heart failure orthopedic nurses education day jeffrey p schaefer msc md frcpc october 30, 2006
TRANSCRIPT
Heart FailureOrthopedic Nurses
Education Day
Jeffrey P Schaefer MSc MD FRCPC
October 30, 2006

Objectives
• Heart Failure– definition– epidemiology– prognosis– diagnosis– management
What is Heart Failure?
A complex clinical syndrome that can result
from any structural or functional cardiac
disorder that impairs the ability of the
ventricle to fill with or eject blood.
American College of Cardiology 2001

Cardinal Manifestations of HF
dyspnea fatigue
limits exercise tolerance
fluid retention
peripheral edemapulmonary congestion
impairment ofFunctional Capacity and QOL
“and / or”

Incidence of CHF
Staging of Heart Failure
NYHA Cardiac Status
• Class I: uncompromised• Class II: slightly compromised
• Class III: moderately compromised
• Class IV: severely compromised
– updated from old NYHA Classification• ‘usual activities’ ‘minimal exertion’

Specific Activity ScaleGoldman Circulation 64:1227, 1981
Stage I
• patients can perform to completion any activity requiring 7 metabolic equivalents – can carry 24 lb up eight steps
– carry objects that weigh 80 lb
– do outdoor work [shovel snow, spade soil]
– do recreational activities [skiing, basketball, squash, handball, jog/walk 5 mph]

Specific Activity ScaleGoldman Circulation 64:1227, 1981
Stage II
• patients can perform to completion any activity requiring 5 metabolic equivalents – have sexual intercourse without stopping
– garden, rake, weed, roller skate
– dance fox trot, walk at 4 mph on level ground
– but cannot and do not perform to completion activities requiring 7 metabolic equivalents

Specific Activity ScaleGoldman Circulation 64:1227, 1981
Stage III
• patients can perform to completion any activity requiring 2 metabolic equivalents – dress, shower without stopping, strip and make
bed, clean windows
– walk 2.5 mph, bowl, play golf, dress without stopping
– but cannot and do not perform to completion any activities requiring 5 metabolic equivalents

Specific Activity ScaleGoldman Circulation 64:1227, 1981
Stage IV
• patients cannot or do not perform to completion activities requiring 2 metabolic equivalents– CAN’T:
• dress without stopping
• shower without stopping
• strip and make bed
• walk 2.5 mph
• bowl, play golf

Prognosis of HF = generally poor
JACC 1993;22:6A-13A

Progression of Cardiac Status
• most patients do not show an uninterrupted and inexorable deterioration
• deterioration may be independent of LV function

Drug Therapy Improves Outcome

Diagnosis of Heart Failure
• Heart Failure is mainly a clinical diagnosis
• HF is correctly diagnosed initially in 50% of
affected patients. Eur Heart J 1991
• High Index of Suspicion
– is your patient at risk???
• “““Rapid Onset Heart Failure””” …
– did we under appreciate the findings?

Symptoms of Heart Failure
• pulmonary– resting or exertional dyspnea– orthopnea– paroxysmal nocturnal dyspnea– cough– wheezes ‘Cardiogenic Asthma’

Symptoms of Heart Failure
• other volume issues– nocturia– lower limb edema– gastrointestinal symptoms
• abdominal bloating• anorexia• fullness in the right upper quadrant
• fatigue• cachexia

Signs of Heart Failure
• delirium
• vital signs - normal or abnormal
• fluid weight gain
• peripheral edema– detected when extracellular volume > 5 l– stasis dermatitis– chronic venous stasis– hyperpigmentation– ulceration


Signs of Heart Failure
Distinguishing JVP/CPvariation with respiration
variation with position
varies with hepatic pres
occludes
non-palpable
wave form
elevation of JVP > 4.5 cmspec = 90% sens = 30%
Palpate Contralateral Carotid Artery
- if what you FEEL is not= to what you SEE --> JVP

Signs of Heart Failure
– S3 (Ken-tuc-ky)• sensitivity for HF = 24%• specificity for HF = 99%
– S4 (Ten-nes-see)• reduced ventricular compliance
– pulmonary examination• crackles (may be absent even with edema)• signs of pleural effusion• wheezes

B-type Natriuretic Peptide (BNP)

Post-op HF LabsCBC exclude anemia, adequate platelets
Electrolytes diuretic effect on potassium
low sodium is c/w heart failure
Creatinine diuretic response
safety of ACE / ARB
Mg arrhythmia risk
Albumin edema issues
Troponin T recent myocardial infarction?
INR and PTT in case of heparin or thrombolytics
Type & Screen in case transfusion needed
Post-OP HF: labs
• Chest Radiography– ‘the best chest examination’
• Electrocardiography– confirm rhythm– LVH?– ischemia?
• Echocardiography– variably helpful
• Thallium– variably helpful

Diagnostic Imaging

‘Congestive’ heart failure
Pulmonary Edema indistinct arteries
interstitial markings
increased
redistributed
peribronchial cuff pleural effusions
Ventricle enlargedincreased CT ratio
enlarged silhouette

Interstitial Pulmonary Edema

What’swronghere?
Small Cardiac
Silhouette
this effusionis from
tuberculosis

Common causes of Heart Failure
• Heart Failure = High Operative Risk– patients should not go to OR if heart failure is
not controlledRisk Calculator
http://www.vasgbi.com/riskscores.htm
• Poor left ventricular function– coronary artery disease– hypertension
• Valvular heart disease• Fluid Retention

Other causes of Heart FailureInfections (viruses (including HIV) bacteria, parasites)
Pericardial diseases
Drugs (alcohol, doxorubicin, cyclophosphamide, cocaine)
Connective tissue disease
Infiltrative disease (e.g., amyloidosis, sarcoidosis, hemochromatosis, malignancy)
Persisting tachycardia
Obstructive cardiomyopathy
Neuromuscular disease (e.g., muscular or myotonic dystrophy, Friedreich's ataxia)
Metabolic disorders (e.g., glycogen storage disease type 2 [Pompe's disease] and type 5 [McArdle's disease])
Nutritional disorders (e.g., beriberi, kwashiorkor)
Pheochromocytoma
Radiation
Endomyocardial fibrosis
Eosinophilic endomyocardial disease
High-output heart failure (e.g., intracardiac shunt, atrioventricular fistula, beriberi, pregnancy, Paget's disease, hyperthyroidism, anemia)
Peripartum cardiomyopathy
Dilated idiopathic cardiomyopathy
Approach to causes of Heart Failure
• Cardiac causes– pericardium– myocardium– endocardium– neuro-electrical system
• Non-cardiac causes– pre-load & after-load– other organ dysfunction
• anemia, respiratory disease, sepsis…
– iatrogenesis & adherence

Cardiac Causes of HF
• 1 Pericardium– tamponade, constrictive pericardial disease

Cardiac Causes of HF
• 2 Myocardium– ischemia
• coronary, non-coronary ischemia (hypoxia / anemia)
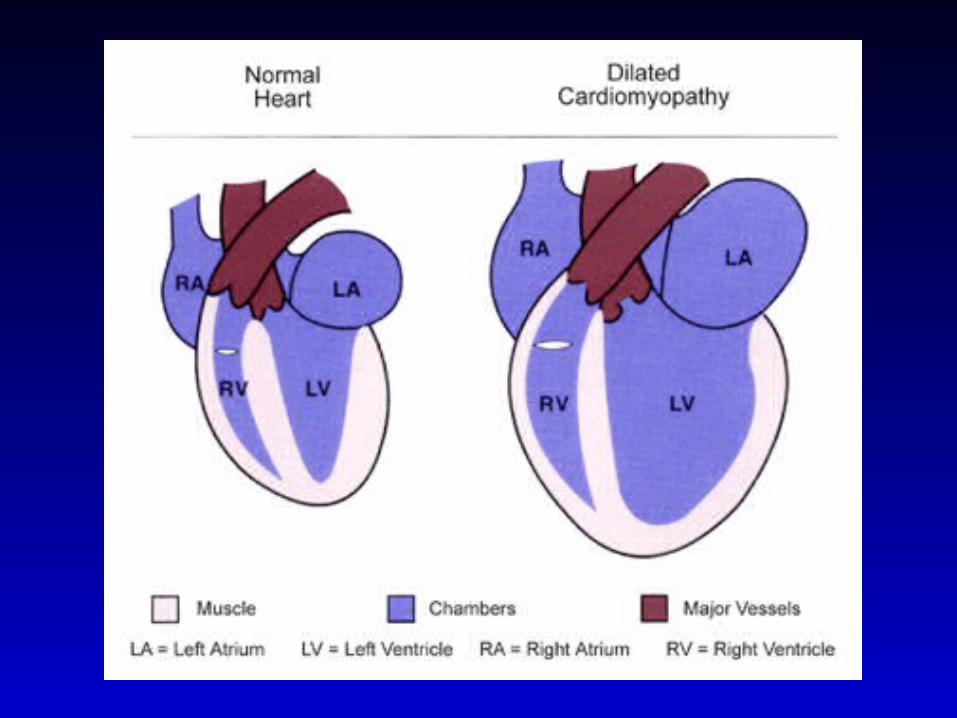
– cardiomyopathy• dilated: idiopathic, alcoholic, end stage CAD-HTN,
peripartum, post-viral• hypertrophic obstructive cardiomyopathy• restrictive: hemochromatosis, amyloidosis, sarcoidosis
– endocrinopathy• thyroid, adrenal disease (cortico / pheo)



Cardiac Causes of HF
• 3 Endocardium– valvular heart disease (including infective)– tumors (myxomas, sarcomas, melanomas)

Cardiac Causes of HF
• 4 Conducting System– tachycardia
• mostly atrial fibrillation• hyperthyroidism• sepsis (use acetaminophen in vulnerable febriles)
– bradycardia• excess medication effect• third degree heart block

Atrial Fibrillation - with rapid rate


Bradycardia - 28 / min

Non-cardiac Causes of HF• Pre-load issues
– too much (or too little) fluid to the heart
• Afterload issues– too much (or too little) resistance to arterial flow
• Examples of causes– saline, renal dysfunction versus blood loss
– medication effect or lack of adherence
– other organ dysfunctions• respiratory, sepsis, anemia, thyroid, liver, neuro...
PreloadSalt + Water (Saline)
=Pulmonary and Tissue Edema

Fluid Shifts Post-Op

Salt, NSAIDS, Coxibs, TZDs, Nephrotoxins --> Fluid Retention
IVcontrast(not po)

Afterload --> Hypertension

Medication
• Bioavailability
• Adherence– we didn’t give– patient didn’t take

• Clin Phar Ther 1995
20 mg IVtwice as useful as
40 mg poin Heart Failure

Management of Heart Failure
Post-operative Period
versus
Chronic Ambulatory

Management of Chronic HF
Ahigh risk
normal heartno HF
Babnormal
heartno HF
Cabnormal
heartprior or
current HF
D
refractory
HF
Asmoking
hypertensionlipid / DMlifestyle
B‘A’+
ACE / ARBBB
valve dxrevascularize
C‘B’ +
diureticsdigoxin
salt restrict
D‘C’ +
transplantmech assistIV inotrope
hospice

Management of Post-op Heart Failure
• Diagnose It !!!
• Determine the cause(s) !!!
• Remove things that make it worse– cardiac related– non-cardiac related
• Initiate things that make it better– cardiac related– non-cardiac related

Cardiac Medications are just Tools

Cardiac EffectsDRUG HR PRE AFTER
diuretics ace-inhibitors arbs beta-blockers ccb
- diltiazem - nefidipine
- amlodipine digoxin nitrates morphine

Case #1POD 2 - total knee replacement
• 75 yr old• past medical history
– heart failure 2 yr ago– MI 3 yr & 7 yr ago– hypertension
• Meds– Pre-op: ASA, ramipril, atorvastatin
• Normal Saline 125 ml/hr since OR– Saline Boluses post-op
• Now: SOB, edema, crackles

• Diagnostics– hx: sob, no chest pain– pe: ++ edema, + crackles, + wheezes– lab: Hgb 100 g/l, CXR: ++ heart size, edema
• What’s the Diagnosis?– HF owing to poor LV fx + saline loading
• What’s the Intervention?– oxygen– stop saline– diuretics– reduce afterload: especially ACE-I / ARB

Case #2POD 3 - ORIF hip
• 87 yr old
• past medical history– moderate hypertension
• Meds– amlodipine, benazepril, HCTZ
– Normal Saline 100 ml/hr since OR
– 2 units blood yesterday
• Now: BP 85/43, HR 150/min, SOB

• Diagnostics– hx: feels weak– pe: tachycardia, JVP elevated– lab: Hgb 105 g/l, K= 3.2, CXR: enlarged heart– ECG: Atrial Fibrillation + LVH
• What’s the Diagnosis?– HF: Atrial Fib + LVH + Volume Expansion
• What’s the Intervention?– oxygen– stop saline– diuretics & +++ potassium– rate control

Case #3POD 4 - pathological hip #, ORIF
• 79 yr old
• past medical history– advanced prostate cancer (no heroics)– hypertension– diabetes
• Meds– Pre-op: ASA, Adalat XL, metformin
• Now: Chest Pain, SOB, edema, crackles,

• Diagnostics– hx: chest pain relieved with S/L NTG– pe: HR 110, 190/100, JVP normal– lab: Hgb 70 g/l, CXR: mild edema– ECG: LVH with ST-T wave changes
• What’s the Diagnosis?– HF: anemia, myocardial ischemia, HTN-> LVH
• What’s the Intervention?– oxygen– transfuse RBCs (pre-diuretic!)– beta-blocker +/- CCB– ASA + (already on heparin)

Summary
• Heart Failure– high index of suspicion– preventative strategies
• Work-up– what are the contributers?
• Therapy– cause oriented

Acknowledgements
• You– thank you for your kind attention