hemodialysis emergencies
TRANSCRIPT
By
Kareem NagatyAssistant lecturer of internal medicine & nephrology
HEMODIALYSIS EMERGENCIES

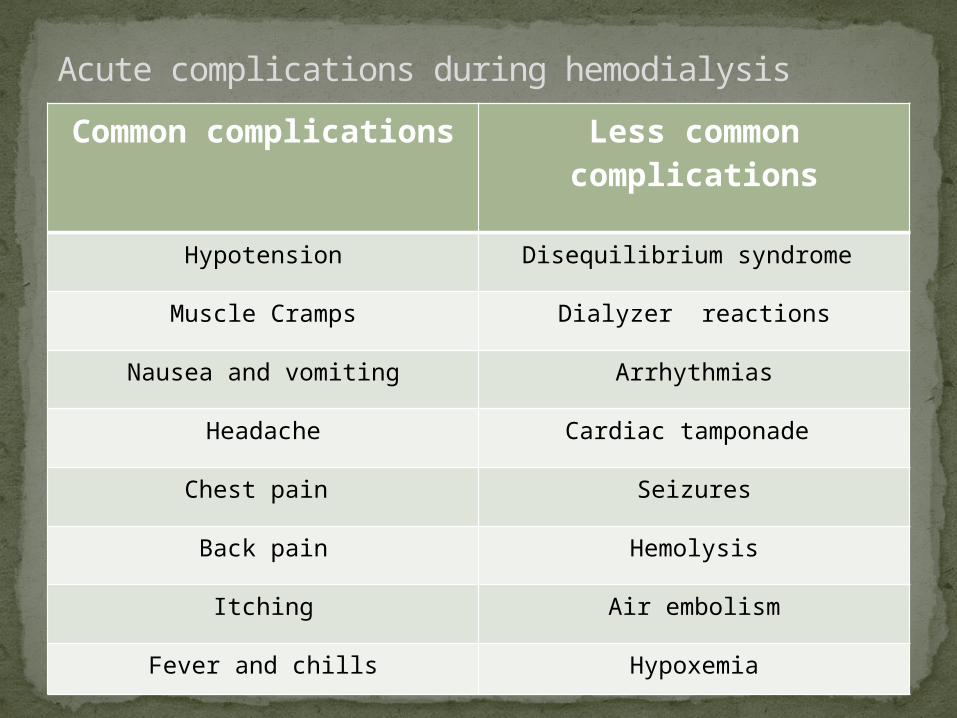
Common complications
Less common complications
Hypotension Disequilibrium syndrome
Muscle Cramps Dialyzer reactions
Nausea and vomiting Arrhythmias
Headache Cardiac tamponade
Chest pain Seizures
Back pain Hemolysis
Itching Air embolism
Fever and chills Hypoxemia
Acute complications during hemodialysis
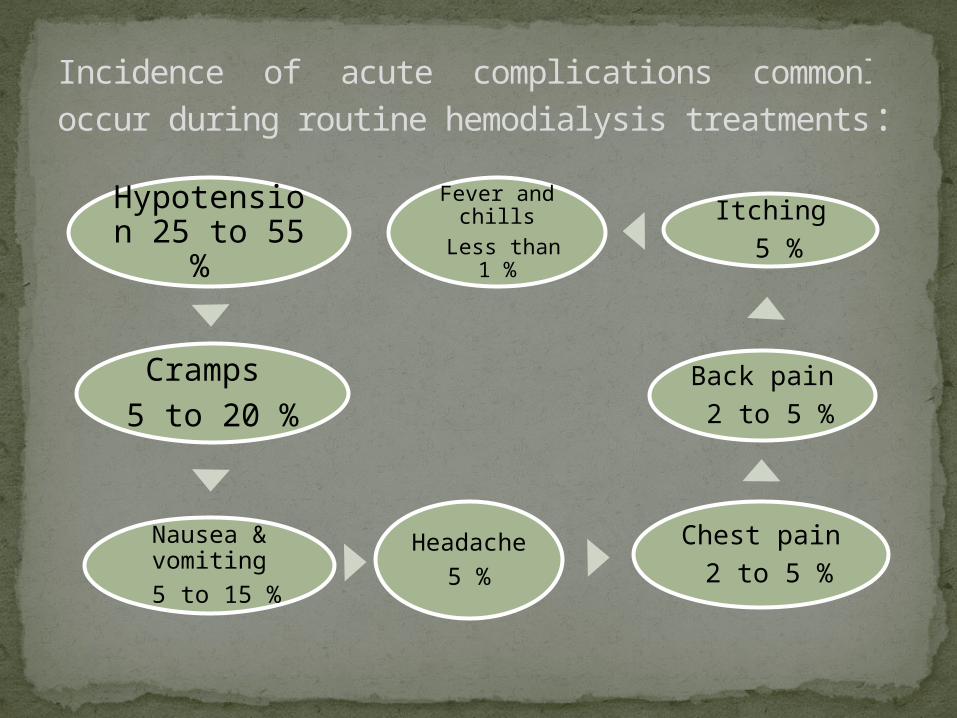
Hypotension 25 to 55
%
Cramps 5 to 20 %
Nausea & vomiting
5 to 15 %
Headache 5 %
Chest pain 2 to 5 %
Back pain 2 to 5 %
Itching 5 %
Fever and chills
Less than 1 %
Incidence of acute complications commonly occur during routine hemodialysis treatments:
Common complications
Less common complications
Hypotension Disequilibrium syndrome
Muscle Cramps Dialyzer reactions
Nausea and vomiting Arrhythmias
Headache Cardiac tamponade
Chest pain Seizures
Back pain Hemolysis
Itching Air embolism
Fever and chills Hypoxemia
Acute complications during hemodialysis
Dialysis associated hypotensio
n
Chronic persistent hypotensio
n
Intradialytic
hypotension (IDH)
Hypotension
Volume related
V.C failure
CardioVascular related
Variable causes
Causes of IDH
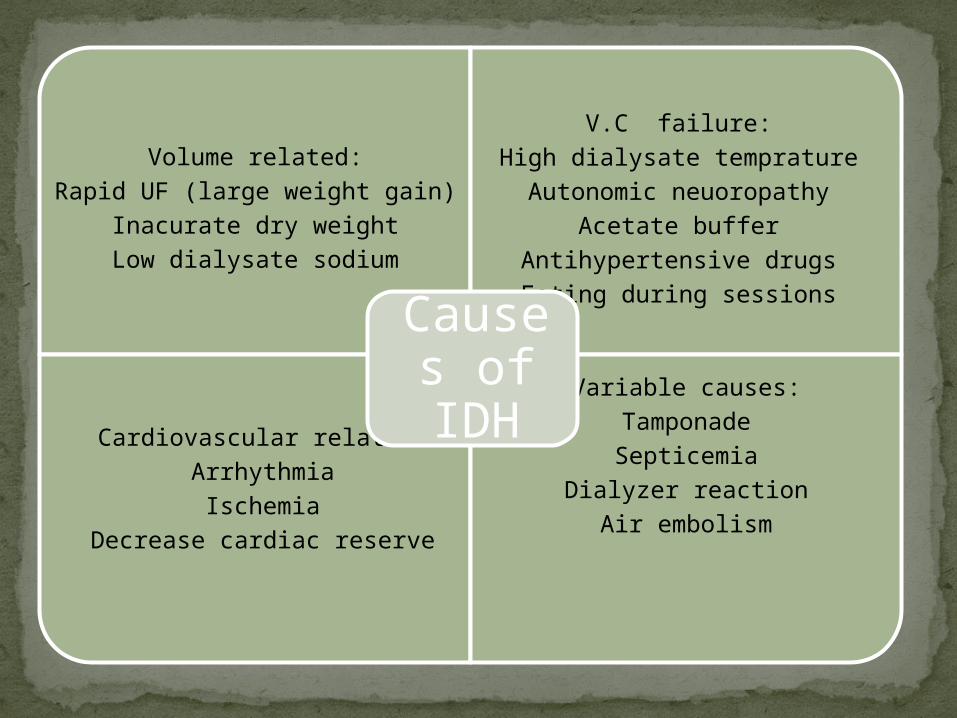
Volume related:Rapid UF (large weight gain)
Inacurate dry weightLow dialysate sodium
V.C failure:High dialysate tempratureAutonomic neuoropathy
Acetate bufferAntihypertensive drugsEating during sessions
Cardiovascular related:ArrhythmiaIschemia
Decrease cardiac reserve
Variable causes:TamponadeSepticemia
Dialyzer reactionAir embolism
Causes of IDH
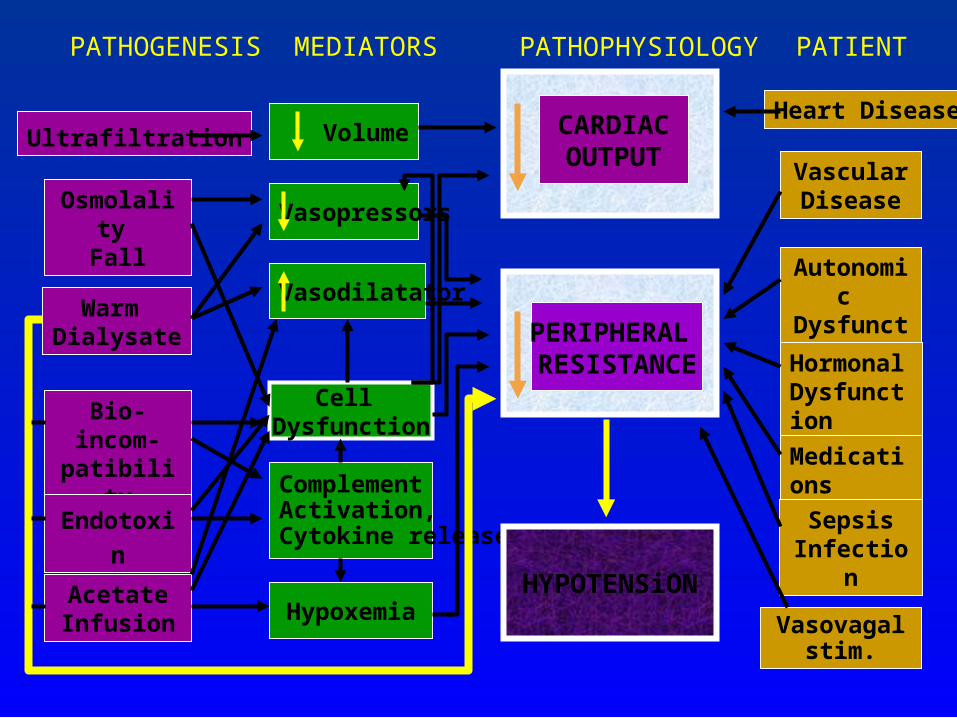
Ultrafiltration
Osmolality Fall
Warm Dialysate
Bio-incom-
patibility
Endotoxin
AcetateInfusion
Volume
Vasopressors
Vasodilatator
Cell Dysfunction
ComplementActivation, Cytokine release
Hypoxemia
Heart Disease
Vascular Disease
Autonomic
DysfunctionHormon
al DysfunctionMedications
SepsisInfection
Vasovagal stim.
HYPOTENSiON
CARDIACOUTPUT
PERIPHERAL RESISTANCE
PATHOGENESIS MEDIATORS PATHOPHYSIOLOGY PATIENT
Volume overload due to suboptimal ultrafiltration, LVH, and interdialytic hypertension.
Fistula thrombosis.
Increased mortality and morbidity.
Sequelae of frequent IDH:
TREATMENTEmergency:_Stop or decrease
rate of UF_Trendelenberg
position_Decrease blood
flow rate_I.V bolus of saline
Etiology: e.g.
_Cardiac disease_Pericardial
disease_Sepsis
Frequent & Resistant:
_Increase time or frequency of HD
_Nocturnal dialysis_Peritoneal dialysis

PREVENTION
Volume related:Rapid UF (large weight gain)
Inacurate dry weightLow dialysate sodium
V.C failure:High dialysate tempratureAutonomic neuoropathy
Acetate bufferAntihypertensive drugsEating during sessions
Cardiovascular related:ArrhythmiaIschemia
Decrease cardiac reserve
Variable causes:TamponadeSepticemia
Dialyzer reactionAir embolism
Causes of IDH
Accurate setting of the "dry weight”.Minimize interdialytic weight gain.Steady, constant ultrafiltration.Increased dialysate sodium concentration.Bicarbonate dialysate buffer.Temperature control.Improvement in cardiovascular performance.Midodrine among patients with autonomic
neuropathy.Avoidance of food ingestion during dialysis.No antihypertensive medications prior to
treatment.
PREVENTION
Accurate setting of the "dry weight”.Minimize interdialytic weight gain.Steady, constant ultrafiltration.Increased dialysate sodium concentration.Bicarbonate dialysate buffer.Temperature control.Improvement in cardiovascular performance.Midodrine among patients with autonomic
neuropathy.Avoidance of food ingestion during dialysis.No antihypertensive medications prior to
treatment.
PREVENTION
Accurate setting of the "dry weight”.Minimize interdialytic weight gain.Steady, constant ultrafiltration.Increased dialysate sodium concentration.Bicarbonate dialysate buffer.Temperature control.Improvement in cardiovascular performance.Midodrine among patients with autonomic
neuropathy.Avoidance of food ingestion during dialysis.No antihypertensive medications prior to
treatment.
PREVENTION
Accurate setting of the "dry weight”.Minimize interdialytic weight gain.Steady, constant ultrafiltration.Increased dialysate sodium concentration.Bicarbonate dialysate buffer.Temperature control.Improvement in cardiovascular performance.Midodrine among patients with autonomic
neuropathy.Avoidance of food ingestion during dialysis.No antihypertensive medications prior to
treatment.
PREVENTION
Accurate setting of the "dry weight”.Minimize interdialytic weight gain.Steady, constant ultrafiltration.Increased dialysate sodium concentration.Bicarbonate dialysate buffer.Temperature control.Improvement in cardiovascular performance.Midodrine among patients with autonomic
neuropathy.Avoidance of food ingestion during dialysis.No antihypertensive medications prior to
treatment.
PREVENTION
Accurate setting of the "dry weight”.Minimize interdialytic weight gain.Steady, constant ultrafiltration.Increased dialysate sodium concentration.Bicarbonate dialysate buffer.Temperature control.Improvement in cardiovascular performance.Midodrine among patients with autonomic
neuropathy.Avoidance of food ingestion during dialysis.No antihypertensive medications prior to
treatment.
PREVENTION
Accurate setting of the "dry weight”.Minimize interdialytic weight gain.Steady, constant ultrafiltration.Increased dialysate sodium concentration.Bicarbonate dialysate buffer.Temperature control.Improvement in cardiovascular performance.Midodrine among patients with autonomic
neuropathy.Avoidance of food ingestion during dialysis.No antihypertensive medications prior to
treatment.
PREVENTION
Accurate setting of the "dry weight”.Minimize interdialytic weight gain.Steady, constant ultrafiltration.Increased dialysate sodium concentration.Bicarbonate dialysate buffer.Temperature control.Improvement in cardiovascular performance.Midodrine among patients with autonomic
neuropathy.Avoidance of food ingestion during dialysis.No antihypertensive medications prior to
treatment.
PREVENTION
Accurate setting of the "dry weight”.Minimize interdialytic weight gain.Steady, constant ultrafiltration.Increased dialysate sodium concentration.Bicarbonate dialysate buffer.Temperature control.Improvement in cardiovascular performance.Midodrine among patients with autonomic
neuropathy.Avoidance of food ingestion during dialysis.No antihypertensive medications prior to
treatment.
PREVENTION

Accurate setting of the "dry weight”.Minimize interdialytic weight gain.Steady, constant ultrafiltration.Increased dialysate sodium concentration.Bicarbonate dialysate buffer.Temperature control.Improvement in cardiovascular performance.Midodrine among patients with autonomic
neuropathy.Avoidance of food ingestion during dialysis.No antihypertensive medications prior to
treatment.
PREVENTION
Accurate setting of the "dry weight”.Minimize interdialytic weight gain.Steady, constant ultrafiltration.Increased dialysate sodium concentration.Bicarbonate dialysate buffer.Temperature control.Improvement in cardiovascular performance.Midodrine among patients with autonomic
neuropathy.Avoidance of food ingestion during dialysis.No antihypertensive medications prior to
treatment.
PREVENTION
The 2007 European best practice guidelines in hemodialysis recommend the following stepped approach to the prevention of IDH:
First-line approach — The first-line approach includes dietary counseling (sodium restriction), no food intake during dialysis, clinical dry weight reassessment, bicarbonate as the dialysis buffer, dialysate temperature of 36.5ºC, and/or appropriate dosing and timing of antihypertensive agents.
PREVENTION
Second-line approach — The second-line approach includes objective methods to assess dry weight, cardiac evaluation, gradual reduction of dialysate temperature from 36.5ºC (lowest 35ºC), consideration of blood volume controlled feedback, increase in dialysis time and/or frequency, and/or use of a high dialysate calcium concentration.
Third-line approach — If other treatment options have failed, the guidelines recommend the third-line approach which involves consideration of midodrine or L- carnitine supplementation or peritoneal dialysis.
PREVENTION
Common complications
Less common complications
Hypotension Disequilibrium syndrome
Muscle Cramps Dialyzer reactions
Nausea and vomiting Arrhythmias
Headache Cardiac tamponade
Chest pain Seizures
Back pain Hemolysis
Itching Air embolism
Fever and chills Hypoxemia
Acute complications during hemodialysis
A cramp is a prolonged involuntary muscle contraction that occurs in a muscle which voluntarily contracts when it is already in its most shortened position.
Cramps tend to occur most frequently near the end of hemodialysis treatments.
Most commonly involve the muscles of the lower extremity, but the muscles of the hands, arms, and abdomen may also be affected. Cramps occur more often in older, nondiabetic, anxious patients. Low PTH values and high serum creatine phosphokinase concentrations are also more frequent among patients with dialysis-associated cramps
Muscle cramps
Plasma volume contraction. Hyponatremia. Tissue hypoxia. Hypomagnesemia. Carnitine deficiency. Elevated serum leptin levels.
The etiology of hemodialysis-associated cramps
The reversal of low blood pressure.
Hypertonic saline or dextrose: triple saline or 50% dextrose are equally effective.
_hypertonic saline may be preferred among those with volume depletion.
_hypertonic dextrose may be the better therapeutic option (in nondiabetic patients) because it does not adversely affect salt and water balance.
Mannitol infusion: not preferred.
Local massage of the affected muscle and the application of moist heat
TREATMENT
Minimize interdialytic weight gains.Prevention of dialysis-associated hypotension.Higher dialysate sodium concentration.Carnitine supplementation.Quinine sulfate.Vitamin E.Others.
PREVENTION
Minimize interdialytic weight gains.Prevention of dialysis-associated hypotension.Higher dialysate sodium concentration.Carnitine supplementation.Quinine sulfate.Vitamin E.Others.
PREVENTION
Minimize interdialytic weight gains.Prevention of dialysis-associated hypotension.Higher dialysate sodium concentration.Carnitine supplementation.Quinine sulfate.Vitamin E.Others.
PREVENTION
Minimize interdialytic weight gains.Prevention of dialysis-associated hypotension.Higher dialysate sodium concentration.Carnitine supplementation.Quinine sulfate.Vitamin E.Others.
PREVENTION
Minimize interdialytic weight gains.Prevention of dialysis-associated hypotension.Higher dialysate sodium concentration.Carnitine supplementation:_ Carnitine may be given intravenously (20
mg/kg) after hemodialysis or orally (330 mg two to three times per day).
Quinine sulfate.Vitamin E.Others.
PREVENTION
Minimize interdialytic weight gains.Prevention of dialysis-associated hypotension.Higher dialysate sodium concentration.Carnitine supplementation.Quinine sulfate:_decreased excitability of the motor end-plate to
nerve stimulation and increased muscle refractory period, thereby preventing prolonged involuntary muscle contraction.
_not used due to side effects.Vitamin E.Others.
PREVENTION
Minimize interdialytic weight gains.Prevention of dialysis-associated hypotension.Higher dialysate sodium concentration.Carnitine supplementation.Quinine sulfate.Vitamin E: _400 I.U alone or in combination with vitamin
C.Others.
PREVENTION
Minimize interdialytic weight gains.Prevention of dialysis-associated hypotension.Higher dialysate sodium concentration.Carnitine supplementation.Quinine sulfate.Vitamin E.Others:_short acting benzodiazepines, nifedipine ,
phenytoin , creatine monohydrate, carbamazepin , amitriptyline , and gabapentin.
_they are still under investigations.
PREVENTION
Common complications
Less common complications
Hypotension Disequilibrium syndrome
Muscle Cramps Dialyzer reactions
Nausea and vomiting Arrhythmias
Headache Cardiac tamponade
Chest pain Seizures
Back pain Hemolysis
Itching Air embolism
Fever and chills Hypoxemia
Acute complications during hemodialysis
Hypotension.
Early manifestations of Disequilibrium syndrome.
Gastroparesis (cause nausea and vomiting).
High dialysate sodium or calcium (cause nausea and vomiting).
Caffeine use (cause headache).
Metabolic disturbances: eg. hypoglycemia, hypernatremia, and hyponatremia (cause headache).
ETIOLOGY OF HEADACHE, NAUSEA, AND VOMITING
TTT of hypotension.
Detection and management of Disequilibrium syndrome.
Antiemetics: eg. Metoclopramide.
Acetaminophen.
TREATMENT
Prevention of hypotension.
Decrease dialysate sodium.
Metoclopramide: 10 mg prior to dialysis session if persistent vomiting.
A cup of coffee in heavy caffeine user suffering from headache.
Causious trial of magnesium supplementation in persistent headache.
PREVENTION
Common complications
Less common complications
Hypotension Disequilibrium syndrome
Muscle Cramps Dialyzer reactions
Nausea and vomiting Arrhythmias
Headache Cardiac tamponade
Chest pain Seizures
Back pain Hemolysis
Itching Air embolism
Fever and chills Hypoxemia
Acute complications during hemodialysis
Non-specific back pain sometimes associated with chest pain.
Chest pain may be:_mild non-specific_hypotension_ disequilibrium syndrome _angina_acute coronary syndrome_hemolysis_air embolism_pulmoary embolism
CHEST PAIN & BACK PAIN
The presence of cardiovascular disease is an important predictor of mortality in patients with ESRD.
Angina is the commonest presentation of CAD in dialysis patient.
Frequent episodes of hypotension during hemodialysis may be the presentation of CAD.
Exertional dyspnea, (intradialytic or interdialytic), sudden cardiac arrest or death, and arrhythmias are less common presentations.
Angina
There is extremely poor prognosis in dialysis patients with an acute myocardial infarction (AMI), this may be due in part to a relatively increased number of "atypical clinical presentations" resulting in underdiagnosis and undertreatment. As an example, the presence of dyspnea alone due to an acute myocardial infarction in an individual scheduled to undergo a regular chronic dialysis procedure may be mistakenly attributed to volume overload. In addition, baseline abnormalities on the electrocardiogram, such as left ventricular hypertrophy, may mask characteristic changes with ischemia.
ACUTE CORONARY SYNDROME
Extremely uncommon in dialysis patients during hemodialysis sessions.
May be observed after manipulation of thrombus or occlusion of the dialysis access.
Pulmoary embolism
Common complications
Less common complications
Hypotension Disequilibrium syndrome
Muscle Cramps Dialyzer reactions
Nausea and vomiting Arrhythmias
Headache Cardiac tamponade
Chest pain Seizures
Back pain Hemolysis
Itching Air embolism
Fever and chills Hypoxemia
Acute complications during hemodialysis
May be accompined by other minor allergic symptoms.
May be low-grade hypersensitivity to dialyzer or blood circuit components.
Antihistaminics may be given during dialysis session.
Chronic pruritis may be due to uremia, elevated phosphorus level or viral hepatitis.
Uremic pruritis may be treated by: increase dialysis dose, high flux membranes, EPO, Primrose oil or tacrolimus oint.
ITCHING
Common complications
Less common complications
Hypotension Disequilibrium syndrome
Muscle Cramps Dialyzer reactions
Nausea and vomiting Arrhythmias
Headache Cardiac tamponade
Chest pain Seizures
Back pain Hemolysis
Itching Air embolism
Fever and chills Hypoxemia
Acute complications during hemodialysis
You should seek for the source of infection.
Special consideration should be given to vascular access.
Infection control practice should be followed in hemodialysis unit.
FEVER & CHILLS
Common complications
Less common complications
Hypotension Disequilibrium syndrome
Muscle Cramps Dialyzer reactions
Nausea and vomiting Arrhythmias
Headache Cardiac tamponade
Chest pain Seizures
Back pain Hemolysis
Itching Air embolism
Fever and chills Hypoxemia
Acute complications during hemodialysis
A central nervous system disorder described in dialysis patients. It is characterized by neurologic symptoms of varying severity that are thought to be due primarily to cerebral edema.
New patients just being started on hemodialysis are at greatest risk, particularly if the BUN is markedly elevated.
Other predisposing factors include severe metabolic acidosis, older age, pediatric patients, and the presence of other central nervous system disease.
Dialysis disequilibrium syndrome
PATHOGENESIS
Reverse osmotic shift
Intracerebral acidosis
Dialysis disequilibrium syndrome
Acute symptoms develop during or immediately after hemodialysis.
Early findings include headache, nausea, disorientation, restlessness, blurred vision, and asterixis.
More severely affected patients progress to confusion, seizures, coma, and even death.
Milder signs and symptoms associated with dialysis — such as muscle cramps, anorexia, and dizziness developing near the end of a dialysis are also part of this syndrome.
CLINICAL MANIFESTATIONS
Uremia.Subdural hematoma.Cerebral infarction.Intracerebral hemorrhage.Meningitis.Metabolic disturbances (hyponatremia,
hypoglycemia).
DIFFERENTIAL DIAGNOSIS
Symptoms are self-limited and usually disappear within several hours.
Mild nonspecific symptoms, such as nausea, vomiting, or headache, is symptomatic.
Sever life thereatening symptoms: _ABC_Dialysis is stopped in the patient with seizures or coma._raising the plasma osmolality with either hypertonic
saline or 12.5 g of hypertonic mannitol. Some physicians administer 50 % dextrose solution.
TREATMENT
Prevention is the mainstay of therapy in the DDS.
A new dialysis patients with very high BUN concentrations or neurologic symptoms, The initial dialyses should be gentle:
_the initial session not more than 2 hours._low blood flow rate of 150 to 250 mL/min._small surface area dialyzer._concurrent rather than countercurrent blood and
dialysate flow._repeated daily for three or four days with gradual
increase in time and blood flow rate._marked fluid overload can be treated with ultrafiltration.
PREVENTION

Your Text Here