health professionals learning qualitative research in
TRANSCRIPT

RESEARCH ARTICLE Open Access
Health professionals learning qualitativeresearch in their workplace: a focusedethnographyLuca Ghirotto* , Ludovica De Panfilis and Silvia Di Leo
Abstract
Background: The interest for qualitative research methodology has expanded beyond theoretical academicresearch on medical education, gathering interest from all healthcare professionals. Qualitative research haspotentials in exploring the social, emotional, psychological aspects of care and in broadening professionals’scientific competencies. Nonetheless, qualitative research has still not been embraced within formal and academiccurricula for future professionals, preventing newer generations from appreciating the value of its epistemologicaland methodological aspects and from using it in the development and implementation of clinical research. Thepurpose of this study was to comprehend the attitudes of health professionals learning and conducting qualitativestudies within a practical training program developed in their workplace.
Methods: The present work consisted of a focused ethnography, including 14 professionals during their one-yearattendance training on qualitative research methodology. Strategies used for collecting data included participantobservations, field notes, semi-structured interviews, and a focus group. All the data were analyzed consistently withethnographic indications.
Results: Analyses allowed us to evidence the educational, motivational, group-related and organizational factorsinfluencing the attitudes and skill acquisition of healthcare professionals learning and conducting qualitativeresearch within a practical training program developed in their workplace. Prior educational background wasperceived as a sort of barrier. Nonetheless, the training boosted a change in attitude both in terms of appreciationof the research approach and trainees’ emotional involvement with research participants. Doing a qualitative studyin a multidisciplinary team raised in-group dynamics that hindered bringing the studies to conclusion. Traineesrepeatedly lamented the difficulty in managing time to devote to research-related activities and questioned thefeasibility of adopting this methodology for conducting research in their workplace.
Conclusions: Continual education training on the methodological aspects and practical implications of qualitativeresearch may foster a renewed attitude towards one’s professional education, while making inter-professionalrelationship issues emerge. Nonetheless, broadening the perspectives of professionals on their clinical practice by meansof learning qualitative methodology may have an evident quality improvement return. Strategies for future qualitativeresearch methodology hands-on training addressed to health professionals in continuing education are proposed.
Keywords: Continuing learning, Continuing medical education, Healthcare professionals, Professional development,Qualitative Research methods, Research skills, Clinical Cancer center, Cancer Research
© The Author(s). 2020 Open Access This article is licensed under a Creative Commons Attribution 4.0 International License,which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you giveappropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate ifchanges were made. The images or other third party material in this article are included in the article's Creative Commonslicence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commonslicence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtainpermission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to thedata made available in this article, unless otherwise stated in a credit line to the data.
* Correspondence: [email protected] USL - IRCCS di Reggio Emilia, Viale Umberto I°, 50, 42123 ReggioEmilia, Italy
Ghirotto et al. BMC Medical Education (2020) 20:269 https://doi.org/10.1186/s12909-020-02191-5

BackgroundIn recent years the interest for qualitative research meth-odology and methods (QRM) has gradually expandedbeyond the mere theoretical academic research onmedical education, gathering interest from all healthcareprofessionals (HPs) [1–3] thanks to its potential inexploring the social, emotional, psychological aspects ofcare [4] and in broadening professionals’ scientificcompetencies. Nonetheless, QRM has still not beenembraced within formal and academic curricula forfuture HPs [4–7], preventing newer generations fromappreciating the value of its epistemological andmethodological aspects and from using it in the develop-ment and implementation of clinical research. Charmazhighlights the limited coverage of qualitative research ingeneral methods courses, non-existent or insufficientundergraduate courses and a scarcity of in-depth quali-tative methods courses in graduate programs [8].Accordingly, evidence on HPs’ training in QRM is also
sparing and limited to the academic environment [9–11], with few works addressing QRM in Continual Med-ical Education (CME) and its application in HPs’ work-place [12–15]. A study performed by Calderón describesan online teaching program for primary HPs, highlight-ing specific aspects that should be considered in the de-sign and development of QRM training within healthservices [12]. Featherstone and colleagues [13] as well asHepworth and colleagues [14], reporting on their experi-ence with primary care and general practitioners re-spectively, provide information on which areas of QRMHPs consider most feasible (i.e., coding) or more chal-lenging (i.e., QRM philosophy and theoretical underpin-nings) [12, 14]. Authors highlight the career paths, timeconstraints, and professional background that influencethe way HPs approach QRM training [12]. These studiesaddressed concise QRM training programs and did notexplore the experience nor the benefits perceived byHPs in employing QRM within their research activities.As far as we know, no studies exist on the realexperience of HPs performing qualitative research.Herein we report the findings from an ethnographic
research on a one-year QRM training to enable HPsto perform qualitative research within their workenvironment.
MethodsMethodological approachWe employed an ethnographic approach previouslyused by Ng et al. for studying HPs education and prac-tice [16] and recently discussed as a suitable approachin medical education research [17]. In particular, wefollowed a specific method defined in scientific litera-ture as rapid ethnographic research [18] or focusedethnography [19]. Ethnography represents a validated
methodological approach to study personal experiencesand behaviors through the direct observation ofsituations as they enfold in their natural setting [19].Since ethnographic research is exploratory in nature, ingeneral, research questions are not necessarily specified[20]. Equally, focused ethnography (FE) entails enteringthe field with a defined research question [17, 18],undertaking fieldwork in a short timeline [19]. Further-more, compared to traditional ethnographies, FE drawsmore heavily on interviewing than on participant obser-vation [17]. This method was consistent with medicaleducation ground, which consists of limited and well-defined social episodes or scripted interactions [17].For our study’s purposes, we formulated the followinggenerative research question: what are the attitudes ofHPs towards learning and conducting QRM within apractical training program developed in theirworkplace?
The organizational settingThe present work was carried out in a Clinical CancerCentre (Azienda USL – IRCCS, the public healthauthority of the Reggio Emilia province) in northernItaly, in the setting of a qualitative research trainingcourse, entitled “Carrying out qualitative research: anopportunity for health professionals”. The course wasadvocated by the Scientific Director to accomplish oneof the mission goals of the Centre, i.e. developing andimplementing training programs aimed at improvingHPs’ research competencies. Motivations supporting thedevelopment of such a training within a Clinical CancerCentre concern the importance QRM for understandingcancer care in its complexity. As noted elsewhere [21],cancer researchers have been increasing their focus onpatient preferences and experiences with care. An un-derstanding of how these areas affect oncology practicerequired HPs working within the Centre to learn re-search methods suitable to develop a morecomprehensive knowledge of the cancer-relatedphenomena, including methods to describe and explainunderlying motivations and potential causes of specificoutcomes [21]. Even if the training was endorsed by theScientific Directorate of the Clinical Cancer Centre andwas addressed primarily to the Clinical Cancer Centreprofessionals, it was opened to all the employees of themain General Hospital and other services of the publiclocal health authority, Azienda USL – IRCCS of ReggioEmilia (including colleagues working at the Departmentof Health Sciences of the University nearby).
The trainingThe QRM training program was designed and con-ducted by a qualitative research methodologist (LG) anda psycho-oncologist expert in QRM (SDL). Its structure
Ghirotto et al. BMC Medical Education (2020) 20:269 Page 2 of 15

and duration have been planned in line with two strictlyinterconnected objectives, i.e. providing HPs with no-tions and skills in QRM and getting them able to carryout qualitative research in all its steps, from the develop-ment of the research protocol to its concrete implemen-tation until the publication of the study results.Instructors chose to teach QRM through the lens of a
particular research tradition: Grounded Theory (GT).Some authors [22] recommend GT for hands-on skill-building lessons to impart the fundamentals of qualitativeinquiry and methods of inductive theory construction.Moreover, as remarked by Charmaz [8], GT strategies en-able trainees to learn to do qualitative analysis, to raise theanalytic level of their qualitative research projects, and toincrease their methodological skills. Moreover, teacherschose GT given their expertise in this methodology and,consequently, facilitating trainees’ involvement in con-ducting real qualitative research.Participation to the training was voluntary, and all
interested candidates from any professional backgrounde-mailed the teachers a brief resume, adding, asrequested, some information on their motivation intaking part in the program. Selection criteria werehaving basic comprehension in research methodologyand intermediate-level English knowledge. Participants -15 HPs working at the Clinical Cancer Centre, the LocalHealth Authority, or the Department of Health Sciencesof the University nearby - were identified by the teacherstogether with the Scientific Director. Their initial moti-vations to take part in the training included curiosity to-ward the topic of QRM, willing to complete theirprevious research-related training and to be involved inthe Scientific Directorate research programs.The training started in October 2015 and had a
planned duration of 12 months, so that trainees couldaccommodate both training’s requirements and their jobresponsibilities. According to the training’s objectives,teaching was carried out through multiple didactic tech-niques (i.e., lecture, classwork, working groups, individ-ual work, simulations, and practice), and an e-learningplatform was also available. Trainees were committedfor 120 training hours (30 h for attending lectures andindividual study, 70 h for simulations, teamwork and re-search practice within small groups; 20 h of individualresearch-related work). All the time spent within theprogram has been recognized as part of the workinghours. Every participant would have earned 50 CMEcredits after training’s completion.Table 1 summarizes the course’s syllabus excerpt out-
lining contents, performed activities, related teachingmethods, and expected outputs. HPs could consultteachers at any time, beyond formalized sessions.Once trainees individually developed their research
question (phase 1), teachers selected the three most
relevant, innovative, and feasible questions and then di-vided participants into three groups, asking them to con-duct a GT study, beginning from the three researchquestions. The trainees who initially formulated the se-lected research questions assumed the role of principalinvestigators (PIs), and the teachers chose their teammembers according to similarities in research’s interests.The three generative questions were: a) what is going onfrom patients, clinicians and other key-informants’ pointof view when HPs propose surgery to a head and neckcancer patient?, b) what happens when hospital HPs ac-company for the first time a patient to death?, c) what isthe hospital assistance of migrant cancer patients? Todate, the group dealing with the first research questionpublished the study [23], while the other two groupssubmitted the manuscripts only recently.
Sample and participantsParticipation in the training implied involvement in theFE. The participants in this study comprised 14 trainees(7 nurses, a speech therapist; a laboratory technician; theinformation specialist of the Medical Library; a dietician;a physiotherapist; an internist and a palliative care phys-ician) and a trainer. Three out of the trainees were PIsof the GT research protocols (the internist, a nurse, thespeech therapist). One trainee withdrew from the courseafter the opening lecture. We show the participants’demographics and characteristics in Table 3.
Data collectionThe data collected for this FE regarded the trainees asthey were attending the course and undertaking the GTstudy. An external researcher (LDP) participated as theobserver to 12 of the 20 training sessions foreseen intraining, in order to gain a complete representation ofthe trainees’ experience.As to strategies used for collecting data, we employed
unobtrusive participant observations consisting of simul-taneously combining interviewing of trainees, directparticipation and observation, and introspection [24].Participant observation allowed a prolonged social inter-action among the researcher and the informants duringwhich observational field notes were collected. The fieldnotes provided context and insights to support theunderstanding of what trainees thought about and howthey experienced the QRM training. Informal conversa-tions with participants were, also, documented by LDP,who in particular observed relational dynamics, verbaland non-verbal behaviors of trainees. LDP wrote notesabout what was going on during the training sessions,the spoken words of teachers and trainees, on her re-search diary, as much as possible in real time. Informalconversations were jotted down soon after their conclu-sion. Then, periodically, LDP wrote a more detailed
Ghirotto et al. BMC Medical Education (2020) 20:269 Page 3 of 15

Table 1 – “Carrying out qualitative research: an opportunity for health professionals” syllabus (excerpt)
#Phaseandmonth
Content Activity Didactic method Expected output
#1month1
Introduction to qualitativeresearch and GT, along with thevalue of the research question
Teachers explain how to define a GT researchquestion and trainees write a possible one
Lecture Drafting a research question
#2month1
Is my research question new? Every trainee performs a literature search Individual work Redefinition of the researchquestion
#2month1
The research question in GT Teachers discuss each research question, andchoose the three that are correct and mostfeasible
Class discussion,guided byteachers
Formation of three researchgroups and definition of the PI
#2month2
The groups’ research questions Each group, guided by PI, re-defines the researchquestion
Group discussionwithout teachers
Reaching an agreement
#2month2
The groups’ research questions Each group PI explains and discusses the finalversion of the research question
Class discussion,guided byteachers
Redefinition of the researchquestion
#2month2
Writing a GT research protocol forthe EC
Teachers explain how to write a GT researchprotocol and the local EC requests
Lecture Definition of the protocolcontents
#2month2
The qualitative interview Every trainee studies material about qualitativeinterviewing and keeps writing the researchprotocol
Individual work Drafting possible themes forthe interview
#2month3
The qualitative interview guide Teachers counsel each group regarding theproposed interviews
Group discussionwith teachers
Shared definition of theinterview guide
#2month3
Open coding Teachers explain what GT coding is and inviteeach group to open code an interview sample
Class work,tutored byteachers
Completion of the interviewopen coding
#2month3
Focused coding and the inter-coders’ agreement
Teachers invite each group to reach anagreement on the focused coding of theinterview sample
Group work,tutored byteachers
Reaching an understanding offocused coding
#2month3
Ethical aspect of qualitativeresearch
Teachers explain how to accomplish researchethics and provide information about thedocumentation to be presented to the EC
Lecture Writing informed consent andcollecting the documentationrequested by the EC
#2month4
Writing the research protocol Each group finalizes the writing of the protocol Individual andgroup work
Submission of the researchprotocols to the EC
#3month7
The initial sampling Each group gets access to the field and collectsthe first interviews
Individual andgroup work
Having at least 7 interviewsconducted and transcribed
#4month8
Open coding Each group codes the first interviews Individual andgroup work,tutored byteachers
Open codes
#4month9
Focused coding Each group discusses the provisional focusedcoding with teachers
Group work,tutored byteachers
Definition of focusedcategories. Each group keepsinterviewing and coding
# 5month9
Theoretical sampling andsaturation
Teachers define the method for following thetheoretical sampling with trainees and explainsaturation
Lecture andgroup work,tutored byteachers
Definition of the final samplecharacteristics
# 5month10
Final data collection and analysis Each group performs focused coding on the datacollected
Individual andgroup work,tutored byteachers
Reaching saturation
#5month11
Theoretical coding Teachers explain theoretical coding and theprocedure for working theoretically with the data
Lecture andgroup work,tutored by
Drafting the theoretical model
Ghirotto et al. BMC Medical Education (2020) 20:269 Page 4 of 15
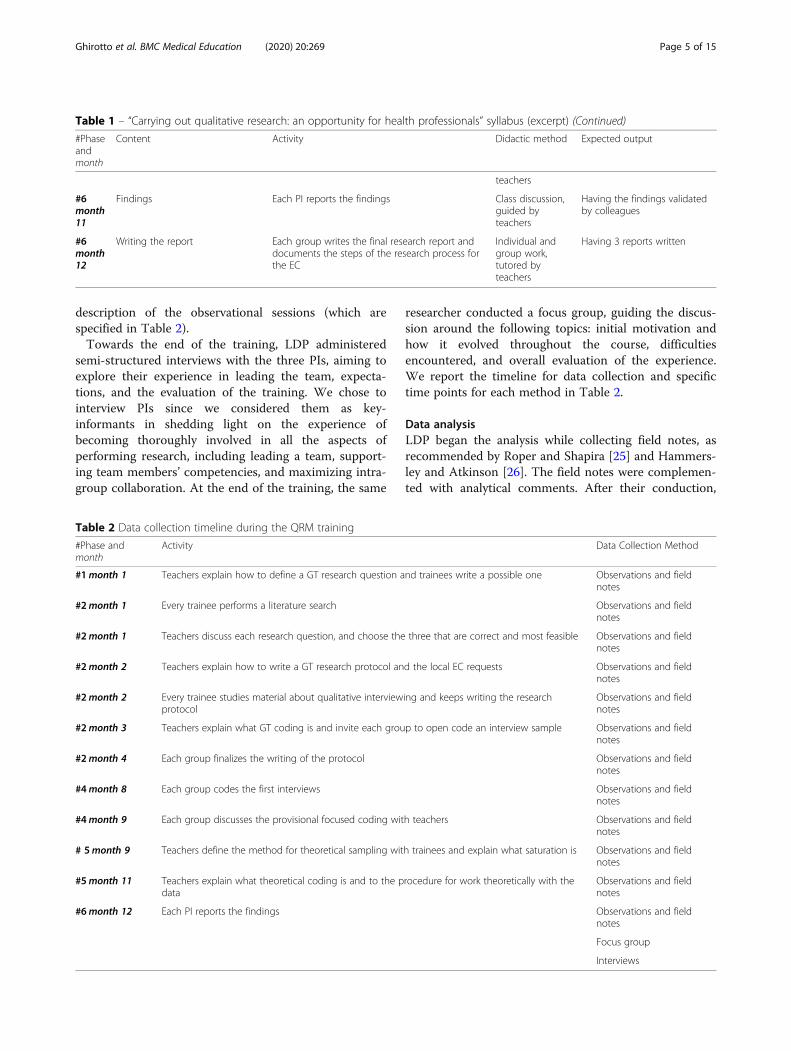
description of the observational sessions (which arespecified in Table 2).Towards the end of the training, LDP administered
semi-structured interviews with the three PIs, aiming toexplore their experience in leading the team, expecta-tions, and the evaluation of the training. We chose tointerview PIs since we considered them as key-informants in shedding light on the experience ofbecoming thoroughly involved in all the aspects ofperforming research, including leading a team, support-ing team members’ competencies, and maximizing intra-group collaboration. At the end of the training, the same
researcher conducted a focus group, guiding the discus-sion around the following topics: initial motivation andhow it evolved throughout the course, difficultiesencountered, and overall evaluation of the experience.We report the timeline for data collection and specifictime points for each method in Table 2.
Data analysisLDP began the analysis while collecting field notes, asrecommended by Roper and Shapira [25] and Hammers-ley and Atkinson [26]. The field notes were complemen-ted with analytical comments. After their conduction,
Table 1 – “Carrying out qualitative research: an opportunity for health professionals” syllabus (excerpt) (Continued)
#Phaseandmonth
Content Activity Didactic method Expected output
teachers
#6month11
Findings Each PI reports the findings Class discussion,guided byteachers
Having the findings validatedby colleagues
#6month12
Writing the report Each group writes the final research report anddocuments the steps of the research process forthe EC
Individual andgroup work,tutored byteachers
Having 3 reports written
Table 2 Data collection timeline during the QRM training
#Phase andmonth
Activity Data Collection Method
#1month 1 Teachers explain how to define a GT research question and trainees write a possible one Observations and fieldnotes
#2month 1 Every trainee performs a literature search Observations and fieldnotes
#2month 1 Teachers discuss each research question, and choose the three that are correct and most feasible Observations and fieldnotes
#2month 2 Teachers explain how to write a GT research protocol and the local EC requests Observations and fieldnotes
#2month 2 Every trainee studies material about qualitative interviewing and keeps writing the researchprotocol
Observations and fieldnotes
#2month 3 Teachers explain what GT coding is and invite each group to open code an interview sample Observations and fieldnotes
#2month 4 Each group finalizes the writing of the protocol Observations and fieldnotes
#4month 8 Each group codes the first interviews Observations and fieldnotes
#4month 9 Each group discusses the provisional focused coding with teachers Observations and fieldnotes
# 5month 9 Teachers define the method for theoretical sampling with trainees and explain what saturation is Observations and fieldnotes
#5month 11 Teachers explain what theoretical coding is and to the procedure for work theoretically with thedata
Observations and fieldnotes
#6month 12 Each PI reports the findings Observations and fieldnotes
Focus group
Interviews
Ghirotto et al. BMC Medical Education (2020) 20:269 Page 5 of 15

then, both interviews and the FG were audio-recordedand verbatim transcribed. The researcher managed thefield notes similar to the interview and FG data: thedataset was inductively analyzed employing triangula-tion, with the intent of providing a more in-depth andholistic understanding of the phenomenon [19]. Thisapproach also sustained the comparison of emergingpatterns across the different kinds of data (interviews,field notes, and FG). The analysis included a five-stepprocess [27]:
(i.) sorting of collected material (field notes, interviewsand FG transcripts were read extensively);
(ii.) descriptively coding of field notes, interviews andFG (LDP descriptively labelled the data, with codes’names close to the raw data. The researcherreviewed all data line by line and identified words,phrases, and events);
(iii.)questioning of data to find similarities anddifferences (LDP organized codes and formattedthem into tables according to data type. Then, shewrote descriptive accounts of the data from thedifferent sources. Through meetings, authorsreached an agreement about the main similaritiesand differences emerging during this step);
(iv.)grouping of codification labels into behavioralpatterns (LDP grouped codes into categories. Theemerging behavioral patterns were compared withraw data and descriptive accounts);
(v.) interpreting, through comparison of participants’meanings and categories (categories were regroupedinto the following main factors: educational,motivational, group-related and organizationalfactors) and defining final conceptualization(authors added meaningful quotations and fieldnotes excerpts to the final report).
ReflexivityThe external researcher of this study has a master’s degreein Philosophy, an MD in Palliative Medicine, and a PhD inMedical Bioethics. She had previous experience in con-ducting ethnographic studies within her PhD project. Sheengaged actively with research participants, trying to bal-ance the inside versus outside continuum in conductingobservations, collecting data, and interviewing participants.Her philosophical background influenced data analysis, asshe might have been more likely to notice and highlightrelational issues emerging from learning QRM. LG andSDL served as consultants and discussants during the datacollection and analysis. LG holds a MA in Education and aPhD in Cognitive and Education Sciences, during whichhe deepened the qualitative methodology. He serves asmethodologist and head of Qualitative ResearchUnit within the setting where this study was conducted.
SDL is psychotherapist with expertise in oncology and re-search methods. She works at the Clinical Cancer Centeras the coordinator of the Psycho-oncology Unit.
ResultsLDP carried out the ethnographic observations through-out twelve sessions, over a 12-month period. The observa-tions lasted two hours for each session on average. Allthree PIs agreed to be interviewed, and each interview hada mean duration of 25min. The final focus group meeting,which lasted 120min, was attended by 6 of the 14 trainees(two physicians, three nurses, one laboratory technician),and by one of the two instructors. Table 3 shows the char-acteristics of the trainees who participated in the study.Educational, motivational, group-related and
organizational factors were identified as influencing theattitudes and skill acquisition of HPs learning andconducting QRM within a practical training programdeveloped in their workplace.
The role of the educational backgroundPrior educational background was perceived as a sort ofbarrier. In most cases, participants voiced that theirbackground in evidence-based medicine had indirectlyprevented their interest and involvement in QRMbefore, and that they had embarked in this experiencewith few expectancies. During the first meeting, teacherscollected trainees’ initial expectations: two participants(the laboratory technician and the dietician) have neverheard of QRM, the nurses’ manager and a nurse whohad previously conducted qualitative studies, and theothers declared to have some hint. Most of the traineesstated that they had a deep curiosity and that theywanted to understand if the qualitative results of theirresearch would be applicable in the workplace. However,none of the trainees was sure that qualitative researchcould be a rigorous research method. Introductory lec-tures were informally commented to be exciting butvague. GT methodology, in particular, was stated as hav-ing a “philosophical flavor” perceived distant from whatsome of the participants were used to.
Participants gathered for the first lecture seem to payattention to the content. There is silence. Most ofthem are nodding when the teachers explain whatqualitative research is and why to carry out qualitativestudies in health field. When Grounded Theory isintroduced, two health professionals raise their handsand question “what does it mean we are supposed totheorize?” (Excerpt from field notes, month 1)
A nurse states: “I come from a purely quantitativebackground, so it will be difficult for me to switch
Ghirotto et al. BMC Medical Education (2020) 20:269 Page 6 of 15

to a different mind-set! The contents we discuss aredifficult to understand!”. (Excerpt from field notes,month 2)
During the second meeting, where each participanthad been requested to share with the whole group a gen-erative research question previously conceived, and re-ceived feedback by teachers, some trainees proposedquestions for a GT method, while others proposed vagueor not appropriate ones. The teachers did not find fittinga GT, the research questions about technical procedures(for example, “how is the neurosurgery implementedwhen a neurophysiological monitoring is available?” or“is the infusion of chemotherapy that causes serious sideeffects managed properly by nurses?”), with hypothesis-driven pre-assumptions (“how do family dynamics affectthe choice to undertake a profession in the health sec-tor?” or “why do healthcare professionals read little?”),or, finally, too vague and far-reaching (“how does theawareness in health professionals regarding the idea oftheir ‘limit’, illness and death change?”). Even during thefourth meeting, some trainees were still confused aboutone of the chosen research topics (i.e. the second gen-erative research question we mentioned above).During the following meetings, it was observed that
trainees repeatedly asked the teachers for clarifications onconcepts and vocabulary used. Some participants,especially those with a strong quantitative background,continued to express their doubts about the
epistemological legitimacy of the label “scientific” forQRM. These persisting questioning pushed teachers todiscuss the methodological and epistemological QRM un-derpinnings till trainees submitted the research protocolsto the Ethical Committee. Discussions were often aboutthe meaning of conducting a naturalistic inquiry in health,the interpretative turn, the role of human and social sci-ences in comprehending health-related phenomena, andthe constructivist research paradigm. Moreover, observa-tions have been made about participants needing tounderstand what they had to do during the phases ofdrafting their interview guides for the protocol and thephases of coding. The tasks the teachers planned to ac-complish have been perceived too broad.
[During a group meeting on interviews coding] theteacher asks the participants to conceptually codethe data, word by word or incident by incident ifconvenient. The nurse asks: “how many labels youwant from this interview?”. The PI doubts the groupcan do this. The teacher says he is available forcomment on their provisional coding. (Excerpt fromfield notes, month 8)
Trainees preferred support from time to time in focus-ing their work on a specific aim.At the end of the training, most of the participants
gained a sense of trust toward the scientificity and rigorof non-quantitative evidence construction, still revealing
Table 3 Participants’ characteristics (trainees)
Role Profession Gender Age Education Work Place
Trainee/researcher Information specialist of theHospital Medical Library
F 41–50 Humanities Clinical Cancer Centre
Trainee/researcher Physiotherapist M 31–40 Rehabilitation Sciences Local Health Authority
Trainee/Principal Investigator Professor of Scientific Evidencesfor Nursing
M 61–70 Nursing University
Trainee/researcher Dietician F 31–40 Nutrition Sciences Local Health Authority
Trainee/researcher Nurse, responsible of PalliativeCare Unit Training
F 51–60 Nursing Clinical Cancer Centre
Trainee/researcher Palliativist F 31–40 Medicine Clinical Cancer Centre
Trainee/researcher Nurses’ Manager F 41–50 Nursing Clinical Cancer Centre
Trainee/researcher Nurse F 31–40 Nursing Local Health Authority
Trainee/Principal Investigator Oncologist F 31–40 Medicine Clinical Cancer Centre
Trainee/researcher Laboratory Technician F 31–40 NeurophysiopathologyTechniques
General Hospital
Trainee/Principal Investigator Speech Therapist F 31–40 Speech Therapy andRehabilitation Sciences
University
Trainee/researcher Nurses Manager F 51–60 Nursing Local Health Authority
Trainee/researcher Physiotherapist F 41–50 Rehabilitation Sciences University
Trainee/researcher Physiotherapist F 31–40 Rehabilitation Sciences General Hospital
Ghirotto et al. BMC Medical Education (2020) 20:269 Page 7 of 15

not to be autonomous in performing activities like defin-ing the research question, the interview guide and thecoding. During the final FG meeting, the teacher empha-sized this, highlighting positively the effort some of thetrainees put into the training activities but alsocommenting that, in her view, especially people withlong-lasting experience in a clinical and quantitativeresearch would need an interdisciplinary team for doingqualitative research. Contextually, the trainees com-plained about having “wasted time” in the activities re-lated to research question definition, preferring to havehad a “prepackaged” research question. This preferenceemerged mostly from clinicians.Initial curiosity seemed to turn into pleasure, as stated
by one participant during the final FG meeting.
“I have to admit it was a pleasant surprise, eventhough it is an undefined topic.” (Nurse)
Another trainee evidenced
“The pleasure to look back and reflect over thingsand observe them in depth!” (Physician).
Motivational aspects and difficulties in learning andconducting QRMMotivations and personal investment in the trainingwere observed, since the first meeting, when traineesseemed to have understood that the training would haverequired a personal commitment. A nurse voiced:
“I know that qualitative research is a demandingtask” (Nurse).
Generally, it could be observed that some steps(constructing the research question, performing inter-views, and coding) were perceived particularly challen-ging. One of the PIs reported:
“Constructing the question that drove us to do thestudy and the search for categories were theelements that seemed most critical to me.” (Nurse).
Difficulties in QRM skill acquisition emerged mainlyfrom interviewing. The members of two groups strug-gled both to cope with their feelings elicited by theresearch topics (generating questions a. and b.) andto bracket their sensitivity and professional back-ground. The third group whose research question was‘what the hospital assistance of migrant cancer pa-tients is’, decided not to interview patients. Theyfeared to live an emotional burden facing “frail” pa-tients. Besides, they were strongly motivated in being
involved in the research as they perceived it relevantfor local policies.The majority of the trainees highlighted the emotional
difficulties in being so close to research participantsduring the interviews. From the analysis of the fieldnotes, the recurrent words and phrases used to describethe personal emotions related to interviewing were:“feeling in difficulty”, “I feel uneasy”, “after the interviewI felt emotionally upset”, “agitated”, “embarrassed”, “Ifeel afraid”, “I was anxious all the time”. A nurse stated:
“It was a completely new and unknown experiencefor me. So, it was a dive into the dark, let’s say... andlike all new experiences, they scare you because youdo not know how to manage them” (Nurse).
As the training progressed, trainees began to report ontheir perceived professional and personal growth comingfrom the process of enquiring on real experiences livedby the study participants; this widely emerged duringboth formal and informal conversations.The trainees have highlighted, especially at the end of
the course, that the knowledge of a research method notbased exclusively on the production of quantifiable evi-dence has fueled an unusual approach to the relation-ship. In essence, it was noted by nurses and physiciansthat deepening experiences of patients and family mem-bers, as qualitative interviewing demanded, was usuallyimpracticable in clinical practice.
“It gave me a lot, taught me the right way to relate tothe person ... because ... in the end you see their pointof view, which in the hospital is always left a littleaside. Doing qualitative research has fueled a differenttype of relationship with the subjects” (Physician).
“This can really change you... it can change yourapproach with people, with patients ... like in theconstruction of the interviews above all, that is, Iinitially asked questions to them too directly, withwords a little ... that is ... too direct, too even a bitspecialized perhaps“ (Nurse).
Despite the worries, the trainees felt involved ininterviewing with pleasure and a sense of fulfilment.But this motivational energy weakened during thesubsequent stages of the training. A significant changein personal commitment has been observed from thephase that a trainee has called “desk research” (phase#5). Motivation cooled down, especially after the datacollection phase, during which trainees repeatedlycomplained about the difficulty in managing time todevote to research-related activities because of their
Ghirotto et al. BMC Medical Education (2020) 20:269 Page 8 of 15

busy work schedules and shifts. Also, the instructorparticipating in the FG confirmed that trainees
“seemed to have prioritized practical activities over… data analysis and reporting, which are part of theresearch … as important as the other tasks”.
At the beginning of the training, participants werealways on time and attended regularly. This behaviorchanged throughout the training and, during the finalsessions, some participants were often absent, or theydid not do the assigned homework. During the finalfocus group, all trainees commented on their experiencewith QRM as positive, and that the course had rewardedtheir initial interest in learning a research approach.
“I had no expectations; I approached qualitativeresearch as a tabula rasa [clean slate], and all thereasons I had to participate have been met beyondmy expectations” (Physiotherapist).
As to the instructor, she commented that she feltcomfortable working with the trainees and evaluated theexperience of teaching QRM to colleagues in themedical field as positive.
Group-related factors: teamworkingAs the instructor remarked during the final FG, thetraining was based on participants’ interdisciplinaryteamwork as means to perform a GT qualitative study.Although the training emerged as an opportunity forenhancing participants’ personal and professional growththrough the interaction between professionals withdifferent background and roles, it also activated specificin-group dynamics.During the first session, teachers shared with the
participants a sort of code of conduct requiring theannulment of professional hierarchies for successfullycarrying out a joint project. Nevertheless, at the begin-ning of the training, we could repeatedly observe thatthe dynamic shaping the relationships between partici-pating HPs was based more on the different roles theyhad within their workplaces rather than on the commu-nion of intent. Participants often mentioned that:
“Working with physicians, telling them what to do… it is not the way I am used to. I do not know if Iwill be able to coordinate the team” (Speech therap-ist, PI).
Moreover:
“I play a different role every day; it’s kind of …strange to me. When I clearly understood that
qualitative research is not done without working ina team, I concentrated on this aspect and learned toappreciate the effort to achieve a shared result, toharmonize ideas, to reach a result together” (Phys-ician, PI).
The PIs were invested in an exclusive responsibility;not all of them felt to be prepared to.
“[As the PI of my research project] it was not easyto manage a group of people with managerial roles;however, trying to achieve a sort of working balancebetween professional roles and hierarchies was verystimulating. I put myself to the challenge” (Speechtherapist).
“At the beginning, I did not want this task, Ithought it was too demanding (...) but then theatmosphere that was created, what I learned inmanaging different thoughts and methods, paid meback for the effort” (Nurse)
“If I think of words that identify teamwork, I canuse ‘harmony, positive approach, desire to do, goodharmony, energy’” (Physician)
Teamwork was also described as a viaticum fordialogue and collaboration between different profes-sionals. As trainees have often underlined, doingresearch together meant changing habits in communica-tion among professionals.
“Until now, I had never worked so closely with adoctor! I think it is a way to understand each otherand lay the foundations for positive future collabor-ation” (Nurse).
While the collaboration among team members wasfundamental to overcome issues related to protocolwriting and interview-related worries, as to time for dataanalysis and reporting, teamwork was also the scenery ofarguments among members.
“Fortunately, I had people at my side who helpedme a lot, and then slowly, the anxiety and fear havefaded and instead has given way to the curiosity of... precisely being part of something I had neverbeen part of” (Nurse).
The members are very serious at the beginning ofthe meeting. The teacher welcomes all and asks
Ghirotto et al. BMC Medical Education (2020) 20:269 Page 9 of 15

how the analysis went so far. Participants look ateach other. The PI starts saying they need an exter-nal point of view because they did not reach anagreement about categories and the theoreticalmodel. The teacher reminds us that all the state-ments from the data have to be justified by the datathemselves. A member says that they stated some-thing that there is not in the interviews. Anotherone explains that she does not agree. The PI looksat the teacher like saying: you see? (Excerpt fromfield notes, month #11)
In the group led by the nurse, it was possible tonotice how teamwork has never been fully realized:after having completed the first data analysis,personalism emerged during the most conceptualanalyzes of their GT. The members discussed, in thepresence and via email, the possible interpretationsof the data and conceptual categories. These discus-sions became more heated when the group wasasked to define a theoretical model, that is, therelationship between the conceptual categories. Eachof the members had a different interpretation andwanted it to be accepted.In the group led by a doctor, on the other hand, it
seemed that teamwork has been more peaceful. Duringthe group meetings with the trainers, the PI reportedseveral times that she was satisfied with the teamwork.From the field notes, her leadership emerged as feeble.In the group led by the speech therapist, that com-
pleted the research and first published the article, themembers were able to differentiate competencies andtasks and, most importantly, to put aside their personalresearch interests in favor of that one of the groups. Thelibrarian commented:
“Even if you do not care about the topic, you donot ignore it for reaching the goal. I have toabstract myself from my research interests.Maybe some people are only interested in oneaspect, and they know a detail. Sometimes it isbetter not to know anything. I do not knowanything: without prejudice, maybe I am theexpert on anything”.
Organizational factors: the feasibility of QualitativeResearch and its relation to the work settingBeyond educational, motivational and group-relatedfactors which affected attitudes towards conductingQRM and competencies’ acquisition, organizational fac-tors were identified as influencing skills’ deployment.Trainees often questioned the feasibility of implement-ing QRM in their workplace. Although this issue oftenemerged during the various phases of the training,
observations performed during the last sessions led par-ticipants’ beliefs to come to light explicitly. Opinionsexpressed by trainees toward this topic differed byprofessional role. Nurses with no managerial responsi-bilities and non-medical professionals were doubtfulconcerning the applicability of qualitative research intheir workplace, in consideration of difficulties theyperceived in putting their acquired QRM competenciesinto their future practice.In particular, feeling to be the only one in the work-
place to know and appreciate qualitative researchaffected the perception of QRM being feasible in thefuture.
“It is difficult to move forward if your colleaguesdo not understand the benefit of QRM, especiallysince this type of research requires a considerableamount of energy and dedication. It would be apity not to be able to use it more” (Nurse in aday hospital).
“Since I work in a lab, [QRM] will certainly not helpme because it is a technical field, and I regret that.However, that does not mean it has not helped toopen my mind and make me want to try. But thefact is that I am quite sure I am not going to use itanymore.” (Laboratory Technician).
On the contrary, physicians and nurse managers weremore optimistic about the application of QRM in theirarea. This was clear since the first meeting when a phys-ician stated
“I started the training because I had noticed thecuriosity of colleagues with a similar research meth-odology and the need to understand in detail somesensitive issues. Since I work in oncology, I realizedthat there are several issues that quantitativemethods cannot explore”.
During the FG, she confirmed her initial idea:
“I have to say that many of my current researchprojects are the result of this training” (Physician).
Another physician recognized the similarity betweenQRM and previous training in narrative medicine andoften reported her experience during the training. Dur-ing the final interview, she stated that
“(QRM) extends my previous training in narrativemedicine. I do not think I will have difficulty usingit again” (Physician).
Ghirotto et al. BMC Medical Education (2020) 20:269 Page 10 of 15

For all the participants, what alarmed the most aboutimplementing future qualitative studies was the work-load QRM needed. Nonetheless, it was observed thattrainees who could rely on the help of the teachers andcolleagues expressed the willing to plan other research.While at the beginning of the training participants did
not know how much QRM could help them in theirwork, during the FG, they made suggestions on the im-plementation of strategies to raise colleagues’ awarenessabout the usefulness of the QRM (at the institutionallevel and within their workplaces).The perception of QRM feasibility in the workplace
also varied according to what was considered a relevanttopic by trainees. Informal conversations informed thatsome of the members of the group dealing with the nov-ices experiencing for the first time the death of a patienttook the training as a mere research exercise as the topicwould have not substantial implications for the clinicalpractice. The dietician and the physiotherapist, in par-ticular, were those who doubted the utility of addressingsuch a research topic. PIs of the other two groups, con-trariwise, perceived the topic had value for practitioners.During an informal conversation, the nurse managersaid:
“I will use the research findings to modify the carepathway and inform the practices in use”.
DiscussionThe purpose of this study was to comprehend the atti-tudes of HPs learning and conducting QRM within apractical training program developed in their workplace.Following an ethnographic approach allowed us to illu-minate the social actions and interactions that occurwithin a specific context and, in particular, to emphasizethe factors influencing HPs attitudes and skill acquisi-tion. As Kuper and colleagues pointed out [28], aspectsof medical education should be investigated as the prod-ucts of interactions between two or more individuals orgroups. This was the case of learning and conductingQRM. This could be seen as broadening the methodo-logical horizons in medical education [17, 28].Based on our observations and analyses, we found that
one of the significant limitations to spreading of QRM isthe researcher’s methodological mind-set. Most oftenHPs were educated to an exclusively evidence-basedapproach which made them skeptical about the rigorousmethodology and usefulness in the medical field, inagreement with findings from previous works [11, 29,30]. To limit the risk that previous educationalbackground would prevent acquiring skills for QRM,academic curricula should address qualitative method-ology, at least by informing about the benefit of usingqualitative evidence in clinical reasoning [31].
This educational bias was, however, overcome byeducating participants on the purpose of the qualitativeapproach and the validity and academic rigor of qualita-tive methodology, in agreement with other experiencesin literature [4, 32]. The hands-on experience in carryingout their qualitative research projects in a real settingfurther corroborated their appreciation for the approachand provided them with a new skill set, includingqualitative interviewing and inductive data analysis. Itappeared that learning QRM by doing it, and especiallyby performing a GT [8], within a tutored setting, is anessential and promising pedagogy. Besides, qualitativehealth research always requires practical activities ratherthan mere theoretical and abstract discourses [33].Once participants embraced the new mind-set and
mastered their new skills, they recognized the positiveeffect QRM training had also had on their relationshipswith colleagues that covered different professional roles.This also led to experience the potential of the teameffort in pursuing projects, also beyond the scope ofQRM. It is worth a mention the responsibility PIs’ arecalled to take for managing intra-group dynamics,especially in a context of QRM interprofessionalcollaboration.Moreover, learning-by-doing how to design and con-
duct QRM can be thought as a means for humanizingcare provided by HPs. Todres et al. [34] describe themutual relationship between a person-centred valueframework for health care and the implications of thefindings of QRM as a systematic whole for humanizingcaring practices [34]. They stress that a humanizing em-phasis on care requires a particular kind of ‘knowledgefor care’ and needs studies with specific epistemologicaland methodological characteristics. Such characteristicsare intrinsic to QRM and require, as our trainees real-ized, personal involvement, openness to contexts, andsensitive relationship to research participants, especiallywithin cancer care [21]. While Todres and colleagues[34] portray a reciprocal relationship between thisframework for care and QRM, we can move forward thisconcept, proposing a complementary relationship be-tween care humanization and learning-by-doing QRM,about which we hope further research will be carried outin oncological settings.Finally, the study documented another obstacle in the
time constraints of HPs and the future feasibility ofQRM training. Given that participants already had busyworking schedules, the project required they additionallyresort to, or develop, time-management skills, in orderto be able to complete the study. This aspect of time-management skills was also described by Calderón [12]in a commentary summarizing an eight-year qualitativeonline training experience addressed to GPs, and byFeatherstone et al. [13] in their ten-year follow up on
Ghirotto et al. BMC Medical Education (2020) 20:269 Page 11 of 15

qualitative research training in primary care. PIs shouldhave the capacity of helping team members in managingtime and tasks. Nonetheless, the time qualitative re-search requires is an element to be taken into consider-ation in the evaluation of the behaviors of HPs doingresearch in their workplace. It is quite impossible toforesee how much time a qualitative study needs to becarried out. Facilitators to motivate HPs to attend QRMcourses may include defining in advance a formal learn-ing agreement among trainees and their clinical man-agers in terms of mandate and research topic toinvestigate. HPs need to have their research-related timerecognized as part of their profession. CME creditsshould be flexibly accredited by managers and at leasttwo colleagues from the same unit or ward should at-tend the training to avoid sense of isolation.One last noteworthy consideration is on the transfer
of QRM skills and applicability in HPs’ departments orunits. In our study, the possibility of achieving thisappeared to depend on the perceived work-related rele-vance of the research topic and the presence of othercolleagues sharing an appreciation for QRM. Asdescribed by Hunt et al. [35], projecting oneself intoperforming qualitative research in the future has to dowith one’s expectation, or not, to be alone and isolatedin playing learned skills. Contextually, from our analysisthe importance of connecting research topics to profes-sional practice emerged. HPs’ clinical and work activitiesinform research interests, so it is inevitable that HPs’expectations about QRM involve what research can dofor helping them in their workplace [12].Findings from our ethnographic study supported the
funding by the Clinical Cancer Center Scientific Direct-orate of two further editions of the training, involving34 HPs. The results of the qualitative researches carriedout during these training programs were reportedwithin local, national and international events. Traineeshad the chance to present their work to them col-leagues and managers during a seminar. Their studieswere commented by an invited lecture from abroad.This allowed spreading awareness around QRM andthe added value of applying this type of research inhealthcare settings.As to research relaunch about HPs learning QRM
within the workplace, it would be interesting to isolatesensitive outcomes to evaluate over time. This coursewas an opportunity for trainees to reflect on the rela-tionship with teammates and the participants of theirGT studies (colleagues, patients and family members).Learning how to conduct QRM studies may also meanlearning how to deal with feelings, overcome hierarchyissues, work together for a common goal, improve rela-tionships in the workplace. Besides, acquiring QRMcompetencies may positively affect the personal skills in
communicating with patients and users. Further researchto evaluate the impact of QRM training not only on par-ticipants’ learning but, more importantly, on workplaceclimate and care quality is suitable.
Strategies for future qualitative research methodologyhands-on training addressed to health professionals incontinuing educationIn the last decades, an interesting debate has arousedconcerning the problem of teaching QRM, or ‘how toteach the tools of an uncertain trade for use on an un-known job’, as synthesized by Mason [36]. This FE addsinsights on how to design a future learning-by-doingstyle QRM training to HPs. Following our main results,we may propose points worth considering.In general, QRM trainers should provide ways for
others to learn doing research by researching. Teachersshould also avoid abstract descriptions of methods be-fore the novices understanding of what research is and isabout [37]. In this regard, planning a syllabus is recom-mendable: it would avoid improvisation and allowsteachers to make a learning agreement with managersand future participants.Before the beginning, we may suggest the following
strategies:
– Hands-on training requires CME providers to beflexible in allowing varied didactic techniques and aflexible schedule. We suggest the trainers share thesyllabus with both CME Scientific Committee andfuture participants’ managers. For the subsequenteditions of the QRM training, we planned to discussin advance HPs candidates’ participation withmanagers.
– As to organizational factors, time constraints shouldbe taken into account. Managers, who have agreedon the participation of their colleagues, are awarethat doing research is a time-consuming activity.Acknowledging proper CME credits or lighteningordinary workload are facilitating factors. In anycase, QRM activities have to be reckoned as workinghours.
– Trainers should contact managers and ask them toencourage HPs participating QRM trainingprograms, mainly if these include teamworkeducation, in order to nurture a positive culture oflearning and teamwork within the workplace, inaccordance to what suggested elsewhere [38].
– It has been reported [4, 11] that cognitivedissonance is an ingredient of QRM learning andpractice to be managed by the trainers and,hopefully, by peers. As several authors pointed out[39–41], experienced mentorship plays a pivotal rolein becoming confident on how to conduct
Ghirotto et al. BMC Medical Education (2020) 20:269 Page 12 of 15

qualitative research. The training staff shouldinclude methodologists as teachers and trainers andexperienced tutees.
– As to group-related factors, we noted that being aPI is demanding. PI has to manage intra-groupdynamics, and they should be prepared or, atleast, accompanied by trainers. According to ourfindings, the characteristics of teams that have ledto successful participation in teamwork (andpositive outcomes for team performance) [38]include: the ability of the PI to differentiate thecompetencies within the group; the capacity ofthe members to put aside their personal researchinterests (and personalism) in favor of that one incommon. If the QRM training involvesconducting real qualitative studies, deciding whowill be a PI is unavoidable. A preliminaryworkshop about what being PI in a research teammeans may be advisable. This strategy may limitlikely hierarchy-related issues.
During the training, we may highlight the followingstrategies:
– as to educational factors, we already pled forintegrating QRM within academic curricula astaking qualitative evidence is becoming more andmore beneficial for clinical reasoning [31]. For futuremethodological training within the workplace, it iscrucial to teach ontological and epistemologicalessentials since they are prerequisites tocomprehend QRM. We suggest discussingontological and epistemological underpinnings whiledoing research activities by planning in-betweensessions for reflexivity and thoughts-sharing.Experiential learning is advantageous to understandboth the philosophical orientation and practicalskills necessary to conduct QRM [11]. Moreover,this fashion fits the practice-oriented attitude ourparticipants showed.
– Sessions for freely sharing personal accounts(feelings, comments, opinions) among trainers andtrainees should be planned in order to deal withmotivational factors. According to therecommendations from a systematic review aboutHPs’ experience of teamwork education [38], thefirst meeting should explore participant learningneeds and their prior experiences of working inteams before implementing teamwork educationprograms. Then, from time to time, allowingtrainees to voice their perceived difficulties indedicated debriefing and reflection sessions could bea form of support and a facilitating factor for skills’acquisition.
– We also suggest keeping the level of trainees’commitment as high as possible by selecting QRMprojects perceived to have a practical value. Also,having process evaluation sessions may periodicallyre-motivate trainees’ participation.
At the end of the training, we suggest the followingstrategies:
– PIs and team members should arrange briefmeetings within the wards or units to present theirresearch to colleagues and managers;
– Trainers, along with trainees, should organize aCME event as an opportunity to raise awarenessabout QRM and its value for healthcare.
Strengths and limitationsLimiting a training assessment to participants’ satisfac-tion and learning questionnaires, necessary for CMEs,reduces the possibility of taking into account personaland contextual aspects. In this case, we conducted aqualitative assessment through FE to better understandthe attitudes of the HPs towards new learning. The re-sults discussed here have allowed us to understand, astrainers, what barriers and facilitators HPs have experi-enced and how to enhance future methodological train-ing offer. Besides, as recently outlined [17], FE offers amethodological approach tailored to medical educationcharacteristics and should be a part of the qualitativetoolkit in medical and health sciences educationresearch.There are also methodological limits which it is essen-
tial to discuss. Only six out of 14 trainees participated inthe FG. Tracing the reasons for non-participation wasnot possible. We can hypothesize that those who partici-pated in the FG were more likely to be satisfied with thetraining they attended. As one teacher was present dur-ing the FG, trainees could be influenced during the dis-cussion. Nonetheless, including a teacher together withtrainees enriched our dataset, providing observationsfrom a different point of view. Mostly, collected datawere about trainees and teachers appeared rarely in thefield notes. Only a researcher could analyze the data.Nevertheless, data collection included triangulation, asthe researcher compared data from different sources.The last limitation, and a research relaunch as well, wewould like to note the choice of teaching trainees withthe means of conducting a GT study. This method wasparticularly demanding in terms of time, resources andrequested preparation and could have impacted the re-sults of this ethnographic study. Nonetheless, it appearedto be the most comprehensive methodology for makingthe peculiarities of qualitative interpretative research ap-preciable [8]. Exploring the implication of learning how
Ghirotto et al. BMC Medical Education (2020) 20:269 Page 13 of 15

to conduct GT studies, precisely, rather than anothertype of qualitative investigations, needs further and com-parative analyses.
ConclusionsTaken together, these findings show an appreciation forQRM among HPs and its added value in exploring themany aspects of the healthcare setting that cannot bestudied through quantification. The ethnographic ap-proach provided us with the methodological tools todraw and build upon the wealth of personal experiencescollected by HPs throughout their career. Our findingsshow that QRM training within the workplace elicit anumber of factors to take into account. Learning qualita-tive methodology may foster a renewed attitude towardsone’s professional education, while making inter-professional relationship issues emerge. Nonetheless,broadening the perspectives of professionals on theirclinical practice by means of learning QRM may have anevident quality improvement return.The development and application of QRM across
clinical practice could benefit from (i) dissemination onQRM value and potential in improving everyday clinicalpractice through brief seminars, and (ii) coordinationwith medical management to allow the implementationof QRM training within working hours and withinclearly defined healthcare quality improvementstrategies.
AbbreviationsCME: Continual Medical Education; EBM: Evidence-based Medicine;FE: Focused Ethnography; FG: Focus Group; GT: Grounded Theory; HP: HealthProfessional; PI: Principal Investigator; QRM: Qualitative ResearchMethodology & Methods
AcknowledgementsThe authors acknowledge the contribution made by the trainees. Authorsare grateful to Manuella Walker (Pisa, Italy) for assisting in the editing of thepaper and wish to thank the reviewers that patiently helped them improvingthe manuscript.
Authors’ contributionsLG conceived and designed the focused ethnography. All the authorsdiscussed the data collection strategy and agreed on data triangulationactivities. LDP collected the data and conducted participant observations. LGand LDP interpreted the data and SDL gave a third opinion in case ofdisagreement. All the authors agreed on the overall interpretation. LGdrafted the articles and LDP and SDL detailed its final version. All the authorsrevised the article critically. All the authors agreed to be accountable for allaspects of the study in ensuring that questions related to the accuracy orintegrity of any part of the work are appropriately investigated and resolved.All the authors have read and approved the manuscript.
Authors’ informationLuca Ghirotto, Ph.D. in Cognitive Sciences and Education is head ofQualitative Research Unit at the Scientific Directorate of Azienda USL – IRCCSdi Reggio Emilia, and works at the Department of Human Sciences,University of Verona, Italy as researcher in special and inclusive education.Ludovica De Panfilis, Ph.D. in Medical Bioethics, is a philosopher with an M.D.in Palliative Medicine. Currently she is head of the Unit of Bioethics at theScientific Directorate of the Azienda USL – IRCCS di Reggio Emilia (Italy).
Silvia Di Leo is a psychologist, specialized in systemic-relational therapy, andpsycho-oncologist. She worked at the Palliative Care Unit of the ResearchHospital “Arcispedale S. Maria Nuova” in Reggio Emilia. Now she coordinatesthe Unit of Psycho-Oncology of the Azienda USL – IRCCS di ReggioEmilia (Italy).
FundingNot applicable.
Availability of data and materialsWe do not have ethics approval to make raw data from this study availablefor sharing.
Ethics approval and consent to participateAccording to the Reggio Emilia Hospital “Arcispedale Santa Maria Nuova”internal regulation regarding continuing medical education (CME), theresearcher could dispense with informed consent as the study concernededucational practices and quality improvement. Moreover, in accordancewith internal procedures, the training was endorsed by the competent bodyof the Hospital (CME Scientific Committee) and not submitted to the LocalEthical Committee (Provincial Ethical Committee of Reggio Emilia). Theresearcher, however, adopted specific participant protection procedures.Usually, the trainees are asked to evaluate the curricula and the classroommanagement methods anonymously, filling in a sort of customer satisfactionsurvey. In this case, the researcher asked teachers to agree with trainees toinvolve them in the focused ethnography, with the aim of both evaluatingthe training and discussing their in-service training experience. As the partici-pation in the training implied involvement in the study, teachers made surethat trainees were fully aware of this. Participants had received this informa-tion before the training started, and during the first meeting teachers intro-duced the external researcher (LDP). Trainees were adequately informedabout her role of external observer. Trainees were also informed about confi-dentiality: they were reassured that the method of making observationswould not result in personal identification or harm. Again, participation bythe trainees in interviews and the FG was on a voluntary basis. The re-searcher gathered verbal consent prior to audio recording and audio-registered the consent soon after. It was also clearly stated that all and anyinformation obtained as a consequence of this study would be guaranteedand protected as indicated under the Italian Law on Privacy and, as such,could not possibly be traced.
Consent for publicationParticipants gave consent for anonymous quotes to be published from theresearch.
Competing interestsThe authors declare that they have no competing interests.
Received: 4 November 2019 Accepted: 10 August 2020
References1. Bunniss S, Kelly DR. Research paradigms in medical education research. Med
Educ. 2010;44:358–66.2. Wilson I. Qualitative research in medical education. Med Educ. 2010;44:942.3. Dornan T, Kelly M. What use is qualitative research? Med Educ. 2017;51:7–9.4. von Unger H, Werwick K, Lichte T, Herrmann M. Learning about general
practice through qualitative interviews: lessons from a seminar course withmedical students. Med Teach. 2010;32:e127–32.
5. Arieli D, Tamir B, Man M. Teaching qualitative research as a means ofsocialization to nursing. Nurse Educ Today. 2015;35:795–9.
6. Rosenkranz SK. Wang S, Hu. W Motivating medical students to do research:a mixed methods study using Self-Determination Theory BMC Med Educ.2015;15:95.
7. Reising DL. Establishing student competency in qualitative research: canundergraduate nursing students perform qualitative data analysis. J NursEduc. 2003;42:216–9.
8. Charmaz K. Teaching theory construction with initial grounded theory tools:a reflection on lessons and learning. Qual Health Res. 2015;25:1610–22.
9. Britten N. Making sense of qualitative research: a new series. Med Educ.2005;39:5–6.
Ghirotto et al. BMC Medical Education (2020) 20:269 Page 14 of 15

10. Hein SF. "I don't like ambiguity": an exploration of students' experiencesduring a qualitative methods course. Alberta J Educ Res. 2004;50:22–38.
11. Cooper R, Fleischer A, Cotton FA. Building connections: an interpretativephenomenological analysis of qualitative research: students’ learningexperiences. TQR. 2012;17:1–16.
12. Calderón C. La enseñanza-aprendizaje de la investigación cualitativa en elmedio sanitario. Cien Saude Colet. 2012;17:595–602.
13. Featherstone VA, Barbour RS, Garner J. A reflection on ten years’ experienceof providing qualitative research training in primary care. Prim Health CareRes Dev. 2007;8:198–206.
14. Hepworth J, Kay M. General practitioners learning qualitative research: acase study of postgraduate education. Aust Fam Physician. 2015;44:760–3.
15. Eakin JM, Mykhalovskiy E. Teaching Against the Grain: A Workshop onTeaching Qualitative Research in the Health Sciences. Conference Report: ANational Workshop on Teaching Qualitative Research in the Health Sciences.Forum Qual Soc Res. 2005;6:43 paragraphs.
16. Ng SL, Bisaillon L, Webster F. Blurring the boundaries: using institutionalethnography to inquire into health professions education and practice. MedEduc. 2017;51:51–60.
17. Andreassen P, Christensen MK, Møller JE. Focused ethnography as anapproach in medical education research. Med Educ. 2020;00:1–7.
18. Harris KJ, Jerome NW, Fawcett SB. Rapid assessment procedures: a reviewand critique. Hum Organ. 1997;56:375–8.
19. Higginbottom GMA, Pillay JJ, Boadu NY. Guidance on performing focusedethnographies with an emphasis on healthcare Research. TQR. 2013;18:1–16.
20. Reeves S, Peller J, Goldman J, Kitto S. Ethnography in qualitative educationalresearch: AMEE guide no. 80. Med Teach. 2013;35:e1365–79.
21. Hannum SM, Dy SM, Smith KC, et al. Proposed criteria for systematicevaluation of Qualitative oncology Research. J Oncol Pract. 2019;15:523–9.
22. Henwood K, Pidgeon N. Grounded theory in psychological research. In:Camic PM, Rhodes JE, Yardley L, editors. Qualitative research in psychology:expanding perspectives in methodology and design. Washington, DC:American Psychological Association; 2003. p. 131–55.
23. Losi E, Guberti M, Ghirotto L, Di Leo S, Bassi MC, Costi S. Undergoing headand neck cancer surgery: A grounded theory. Eur J Cancer Care. 2019;e13062. https://doi.org/10.1111/ecc.13062.
24. Denzin N. Interpretative interactionism. London: SAGE; 1989.25. Roper JM, Shapira J. Ethnography in nursing Research. SAGE: Thousands
Oaks, CA; 2000.26. Hammersley M, Atkinson P. Ethnography: principles in practice. New York:
Routledge; 2007.27. Robinson SG. The relevancy of ethnography to nursing Research. Nurs Sci
Q. 2013;26:14–9.28. Kuper A, Reeves S, Albert M, Hodges BD. Assessment: do we need to
broaden our methodological horizons? Med Educ. 2007;41:1121–3.29. Johansson EE, Risberg G, Hamber K. Is qualitative research scientific, or
merely relevant? Research-interested primary care and hospital physicians'appraisal of abstracts. Scand J Prim Health Care. 2003;21:10–4.
30. Goguen J, Knight M, Tiberius R. Is it science? A study of the attitudes ofmedical trainees and physicians toward qualitative and quantitativeresearch. Adv Health Sci Edu Theory Pract. 2008;13:659–74.
31. Dìaz Crescitelli ME, Ghirotto L, Artioli G, Sarli L. Opening the horizons ofclinical reasoning to qualitative research. Acta Biomed. 2019;90:8–16.
32. Parsons GN, Kinsman SB, Ubel PA. Encourage qualitative research toimprove students' clinical skills! Acad Med. 1998;73:933–4.
33. Qualitative MJ, Research H. Creating a new discipline. Walnut Creek, CA: LeftCoast Press; 2012.
34. Todres L, Galvin KT, Holloway I. The humanization of healthcare: a valueframework for qualitative research. Int J Qual Stud Health Well-being. 2009;4:68–77.
35. Hunt MR, Mehta A, Chan LS. Learning to think qualitatively: experiences ofgraduate students conducting Qualitative Health Research. Int J QualMethods. 2009;8:129–35.
36. Mason OJ. Teaching qualitative research methods: some innovations andreflections on practice. Psychology Teaching Review. 2002;10:68–75.
37. Roth W-M. Textbooks on Qualitative Research and Method/Methodology:Toward a Praxis of Method [63 paragraphs]. FQS. 2006;7, Art. 11.
38. Eddy K, Jordan Z, Stephenson M. Health professionals' experience ofteamwork education in acute hospital settings: a systematic review ofqualitative literature. JBI Database System Rev Implement Rep. 2016;14:96–137.
39. Brink EJ. Learning how to do research requires a mentor. West J Nurs Res.1995;17:351–2.
40. Morse JM. Learning to drive from a manual? Qual Health Res. 1997;7:181–3.41. Kuckelman Cobb A, Hoffart N. Teaching Qualitative Research through
participatory coursework and mentorship. J Prof Nurs. 1999;15:331–9.
Publisher’s NoteSpringer Nature remains neutral with regard to jurisdictional claims inpublished maps and institutional affiliations.
Ghirotto et al. BMC Medical Education (2020) 20:269 Page 15 of 15