healthcare associated infections across the health...
TRANSCRIPT

Healthcare associated Healthcare associated infections across the health and infections across the health and
social care communitysocial care communityProfessor Brian Professor Brian DuerdenDuerden CBECBE
Inspector of Microbiology and Infection Inspector of Microbiology and Infection Control,Control,
Department of Health, London Department of Health, London

Infection is differentInfection is different…………..
………….it spreads!.it spreads!

HCAIHCAI
Knows no boundaries across health and Knows no boundaries across health and social caresocial careBacteria move with peopleBacteria move with people
Affects all health and social care settingsAffects all health and social care settings–– Responsibility across the whole health and Responsibility across the whole health and
social care communitysocial care community

Health and social care communityHealth and social care community
NHSNHS–– SHAs SHAs –– performance managementperformance management–– PCTs PCTs –– commissioners and providerscommissioners and providers
General practiceGeneral practiceCommunity hospitalsCommunity hospitals
–– Acute Trusts/Acute Trusts/FTsFTs–– Mental Health Trusts Mental Health Trusts –– Ambulance TrustsAmbulance Trusts
Independent sectorIndependent sector–– Hospitals; independent treatment centresHospitals; independent treatment centres–– Nursing & care homesNursing & care homes
Health Protection AgencyHealth Protection Agency

The HCAI challengeThe HCAI challenge……....
MRSA bacteraemiaMRSA bacteraemia–– 2001/2 72912001/2 7291–– 2002/3 74262002/3 7426–– 2003/4 77002003/4 7700–– 2004/5 72122004/5 7212–– 2005/6 70972005/6 7097–– 2006/7 6383 2006/7 6383 –– 2007/8 44382007/8 4438
C. difficile C. difficile infectioninfection>65 years>65 years
–– 2004 443142004 44314–– 2005 517672005 51767–– 2006 556812006 55681–– 2007 503922007 50392
……...why?...why?

1970 1970 –– 2000: a dichotomy2000: a dichotomyMicrobiology & Microbiology & Infection ControlInfection Control–– New antibioticsNew antibiotics–– New societiesNew societies–– New journalsNew journals–– New guidelinesNew guidelines–– New diseasesNew diseases
Infection control was Infection control was the province of the the province of the infection specialistsinfection specialists
Modern medicineModern medicine–– Increased life Increased life
expectancyexpectancy–– Cancer treatmentCancer treatment
ImmunosuppressionImmunosuppression–– Complex surgeryComplex surgery
Transplants Transplants –– Chronic illnessesChronic illnesses
Renal dialysisRenal dialysis–– LongLong--term careterm care
Infection Infection –– a nuisancea nuisance

Reducing HCAIReducing HCAI……..
Change the mindsetChange the mindsetFrom: From: 1) create a system to deliver specialist clinical 1) create a system to deliver specialist clinical
carecare2) take measures to prevent infection 2) take measures to prevent infection To:To:1) create a safe environment for patient care1) create a safe environment for patient care2) deliver specialist clinical care within that 2) deliver specialist clinical care within that
environmentenvironment

Responsibility for HCAIResponsibility for HCAIClinicians & carersClinicians & carers–– Safe patient careSafe patient care–– DiagnosisDiagnosis–– TreatmentTreatment–– PreventionPrevention–– ControlControl
Boards/Boards/CExCEx/managers/managers–– Corporate Corporate
environmentenvironment–– Make it happenMake it happen
Government/DHGovernment/DH–– Set standardsSet standards–– Ensure priorityEnsure priority–– Set targetsSet targets–– Monitor outcomeMonitor outcome–– Performance Performance
managementmanagement
………………..and..and

…….... legislationlegislation
Health Act 2006Health Act 2006–– Statutory Code of Practice : all NHS bodiesStatutory Code of Practice : all NHS bodies–– Compliance assessed by the Healthcare Compliance assessed by the Healthcare
CommissionCommissionAnnual Annual healthcheckhealthcheckImprovement noticesImprovement noticesAnnual specialist inspections from 2008Annual specialist inspections from 2008--99

Health and Social Care Act 2008Health and Social Care Act 2008
Care Quality CommissionCare Quality CommissionExtends COP to independent sector and all care Extends COP to independent sector and all care settingssettingsRegistrationRegistration–– NHS bodies: 2009/10NHS bodies: 2009/10–– Independent sector 2010/11 (continuation of current Independent sector 2010/11 (continuation of current
registration registration –– Care Standards Act)Care Standards Act)Compliance with revised Code of PracticeCompliance with revised Code of Practice–– Effective April 2009Effective April 2009–– Demonstrate compliance with registrationDemonstrate compliance with registration–– Restructured; same content and purposeRestructured; same content and purpose

HCAI focusHCAI focus
2004 and before2004 and before–– Hospital acquired infectionHospital acquired infection20052005--0707–– Other healthcare settingsOther healthcare settings–– Healthcare associated InfectionsHealthcare associated Infections20082008–– The wider health and social care communityThe wider health and social care community

MRSA Target 2005MRSA Target 2005--0808
‘‘Halve MRSA infections by 2008Halve MRSA infections by 2008’’–– MRSA bacteraemiaMRSA bacteraemia–– Baseline 2003Baseline 2003--04; Start date April 200504; Start date April 2005Depends upon mandatory surveillance Depends upon mandatory surveillance being accurate and timely being accurate and timely –– CExCEx signsign--offoff
Target measured AprilTarget measured April--June 2008June 2008
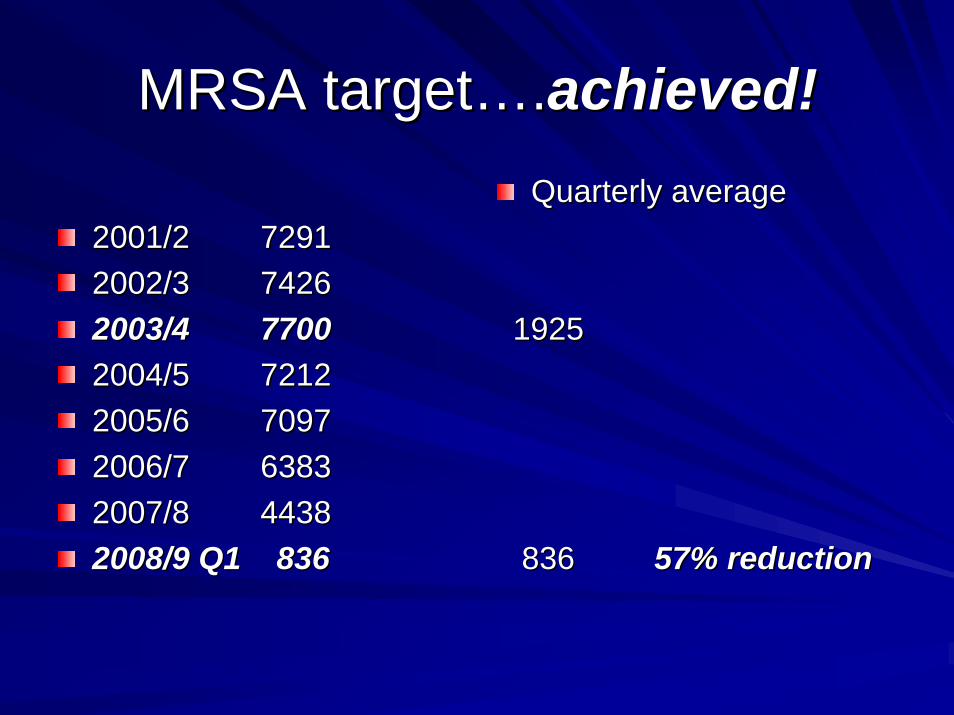
MRSA targetMRSA target……..achieved!achieved!
2001/2 72912001/2 72912002/3 74262002/3 74262003/4 77002003/4 77002004/5 72122004/5 72122005/6 70972005/6 70972006/7 6383 2006/7 6383 2007/8 44382007/8 44382008/9 Q1 8362008/9 Q1 836
Quarterly averageQuarterly average
19251925
836 836 57% reduction57% reduction

How have we changed practice?How have we changed practice?
ManagementManagement–– emphasis on infection control emphasis on infection control
Enhanced surveillance (HPA)Enhanced surveillance (HPA)–– MRSA & MRSA & C. difficileC. difficile
Clinical practice protocolsClinical practice protocols–– Saving Lives & Essential StepsSaving Lives & Essential Steps
Cleanliness and hygieneCleanliness and hygiene–– hand hygienehand hygiene–– environmental cleaningenvironmental cleaning
TrainingTrainingTargets and performance managementTargets and performance managementLegislation Legislation –– Code of PracticeCode of Practice
‘‘Saving livesSaving lives’’ & & ‘‘Essential stepsEssential steps’’
Two componentsTwo components–– Self assessment tools for all types of Self assessment tools for all types of
organisation organisation –– reflect reflect CoPCoP core dutiescore duties–– High Impact Interventions (Care Bundle High Impact Interventions (Care Bundle
approach) approach) 7 in 7 in ‘‘Saving livesSaving lives’’; ; 3 in 3 in ‘‘Essential stepsEssential steps’’
-- plus guidance notesplus guidance notes

High Impact InterventionsHigh Impact InterventionsSaving livesSaving lives–– Central venous Central venous
catheterscatheters–– Peripheral line carePeripheral line care–– Dialysis cathetersDialysis catheters–– Surgical site Surgical site
managementmanagement–– Urinary cathetersUrinary catheters–– Ventilator Ventilator
managementmanagement–– Clostridium difficileClostridium difficile
Essential stepsEssential steps–– PreventingPreventing the spread the spread
of infectionof infectionHand hygieneHand hygienePPEPPEAseptic technique Aseptic technique Safe disposal of sharpsSafe disposal of sharps
–– Urinary catheter careUrinary catheter care–– EnteralEnteral feedingfeeding

‘‘Saving livesSaving lives’’ guidanceguidance
October 2006 October 2006 –– MRSA screening MRSA screening June 2007June 2007–– Blood Culture protocolBlood Culture protocol–– Antimicrobial prescribing frameworkAntimicrobial prescribing frameworkSeptember 2007September 2007–– Isolation and Isolation and cohortingcohorting

MRSA target MRSA target –– beyond 2008beyond 2008Headline message: continue to improveHeadline message: continue to improve–– The target is a ceilingThe target is a ceiling–– Get as much below as possibleGet as much below as possible–– Year on year reductionsYear on year reductions
Mandatory surveillance system will continueMandatory surveillance system will continue
SHA envelopes for the targetSHA envelopes for the target–– SHAs performance manage Trusts within envelopeSHAs performance manage Trusts within envelope–– Achieved or better Achieved or better –– at least maintain; aim to reduce furtherat least maintain; aim to reduce further–– Not reached Not reached –– continue with performance management and continue with performance management and
monitoring to achieve the target monitoring to achieve the target –– and beyondand beyond

MRSA bacteraemia in the communityMRSA bacteraemia in the community
PrePre--48 hour cases: 30% of all cases48 hour cases: 30% of all casesRCA RCA –– must include primary caremust include primary care–– Chronic conditionsChronic conditions
Indwelling devicesIndwelling devices
–– Underlying pathology increasing susceptibilityUnderlying pathology increasing susceptibility–– Repeat Repeat attendersattenders–– Contact with healthcare settingsContact with healthcare settings–– Community hospitalsCommunity hospitals–– Residential careResidential care……..and so must the actions!..and so must the actions!
MRSA screeningMRSA screening
All elective admissions by March 2009All elective admissions by March 2009Not maternity, ophthalmic, dental, endoscopiesNot maternity, ophthalmic, dental, endoscopies
–– DH monitors implementation from OctoberDH monitors implementation from October
All admissions All admissions asapasap and at latest by and at latest by 20102010--1111

Why are we screening?Why are we screening?
Colonisation precedes infection Colonisation precedes infection –– mostlymostlyColonised patient isColonised patient is–– At risk of developing an infectionAt risk of developing an infection–– A possible source for transmission to othersA possible source for transmission to othersIsolate MRSA +Isolate MRSA +veve patients if possiblepatients if possibleScreening AND decolonisationScreening AND decolonisation–– Reduces the risk for the individualReduces the risk for the individual–– Reduces the risk of transmissionReduces the risk of transmission

DecolonisationDecolonisation
Body wash, shampoo, nasal creamBody wash, shampoo, nasal cream–– 5 days5 daysSuccess rate Success rate –– Depends on timeDepends on time–– egeg 1 week, 90%; 3 months 601 week, 90%; 3 months 60--70%70%BUT immediately reduces the BUT immediately reduces the bioburdenbioburden of of MRSAMRSA–– Covers the period of highest risk and of Covers the period of highest risk and of
interventionsinterventions

Screening and patient flowScreening and patient flow
Where to screen and when?Where to screen and when?–– PrePre--admission clinicadmission clinic–– On admission (emergency admissions)On admission (emergency admissions)–– In primary careIn primary care–– Nursing/care home patients?Nursing/care home patients?Who does it?Who does it?Who administers the decolonisation Who administers the decolonisation regimen regimen –– hospital and/or primary carehospital and/or primary care
………………..needs to be a partnership..needs to be a partnership

C. difficile C. difficile target target –– present statuspresent status
C. difficile C. difficile infectioninfection>65 years>65 years
–– 2004 443142004 44314–– 2005 517672005 51767–– 2006 556812006 55681–– 20072007 5039250392
2007/8 453342007/8 45334+ 2+ 2--64 years 10059 64 years 10059

C. difficile C. difficile voluntary reporting 1991 voluntary reporting 1991 –– 2005: 2005: England, Wales and Northern IrelandEngland, Wales and Northern Ireland
0
5000
10000
15000
20000
25000
30000
35000
40000
45000
50000
1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005
year
num
ber o
f rep
orts

1991 1991 -- 19941994
1991 1991 -- 92 : large outbreak in Manchester92 : large outbreak in Manchester–– 170+ cases; 17 deaths (at least)170+ cases; 17 deaths (at least)–– Elderly patients; winterElderly patients; winter–– High antibiotic useHigh antibiotic useReference Lab Reference Lab PyMSPyMS typing confirmed typing confirmed crosscross--infectioninfectionParliamentary questions!Parliamentary questions!Smaller outbreaks widespreadSmaller outbreaks widespread

C. difficileC. difficile ““new new superbugsuperbug”” hits the national hits the national press Mon. June 6press Mon. June 6thth 2005. Jeremy 2005. Jeremy LauranceLaurance ––
Health Editor, The IndependentHealth Editor, The Independent

C. difficile C. difficile deaths 1999deaths 1999--2006200619991999 20012001 20022002 20032003 20042004 20052005 20062006 20072007
6,4806,480 8,3248,324
4,0564,056
4949
3,5643,564
5555
DC DC recordrecord
975975 1,2141,214 1,4281,428 1,7881,788 2,2472,247 3,8073,807
UCUC 531531 691691 756756 958958 1,2451,245 2,0742,074
% as % as UCUC
5454 5757 5353 5555 5555 5454
Office of National Statistics

How does CDI happen?How does CDI happen?
Broad spectrum antibioticsBroad spectrum antibioticsTransmissible sporesTransmissible spores–– Survive in environmentSurvive in environmentC. difficile C. difficile overgrowth and attachmentovergrowth and attachmentToxin productionToxin production–– Toxin A (Toxin A (enterotoxinenterotoxin))–– Toxin B (Toxin B (cytotoxincytotoxin))–– Binary toxin (? effect)Binary toxin (? effect)

Clinical presentation and pathologyClinical presentation and pathology
AntibioticAntibiotic--associated diarrhoeaassociated diarrhoea–– Mild, distressing, severeMild, distressing, severeDehydration, blood lossDehydration, blood lossPseudomembranousPseudomembranous colitiscolitis–– EndoscopyEndoscopy, histopathology, histopathologyPerforationPerforationToxic Toxic megacolonmegacolon

C. difficileC. difficile epidemiologyepidemiology
Acute hospitals (secondary care)Acute hospitals (secondary care)–– 7070--80% of cases80% of cases–– Significant preSignificant pre--48 hours component48 hours componentCommunity hospitalsCommunity hospitalsNursing/care homesNursing/care homesGeneral population General population –– Small but may be significantSmall but may be significant

CDI Target CDI Target –– 20082008--20112011National CDI target reductionNational CDI target reduction–– 30% reduction by 201030% reduction by 2010--11, baseline 200711, baseline 2007--88–– Performance management on SHA envelopesPerformance management on SHA envelopes
Population based (SHA and PCT)Population based (SHA and PCT)Differential reductions to reach standard rateDifferential reductions to reach standard rate
(/10,000 population)(/10,000 population)
–– Acute Trust targetsAcute Trust targetspostpost--48 hours after admission48 hours after admission
Standard per 1000 admissionsStandard per 1000 admissions
–– Minimum reduction set for all Minimum reduction set for all

CMO/CNO/CMO/CNO/CPhOCPhO guidance: Dec 2006guidance: Dec 2006
Antibiotic prescribingAntibiotic prescribing–– Limit broad spectrum agentsLimit broad spectrum agents–– Limit IV Limit IV andand oral coursesoral courses
Prompt diagnostic tests Prompt diagnostic tests –– Toxins A+BToxins A+B–– isolates for typing if outbreak suspected isolates for typing if outbreak suspected
Isolation/segregation/Isolation/segregation/cohortingcohorting of casesof casesInfection control Infection control –– handwashinghandwashing, gloves, gowns, gloves, gownsDecontamination/cleaning Decontamination/cleaning –– increaseincrease–– ChlorineChlorine--based disinfectantbased disinfectant


Antibiotic policy Antibiotic policy –– CDI preventionCDI prevention
Stewardship Stewardship –– only use when good only use when good indicationindicationRestrict use of broad spectrum agentsRestrict use of broad spectrum agentsReasons for prescribing recordedReasons for prescribing recordedStop dates Stop dates –– review by pharmacistsreview by pharmacistsProphylaxis Prophylaxis –– single dosesingle doseAudit, training and reviewAudit, training and reviewRole of Antimicrobial Management TeamRole of Antimicrobial Management Team

Antimicrobials Antimicrobials –– unique therapeuticsunique therapeutics
Aim to affect the bacteria Aim to affect the bacteria –– not the patientnot the patientNot specific to the disease agentsNot specific to the disease agents–– Effect on normal floraEffect on normal floraSelect for resistant organismsSelect for resistant organismsInduce vulnerability to some infectionsInduce vulnerability to some infections
Mostly prescribed by nonMostly prescribed by non--specialists (in specialists (in infection)infection)

Preventing HCAIPreventing HCAIEnsure management attentionEnsure management attention–– Commissioning and monitoringCommissioning and monitoring
Improve clinical careImprove clinical care–– Hand hygieneHand hygiene–– Aseptic proceduresAseptic procedures–– Saving Lives Saving Lives andand Essential StepsEssential Steps–– Care home guidanceCare home guidance
Antimicrobial stewardshipAntimicrobial stewardship–– Across the health economyAcross the health economy
Audit and trainingAudit and training

Commissioning and deliveryCommissioning and delivery
Commissioners to include IP&C in Commissioners to include IP&C in commissioned servicescommissioned servicesContract monitoring to include review of Contract monitoring to include review of IP&C provisionIP&C provision–– Target numbersTarget numbers–– Process monitoringProcess monitoringProvider services to include IP&CProvider services to include IP&C

What is needed?What is needed?Partnership across health and social care Partnership across health and social care communitycommunityIP&C in all provider unitsIP&C in all provider unitsCommon antimicrobial prescribing policyCommon antimicrobial prescribing policyCommissioning expertiseCommissioning expertise–– Requirements in contracts for IP&CRequirements in contracts for IP&C
Support in the communitySupport in the community–– AdviceAdvice–– Training Training –– Implementation Implementation