heart rate after cardiac transplantation -...
TRANSCRIPT

Heart Rate after Cardiac Transplantation
By W. BECK, M.SC., M.MED., C. N. BARNARD, M.D., PH.D.,
AND V. SCHRIRE, M.D., PH.D.-
SUMMARYTwo patients who have undergone heart transplantation 7 and 15 months previously
were studied to determine basal heart rate, the effects of exercise, and acute changes invenous return and blood pressure as well as of vagal stimulation. In one case the effectsof body temperature, isoprenaline (isoproterenol), beta blockade, and atropinization onheart rate were studied. Mean resting heart rates of 110 and 90, respectively, wereobserved in the two cases without any significant change with time since the surgicalimplantation. Sinus arrhythmia was not observed and heart rate was found to increasewith exer'cise following isoprenaline infusion and following increase in- body temperature.A'decrease was observed after beta blockade, but no significant direct or baroreceptorreflex effects could be produced by changes in venous return, systemic blood pressure,,vagal stimulation, and atropinization. Both patients are thus effectively denervated,and there is no evidence of reinnervation to date.
Additional Indexing Words:Atropinization Blood pressureBaroreceptor reflex Exercise
Reinnervation Vagal stimulation
CARDIAC TRANSPLANTATION resultsin complete denervation depriving the
heart of one of its major rate-regulatingmechanisms. It is the purpose of this paper toreport on the resting heart rate, changes thatoccur after various circulatory manipulationsin the denervated state, and on the search forevidence of reinnervation in two patients whohave survived cardiac transplantation for 15and 7 months, respectively.
Report of Cases and MethodsCase 1The first subject of this study was a 58-year-old
white male who underwent cardiac transplanta-tion on January 2, 1968, for intractable cardiacfailure due to ischemic heart disease.' In additionhe had generalized atherosclerosis with nonsymp-tomatic peripheral vascular disease. The donorheart was obtained from a 22-year-old Negro
From the Cardiac Clinic, Groote Schuur Hospital,the Council for Scientific and Industrial ResearchCardiovascular-Pulmonary Research Group, and theyDepartments of Medicine and Surgery, University ofCape Town, Cape Town, South Africa.
Circulation, Volume XL, October 1969
Beta blockadeIsoprotereno'
Venous pressure
male who had had a fatal subarachnoid hemor-rhage (table 1). Postoperatively the patient re-quired digitalis and furosemide to assist his cardiacstatus. Maintenance immunosuppressive therapyconsisted of prednisone and azathioprine. A courseofil:tilymphocytic globulin was administered 6months after surgery, during an episode of acuterejection. His clinical course has fluctuatedbetween being reasonably well and active tobeing virtually moribund. The latter state hasbeen attributed to an episode of acute rejectioncomplicated by Listerella monocytogenes septi-cemia and severe jaundice presumably related toazathioprine toxicity. Prior to this he had had atleast one episode of deterioration t6f cardiacfunction with signs of circulatory `insufflciencydiagnosed as a minor episode of rejection,requiring increased dosage of immunosuppressivedrugs. For the past 6 months and up to the timeof writing his condition has progressively deterio-rated.- His effort tolerance is obviously reduced,mainly due to dyspnea and partly due to atrophyof the leg muscles (peripheral vascular disese.plus steroid myopathy?).
Clinical signs of congestive heart laiiAre7'we6einitially 'difficult to evaluate because 61-the ef`fftsof large d'oses of steroids but latterl'ypeip`isf-stlyielevat6d jugular venous presstresightIheia-tomegdy, and edemae df -the :1cgsthav bee
437
by guest on April 22, 2018
http://circ.ahajournals.org/D
ownloaded from

BECK ET AL.
ABO and Le2Q Tabl g Is
Incompatible Reverse TentativeAM1 4 ,t* .- A Mismatches: gradingenticai donor +ve donor -ve after
ABO ab ab r - ;cjd ,a antigens recipient -ve recipient +ve Terasakia~ ~ ~ ~~ ~ ~ ~~~~~ba b
tCtt*iA r!--Case 1Donor 0 ++ ++ + + -- -Recipient B -+ +- + - - 2 4a, 6b SyAii!:yv CCase 2 Kii IUa2 'U U8. I il &
Donor F i<h g' u .: 0 fRecipient `42-43'i'''h +'- -a -r4b,ei C
"RyJf,5iI.. UI .2-4A. 1.-
tp;c) Z'I l,
i{^")'!U 5{tk cR;wXi? jI v 42e|ft0 5>> 'J(j-;1 44^tt Z,f,,I Xw3l9present.. lgeds%sstp IoaM1'Chti;ge-s-, itn-VeI?ots e turtiMdevelope tRWtelglvtEntaffiX,\9,5f ulq s m venousthe apex,, ges v, 0 3 ee <3 4w i-rj employed.Radilo°gl? et slaw atWi>s bee9n.TIgV(1lvjSmaepySj'y2s rwj4wth theabnorrnalV' I]}C PiJ('ULin*g!( asibnsize. lt>djr s
,p! EYfelYmC71iX;Ea iatisantfSUtypfe irNE ?grassulre ofin size. e eYectrocaretogram nas r,wi1 fa p e1n QttI 15 sec.persistent sinus tachycardia. Extensive T-wave Arterial pressure was recorded trdi a needle ininversion has developed in the course of time.2 the radial artery, and the heart rate was measuredPartial catheterization during the second acute from tbh ji. ffip 2;res fso alteredpbstoper~tisoA~~ 9onfirmed the presence of .LyanggigRbody °postoper g bod -~~~~postue, ~ embent to
an abno~4-j)81`sFentral venous pressure a hnprgt oitonteaIie suringan abnormaI1y lacutut. tte, venous presawr aic output by
Resting heart rate nav been recordea Dy lthe-dye-dilution technic. A manometer was fixedelectrocardiograms performed daily or every to the patient's chest at the level of the tricuspidsecond day initially and latterly at twice weekly valve to minimize changes in zero level.
Ahe ip qt ~sN*4tS hi stW4JIutnt *i3 kils-34fr res inAqrtic Pr4essurzrn*ais's0I e3iotciz* dABic4 '~Wsk t th Aegie%t$ueinS. i a-art lw ste~iJ#r!" siii,r¢za,JMLj s >IMq1r indfre&I7tr,41e4 were rneasiiredf aft r oamy7I fnJ)fre~~ A'~~rJ%wia ~~~& s~~e!jw ~~$bmy~ rianwrip
Dlspfj&uei* vas AbmItgAe flQr 'W q hi2 ikis i; pEbioxgk0eaefsohu£r gf~s me~ie lysthrWf4j aKl Bt g P<4W5~froa- atIoItiaud(y rzina eJngmonitpred. The efctpt of v.aga- stimuy t ion
iQwti£it xi +edeaJotiiwe. p fg day -a sta#t4 Wgoiti1tI1r34alli>fi&I& ffe;74YfM*alevextastr&<}eF*oay drugs, such as aw 4,*l4 Xfig wtef aXbeiateeordidTh f̂f m1 b4y,tXppextwe intravenously, pro}ranolol 0.2 mg/kg intravenous-aatht iitw rear4d l> UtirIh a* >t1 ly and nb is- alets art ratemi4nghraxItea Jyduning;$r)br ill were observed.CnLrks~imding*t"fLthe 4irkt~ 2pwQdO OfZ re}etiQuttovANlu)Rofdthuq4f ra4t etc rwsejiaSk, V;' ' sir'
*3rh( iQ*tAt sA rtfte,4ihojtAR of~a£¢ 41$lig£os k % ld .tiWn4j Qa* tt£M. wtsY;ismepe3 arwn roa 1 ,euomsSsi us pessure atng e an
vbhuw*sty4riadl letween aod:. 11 iFA-.tvr r shewJie&hair 8Eial No eJmo Uvrfrfo~iistii*tioRi nfW prft'aololXt eFr0(X2 ~a5ot a yeai},½ittr j'wEic~hr 'o'Anti6ie Ie4rlot*mg/kg of body weight ixwn tbopai rated and when seen_hereL his disability was1# t -#a jwnJfiri4 )]?yfiar,;to a totk(fT o>^gtfif< 16t-t i1)tmA) z31moi'nQ]
,en<-7hf l>f Nkn<~e 8fbraefw~-- pres~ence of sevpv>tJ it. £w0e1uit-a-jlVozeQ4i QcckAr\4
.-
438
by guest on April 22, 2018
http://circ.ahajournals.org/D
ownloaded from
IEART RATE AFTER CARDIAC TRANSPLANTATION
;left !r riMu1SrX ordial7-al d;ysfunptiqpC2 withinsignificant mitral and aortic insufficiency. Car-diac allograft transplantation was performed on
rSeptember 7, 1968 _4he donor heart being>~nehttSi&';1ir6 ini 6-year-old hypertensiveiaiewa e, 4- hypertrophfid heart (table
1 ThM ptttenTt was g1Ve5n an initia4f course of anti-lymphocyte globulin and q presenetis being main-tained on steroids and a"othiopriie but has notrequired digitalis or diuretic therap:y since his dis-charge from hospital. Hist'xercise4olerance is ex-cellent; the heart size has rtmained ormal and un-changed throughout. Tberei has bee no reductionin electrocardiographi&t v>oltae, iandrthe,_ST-Twave changes of severee¢:lef-l-veiitricula= yper-
,trop1yhyase isappeare. H -ilias7hai ho; funk>-epis6cdes of rejection or erios2 compcttnE of
immunosuppressive therapy. *PeTrissionA to ter-form full hemodynamid evaluatibn has beenrefused, and we have been able to observe qnlythe resting rate and the,-"effects f the Valslvamaneuver, posture, exercise, amylinitrite inlfla-tion, and vagal stimulation on 6ne occasioi 7months after operation.
; ''i s t§- 'v 0'E 'J it - -', 8¢_>,ults CDOThe mean monthly heart rate at rest for the
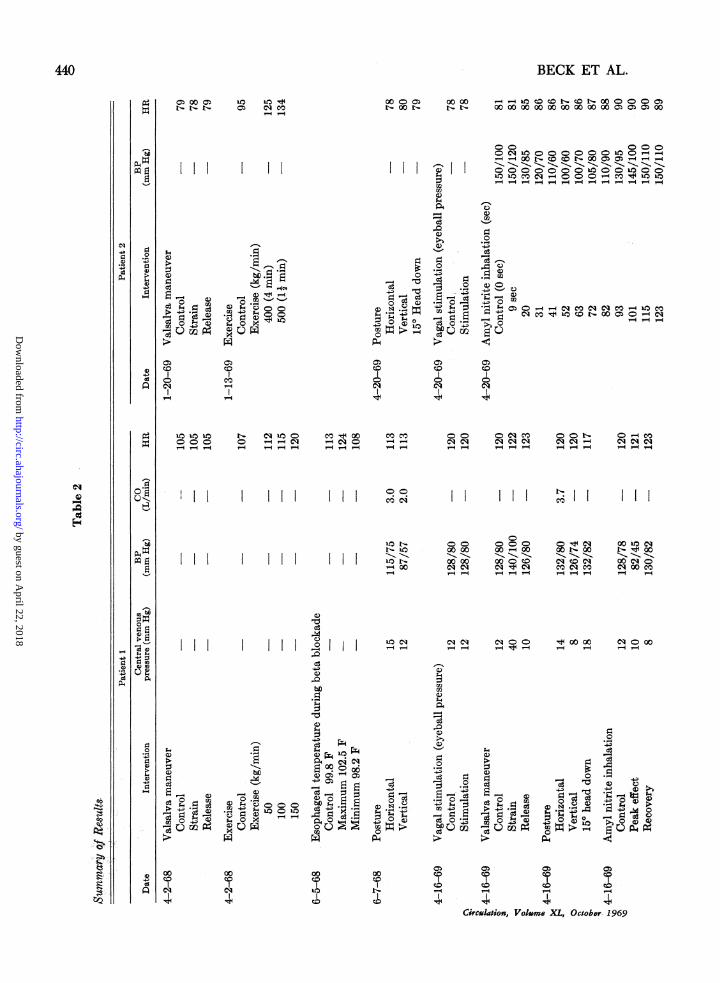
first two patients is shown in figure 1. In thefirst patient the heartyrate has varied between,
5 5 and i1 beaits/m at rest, an fRi the'second patient between 75 and 105. There has
[,_ben rpsignificant,g(hangei,Jt mean iqnWthly.'<4lues> thieiratiop eit1f&-_3case.!
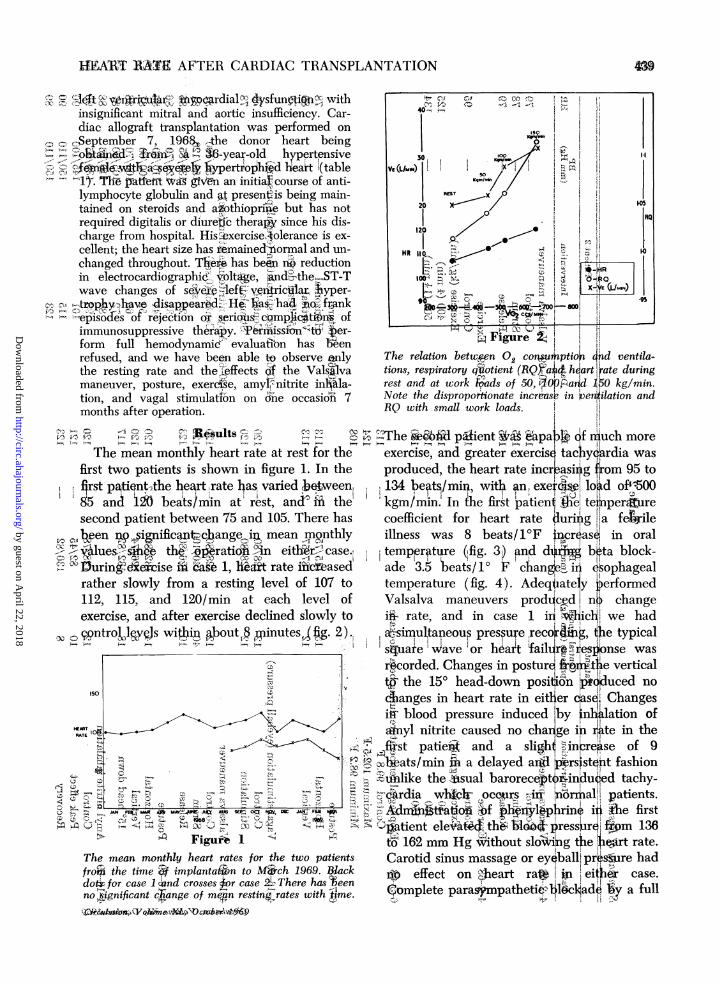
XlDuring- icise iig b`ak 1, ihZt rate ifcbasedrather slowly from a resting level of 107 to112, 115, and 120/min at each level ofexercise, and after exercise declined slowly to
; q0 ntroljjvW winip ibout1;minutesfg. 2)..
ISO
X~~~~~~._
tr~~~~~~~1JAN FE!.q M MMUE J *J SEfr' Ota PM DM JA.FERFt6.
Figure I-The mean monthly heart rates for the two patientsfroF the time implantaion to Mich 1969. Blackdo for case 1 '!nd crosses or case There has ieen
no jignificant ch(ange of metn restin ojrates with 4me.
toi&^st..X pn6$gg
The relation betwpen Q coruiptioi 4nd ventila-tions, respiratory quotient (RQXain heart ate duringrest and at work kads of 50, -iO arXd ,50 kg/min.Note the dispropotionate increase in peroilation andRQ with small work loads.
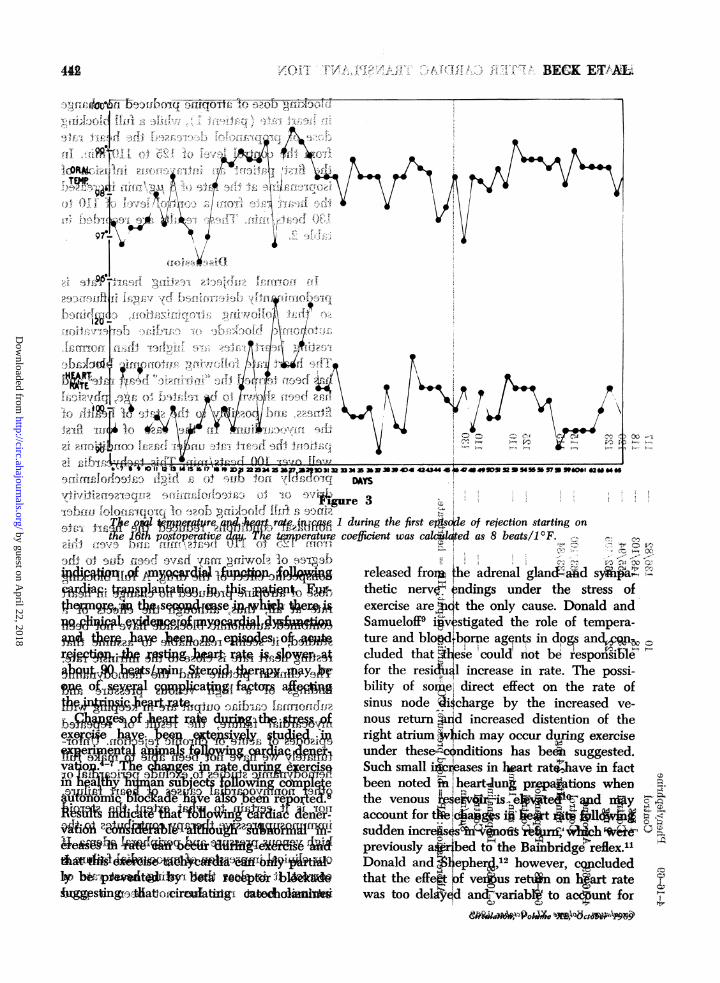
The @&6fld pMient &apakg df niuch moreexercise, and greater exercise tac yqtrdia wasproduced, the heart rate increasiig from 95 to134 beats/min, with an, exercaiw lo d of-''500Xkgm/min. In the first patienl ,Wel teper urecoefficient for heart rate durig Ia fetxileillness was 8 beats/10F inr as6 in oraltempjerFture (|fig. 3) and dipji beta block-ade 3.5 teats!o1 ; chang irn esophagealtemperature (fig. 4). Adeqtsately performedValsalva maneuvers produced nW changei.i- rate, and in case 1 in wicli! we hada,-simultaneous pressure recordii4, te typical
is4uaae pave or heart failurd tFhese was
,r,corded. Changes in posturE fi te verticali;p the 15° head-down positoion &iduced noclanges in heart rate in either qasqJ Changesiii blood pressure induced 'by inNtlation of.inyl nitrite caused no chaiige inrlte in the
f.ist patiei-A and a sligh in re4se of 92\ hsi ats/min ii a delayed ard iirsnsteit fashion2fiu'nlike the sual baroreceptoinsinduqed tachy-7&Ardia whkoI- occwrs, an lormaW patients.ids 'tla6oi bf hlphrmn ii the first(it atient eleiba'cth& b poressre ftm 136
to3 162 mm Hg without slo6Witg the ort rate.Carotid sinus massage or ey ball: pr s ure hadlb effect on jheart ra*. eiter case.
Complete paras;mpathetie ll&cl ad'a y a full
9a
!7-;
.-;
InI-I
C",0 11 Fr,
HEART -"RATE 14
C45ttt-)=I0
by guest on April 22, 2018
http://circ.ahajournals.org/D
ownloaded from
BECK ET AL.
I0 i R1
I- "14
o Z,
000C0) 00 00 _- " o CD coQ 0000 0Ct o0ot- J - oo oo 00 00 00 0000 0000oo o00
1-4
,0
.a)
0
c3
Ca0
-. d cd
0 0-00
0N 0CO CO
--00 )0 O')10 10 CO O- 000O O 101
- --q -- - - -
CO
o u:C- es xo0 o rc
-4 104
0
COI_ HH~HH_
0eq
10110 t- C t10o CO 100 cOo00 0 o o - C) o--- - -4 - - - - - - __-4
I I I 0 0.
00O)C)eqCO ,c001z 0CO.c'0 Ne Ceqeeq qcq eqeqeqCP- r- r-i "- -i V-4- - r- -4 r-
11 HI
U1D1- 00C 000It<-t 0000 00o-o00
II t o X oo000 CO- 00 o cq ea 'cq- -- -- -
0
.0
q1)
bC.5
S S cqo q
> _ ~~S50o *
.00
too
la C9 q C' C 0 'O q 00 00 C o o00
'.4
0
'.4 ~~ ~ ~ ~ ~ ~ 4
04
0+ 0
('s C) E g$+4 0 0.-¢
C3 -a 0
14 -~ 0-
COCO
CO
Circulation, Voimne XL, October 1969
440
0.2a
0
4)
140
4)7)
ka)Q
0Sa
C30C3m
c3
mf*
C5)
r-
3o SV ;-
_E4
4)-4;
4
00t- 00qo CqeCS CO C'CD eq cor- r- Y-
0010l eqt-lq 00
ooq 00 C4-4 4-4
to
0
044
.H
a)04
04
.4-0
0
(14
0
14
0
'4$.
41e 'OD
.400
.44.C
S. ,t2
00
COeq
00cooC4eq
by guest on April 22, 2018
http://circ.ahajournals.org/D
ownloaded from

HEART RATE AFTER CARDIAC TRANSPLANTATION
t- a)o c e10t O o'q '> cl N - C4 cr-
C:cq1 0 "tiCO -OCo CD La NCO dq e coT-q r-- --4rq
qOCO
Co
0COCO ~I I Ir--l r--l r--4 Cq
S1) ;- c
c = S c U E ; o E E ° t
O 0 "1
bo
00 P4 0 0 :3.
O COC.0 C.0~~Io
$ 4 ~ ~ ~ ~~~~~~~ I IC C.c0 Co
Circulation,. Volume XL, October 1969
blocking dose of atropine produced no changein heart rate (patient 1), while a full blockingdose of propranolol decreased the heart ratefrom the control level of 125 to 110/min. Inthe first patient an intravenous infusion ofisoprenaline at the rate of 8 ug/min increasedthe heart rate from a control level of 110 to130 beats/min. These results are recorded intable 2.
DiscussionIn normal subjects resting heart rate is
predominantly determined by vagal influencesso that following atropinization, combinedautonomic blockade or cardiac denervationresting heart rates are higher than normal.The heart rate following autonomic blockadehas been termed the "intrinsic" heart rate3 andhas been shown to be related to age, physicalfitness, and possibly to the state of health ofthe myocardium. In the case of our firstpatient the heart rate under basal conditions iswell over 100 beats/min. This tachycardia isprobably not due to a high catecholaminedrive or to catecholamine supersensitivitysince a full blocking dose of propranolol undernonbasal conditions reduced the heart ratefrom 125 to 110 beats/min and even thisdegree of slowing may have been due to thenonspecific effect of the drug. A full blockingdose of atropine produced no change in heartrate at all; thus, although the effects of a
combined autonomic blockade have not beenstudied, it seems reasonable to assume thatresting heart rate is close to the intrinsic rate.The clinical picture and the hemodynamicfindings of a high venous pressure andsubnormal cardiac output are in keeping withmyocardial failure, the result of repeatedepisodes of acute or chronic rejection. Unfor-tunately we have not been able to make fullhemodynamic studies to exclude pericardial or
other nonmyocardial causes of heart failure,nor is it certain to what extent the steroidimmunosuppressive therapy contributes to thehigh venous pressure and peripheral edema. Ifour clinical impression of myocardial failure iscorrect, it is clear that resting heart rate or
intrinsic heart rate has not been a good
11
&4
;4'
c)
14
0
a30
04
c;
-4'
110
Ua2&40Ai
m*.on
0e-pQo
¢1
441
by guest on April 22, 2018
http://circ.ahajournals.org/D
ownloaded from
r- '4!,, BECK ETA
JR4 lu 5, .4- 4
i 4i-%~~~~~~~4
4g\tr~ ~~~~~~~~~~~~0-3@ f5 ,,2 vss=St 5Xsr
t f -tz;e s$i z2}£4,$;...........................r,, 20;{t -5tFy<S
0.~~ ~~~~~4i/ -v
F.~~~~ ~~~~~~~~~~~~ r s*o-l s---E- £s, T'
,l f rf-f /-,
r t-4j . 4. 4 43
t-ab i fl-lo-fune-olc3i 10f'''7 g@io-b-l-no3fQ-';I f--vr I t.T1rJr, effX 3 'U-f,D's ffi.S L^N,sy8>7 Sf'fffli t I V
tIART ~ Ij6 postoperati ze c i wa .& edI 8I beatsIOF
I 4~~~~~~~~~~~~~~~~~I-
~ 4:(~lfe4~(fJ!Ire raeratururn,h irteljo'eo ejcinstrigo'I w 9o D eilv;ti ft it-fa t :SgX - miajaO !r
.7 S-e po£opertavfdwq. Th,e t4nperatuie coeffcient was clakWked as 8 beat.s/i 0F. ,-a -, 4-9sVi).§fX).1,.S,i,,4f.4t%.01 '144_:X\L.,.-A f ,*r-3fi, i -ojgb api9t)If !Fjv d- -a:pf-jl-sgvyofiA lIo bE3
ea9jn tbs seMhY#i,.,e ursfingeers
.i 1t83,S£9j;e9Aer.l9fItuu1h
WW,.Osme g wtfdTXp4% 3
imnaIm an su ject tuowin cormoIe
g a so 4 f
~uggesking r iacirafaltfo rtgia d o1I fixior,^gf t T kr
sing .^<>.-ea.-cig dlhln*
released frorxt the adrenal glancf4id syk#hthetic nerve ndings under the stress ofexercise are Qic t the only cause. Donald andSamueloff9 igvestigated the role of tempera-ture and blo,drborpe agqnts in dogs andc1cluded that §14ese couldrnot be responsibilefor the resiA&l increase in rate. The possi-bility of some,; direct effect on the rate ofsinus node Oi$charge by the increased ve-nous return ?and increased distention of theright atrium 4ich may occur duning exerciseunder these4xcnditions has beei suggested.Such small iiWreases in heart rat"have in factbeen noted biheartung prations whenthe venous Ie tsbe: id nyaccount for t;c gs io: rt :lsudden increes sno r %ch Xpreviously a#.bed to the Bainbridgereflex.1Donald and 3liepher, 12 however, cq ludedthat the effe" !f veius retfin on h%art ratewas too delhd an-variablt to acdTunt for
C.">PC-
\t8
442,
f'tw in?,,
TEMP.
97
-1-:, 0 f,~
4.4Q(.
.4
by guest on April 22, 2018
http://circ.ahajournals.org/D
ownloaded from
v I I I
HEART RE AFTER CARDIAC TRANSPLANTATION 443
v . 4-i-.i . 5; ? iQ.
§ei-t F0e~dS-,- *+; Xs tp;>t,,;,2-IM.Aw_
f J. I |4
-;wie;) H }; 4Z .J; 06b <, x *t ¢- r Xa [ w1 t i, 2"a ¢S^
REWMIII '
- t. J,S.j
t 7-1;*[ t
f -r<Y;wa>t 1J
ft t't8; ~
T..
[f ffff i2-jS'>f) j-,-,tt'",fl g 9 iZ ) <} j )\^g ', _% . ,f [ t.t {) .{ g X S ( t. 3 2 ' t s 4 A t1 A c} _;) f5.8 3 .-3.f X ifl,;, §. .e
z
5 tr rf i.O (.J gRCGq § i ). - &.'vS 'S( t> t xD >9 7, r T $ X ; lr i ¢5 }'
:..j
v :e.
s S T otaJ s z [() '-t >'+C j >.tsr v R w 4 f > / = s. t s -? Si. ''2. s. .-'.$ 't' ".-<- (
,, C X .-t-r;;z.<'1 tr- .
§ g i ;§ 2 ; > 4;
J§' ''i ' @' } ' - ,. <. $ 0 if L e i' . >: 7r,-s s j*,-- t ,aj ; b [-E E e j I so t gc WS8 ,4;, ,2 , - x w (, ,d . ) j 4 > *4 e w $ 2 . u rvi t ja;¢ ,', 7 w ,5 s t iW § t 8 ; ' ' fi ' '*; i- i ' ^; d c-- . r c i t'i ^' t ;^ g -s 0< it:D i; $ t + - r 2 > M s
i3tW_2 > >,
t v 0g t ;,+,j , ; .i.-.d,0.U.s
H R k X t r - j-s
8 . - 9 c- t, | § } Ji -t A fi t
J ; 7 , ;s t.' [ {,' r>;; - ej; v. * t- a {!, N * X ¢ * r, 3 't * 4 > M r *..;,.t
i 7 @".f wR ,$ i ;t a r, Es;s,r s _., D _, ..... f st \ L:> r ) F r.t E r,-t t * i
i f. y fi _ i, , ,r S t\tv -r - § {? - tt @ (3 3 -:; a, ._e f 8 z
4'5ggA CSJt4 ->r3<>>-rOr
3,' _t.,S,_ $;=;--[ , t i ¢ X \ 4 azi > ;< tcfb 7.' *-*4* x Q J J < r 5 > .e W r >_ ..@ < . .. t_ftSS, " /-- X * - -- r ^ s J '. $ f te t -i 4; )rw- b 9 1>
)-) J, ,.
-iI-v ,~ik
P. I,.
IIJ'Of
*rv 7 s -<9f .3f4) ;' 3t..S.w.
| 2~~~~~- O;e tr x^ .i'attr 0
zl:T f-"-. . .§.. ' _ ''.;t J sX ..... }S 2g ,i iiS flsa i~~Af
d.ll
t: -I[\.Rt-,- y3, ,liftAR
C->Tw '
Sr7?f X
- s vr-+S
Z-t rlsa
S$ ,r-
-XE )
st (',_.
.t[w$-X.,. .t
a ;.
T.,)i
fi -.-! i $
X s:,),
.'-' '#'C r
,S'0 i_ '$ g
IJ
ol rl-.
E ,;9'_.t
< j 6 - X, i R si 4 ; t cn k i :-A ( i <
V .' N r 4 ,. ,^, S>} ; g.'t i 4vS t y x S ' ;j JlS X g p< t g .;t 3 .x z 1t\&t i k 1W;d . f?f.; g-to ors yo-it S st. t- {s.; to ? E 2+ ,_ t rt ,, 9 jf § 2-jb f-,tF'Kvo* T +, t g f > r z 6'' f x, t--s
~~~~~~~4w . ? i t;3 .1t. I , I I g >=g*rgt<Is-S
557 39ti]t13tji 6Q-Pi>/\-t5S1,nfq ;MS"p>ki>fp
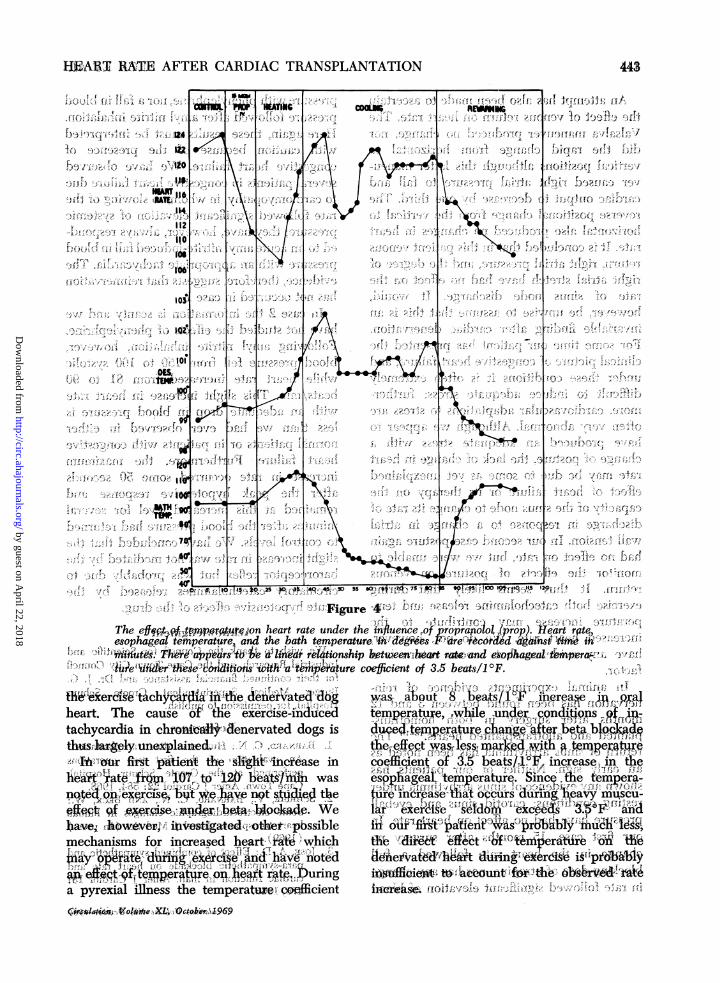
The efffpt^f-E-,;t su q,n heart rate under the influeneof rornlol "XPr`p Reart rgtq.2 -esophageaItrature'and the bath temperature.VVdfiAg*s,--Fre diW#d -a'di-st h>;H22t
ttfiift-tiZtetW teffiperaurBnwi#%e c<0cin o . bas1°F4-i$ss ,r k5,>*e 6.sopa-. i- tw , '^ 6&'i)
heart. Thcas oe eecs-n she e y e;ielacn a.fFttachyear teiain cti1;de vte Adt idogs ip beted,emW itraw-,adetrhgud,9aI\~t<fu -retei sw-;icaei coe&fiient of3.5beatsl :,inreseOF.f
teF. ierk fwg&`tachL figedgatedffI d'r-posii1 pu:ff;)ftit8qaj re>W=mcr6e
apyrexil illnes te tmea,ie nt tepratueieXX;gg ",unde_jg~',,>r F, ,,g,,; l't <
CN,,I ,,J'O %lie...cOt.^;I&
by guest on April 22, 2018
http://circ.ahajournals.org/D
ownloaded from

BECK ET AL.
An attempt has also been made to ascertainthe effect of venous return on heart rate. TheValsalva maneuver produced no change, nordid the rapid change from horizontal tovertical positions although this latter maneu-ver caused right atrial pressure to fall andcardiac output to decrease by one third. Thereverse positional change from the vertical tohorizontal also produced no changes in heartrate. It is concluded that in this patient venousreturn, right atrial pressure, and the degree ofright atrial stretch have had no effect on therate of sinus node discharge. It would,however, be unwise to assume that this is aninvariable finding after cardiac denervation.For some time our patient has presented theclinical picture of congestive heart failure, andunder these conditions it is often extremelydifficult to induce adequate stress; further-more, cardiovascular adaptations to stress areoften very abnormal. Although we appear tohave produced an adequate stress with achange of posture, the lack of change in heartrate may be due to some as yet unexplainedeffect of heart failure or its therapy on thecapacity of the sinus node to change its rate ofdischarge in response to a change in atrialwall tension. In our second case posture againhad no effect on rate, but we were unable tomonitor the effects of posture on venousreturn. It thus seems likely that duringexercise both catecholamine release and tem-perature increase may contribute to theincreased heart rate. We do not, however,have any evidence that venous return is afactor.
In animal experiments evidence of rein-nervation has been found between 3 and 12months after surgery in both homotrans-planted and allotransplanted hearts.'3-16 Therelturn of sinus arrhythmia has been noted asan early sign. Neither of our patients hasshown any evidence of sinus arrhythmia underresting conditions; carotid sinus and eyeballpressure have had no affect on heart rate. Inour first case, 15 months after surgery nochange in the heart rate followed a fullblocking dose of atropine, nor has any changein rate followed significant elevation of blood
pressure with phenylephrine, nor a fall in bloodpressure followed after amyl nitrite inhalation.Here again, these results must be interpretedwith caution because of the presence ofcongestive heart failure. We have observedseveral patients in congestive heart failure dueto cardiomyopathy, in whom no slowing of therate followed significant elevation of systemicpressure; they have, however, always respond-ed to an acute amyl nitrite-induced fall in bloodpressure with an appropriate tachycardia. Theevidence, therefore, suggests that reinnervationhas not occurred in case 1.
In case 2 the information is scanty and wehave not studied the effects of phenylephrine.Following amyl nitrite inhalation, however,blood pressure fell from 150 to 100 systolicwhile heart rate increased from 81 to 90beats/min. This slight increase in heart ratewith an adequate drop in blood pressure isless than we had ever observed in eithernormal patients or in patients with congestiveheart failure. Furthermore, the maximumincrease in rate occurred some 50 secondsafter the peak hypotensive response andremained at this increased level for severalminutes after the blood pressure had returnedto control levels. We have concluded that theslight increase in rate was not mediated by thebaroreceptor reflex but was probably due tocirculatory catecholamines released by theacute hypotensive effects of the drug.
AcknowledgmentWe wish to thank the Council for Scientific and
Industrial Research, and the Cape Town City Councilfor their continued financial assistance and Dr. J. G.Burger, Medical Superintendent, Groote SchuurHospital, for permission to publish.
References1. BARNARD, C. N.: Human cardiac transplantation:
An evaluation of the first two operationsperformed at the Groote Schuur Hospital,Cape Town. Amer J Cardiol 22: 584, 1968.
2. SCHRIRE, V., BARNARD, C. N., AND BECK, W.:Some electrocardiographic changes in humanheart transplants. Israde J Med Sci (In press)(1969).
3. JOSE2 A. D.: Effect of combineed sympathetic andpara-sympathetic blockade on heart rate andcardiac function in man. Amer J Cardiol 18:476, 1966.
Circulation, Volume XL, October 1969
444
by guest on April 22, 2018
http://circ.ahajournals.org/D
ownloaded from
HEART RATE AFTER CARDIAC TRANSPLANTATION
4. ASHKAR, E.: Heart rate and blood pressure indogs with autonomic denervation. Amer J
Physiol 210: 956, 1966.5. DONALD, D. E., AND SHEPHE:RD, J. T.: Sustained
capacity for exercise in dogs after completecardiac denervation. Amer J Cardiol 14: 853,1964.
6. DONALD, D. E., AND SHEPHERD, J. T.: Responseto exercise in dogs with cardiac denervation.Amer J Physiol 205: 393, 1963.
7. BnouHA, L., CONNON, W. B., AND DWL, D. B.:The heart rate of the sympathectomised dog in
rest and exercise. J Physiol 87: 345, 1936.8. SUrrTON, J. R., COLE, A., GUNNING, J., HICKIE, J.
B., AND SELDON, W. A.: The control of heartrate in healthy men: Preliminary communica-tion. Lancet 12: 1398, 1967.
9. DONALD, D. E., AND SAMUELOFF, S. L.: Exercisetachyeardia not due to blood-borne agents incanine cardiac denervation. Amer J Physiol211: 703, 1966.
10. BLINKS, J. R.: Positive chronotropic effect ofincreasing right atrial pressure in the isolatedmammalian heart. Amer J Physiol 186: 299,1956.
1 1. PATHAK, C. C.: The fallacy of the Bainbridgereflex. Amer Heart J 72: 577, 1966.
12. DONALD, D. E., AND SHEPHERD, J. T.: Changes inheart rate on intravenous infusion in dogs withchronic cardiac denervation. Proc Soc Exp BiolMed 113: 315, 1963.
13. DONG, E., Jn., HmuzRLY, E. J., Louw, R. N., AND
SHUMWAY, R. E.: Performance of the hearttwo years after autotransplantation. Surgery56: 270, 1964.
14. DONG, E., JR., FowKEs, W. L.. HuRixy, E. J.,HANCOCK, E. W., AND DILLSBURY, R. C.:Hemodynamic effects of cardiac autotrans-plantation of the heart. Circulation 29 (Suppl.I): I-77, 1964.
15. WILLMAN, V. L., COOPER, T., AND HANLON, C.R.: Return of neural responses after autotrans-plantation of the heart. Amer J Physiol 207:187, 1964.
16. LOWER, R. R., KONTAS, H. A., KosEucy, J. C.,SEWELL, D. H., AND GRAHAM, W. H.:Experiences in heart transplantation: Technic,physiology and rejection. Amer J Cardiol 22:766, 1968.
wr-w-w w v W-w ww-_ww w w v Wl w w v lw
I
OSTAGE YEMENARAB REPUBLIC
Circulation, Volume XL, October 1969
445
by guest on April 22, 2018
http://circ.ahajournals.org/D
ownloaded from

W. BECK, C. N. BARNARD and V. SCHRIREHeart Rate after Cardiac Transplantation
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1969 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.40.4.437
1969;40:437-445Circulation.
http://circ.ahajournals.org/content/40/4/437located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. and Rights Question and Answer
Permissionsthe Web page under Services. Further information about this process is available in thewhich permission is being requested is located, click Request Permissions in the middle column ofClearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of the CopyrightCirculationoriginally published in Requests for permissions to reproduce figures, tables, or portions of articlesPermissions:
by guest on April 22, 2018
http://circ.ahajournals.org/D
ownloaded from