health inequalities action plan - bradford … - bradford... · 2014-03-27 · health inequalities...
TRANSCRIPT

Health Inequalities Action Plan
Bradford and Airedale Health and Wellbeing Board
2013 – 2017
T H E B R A D F O R D D I S T R I C T H E A LT H A N D W E L L B E I N G S T R AT E G Y

I am delighted to introduce the Health Inequalities Action Plan, which has been developed by the Bradford and Airedale Health and Wellbeing Board to support the Joint Health and Wellbeing Strategy (JHWS). The plan is intended to be read alongside the JHWS as it ensures that, as we strive to improve the health and wellbeing for the whole population of Bradford District, we also remain mindful of the significant inequalities within the district – the fact that in some parts of the district, people lead far shorter, less healthy lives than those in other areas. The plan spells out that we have the greatest chance of reducing inequalities in health and wellbeing if organisations, communities and individuals continue to work closely together. Our commitment to sustaining and developing partnership working has never been more important than it is now as we try to sustain progress in the face of significant reductions in public spending.
This plan describes the Lead Partnership for each of the 18 priorities in the JHWS, and each of those Partnerships will lead or co-ordinate the work which ensures we continue to focus upon improving the health and wellbeing of those whose needs are greatest and to make tackling health inequalities a top priority.
Councillor David Green
Leader of Bradford CouncilChair of Bradford and Airedale Health and Wellbeing Board
Hea
lth In
equa
litie
s A
ctio
n Pl
an
2
Foreword

What are health inequalities?“Health inequalities” are the differences in the health of different parts of the population. For example, people in more deprived areas have a shorter life expectancy than those who live in less deprived areas. Inequalities also exist in other aspects of people’s health – for example, people in more deprived areas tend to smoke more, drink more alcohol, and are more likely to experience long-term illness. Inequalities also exist between groups according to other factors, such as gender, ethnic background, certain sorts of disability and sexual orientation. Whilst the health of the population has improved continuously since the industrial revolution, the rate of improvement in those from poorer backgrounds has generally been slower than for those who are more affluent. This means that, in health terms, the gap between the most and least deprived is widening.The Local Authority, the NHS locally, and other organisations work hard to ensure that differences between groups are as small as possible – we want to ensure that, wherever possible, an individual’s health and wellbeing is not determined by the area in which they were born, or in which they live, or – for example - their ethnicity.
Why do inequalities matter?In the past two decades there has been an increased focus on reducing inequalities, and in Spring 2013, the Secretary of State for Health said:“Everyone should have the same opportunity to lead a healthy life no matter where they live or who they are, which is why we must continue to work to narrow the gap in health inequalities. Local areas must work together to address the health needs of their population and make a real difference in tackling health inequalities.”
There are a number of reasons why people think that inequalities are important.Possibly the most important reason is that the effect inequalities have seems unfair. Put simply, the poorer a person is, the less likely they are to survive infancy and the less likely they are to live into old age.Additionally, evidence suggests that where the greatest inequalities exist, the health of the whole population – even the relatively affluent – is worse than it would be if inequalities were less significant.There is also an acceptance that inequalities begin in childhood, and subsequently widen over an individual’s lifetime. That is to say that if children have very different experiences of health when they are very young, then they will experience even greater differences as adults.Furthermore, inequalities in health and its determinants can trigger other problems – such as crime, poor educational outcomes, and mental health issues such as situational depression. This can in turn make areas more deprived, and this can widen the gap in inequalities. As such, it becomes a vicious circle.Finally, because Bradford is more deprived than other areas, any argument that inequalities do not matter could logically be extended to say that it is acceptable for the population of Bradford to experience poorer health than those of its neighbours.
What leads to inequalities?There are a number of factors which lead to Health Inequalities. Most experts tend to place these factors into a small number of groups – such as those listed below. It is important, however, to bear in mind that experts think of these as the factors which are likely to lead to poorer health. There is every reason to believe that people can live healthy lives even in the harshest circumstances.
Health Inequalities Action Plan Health Inequalities
Health Inequalities A
ction Plan
3
Social factors:These are issues which affect the population as a whole, but do not necessarily affect everybody equally. Examples include government policies, the availability of work, general levels of wages, taxation and how much things cost – particularly the prices of essentials such as fuel, transport, food, and clothing. These big, broad considerations can affect how much the public sector can spend on health and wellbeing.
Living and working conditions:These include the important issues for people as they go about their lives, day in, day out: things like education, training and employment, housing, public transport and amenities. It also includes basic facilities like reliable utility supplies (gas, water and electricity) and being able to get hold of essential goods like food and clothing.
Social and community networks: A person’s “network” includes his or her family, friends and social circles – and the way all of those people together support, influence, advise and guide the individual. A strong network of family and friends can help to ensure that an individual has a healthy lifestyle. Sometimes, individuals living alone may not have any “network”; sometimes the “network” can have an unsupportive effect, such as encouraging the consumption of alcohol to excess.
Individual lifestyle factors: These are sometimes described as lifestyle choices, because they tend to refer to things that people can generally choose to do, or not do. This would include things such as tobacco use, alcohol consumption, and drug use, whether people eat healthily and whether they take regular physical exercise. These choices are influenced by the environment in which the individual lives – how friends and family act, how products are advertised and so on.
Healthcare factors:There is evidence to suggest that sometimes the parts of the population in the greatest need are poorly understood. This can mean that services are constructed and
commissioned to address the needs of the whole population, but not in such a way that inequalities are addressed.Additionally, low-cost healthcare is sometimes under-used in a population. When this happens, it tends to be the most deprived parts of the population who are worst affected, because illness and disease is most prevalent in those areas. This therefore leads to a widening of the gap between the most and least deprived areas of a population.
Personal factors: These include some of the basic definitions of who people are: age, sex, ethnicity and genetic factors. There is nothing that can be done to change these factors – but understanding more about the population can help us to develop strategies, policies and practices, and can influence the way the Local Authority and the NHS communicate with people.
Addressing inequalitiesBecause inequalities are so complex, we cannot always deal with them in the same way. For example: • Some of the time, we focus on particular
parts of Bradford District, because it is most important to ensure that health and wellbeing in the most deprived areas ‘catches up’ with the less deprived areas. In other instances, the focus is on the whole of Bradford District
• Sometimes, campaigns to improve health and wellbeing need to be focused on individuals; sometimes on the population as a whole
Through wide consultation with partnerships across the District, each of the priorities within the Joint Health and Wellbeing Strategy now has an agreed set of commitments (action points) that will be delivered against to reduce inequalities in that particular area of health and wellbeing.
Hea
lth In
equa
litie
s A
ctio
n Pl
an
4

Health Inequalities A
ction Plan
5
Pr
iorit
y 1:
Red
uce
and
alle
viat
e th
e im
pact
of c
hild
pov
erty
Rel
evan
t sta
ndar
ds a
gain
st w
hich
to m
onito
r pro
gres
s on
this
prio
rity
coul
d in
clud
e:
The
num
ber o
f chi
ldre
n liv
ing
in re
lativ
e po
vert
y
Embe
d ch
ild p
over
ty in
exi
stin
g lo
cal
stra
tegi
es to
focu
s re
sour
ces
on
alle
viat
ing
child
pov
erty
Offs
et th
e ne
gativ
e im
pact
of w
elfa
re
refo
rmIn
crea
se u
ptak
e of
free
sch
ool m
eals
an
d ‘p
over
ty-p
roof
’ the
sch
ool d
ay b
y id
entif
ying
and
rem
ovin
g ba
rrie
rs to
le
arni
ng fo
r chi
ldre
n in
pov
erty
Impr
ove
hous
ing
qual
ity a
nd re
duce
fu
el p
over
ty fo
r chi
ldre
n liv
ing
in
pove
rty
Enco
urag
e po
sitiv
e pa
rent
ing
to
impr
ove
resi
lienc
e an
d he
lp p
aren
ts
prot
ect c
hild
ren
from
the
effe
cts
of
pove
rty
Mak
e em
ploy
men
t acc
essi
ble
for
fam
ilies
now
and
chi
ldre
n in
the
futu
reR
educ
e ra
tes
of a
ccid
enta
l inj
ury
to
child
ren
in p
over
ty
Del
iver
the
Chi
ld P
over
ty S
trate
gyl N
o ch
ild to
live
in s
ub-s
tand
ard
hous
ing
l E
very
fam
ily c
an a
cces
s th
e su
ppor
t the
y ne
ed (e
g. D
ebt a
dvic
e; b
enefi
ts a
nd c
aree
rs
advi
ce; m
enta
l hea
lth; d
omes
tic v
iole
nce
supp
ort;
disa
bilit
ies
serv
ices
)l C
hild
ren
and
youn
g pe
ople
take
adv
anta
ge
of e
duca
tion,
em
ploy
men
t and
trai
ning
op
port
uniti
es (c
ontin
ue to
redu
ce th
e ga
p be
twee
n ch
ildre
n at
foun
datio
n st
age,
key
sta
ge 2
and
key
st
age
4)l B
reak
the
cycl
e of
wor
kles
snes
s by
und
erta
king
po
sitiv
e ac
tion
for v
ulne
rabl
e gr
oups
(low
inco
me
fam
ilies;
une
mpl
oyed
adu
lts; t
hose
who
are
NEE
T or
at r
isk
of b
ecom
ing
NEE
T.l P
ositi
ve p
aren
ting
build
s re
silie
nce
in c
hild
ren
and
fam
ilies
to a
ddre
ss in
equa
litie
s pa
rticu
larly
he
alth
rela
ted
issu
es
Brad
ford
Cou
ncil
–C
hild
ren’
s Se
rvic
es;
Adul
t and
Com
mun
ity
Serv
ices
;R
even
ues
and
Bene
fits;
H
ousi
ng;
Car
bon
Red
uctio
n an
d C
limat
e Se
rvic
es;
Pare
ntin
g Bo
ard;
Third
sec
tor;
Scho
ols;
Col
lege
s;Jo
b C
entre
Plu
s
Chi
ldre
n’s
Trus
t(C
hild
Pov
erty
Bo
ard;
Pro
sper
ity
and
Reg
ener
atio
n Pa
rtner
ship
)
Are
as fo
r Act
ion
Com
mitm
ents
Del
iver
y pa
rtne
rsO
vers
eein
g(a
nd s
uppo
rtin
g)
part
ners
hip
Hea
lth In
equa
litie
s A
ctio
n Pl
an
6
Pr
iorit
y 2:
Red
uce
infa
nt m
orta
lity
Rel
evan
t sta
ndar
ds a
gain
st w
hich
to m
onito
r pro
gres
s on
this
prio
rity
coul
d in
clud
e:
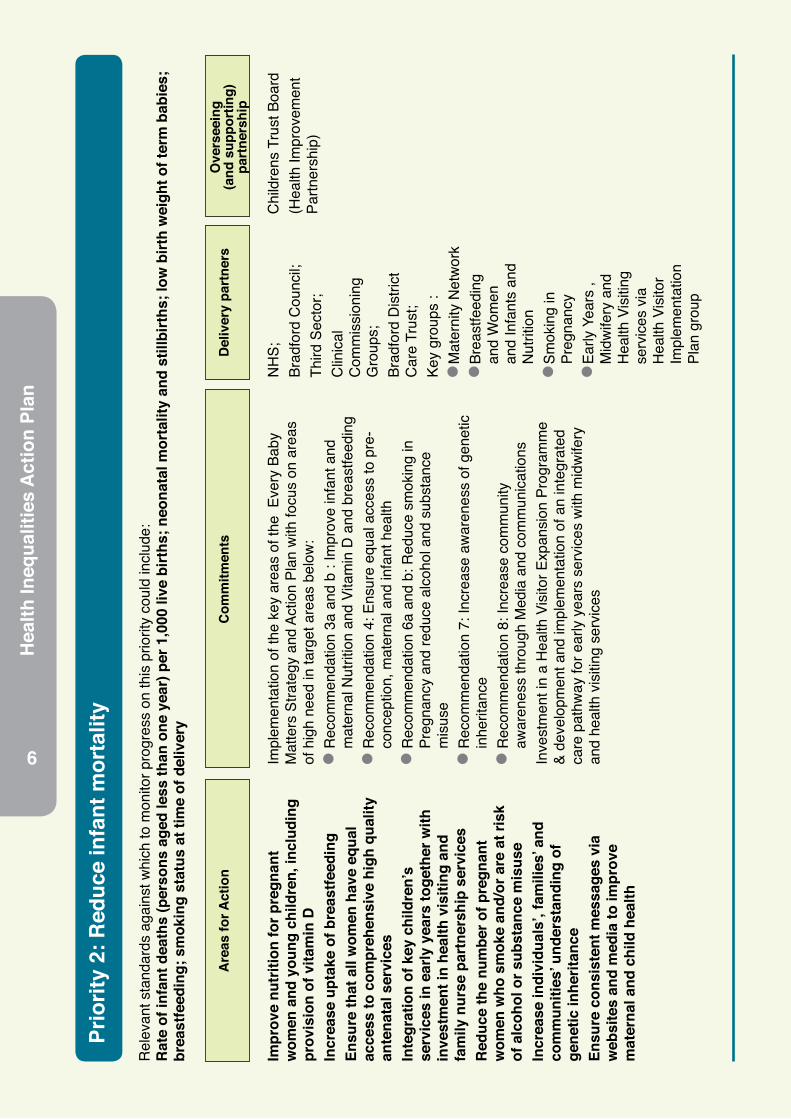
Rat
e of
infa
nt d
eath
s (p
erso
ns a
ged
less
than
one
yea
r) p
er 1
,000
live
birt
hs; n
eona
tal m
orta
lity
and
still
birt
hs; l
ow b
irth
wei
ght o
f ter
m b
abie
s;
brea
stfe
edin
g; s
mok
ing
stat
us a
t tim
e of
del
iver
y
Impr
ove
nutr
ition
for p
regn
ant
wom
en a
nd y
oung
chi
ldre
n, in
clud
ing
prov
isio
n of
vita
min
DIn
crea
se u
ptak
e of
bre
astfe
edin
gEn
sure
that
all
wom
en h
ave
equa
l ac
cess
to c
ompr
ehen
sive
hig
h qu
ality
an
tena
tal s
ervi
ces
Inte
grat
ion
of k
ey c
hild
ren’
s se
rvic
es in
ear
ly y
ears
toge
ther
with
in
vest
men
t in
heal
th v
isiti
ng a
nd
fam
ily n
urse
par
tner
ship
ser
vice
sR
educ
e th
e nu
mbe
r of p
regn
ant
wom
en w
ho s
mok
e an
d/or
are
at r
isk
of a
lcoh
ol o
r sub
stan
ce m
isus
eIn
crea
se in
divi
dual
s’, f
amili
es’ a
nd
com
mun
ities
’ und
erst
andi
ng o
f ge
netic
inhe
ritan
ceEn
sure
con
sist
ent m
essa
ges
via
web
site
s an
d m
edia
to im
prov
e m
ater
nal a
nd c
hild
hea
lth
Impl
emen
tatio
n of
the
key
area
s of
the
Eve
ry B
aby
Mat
ters
Stra
tegy
and
Act
ion
Plan
with
focu
s on
are
as
of h
igh
need
in ta
rget
are
as b
elow
:l R
ecom
men
datio
n 3a
and
b :
Impr
ove
infa
nt a
nd
mat
erna
l Nut
ritio
n an
d Vi
tam
in D
and
bre
astfe
edin
g l R
ecom
men
datio
n 4:
Ens
ure
equa
l acc
ess
to p
re-
conc
eptio
n, m
ater
nal a
nd in
fant
hea
lthl R
ecom
men
datio
n 6a
and
b: R
educ
e sm
okin
g in
Pr
egna
ncy
and
redu
ce a
lcoh
ol a
nd s
ubst
ance
m
isus
el R
ecom
men
datio
n 7:
Incr
ease
aw
aren
ess
of g
enet
ic
inhe
ritan
cel R
ecom
men
datio
n 8:
Incr
ease
com
mun
ity
awar
enes
s th
roug
h M
edia
and
com
mun
icat
ions
In
vest
men
t in
a H
ealth
Vis
itor E
xpan
sion
Pro
gram
me
& de
velo
pmen
t and
impl
emen
tatio
n of
an
inte
grat
ed
care
pat
hway
for e
arly
yea
rs s
ervi
ces
with
mid
wife
ry
and
heal
th v
isiti
ng s
ervi
ces
NH
S;Br
adfo
rd C
ounc
il;Th
ird S
ecto
r;C
linic
al
Com
mis
sion
ing
Gro
ups;
Brad
ford
Dis
trict
C
are
Trus
t;Ke
y gr
oups
:l M
ater
nity
Net
wor
kl B
reas
tfeed
ing
and
Wom
en
and
Infa
nts
and
Nut
ritio
n l S
mok
ing
in
Preg
nanc
y l E
arly
Yea
rs ,
Mid
wife
ry a
nd
Hea
lth V
isiti
ng
serv
ices
via
H
ealth
Vis
itor
Impl
emen
tatio
n Pl
an g
roup
Chi
ldre
ns T
rust
Boa
rd(H
ealth
Impr
ovem
ent
Partn
ersh
ip)
Are
as fo
r Act
ion
Com
mitm
ents
Del
iver
y pa
rtne
rsO
vers
eein
g(a
nd s
uppo
rtin
g)
part
ners
hip

Health Inequalities A
ction Plan
7
NH
S;Br
adfo
rd C
ounc
il;Th
ird S
ecto
r;C
linic
al
Com
mis
sion
ing
Gro
ups;
Brad
ford
Dis
trict
C
are
Trus
t;Ke
y gr
oups
:l M
ater
nity
Net
wor
kl B
reas
tfeed
ing
and
Wom
en
and
Infa
nts
and
Nut
ritio
n l S
mok
ing
in
Preg
nanc
y l E
arly
Yea
rs ,
Mid
wife
ry a
nd
Hea
lth V
isiti
ng
serv
ices
via
H
ealth
Vis
itor
Impl
emen
tatio
n Pl
an g
roup
Pr
iorit
y 3:
Pro
mot
e ef
fect
ive
pare
ntin
g an
d ea
rly y
ears
dev
elop
men
t
Rel
evan
t sta
ndar
ds a
gain
st w
hich
to m
onito
r pro
gres
s on
this
prio
rity
coul
d in
clud
e:
Chi
ld d
evel
opm
ent a
t 2 to
2.5
yea
rsSc
hool
read
ines
sFo
unda
tion
Stag
e Pr
ofile
s re
sults
Nar
row
ing
the
gap
in F
ound
atio
n St
age
profi
le re
sults
bet
wee
n de
priv
ed a
nd le
ss d
epriv
ed a
reas
Incr
ease
par
enta
l vo
ice
and
part
icip
atio
n in
ser
vice
dev
elop
men
tIn
crea
se a
cces
s to
ser
vice
s by
pr
ovid
ing
info
rmat
ion,
adv
ice
and
guid
ance
on
avai
labl
e se
rvic
esPr
ovid
e ea
rly s
uppo
rt to
par
ents
and
ca
rers
in ti
mes
of d
ifficu
ltyIm
prov
e re
latio
nshi
ps w
ith a
dult
serv
ices
Ensu
re s
taff
are
wel
l tra
ined
and
su
ppor
ted
to d
eliv
er s
ervi
ces
usin
g ev
iden
ce-b
ased
app
roac
hes
Ensu
re a
ll be
low
are
impl
emen
ted
parti
cula
rly w
here
de
priv
atio
n is
hig
h an
d Fo
unda
tion
Stag
e pr
ofile
resu
lts
are
low
:
l R
evie
w p
aren
t rep
rese
ntat
ion
on c
hild
ren’
s ce
ntre
ad
viso
ry b
oard
s an
d im
plem
ent a
ctio
n pl
an
l In
crea
se ta
ke u
p of
the
stat
utor
y 2
year
old
ear
ly
educ
atio
n en
title
men
t by
the
mos
t dis
adva
ntag
ed
child
ren
l Im
plem
ent t
he In
tegr
ated
Car
e Pa
thw
ay
l P
ilot a
team
aro
und
the
fam
ily m
odel
and
Fam
ily
Com
mon
Ass
essm
ent F
ram
ewor
k (C
AF)
l R
evie
w Y
oung
Car
ers
Partn
ersh
ip a
nd im
plem
ent
revi
sed
actio
n pl
an.
l N
utrit
ion
train
ing
to b
e ro
lled
out a
cros
s al
l chi
ldre
n’s
cent
res
Early
Chi
ldho
od
Serv
ices
/ Chi
ldre
n’s
Cen
tres;
Partn
ersh
ip a
cros
s C
hild
ren
Serv
ices
, sc
hool
s N
HS
and
Third
sec
tor;
Hea
lth V
isiti
ng
Impl
emen
tatio
n G
roup
:
Mid
wife
ry, H
ealth
Vi
sitin
g;
Fam
ilies
Firs
t Tea
m;
Chi
ldre
ns T
rust
Pa
rtner
s; W
omen
an
d In
fant
s N
utrit
ion
Gro
up
Chi
ldre
n’s
Trus
t (H
ealth
Impr
ovem
ent
Partn
ersh
ip)
Are
as fo
r Act
ion
Com
mitm
ents
Del
iver
y pa
rtne
rsO
vers
eein
g(a
nd s
uppo
rtin
g)
part
ners
hip

Hea
lth In
equa
litie
s A
ctio
n Pl
an
8
Pr
iorit
y 4:
Ens
ure
youn
g pe
ople
are
wel
l pre
pare
d fo
r adu
lthoo
d an
d w
ork,
with
a fo
cus
on
help
ing
child
ren
with
dis
abili
ties
to m
axim
ise
thei
r cap
abili
ties
Rel
evan
t sta
ndar
ds a
gain
st w
hich
to m
onito
r pro
gres
s on
this
prio
rity
coul
d in
clud
e:
Pupi
l abs
ence
Firs
t tim
e en
tran
ts to
the
yout
h ju
stic
e sy
stem
16-1
8 ye
ar o
lds
not i
n ed
ucat
ion,
em
ploy
men
t of t
rain
ing
Und
er 1
8 co
ncep
tion
Empl
oym
ent f
or th
ose
with
a lo
ng te
rm h
ealth
con
ditio
n, in
clud
ing
thos
e w
ith a
lear
ning
diffi
culty
/dis
abili
ty o
r men
tal i
llnes
sH
ospi
tal a
dmis
sion
s ca
used
by
unin
tent
iona
l and
del
iber
ate
inju
ries
in u
nder
18s
Emer
genc
y ad
mis
sion
s fo
r chi
ldre
n w
ith lo
wer
resp
irato
ry tr
act i
nfec
tion
Incr
ease
par
ticip
atio
n in
lear
ning
by
ensu
ring
oppo
rtun
ities
are
acc
essi
ble
to a
llEn
able
lear
ners
to w
ork
tow
ards
th
eir fi
rst f
ull L
evel
2 o
r Lev
el 3
qu
alifi
catio
n an
d im
prov
e th
eir l
ife,
care
er a
nd e
cono
mic
pro
spec
tsD
eliv
er h
igh
qual
ity le
arni
ng
oppo
rtun
ities
for y
oung
peo
ple,
th
roug
h co
ntin
uous
impr
ovem
ent
To h
elp
youn
g pe
ople
and
par
ents
/car
ers
to a
cces
s th
e rig
ht p
athw
ays
for l
earn
ing
and
inde
pend
ence
thro
ugh:
l A
pplic
atio
n of
new
fund
ing
stre
ams
l P
rovi
sion
of 3
Per
sona
l Adv
iser
s to
wor
k w
ith
youn
g pe
ople
, par
ents
and
sch
ools
to d
evel
op a
nd
impl
emen
t the
Edu
catio
n, H
ealth
and
Soc
ial C
are
Plan
s
Col
lege
s;
Spec
ial S
choo
ls;
Mai
nstre
am S
choo
ls;
Adul
t Ser
vice
s;Em
ploy
ers;
Educ
atio
n Fu
ndin
g Ag
ency
(EFA
).
Chi
ldre
n’s
Trus
t (S
trate
gic
Dis
abilit
y Pa
rtner
ship
; Lea
rnin
g D
isab
ility
Partn
ersh
ip;
Hea
lth Im
prov
emen
t Pa
rtner
ship
)
Are
as fo
r Act
ion
Com
mitm
ents
Del
iver
y pa
rtne
rsO
vers
eein
g(a
nd s
uppo
rtin
g)
part
ners
hip

Health Inequalities A
ction Plan
9
Pr
iorit
y 5:
Red
uce
child
hood
obe
sity
and
incr
ease
leve
ls o
f phy
sica
l act
ivity
and
hea
lthy
eatin
g in
chi
ldre
n an
d yo
ung
peop
le
Rel
evan
t sta
ndar
ds a
gain
st w
hich
to m
onito
r pro
gres
s on
this
prio
rity
coul
d in
clud
e:
Exce
ss w
eigh
t in
4-5
and
10-1
1 ye
ars
The
num
ber o
f chi
ldre
n liv
ing
in re
lativ
e po
vert
y
Enco
urag
e an
d su
ppor
t hea
lthy
grow
th a
nd w
eigh
t of c
hild
ren
Prom
ote
heal
thie
r foo
d ch
oice
s an
d im
prov
e th
e nu
triti
onal
qua
lity
of
food
in s
choo
lsIn
crea
se e
very
day
play
and
phy
sica
l ac
tivity
opp
ortu
nitie
s fo
r chi
ldre
n Pr
omot
e en
viro
nmen
ts a
nd
prac
tices
that
sup
port
chi
ldre
n to
ea
t hea
lthie
r foo
ds a
nd to
be
activ
e th
roug
hout
eac
h da
yPr
ovid
e pe
rson
alis
ed a
dvic
e an
d su
ppor
t for
chi
ldre
n an
d th
eir
fam
ilies
thro
ugh
a ch
ild h
ealth
y w
eigh
t pat
hway
Incr
ease
sup
port
and
trai
ning
for
educ
atio
n an
d ch
ildca
re s
taff
to
impl
emen
t hea
lth im
prov
emen
t ac
tivity
and
incr
ease
ava
ilabi
lity
and
acce
ssib
ility
of e
vide
nce
base
d ch
ildre
n’s
lifes
tyle
wei
ght
man
agem
ent s
ervi
ces
l T
o de
velo
p a
child
obe
sity
stra
tegy
and
im
plem
enta
tion
plan
for B
radf
ord
dist
rict b
y Ja
n 20
14l T
o ha
lt th
e in
crea
se o
f and
sta
rt se
eing
a y
ear
on y
ear r
educ
tion
in th
e pr
eval
ence
of o
besi
ty in
ch
ildre
n ag
ed 4
-5 y
ears
Brad
ford
Cou
ncil;
Brad
ford
Dis
trict
C
are
Trus
t;Th
ird S
ecto
r;C
linic
al
Com
mis
sion
ing
Gro
ups;
Scho
ols;
Chi
ldre
n’s
Cen
tres;
Hea
lth a
nd
Wel
lbei
ng T
eam
;Br
adfo
rd T
each
ing
Hos
pita
ls
Foun
datio
n Tr
ust.
Chi
ldre
n’s
Trus
t (H
ealth
Impr
ovem
ent
Partn
ersh
ip)
Are
as fo
r Act
ion
Com
mitm
ents
Del
iver
y pa
rtne
rsO
vers
eein
g(a
nd s
uppo
rtin
g)
part
ners
hip
Hea
lth In
equa
litie
s A
ctio
n Pl
an
10
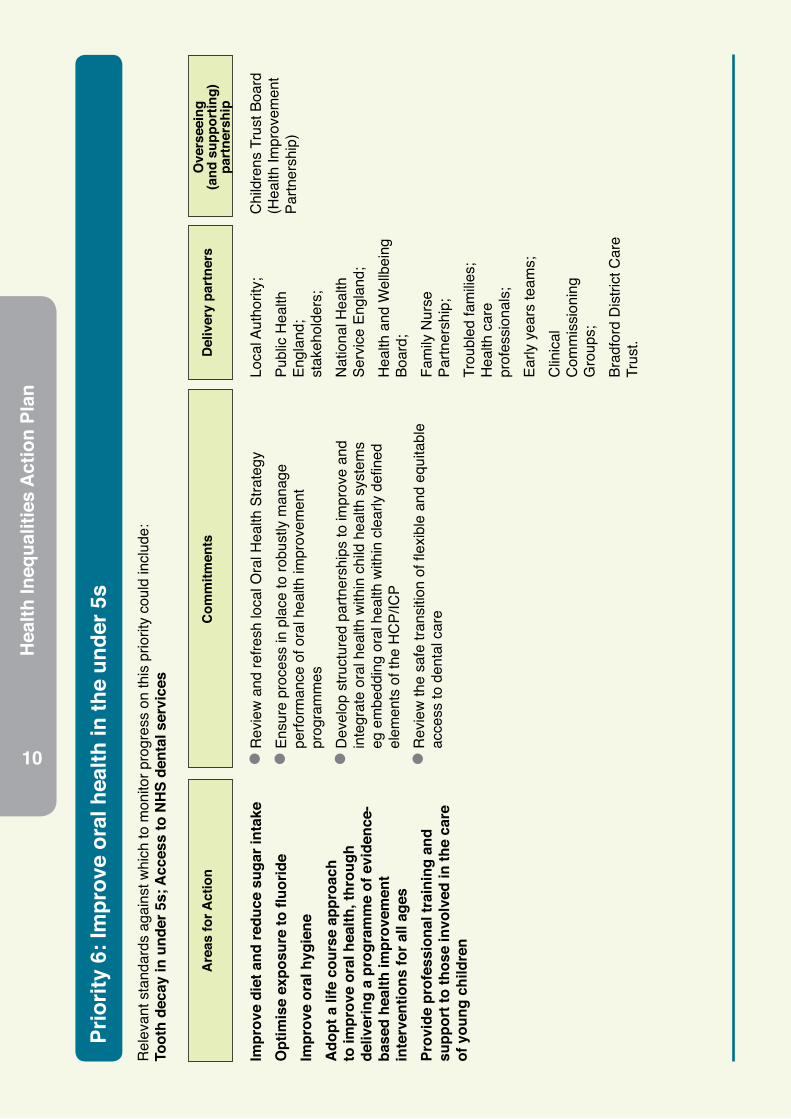
Pr
iorit
y 6:
Impr
ove
oral
hea
lth in
the
unde
r 5s
Rel
evan
t sta
ndar
ds a
gain
st w
hich
to m
onito
r pro
gres
s on
this
prio
rity
coul
d in
clud
e:
Toot
h de
cay
in u
nder
5s;
Acc
ess
to N
HS
dent
al s
ervi
ces
Impr
ove
diet
and
redu
ce s
ugar
inta
keO
ptim
ise
expo
sure
to fl
uorid
eIm
prov
e or
al h
ygie
neA
dopt
a li
fe c
ours
e ap
proa
ch
to im
prov
e or
al h
ealth
, thr
ough
de
liver
ing
a pr
ogra
mm
e of
evi
denc
e-ba
sed
heal
th im
prov
emen
t in
terv
entio
ns fo
r all
ages
Pr
ovid
e pr
ofes
sion
al tr
aini
ng a
nd
supp
ort t
o th
ose
invo
lved
in th
e ca
re
of y
oung
chi
ldre
n
l R
evie
w a
nd re
fresh
loca
l Ora
l Hea
lth S
trate
gy
l E
nsur
e pr
oces
s in
pla
ce to
robu
stly
man
age
perfo
rman
ce o
f ora
l hea
lth im
prov
emen
t pr
ogra
mm
es
l D
evel
op s
truct
ured
par
tner
ship
s to
impr
ove
and
inte
grat
e or
al h
ealth
with
in c
hild
hea
lth s
yste
ms
eg e
mbe
ddin
g or
al h
ealth
with
in c
lear
ly d
efine
d el
emen
ts o
f the
HC
P/IC
P
l R
evie
w th
e sa
fe tr
ansi
tion
of fl
exib
le a
nd e
quita
ble
acce
ss to
den
tal c
are
Loca
l Aut
horit
y;Pu
blic
Hea
lth
Engl
and;
st
akeh
olde
rs;
Nat
iona
l Hea
lth
Serv
ice
Engl
and;
H
ealth
and
Wel
lbei
ng
Boar
d;
Fam
ily N
urse
Pa
rtner
ship
; Tr
oubl
ed fa
milie
s;
Hea
lth c
are
prof
essi
onal
s;
Early
yea
rs te
ams;
C
linic
al
Com
mis
sion
ing
Gro
ups;
Brad
ford
Dis
trict
Car
e Tr
ust.
Chi
ldre
ns T
rust
Boa
rd
(Hea
lth Im
prov
emen
t Pa
rtner
ship
)
Are
as fo
r Act
ion
Com
mitm
ents
Del
iver
y pa
rtne
rsO
vers
eein
g(a
nd s
uppo
rtin
g)
part
ners
hip

Health Inequalities A
ction Plan
11
Pr
iorit
y 7:
Impr
ove
the
men
tal h
ealth
of p
eopl
e in
Bra
dfor
d D
istr
ict
Rel
evan
t sta
ndar
ds a
gain
st w
hich
to m
onito
r pro
gres
s on
this
prio
rity
coul
d in
clud
e:
Peop
le w
ith m
enta
l illn
ess
or d
isab
ility
in s
ettle
d ac
com
mod
atio
n; P
eopl
e in
pris
on w
ho h
ave
a m
enta
l illn
ess
or s
igni
fican
t men
tal i
llnes
s;
Hos
pita
l adm
issi
ons
as a
resu
lt of
sel
f har
m; E
xces
s un
der 7
5 m
orta
lity
in a
dults
with
ser
ious
men
tal i
llnes
s; S
uici
de; R
educ
ing
prem
atur
e de
aths
in p
eopl
e w
ith s
erio
us m
enta
l illn
ess;
Em
ploy
men
t of p
eopl
e w
ith m
enta
l illn
ess;
Pro
port
ion
of a
dults
in c
onta
ct w
ith s
econ
dary
men
tal
heal
th s
ervi
ces
who
live
inde
pend
ently
with
or w
ithou
t sup
port
; Em
otio
nal w
ellb
eing
of l
ooke
d af
ter c
hild
ren;
Pro
port
ion
of a
dults
in c
onta
ct
with
sec
onda
ry m
enta
l hea
lth s
ervc
es in
pai
d em
ploy
men
t; Pa
tient
exp
erie
nce
of c
omm
unity
men
tal h
ealth
ser
vice
s; D
omes
tic a
buse
Incr
ease
com
mun
ity b
ased
men
tal
heal
th c
are
Incl
ude
fam
ilies
and
car
ers
in h
elp
and
supp
ort
Supp
ort p
eopl
e w
ith m
enta
l ill
heal
th
to li
ve w
ell,
cope
with
ill h
ealth
and
no
t to
be le
ft ou
t of s
ocie
tyIm
prov
e ph
ysic
al h
ealth
of p
eopl
e w
ith m
enta
l illn
ess
Prov
ide
choi
ces
of g
ood
qual
ity c
are,
in
clud
ing
acce
ss to
psy
chol
ogic
al
ther
apie
sD
evel
op p
ublic
hea
lth m
enta
l hea
lth
and
suic
ide
prev
entio
n st
rate
gies
l L
ink
men
tal h
ealth
initi
ativ
es to
wid
er d
eter
min
ants
th
ereb
y ta
king
a h
olis
tic a
ppro
ach
whi
ch in
clud
es
fam
ily, e
nviro
nmen
t, co
mm
unity
, cul
ture
and
pov
erty
&
depr
ivat
ion.
l Im
prov
e ph
ysic
al h
ealth
of p
eopl
e w
ith m
enta
l ill
heal
th, a
ddre
ssin
g di
agno
stic
ove
rsha
dow
ing,
ac
cess
to p
sych
olog
ical
ther
apie
s an
d pr
imar
y ca
re.
Acce
ss to
men
tal h
ealth
bed
s an
d su
ppor
t fro
m
acut
e be
dsl Im
prov
e su
ppor
t for
peo
ple
expe
rienc
ing
diffi
culti
es
acce
ssin
g se
rvic
es d
ue to
bar
riers
link
ed to
age
, et
hnic
ity, d
isab
ility
and
lang
uage
l In
crea
se e
arly
inte
rven
tion,
impr
ove
acce
ss to
se
rvic
es in
clud
ing
thro
ugh
web
bas
ed a
pplic
atio
ns
Brad
ford
Dis
trict
C
are
Trus
t;Th
ird S
ecto
r;C
linic
al
Com
mis
sion
ing
Gro
ups;
Pros
perit
y an
d R
egen
erat
ion
Partn
ersh
ip;
Brad
ford
Cou
ncil;
Aire
dale
NH
S Fo
unda
tion
Trus
t;Br
adfo
rd T
each
ing
Hos
pita
ls F
ound
atio
n Tr
ust;
Wes
t Yor
kshi
re J
oint
Se
rvic
es.
Hea
lth Im
prov
emen
t Pa
rtner
ship
Are
as fo
r Act
ion
Com
mitm
ents
Del
iver
y pa
rtne
rsO
vers
eein
g(a
nd s
uppo
rtin
g)
part
ners
hip

Hea
lth In
equa
litie
s A
ctio
n Pl
an
12
Pr
iorit
y 8:
Impr
ove
heal
th a
nd w
ellb
eing
for p
eopl
e w
ith p
hysi
cal d
isab
ilitie
s, le
arni
ng d
isab
ilitie
s,
sens
ory
need
s an
d lo
ng te
rm c
ondi
tions
R
elev
ant s
tand
ards
aga
inst
whi
ch to
mon
itor p
rogr
ess
on th
is p
riorit
y co
uld
incl
ude:
R
educ
e pr
emat
ure
deat
h in
peo
ple
with
lear
ning
dis
abili
ties;
Hea
lth re
late
d qu
ality
of l
ife fo
r peo
ple
with
long
term
con
ditio
ns; P
ropo
rtio
n of
pe
ople
feel
ing
supp
orte
d to
man
age
thei
r con
ditio
n; E
mpl
oym
ent o
f peo
ple
with
long
-term
con
ditio
ns; U
npla
nned
hos
pita
lisat
ion
for c
hron
ic
ambu
lato
ry c
are
sens
itive
con
ditio
ns, a
sthm
a, d
iabe
tes
and
epile
psy
in u
nder
19s
and
adu
lts; H
ealth
-rel
ated
qua
lity
of li
fe fo
r car
er; P
eopl
e m
anag
e ow
n su
ppor
t as
muc
h as
they
wis
h, s
o ar
e in
con
trol
of w
hat,
how
and
whe
n su
ppor
t is
deliv
ered
to m
atch
thei
r nee
ds, P
ropo
rtio
n of
adu
lts w
ith le
arni
ng d
isab
ilitie
s w
ho li
ve in
thei
r ow
n ho
me
or w
ith th
eir f
amily
; Pro
port
ion
of a
dults
with
lear
ning
dis
abili
ties
in p
aid
empl
oym
ent;
Perm
anen
t adm
issi
ons
aged
18-
64 to
resi
dent
ial a
nd n
ursi
ng c
are
hom
es; E
xces
s un
der 6
0 m
orta
lity
rate
in a
dults
with
a le
arni
ng
disa
bilit
y
Supp
ort p
eopl
e w
ith d
isab
ilitie
s, lo
ng
term
illn
ess
and
sens
ory
need
s w
ith
empl
oym
ent,
skill
s an
d le
arni
ngD
evel
op in
tegr
ated
ser
vice
s fo
r m
anag
emen
t of l
ong-
term
con
ditio
nsIm
prov
e ho
usin
g, a
ssis
tive
tech
nolo
gy a
nd s
uppo
rt a
t hom
eEn
sure
info
rmat
ion
and
acce
ss to
se
rvic
es is
ava
ilabl
e fo
r all
Faci
litat
e tr
ansi
tions
from
chi
ld to
ad
ult s
ervi
ces
Dev
elop
spe
cial
ist s
ervi
ces
and
path
way
s fo
r reh
abili
tatio
n an
d ca
reEn
sure
Bra
dfor
d D
istr
ict b
enefi
ts
from
regi
onal
com
mis
sion
ing
for H
IV
& A
IDS
l M
ake
sure
dis
able
d pe
ople
hav
e en
ough
mon
ey to
m
ake
heal
thy
life
choi
ces
l S
uppo
rt D
isab
led
Peop
le to
hav
e op
portu
nitie
s to
de
velo
p sk
ills, t
o w
ork
and/
or d
o ac
tiviti
es th
at a
re
mea
ning
ful t
o th
eml D
evel
op h
ousi
ng, n
eigh
bour
hood
s an
d ac
cess
to
trans
port
that
giv
e di
sabl
ed p
eopl
e a
real
cho
ice
abou
t whe
re th
ey li
vel Im
prov
e ac
cess
to h
ealth
car
e by
–
Rai
sing
aw
aren
ess,
und
erst
andi
ng a
nd a
ctio
ns o
f H
ealth
Car
e Pr
ofes
sion
als
–
Giv
ing
peop
le k
now
ledg
e an
d vo
ice
to m
ake
info
rmed
cho
ices
and
dec
isio
ns
Brad
ford
Dis
trict
Car
e Tr
ust;
Third
Sec
tor;
Clin
ical
C
omm
issi
onin
g G
roup
s;Pr
ospe
rity
and
Reg
ener
atio
n Pa
rtner
ship
;Br
adfo
rd C
ounc
il;Ai
reda
le N
HS
Foun
datio
n Tr
ust;
Brad
ford
Tea
chin
g H
ospi
tals
Fou
ndat
ion
Trus
t;W
est Y
orks
hire
Joi
nt
Serv
ices
;H
ealth
Impr
ovem
ent
Partn
ersh
ip
Stra
tegi
c D
isab
ility
Partn
ersh
ipLe
arni
ng D
isab
ility
Partn
ersh
ip
Are
as fo
r Act
ion
Com
mitm
ents
Del
iver
y pa
rtne
rsO
vers
eein
g(a
nd s
uppo
rtin
g)
part
ners
hip

Health Inequalities A
ction Plan
13
Pr
iorit
y 9:
Impr
ove
diag
nosi
s, c
are
and
supp
ort f
or p
eopl
e w
ith d
emen
tia a
nd im
prov
e th
eir,
and
thei
r car
ers’
, qua
lity
of li
feR
elev
ant s
tand
ards
aga
inst
whi
ch to
mon
itor p
rogr
ess
on th
is p
riorit
y co
uld
incl
ude:
D
emen
tia a
nd it
s im
pact
s; E
nhan
cing
qua
lity
of li
fe fo
r car
er;,
Enha
ncin
g qu
ality
of l
ife fo
r peo
ple
with
dem
entia
; Car
er-r
epor
ted
qual
ity o
f life
; Pr
opor
tion
of c
arer
s w
ho re
port
that
they
hav
e be
en in
clud
ed o
r con
sulte
d in
dis
cuss
ion
abou
t the
per
son
they
car
e fo
r; O
vera
ll sa
tisfa
ctio
n of
peo
ple
who
use
ser
vice
s w
ith th
eir c
are
and
supp
ort;
Ove
rall
satis
fact
ion
of c
arer
s so
cial
ser
vice
s; E
stim
ated
dia
gnos
is ra
te fo
r peo
ple
with
de
men
tia
Are
as fo
r Act
ion
Com
mitm
ents
Del
iver
y pa
rtne
rsO
vers
eein
g(a
nd s
uppo
rtin
g)
part
ners
hip
Impr
ove
diag
nosi
s of
ear
ly a
nd la
te
onse
t dem
entia
Impr
ove
plan
ning
for d
emen
tia c
are
Impr
ove
early
inte
rven
tion
to s
uppo
rt
end
of li
fe p
lann
ing
Inte
grat
e he
alth
and
soc
ial c
are
to
prom
ote
inde
pend
ence
and
faci
litat
e co
mm
unity
bas
ed c
are
Impr
ove
acce
ss to
inte
rmed
iate
car
eR
educ
e us
e of
non
ther
apeu
tic a
nti-
psyc
hotic
med
icat
ion
l Im
prov
ed in
tegr
atio
n of
hea
lth a
nd s
ocia
l car
e re
sulti
ng in
coo
rdin
ated
ser
vice
s an
d in
form
atio
n sh
arin
gl St
anda
rdis
atio
n of
pro
visi
on a
cros
s th
e di
stric
t with
a
mor
e eq
uita
ble
serv
ice
for e
very
one
with
dem
entia
an
d th
eir c
arer
s.
l C
ompl
ete
the
Dem
entia
Hea
lth N
eeds
Ass
essm
ent,
ensu
ring
enga
gem
ent o
f mem
bers
and
that
the
findi
ngs
are
refle
cted
in th
e D
emen
tia S
trate
gy A
ctio
n Pl
an
l En
sure
that
the
maj
ority
of p
eopl
e w
ith d
emen
tia
are
diag
nose
d, a
nd th
at in
terv
entio
n is
ear
ly in
thei
r pa
thw
ay w
ithin
GP/
NH
S re
cord
s by
sta
ndar
disa
tion
of M
emor
y As
sess
men
t and
Tre
atm
ent S
ervi
ce
(MAT
S)
l Im
prov
e qu
ality
of c
are
in g
ener
al h
ospi
tals
and
car
e ho
mes
ens
urin
g pe
ople
with
dem
entia
rece
ive
the
high
est s
tand
ard
of c
are
and
that
ant
i psy
chot
ic
med
icat
ion
is u
sed
appr
opria
tely
and
mon
itore
dl Im
prov
ed p
ublic
and
pro
fess
iona
l aw
aren
ess
and
unde
rsta
ndin
g of
dem
entia
and
ser
vice
s av
aila
ble.
l R
educ
e th
e st
igm
a as
soci
ated
with
dem
entia
in a
ll co
mm
uniti
es in
clud
ing
Blac
k an
d M
inor
ity E
thni
c (B
ME)
com
mun
ities
Dem
entia
Stra
tegy
G
roup
– P
artn
ers
incl
ude
Brad
ford
C
ounc
il; B
radf
ord
Dis
trict
Car
e Tr
ust;
repr
esen
tativ
es fr
om
the
Dis
trict
’s C
CG
s;
repr
esen
tativ
es
from
the
Dis
trict
’s Ac
ute
trust
s;
repr
esen
tativ
es o
f Th
ird s
ecto
r gro
ups
incl
udin
g Th
e Al
zhei
mer
’s So
ciet
y, M
eri Y
arda
in, K
IVC
A an
d Po
sitiv
e M
inds
.
Olde
r Peo
ple’s
Partn
ersh
ip
Brad
ford
Dis
trict
Car
e Tr
ust;
Third
Sec
tor;
Clin
ical
C
omm
issi
onin
g G
roup
s;Pr
ospe
rity
and
Reg
ener
atio
n Pa
rtner
ship
;Br
adfo
rd C
ounc
il;Ai
reda
le N
HS
Foun
datio
n Tr
ust;
Brad
ford
Tea
chin
g H
ospi
tals
Fou
ndat
ion
Trus
t;W
est Y
orks
hire
Joi
nt
Serv
ices
;H
ealth
Impr
ovem
ent
Partn
ersh
ip

Hea
lth In
equa
litie
s A
ctio
n Pl
an
14
Pr
iorit
y 10
: Pro
mot
e th
e in
depe
nden
ce a
nd w
ellb
eing
of o
lder
peo
ple
Rel
evan
t sta
ndar
ds a
gain
st w
hich
to m
onito
r pro
gres
s on
this
prio
rity
coul
d in
clud
e:
Falls
and
inju
ries
in th
e ov
er 6
5s: H
ealth
rela
ted
qual
ity o
f life
for o
lder
peo
ple;
Hip
frac
ture
s in
ove
r 65s
; Im
prov
ing
reco
very
from
inju
ries
and
trau
ma;
Impr
ovin
g re
cove
ry fr
om fr
agili
ty fr
actu
res;
Hel
ping
old
er p
eopl
e to
reco
ver t
heir
inde
pend
ence
afte
r illn
ess
or in
jury
; Pro
port
ion
of
peop
le w
ho u
se s
ocia
l ser
vice
s w
ho h
ave
cont
rol o
ver t
heir
daily
life
; Pro
port
ion
of p
eopl
e us
ing
soci
al c
are
who
rece
ive
self-
dire
cted
sup
port
an
d th
ose
rece
ivin
g di
rect
pay
men
ts; P
erm
anen
t adm
issi
ons
ages
65+
to re
side
ntia
l and
nur
sing
car
e ho
mes
; Pr
opor
tion
of o
lder
peo
ple
(65
and
over
) who
wer
e st
ill a
t hom
e 91
day
s af
ter d
isch
arge
from
hos
pita
l int
o re
able
men
t/reh
abili
tatio
n se
rvic
es; P
ropo
rtio
n of
old
er p
eopl
e (6
5+)
disc
harg
ed fr
om h
ospi
tal w
ith th
e cl
ear i
nten
tion
that
they
will
mov
e on
/bac
k to
thei
r ow
n ho
me
out o
f tho
se d
isch
arge
d fr
om h
ospi
tal;
Aver
age
num
ber o
f del
ayed
tran
sers
of c
are
attr
ibut
able
to s
ocia
l car
e; B
erea
ved
care
rs’ v
iew
s on
qua
lity
of c
are
in th
e la
st 3
mon
ths
of li
fe
Prom
ote
pers
onal
isat
ion
and
enha
nce
qual
ity o
f life
for p
eopl
e w
ith lo
ng-te
rm
cond
ition
s ca
re a
nd s
uppo
rt n
eeds
Hel
p pe
ople
to re
cove
r fro
m e
piso
des
of il
l hea
lth o
r fol
low
ing
inju
ry,
prev
entin
g de
terio
ratio
n, d
elay
ing
depe
nden
cy a
nd s
uppo
rtin
g re
cove
rySu
ppor
t peo
ple
to m
axim
ise
thei
r in
com
es th
roug
h go
od w
elfa
re
bene
fits
advi
ce, e
duca
tion
and
trai
ning
an
d su
ppor
t to
stay
or r
etur
n to
em
ploy
men
tEn
sure
a p
ositi
ve e
xper
ienc
e of
car
e an
d su
ppor
t; tr
eatin
g an
d ca
ring
for
peop
le in
a s
afe
envi
ronm
ent a
nd
prot
ectin
g pe
ople
from
avo
idab
le h
arm
Ensu
re p
eopl
e ex
perie
nce
serv
ices
that
su
ppor
t the
m to
enj
oy a
goo
d qu
ality
of
life
l C
ontin
ue to
dev
elop
pre
vent
ativ
e an
d ea
rly
inte
rven
tion
appr
oach
es, i
nclu
ding
sel
f car
e, to
redu
ce
heal
th in
equa
litie
s ex
perie
nced
by
olde
r peo
ple
and
ensu
re th
at s
uppo
rt is
focu
sed
on th
e ar
eas
with
mos
t ne
ed.
l W
iden
the
offe
r of i
nnov
ativ
e ap
proa
ches
to
mai
ntai
ning
inde
pend
ence
of o
lder
peo
ple.
Thi
s w
ill in
clud
e th
e de
velo
pmen
t of l
ocal
‘sup
port
hubs
’ and
he
alth
and
wel
lbei
ng c
ham
pion
s to
incr
ease
affo
rdab
le
care
cho
ices
for p
eopl
e liv
ing
on lo
w in
com
es.
l S
uppo
rt pl
anni
ng fo
r ret
irem
ent f
or o
ver 5
0s to
ena
ble
a sm
ooth
tran
sitio
n fro
m e
mpl
oym
ent,
so th
at p
eopl
e ca
n en
joy
wel
lbei
ng in
retir
emen
t. Th
ere
will
be a
fo
cus
on p
eopl
e in
low
pai
d em
ploy
men
t.
l P
rom
ote
inte
rgen
erat
iona
l app
roac
hes
to b
ring
com
mun
ities
toge
ther
to in
crea
se s
ocia
l int
erac
tion
betw
een
peop
le w
here
ther
e ar
e hi
gh le
vels
of
isol
atio
n.
l D
eliv
er th
e G
reat
Pla
ces
to G
row
Old
Pro
gram
me
ensu
ring
a w
ide
rang
e of
hou
sing
opt
ions
are
of
fere
d an
d m
ade
avai
labl
e w
hich
resu
lts in
gre
ater
in
depe
nden
ce fo
r old
er p
eopl
e.
Old
er P
eopl
es
Partn
ersh
ip P
riorit
y 10
gro
up N
HS;
th
ird s
ecto
r; Lo
cal
Auth
ority
; CC
Gs;
So
cial
Hou
sing
Pr
ovid
ers
Old
er P
eopl
e’s
Partn
ersh
ip
Are
as fo
r Act
ion
Com
mitm
ents
Del
iver
y pa
rtne
rsO
vers
eein
g(a
nd s
uppo
rtin
g)
part
ners
hip

Health Inequalities A
ction Plan
15l C
ontin
ue to
dev
elop
pre
vent
ativ
e an
d ea
rly
inte
rven
tion
appr
oach
es, i
nclu
ding
sel
f car
e, to
redu
ce
heal
th in
equa
litie
s ex
perie
nced
by
olde
r peo
ple
and
ensu
re th
at s
uppo
rt is
focu
sed
on th
e ar
eas
with
mos
t ne
ed.
l W
iden
the
offe
r of i
nnov
ativ
e ap
proa
ches
to
mai
ntai
ning
inde
pend
ence
of o
lder
peo
ple.
Thi
s w
ill in
clud
e th
e de
velo
pmen
t of l
ocal
‘sup
port
hubs
’ and
he
alth
and
wel
lbei
ng c
ham
pion
s to
incr
ease
affo
rdab
le
care
cho
ices
for p
eopl
e liv
ing
on lo
w in
com
es.
l S
uppo
rt pl
anni
ng fo
r ret
irem
ent f
or o
ver 5
0s to
ena
ble
a sm
ooth
tran
sitio
n fro
m e
mpl
oym
ent,
so th
at p
eopl
e ca
n en
joy
wel
lbei
ng in
retir
emen
t. Th
ere
will
be a
fo
cus
on p
eopl
e in
low
pai
d em
ploy
men
t.
l P
rom
ote
inte
rgen
erat
iona
l app
roac
hes
to b
ring
com
mun
ities
toge
ther
to in
crea
se s
ocia
l int
erac
tion
betw
een
peop
le w
here
ther
e ar
e hi
gh le
vels
of
isol
atio
n.
l D
eliv
er th
e G
reat
Pla
ces
to G
row
Old
Pro
gram
me
ensu
ring
a w
ide
rang
e of
hou
sing
opt
ions
are
of
fere
d an
d m
ade
avai
labl
e w
hich
resu
lts in
gre
ater
in
depe
nden
ce fo
r old
er p
eopl
e.
Old
er P
eopl
es
Partn
ersh
ip P
riorit
y 10
gro
up N
HS;
th
ird s
ecto
r; Lo
cal
Auth
ority
; CC
Gs;
So
cial
Hou
sing
Pr
ovid
ers
Pr
iorit
y 11
: Inc
reas
e em
ploy
men
t opp
ortu
nitie
s an
d tr
aini
ng
Rel
evan
t sta
ndar
ds a
gain
st w
hich
to m
onito
r pro
gres
s on
this
prio
rity
coul
d in
clud
e:
Empl
oym
ent f
or th
ose
with
long
term
hea
lth c
ondi
tion
incl
udin
g th
ose
with
a le
arni
ng d
ifficu
lty/d
isab
ility
or m
enta
l illn
ess;
Peo
ple
are
able
to
find
empl
oym
ent w
hen
they
wan
t, m
aint
ain
a fa
mily
and
soc
ial l
ife a
nd c
ontr
ibut
e to
com
mun
ity li
fe, a
nd a
void
lone
lines
s or
isol
atio
n
Incr
ease
the
num
ber o
f bus
ines
s st
art-u
psIn
crea
se s
ocia
l ent
erpr
ise
grow
thC
reat
e m
ore
appr
entic
eshi
psR
etai
n gr
adua
tes
in g
reat
er n
umbe
rsD
evel
op a
sin
gle
gate
way
for
empl
oyer
sIn
crea
se th
e nu
mbe
r of l
earn
ers
acce
ssin
g pr
e-en
try
ESO
L (E
nglis
h fo
r Spe
aker
s O
ther
Lan
guag
es)
Incr
ease
acc
ess
to b
asic
lite
racy
/nu
mer
acy
cour
ses
Pr
omot
e gr
owth
of e
xist
ing
smal
l and
m
ediu
m e
nter
pris
esPr
omot
e op
port
uniti
es fo
r dis
able
d pe
ople
and
peo
ple
with
wor
k lim
iting
ill
ness
to g
ain
and
reta
in e
mpl
oym
ent
l P
rovi
de e
ffect
ive
empl
oym
ent a
nd tr
aini
ng ro
utes
ou
t of p
over
ty a
nd o
ther
life
circ
umst
ance
s lik
ely
to
get i
n th
e w
ay o
f pos
itive
hea
lth o
utco
mes
l S
uppo
rt so
cial
ent
erpr
ise
grow
th in
clud
ing
invo
lvem
ent o
f the
third
sec
tor i
n se
rvic
e pl
anni
ng
and
deliv
ery
l S
uppo
rt pe
ople
to s
et u
p in
bus
ines
s l P
rom
ote
grea
ter u
ptak
e of
app
rent
ices
hips
by
empl
oyer
sl In
crea
se th
e nu
mbe
r of l
earn
ers
acce
ssin
g pr
e-en
try
ESO
L (E
nglis
h fo
r Spe
aker
s O
ther
Lan
guag
es)
l In
crea
se a
cces
s to
bas
ic li
tera
cy/n
umer
acy
cour
ses
l P
rom
ote
oppo
rtuni
ties
for d
isab
led
peop
le a
nd
peop
le w
ith w
ork
limiti
ng il
lnes
s to
gai
n an
d st
ay in
em
ploy
men
t
Pros
perit
y an
d R
egen
erat
ion
Partn
ersh
ip,
Empl
oym
ent a
nd
Skills
Boa
rd, B
radf
ord
Brea
kthr
ough
and
Get
Br
adfo
rd W
orki
ng
Pros
perit
y an
d R
egen
erat
ion
Partn
ersh
ip
(Em
ploy
men
t an
d Sk
ills
Boar
d, B
radf
ord
Brea
kthr
ough
, Get
Br
adfo
rd W
orki
ng
Are
as fo
r Act
ion
Com
mitm
ents
Del
iver
y pa
rtne
rsO
vers
eein
g(a
nd s
uppo
rtin
g)
part
ners
hip

Hea
lth In
equa
litie
s A
ctio
n Pl
an
16
Pr
iorit
y 12
: Pro
mot
e he
alth
ier l
ifest
yles
in th
e w
orkp
lace
Rel
evan
t sta
ndar
ds a
gain
st w
hich
to m
onito
r pro
gres
s on
this
prio
rity
coul
d in
clud
e:
Sick
ness
abs
ence
rate
Impr
ove
occu
patio
nal h
ealth
and
sa
fety
in w
orkp
lace
sPr
omot
e he
alth
y w
ork
styl
es in
the
wor
k pl
ace
Enco
urag
e an
d su
ppor
t em
ploy
ees
to a
dopt
hea
lthie
r life
styl
es
l Im
prov
e oc
cupa
tiona
l hea
lth a
nd s
afet
y pr
actic
e in
w
orkp
lace
sl P
rom
ote
awar
enes
s of
hea
lth is
sues
wor
kpla
ces
l P
rom
ote
heal
thy
wor
k st
yles
in w
orkp
lace
s l E
ncou
rage
and
sup
port
empl
oyee
s to
ado
pt h
ealth
ier
lifes
tyle
s
Pros
perit
y an
d R
egen
erat
ion
Partn
ersh
ip,
Empl
oym
ent
and
Skills
Bo
ard,
Bra
dfor
d Br
eakt
hrou
gh
and
Get
Bra
dfor
d W
orki
ng, B
radf
ord
Cha
mbe
r
Pros
perit
y and
Re
gene
ratio
n Pa
rtner
ship
(Em
ploym
ent a
nd
Skills
Boa
rd, B
radf
ord
Brea
kthro
ugh,
Bra
dfor
d Ch
ambe
r)
Are
as fo
r Act
ion
Com
mitm
ents
Del
iver
y pa
rtne
rsO
vers
eein
g(a
nd s
uppo
rtin
g)
part
ners
hip
Health Inequalities A
ction Plan
17
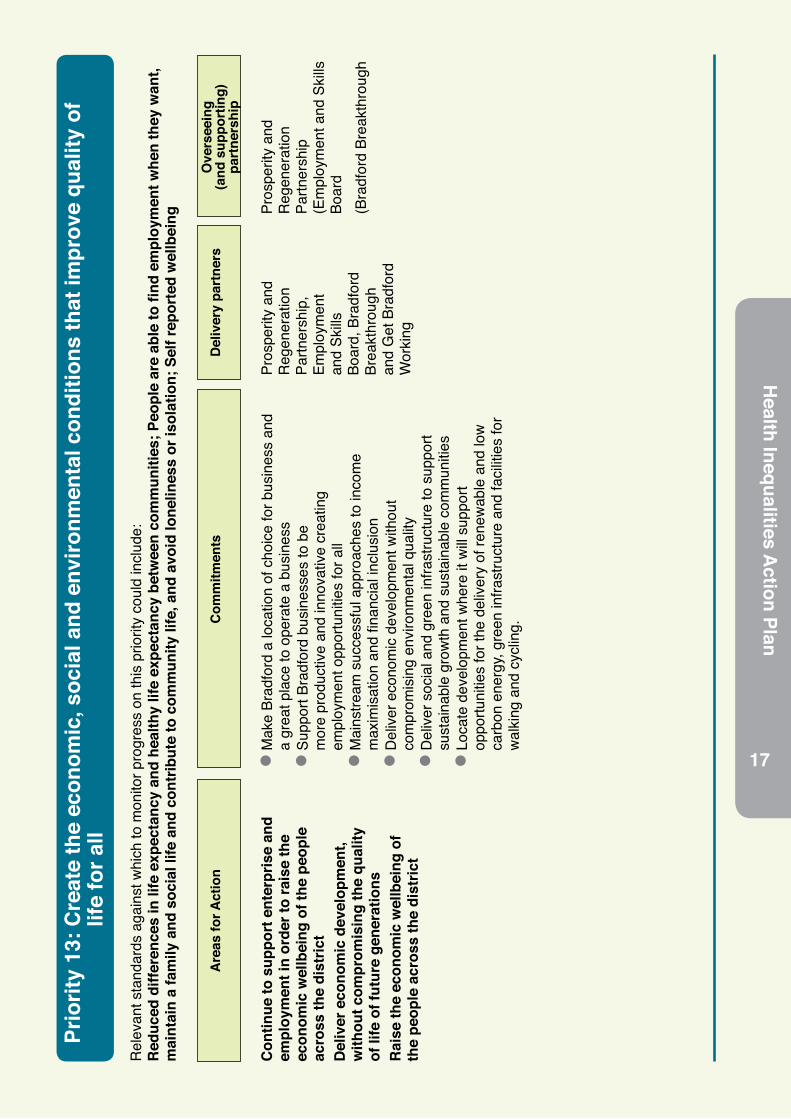
Pr
iorit
y 13
: Cre
ate
the
econ
omic
, soc
ial a
nd e
nviro
nmen
tal c
ondi
tions
that
impr
ove
qual
ity o
f lif
e fo
r all
Rel
evan
t sta
ndar
ds a
gain
st w
hich
to m
onito
r pro
gres
s on
this
prio
rity
coul
d in
clud
e:
Red
uced
diff
eren
ces
in li
fe e
xpec
tanc
y an
d he
alth
y lif
e ex
pect
ancy
bet
wee
n co
mm
uniti
es; P
eopl
e ar
e ab
le to
find
em
ploy
men
t whe
n th
ey w
ant,
mai
ntai
n a
fam
ily a
nd s
ocia
l life
and
con
trib
ute
to c
omm
unity
life
, and
avo
id lo
nelin
ess
or is
olat
ion;
Sel
f rep
orte
d w
ellb
eing
Con
tinue
to s
uppo
rt e
nter
pris
e an
d em
ploy
men
t in
orde
r to
rais
e th
e ec
onom
ic w
ellb
eing
of t
he p
eopl
e ac
ross
the
dist
rict
Del
iver
eco
nom
ic d
evel
opm
ent,
with
out c
ompr
omis
ing
the
qual
ity
of li
fe o
f fut
ure
gene
ratio
nsR
aise
the
econ
omic
wel
lbei
ng o
f th
e pe
ople
acr
oss
the
dist
rict
l M
ake
Brad
ford
a lo
catio
n of
cho
ice
for b
usin
ess
and
a gr
eat p
lace
to o
pera
te a
bus
ines
sl S
uppo
rt Br
adfo
rd b
usin
esse
s to
be
mor
e pr
oduc
tive
and
inno
vativ
e cr
eatin
g em
ploy
men
t opp
ortu
nitie
s fo
r all
l M
ains
tream
suc
cess
ful a
ppro
ache
s to
inco
me
max
imis
atio
n an
d fin
anci
al in
clus
ion
l D
eliv
er e
cono
mic
dev
elop
men
t with
out
com
prom
isin
g en
viro
nmen
tal q
ualit
yl D
eliv
er s
ocia
l and
gre
en in
frast
ruct
ure
to s
uppo
rt su
stai
nabl
e gr
owth
and
sus
tain
able
com
mun
ities
l L
ocat
e de
velo
pmen
t whe
re it
will
supp
ort
oppo
rtuni
ties
for t
he d
eliv
ery
of re
new
able
and
low
ca
rbon
ene
rgy,
gree
n in
frast
ruct
ure
and
faci
litie
s fo
r w
alki
ng a
nd c
yclin
g.
Pros
perit
y an
d R
egen
erat
ion
Partn
ersh
ip,
Empl
oym
ent
and
Skills
Bo
ard,
Bra
dfor
d Br
eakt
hrou
gh
and
Get
Bra
dfor
d W
orki
ng
Pros
perit
y an
d R
egen
erat
ion
Partn
ersh
ip
(Em
ploy
men
t and
Ski
lls
Boar
d (B
radf
ord
Brea
kthr
ough
Are
as fo
r Act
ion
Com
mitm
ents
Del
iver
y pa
rtne
rsO
vers
eein
g(a
nd s
uppo
rtin
g)
part
ners
hip
Hea
lth In
equa
litie
s A
ctio
n Pl
an
18
Pr
iorit
y 14
: Del
iver
a h
ealth
ier a
nd s
afer
env
ironm
ent
Rel
evan
t sta
ndar
ds a
gain
st w
hich
to m
onito
r pro
gres
s on
this
prio
rity
coul
d in
clud
e:
Kill
ed o
r inj
ured
on
Engl
and’
s ro
ads;
Vio
lent
crim
e; R
e-of
fend
ing;
Use
of g
reen
spa
ce fo
r exe
rcis
e / h
ealth
reas
ons;
Sel
f rep
orte
d w
ellb
eing
; Pu
blic
sec
tor o
rgan
isat
ions
sus
tain
able
man
agem
ent p
lans
; Pro
port
ion
of p
eopl
e w
ho u
se s
ervi
ces
who
feel
saf
e
Cre
ate
a gr
eene
r, cl
eane
r and
mor
e su
stai
nabl
e en
viro
nmen
t whi
ch
mak
es b
est u
se o
f our
reso
urce
s an
d po
sitiv
ely
affe
cts
clim
ate
chan
geSu
ppor
t peo
ple
from
diff
eren
t ba
ckgr
ound
s to
get
on
wel
l to
geth
erH
elp
ever
yone
to fe
el s
ecur
e an
d at
eas
e, in
clud
ing
exte
ndin
g co
mm
unity
invo
lvem
ent i
n ta
cklin
g cr
ime
and
in s
tren
gthe
ning
co
mm
uniti
es
l C
o-or
dina
te a
ctio
n to
redu
ce th
e nu
mbe
r of p
eopl
e w
ho a
re k
illed
or s
erio
usly
inju
red
on th
e ro
ads
with
a
parti
cula
r foc
us o
n ar
eas
whe
re h
ighe
r rat
es o
f ac
cide
nts
occu
r l C
o-or
dina
te a
ctio
n to
redu
ce th
e le
vels
of v
iole
nt
crim
e l C
o-or
dina
te a
ctio
n to
redu
ce re
-offe
ndin
gl C
o-or
dina
te a
ctio
n to
redu
ce il
licit
and
othe
r ha
rmfu
l sub
stan
ce u
se, i
ncre
ase
the
num
bers
of
indi
vidu
als
reco
verin
g fro
m d
epen
denc
e/m
aint
aini
ng a
bstin
ence
, and
bui
ld re
cove
ry c
apita
l in
com
mun
ities
Safe
r Roa
ds S
teer
ing
Gro
up;
Wes
t Yor
kshi
re P
olic
e;W
est Y
orks
hire
Pr
obat
ion
Trus
t;Br
adfo
rd C
ounc
il - P
ublic
Hea
lth
Dep
artm
ent;
Third
Sec
tor
orga
nisa
tions
Com
mun
ity S
afet
y Pa
rtner
ship
Are
as fo
r Act
ion
Com
mitm
ents
Del
iver
y pa
rtne
rsO
vers
eein
g(a
nd s
uppo
rtin
g)
part
ners
hip

Health Inequalities A
ction Plan
19
Pr
iorit
y 15
: Inc
reas
e th
e nu
mbe
r of d
ecen
t hom
es a
nd e
nsur
e af
ford
able
war
mth
Rel
evan
t sta
ndar
ds a
gain
st w
hich
to m
onito
r pro
gres
s on
this
prio
rity
coul
d in
clud
e:
Fuel
pov
erty
Exce
ss w
inte
r dea
ths
Perc
enta
ge o
f pop
ulat
ion
affe
cted
by
nois
eSt
atut
ory
hom
eles
snes
sA
ir po
llutio
n
Bui
ld m
ore
hom
es th
at a
re a
fford
able
Red
uce
disr
epai
r and
hea
lth h
azar
ds
in o
lder
priv
ate
hous
ing
likel
y to
be
occu
pied
by
vuln
erab
le p
eopl
e Im
prov
e en
ergy
effi
cien
cy a
nd e
co
stan
dard
sLo
cal a
utho
rity
hous
ing
serv
ice
to
prov
ide
high
qua
lity
serv
ices
Im
prov
e ac
cess
and
ser
vice
s to
vul
nera
ble
peop
le, p
roce
ss
appl
icat
ions
mor
e qu
ickl
y, im
prov
e ch
oice
, and
redu
ce a
nd p
reve
nt
hom
eles
snes
s Im
prov
e th
e de
sign
, qua
lity
and
supp
ly o
f hou
sing
in th
e di
stric
t to
bette
r mee
t the
nee
ds o
f old
er a
nd
vuln
erab
le p
eopl
e
l E
nabl
e an
d su
ppor
t the
del
iver
y of
mor
e ne
w
hom
es, i
n pa
rticu
lar h
ousi
ng w
hich
is a
fford
able
to
acce
ss a
nd m
aint
ain,
bui
lt to
hig
h en
ergy
effi
cien
cy
stan
dard
s.
l Im
prov
e th
e qu
ality
of e
xist
ing
hous
ing
thro
ugh
a co
mpr
ehen
sive
pro
gram
me
of h
ousi
ng s
tand
ards
ad
vice
, sup
port,
equ
ity lo
ans
and
enfo
rcem
ent.
l S
uppo
rt im
plem
enta
tion
of G
reen
Dea
l mea
sure
s to
hom
es a
cros
s th
e di
stric
t; up
date
Fue
l Pov
erty
ac
tion
plan
; tac
kle
exce
ss w
inte
r dea
ths
l Im
plem
ent m
ajor
cha
nge
prog
ram
me
to
hom
eles
snes
s pr
even
tion
and
asse
ssm
ent s
ervi
ces,
im
prov
e pr
ovis
ion
of te
mpo
rary
acc
omm
odat
ion.
Brad
ford
Cou
ncil
regi
ster
ed p
rovi
ders
; ho
usin
g de
velo
pers
;Pr
ivat
e la
ndlo
rds;
ow
ner o
ccup
iers
; ot
her p
ublic
sec
tor
partn
ers;
Hom
eles
snes
s se
rvic
e pr
ovid
ers;
ot
her p
ublic
sec
tor
partn
ers.
Hou
sing
Par
tner
ship
Are
as fo
r Act
ion
Com
mitm
ents
Del
iver
y pa
rtne
rsO
vers
eein
g(a
nd s
uppo
rtin
g)
part
ners
hip
Hea
lth In
equa
litie
s A
ctio
n Pl
an
20
Pr
iorit
y 16
: Enh
ance
soc
ial c
apita
l and
act
ive
citiz
ensh
ip
Rel
evan
t sta
ndar
ds a
gain
st w
hich
to m
onito
r pro
gres
s on
this
prio
rity
coul
d in
clud
e:
Soci
al c
onne
cted
ness
; Old
er p
eopl
e’s
perc
eptio
n of
com
mun
ity s
afet
y
Deve
lop
effe
ctiv
e wa
ys fo
r all
partn
ers
and
partn
ersh
ips
to in
volv
e co
mm
uniti
es, g
roup
s an
d in
divi
dual
s in
th
eir p
lans
and
wor
kSu
ppor
t com
mun
ities
thro
ugho
ut th
e Di
stric
t to
do th
ings
for t
hem
selv
esIn
crea
se o
ppor
tuni
ties
for a
ctiv
e ci
tizen
in
volv
emen
t in
the
Dist
rict
Enco
urag
e pe
ople
from
diff
eren
t ba
ckgr
ound
s to
get
on
well
toge
ther
Crea
te o
ppor
tuni
ties
for i
ndiv
idua
ls,
grou
ps a
nd o
rgan
isat
ions
to g
et to
geth
er
to d
iscu
ss th
eir c
ircum
stan
ces,
nee
ds
and
aspi
ratio
ns, w
ithin
and
bet
ween
co
mm
uniti
es a
nd n
eigh
bour
hood
s
l T
hrou
gh W
ard
and
Equa
lity A
sses
smen
ts m
ap w
here
we
hav
e hig
h an
d low
leve
ls of
socia
l cap
ital a
nd a
ctive
cit
izens
.
l T
hrou
gh W
ard
and
Equa
lity A
sses
smen
ts ide
ntify
Are
as
and
com
mun
ities o
f inte
rests
with
spec
ific h
ealth
and
we
llbein
g ne
eds w
here
enh
ancin
g so
cial c
apita
l cou
ld m
ake
a sig
nifica
nt co
ntrib
ution
l T
hrou
gh W
ard
and
Equa
lity P
lans d
evelo
p an
d co
ordin
ate
com
mun
ity in
itiativ
es th
at su
ppor
t com
mun
ities t
o do
thing
s for
them
selve
s and
eng
age
com
mun
ities
appr
opria
tely
l W
ork w
ith H
ealth
and
Well
being
par
tner
s to
help
deve
lop
supp
ort n
etwo
rks a
nd se
lf help
gro
ups
l E
nsur
e th
ere
is br
oker
age
betw
een
peop
le wa
nting
to
volun
teer
and
org
anisa
tions
seek
ing vo
lunte
ers
Brad
ford
Cou
ncil;
Third
Sec
tor;
NH
S
Stro
nger
Com
mun
ities
Pa
rtner
ship
(Hea
lth Im
prov
emen
t Pa
rtner
ship
Are
as fo
r Act
ion
Com
mitm
ents
Del
iver
y pa
rtne
rsO
vers
eein
g(a
nd s
uppo
rtin
g)
part
ners
hip

Health Inequalities A
ction Plan
21
Pr
iorit
y 17
: Red
uce
harm
from
pre
vent
able
dis
ease
cau
sed
by to
bacc
o, o
besi
ty, a
lcoh
ol a
nd
subs
tanc
e ab
use
Rel
evan
t sta
ndar
ds a
gain
st w
hich
to m
onito
r pro
gres
s on
this
prio
rity
coul
d in
clud
e:
Smok
ing
prev
alen
ce –
15
year
old
s; D
iet;
Exce
ss w
eigh
t in
adul
ts; P
ropo
rtio
n of
phy
sica
lly a
ctiv
e an
d in
activ
e ad
ults
; Sm
okin
g pr
eval
ence
–
adul
ts; S
ucce
ssfu
l com
plet
ion
of d
rug
trea
tmen
t; Pe
ople
ent
erin
g pr
ison
with
sub
stan
ce d
epen
denc
e no
t pre
viou
sly
know
n to
com
mun
ity
trea
tmen
t
Wor
k w
ith p
artn
ers
to p
rom
ote
an
envi
ronm
ent a
nd c
ultu
re th
at m
akes
he
alth
y lif
esty
les
easi
er to
ach
ieve
Dev
elop
tier
ed m
odel
of i
nter
vent
ions
so
the
mos
t effe
ctiv
e in
terv
entio
ns
get t
o th
e rig
ht p
eopl
e at
the
right
tim
eC
omm
issi
on s
peci
alis
t ser
vice
s fo
r th
ose
in g
reat
est n
eed
Prov
ide
brie
f int
erve
ntio
ns a
nd
refe
rral
s to
effe
ctiv
e pr
even
tativ
e se
rvic
es, u
sing
the
prin
cipl
es o
f ‘M
akin
g Ev
ery
Con
tact
Cou
nt’
Incr
ease
acc
ess
to ta
rget
ed h
ealth
ch
ecks
l A
ddre
ss a
cces
s to
low
pric
ed to
bacc
o an
d al
coho
l th
roug
h en
forc
emen
t l R
ecog
nise
the
impo
rtanc
e of
saf
e pl
aces
to ta
ke
part
in p
hysi
cal a
ctiv
ity, w
heth
er th
at b
e w
alki
ng
or c
yclin
g ro
utes
, com
mun
ity c
entre
s or
hea
lth
faci
litie
s an
d im
prov
e ac
cess
ibilit
y in
a p
hysi
cal a
nd
mon
etar
y se
nse
to e
nsur
e av
aila
ble
to th
e w
ider
co
mm
unity
l A
ddre
ss o
besi
ty a
s a
fam
ily is
sue
of m
alno
uris
hmen
t lin
ked
to p
over
ty a
nd d
epriv
atio
nl A
ddre
ss a
cces
s to
low
pric
ed p
oor q
ualit
y fo
od a
nd
take
away
s
Brad
ford
Dis
trict
C
are
Trus
t;Th
ird S
ecto
r;C
linic
al
Com
mis
sion
ing
Gro
ups;
Pros
perit
y an
d R
egen
erat
ion
Partn
ersh
ip;
Brad
ford
Cou
ncil;
Aire
dale
NH
S Fo
unda
tion
Trus
t;Br
adfo
rd T
each
ing
Hos
pita
ls
Foun
datio
n Tr
ust;
Wes
t Yor
kshi
re J
oint
Se
rvic
es
Hea
lth Im
prov
emen
t Pa
rtner
ship
l T
hrou
gh W
ard
and
Equa
lity A
sses
smen
ts m
ap w
here
we
hav
e hig
h an
d low
leve
ls of
socia
l cap
ital a
nd a
ctive
cit
izens
.
l T
hrou
gh W
ard
and
Equa
lity A
sses
smen
ts ide
ntify
Are
as
and
com
mun
ities o
f inte
rests
with
spec
ific h
ealth
and
we
llbein
g ne
eds w
here
enh
ancin
g so
cial c
apita
l cou
ld m
ake
a sig
nifica
nt co
ntrib
ution
l T
hrou
gh W
ard
and
Equa
lity P
lans d
evelo
p an
d co
ordin
ate
com
mun
ity in
itiativ
es th
at su
ppor
t com
mun
ities t
o do
thing
s for
them
selve
s and
eng
age
com
mun
ities
appr
opria
tely
l W
ork w
ith H
ealth
and
Well
being
par
tner
s to
help
deve
lop
supp
ort n
etwo
rks a
nd se
lf help
gro
ups
l E
nsur
e th
ere
is br
oker
age
betw
een
peop
le wa
nting
to
volun
teer
and
org
anisa
tions
seek
ing vo
lunte
ers
Are
as fo
r Act
ion
Com
mitm
ents
Del
iver
y pa
rtne
rsO
vers
eein
g(a
nd s
uppo
rtin
g)
part
ners
hip

Hea
lth In
equa
litie
s A
ctio
n Pl
an
22
Pr
iorit
y 18
: Red
uce
mor
talit
y fr
om c
ardi
ovas
cula
r dis
ease
, res
pira
tory
dis
ease
, dia
bete
s
and
canc
erR
elev
ant s
tand
ards
aga
inst
whi
ch to
mon
itor p
rogr
ess
on th
is p
riorit
y co
uld
incl
ude:
R
ecor
ded
diab
etes
; Alc
ohol
rela
ted
adm
issi
ons
to h
ospi
tal;
Can
cer d
iagn
oses
sta
ge 1
& 2
; Can
cer s
cree
ning
cov
erag
e; A
cces
s to
non
-can
cer
scre
enin
g pr
ogra
mm
es; T
ake
up o
f NH
S H
ealth
Che
cks;
Mor
talit
y fr
om a
ll ca
rdio
vasc
ular
dis
ease
s (in
clud
ing
hear
t dis
ease
and
str
oke)
, can
cer,
liver
dis
ease
, res
pira
tory
dis
ease
s, c
omm
unic
able
dis
ease
s; E
mer
genc
y re
adm
issi
ons
with
in 3
0 da
ys o
f dis
char
ge fr
om h
ospi
tal;
One
-and
five
-ye
ar s
urvi
val f
rom
col
orec
tal,
brea
st, l
ung
canc
er; P
reve
ntab
le s
ight
loss
; Em
erge
ncy
read
mis
sion
s fo
r acu
te c
ondi
tions
that
sho
uld
not u
sual
ly
requ
ire h
ospi
tal a
dmis
sion
; Pro
port
ion
of s
trok
e pa
tient
s re
port
ing
impr
ovem
ent i
n ac
tivity
/life
styl
e
Ensu
re e
arly
det
ectio
n of
ca
rdio
vasc
ular
dis
ease
, res
pira
tory
di
seas
e, c
ance
r and
dia
bete
s,
incl
udin
g he
alth
scr
eeni
ng
Dev
elop
inte
grat
ed c
are
mod
els
to
mee
t ind
ivid
ual n
eed
Impr
ove
man
agem
ent o
f peo
ple
with
ch
roni
c di
seas
e an
d ca
ncer
Red
uce
com
plic
atio
ns a
nd re
peat
ad
mis
sion
s fr
om c
hron
ic d
isea
se
Wor
k w
ith v
ulne
rabl
e an
d hi
gh ri
sk
grou
ps to
redu
ce in
equa
litie
s in
ac
cess
to h
ealth
ser
vice
sIm
prov
e se
lf-ca
re s
uppo
rt
l F
ull i
mpl
emen
tatio
n of
CVD
Sec
onda
ry P
reve
ntio
n Q
ualit
y Im
prov
emen
t (Q
I)Pro
ject
, l C
ontin
ued
impl
emen
tatio
n of
the
Atria
l Fib
rilla
tion
QI
Proj
ect
l D
evel
opm
ent a
nd im
plem
enta
tion
of E
nhan
ced
Hea
rt Fa
ilure
(HF)
pro
ject
for p
atie
nts
with
Hea
rt Fa
ilure
l C
ontin
ued
impl
emen
tatio
n of
the
Res
pira
tory
QI
proj
ect
l M
ore
robu
st im
plem
enta
tion
of s
mok
ing
cess
atio
n in
to s
econ
dary
car
e pa
thw
ays
acro
ss h
ospi
tal a
nd
men
tal h
ealth
car
el D
evel
opm
ent,
impl
emen
tatio
n an
d ev
alua
tion
of
dire
cted
enh
ance
d se
rvic
es (D
ES) f
or h
yper
tens
ion
tele
mon
itorin
g in
Bra
dfor
d D
istri
ct C
CG
.l U
sing
the
findi
ngs
of th
e D
iabe
tes
revi
ew a
nd o
ther
pl
ans
to im
prov
e ca
re a
nd o
utco
mes
for p
atie
nts
with
di
abet
esl A
ll w
ith s
peci
fic e
ncou
rage
men
t and
sup
port
of
prac
tices
with
mos
t dep
rived
pra
ctic
e po
pula
tions
to
fully
par
ticip
ate
Aire
dale
Wha
rfeda
le
and
Cra
ven
and
Brad
ford
City
and
Br
adfo
rd D
istri
cts
CC
G
Publ
ic H
ealth
team
s;Pr
imar
y ca
re te
ams;
Seco
ndar
y ca
re
team
s;C
linic
al S
peci
alty
Le
ads;
Clin
ical
C
omm
issi
onin
g G
roup
s;Pr
ovid
ers;
Tran
sfor
mat
ion
and
Inte
grat
ion
Gro
up;
Tran
sfor
mat
ion
Cha
nge
Boar
d;Br
adfo
rd a
nd A
ireda
le
Col
labo
rativ
e C
omm
issi
oner
s Fo
rum
; C
ance
r Loc
al A
rea
Net
wor
k ;
Res
pira
tory
Qua
lity
Impr
ovem
ent G
roup
;St
roke
Stra
tegy
Gro
up;
Dia
bete
s re
view
boa
rd;
Self
care
net
wor
k
Are
as fo
r Act
ion
Com
mitm
ents
Del
iver
y pa
rtne
rsO
vers
eein
g(a
nd s
uppo
rtin
g)
part
ners
hip

References
l UCL Institute of Health Equity. 2008. ‘Fair Society Healthy Lives’ (The Marmot Review). http://www.instituteofhealthequity.org/projects/fair-society-healthy-lives-the-marmot-review
l BMDC. 2012. “Good Health and Wellbeing, Strategy to Reduce Health Inequalities, 2013-2017” http://www.bradford.gov.uk/bmdc/Consultations/consultation_health_wellbeing_strategy
l BMDC. 2013. Shadow Health and Wellbeing Board, Joint Health and Wellbeing Strategy. http://tinyurl.com/b8ynkxs
l HM Government. 2010. The Foundation Years: preventing poor children becoming poor adults: The report of the Independent Review on Poverty and Life Chances. http://webarchive.nationalarchives.gov.uk/20110120090128/http:/povertyreview.independent.gov.uk/media/20254/poverty-report.pdf
l Report of the Strategic Director, Children’s Services to the meeting of the Bradford Children’s Trust Board to be held on 16 July 2012. The Annual Analysis of Teacher Assessment, Test and Examination Results 2010/11
l Weich S, Nazroo J, Sproston K, McManus S, Blanchard M, Erens B, et al. Common mental disorders and ethnicity in England: the EMPIRIC study.Psychol Med 2004; 8: 1543–51.
l Kirkbride JB, Barker D, Cowden F, Stamps R. Yang M, Jones PB, et al. 2008. Psychoses, ethnicity and socio-economic status. The British Journal of Psychiatry (2008) 193: 18-24.
l Alzheimer’s Society. 2012. Mapping the Dementia Gap 2012. Progress on improving diagnosis of dementia 2011-2012
l Dementia UK. 2007. A report into the prevalence and cost of dementia prepared by the Personal Social Services Research Unit (PSSRU) at the London School of Economics and the Institute of Psychiatry at King’s College London, for the Alzheimer’s Society
l Housing Requirements Study 2008, Bradford Metropolitan District Council and Opinion Research Services, Swansea http://www.bradford.gov.uk/NR/rdonlyres/F799F48E-8801-49E6-BA40-5AF6A3F35EFA/0/2HousingRequirementsStudy.pdf
l Wilkinson R. Pickett K. 2010. The Spirit Level: Why Equality is Better for Everyone.
l BMDC. 2011. Bradford District Residents’ Perception Survey http://www.bradford.gov.uk/bmdc/bdp/news/news_archive/news_2011/Bradford_District_Residents_Perceptions_Survey
l Department of Health. 2010. Healthy lives, healthy people: our strategy for public health in England
l Bradford and Airedale Health and Lifestyle Survey 2007-2008
Health Inequalities A
ction Plan
23

The wording in this publication can be made available in other formats such as large print. Please call 01274 437563.