helen presentation for upload
TRANSCRIPT

Translating research findings into improved
outcomes for those affected by Rett syndrome:
where are we in this journey?
Professor Helen Leonard
Telethon Institute for Child Health Research
Perth, Western Australia
Sunshine Coast March 2014
Dedicated to Dr Athel Hockey

A Progressive Syndrome of Autism, Dementia,
Ataxia, and Loss of Purposeful Hand Use in
Girls: Rett’s Syndrome: Report of 35 CasesBengt Hagberg, MD, Jean Aicardi MD,Karin Dias, MD, and Ovidio Ramos MD
Thirty-five patients, exclusively girls, from three countries had a uniform and striking progressive encephalopathy. After
normal general and psychomotor development up to the age of 7 to 18 months, developmental stagnation occurred,
followed by rapid deterioration of higher brain functions. Within one-and-a-half years this deterioration led to severe
dementia, autism, loss of purposeful use of the hands, jerky truncal ataxia, and acquired microcephaly. The destructive
stage was followed by apparent stability lasting through decades. Additional insidious neurological abnormalities
supervened, mainly spastic parapareses, vasomotor disturbances of the lower limbs, and epilepsy. Prior extensive
laboratory investigations have not revealed the cause. The condition is similar to a virtually overlooked syndrome
described by Rett in the German literature. The exclusive involvement of females, correlated with findings in family data
analyses, suggests a dominant mutation on one X chromosome that results in affected girls and nonviable male
hemizygous conceptuses.
Hagberg B, Aicardi J, Dias K, Ramos 0: A progressive syndrome of autism, dementia, ataxia, and loss of
purposeful hand use in girls: Rett’s syndrome: report of 35 cases. Ann Neurol 14:471-479, 1983

The pathway for a child with Rett syndrome in 2014
• When a girl today in 2014 develops the tell-tale symptoms articulated by Hagberg in 1983
• What will the pathway be for this child?
• What will be the influence of the Rett research journey on the future pathway for this child and her family?

What do families want to know?
What is the cause?
What do we do now?
What is her future?
Will she walk?
Will she talk?
What is the best therapy?
Will she get epilepsy?
Which specialists should
we see?
What is the best sort of
school?
How can we best use
functional abilities in daily
life?
Is there a suitable respite
available?
How can we support our
teenager making
friendships?
How can we plan for her
future day activity and
medical care needs?
What are the ingredients for a good
quality of life?
How can we support her physical
wellbeing and social contacts?
How can we support independent
living?

What are other important questions for families and clinicians?
• What determines why girls and women with Rett syndrome, although sharing many symptoms, can be very different from one other?
• How can we modify/improve the clinical course by making changes to the environment or by implementing medical treatments and interventions?

Imagine
And so what has changed over these 40 years in terms of:
Cause
Diagnosis
Understanding variability
Clinical course
Management
Quality of life
Life expectancy

Model of Research Translation
Researchers &
Knowledge
Users
Knowledge
exchange
Creation of
Questions &
Methods
Consultation
with
stakeholders
Partnerships
formed with
collaborators and
stakeholders
Literature
Research forums
Research
ProcessContinued
engagement/
relationship
management
Ongoing
reporting to
stakeholders
Feedback
processes
Knowledge
from
research
findings
Dissemination of
knowledge
Publications &
Conference
Presentations
Public
seminars/
Info sessions
Social &
other media
Plain
language
summaries
Stakeholder
feedback
ImpactsInfluencing
subsequent
rounds of
research
Communicating
the impacts of
our research
Evaluation of research
implementation
Implementation
of knowledge
Apply the
knowledge
we gain to
tackle health
challenges
Patents
Guidelines
Clinical practice
New drugs
Service provision
Policy
Implications of
knowledgeDetermine how this
knowledge could
make a difference
Work with stakeholders
to determine Contextual
relevance of knowledge
Discovery
• Pathway populated by many people
• Researchers cannot work in isolation from
each other or the community
• End-point of any research is to bring benefit
to population under study

Andreas Rett•First description of 22 girls by Andreas Rett
Presentation in 1980 in Manchester led to a joint French, Swedish, Portuguese publication in Annals of Neurology in 1983
The Rett Syndrome Journey
1966
Vienna Criteria
• First Clinical Criteria for Diagnosis of Rett syndrome
1983 1985 1988 1993 1995
Establishment of the Australian Rett syndrome study
Hagberg’s variant model

Identification of the genetic cause of Rettsyndromea mutation in the MECP2 gene
The Rett Syndrome Journey
201420102007200320021999
Establishment of InterRettReversal of Rett syndrome in a mouse model
Rett Syndrome: Revised Diagnostic Criteria and Nomenclature
Families in Australia and around the world participating in researchChildren with Rett syndrome being diagnosed earlierMore known about the clinical variationBetter management through the development of guidelines


Understanding the Biological Cause:Serendipity or not
Kankirawatana P, Leonard H, Ellaway C, Scurlock J, Mansour A, Makris CM, Dure LS,
Friez M, Lane J, Kiraly-Borri C, Fabian V, Davis M, Jackson J, Christodoulou J,
Kaufmann WE, Ravine D, Percy AK. Early progressive encephalopathy in boys
and MECP2 mutations.Neurology. 2006;67(1):164-6.
Zhang J, Bao X, Cao G, Jiang S, Zhu X, Lu H, Jia L, Pan H, Fehr S, Davis M,
Leonard H, Ravine D, Wu X. What does the nature of the MECP2 mutation tell us
about parental origin and recurrence risk in Rett syndrome?
Clinical Genetics. 2012;82(6):526-33.

Understanding the Biological Cause:What has been achieved?
•
Cheadle JP, Gill H, Fleming N, Maynard J, Kerr A, Leonard H, Krawczak M, Cooper DN, Lynch S, Thomas N, Hughes H, Hulten M, Ravine D, Sampson JR, Clarke A. Long-read sequence analysis of the MECP2 gene in Rett syndrome patients: correlation of disease severity with mutation type and location (vol 9, pg 1119, 2000). Human Molecular Genetics. 2000;9(11):1717-.

Implications for familiesWhat has been achieved?
• We know the cause of Rett syndrome for the majority
• Most children with Rett syndrome in developed countries are being diagnosed earlier
• What does that mean for families –depending on where they live
• US, Europe, Australia, China

Diagnosis: What do families say?
Delay in diagnosis is a source of stress• “Because she is atypical we did not get a diagnosis until she was about 6 years old.
This caused anguish for us as parents.”
• Having a diagnosis
• Helped families understand the cause of their child’s illness (even after the child had died)• “We now know how to deal with each symptom of the disorder that appears as she grows. If
we didn't have a diagnosis, the constant stereotypes and breath holding would be more difficult and scary to watch”
• Facilitated access to appropriate services and management• “Rett syndrome has opened up a number of avenues of support (which is fantastic) including
automatic inclusion into programs such as Very Special Kids. Since diagnosis the level of respite and case management has improved dramatically.”
Leonard H, Davis MR, Turbett GR, Laing NG, Bower C, Ravine D. Effectiveness of posthumous molecular diagnosis from a kept baby tooth. Lancet 2005;366(9496):1584-1584.

The Diagnostic Odyssey to Rett Syndrome:The Experience of an Australian Family
• My daughter was eventually diagnosed with the neurologicaldisorder Rett syndrome a month after her 3rd birthday. For over ayear prior to diagnosis, she had been tested for a range of genetic andmetabolic disorders that I just knew she didn’t have at considerable costto the health system.
• Unfortunately, at the time, specialists we consulted were not up to date with thevariances of clinical symptoms in girls suffering with Rett syndromeand they were persistent in looking to other disorders for answers.
• Doctors refused to test for Rett syndrome because
• Head growth hadn’t decelerated
• Normal stature
• Physically delayed at 6 months
• Hand mouthing rather than stereotypies
Knott M, Leonard H, Downs J. The diagnostic odyssey to Rett syndrome: The experience of an Australian family. American Journal of Medical Genetics Part A. 2012;158A(1):10-2.

The Diagnostic Odyssey to Rett Syndrome:The Experience of an Australian Family
Key messages
• Families often experience considerable frustration during the process of reaching the diagnosis
• Clinicians need to be aware of the range of presentations
• Families and clinicians need to be working partners at the time of diagnosis and beyond
• Family perspectives need to inform clinical pathways
• Achieving a diagnosis can bring benefit to the family in short and long term
“Knowledge is Power”
Knott M, Leonard H, Downs J. The diagnostic odyssey to Rett syndrome: The experience of an Australian family. American Journal of Medical Genetics Part A. 2012;158A(1):10-2.

What has and has not been achieved?
• The age at diagnosis decreased from a median
of 4.5 years before 1999 to 3.5 years afterward
• There is a small percentage of children in whom a genetic cause
has not been identified
• Children with certain groups of MECP2 mutations may be being
missed and not diagnosed till they are older

Relationship between mutation type & age when diagnosed
0
10
20
30
40
50
60
Fehr S, Bebbington A, Ellaway C, Rowe P, Leonard H, Downs J. Altered attainment of developmental milestones influences the age of diagnosis of Rett syndrome.Journal of Child Neurology 2011;26(8):980-7.

And does it matter where in the world you live?
Lim F, Downs J, Li J, Bao X, Leonard H. Barriers to diagnosis of a rare neurological disorder in China—Lived experiences of Rett syndrome families. American Journal of Medical Genetics Part A. 2012;158A:1-9.

The next three issues
• What determines the variabilityin the clinical presentation of Rett syndrome?
• What are the common medical complications?
• How can we modify/improve the clinical course by medical, environmental or other interventions?
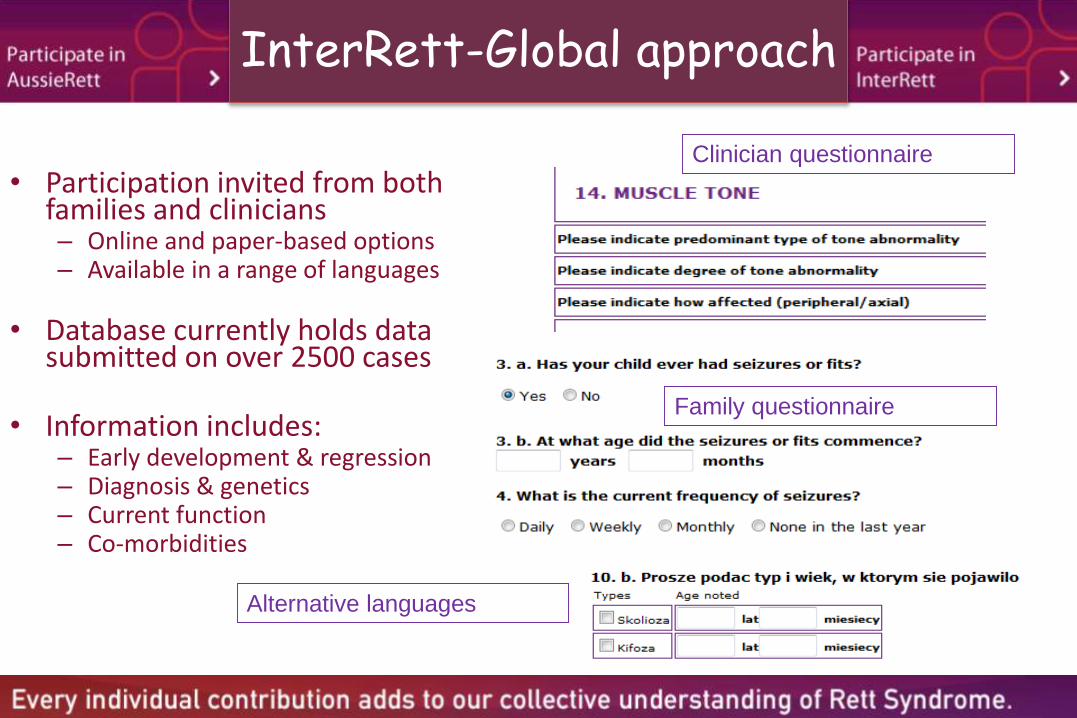
InterRett-Global approach
• Participation invited from both families and clinicians– Online and paper-based options– Available in a range of languages
• Database currently holds data submitted on over 2500 cases
• Information includes:– Early development & regression– Diagnosis & genetics– Current function– Co-morbidities
Clinician questionnaire
Alternative languages
Family questionnaire

What has and is being achieved through working together collaboratively
•

Understanding clinical variabilityWhat has been achieved?
Louise S, Fyfe S, Bebbington A, Bahi-Buisson N, Anderson A, Pineda M, Percy A, Ben Zeev B, Wu XR, Bao XH, MacLeod PM, Armstrong J, Leonard H. InterRett, a model for international data collection in a rare genetic disorder. Research in Autism Spectrum Disorders. 2009;3(3):639-59.
Argen&na
Austria
Canada
China
France
Germany
Greece
Hong6Kong
Ireland
Israel
Mexico
New6Zealand
Other6Countries
Spain
The6Netherlands
UK
USA
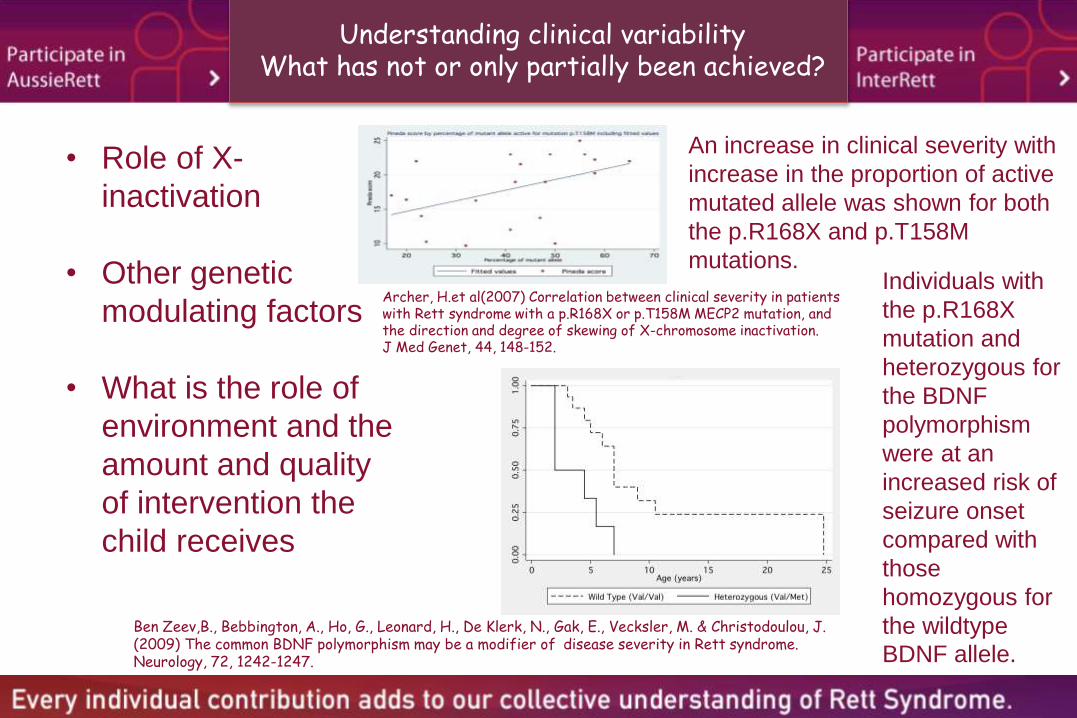
Understanding clinical variabilityWhat has not or only partially been achieved?
• Role of X-
inactivation
• Other genetic
modulating factors
• What is the role of
environment and the
amount and quality
of intervention the
child receives
An increase in clinical severity with
increase in the proportion of active
mutated allele was shown for both
the p.R168X and p.T158M
mutations.
Individuals with
the p.R168X
mutation and
heterozygous for
the BDNF
polymorphism
were at an
increased risk of
seizure onset
compared with
those
homozygous for
the wildtype
BDNF allele.
Ben Zeev,B., Bebbington, A., Ho, G., Leonard, H., De Klerk, N., Gak, E., Vecksler, M. & Christodoulou, J. (2009) The common BDNF polymorphism may be a modifier of disease severity in Rett syndrome. Neurology, 72, 1242-1247.
Archer, H.et al(2007) Correlation between clinical severity in patients with Rett syndrome with a p.R168X or p.T158M MECP2 mutation, and the direction and degree of skewing of X-chromosome inactivation. J Med Genet, 44, 148-152.

Functional abilities: general gross motorZ scores by age-group
-0.8
-0.6
-0.4
-0.2
0
0.2
0.4
0.6
0.8
<8 years 8<13 years 13<19 years >19 years
Z s
co
re
Downs et al. Mobility profile in Rett syndrome as determined by video analysis. Neuropediatrics 2008;39(4):205-210.

Mobility by mutation

Functional abilities: hand function by age-group
0.1
1
10
<8 years 8<13 years 13<19 years >19 years
Od
ds r
ati
o
Downs et al. Level of purposeful hand function as a marker of clinical severity in Rett syndrome. Developmental Medicine & Child Neurology 2010 ;52(9):817-23.
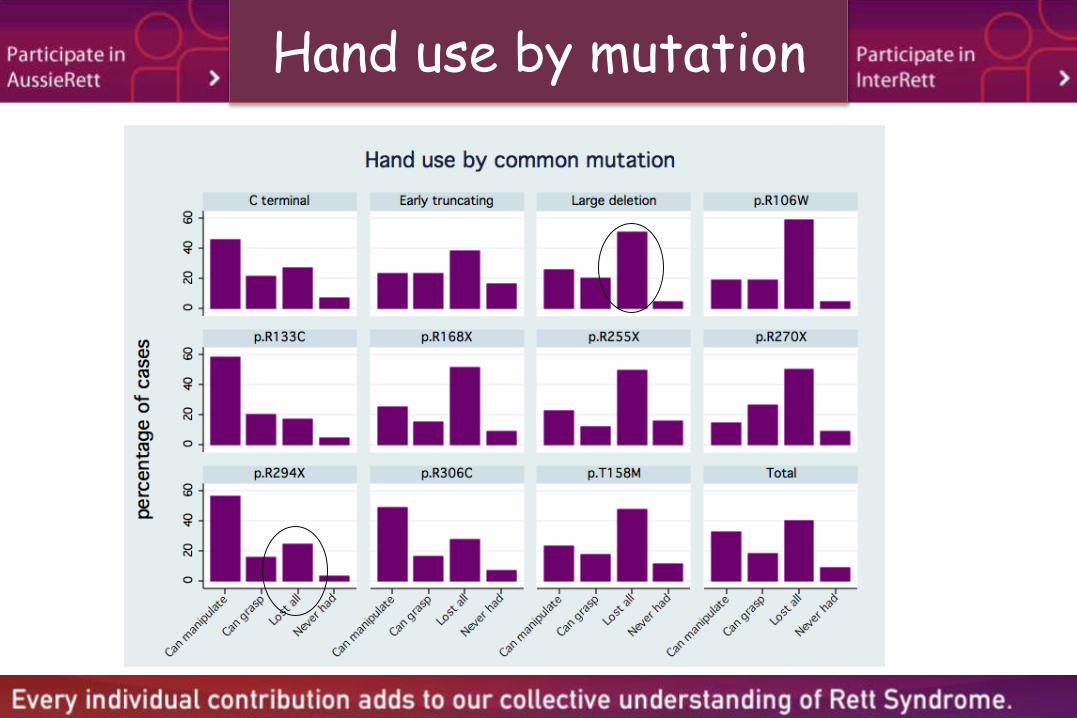
hand-use_purple.gph
Hand use by mutation
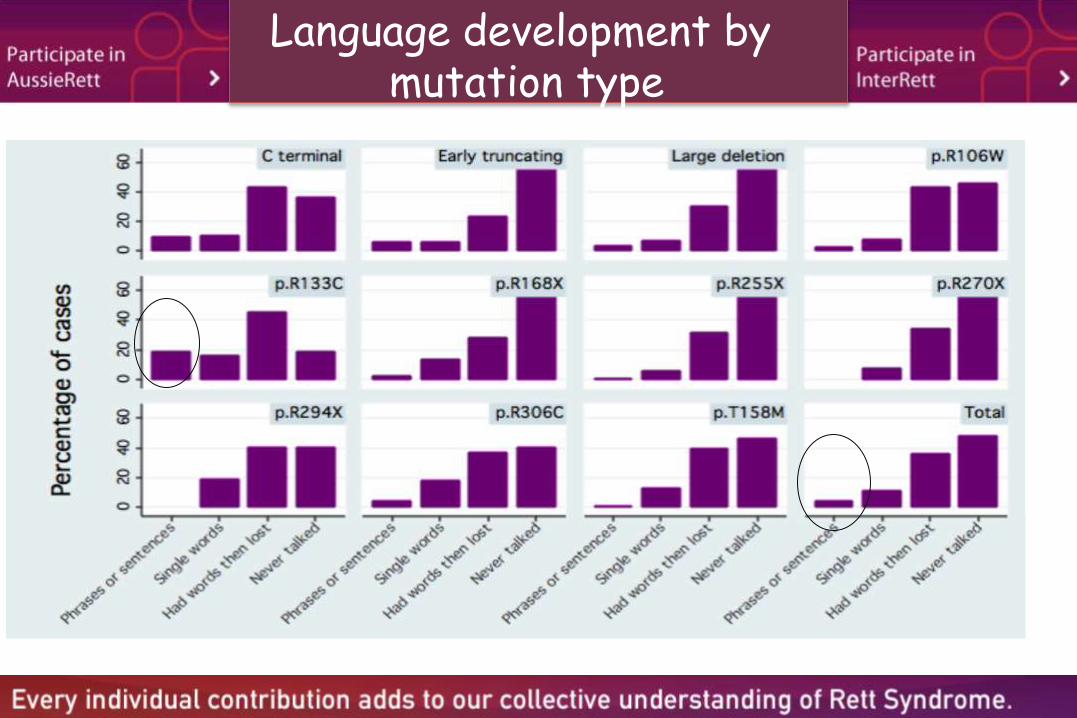
Language development by mutation type

Scoliosis
Fracture
Epilepsy
Sleep
Behavioural disturbance
Breathing abnormalities
Poor growth
Medical Issues

Scoliosis: risk of onset by mutation
0.1
1
10
p.R29
4X
p.R30
6C
p.R13
3C
C-ter
min
al d
elet
ions
p.T15
8M
p.R16
8X
p.R25
5X
p.R27
0X
Large
genom
ic d
elet
ions
Haza
rd R
ati
o
Ager et al. Predictors of scoliosis in Rett syndrome. Journal of Child Neurology, 2006, 21 (9): 809-813.
• Three quarters had
developed scoliosis by 13
years of age
• Median age at onset 9.80
years
• Earlier onset associated
with
a) compromised early
development
b) poor mobility at 10
months
c) never walking
• p.R294X mutation
provided some protective
effect

What do we know, have learned about fractures in Rett syndrome
84 (ex 236) fractured at least once
32 had more than one fracture (maximum 9)
151 fracture episodes
Fracture Incidence Rates
43.3/1000 py - Rett
11.4/1000 py - General Population
(females <20yrs – Cooley & Jones)
Downs et al. Early Determinants of Fractures in Rett Syndromein Rett syndrome. Pediatrics 2008 ; 121: 540-546.

Association of fracture rate with mutation type in Rett syndrome
0.1
1
10
100
Hazard
Ratio
Downs et al. Fractures in Rett syndrome. Pediatrics 2008 ; 121:540-546.
• Fracture risk was
increased
specifically in
cases with
p.R270X and in
cases with
p.R168X
mutations.
• Epilepsy also
increased fracture
risk, even after
adjustment for
genotype.
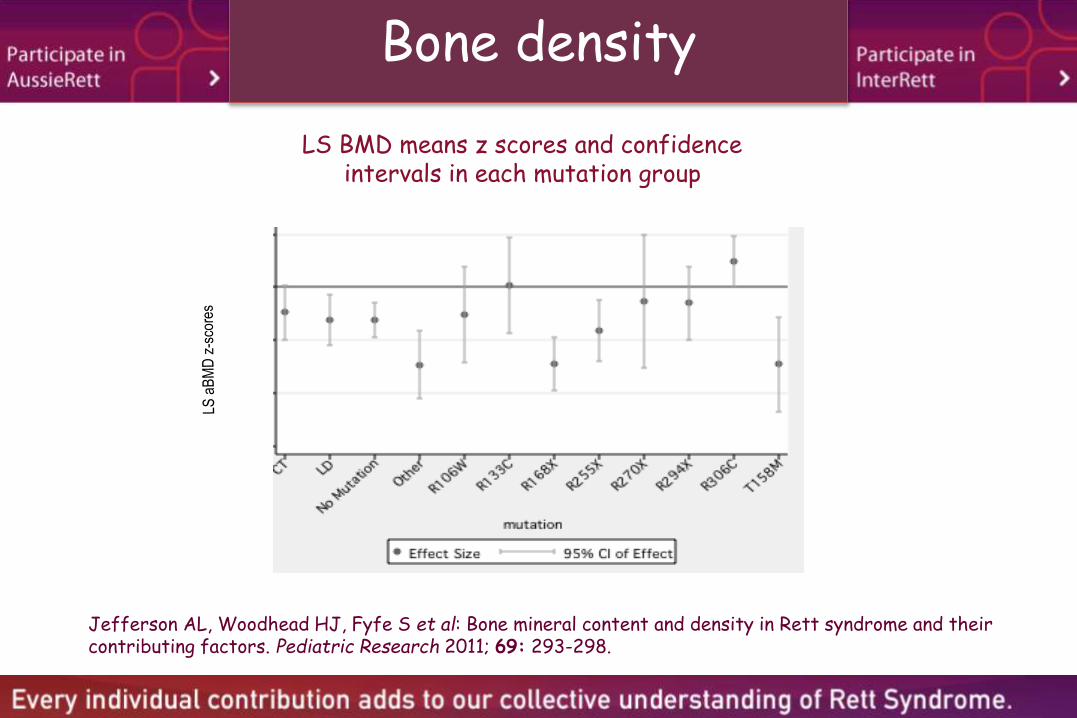
Bone density
LS BMD means z scores and confidence intervals in each mutation group
Jefferson AL, Woodhead HJ, Fyfe S et al: Bone mineral content and density in Rett syndrome and their contributing factors. Pediatric Research 2011; 69: 293-298.

Need for Bone Health Guidelines in Rett syndrome
• High risk of osteoporosis and 4 times the rate
of fracture
• Risk of fracture increased with
• Presence of epilepsy, the p.R168X or p.R270X
mutation in Rett syndrome
• Prior fracture
• Vitamin D insufficiency, physical inactivity, poor
balance and muscle weakness as in the general
population
• No current intervention studies
Creation of
Questions &
Methods
Consultation
with
stakeholders
Partnerships
formed with
collaborators
and
stakeholders
Literature
Research forums

What are we doing?
• Current longitudinal study of factors affecting bone mineral density and fracture in Rett syndrome
• Developing guidelines using combination of literature review, consultations with consumers, findings of ongoing studies and an expert panel
• Will consider prevention, screening, monitoring and management

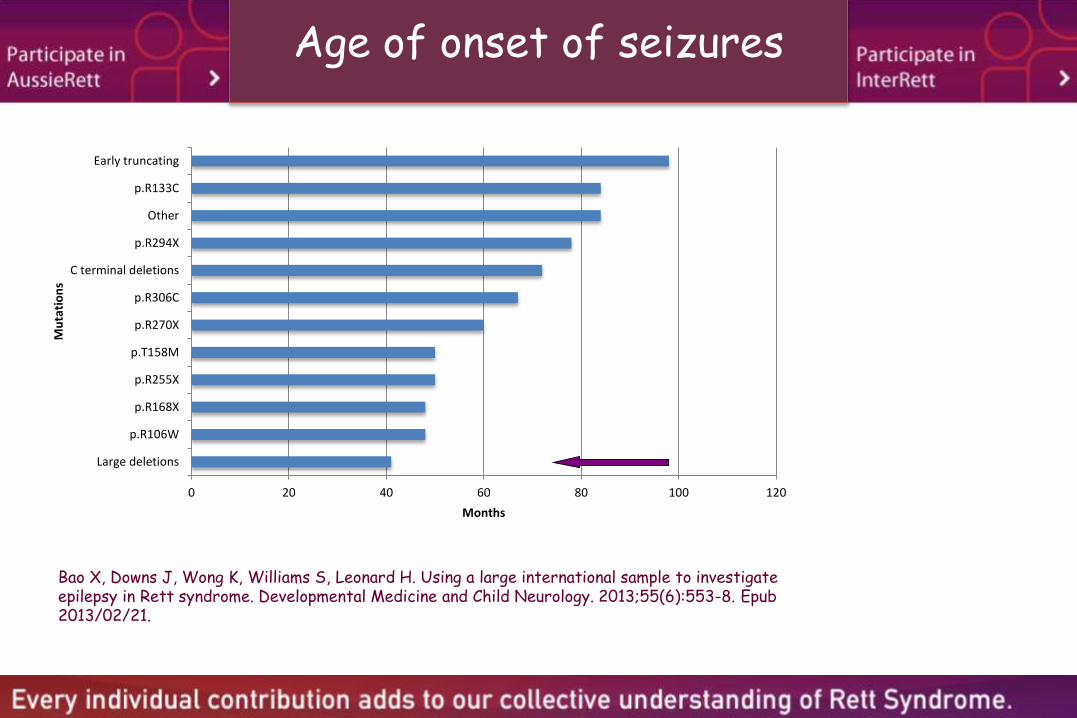
Seizures: What have we learned?
• Median age of onset of seizures
• Age of onset varies by mutation type
0 20 40 60 80 100 120
Large deletions
p.R106W
p.R168X
p.R255X
p.T158M
p.R270X
p.R306C
C terminal deletions
p.R294X
Other
p.R133C
Early truncating
Months
Mu
tati
on
sAge of onset of seizures
Bao X, Downs J, Wong K, Williams S, Leonard H. Using a large international sample to investigate epilepsy in Rett syndrome. Developmental Medicine and Child Neurology. 2013;55(6):553-8. Epub2013/02/21.

What happens to seizures with age?
0.1
1
10
100
<7 years 7<12 years 12<17 years >17 years
Se
izu
re r
ate
ra
tio
Jian et al. Seizures in Rett syndrome: an overview from a one-year calendar study. European Journal of Paediatric Neurology 2007;11(5):310-7.

Are seizures related to mutation type?
Bao X, Downs J, Wong K, Williams S, Leonard H. Using a large international sample to investigate epilepsy in Rett syndrome. Developmental Medicine and Child Neurology. 2013;55(6):553-8. Epub 2013/02/21.
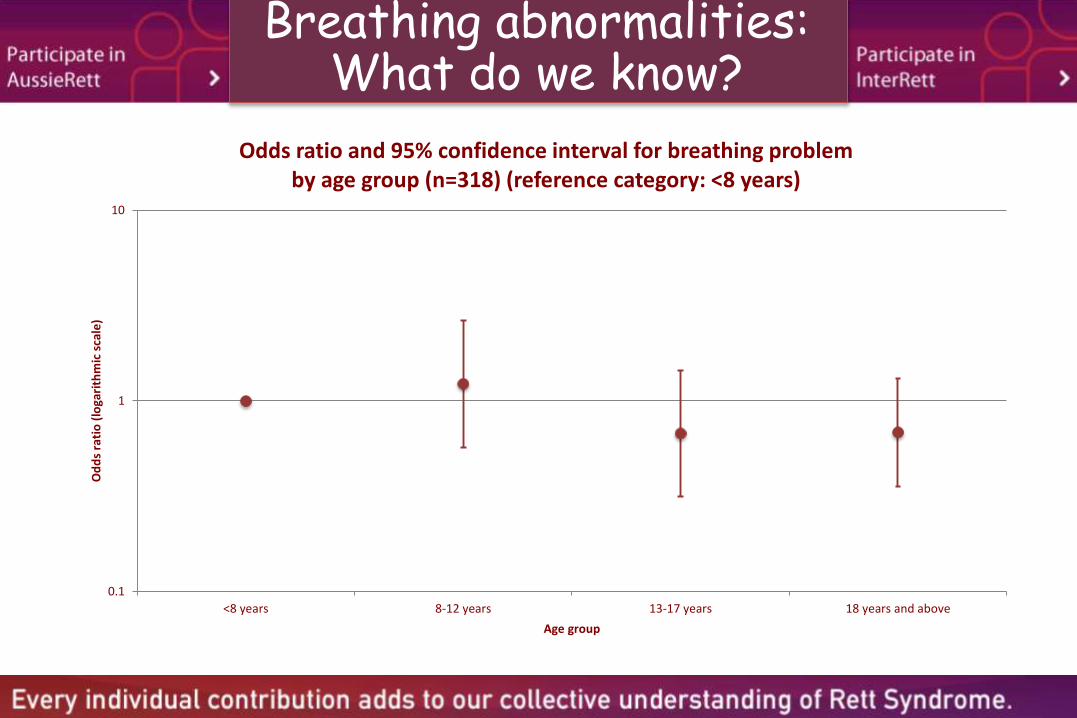
Breathing abnormalities: What do we know?
0.1
1
10
<8 years 8-12 years 13-17 years 18 years and above
Od
ds
rati
o (
loga
rith
mic
sca
le)
Age group
Odds ratio and 95% confidence interval for breathing problemby age group (n=318) (reference category: <8 years)

Breathing abnormalities: What do we know?
0.1
1
10
100
C-terminaldeletions
Earlytruncating
Large deletions p.R106W p.R133C p.R168X p.R255X p.R270X p.R294X p.R306C p.T158M
Od
ds
rati
o (
loga
rith
mic
sca
le)
Mutation type
Adjusted odds ratio and 95% confidence interval for breathing problemby mutation type (n=198) (reference category: p.R133C)

Improved life expectancy over time
Freilinger M, Bebbington A, Lanator I, De Klerk N, Dunkler D, Seidl R, Leonard H, Ronen GM. Survival with Rett syndrome: comparing Rett's original sample with data from the Australian Rett syndrome Database. Developmental Medicine and Child Neurology. 2010;52(10):962-5.

Pervasive disorder of growth
Contributing factors
• Feeding difficulties
• Oromotor dysfunction
• Other digestive tract disorders
• Additional neurological complexities
• Increased energy requirements

Feeding difficulties and poor growth
• Difficulty in maintaining growth is one of the core features of Rett
syndrome

Pervasive disorder of growth

Concern about food intake by age group

Concern about food intake according to mutation type

Enteral (Peg) feeding as an option
• Progressive decline in height, weight and body mass index (BMI) z- scores in Rett syndrome
• Likely influenced by mutation type (e.g. C-terminal deletions were more likely to have a normal weight.)
• Gastrostomy is therefore a clear option
• Approximately one quarter of subjects in the Australian cohort are receiving enteral nutritional support
Oddy WH, Webb KG, Baikie G, Thompson SM, Reilly S, Fyfe SD, Young D, Anderson AM, Leonard H. Feeding experiences and growth status in a Rett syndrome population. Journal of Pediatric Gastroenterology and Nutrition. 2007;45(5):582-90.
Bebbington A, Percy A, Christodoulou J, Ravine D, Ho G, Jacoby P, Anderson A, Pineda M, Ben Zeev B, Bahi-Buisson N, Smeets E, Leonard H. Updating the profile of C-terminal MECP2 deletions in Rett syndrome. Journal of Medical Genetics. 2010;47(4):242-8.
Tarquinio D, Motil K, Hou W, Lee H, Glaze D, Skinner S, Neul J, Annese F, McNair L, Barrish J, Geerts S, Lane J, Percy A. Reference growth standards in Rett syndrome. Neurology. 2012 79(16):1653-61.

Type of feeding by mutation type

Model of Research Translation
Researchers &
Knowledge Users
Knowledge
exchange
Creation of
Questions &
Methods
Consultation
with
stakeholders
Partnerships
formed with
collaborators and
stakeholders
Literature
Research forums
Research
ProcessContinued
engagement/
relationship
management
Ongoing
reporting to
stakeholders
Feedback
processes
Knowledge
from
research
findings
Dissemination of
knowledge
Publications &
Conference
Presentations
Public
seminars/
Info sessions
Social & other
media
Plain language
summaries
Stakeholder
feedback
ImpactsInfluencing
subsequent
rounds of
research
Communicating
the impacts of
our research
Evaluation of research
implementation
Implementation
of knowledge
Apply the
knowledge
we gain to
tackle health
challenges
Patents
Guidelines
Clinical practice
New drugs
Service provision
Policy
Implications of
knowledgeDetermine how this
knowledge could make
a difference
Work with stakeholders to
determine Contextual
relevance of knowledge

GI guideline project –initial groundwork
• Literature review• Search and key words included combinations of Rett syndrome,
cerebral palsy, developmental disability, intellectual disability, co-morbidity, gastrointestinal, growth and feeding.
• Limited to full papers in English from 1986 to 2011.
• Statements relevant to the clinical assessment and management of poor growth in Rett syndrome were extracted from the full text.
• Parent-reported information• Rettnet, an online email information interchange for parents/persons
with a Rett syndrome interest, was used to collect parent and caregiver perspectives on poor growth and contributing factors such as calorie intake and feeding difficulties.
• Postings from January 2008 to March 2009 were extracted and reviewed.
Research
ProcessContinued
engagement/
relationship
management
Ongoing
reporting to
stakeholders
Feedback
processes
Creation of
Questions &
Methods
Consultation
with
stakeholders
Partnerships
formed with
collaborators
and
stakeholders
Literature
Research forums

Recruitment
Profession Number
Child neurologist 7
Gastroenterologist 6
Clinical geneticist 4
Paediatrician 3
Physiotherapist/ occupational therapist 2
Speech pathologist 2
Others 3
• We contacted 57 clinicians from across the world• 38 recruited, from USA, Australia, UK, Sweden, Austria, Belgium, Canada, Israel• Of the 38, 27 provided data

Multistage review process
• The initial guideline draft had 47 statements and 35 questions and included sections on – assessment of calorie intake– feeding difficulties – anthropometric measures and other clinical assessments– ways of increasing calorie intake – address feeding difficulties– use of gastrostomy
• The final guidelines document comprised 45 separate statements

Benefits of gastrostomy
Item Medianresponse
n/N(%)
1.Benefitsofgastrostomyincludethefollowing32,42
:
Decreasednumberoffeedingtimes Agree 19/25(76.0)
Shorterdurationofmealtimes Agree 24/25(96.0)
Reducedvomitingandreflux Neitheragreeordisagree
22/25(88.0)
Reducedchestinfection Agree 24/25(96.0)
Reducedconstipationandpain Neitheragreeordisagree
23/24(95.8)
Gastrostomyshouldbeconsideredinchildrenwith:
Failuretothrivedespiteeffortstoincreasethecalorieintake Stronglyagree
20/20(100)
Oromotordysfunctioncausingunsafeswallow Stronglyagree
20/20(100)
Unusuallylongfeedingtimewithresultantstresstothecarerandthechild
Agree 19/20(95.0)
2.Gastrostomymayalsobeassociatedwithimprovedqualityoflifeofcaregivers
32
Agree 24/25(96.0)

Recommendations now publishedWhat has been achieved?
Dissemination of
knowledgePublications &
Conference
Presentations
Public
seminars/
Info sessions
Social &
other media
Plain
language
summaries
Stakeholder
feedback

Recommendations now publishedWhat has been achieved?
Dissemination of
knowledgePublications &
Conference
Presentations
Public
seminars/
Info sessions
Social &
other media
Plain
language
summaries
Stakeholder
feedback
Leonard H, Ravikumara M, Baikie G, Naseem N, Ellaway C, Percy A, Abraham S, Geerts S, Lane J, Jones M, Bathgate K, Downs J. Assessment and management of nutrition and growth in Rett syndrome. Journal of Pediatric Gastroenterology and Nutrition. 2013;57: 451–460.

Recommendations now publishedWhat has been achieved?
Dissemination of
knowledge
Publications &
Conference
Presentations
Public
seminars/
Info sessions
Social &
other media
Plain
language
summaries
Stakeholder
feedback

Recommendations now publishedWhat has been achieved?
Dissemination of
knowledge
Publications &
Conference
Presentations
Public
seminars/
Info sessions
Social &
other media
Plain
language
summaries
Stakeholder
feedback

Gallbladder disease in Rett syndrome
Item Level of
evidencea
Median
response
n/N b
(%)
Assessment
1. Screaming or apparent abdominal pain is suggestive of gall
bladder dysfunction24
4 Agree 15/16
(93.8)
2. The triad of apparent pain, vomiting and fever is the usual mode of presentation of cholecystitis
25
3 Agree 16/16 (100)
3. Exclude GERD as a cause of pain26
3 Agree 15/16
(93.8)
4. An ultrasound scan can be used to identify the presence of gallstones
25
3 Agree 15/16 (93.8)
5. Oral cholecystogram or a CCK or HIDA scan can be used
to confirm biliary dyskinesia25,27,29
3, 3, 3 Agree 13/13
(100)
Treatment
1. Ursodeoxycholic acid may be considered in an
asymptomatic patient with gallstone(s).
Neither agree
or disagree
10/11
(90.9)
2. The treatment of cholecystitis is cholecystectomy Neither agree or disagree
13/14 (92.9)
3. Cholecystectomy can be considered in cases of cholecystitis
after antibiotic treatment
Agree 14/15
(93.3)
4. Cholecystectomy is advised for all non-symptomatic patients with sludge or non-calcified stones that have not
resolved in 2 to 3 months40
3 Neither agree or disagree
10/12 (83.3)
4. The treatment of biliary dyskinesia is cholecystectomy28
3 Agree 11/13 (84.6)
5. The treatment of cholelithiasis is cholecystectomy24
4 Agree 13/14
(92.9)

Dissemination of
knowledgePublications &
Conference
Presentations
Public
seminars/
Info sessions
Social &
other media
Plain
language
summaries
Stakeholder
feedback
Prevalence of gall bladder disease in
Rett syndrome approximately 2%
Why is gall bladder disease more
common than expected-possibly
related to cholesterol metabolism
Gallbladder disease in Rett syndrome

Common symptoms & treatment of gall bladder disease
• Screaming or apparent abdominal pain may indicate
gall bladder dysfunction
• Pain, vomiting and fever common presentation
• Ultrasound can be used to diagnose gall stones
• Removal of gallbladder usual treatment

Recommendations now publishedWhat has been achieved?
Dissemination
of knowledge
Publications &
Conference
Presentations
Public
seminars/
Info sessions
Social &
other media
Plain
language
summaries
Stakeholder
feedback

Recommendations now publishedWhat has been achieved?
Dissemination
of knowledge
Publications &
Conference
Presentations
Public
seminars/
Info sessions
Social &
other media
Plain
language
summaries
Stakeholder
feedback
How should nutrition
and growth be assessed?
What investigations are
needed?
How can feeding ability be
assessed?
What are the symptoms of
feeding difficulties and how
can they be managed?
All about enteral feeding

Dissemination
of knowledge
Publications &
Conference
Presentations
Public
seminars/
Info sessions
Social & other
media
Plain
language
summaries
Stakeholder
feedback
When should enteral
tube feeding be
considered?
What are the types of
enteral tube feeding?
How can feeding ability be
assessed?
How should enteral tube feeding
be monitored?
Enteral tube feeding
Recommendations now publishedWhat has been achieved?

Gastrostomy Satisfaction
Satisfaction with surgery
Recommend for other girls
and women
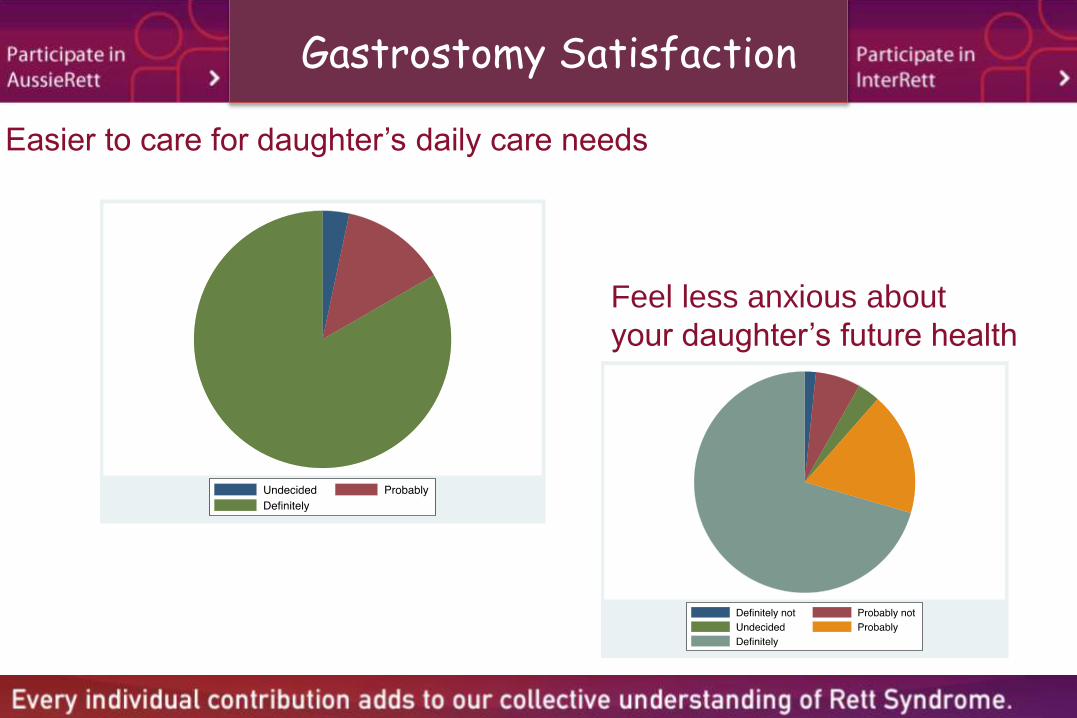
Gastrostomy Satisfaction
Easier to care for daughter’s daily care needs
Feel less anxious about
your daughter’s future health

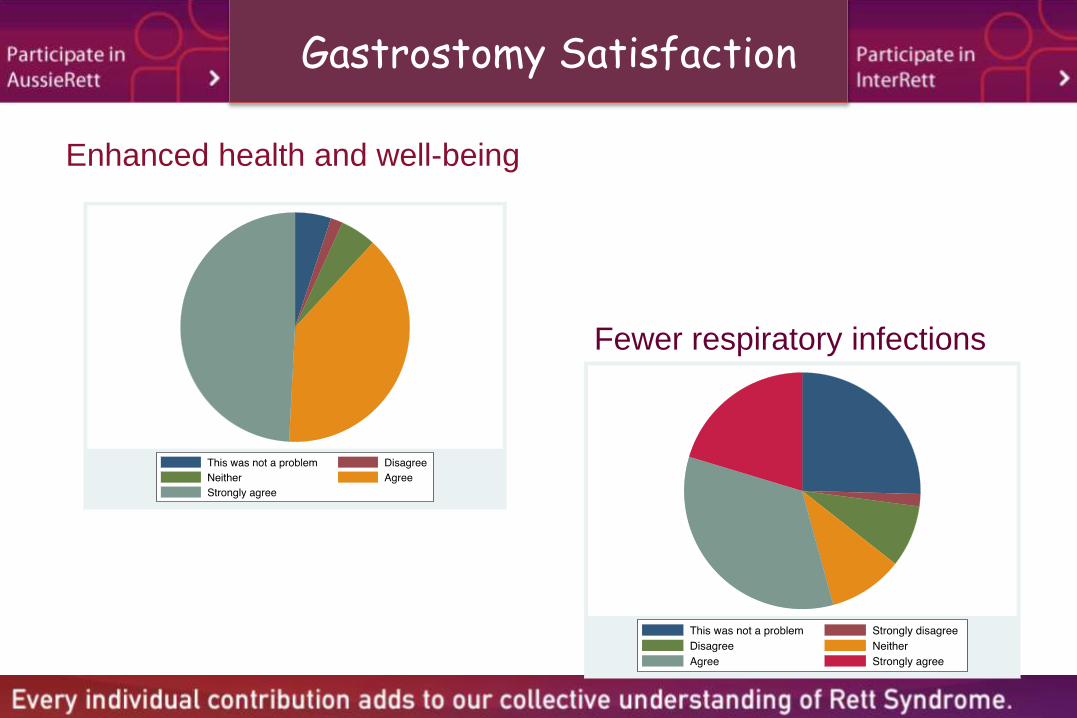
Gastrostomy Satisfaction
Satisfaction with weight gain
Ease of giving medication
Gastrostomy Satisfaction
Enhanced health and well-being
Fewer respiratory infections

Recommendations now publishedWhat has been achieved?
Dissemination
of knowledgePublications &
Conference
Presentations
Public
seminars/
Info
sessions
Social &
other media
Plain
language
summaries
Stakeholder
feedback
In this booklet we discuss
• Reflux
• Constipation
• Abdominal bloating
For each symptom
we discuss
• Assessment
• Investigation
• Management

Behaviour & Quality of everyday life : What do we know and what don’t we know?
• We haven’t been able to measure behaviour very well and need to develop a better instrument for doing this
• Although some girls and women with Rett syndrome appear to have challenging behaviours no research has been carried out to investigate how these behavioursmay be treated
• We probably need a better measure of quality of life
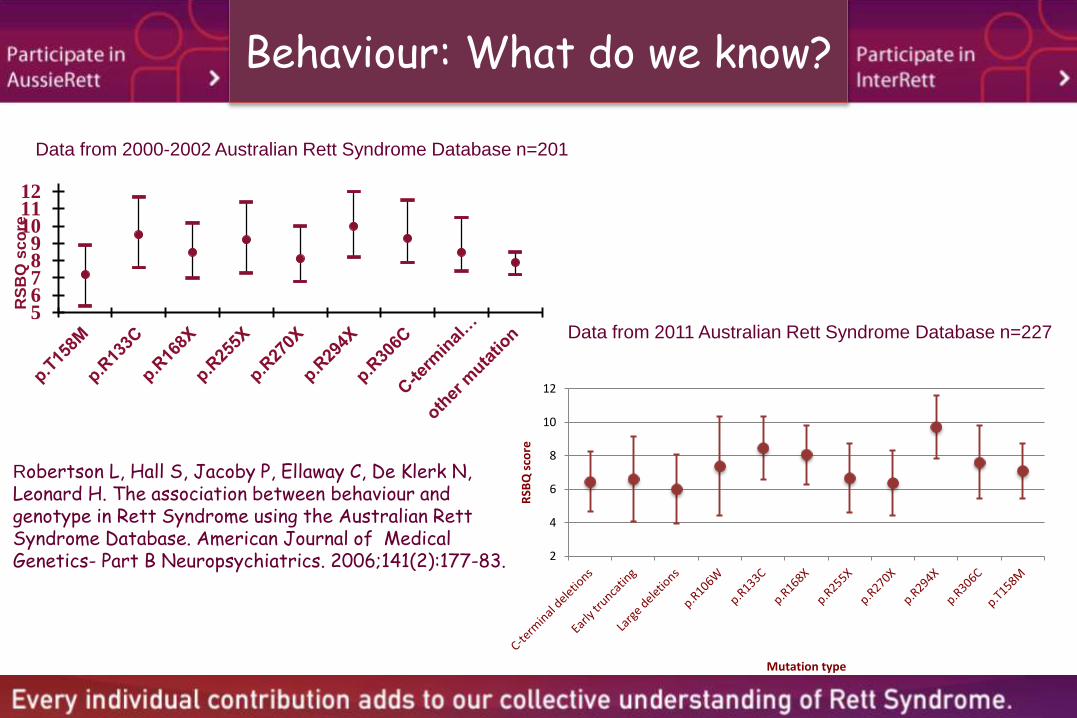
Behaviour: What do we know?
2
4
6
8
10
12
RSB
Q s
core
Mutation type
56789
101112
RS
BQ
sc
ore
Robertson L, Hall S, Jacoby P, Ellaway C, De Klerk N, Leonard H. The association between behaviour and genotype in Rett Syndrome using the Australian Rett Syndrome Database. American Journal of Medical Genetics- Part B Neuropsychiatrics. 2006;141(2):177-83.
Data from 2000-2002 Australian Rett Syndrome Database n=201
Data from 2011 Australian Rett Syndrome Database n=227

Quality of life by mutation group
-15
-10
-5
0
5
10
15
20
25
30
p.R294X p.R133C Cterminal
p.R168X p.T158M p.R306C Largedeletion
p.R270X p.R255X p.R106W
Psych
oso
cia
l su
mm
ary
sco
re
Lane JB, Lee HS, Smith LW, Cheng P, Percy AK, Glaze DG, Neul JL, Motil KJ, Barrish JO, Skinner SA, AnneseF, McNair L, Graham J, Khwaja O, Barnes K, Krischer JP. Clinical severity and quality of life in children and adolescents with Rett syndrome. Neurology. 2011;77(20):1812-8. Epub 2011/10/21.

Sleep problems: What do we know?
0-7 Years 8-12 Years 13-17 Years 18+ Years0
0.2
0.4
0.6
0.8
1
Age group
Fit
ted
Pro
ba
bil
ity
Any sleep problem
0-7 Years 8-12 Years 13-17 Years 18+ Years0
0.2
0.4
0.6
0.8
1
Age group
Fit
ted
Pro
ba
bil
ity
Night laughing
Presence
Persistent
0-7 Years 8-12 Years 13-17 Years 18+ Years0
0.2
0.4
0.6
0.8
1
Age group
Fit
ted
Pro
ba
bil
ity
Night screaming
Presence
Persistent
0-7 Years 8-12 Years 13-17 Years 18+ Years0
0.2
0.4
0.6
0.8
1
Age group
Fit
ted
Pro
ba
bil
ity
Night waking
Presence
Persistent

Sleep problems: What don’t we know?
2000 2002 2004 2006 2009−0.3
−0.2
−0.1
0
0.1
0.2
0.3
Questionnaire Year
Ab
so
lute
Ris
k C
ha
ng
e
Effect of treatment on sleep problem
Average effect
95% CI
We’re not doing well at treating sleep problems

What are some of the ingredients of quality of life ?
• Involvement in life situations with meaningful reward– Physical activity– Learning new information– Social relationships– Going out
• Allows for friendships, fun and development of self-identity
Andrews J, Leonard H, Hammond G, Girdler S, Rajapaksa R, Bathgate K, Downs J. Community participation for girls and women living with Rett syndrome. Disability and Rehabilitation. In press.
Walker E, Crawford F Leonard H. Community Participation: Conversations with parent-carers of young women with Rett syndrome. Journal of Intellectual & Developmental Disability. In press.

Translation
•

Ongoing challenge of maintaining the rage about Rett syndrome
Dissemination of
knowledgePublications &
Conference
Presentations
Public
seminars/
Info sessions
Social &
other media
Plain
language
summaries
Stakeholder
feedback

Participation
• school and/or day placement
• minimal hospital admissions
Genetic presentation
• Type of MECP2 mutation
• X inactivation status
• Other genetic factors
• Sporadic presentation
Developmental course prior to diagnosis eg,
duration of period prior to developmental regression,
learning to walk
Optimal well-being, quality and duration of life
Environmental factors
• early therapy interventions,
• ongoing therapy,
• medical management (eg monitoring, medications,
orthoses)
• surgical management (eg monitoring, gastrostomy,
spinal surgery)
• respite, home modifications, supportive community,
financial resources
Activity
• mobility
• hand function
• ability to communicate
• adequacy of sleep
Individual function factors
• bone health
• control of scoliosis
• growth and maintenance of weight
• control of epilepsy
• manageable behaviour
Family functioning
• Function, eg physical and mental health of parents and
siblings
• Activity, eg recreation, family holidays
• Participation, eg parental employment, smooth
transitions between life stages
• Personal factors, eg resilience
The whole picture: the complexity of Rett syndrome goes beyond the biology

Thanks go to...
• NIH (2004-2008)
• NHMRC (2004-2008)
• NHMRC (2111-2013)
• International Rett Syndrome
Foundation (InterRett)
• Financial Markets Foundation for
Children (1999)
• Rett Syndrome Association
Research Fund (2002)
• The families and clinicians who have
supported the research so well over 18
years
• Bill Callaghan and the Rett Syndrome
Association of Australia
• Australian Paediatric Surveillance Unit
• Janelle Lillis and family
Recent funding NIH 1 R01 HD043100-01A1, NHMRC #303189 & #100384, IRSF