health care reform and the work of the super committee peter c. damiano director, public policy...
Post on 19-Dec-2015
213 views
TRANSCRIPT

Health Care Reform and the Work of the Super Committee
Peter C. Damiano
Director, Public Policy Center
University of Iowa
Johnson County Livable Community
November 14, 2011

Today’s Topics
• The Patient Protection and Affordable Care Act (PPACA)
• What is already in place
• What’s yet to come
• ACA and public health
• IA Safety Net project
• Discussion
• What about the Super Committee
• What about the Election/Courts
What have we created?
The Patient Protection and Affordable Care Act (PPACA)
• Signed into law March 2010
• Emphasis on:
Individual insurance market
Small business insurance market
• Few implications for large employer-based insurance
Already self-insured

Market-based reform
•Right of center approach to reform:
Similar to proposals by Richard Nixon, Robert Dole and Mitt Romney
Left of center approach-single payer
•Uses primarily private insurance companies:
Some Gov’t program expansion

Health care reform 2010-19 Style

Why Reform Health Care in US
• Cost
• Access to Care – right vs. privilege
• Quality

Coverage in new plan
•Net 32 million more insured
•Decline of 3 million from employers
•Decline of 5 million from non-group
New insureds
Private insurance Public insurance
16 million
24 million
Source: CBO report to Congress, March 2010
Policies Already in Place
25 reforms enacted in 201018 of 21 enacted in 2011

Current policies (fall 2010)
• Cover children up to 26 on parent’s policies
• State/federal high risk pools
• Eliminate pre-existing conditions for children
• Can’t rescind coverage for illness
• Can’t impose yearly and lifetime caps

Pre-existing conditions removed?

Current policies (fall 2010)
• Small-business tax credits: Small businesses (fewer than 25 employees and average wages under $50,000) that offer health care benefits eligible for tax credits of up to 35% of premiums for 2 years

Current policies (fall 2010)
• Establish process to review premium increases
• States must report trends in premium increases for inclusion in Exchanges
• Establish Center for Medicare and Medicaid Innovation
Current policies (2011)
•Discounts to fill doughnut hole-50% discount on brand name drugs
•Minimum Medical Loss Ratios-requires reporting proportion of dollars spent on clinical services/quality
-must be at least 85% large group
-80% individual and small group
-debate about agent fees

Cost of reform
•Total cost: $940 billion first ten years
• Impact on deficit:
$124 Billion in reductions in the deficit first ten years
$1.2 Trillion second ten years
Source: Congressional Budget Office, March 2010

Cost of reform
• Impact on Medicare/SS solvency:
Extend Medicare trust fund solvency 12 years (2017 to 2029)
- higher payroll taxes (0.9%) on those making over $200,000
- lower hospital payment rates
SS improved by taxing highest benefit plans in 2018
Source: Medicare and Social Security Trustee Report, August 2010

Financing Reform
• 10% tax on Indoor Tanning Services
• Non-profit hospitals must conduct community needs assessment and develop a financial assistance policy or face $50,000 tax for failure to meet this
• Reduced deductions for OTC drugs for Flex or Health Saving Accounts
• Reduced deductions for non-medical distributions from Flex or Health Saving Accounts

So What’s Next

If the ACA goes through unchanged
2014-19

Future Financing of Reform
•Medicare payroll tax on investments (2012):
3.8% on investment income for families >$250,000
•Excise tax on investments (2019):
40% on “Cadillac” plans
Source: Congressional Budget Office, March 2010

Future policies (2014)
• Individual mandate begins.
• Large employer mandate begins (over 50 employees only)
• Medicaid expansion begins.
• Health insurance Exchanges begin to operate.
Individual
Small businesses
Exchanges generally
• Health insurance marketplace (bazaar)
• Offer regulated products that meet standards
• Require two multi-state plans in each Exchange (federal employee plans)
• At least one plan must be offered by a non-profit entity
Coverage for children
•Medicaid: up to 133% of FPL
No change for Iowa
•CHIP: up to state approved level
300% FPL in Iowa-no change
•Exchange: 300% of FPL and up
Coverage for Adults
• Medicaid: up to 133% of FPL
Gets rid of categorical eligibility
Eliminates IowaCare program (probably)
• Exchange: 133% of FPL and up
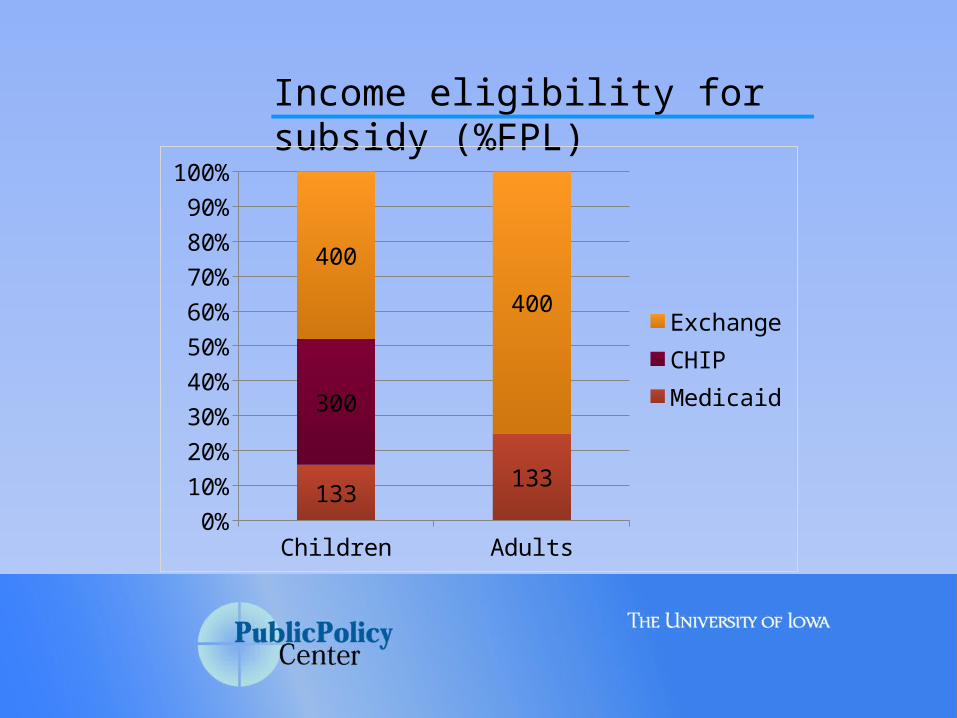
Income eligibility for subsidy (%FPL)
Children Adults0%
10%20%30%40%50%60%70%80%90%
100%
133133
300
400
400ExchangeCHIPMedicaid

Health Insurance Exchange
• American Health Benefit Exchanges
Individuals
100-200% FPL: $1,983/individual and $3,967/family;
200-300% FPL: $2,975/individual and $5,950/family;
300-400% FPL: $3,987/individual and $7,973/family

Health Insurance Exchange
• Small Business Health Options Program (SHOP) Exchanges
Up to 100 employees
The ACA, Public Health and the Iowa Safety Net

Preventive coverage
• All new group and individual health plans will be required to provide free preventive care for proven preventive services. (2010)
• New Medicare prevention coverage (2011)

Public Health and Prevention$250 million (2010)
4 Activities
1. Community and Clinical Prevention: $126M• Putting Prevention to Work: $74M• Primary and Behavioral Health Integration: 20M• Obesity Prevention and Fitness:$16M• Tobacco Cessation: $16M
2. Public Health Infrastructure: $70M • Public Health Infrastructure: $50M• Epidemiology and Lab Capacity: $20M
Public Health and Prevention 2010
3. Research and Tracking: $31M• Surveillance: $21M• Community Preventive Services Task Force: $5M• Clinical Preventive Services Task Force: $5M
4. Public Health Training: $23M• Public Health Workforce: $8M• Public Health Training Centers: $15M

Public Health and Prevention 2011
• National Prevention, Health Promotion and Public Health Council • Senior officials across gov’t agencies• Created by Executive Order June, 2011

ACA creates changes and opportunities for safety net providers-currently uncertain environment
• Increasing public and private coverage • Funds for FQHCs• Establishment of ACOs• Funds for HIT, HIE, EHRs and meaningful use• Medical home development
Indirect ACA and Public Health issues
Iowa Safety Net, the ACA and Related Primary Care Delivery System Changes

Iowa Safety Net and the ACA
Study goal: Use Iowa as a model to inform policymakers about the impact of the ACA and related delivery system changes on safety net providers and payers• Uses Iowa Safety Net Network and national
advisory committee to inform process• Emphasis is on primary care• Funded by The Commonwealth Fund with
additional support from Wellmark Foundation

1. Conduct background inventory of safety net providers/payers
2. Evaluate impact of the ACA as implementation moves forward
3. Identify opportunities for collaboration and coordination between public and private providers to improve efficiency
Iowa Safety Net and the ACA

1. Safety net providers• FQHCs• Rural health clinics• Title X funded family planning clinics• Comm. MH/SA centers• Free clinics
• Provider Networks/Financing/Patients
Iowa Safety Net and the ACA

2. Safety net payers• Medicare• Medicaid• CHIP• Title V• Ryan White
• Financing/Patients
Iowa Safety Net and the ACA

• Assist policymakers and safety net providers to plan for change-financial and organizational
• Conduct large scale strategic planning effort not otherwise possible
• Using national and state-level experts with academic assistance to evaluate the potential impacts of ACA on states
• Identify opportunities for integration and coordination in the health care delivery system.
Major Goals of the Iowa Safety Net Project

Provider Concerns Benefits Opportunities
RHC Manpower shortageChanges necessary to take advantageSmaller clinics not prepared to take advantage
Reimbursed for servicesAccess to specialty care
Depends on RHC inclusionWork with local boardsRHC affiliate with private providers
Free Clinics Concern about it being overturnedstaff shortages
Access to affordable insurance easierPeople feel more welcome
Not hopeful
Local Public Health Dept.
Certain groups and industries attempting to carve out their piece to remain viable as ACA develops
Remove fragmentation and streamlining will help make better use of public $$
Benefits of partnerships between private providers and state/federal public health programs
An FQHC Congress won’t support ACA Fewer uninsuredMore resources
Integration and coordination with private providers
An FQHC Unfamiliarity in navigating system (patients)Worker shortage (provider)Funding stream uncertainty (primary care)Disjointed funding stream (Care system)
Iowa as a leaderHealth improvements with basic primary careReimbursement for group previously uncovered
Developing capacityManaging chronic illness improvementsGreater patient empowerment
Your Concerns, Benefits and Opportunities regarding ACA in Iowa

Provider Concerns Benefits OpportunitiesIowa Dept of Public Health
Individual groups and industries will try to carve out their “piece” in order to remain viable, as opposed to integrating and de-fragmenting the system.
Removing fragmentation should make direct state/federal funding more efficient
More partnering by IDPH with private providers for federal and state-funded public health programs (i.e cancer screenings and child wellness)
Family Planning
How safety net providers who deal with specialty areas of practice are incorporated and included. 2.PCP utilize expertise of family planning clinics (collaboration is necessary)3. What to do about undocumented workers, people transitioning between jobs, life stages- not included? How will FPA provide services?
More opportunities for services to be available to
Your Concerns, Benefits and Opportunities regarding ACA in Iowa

If the ACA does not go through as planned
1) Election2) Supreme Court decision

If the ACA does not go through as planned
The 2012 Election

How bad is the problem?
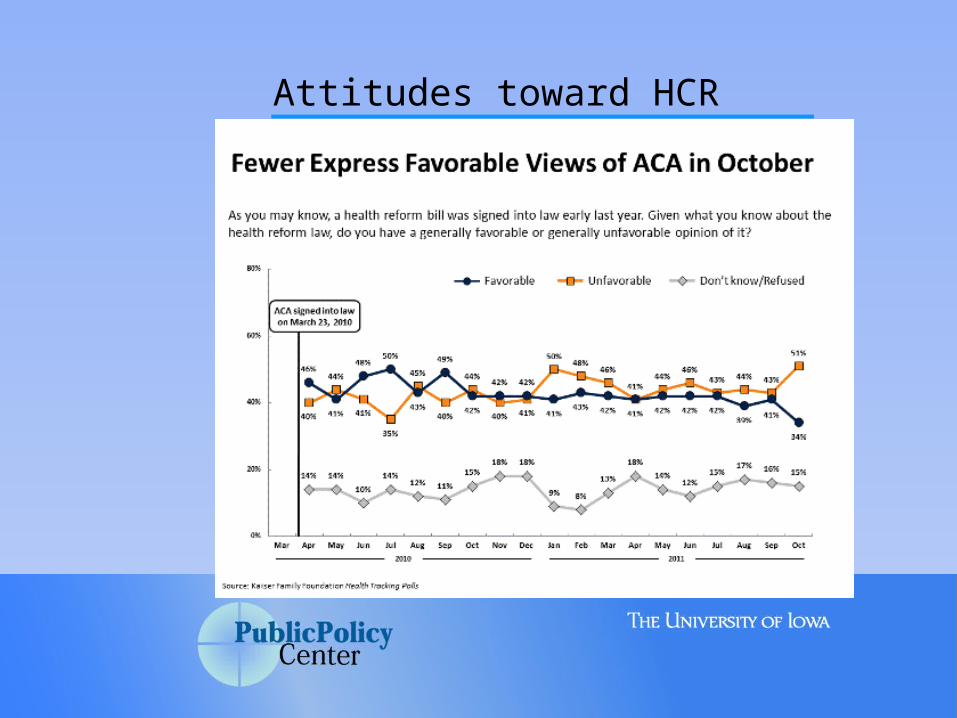
Attitudes toward HCR

If the ACA does not go through as planned
Supreme Court Decision

“States’ Right?”

Supreme court challenge
• November 14-Supreme Court said it will hear challenge
• Decision likely late June• Focus:
1. Individual mandate
2. Jurisdictional issue: can they rule before a tax goes into affect (the fine–1867 Anti-injunction act)
3. Medicaid expansion and cost to the state
4. Declined considering penalties to states that they and other employers would face (1985 ruling that states must comply with employer-related laws)
Lower court rulings
• 30 lawsuits have been filed• Half of the states have filed briefs against ACA• Federal appeals courts (four rulings):
• Commerce clause at issue• Two upheld the law• One ruling it unconstitutional• One saying ruling premature (not in place)• Social security, civil rights acts, tax power
Supreme court case from:• National Federation of Independent Business v.
Sebelius, 11-393; Department of Health and Human Services v. Florida, 11-398; and Florida v. Department of Health and Human Services, 11-400.
DC Court of Appeal Ruling
November 7, 2011 ruling• Majority opinion: Laurence H. Silberman• 2-1 in support of individual mandate
“The right to be free from federal regulation is not absolute, and yields to the imperative that Congress be free to forge national solutions to national problems, no matter how local — or seemingly passive — their individual origins,” he wrote. The fact that Congress may have never issued an individual mandate to purchase something before, a central argument for many opposing the law, “seems to us a political judgment rather than a recognition of constitutional limitations,”
NY Times, Nov. 8, 2011

The Super Committee and Health Care Reform

The Budget Control Act (PL 112-25)
• Passed-August 2, 2011• Increased debt ceiling by $2.1 trillion over 10 years• Aimed to reduce deficit by $2.3 trillion over 10 yrs by:
1. Caps on Discretionary spending ($0.9 billion)
2. Super Committee deficit reduction plan charged to find at least $1.2 trillion in deficit reduction to avoid “sequestration”
• Sequestration is automatic, across the board spending cuts
Redhead, CS. Budget Control Act: Potential Impact of Automatic Spending Reductions on Health Reform. Cong. Research Services

The Super Committee
• Democrats• Sen. Patty Murray (D-Wash)• Sen. Max Baucus (D-Mont)• Sen. John Kerry (D- Mass)• Rep. Xavier Becerra (D-CA)• Rep. James Clyburn (D-SC)• Rep. Chris Van Hollen (D-
MD)
• Republicans• Sen. Jon Kyl (R-AZ)• Sen. Rob Portman (R-OH)• Sen. Pat Toomey (R-PA)• Rep. Jeb Hensarling (R-Tex.)• Rep. Dave Camp (R-MI)• Rep. Fred Upton (R-MI)
The Super Committee
• Sept. 8:First organizational meeting• Sept. 13: First public hearing, • Oct. 14: House and Senate committees must
submit recommendations to the committee • Nov. 23: Vote on a plan with at least $1.2 trillion
in deficit reduction.• Dec. 2: Committee submits report and legislative
language to president/Congress.• Dec. 9: Any House or Senate committee to
which the supercommittee bill is referred must report it to the full House.

Super Committee Schedule
• Dec. 23: A majority vote (a “yes” vote by seven of the panel’s 12 members) is required Jan. 15, 2012: “trigger” leading to $1.2 trillion of future spending cuts goes into effect
• February 2012: First $900 billion of debt ceiling increase runs out.
• February/March 2012: During this period, 15 days after the president uses his authority in the bill to increase the debt ceiling a second time, is the deadline for Congress to consider a resolution of disapproval for the second tranche ($1.2-$1.5 trillion) of debt limit increase.

Super Committee Schedule
• Fall/Winter 2012: The additional $2.1-$2.4 trillion of borrowing authority from this law runs out.
• Jan. 2, 2013: OMB orders sequestrations for defense and non-defense categories of spending necessary to meet spending cuts required by the “trigger."

Democratic proposal
• $2.3 trillion tax and cut proposal• $1 Trillion in new taxes• $350 billion in Medicare savings
• $250 billion from providers• $100 billion from beneficiaries• Fixes “Sustainable Growth Rate”• Physician reimbursement cut
• $50 billion in Medicaid savings• $8 billion from Prevention and Public Health
Fund

Republican proposal
1. Cut deficits by $1.2 trillion
2. $350 billion in new revenues, derived largely from a revision to the tax code that would limit some deductions and subsidies
3. Lowering the top tax rate to 28 percent.
If no proposal
If no proposal
Sequestration
1. BCA sets out discretionary spending limits through FY 2021
2. Begins if no agreement or OMB determines spending too high, president orders sequestration
3. All accounts reduced proportionally within category
4. $109.3 billion in cuts per year beginning in FY 2013
• Half from defense

If no proposal
Sequestration Health Impact (9% first year)
1. Medicaid not automatically cut
2. CDC-cut $740 million in 2011 already
3. Medical research
4. Disease prevention-reducing prevention fund
5. HIV/AIDS drug and treatment programs

CBO Estimates if no proposal (2013-2021)
• Reductions from 10% (2013) to 8.5% (2021) in caps on new discretionary appropriations for defense programs, outlay savings $454 billion.
• Reductions from 7.8% (2013) to 5.5% (2021) in caps on new discretionary appropriations for nondefense programs, outlay savings $294 billion.
• Reductions of 2% each year in most Medicare spending to providers, savings of $123 billion, and
• About $31 billion in outlays from reductions in premiums for Part B of
• An estimated reduction of $169 billion in debt-service costs.

Alternatives
1. Two step process• Super Committee sets a figure for
increased revenue from tax reform-• Set in legislation by congressional
committees
2. Turn off automatic cuts (President is opposed)
Exempted Health Accounts
• All Veterans Affairs programs • Grants to States for Medicaid • Children’s Health Insurance Fund• Black Lung Disability Trust Fund Refinancing• Medical Facilities Guarantee and Loan • Department of Defense Medicare-Eligible Retiree Fund
Payments to Health Care Trust • Radiation Exposure Compensation Trust • Vaccine Injury Compensation • Energy Employees Occupational Illness Fund • Postal Service Retiree Health Benefits Fund • Retirement Pay and Medical Benefits for
Commissioned Officers, Public Health Service

Devil is in the details
• Implementation is critical
State and Federal level
•Cost containment critical
Care and premiums in the exchange

Discussion