (%) N (%) N (%)
‘‘in vivo’’ evidence that expansion of a-SMA–positive HSCsZone is an early event in human viral hepatitis, occurring during
Absent 4 (44) 1 (12) 0 (0) 1 (12) the acute phase and related to a cirrhotic evolution. In fact,Low grade 4 (44) 6 (75) 2 (22) 5 (63) most of our patients whose cirrhosis recurred after trans-*High grade 1 (12) 1 (11) 7 (78) 2 (25) plantation showed a high-grade a-SMA–positive HSC ex-
Zone 2 pression in liver biopsies performed between 3 and 6 monthsAbsent 3 (33) 0 (0) 0 (0) 1 (12)
after OLT. Most of these biopsy specimens (67%) featuredLow grade 4 (44) 3 (37) 1 (11) 3 (37)acute hepatitis. In accordance with our previous study,11 a-High grade 2 (22) 5 (63) 8 (89) 4 (50)SMA–positive HSCs were observed both in the area of liverZone 3damage and in apparently normal parenchyma. This confirmsAbsent 1 (11) 0 (0) 0 (0) 0 (0)
Low grade 3 (33) 2 (25) 0 (0) 1 (12) that the activation and/or proliferation of HSCs does notHigh grade 5 (57) 6 (75) 9 (100) 7 (88) necessarily coincide topographically with necro-inflamma-
tory lesions. Such an observation supports the existence ofNOTE. At t1 , high-grade expression of immunoreactive HSC was more
soluble factors capable of modulating the function or pheno-frequently observed in group I than in group II. Number of cases showingtype of HSCs in a pre-inflammatory step.16
high grade of a-SMA–reactive HSC in zone 1 significantly increased inIn our model, the most significant HSC expansion waspatients who developed cirrhosis (group I). For explanation of t0 and t1 see
observed at t1 in zone 1. This seems to be consistent withTable 2.* P õ .006. the well-known observation that the area where the accumu-
AID Hepa 0017 / 5p24$$$321 07-10-97 12:24:13 hepa WBS: Hepatology
HEPATOLOGY Vol. 26, No. 2, 1997 GUIDO ET AL. 313
FIG 2. Liver biopsy taken at t1 : high grade (score 3) a-SMA expression in sinusoidal hepatic stellate cells is associated with mild necro-inflammatorylesions. (Avidin biotin complex method; original magnification 1300.)
lation of extracellular matrix begins in the fibrotic liver is As for the histological examination, we observed a statisti-cally significant correlation between the absence of sinusoidalrelated to the type of disease: in chronic hepatitis, as well as in
hemochromatosis, portal and periportal zones are primarily cell hyperplasia at t1 and the lack of any cirrhotic evolution.Though the phenotype of these sinusoidal cells was not in-involved. We have already shown an association, in chronic
viral hepatitis,11 between high-grade portal-periportal inflam- vestigated in depth, most of them had the features of Kupffercells. It has been shown that activated Kupffer cells secretemation and high-grade a-SMA–expressing HSCs in zone 1.
We have also shown that after interferon therapy the amount different cytokines, inducing HSC proliferation and pheno-typic modulation.19,20 However, sinusoidal endothelial cellsof a-SMA–positive HSCs decreases, particularly in zone 1.
The present data seem to confirm zone 1 as being the ‘‘cru- have also been shown to release factors involved in liverfibrosis following insult.21 Our observation is in keeping withcial’’ zone in the fibrogenetic mechanisms in viral hepatitis.
Portal-periportal necro-inflammatory lesions typical of viral the hypothesis that, in the absence of activated Kupffer (orendothelial) cells, most HSC stimulating factors are not avail-hepatitis may cause cytokine secretion by the inflammatory
cells in these areas, and stimulate HSCs expansion and activa- able and this may reduce fibrogenesis, positively affectingthe outcome of the disease.tion in zone 1. In experimental models, in which cytotoxic
drugs were used to induce liver injury specifically in zone We failed to show any association between the severity ofthe liver histology and cirrhotic evolution at any time, though3, an increase in the HSCs in zone 3 was also followed by
central-central fibrous septum formation.15 most biopsy specimens in group I featured acute hepatitisand showed high-grade portal-periportal and lobular hepati-In the biopsies performed at t2 we did not find any correla-
tion between HSCs and cirrhotic evolution and the percent- tis more frequently than group II. The small number of casesmay explain the absence of a statistically significant correla-age of cases showing high-grade a-SMA–positive HSCs de-
creased. We do not have an explanation for this change. It tion.In conclusion, in posttransplantation viral hepatitis pa-may be that apoptosis of the myofibroblast-like cells occurs,
as shown in other models17 or that in more advanced disease tients, an early expansion of a-SMA–expressing HSCs, espe-cially in zone 1, seems to represent an unfavorable event,other cells (such as portal, septal, and perivenular fibroblasts)
support fibrogenesis more than HSCs.18 indicating a high risk of the development of cirrhosis.
AID Hepa 0017 / 5p24$$$321 07-10-97 12:24:13 hepa WBS: Hepatology

314 GUIDO ET AL. HEPATOLOGY August 1997
9. Nouchi T, Tanaka Y, Tsukada T, Sato C, Marumo F. Appearance of a-Acknowledgment: The authors are grateful to Luciana Po-smooth muscle actin positive cells in hepatic fibrosis. Liver 1991;11:letto for technical assistance and to Frances Coburn for edit-100-105.
ing the manuscript. 10. Yamaoka K, Toshihiko N, Marumo F, Sato C. a-Smooth muscle actinexpression in normal and fibrotic human livers. Dig Dis Sci 1993;8:
REFERENCES 1473-1479.11. Guido M, Rugge M, Chemello L, Leandro G, Fattovich G, Giustina G,
1. Fattovich G, Brollo L, Boscaro S, Pontisso P, Giustina G, Criscuolo D, Cassaro M, et al. Liver stellate cells in chronic viral hepatitis: the effectMaladorno D, et al. Long-term effect of low dose recombinant interferon of interferon therapy. J Hepatol 1996;24:301-307.therapy in patients with chronic hepatitis. Brit J Hepatol 1989;9:331- 12. Scheuer PJ. Classification of chronic viral hepatitis: a need for reassess-337. ment. J Hepatol 1991;13:372-374.
2. Fattovich G, Farci P, Rugge M, Brollo L, Mandas A, Pontisso P, Giustina 13. Thung SN, Gerber M Histopathology of liver transplantation. In: FabryG, et al. A randomized controlled trial of lymphoblastoid interferon- in TL, Klion FM, eds. Guide to Liver Transplantation. New York: Igaku-patients with chronic hepatitis B lacking HBeAg. HEPATOLOGY 1992;15: Shoin, 1992:265-298.584-589. 14. Johnson SJ, Hines JE, Burt AD. Phenotypic modulation of perisinusoidal
3. Alberti A, Chemello L, Bonetti P, Casarin C, Diodati G, Cavalletto L, cells following acute liver injury: a quantitative analysis. Int J Exp PatholCavalletto D, et al. Treatment with interferon(s) of community acquired 1992;73:765-772.chronic hepatitis and cirrhosis type C. J HEPATOLOGY 1993;17(Suppl 15. Geerts A, Lazou JM, De Bleser P, Wisse E. Tissue distribution, quantita-3):S123-S126. tion and proliferation kinetics of fat-storing cells in carbon-tetrachlo-
4. Chen TI, Liaw YF. The prognostic significance of bridging hepatic ne- ride-injured rat liver. HEPATOLOGY 1991;13:1193-1202.crosis in chronic type B hepatitis: a histopathologic study. Liver 1988; 16. Gressner AM, Lotfi S, Gressner G, Lahme B. Identification and partial8:10-15 characterization of a hepatocyte-derived factor promoting proliferation
5. Burt AD. C. L. Oakley lecture (1993): Cellular and molecular aspects of fat-storing cells (parasinusoidal lipocytes). HEPATOLOGY 1992;16:of hepatic fibrosis. J Pathol 1993;170:105-114. 1250-1266.
6. Schmitt-Graff A, Kruger S, Bochard F, Gabbiani G, Denk H. Modulation 17. Darby I, Skalli O, Gabbiani G. a-Smooth muscle actin is transientlyof alpha smooth muscle actin and desmin expression in perisinusoidal expressed by myofibroblasts during experimental wound healing. Labcells of normal and diseased human livers. Am J Pathol 1991;138:1233- Invest 1990;63:21-29.1242. 18. Bhunchet E, Wake K. Role of mesenchymal cell population in porcine
7. Ramadori G, Rieder H, Meyer zum Buschenfelde. Gene expression of serum-induced rat liver fibrosis. HEPATOLOGY 1992;16:1452-1473.smooth muscle a-actin isoform in fat storing cells of rat liver identifies 19. Friedmann SL. The molecular basis for Kupffer cell/lipocyte interaction.them as myofibroblasts. In: Wisse E, Knook DL, Decker K, eds. Cells In: Gressner AM, Ramadori G, eds. Molecular and Cell Biology of Liverof Hepatic Sinusoids. Volume 2. The Netherlands Kupffer Cell Founda- Fibrogenesis. London: Kluwer Academic, 1992:358-392.tion, 1989:464-465. 20. Peterson TC, Isbrucker RA. Fibroproliferation in liver disease: role of
8. Tanaka Y, Nouchi T, Yamane M, Irie T, Miyakawa H, Sato C, Marumo monocyte factors. HEPATOLOGY 1992;15:191-197.F. Phenotypic modulation in lipocytes in experimental liver fibrosis. J 21. Gressner AM. Cytokines and cellular crosstalk involved in the activation
of fat-storing cells. J Hepatol 1995;22(S1):28-36.Pathol 1991;164:273-278.
AID Hepa 0017 / 5p24$$$321 07-10-97 12:24:13 hepa WBS: Hepatology