height as - injury prevention...height wasloweredto 1 5 metres. conclusions-although the height and...
TRANSCRIPT

Injury Prevention 1996; 2: 98-104
ORIGINAL ARTICLES
Height and surfacing as risk factors for injury infalls from playground equipment: a case-controlstudy
David J Chalmers, StephenW Marshall, John D Langley, M Jean Evans,Cheryl R Brunton, Anne-Maree Kelly, Alison F Pickering
Injury PreventionResearch Unit,Department ofPreventive and SocialMedicine, UniversityofOtago MedicalSchool, PO Box 913,Dunedin, New ZealandDJ ChalmersSW MarshallJD LangleyMJ Evans
UniversityDepartment ofCommunity Healthand General Practice,Christchurch SchoolofMedicine,University of Otago,Christchurch, NewZealandCR BruntonAF Pickering
UniversityDepartment ofSurgery, ChristchurchSchool ofMedicine,University ofOtago,Christchurch, NewZealandA-M Kelly
Correspondence to:Dr Chalmers.
AbstractObjectives-Despite the widespread pro-motion of safety standards no epidemi-ological studies have adequatelyevaluated their effectiveness in preven-ting injury in falls from playgroundequipment. This study evaluated theeffectiveness of the height and surfacingrequirements of the New Zealand stan-dard for playgrounds and playgroundequipment.
Setting-Early childhood education cen-tres and schools in two major cities in theSouth Island of New Zealand.
Methods-Data were collected on 300children aged 14 years or less who hadfallen from playground equipment. Ofthese, 110 (cases) had sustained injury andreceived medical attention, while 190(controls) had not sustained injuryrequiring medical attention.
Results-Logistic regression modelsfitted to the data indicated that the risk ofinjury being sustained in a fall was in-creased if the equipment failed to complywith the maximum fall height (odds ratio(OR) = 3-0; 95% confidence interval (CI)0 7 to 13-1), surfacing (OR = 2-3; 95% CI1-0 to 5 0), or safe fall height (OR = 21;95% CI 1 1 to 4 0) requirements. Fallsfrom heights in excess of 1'5 metres in-creased the risk of injury 4-1 times that offalls from 1-5 metres or less and it wasestimated that a 45% reduction in child-ren attending emergency departmentscould be achieved if the maximum fallheight was lowered to 1 5 metres.
Conclusions-Although the height andsurfacing requirements of the New Zea-land standard are effective in preventinginjury in falls from playground equip-ment, consideration should be given tolowering the maximum permissible fallheight to 1-5 metres.(Injury Prevention 1996; 2: 98-104)
Keywords: falls, play.
Each year in New Zealand approximately 7400children aged less than 15 years attend
emergency departments for the treatment ofinjuries sustained while using playgroundequipment, over 1100 are hospitalised, and onedies, giving annual incidence rates per 100 000children of 930 for emergency departmentattendances, 137 for hospitalisations, and amortality rate of 0 15.'-3 These rates do notcompare favourably with those for northernhemisphere countries, but are similar to thosefor Australia.4-6 Fifty eight per cent of theemergency department attendances, 92% ofthe hospitalisations, and 460/0 of the fatalitiesresult from falls.' To reduce these injuries, asafety standard for playgrounds and play-ground equipment was introduced in 1986(NZS 5828).7 This is similar in many respectsto those of other countries.8-" The regulationof equipment height and under surfacing isconsidered a priority. The specificrequirements relating to these factors are des-cribed in the Appendix.There has been widespread promotion of the
standard but given that its implementation isvoluntary, compliance with the aboverequirements is by no means universal. Asurvey of 1135 items of equipment in schooland public playgrounds in Dunedin found that17 o~ had fall heights exceeding 2 5 metres,550% did not have impact absorbing surfaces,and only 4%/ complied with the safe fall heightrequirement. 12
Four studies have attempted to measure theinjury risks associated with height of equip-ment or type of undersurface,'3-'6 but all fourhad methodological problems varying from notcontrolling for exposure'3 1416 or height offall,'3-'5 as well as other confounders. Thesestudies reported evidence of increased risk withincreased equipment height but were equivocalas to the benefits of impact absorbing surfaces,such as bark chips, in comparison to non-impact absorbing surfaces, such as concrete.Because no epidemiological studies have ade-quately evaluated the effectiveness of impactabsorbing surfaces in reducing the incidenceand severity of injuries, vigorous debate hasoccurred,'7-2' with some researchers arguingthat until the evidence is available, no moneyshould be spent on installing expensive surfac-ing materials.22 They argue, further, thatwhereas the sufaces being widely promoted are'designed solely to reduce the risk of oneparticular type of injury, namely, life-
98
on April 2, 2020 by guest. P
rotected by copyright.http://injuryprevention.bm
j.com/
Inj Prev: first published as 10.1136/ip.2.2.98 on 1 June 1996. D
ownloaded from
Risk of injury in playground falls
threatening brain injury.... There is no
evidence available oftheir effectiveness as a riskreduction measure for other injuries'.22 In fact,there is no 'real world' evidence available oftheir effectiveness as a risk reduction measurefor brain injury either.The purpose of the present study was to
examine height and surfacing as risk factors forinjury in falls from playground equipment, andin so doing assess the effectiveness of therequirements of the New Zealand standard inreducing the risk of such injury. The followinghypotheses were tested:
(1) Children injured in fall from play-ground equipment will be more likely thanchildren with minor injuries (or no injuries) tohave fallen from equipment non-compliantwith the requirements ofNZS 5828 regarding:(a) maximum fall height; (b) surfacing; and (c)safe fall heights for specific surfacing materials.
(2) Children injured in falls from play-ground equipment will be more likely to havefallen from greater heights than children withminor injuries (or no injuries).
MethodsThis study was undertaken in Dunedin andChristchurch, the two most populous cities inthe South Island ofNew Zealand, with approx-imately 21 000 and 60 000 children aged 14years or less, respectively. It was restricted toearly childhood education centres (preschoolfacilities for children aged less than 5 years) andschools (for children aged 5 to 14 years).
Cases were children aged 14 years or less whohad sustained injuries in falls from playgroundequipment at an early childhood educationcentre or school, and had received medicalattention. Staff at the emergency departmentsof the Dunedin and Christchurch public hos-pitals recorded the names of all children pres-
enting for treatment who met the abovecriteria. A written invitation to participate,information sheet, and consent form, were
issued to the parent(s) or other care giver(s).The records at Dunedin Hospital were checkedweekly throughout the study period(September 1989 to February 1991), whilethose at Christchurch Hospital were checkedeach weekday (November 1991 to May 1992).A follow up telephone call was made within oneweek to arrange an interview.
Controls were children aged 14 years or lesswho had fallen from playground equipmentand had struck the ground surface but had notsustained an injury for which medical attentionwas sought. Recruitment was through earlychildhood education centres and schools in thearea served by Christchurch Hospital.Incidents were recorded by staff who were
contacted twice weekly by telephone.Typically, the incident would have come to theattention of staffbecause the child had requiredfirst aid or, simply reassurance. Participationwas invited using the same procedures as forcases.On the basis of the age distribution of cases
ascertained in Dunedin it was decided to seek86% of controls from schools and the remain-
ing 14% from early childhood education cen-tres. To maximise the limited time andresources available, only schools with rolls of200 or more pupils were sampled. Early child-hood education centres were similarlyrestricted to only the larger centres. A randomsample of 22 schools and 22 centres from thoselocated in the catchment area for ChristchurchHospital was required to achieve targets of 160and 25 controls, respectively. Schools wererecruited through a direct approach to prin-cipals, while early childhood education centreswere recruited with the assistance of therelevant parent organisations. In only one ins-tance was a school principal not prepared toparticipate and a replacement school wasselected.
After consent, an interview was conductedwith the child (where appropriate), parents orother care givers, teachers, and other witnessesto the incident. To facilitate recall, the inter-view was conducted as soon as practicable and,whenever possible, at the site of the incident.When the latter was not possible, photographsand diagrams of the site were used to assist thechild in describing the incident, with measure-ments being made on site. Identical informa-tion was sought from cases and controls. Thestructured interview covered the gender, age,height, and weight ofthe child; date and time ofthe incident; place of occurrence and type ofequipment; height from which the child fell;type of surface; particle size, depth, and reten-tion of loose fill materials; and body part to hitfirst. Because no economically feasible testequipment was available, the critical dropheights for surfaces were not measureddirectly. The interviews were conducted byone of three persons in Dunedin, and one inChristchurch.For cases, diagnostic information was
obtained from the emergency departmentrecords. For controls, details of any non-medically treated injuries were obtained duringthe interview. Body site, nature, and severity ofinjury were coded according to the abbreviatedinjury scale (AIS)."3
DEFINITIONSThe definitions used were:
(1) A 'fall' was defined as any action, in-cluding jumping, in which a child descended ordropped freely from an item of playgroundequipment to the ground surface below.
(2) The 'height of fall' was defined as thevertical distance the child fell and wasmeasured from the point on the equipment atwhich the child was sitting, standing, kneeling,swinging, or balancing, to the ground surface.
(3) Surfaces were classified as 'impactabsorbing' or 'non-impact absorbing' in accor-dance with NZS 5828 (see Appendix). Thisclassification was made irrespective of criticaldrop height, or, in the case of loose fillmaterials, particle size, depth, and retentioncharacteristics.
(4) The 'safe fall height' for a given surfacematerial was taken from NZS 5828, with theexception of bark chips (table 1). For bark
99
on April 2, 2020 by guest. P
rotected by copyright.http://injuryprevention.bm
j.com/
Inj Prev: first published as 10.1136/ip.2.2.98 on 1 June 1996. D
ownloaded from

Chalmers, Marshall, Langley, Evans, Brunton, Kelly, Pickering
Table 1 Safefall heightsfor selected playground surfacematerials
Safe fall heightMaterial (mm)Impact absorbing
Loose fillBark chips (minimum depth 200 mm) (2500Pea gravel (minimum depth 200 mm) < 2000Sand (minimum depth 300 mm) (2000SyntheticRubber matting < 1600Rubber tiles (1350
Non-impact absorbingConcrete < 250Asphalt ( 50Grass Not applicable*Bare earth Not applicable*
*Grass and bare earth are not considered suitable under fixed orhigh use equipment (NZS 5828: part 1: s105.9).
chips, the safe fall height was set at 2500 mm, themaximum permissable fall height, to reflect theresults of more recent tests conducted in NewZealand.
STATISTICAL ANALYSISAll analyses were conducted using the SASsystem for personal computers.24 Goodness offit in the logistic regression model was assessedusing the test statistic proposed by Hosmer andLemeshow.25 On the basis of preliminarybivariate analyses, all of the logistic regressionmodels were adjusted for place of occurrence(early childhood education centre v school),type of equipment, age (0-9 years, 10-14years), and gender. With one exception, thefalls among 0-4 year olds occurred in earlychildhood centres and the falls among 5 - 9 yearolds occurred in schools. Controlling for placeof occurrence is very similar, therefore, tocontrolling for differences in the risk of injurybetween 0-4 and 5-9 year olds. All wereadjusted also for child height and weight,because these factors are considered to affectthe risk of injury in free falls.26 Additiveinteraction between variables was assessedusing the indices proposed by Rothman,27 andconfidence intervals (CIs) for these indiceswere calculated.28 Attributable proportionswere estimated using the method described byRothman.27
ResultsDuring the periods described above, 126 child-ren meeting the initial case criteria (67 inDunedin and 59 in Christchurch) and 205children meeting the initial control criteriawere interviewed. These represented 780% ofeligible cases in Christchurch, 76o% of eligiblecases in Dunedin, and 96% of eligible controls.After the exclusion of 16 cases and 15 controls,a total of 110 cases (57 from Dunedin and 53from Christchurch), and 190 controls wereentered into the analysis.There were proportionally more males and
older children (aged 10-14 years) among thecases, and while not differing by mean heightthey were heavier than controls (table 2). Forthe cases, the most common site of injury wasthe upper extremity (76%), the most common
Table 2 Personal and injury characteristics of cases andcontrols; values are number (0% ) unless stated otherwise
Cases Controls(n = 110) (n = 190) Test statistic
GenderFemale 51 (46) 114 (60) 5 = 5-234, df= 1Male 59 (54) 76 (40) p = 0022
Age (years)0-4 10 (9) 28 (15)5-9 74 (67) 146 (77) x2= 14143, df= 210-14 26 (24) 16 (8) p= 0001
Mean height (mm) 1265 1240 t = 1-47, p = 0 143Mean weight (kg) 27 25 t = 2-48, p = 0-014
Site of injuryNo injury 0 54 (28)Head 8 (7) 27 (14)Face 2 (2) 28 (14)Abdomen 5 (5) 22 (12)Upper extremity 84 (76) 22 (12)Lower extremity 11 (10) 34 (18)Other 0 3 (2)
Nature of injuryNo injury 0 54 (28)Abrasion 0 32 (17)Contusion 9 (8) 68 (36)Sprain 6 (6) 13 (7)Fracture 65 (59) 0Intracranial 8 (7) 1 (1)Other 22 (20) 22 (11)
Severity of injuryNo injury 0 54 (28)AIS1 minor 35 (32) 131 (69)AI S2 moderate 54 (49) 1 (1)AIS3 serious 17 (15) 0AIS unknown 4 (4) 4 (2)
diagnosis a fracture (590° ), and over half wereassigned an AIS23 severity score of > 2(moderate). In contrast, 54 (28%) of the cont-rols sustained no injury, while for thoseinjured, the most common site was the lowerextremity (18%), the most common injury acontusion (35%), and all but one was assigned aseverity score of 1 (minor). The groups did notdiffer significantly by place of occurrence orequipment type (table 3).For cases, the upper extremity was the most
common body part to hit the ground first(71 %), followed by the lower extremity (14 0 ).For controls, the lower extremity was the mostcommon body part to hit first (41%), followedby the upper extremity (19%). For cases, 63%oof falls from 1 metre and below hit with theupper extremity first, compared with 73%/" offalls from above 1 metre. For controls, 14% offalls from 1 metre and below, the upper ext-remity hit first, compared with 2200 of fallsfrom above 1 metre. To avoid collinearityproblems, body part to hit first was notincluded in the logistic regression models.An initial logistic regression model including
place of occurrence, age, gender, child height,child weight, equipment type, impact surface,and fall height was fit. The model provided anadequate fit to the data (Hosmer-LemeshowC = 4 72, df= 8, p = 0 7866).
NON-COMPLIANCE WITH THE STANDARDTo test hypothesis l(a) the height of interestwas that from which the child fell (that is heightof fall) and whether this exceeded 2 5 metres.Although most children fell from heights of lessthan 2 5 metres, 50% of the cases and 20/ of thecontrols fell from heights exceeding this, imp-
100
on April 2, 2020 by guest. P
rotected by copyright.http://injuryprevention.bm
j.com/
Inj Prev: first published as 10.1136/ip.2.2.98 on 1 June 1996. D
ownloaded from
Risk of injury in playground falls
Table 3 Characteristics offallsfrom playground equipment; values are number (%)unless stated otherwise
Cases Controls(n = 110) (n = 190) Test statistic
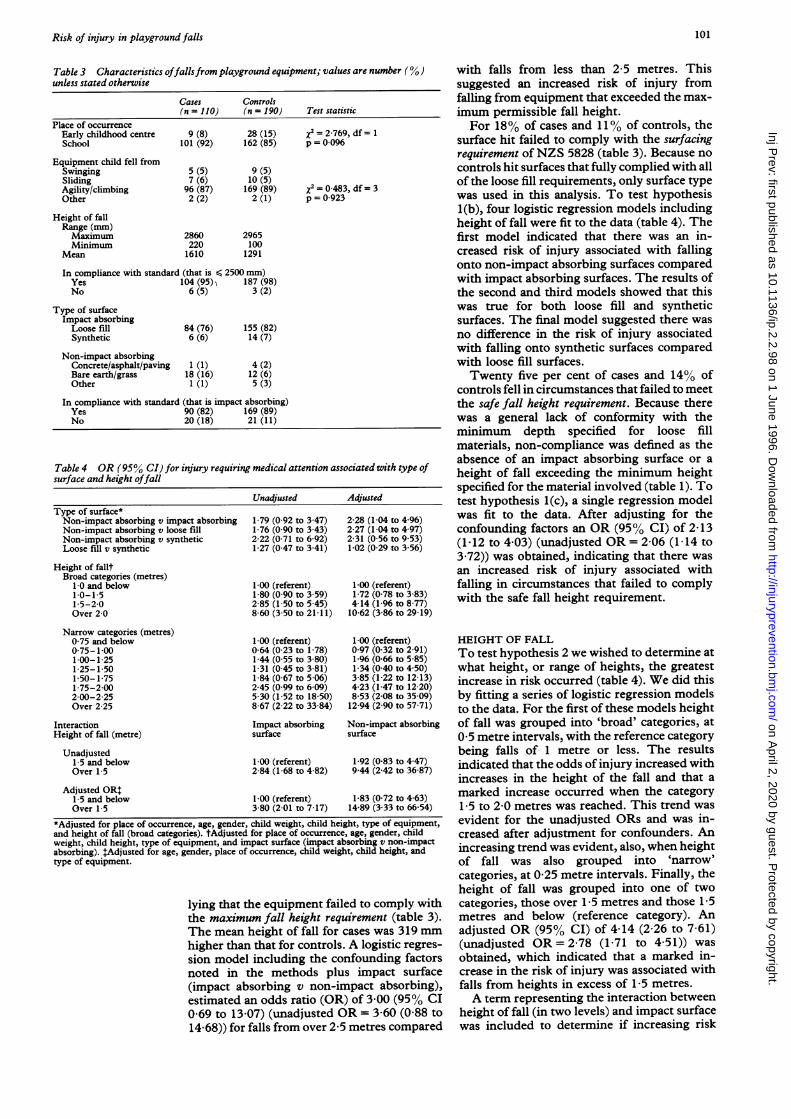
Place of occurrenceEarly childhood centre 9 (8) 28 (15) x2 2-769, df= 1School 101 (92) 162 (85) p = 0096
Equipment child fell fromSwinging 5 (5) 9 (5)Sliding 7 (6) 10 (5)Agility/climbing 96 (87) 169 (89) x2 = 0-483, df= 3Other 2 (2) 2 (1) p= 0-923
Height of fallRange (mm)Maximum 2860 2965Minimum 220 100
Mean 1610 1291
In compliance with standard (that is < 2500 mm)Yes 104 (95)) 187 (98)No 6 (5) 3 (2)
Type of surfaceImpact absorbingLoose fill 84 (76) 155 (82)Synthetic 6 (6) 14 (7)
Non-impact absorbingConcrete/asphalt/paving 1 (1) 4 (2)Bare earth/grass 18 (16) 12 (6)Other 1 (1) 5 (3)
In compliance with standard (that is impact absorbing)Yes 90 (82) 169 (89)No 20 (18) 21 (11)
Table 4 OR (95% CI) for injury requiring medical attention associated with type ofsurface and height offall
UnadjustedType of surface*Non-impact absorbing v impact absorbingNon-impact absorbing v loose fillNon-impact absorbing v syntheticLoose fill v synthetic
Height of falltBroad categories (metres)
1-0 and below1*0-1-51 5-20Over 2-0
Narrow categories (metres)0-75 and below0-75-1 001-00-1-251-25-1 501 50-1 751-75-2002-00-2 25Over 2 25
InteractionHeight of fall (metre)
Unadjusted1-5 and belowOver 1 5
Adjusted OR:1-5 and belowOver 1 5
1-79 (0-92 to 3-47)1-76 (0 90 to 3-43)2-22 (0-71 to 6-92)1-27 (0 47 to 3-41)
1-00 (referent)1-80 (0 90 to 3-59)2 85 (1-50 to 5-45)860 (350 to 21 11)
1-00 (referent)0-64 (0-23 to 1-78)1-44 (0 55 to 3 80)1-31 (0 45 to 3-81)1-84 (0-67 to 5 06)2-45 (0-99 to 6 09)530 (1-52 to 18-50)8 67 (2-22 to 33-84)
Impact absorbingsurface
1-00 (referent)2-84 (1-68 to 4 82)
1-00 (referent)3-80 (201 to 7-17)
Adjusted
2-28 (1-04 to 4-96)2-27 (1-04 to 4-97)2-31 (0-56 to 953)1-02 (0-29 to 3-56)
1-00 (referent)1-72 (0-78 to 3-83)4-14 (1-96 to 8-77)10-62 (3-86 to 29 19)
1-00 (referent)0 97 (0 32 to 2-91)1-96 (0-66 to 5 85)1-34 (0-40 to 4 50)385 (1-22 to 12-13)4-23 (1-47 to 12 20)8-53 (2-08 to 35 09)12-94 (2-90 to 57-71)
Non-impact absorbingsurface
1 92 (0-83 to 4-47)9 44 (2-42 to 36-87)
1-83 (0-72 to 4-63)14-89 (3 33 to 66-54)
*Adjusted for place of occurrence, age, gender, child weight, child height, type of equipment,and height of fall (broad categories). tAdjusted for place of occurrence, age, gender, childweight, child height, type of equipment, and impact surface (impact absorbing v non-impactabsorbing). tAdjusted for age, gender, place of occurrence, child weight, child height, andtype of equipment.
lying that the equipment failed to comply withthe maximum fall height requirement (table 3).The mean height of fall for cases was 319 mmhigher than that for controls. A logistic regres-sion model including the confounding factorsnoted in the methods plus impact surface(impact absorbing v non-impact absorbing),estimated an odds ratio (OR) of 3-00 (95% CI0 69 to 13-07) (unadjusted OR = 3 60 (0-88 to
14 68)) for falls from over 2 5 metres compared
with falls from less than 2 5 metres. Thissuggested an increased risk of injury fromfalling from equipment that exceeded the max-imum permissible fall height.For 18% of cases and 11% of controls, the
surface hit failed to comply with the surfacingrequirement ofNZS 5828 (table 3). Because nocontrols hit surfaces that fully complied with allof the loose fill requirements, only surface typewas used in this analysis. To test hypothesisl(b), four logistic regression models includingheight of fall were fit to the data (table 4). Thefirst model indicated that there was an in-creased risk of injury associated with fallingonto non-impact absorbing surfaces comparedwith impact absorbing surfaces. The results ofthe second and third models showed that thiswas true for both loose fill and syntheticsurfaces. The final model suggested there wasno difference in the risk of injury associatedwith falling onto synthetic surfaces comparedwith loose fill surfaces.Twenty five per cent of cases and 14% of
controls fell in circumstances that failed to meetthe safe fall height requirement. Because therewas a general lack of conformity with theminimum depth specified for loose fillmaterials, non-compliance was defined as theabsence of an impact absorbing surface or aheight of fall exceeding the minimum heightspecified for the material involved (table 1). Totest hypothesis l(c), a single regression modelwas fit to the data. After adjusting for theconfounding factors an OR (95% CI) of 2-13(1.12 to 4 03) (unadjusted OR = 2-06 (1-14 to3-72)) was obtained, indicating that there wasan increased risk of injury associated withfalling in circumstances that failed to complywith the safe fall height requirement.
HEIGHT OF FALLTo test hypothesis 2 we wished to determine atwhat height, or range of heights, the greatestincrease in risk occurred (table 4). We did thisby fitting a series of logistic regression modelsto the data. For the first of these models heightof fall was grouped into 'broad' categories, at0 5 metre intervals, with the reference categorybeing falls of 1 metre or less. The resultsindicated that the odds of injury increased withincreases in the height of the fall and that amarked increase occurred when the category1-5 to 2-0 metres was reached. This trend wasevident for the unadjusted ORs and was in-creased after adjustment for confounders. Anincreasing trend was evident, also, when heightof fall was also grouped into 'narrow'categories, at 0-25 metre intervals. Finally, theheight of fall was grouped into one of twocategories, those over 1 5 metres and those 1-5metres and below (reference category). Anadjusted OR (95% CI) of 4-14 (2-26 to 7-61)(unadjusted OR= 2-78 (1-71 to 4-5 1)) wasobtained, which indicated that a marked in-crease in the risk of injury was associated withfalls from heights in excess of 1-5 metres.A term representing the interaction between
height of fall (in two levels) and impact surfacewas included to determine if increasing risk
101
on April 2, 2020 by guest. P
rotected by copyright.http://injuryprevention.bm
j.com/
Inj Prev: first published as 10.1136/ip.2.2.98 on 1 June 1996. D
ownloaded from

Chalmers, Marshall, Langley, Evans, Brunton, Kelly, Pickering
with increasing height of fall was similar forboth impact absorbing and non-impact absorb-ing surfaces. The interaction term was notsignificant. For both the unadjusted andadjusted estimates, however, the 'relativeexcess risk' (estimated as the OR - 1) forexposure to both factors was greater than thesum of the relative excess risks for exposure tothe factors individually (that is (1 83 - 1) +(3-80 - 1) = 2 63< (14-89 - 1)) (table 4), sug-gesting an additive interaction effect. Calcula-tion of the synergy index (S) and the relativeexcess risk due to interaction (RERI),27 pro-vided further evidence of an additive interac-tion for both the unadjusted model (S = 3 05(95%O CI 0 61 to 15-30); RERI = 5-68 (95%CI - 692 to 18-26)) and the adjusted model(S = 3-83 (95%O CI 0 76 to 19 37);RERI = 10-26 (95%O CI - 11-37 to 31-90)).
ESTIMATES OF ATTRIBUTABLE PROPORTIONTo estimate the potential reduction in atten-dances at emergency departments that could beachieved if all equipment was to comply withthe height and surfacing requirements of NZS5828, we calculated attributable proportionsfor each requirement.27 Annually, in New Zea-land, about 4300 children attend emergencydepartments for injuries from falls from play-ground equipment.' We estimate that 85%(3650) of these children are injured on hittingthe ground surface, and that of these incidents,nearly 60% (2200) occur in schools or earlychildhood education centres.
If all items ofplayground equipment at thesesites complied with the requirement that no fallheight is to exceed 2 5 metres, there would be a3.6% reduction in the number attendingemergency departments (P(proportion of casesexposed) = 0 0545), that is a reduction of 80such attendances. Similarly, if all equipmentwas installed over well maintained impactabsorbing surfaces, there would be a 10%reduction in attendances (P = 0-1818), that is220 fewer attendances. If all equipment met thesafe fall requirement, which requires that bothheight and surface are in conformity, therewould be a 13 5% reduction (P = 0-2545), thatis 300 fewer attendances. If the maximumpermissible fall height were lowered to 1.5metres and all equipment complied, theestimated reduction would be 45%(P = 0 5905), that is 990 fewer attendances.Finally, 5.6%/o (P = 0-056) of cases are att-ributable to the interaction between height offall and impact surface, that is 125 attendances.
Discussion
LIMITATIONSThe selection and recruitment of cases andcontrols for this study presented a number ofchallenges. Cases were selected from childrenpresenting at hospital emergency departmentsbecause this enabled both accessibility and aminimum of delay between injury and inter-view. Checks made with private emergencyservices and general practitioners revealed that
few children injured on playground equipmentpresented at these services. It is unlikely,therefore, that limiting our case selection intro-duced any significant biases.The second, and more demanding challenge,
was to identify a control group who had fallenfrom playground equipment but had not beeninjured, and who would be accessible for inter-view. We chose children from early childhoodeducation centres and schools, as these were theonly setting where personnel maintainedrecords of incidents. As the cases could havebeen injured in any setting, including publicplaygrounds and private homes, we limitedthem to those occurring in the same settings ascontrols, effectively reducing thegeneralizability of the findings.
Controls were limited to only those childrenwho came to the attention of staff. Because notall children who fall from playground equip-ment seek attention, or in some other way cometo the attention of staff, it is possible that thisgroup may have differed from the population ofchildren who fall from equipment. Because weassumed that those who did not seek attentionwere those whose fall was less serious, thisnon-ascertainment would yield conservativeestimates of risk.
Because of sample size and logistics, it wasnecessary to conduct the study in two cities,with the cases being ascertained in Dunedinand Christchurch and the controls being ascer-tained only in Christchurch. This raises thepotential bias that the characteristics of play-grounds and playground equipment in the twocities are different. To address this issue, werepeated the logistic regression analyses withthe Dunedin cases excluded; the results werevery similar to those reported for the full dataset.
Controls were ascertained only from thelarger early childhood education centres andschools. Because these may have been wealthierand better able to provide playgrounds thatcomplied with the standard, this may have ledto overestimates of the effectiveness of theheight and surfacing requirements.A potential source of bias was the definition
of height of fall in a situation where a child issuspended beneath equipment. Using the dis-tance from the lowest part ofthe child's body tothe impact surface is unsatisfactory, given thatmany injuries are to the upper limbs. Where achild is suspended by the hands, for example,the distance traversed by the upper limb duringdescent is much greater than the distancebetween the lowest part of the child's body andthe ground. Height of fall was, therefore,measured from the point where the child lasthad contact with the equipment, as it wasconsidered that this would more accuratelyreflect the distance traversed by the majority ofthe injured body sites. This was consistent withthe measurement for children standing, sitting,kneeling, or balancing.We were unable to examine the effects of
non-compliance with the requirements relatingto particle size, depth, and retention of loose fillmaterials. This was due to a general lack ofcompliance with these requirements and con-
102
on April 2, 2020 by guest. P
rotected by copyright.http://injuryprevention.bm
j.com/
Inj Prev: first published as 10.1136/ip.2.2.98 on 1 June 1996. D
ownloaded from

Risk of injury in playground falls
forms to previously reported results.'2 As itapplied equally to cases and controls, it isdoubtful that this introduced any significantbiases. When we came to examine the safe fallheight requirement, the lack ofconformity withthe minimum depth requirement obliged us toapply a less stringent test of compliance. Hadwe been able to measure the critical drop heightfor each surface directly, then a more precisetest of compliance would have been possible.As with all of the measurements relating tosurfacing, however, any apparent increase inprecision must be weighed against the potentialfor bias due to differences in factors such ascompaction and moisture content, as well asinterventions by maintenance staff (for exam-ple raking), between the time of the fall and thetime of testing. Finally, when we came toexamine height of fall, we were unable to adjustfor the depth of loose fill materials becausethere was insufficient variation in the data, withmost surfaces being less than half of the depthrequired. As a result of these limitations, ourestimates of risk and attributable proportionsmay be conservative.
FINDINGSOur results show that children who fall fromplayground equipment that does not complywith the height and surfacing requirements ofthe New Zealand playground standard (NZS5828) are at increased risk of injury. Firstly,non-compliance with the requirement that nochild should be able to fall from a heightexceeding 2-5 metres increases the odds ofinjury by 3 0 times. Secondly, the odds ofbeinginjured in a fall onto a non-impact absorbingsurface, such as asphalt or concrete, is 2-28times that of falling onto an impact absorbingsurface. Thirdly, non-compliance with the safefall height requirement (that no child shouldfall from a height which exceeds the criticaldrop height for the underlying surface), in-creases the odds ofbeing injured by at least 2 13times.The greatest increase in risk occurred at
heights in excess of 1-5 metres. When theinteraction between height of fall and impactsurface was examined, it was found that thesefactors tended to interact such that the odds ofsustaining injury in falls from heights greaterthan 1-5 metres onto non-impact absorbingsurfaces was very much greater than was thecase when either one of these factors wasinvolved. Not only does this finding havebiological plausibility, but it also confirms theimportance of providing both an impact absor-bing surface and restricting the height fromwhich children may fall.
Compliance with the existing maxin-um fallheight requirement would not significantlyreduce the number of children attendingemergency departments. On the other hand,compliance with the surfacing requirementcould be expected to prevent 220 cases. Thisfigure would increase to 300 fewer cases if thesafe fall height requirement were compliedwith. The greatest reduction would comeabout, however, by lowering the maximum fall
height from 2 5 to 1 5 metres, that is a reductionof 990 cases. These estimates consider onlyinjury occurring in early childhood educationcentres and schools. If all public playgroundsand domestic equipment were to comply withthese requirements, then the reduction inattendances could be very much greater.The findings indicate that both the max-
imum permissable fall height of 2-5 metres andthe present safe fall height requirement shouldbe reviewed. If the maximum permissable fallheight were to be lowered from 2-5 metres to1-5 metres, this could pose a significant prob-lem with regard to existing equipment. Forexample, 59% of the climbing frames inDunedin schools exceeded 1-5 metres whensurveyed in 1989.12 While it might be difficult,therefore, to apply such a restriction retrospec-tively, such a requirement could be introducedfor all future equipment. Informal discussionwith both designers and manufacturersindicated this to be a reasonable proposal. Itshould be possible to design equipment so thatno fall height exceeds 15 metres, while stillproviding children with the challenge andexcitement they seek and that is important fortheir development.29The critical drop height for a given surface
material is presently set at the threshold forserious head injury based on experimental datausing cadavers and animals. While we wereunable to examine this directly, our findingssuggest that this criterion may not be appropri-ate for the prevention of injury to any body siteand, in particular, fractures to the upper limb(see Ball and King22). There are a number ofways in which this issue might be addressed.One would be to re-examine the critical drop*height criterion and set a level appropriate tothe more commonly occurring injuriesassociated with falls from playground equip-ment. A second would be to adopt a lowermaximum permissible fall height of 1-5 metres.A third would be to consider others factorsassociated with surface impacts, but thesewould need to be amenable to change.A significant proportion of school play-
ground equipment does not comply with thesurfacing requirement, and even where animpact absorbing surface has been installed, itis unlikely to comply fully with all of therelevant requirements.'2 Because we wereunable to assess the effectiveness of compliancewith these requirements, further research isrequired. In particular, it would be of con-siderable interest to know if the present depthrequirements for loose fill surface materials areadequate.
ConclusionsWe observed increased risk of injury in fallsfrom heights above those recommended in theNew Zealand playground standard, and in fallsonto surfaces that did not comply with therequirements of the standard. We conclude,therefore, that the height and surfacingrequirements of the standard are effective inpreventing injury in falls from playgroundequipment. We recommend that pending fur-
103
on April 2, 2020 by guest. P
rotected by copyright.http://injuryprevention.bm
j.com/
Inj Prev: first published as 10.1136/ip.2.2.98 on 1 June 1996. D
ownloaded from

Chalmers, Marshall, Langley, Evans, Brunton, Kelly, Pickering
ther research on critical drop heights and otherfactors associated with surface impacts, con-
sideration be given to lowering the maximumpermissible fall height specified in the NewZealand standard (NSZ 5828) from 25 metresto 1 5 metres. This would appear to provide thegreatest opportunity for reducing the incidenceof injury occurring in falls from playgroundequipment.
Appendix: Height and surfacingrequirements of NZS 5828(1) MAXIMUM FALL HEIGHTNo piece of equipment shall be of a height in excess
of 6 m and no fall height therein in excess of 2.5 m.
(NZS 5828: part 3: s2.2.1)
(2) SURFACINGIt is strongly recommended that impact absorbingsurfaces be provided in at least the operating area
around equipment, particularly those itemsfrom which falls are possible. The major con-
sideration in determining the surfacing must be theheight of the apparatus that isgoing to be installedon that surface and the probability of a drop ontothe head from that equipment. (NZS 5828: part
1: s105.9.1)
Impact absorbing surfaces include loose fill (forexample bark chips, pea gravel, sand) andsynthetic materials (for example rubber mat-ting, rubber tiles, wet pour materials) andnon-impact absorbing materials include conc-
rete, asphalt, bare earth, and grass. Additionalrequirements relating to the particle size,depth, and retention of loose fill materials are
specified (NZS 5828: part I: s105.9.2.1). Aprocedure for testing the impact absorbency ofsurface materials, based on ASTM F355-78,3°is specified, with which the 'critical dropheight' for any given surface can be deter-mined. Critical drop height is defined as 'aheight in metres at which head concussion mayoccur, resulting from a peak deceleration of250 g (or a severity index of 1000) or higher'(NZS 5828: part 1: s103.1).
(3) SAFE FALL HEIGHT
The range of heights above a specific surfacingmaterial from which a child may fall with a
minimumpossibility of head concussion. (NZS5828: part 1: s103.1)
This requirement relates to both height andsurfacing, and to assist in the selection of a
suitable surface material, given the maximumfall height of an item of equipment, a table of'safe fall heights' for a number of common
materials is provided (NZS 5828: part 1: tableAl of Appendix A).
The authors wish to thank Dr Gordon Smith, Dr Jean Langlois,and Dr Anna Wailer for their assistance in formulating thehypotheses and in designing this study; Ms Sheila Williams forstatistical assistance; Dr Penelope Keyl and Dr Ron Somers fortheir corments on earlier versions of this paper; Dr Peter
Bamford, Mr Alan Chirnside, Mrs Shirley Searle, and thereception staff of the Dunedin and Christchurch Hospitalemergency departments for their cooperation and assistance inascertaining cases, and the principals, secretaries, and staff ofearly childhood education centres and schools for their coopera-tion and assistance in ascertaining controls. We wish to ack-nowledge also, the support and assistance of local authorities andeducational authorities in Dunedin and Christchurch. Finally,we wish to express our gratitude to the children and their parentsfor agreeing to take part in this study.
This research was funded by means of a grant awarded to DrsJD Langley and DJ Chalmers by the Health Research Council ofNew Zealand. The Injury Prevention Research Unit is fundedjointly by the Accident Rehabilitation and CompensationInsurance Corporation (ACC) and the Health Research Councilof New Zealand.
1 Chalmers DJ. Falls from playground equipment: an over-view. Proceedings of childhood injury prevention forum.Wellington, 23-26 September, 1991. Dunedin: ChildAccident Prevention Foundation, 1992: 1-9.
2 Chalmers DJ, Langley JD. Childhood falls from playgroundequipment resulting in admission to hospital: descriptiveepidemiology. In: Sime JD, ed. Safety in the builtenvironment. London: Spon, 1988: 226-37.
3 Chalmers DJ, LangleyJD. Epidemiology of playgroundequipment injuries resulting in hospitalization. .PaediatrChild Health 1990; 26: 329-34.
4 King K, Ball D. A holistic approach to accident and injuryprevention in children's playgrounds. London: LSS, 1989.
5 Nixon J, Pearn J. Death during play: a study of playgroundand recreation deaths in children. BMJ 1981; 283: 410.
6 Pitt R, cited in King K, Ball D. A holistic approach to accidentand injury prevention in children's playgrounds. London:LSS, 1989.
7 Standards Association of New Zealand. Standardspecification for playgrounds and playground equipment(NZS 5828: 1986). Wellington: Standards Association ofNew Zealand: 1986.
8 Standards Association of Australia. Australian Standard forplayground equipment for parks, schools, and domestic use(AS 1924: 1981). Sydney: Standards Association of Aust-ralia, 1981.
9 British Standards Institution. Play equipmentintended forpermanent installation outdoors (BS 5696: 1986). London:British Standards Institution, 1986.
10 Canadian Standards Association. A guideline on children'splayspaces and equipment (CAN/CSA-Z614-M90). Rex-dale (Toronto): Canadian Standards Association, 1990.
11 ASTM. Standard consumer safety performance specificationfor playground equipment for public use (F1487-93).Philadelphia, PA: American Society for Testing andMaterials, 1993.
12 Evans MJ, Chalmers DJ. Compliance of Dunedin playgroundequipment with the New Zealand standard (NZS 5828).Dunedin: Injury Prevention Research Unit, 1992.
13 SacksJJ, Holt KW, Holmgren P, Colwell LS, Brown JM.Playground hazards in Atlanta child care centers. Am _7Public Health 1990; 80: 986-8.
14 Sosin DM, Keller P, SacksJJ, Kresnow M, van Dyck PC.Surface-specific fall injury rates on Utah school play-grounds. Am J Public Health 1993; 83: 733-5.
15 Mott A, Evans R, Rolfe K, Potter D, Kemp KW, Sibert JR.Patterns of injuries to children on public playgrounds.ArchDis Child 1994; 71: 328-30.
16 Briss PA, SacksJJ, Addiss DG, Kresnow M, O'Neil J.Injuries from falls on playgrounds: effects of day care
center regulations and enforcement. Arch Pediatr AdolescMed 1995; 149: 906-11.
17 Ball D, King K. Risk in the playground: the case of syntheticsurfacing. The Leisure Manager 1990; March: 21-3.
18 Suctliffe R. The real case for synthetic surfacing? The LeisureManager 1990; April: 13-4.
19 King K, Ball D. Synthetic surfaces [letter to the editor]. TheLeisure Manager 1990; May: 8.
20 Suctliffe R. Playground equipment and safety. The Ground-sman 1990; 43: 19-21.
21 Jackson H. The controversy over playground surfaces.ChlldSafety Review 1992; 6: 3.
22 Ball DJ, King KL. Playground injuries: a scientific appraisalof popular concerns. JR Soc Health 1991; 111: 134-7.
23 Association for the Advancement of Automotive Medicine.The abbreviated injury scale (1990 revision). Des Plaines:Association for the Advancement of AutomotiveMedicine, 1990.
24 SAS Institute. SAS language guide for personal computers,
release 6.03 edition. Cary, NC: SAS Institute Inc, 1988.25 Hosmer DW, Lemeshow S. Applied logistic regression. New
York: John Wiley, 1989.26 Warner KG, Demling RH. The pathophysiology of free-fall
injury. Ann Emerg Med 1986; 15: 1088-93.27 Rothman KJ. Modern epidemiology. Boston: Little, Brown,
1986.28 Hosmer DW, Lemeshow S. Confidence interval estimation
ofinteraction.Epidemiology 1992; 3: 452-6.29 Walsh P. Fixed equipment - a time for change. Australi'an
Journal of Early Childhood 1993; 18: 23-9.30 ASTM. Shock-absorbing properties of playing surface systems
and materials (ASTM F355-78). Philadelphia, PA:American Society for Testing and Materials, 1978.
104
on April 2, 2020 by guest. P
rotected by copyright.http://injuryprevention.bm
j.com/
Inj Prev: first published as 10.1136/ip.2.2.98 on 1 June 1996. D
ownloaded from