hematology ferinject presentation - gastro -...
TRANSCRIPT

Ferinject®

Iron Deficiency Anemia-IDAy
• IDA is the most common and widespread pnutritional disorder in the world.
• It is the only nutrient deficiency also prevelant inIt is the only nutrient deficiency also prevelant in industrial countries.
• Some disorders such as IBD are prone to• Some disorders, such as IBD, are prone to develop IDA.1/3 f th IBD’ ti t h d d Hb• 1/3 of the IBD’s patients has reduced Hb.
• Every second patient is ID.
• Kulnigg S et al. Am J Gastroenterol 2007;102:1

Factors to IDA in IBD’s patientsp
Ulcerated intestinal mucosa
IDA Chronic blood loos
Absorption impairment
Elevated hepcidinhepcidin

IDA-Symptomsy p
Fatigue
DizzinessReduced cognitive function
IDA symptoms
Hospitalization(sever cases)
ADL impairment (sever cases)impairment

Fatigue, weakness and impaired physical function adversely affect the lives and well being of your patients (Cancer)the lives and well-being of your patients (Cancer)
Fatigue has a greater impact on the life of a cancer patient than pain1
► In cancer patients, fatigue i ifi tl i t Q L2 3
80
70
Oncologist (n = 197)Patient (n = 419)
significantly impacts QoL2,3
► 61% of cancer patients
70
60
50
40
61%
37%
61%
nse
(%)
psurveyed (n=419) said that fatigue had a more substantial
40
30
20
10
19%Res
pon
effect on their daily lives than pain1
Responses to the question:
0Fatigue Pain
(Patient) Which symptom do you think affects/affected your everyday life more, pain or fatigue?
(Oncologist) Which symptom do you think affects your patients’ everyday life more pain or fatigue?
1. Vogelzang NJ et al. Semin Hemat1997;34:4,
2. Cella D et al. Semin Oncol 1998;25:43,3. Cella D. Cancer 2008;113(6):1480–8.
everyday life more, pain or fatigue?

Oral treatment100–200 mg
Oral treatment
Up to 90% of oral iron is not absorbed Oesophagus
iron
10% absorbed
LiverGallbladder
StomachStomachDuodenum
Colon
Rectum
2008AG, VerlagMED -UNIAnemia in inflammatory bowel diseases. C. Gasche

Oral iron treatment
• Easy to administer & Low cost• Easy to administer & Low cost.• Poor absorption from the gastrointestinal tract.• Gastrointestinal side effects
constipation 35%nausea 10%vomiting 8%diarrhea 6%
Variable compliance• Variable compliance.• Interaction with medications.• Interaction with food.Interaction with food.• Can’t balanced continuance iron loose.
Charytan C et al. Nephron Clin Pract 2005; 100: c55-c62

The majority of patients require at least 1 g of utilizable iron
► Post-Partum:
utilizable iron
– Van Wyck DB et al. Obstet Gynecol 2007;110:267: 1,403 mg iron
– Breymann C et al. Int J Gynaecol Obstet 2008;101:67: 1,347 mg iron
– Seid MH et al. Am J Obstet Gynecol 2008;199:435: 1,504 mg iron
► Heavy Menstrual Bleeding:– Van Wyck DB et al. Transfusion 2009;49:2719: 1,568 mg iron
► Oncology: gy– Tschechne B et al. DHGO Congress poster, Berlin 2010 1,333 mg iron
– I.V. iron other studies: 750–1,200 mg iron
► CKD:– Qunibi WY et al. Nephrol Dial Transplant 2010 (Epub ahead of print): 1,218 mg iron
► IBD:– Kulnigg S et al. Am J Gastroenterol 2007;102:1: 1,399 mg ironKulnigg S et al. Am J Gastroenterol 2007;102:1: 1,399 mg iron
IV Iron Therapy – What are we l ki f ?looking for?• Safety & effectiveness• Safety & effectiveness• Rapid correction of iron deficiency• Low toxicity• Low reactivity with molecules in blood and living
cells• No induction of oxidative stress• Minimum repeated infusion

Ferinject® – Breakthrough next generation I V irongeneration I.V. iron
FERINJECT
• Ferinject® is a stable complex free of dextran• Ferinject is a stable complex free of dextranDesigned to overcome current I.V. iron limitationslimitations
• Ferric carboxymaltose - FCML i i i l d• Low immunogenic potential and iron-induced toxicity
• Well documented safety and tolerability profile• Single dose up to 1000 mg iron in 15 minutesSingle dose up to 1000 mg iron in 15 minutes
only• No test dose required• No test dose required

FERINJECT
• Unique carbohydrate shell• Unique carbohydrate shell• Highly stable type I iron complex
f• Dextran-free• PH 5–7• Physiological osmolarity• Rapid and selective delivery from plasma toRapid and selective delivery from plasma to
RES of the liver,spleen and bone marrow.

Metabolism and toxicity of an ICCMetabolism and toxicity of an ICC
M hTransferrin
Macrophage
Iron(III)-hydroxide/oxide coreICC
Carbohydrate shell
Fe3+
Fe2+
Lysosome
e
Cyt b
Fe2+Ft
F ti
DMT1y
LIPFerroportin
Fe2+ Fe3+ TransferrinHepcidin
CeruloplasminDMT1: Divalent metal transporter 1; LIP: labile iron pool; Ft: ferritin.

Ferinject® provides a more rapid correction of iron deficiency compared with oral iron (IBD)deficiency compared with oral iron (IBD)
Ferinject® (n=136)100
80 p-values for difference:
Oral iron (n=60)
nder
s (%
)
60
p values for difference:
•Week 2: p=0.0051
•Week 4: p=0.0346
•Kaplan-Meier analysis
Res
pon
40
20
yof cumulative Hb
responder rate: treatment comparison,
log-rank test: 0.000920
0Week 4Week 2Baseline
VisitWeek 8 Week 12
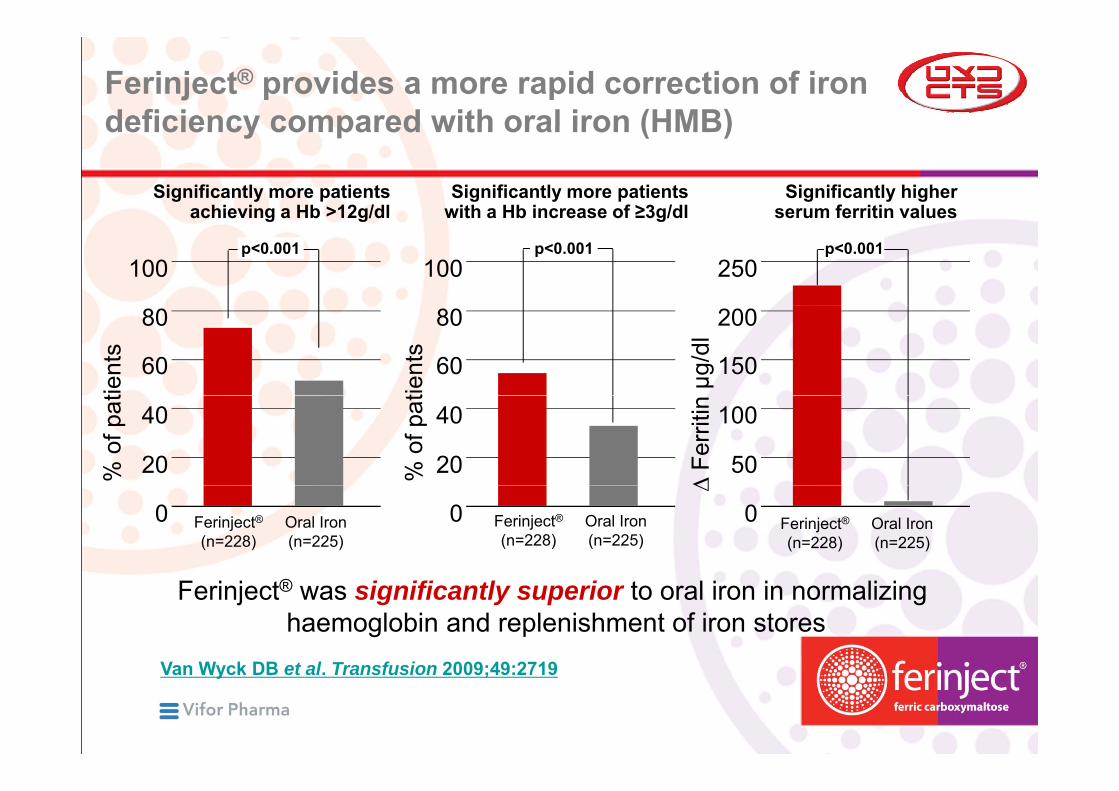
Ferinject® provides a more rapid correction of iron deficiency compared with oral iron (HMB)deficiency compared with oral iron (HMB)
Significantly more patients with a Hb increase of ≥3g/dl
Significantly more patients achieving a Hb >12g/dl
Significantly higher serum ferritin values
100p<0.001
with a Hb increase of ≥3g/dl
100p<0.001
achieving a Hb >12g/dl
250p<0.001
serum ferritin values
80
60
tient
s
80
60
tient
s
200
150µg/d
l
40
20% o
f pat40
20% o
f pat 100
50
∆ Fe
rriti
n
00 Ferinject®(n=228)
Oral Iron(n=225)
0
∆
Ferinject®(n=228)
Oral Iron(n=225)
Ferinject®(n=228)
Oral Iron(n=225)
Ferinject® was significantly superior to oral iron in normalizing haemoglobin and replenishment of iron stores
2719492009T f it lDBW kV 2719:49;2009Transfusion . et alDB WyckVan

Only 1–2 injections of Ferinject®
needed in > 90% of patients1needed in > 90% of patients1
80
60
70
ient
s % 50
60
30
Pat
30
20
1 injection
0
10
Clinical Profile: Anaemia in postpartum
1 injection2 injection3 injections
1 van Wyck DB, 2007y

Ferinject® has a good and well documented safety and tolerability profiletolerability profile
Well tolerated even at single doses up to 1,000 mg iron
vent
s
Well tolerated even at single doses up to 1,000 mg iron
12
10Ferinject® (n=1968) Oral iron (n=834)
vers
e dr
ug e
v 10
8
ents
with
adv 6
4
% p
atie
Headache Nausea Decreased Rash Increased Dizziness Local AbdominalConstipation Abdominal Diarrhoea Faeces Vomiting
2
0Headache Nausea Decreased
serum phosphorus
Rash Increasedalanine
aminotransferase
Dizziness Local injection
site reaction
Abdominal pain
Constipation Abdominal pain
upper
Diarrhoea Faeces discoloured
Vomiting
Qunibi W. ERA-EDTA Congress poster 2008, SwedenL seng Williamson KA & Keating GM Dr gs 2009 69(6) 739
Ferinject® cumulative doses ≥1,000 mg iron in 88% of patients (n =1,736)
Lyseng-Williamson KA & Keating GM. Drugs. 2009;69(6):739
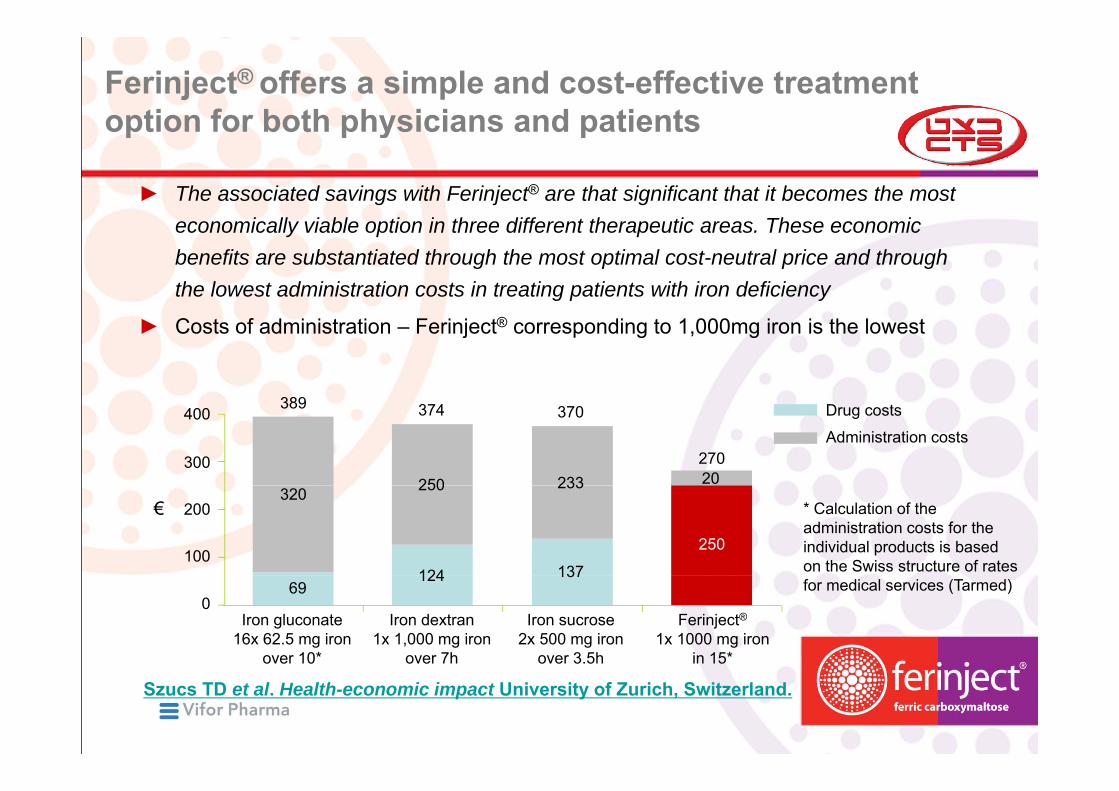
Ferinject® offers a simple and cost-effective treatment option for both physicians and patientsoption for both physicians and patients
► The associated savings with Ferinject® are that significant that it becomes the most economically viable option in three different therapeutic areas. These economic benefits are substantiated through the most optimal cost-neutral price and through the lowest administration costs in treating patients with iron deficiency
► Costs of administration – Ferinject® corresponding to 1,000mg iron is the lowest
400
300
389 374
250
370
23327020
Drug costs
Administration costs
200
100
€320 250
124
233
137
250
* Calculation of the administration costs for the individual products is based on the Swiss structure of rates
069
124 137for medical services (Tarmed)
Iron gluconate16x 62.5 mg iron
over 10*
Iron dextran1x 1,000 mg iron
over 7h
Iron sucrose2x 500 mg iron
over 3.5h
Ferinject®1x 1000 mg iron
in 15*
Szucs TD et al. Health-economic impact University of Zurich, Switzerland.

Ferinject® – Minimal intervention,maximum impactmaximum impact
High dose drip infusions
single dose up to 1000 mg ironin 15 minutes onlyin 15 minutes onlyno test dose required
500 mg (10 ml)concentration 50 mg iron/ml


Thank youThank you