health it summit austin 2013 - keynote presentation "meaningful use stage 2 and meaningful use...
TRANSCRIPT

Liz Johnson, MS, FHIMSS, CPHIMS, RN-BC
VP of Applied Clinical Informatics and CCIO Tenet Healthcare Corporation
ONC Health Information Technology Standards Committee Member
Modern Healthcare Top 25 Clinical Informaticist 2010, 2011 & 2012
Meaningful Use Stage 2 and Meaningful Use Audit Insight December 12, 2013
Austin
TOPICS
Meaningful Use Stage 2 Core Measures - A road to success
2014 Clinical Quality Measures - The challenges and solutions
Meaningful Use Audits - The basics
2

Stage 1 Data capture and sharing
Stage 2 Advanced Clinical Processes & decision support
Stage 3 Improved Outcomes
Supporting Continuous Quality Improvement
Enabling: Better clinical outcomes Patient Engagement Improved population
health Increased transparency
3

Highlights - Stage 2 Meaningful Use
Impact on MU Program
– Reporting Periods for FFY 2014 changed – Penalties definition clarified – Limited options for menu (5/10 vs. 3/6) – Expansion of CQMs to 29 (select 16) and linked to Clinical Decision Support
Impact on Measures
– Patient Engagement is real – eMAR is now required – eRx and Progress notes are now options – CPOE increased thresholds and definition – Medication Reconciliation is now part of Core – Rolled up multiple measures (problem list, med list, med allergy list into other measures) – Expanded Summary of Care document with electronic exchange component (beyond the sandbox) – Eliminated “capability to exchange key clinical information” measure
Impact on Standards and Certification
– New 2014 Edition of Certified EHR Technology (CEHRT) – Standard changes for Smoking Status, new standard for Preferred Language
4

Stage 2 Core Measures Core Objective Measure is Changing
From “this” to “this” Managing the
Change at Tenet Challenges
1. CPOE for Med, Lab and Rad Orders
• Threshold increased from 30% to 60% for use of CPOE for medication orders, 30% of laboratory, and 30% of radiology
• Denominator changed
from “unique patient” and “at least one medication” to “all medications orders”
Continuing to use our dashboard reporting and adoption strategy (corporate –to- hospital –to- user approach)
A logic change to the CPOE calculations to incorporate additional order types to better represent lab and radiology workflows resulted in drops in CPOE rates for many facilities. As new workflows were incorporated, results recovered.
5
Stage 2 Core Measures Core Objective Measure is Changing
From “this” to “this” Managing the
Change at Tenet Challenges
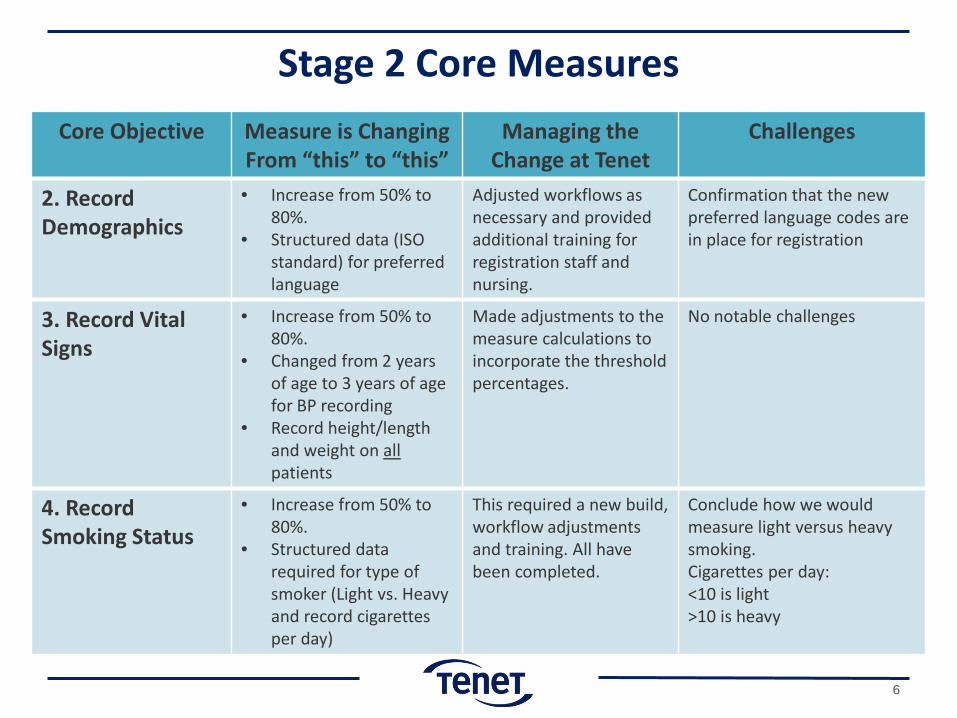
2. Record Demographics
• Increase from 50% to 80%.
• Structured data (ISO standard) for preferred language
Adjusted workflows as necessary and provided additional training for registration staff and nursing.
Confirmation that the new preferred language codes are in place for registration
3. Record Vital Signs
• Increase from 50% to 80%.
• Changed from 2 years of age to 3 years of age for BP recording
• Record height/length and weight on all patients
Made adjustments to the measure calculations to incorporate the threshold percentages.
No notable challenges
4. Record Smoking Status
• Increase from 50% to 80%.
• Structured data required for type of smoker (Light vs. Heavy and record cigarettes per day)
This required a new build, workflow adjustments and training. All have been completed.
Conclude how we would measure light versus heavy smoking. Cigarettes per day: <10 is light >10 is heavy
6

7

Stage 2 Core Measures Core Objective Measure is Changing
From “this” to “this” Managing the
Change at Tenet Challenges
5. Implement Clinical Decision Support Interventions
• Increased from 1 to 5 clinical decision support (CDS) interventions implemented and must be related to 4 or more CQMs.
• Also incorporated the drug/drug and drug/allergy interaction measure into this measure.
CDS rule list was analyzed against the requirements. All of the rules trigger off problems or diagnoses as interventions target patient populations or groups of patients. Workflows and operational processes may need to be addressed in future. 5 CDS choices will also require increase in documentation kept for audit purposes.
This effort has clearly been impacted by the selection of rules as related to CQMs triggered by diagnoses coding.
8
Good to know: The 4 or more CQMs chosen to relate to the 5 CDS interventions can be any of the 29 from the final rule and not limited to the 16 CQMs chosen for the required reporting.
– Implement five clinical decision support interventions
related to four or more clinical quality measures at a relevant point in patient care for the entire EHR reporting period.
– In addition, the clinical decision support interventions must be related to high-priority health conditions.
– CMS also “suggests” that 1 of 5 be related to improving healthcare efficiency. (CDS support to avoid unnecessary or inappropriate care)
Requirements
To Do: Choose 5 -7 CDS interventions related to 4 CQMs and high priority conditions. 1 could be related to improving healthcare efficiency
9

An intervention is evidence-based and is linked to referential supports. The measure requirements state that the hospital is to:
enable a limited set of identified users to select (i.e., activate) one or more electronic clinical decision support interventions (in addition to drug-drug and drug-allergy contraindication checking) based on each one and at least one combination of the following data:
(A) Problem list; (B) Medication list; (C) Medication allergy list; (D) Demographics; (E) Laboratory tests and values/results; (F) Vital signs.
Requirements: Interventions and Triggers
To Do: Document what triggers the CDS interventions we choose and who enters the data
10
Stroke 6 - CDS rule to fire when ischemic stroke patient has LDL lab value greater than 100, or no value (not tested) within the first 24 hours of admission. Confirm patient is discharged with medication of Statin Stroke 5 - CDS rule to fire when ischemic stroke patient is admitted. Confirm patient is administered medication of an antithrombotic by end of day 2.
Examples

Stage 2 Core Measures Core Objective Measure is Changing
From “this” to “this” Managing the
Change at Tenet Challenges
6. Incorporate Lab Results into EHR
• Increase from 40% to 55% • Moved from a menu to a
core measurement
No change for Tenet except for the increased threshold. Continue to monitor the dashboard
Good to know: LOINC is the standard when transmitting lab results to outside entities (i.e. CDA docs)
7. Generate Patient Lists
• No change in objective • Moved from a menu to a
core measurement
No change No notable challenges
8. Automatically track medications from order to administration (eMAR)
• New Core Measure • eMAR is implemented and
used for more than 10% of medication orders
• and tracking of the administration of all doses of the medications using computer assisted technology (required)
Monitoring of reports for all aspects of eMAR and bar coding is in progress. There is ongoing review of eMAR dashboards by each hospital and the IMPACT team
Address workflow for system downtime and also how documentation of barcoding occurs. Use operational reports to monitor and apply corrective action.
11
Good to know: if an event prevented the ability to complete the administration, (i.e. meds not barcoded) the order would not count in the numerator. Also, if med admin is completed but with a response from the patient (i.e. patient vomited), the patient response is not considered a part of the measure and the order would count in numerator.

Stage 2 Core Measures Core Objective Measure is Changing
From “this” to “this” Managing the
Change at Tenet Challenges
9. Provide patients the ability to view online, download and transmit their health information
New Core Measure Consolidates/Replaces these two Stage 1 measures: • eCopy of HI measure • Provide patients with an
electronic copy of their discharge instructions at time of discharge, upon request
• 50% threshold remains New requirements : • More than 5% of all patients
will view, download or transmit to a third party their information during the reporting period
• Required data elements for summary of care are now satisfied by using the Consolidated CDA standard.
• Implementation of the Patient Portal has been a major design, build, test and workflow adjustment effort.
• Strong operational support and process adjustments are necessary to engage patients.
• Built reports to monitor each step of all processes to ensure measurement objectives.
Organization will now be required to attest for the “patients” adoption and use of EHR. We developed a report to monitor “opt in”, “opt out” in order to gage patient engagement and plan patient education. Clarify who will provide instructions/access to the portal for the patient (registration, nursing or both) Address portal content requirements related to sensitive information (HIV results, etc.)
12

Current Workflow for “View and Download” Each patient will be asked at admission if they would like to set up a portal (opt in/out)
If patient says yes (opt in), staff enter information into ADT and EHR systems.
If patient says no (opts out) The hospital will provide
information describing how to opt in to patient portal at a later date
Once registered, a email invitation is sent. A link in the invite takes the patient to a page with instructions to verify information and enter a password. Access is granted with ability to view, download, and transmit information.
13
Stage 2 Core Measures Core Objective Measure is Changing
From “this” to “this” Managing
the Change at Tenet
Challenges
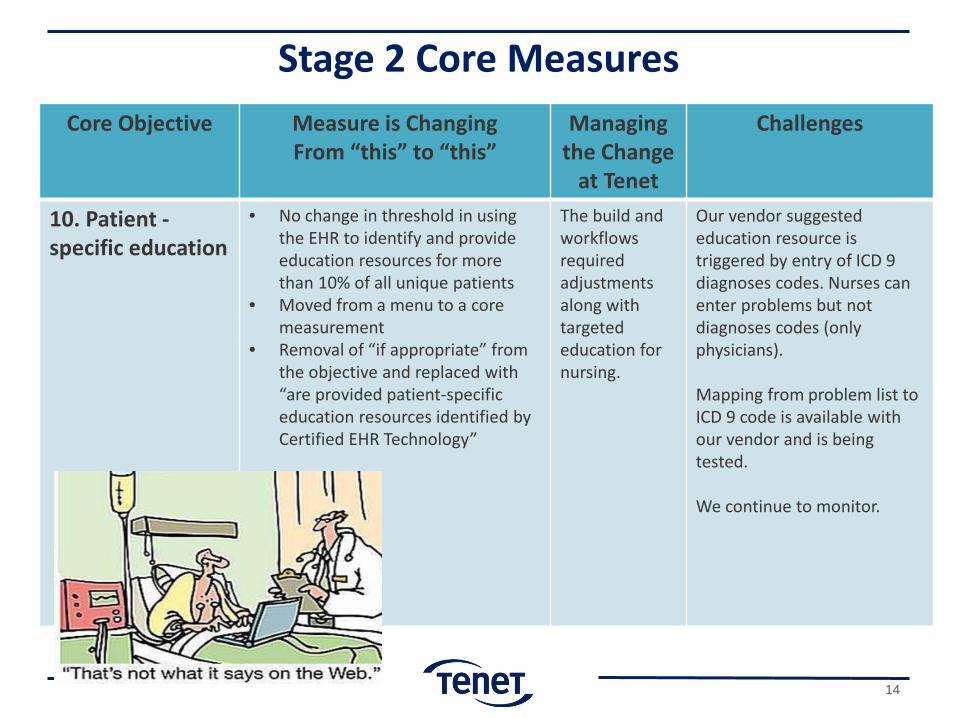
10. Patient - specific education
• No change in threshold in using the EHR to identify and provide education resources for more than 10% of all unique patients
• Moved from a menu to a core measurement
• Removal of “if appropriate” from the objective and replaced with “are provided patient-specific education resources identified by Certified EHR Technology”
The build and workflows required adjustments along with targeted education for nursing.
Our vendor suggested education resource is triggered by entry of ICD 9 diagnoses codes. Nurses can enter problems but not diagnoses codes (only physicians). Mapping from problem list to ICD 9 code is available with our vendor and is being tested. We continue to monitor.
14
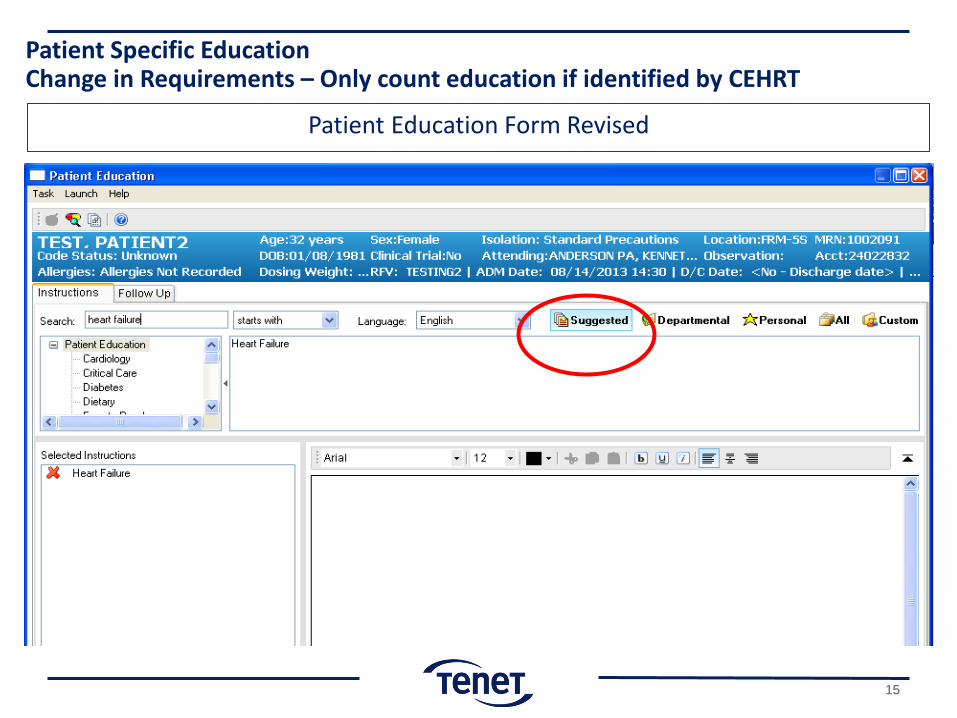
Patient Education Form Revised
Patient Specific Education Change in Requirements – Only count education if identified by CEHRT
15

Stage 2 Core Measures Core Objective Measure is Changing
From “this” to “this” Managing the Change at
Tenet Challenges
11. Medication Reconciliation
• No change in threshold for medication reconciliation for more then 50% of patients upon transitions of care
• Moved from a menu to a core measurement
Ongoing refinement of workflow, continuous education and regular monitoring of adoption continues. Reports developed to monitor daily activity , MU thresholds, and Tenet thresholds.
Promotion of adoption of medication reconciliation at individual hospital has highlighted challenges based on local nuances.
16
Good to know: regulation does not provide when the reconciliation occurs (admit versus discharge); only that it occurs

Stage 2 Core Measures Core Objective Measure is Changing
From “this” to “this” Managing the
Change at Tenet Challenges
12. Transition of Care Summary (Summary of Care)
• No change in threshold for providing a summary of care document for more than 50% of transitions of care and referrals .
• Moved from a menu to a core measurement
New Requirements: • 10% of the SOC documents
must be provided via electronic transmission using Consolidate CDA standard
• Conducts one or more successful electronic exchanges of a SOC with a recipient who has different EHR technology than the sender's EHR technology, OR conducts one or more successful tests with the CMS designated test EHR during the EHR reporting period.
Tenet has the content of the SOC almost completed Electronic SOC transmission at 10% is new and the referral transfer from provider to provider takes some work to figure out. Direct exchange addresses (are needed for this measure. Analysis for performing successful electronic exchange is well underway.
Process includes multiple workflows to address transition of care to various organizations. Our vendor designed this to be a physician workflow. Many external organizations are not able to receive electronic content and thus must create workflow to address various modes of transmission (paper, fax, and direct email) Important to recognize caretaker / ownership of the record for release of information (HIM, Quality, etc..)
17

Electronic Summary of Care Document
CDA
Cerner Care Aware Multimedia
Manager (CAMM)
HUB 1
Cerner Millennium
3rd Party External
Recipient
Receiver HISP
Cerner HISP *
OPS Job Creates CDA document on
scheduled Basis
User selects from a list of Direct addresses to
transmit summary to.
NOTE: If 3rd party is outside of our vendor AND NOT part of Tenet organization – Counts for Measure 3
Work with your vendor
* HISP – Health Information Service Provider
18
Stage 2 Core Measures Core Objective Measure is Changing
From “this” to “this” Managing the Change
at Tenet Challenges
13. Capability to submit immunizations data to registries or immunization information systems
• Moved from a menu to a core measurement
• Went from a test to
successful ongoing transmission of immunization data
Tenet continues to work with all hospitals and all state agencies to get regular reporting instituted. This has required an increase in oversight, control and monitoring.
• Actual contracted vendor solutions proving unacceptable to evolving technical state connectivity message protocol requirements.
• State laws that exceed MU requirements (e.g. SC law requires all immunizations be reported even those not in EHR; like HR captured employee immunizations).
For stage 2, vendor ability to handle ongoing evidence requirements is an issue.
19
Stage 2 Core Measures Core Objective Measure is Changing
From “this” to “this” Managing the
Change at Tenet Challenges
14. Capability to submit electronic data on reportable lab results to public health agencies
• Moved from a menu to a core measurement
• Went from a test to
successful ongoing submission of reportable laboratory results
Tenet is implementing Health Sentry. We are working with our vendor to get a transmission report for audit evidence. Also working with all hospitals and all state agencies to get regular reporting instituted.
• For stage 2, vendor ability to handle ongoing evidence requirements is an issue.
• Confirm CEHRT is capable of populating LOINC codes for all required labs reported.
15. Capability to submit electronic syndromic surveillance data to public health agencies
• Moved from a menu to a core measurement
• Went from a test to
successful ongoing submission of electronic syndromic surveillance data
Tenet is implementing Health Sentry. We are working with our vendor to get a transmission report for audit evidence. Also working with all hospitals and all state agencies to get regular reporting instituted.
• State laws that exceed MU requirements (e.g. NC law requires real time and more robust data set).
• For stage 2, make sure that vendor is providing you the ability to support ongoing evidence requirements. Example, there is no report reflecting actual daily submission everyday.
20

Stage 2 Core Measures
Core Objective Measure is Changing From “this” to “this”
Managing the Change at Tenet
Challenges
16. Security Risk Analysis
• Conduct or review security analysis and incorporate in risk management process; added encryption and data at rest
Having gained recent experience with the Figliozzi (CMS Medicare) audit , they are now asking that if any security issue or corrective action is planned, to provide plan and completed dates (new).
MU Audits now looking to confirm remediation plan and completion dates identified in risk analysis are being addressed. Need to include remediation plans in documentation.
21

Stage 2 Menu Measures (3 of 6 required) Core Objective Measure is Changing
From “this” to “this” Managing the
Change at Tenet Challenges
1. Imaging Results New - more than 20% of imaging results are accessible through CEHRT
Tenet has achieved this - we will be validating this functionality and threshold in January for all hospitals.
Confirm definition of images. At a minimum it should include what is reported in the CPOE Radiology denominator.. Can also include (EKGs, video, etc.)
2. Record Family Health History
New - record family health history of one or more first degree relatives for more than 20% of unique patients
Design changes were needed, as well as workflow and training - all completed. Made use of default field functionality.
Address workflow to include capturing family history as it relates to “adoptions”
3. Generate and transmit permissible discharge prescriptions electronically (eRx)
New - more than 10% electronic prescribing (eRx) of discharge medication orders. Implement drug formulary checks measure is included in this measure
New functionality – go live 10/28. new workflows, training. Multiple reports generated to evaluate performance in progress as well as dashboard monitoring
Awareness that not every pharmacy accepts nor does every patient want electronic prescriptions. Schedule II – V drugs require special attention and most cannot be prescribed electronically
22

Stage 2 Menu Measures (3 of 6 required) Core Objective Measure is Changing
From “this” to “this” Managing the
Change at Tenet Challenges
4. Record Advance Directives
Record status of advance directives as structured data for more than 50% of patients 65 years or older.
No change. Tenet continues to successfully meet this measure.
No notable challenges
5. Provide structured electronic lab results to ambulatory providers
New - provide structured electronic lab results to EP(physician practices) for more than 20%
Not a chosen menu measure for Tenet but we plan to review this next year
Hospital EHR is centralized, but physician offices utilize multiple vendors
6. Record electronic notes in patient records
New - enter at least one electronic progress note created, edited and signed for more than 30% of unique patients
Not a chosen menu measure for Tenet. We are not live on physician notes yet but this is a major focus in the 2014 IMPACT plan.
For some, it will require the acquisition and implementation of physician documentation applications / modules
23
Good to know: LOINC is the required standard for EPs
TOPICS
• Meaningful Use Stage 2 Core Measures - A road to success
• 2014 Clinical Quality Measures - The challenges and solutions
• Meaningful Use Audits - The basics
24
2014 Clinical Quality Measures - Key Themes • Beginning in 2014, reporting of Clinical Quality Measures (CQM) will
be independent of MU stage ― CQM measures are the same for Stage 1 or Stage 2
• Measures and reporting align (NOT YET) with other quality
reporting initiatives ― PQRS, ACO and NQCA (Patient Centered Medical Home)
• Almost all of the CQM’s that are included in the hospital Inpatient
Quality Reporting (IQR) program now have electronic equivalents included in the MU program ― There is extensive discussion in the final rule about the
intention of CMS to convert the hospital IQR and VBP program to electronic measures, as early as 2015
25
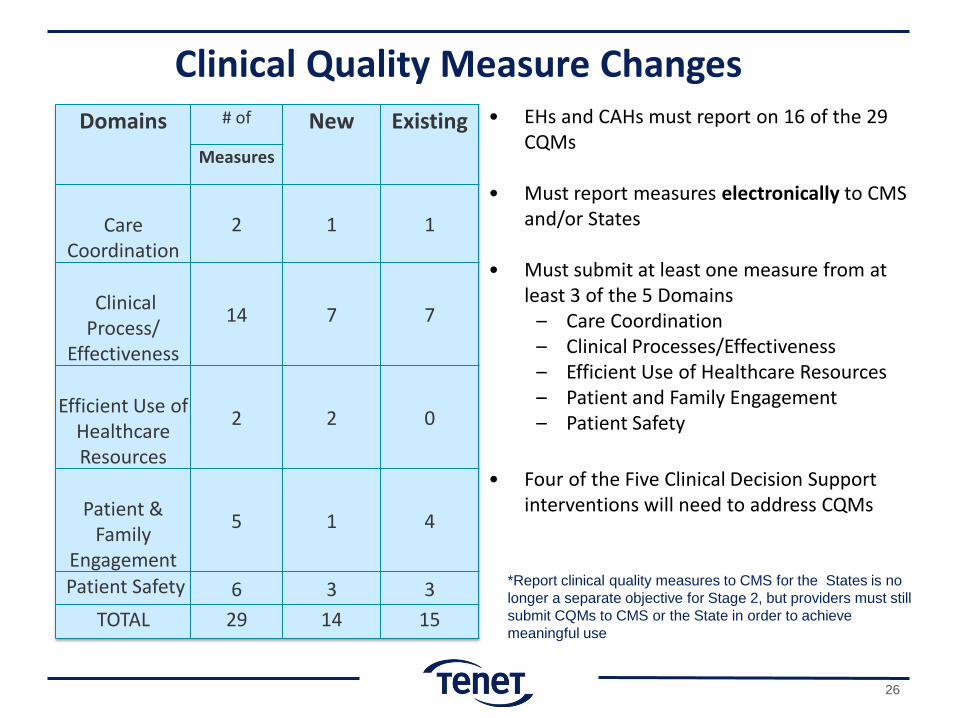
• EHs and CAHs must report on 16 of the 29 CQMs
• Must report measures electronically to CMS
and/or States • Must submit at least one measure from at
least 3 of the 5 Domains – Care Coordination – Clinical Processes/Effectiveness – Efficient Use of Healthcare Resources – Patient and Family Engagement – Patient Safety
• Four of the Five Clinical Decision Support
interventions will need to address CQMs
Domains # of New Existing Measures
Care
Coordination 2 1 1
Clinical Process/
Effectiveness
14 7 7
Efficient Use of
Healthcare Resources
2 2 0
Patient &
Family Engagement
5 1 4
Patient Safety 6 3 3 TOTAL 29 14 15
*Report clinical quality measures to CMS for the States is no longer a separate objective for Stage 2, but providers must still submit CQMs to CMS or the State in order to achieve meaningful use
Clinical Quality Measure Changes
26

Tenet’s MU CQMs Chosen for 2014 Reporting
VTE Stroke ED VTE-1: Prophylaxis within 24 hours of admission
Stroke-2: Discharged on antithrombotic therapy
ED-1: Median time from ED arrival to ED departure for admitted ED patients
VTE-2: Prophylaxis within 24 hours of admission for an ICU patient
Stroke-3: Anticoagulation Therapy for Atrial Fibrillation/Flutter
ED-2: Admit decision time to ED departure time for admitted patients
VTE-3: Overlap therapy Stroke-4: Thrombolytic therapy in 2 hours
ED-3: Median time from ED arrival to ED departure for discharged ED patients
VTE-4: Platelet monitor Stroke-5: Antithrombotic therapy by end of hospital day 2
VTE-5: Discharge Instructions Stroke-6: Discharged on Statin Medication
VTE-6: Potentially Preventable VTE Stroke-8: Stroke Education
Stroke-10: Assessed for Rehabilitation
The list above meets 4 of the 5 clinical domains as required
27

TOPICS
Meaningful Use Stage 2 Core Measures - A road to success
2014 Clinical Quality Measures - The challenges and solutions
Meaningful Use Audits - The basics
28

29
Tenet

The Center for Medicare and Medicaid have established a process for program audits under the final rule:
CMS states that “an eligible professional (EP), eligible hospital, or critical access hospital (CAH) attesting to receive an incentive payment for either the Medicare or Medicaid Electronic Health Record (EHR) Incentive Program may be subject to an audit”
Two types of audits:
– Pre-payment audits will be random and may target suspicious or anomalous data through edit checks built in CMS and State systems
– Post-payment audits can occur during the course of the program
CMS audit process includes the following: – Initial request letters are sent to providers selected for an audit – The initial review process will be conducted using information provided in
response to the request letter – In some cases an on-site review at the provider’s location may follow
30
Just the Facts

31
CMS recommends that eligible hospitals, eligible professionals and critical access hospitals retain all relevant supporting documentation, in either paper or electronic format, used to complete the Attestation process.
All attestation evidence of successful compliance with meaningful use
objectives and clinical quality measures must be retained for six years post attestation.
Documentation to support payment calculations (such as cost report data) are included in the current documentation retention requirements.
Have the documents of evidence always at the ready:
Medicare - CMS and its contractor, Figliozzi and Company, are performing audits on Medicare and dually-eligible (Medicare and Medicaid) providers who are participating in the EHR Incentive Programs Medicaid - States, and their contractor, are performing audits on Medicaid providers participating in the Medicaid EHR Incentive Program OIG - The Office of Inspector General also has been directed by Congress to provide oversight to the State Program
Who are the Auditors?
32

The Audit Request Letters
33
Dear Tenet…

What we are seeing in the letters: Proof required for attestation items:
– Screen shots of dictionary settings to show everyday compliance and to show proof of the use of a certified system the entire reporting period
– Logs or reports showing alerts firing for the reporting period
MU measure reports must show CEHRT vendor and system name: – Documentation from other source systems must show calculations, including numerator
and denominator, time period and NPI or provider name. No spreadsheets
Data exchange proof (CCD and public health) with screen shots from CEHRT:
– Date of test, statement of transmission success or failure – Letter or e-mail from receiving provider stating date, name of provider and success or failure of
test
HIPAA Security Risk Assessment – Must be specific for your EHR modules and release level – Must name each hospital or entity that it covers , ideally by NPI specifically – Report should be dated prior to the end of the reporting period
34
Specific to Medicaid: • Must prove you completed your adoption, implementation or
upgrade • Must provide contracts, purchase orders and proof of payments
35
What we are seeing in the letters:
36

Contact Information
LIZ JOHNSON, MS, FHIMSS, CPHIMS, RN-C Vice President, Applied Clinical Informatics and CCIO Tenet Healthcare Corporation Headquarters 1445 Ross Avenue, Suite 1400 Dallas, TX 75202 Office 469.893.2039 e-mail: [email protected]
37

APPENDIX
38
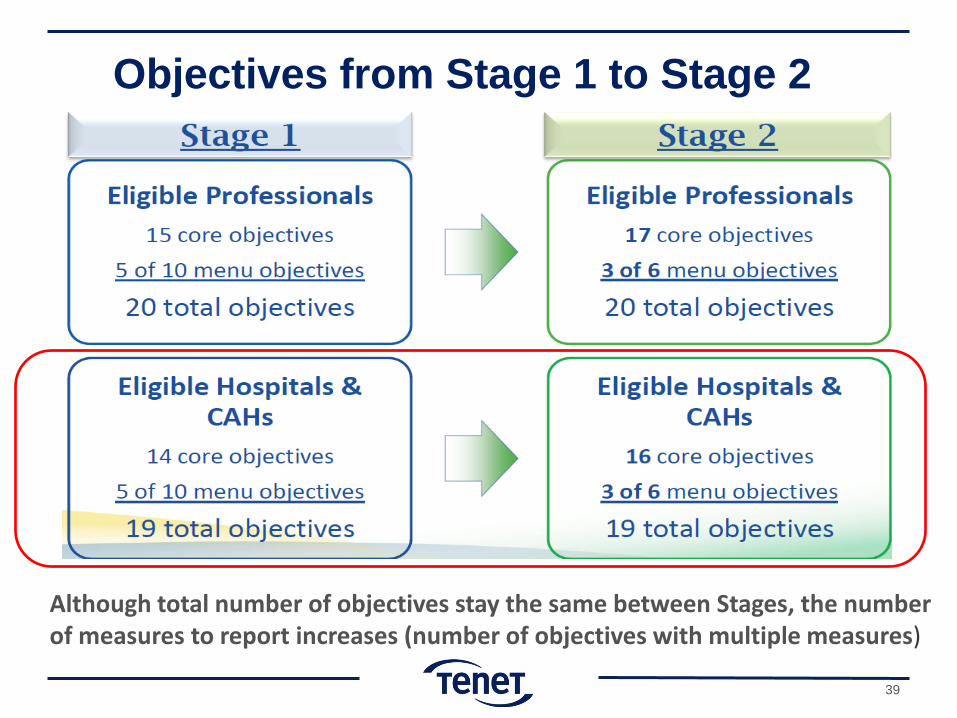
Objectives from Stage 1 to Stage 2
Although total number of objectives stay the same between Stages, the number of measures to report increases (number of objectives with multiple measures)
39

Stage 2 CQM Measures (14) Hearing screening prior to hospital discharge (EHDI-1a)
AMI-2: Aspirin Prescribed at Discharge for AMI
AMI-7a: Fibrinolytic Therapy received within 30 minutes of hospital arrival ** AMI-8a: Primary Percutaneous Coronary Intervention (PCI)** AMI-10: Statin Prescribed at Discharge VTE-3: VTE Patients with Overlap of Anticoagulation Therapy *
VTE 4: Patients Unfractionated Heparin (UFH) Dosages/Platelet Count Monitoring by Protocol (or Nomogram) * Stroke-2: Ischemic stroke – Discharged on anti-thrombotic therapy *
Stroke-3: Ischemic stroke – Anticoagulation Therapy for Atrial Fibrillation/Flutter * Stroke-4: Ischemic stroke – Thrombolytic Therapy *
Stroke-5: Ischemic stroke – Antithrombotic therapy by end of hospital day two *
Stroke-6: Ischemic stroke – Discharged on Statin Medication *
Elective Delivery Prior to 39 Completed Weeks Gestation
Exclusive Breastfeeding at Hospital Discharge
Clinical Process/ Effectiveness
Domain
*Stage 1 CQM currently tracked electronically **Value Based Purchasing
40

Stage 2 CQM Measure (2) Stroke-10: Ischemic or hemorrhagic stroke –Assessed for Rehabilitation *
ED-3: Median time from ED arrival to ED departure for discharged ED patients *
Care Coordination
Domain
Stage 2 CQM Measure (2) PN-6: Initial Antibiotic Selection for Community-Acquired Pneumonia (CAP) in Immunocompetent Patients**
SCIP-INF-2: Prophylactic Antibiotic Selection for Surgical Patients for discharged ED patients**
Efficient Use of Healthcare Resources
Domain Stage 2 CQM Measure (5)
Home Management Plan of Care Document Given to Patient/Caregiver
VTE-5: VTE discharge instructions *
Stroke-8: Ischemic or hemorrhagic stroke –Stroke education *
ED-1 Emergency Department Throughput – Median time from ED arrival to ED departure for admitted ED patients * ED-2 Emergency Department Throughput –admitted patients – Admit decision time to ED departure time for admitted patients *
Patient and Family Engagement
Domain *Stage 1 CQM currently tracked electronically ** Value Based Purchasing
41

Stage 2 CQM Measure (6) VTE-1: Venous Thromboembolism Prophylaxis * VTE-2: Venous Thromboembolism Prophylaxis - Intensive Care Unit (ICU) * VTE-6: Incidence of potentially preventable VTE * SCIP-INF-9: Urinary catheter removed on Postoperative Day 1 (POD1) or Postoperative Day 2 (POD2) with day of surgery being day zero
SCIP-INF-1: Prophylactic Antibiotic Received within 1 Hour Prior to Surgical Incision**
Healthy Term Newborn
Patient Safety Domain
*Stage 1 CQM currently tracked electronically ** Value Base Purchasing
CQM 29 Measures
ACO 1
IQR 12
VBP 7
Measure Overlap
** Value Based Purchasing overlaps with 5 of the CQM measures and also includes 2 additional measures: PN-3b: Blood Cultures Performed in the Emergency Department Prior to Initial Antibiotic Received in Hospital
SCIP-INF-3: Prophylactic Antibiotics Discontinued Within 24 Hours After Surgery End Time
42
43
EH Audit Response This is How Tenet Does It

Tenet Audit Response Process (Medicare)
Alert!
• Receive notification of Audit • Communicate Audit to Tenet Audit Activation Team (TAAT)*
Take Action
• Convene Audit response meeting within 36 hours • Gather documentation and develop Audit response
Finalize and Submit
• TAAT performs final audit of prepared documents/response and then approves
• Approved response and documents sent to requesting agency
* TAAT has senior representation from Applied Clinical Informatics, Audit, Government Programs & Compliance.
44

Tenet EH Audit Response
First request for additional information
Approximately 3 weeks after submitting initial materials, Tenet received 2 additional questions:
• Auditors were unclear as to whether the report provided for measure calculations came from CEHRT; asked for additional documentation
• Asked for validation that the CDS rule had been active during the entire reporting period
Tenet Audit Activation Team gathered again, reviewed and provided additional material via portal and FedEx within 5 days:
• Screen shots from the CHPL site showing Tenet’s self-certification
• Screen shots showing activation start and end for the rule
45
Second request for additional information
Approximately one month later, Tenet received another request asking for:
• Confirmation of the percent of patient encounters captured in the CEHRT. Since Tenet captures all encounters in CEHRT, this was answered by simply stating the following:
For the EHR Incentive Program, Hospital had 1,638 patient encounters occur (admitted or discharged) during the reporting period. All 1,638 patient encounters were entered into the EHR system, therefore the percentage is 100%.
• Documentation that CQMs had been submitted . This request was withdrawn the following day.
• A copy of the security risk assessment. This had been provided previously as documentation with the first request but was provided again.
Tenet EH Audit Response
46
Success! Determination letter received on October 23, 2012 approximately 3 weeks after the last information request, 3 months after the initial request.
We have completed our meaningful use audit of the certified Electronic Health Record (EHR) technology of your hospital in accordance with Section 13411 of the Health Information Technology for Economic and Clinical Health Act (HITECH Act), as included in Title XIII, Division A, Health Information Technology and in Title IV of Division B, Medicare and Medicaid Health Information Technology of the American Recovery and Reinvestment Act of 2009. The HITECH Act provides the Secretary, or any person or organization designated by the Secretary, the right to audit and inspect any books and records of any organization receiving an incentive payment.
We performed a desk review on your facility’s meaningful use attestation for the Program Year 2011 and Payment Year 1. Based on our desk review of the supporting documentation furnished by the facility, we have determined that your hospital has met the meaningful use criteria.
This audit does not preclude your hospital from future audits in this payment year or in subsequent years. Thank you for your assistance and cooperation.
47