health care provider-patient communication and self …
TRANSCRIPT

HEALTH CARE PROVIDER-PATIENT COMMUNICATION
AND SELF-CARE BEHAVIORS AMONG TYPE 2 DIABETES
AT MAHOSOT HOSPITAL, VIENTIANE CAPITAL, LAO PDR
BY
MR. KENGHER VAXENG
AN INDEPENDENT STUDY SUBMITTED IN PARTIAL
FULFILLMENT OF THE REQUIREMENT FOR THE DEGREE
OF MASTER OF PUBLIC HEALTH
HEALTH SERVICE MANAGEMENT
FACULTY OF PUBLIC HEALTH
THAMMASAT UNIVERSITY
ACADEMIC YEAR 2017
COPYRIGHT OF THAMMASAT UNIVERSITY
Ref. code: 25606017090090UFM

HEALTH CARE PROVIDER-PATIENT COMMUNICATION
AND SELF-CARE BEHAVIORS AMONG TYPE 2 DIABETES
AT MAHOSOT HOSPITAL, VIENTIANE CAPITAL, LAO PDR
BY
MR. KENGHER VAXENG
AN INDEPENDENT STUDY SUBMITTED IN PARTIAL
FULFILLMENT OF THE REQUIREMENT FOR THE DEGREE
OF MASTER OF PUBLIC HEALTH
HEALTH SERVICE MANAGEMENT
FACULTY OF PUBLIC HEALTH
THAMMASAT UNIVERSITY
ACADEMIC YEAR 2017
COPYRIGHT OF THAMMASAT UNIVERSITY
Ref. code: 25606017090090UFM

(1)
INDEPENDENT STUDY HEALTH CARE PROVIDER-PATIENT
COMMUNICATION AND SELF-CARE
BEHAVIORS AMONG TYPE 2
DIABETES AT MAHOSOT HOSPITAL,
VIENTIANE CAPITAL, LAO PDR
Author Mr. Kengher Vaxeng
Degree Master of Public Health
Major Field/Faculty/University Health Service Management
Faculty of Public Health
Thammasat University
Independent Advisor Pornthip Chompook, Ph.D.
Independent Co-Advisor Assoc. Prof. Chaweewon Boonshuyar, M.S.P.H
Academic Year 2017
ABSTRACT
This cross-sectional study was aimed to evaluate health care provider-
patient communication and self-care behaviors among Type 2 Diabetes at Mahosot
Hospital, Vientiane Capital, Lao PDR. Descriptive statistics and multiple linear
regression were used to determine the relationship between independent variables and
dependent variables. Data collection was conducted by interviewing 226 participants
visited OPD, Mahosot Hospital.
The finding shows health care provider-patient communication was good
(58.0%). For social supports, over half of participants had a moderate to good family
supports (59.7%), more than half of participants had poor peer supports (63.3%), and
most of participants received information of Type 2 Diabetes Mellitus (92.5%).
However, self-care behaviors was poor (59.7%). Regarding to self-care behaviors on
dietary practice, more than half of participants was poor (62.4%) while moderate self-
care behaviors with dietary was 30.5%. In addition, 6.6% of participants were current
smokers. 16.8% of participants were current alcohol drinkers. 75.2% did not check
blood sugar at home because of no equipment. Also, 58% of participants had never
examined feet for sores or wounds. In addition, 34.5% had forgotten to take disbetic
Ref. code: 25606017090090UFM

(2)
drugs, and 54% of participants had poor medical adherence. Over half of participants
(58.8%) had depression. After using a multiple linear regression model, age was
associated with self-care behaviors (b= 0.16, p=0.002). This shows the higher age had
better self-care behaviors. In addition, education was associated with self-care
behaviors (b= 3.19, p=0.022). Moreover, health care provider-patient communication
were significantly related to self-care behaviors (b= -0.25, p = 0.043).
This study shows that health care provider-patient communication is crucial
for self-care behaviors among Type 2 Diabetes. Further studies should emphasize on
how to improve this communication to help adjust life styles in order to prevent diabetes
complications.
Keywords: Health care provider-patient communication, Self-care behaviors, Type 2
Diabetes, Social supports, Lao PDR.
Ref. code: 25606017090090UFM

(3)
ACKNOWLEDGEMENTS
First of all, I am very thankful to the Ministry of Health of Lao PDR and
Asian Development Bank (ADB) for funding me the scholarship for me to study in
Thammasat University. I also would like to express my deepest gratitude to my advisor
Lec. Dr. Pornthip Chompook, Ph.D for her enormous effort and guidance from the
beginning of my research proposal until the finalized results. She spent much of her
time for supporting and helping of all her advisees including myself. In addition, she
untiring help and supervision for my research. At the same time, I also would like to
express my sincere gratitude to my co-advisor Assoc. Prof. Chaweewon Boonshuyar,
M.S.P.H for her thoughtful comments and she spent much of her time to helping me
some data analysis. I have been great honor by her encouragement and guidance for
everything. I am indebted and grateful to both of my advisor and co-advisor who
cooperate and help together for fulfilling of our need in our academic life.
Secondly, I would like to extend my thankful and sincere gratitude to
director of Mahosot Hospital to give facilitate for data collection at OPD and thankful
for two nurses to helpful me in the process of data collection. Also, thankful for Type
2 Diabetes to give information in this research. Moreover, I also would like to express
my deepest to all of my teachers, staffs at Faculty of Public Health office for their
supports and guidance the learning process in the Faculty and thankful to all of my
classmate as it was a magnificent learning experiences.
Finally, I would like to express my deepest gratitude and love for my family
to encouragement and supports me for my whole life to study during this period. Then
I want to give my thanks to all of my friends in Lao PDR and Bangkok who always
give hands and encourage me. It has been great appreciation for me that I have many
excellent and sincere friends. Therefore, these supports and help make me indebted with
gratitude and with them, it would not be fulfilled and achieve for my goal.
Mr. Kengher VAXENG
Ref. code: 25606017090090UFM
(4)
TABLE OF CONTENTS
Page
ABSTRACT (1)
ACKNOWLEDGEMENTS (3)
LIST OF TABLES (7)
LIST OF FIGURES (8)
LIST OF ABBREVIATION (9)
CHAPTER 1 INTRODUCTION 1
1.1 Rationale and Justification 1
1.2 Objectives 3
1.3 Variables of the study 3
1.4 Operational definitions 4
1.5 Conceptual framework 7
CHAPTER 2 LITERATURE REVIEW 8
2.1 Situation of Diabetes Mellitus in Lao PDR 8
2.2 Diabetes Mellitus 9
2.3 Type 2 Diabetes Mellitus 10
2.4 Theory of self-care 13
2.5 Self-care behaviors 14
2.6 Social supports 18
2.7 Health care provider-patient communication 19
2.8 Review of relevant studies 21
Ref. code: 25606017090090UFM

(5)
CHAPTER 3 MATERIALS AND METHODS 24
3.1 Study design 24
3.2 Study site 24
3.3 Population 24
3.4 Sample size 24
3.5 Inclusion and exclusion criteria 25
3.6 Research Instrument 25
3.7 Ethical consideration 27
3.8 Data collection 28
3.9 Data management and analysis 28
CHAPTER 4 RESULTS AND DISCUSSION 29
4.1 Personal characteristics 29
4.2 Diabetes status 32
4.3 Self-care behaviors 34
4.4 Social supports 45
4.4.1 Family supports 45
4.4.2 Peer supports 47
4.4.3 Source of information of Type 2 Diabetes Mellitus 48
4.5 Health care provider-patient communication 49
4.6 Satisfaction to health services system 52
4.7 Factors associated with self-care behaviors 54
4.8 Self-care behaviors and Fasting Blood Sugar 59
4.9 Discussion 59
CHAPTER 5 CONCLUSION AND RECOMMENDATION 63
5.1 Conclusion 63
5.2 Recommendation 65
Ref. code: 25606017090090UFM
(6)
REFERENCES 66
APPENDICES
APPENDIX A Questionnaire form (English) 72
APPENDIX B Certificate of approval by National Ethic Committee 95
APPENDIX C Informed Sheet 96
APPENDIX D Informed Cosent Form 99
BIOGRAPHY 101
Ref. code: 25606017090090UFM

(7)
LIST OF TABLES
Tables Page
2.1 Treatment goals for Diabetes 18
4.1 Personal characteristics (n=226) 30
4.2 Diabetes status (n=226) 32
4.3 Level of self-care behaviors (n=226) 34
4.4 Level of eating behaviors (n=226) 35
4.5 Eating behaviors (n=226) 36
4.6 Smoking habits (n=226) 39
4.7 Alcohol drinking (n=226) 40
4.8 Physical activities (n=226) 41
4.9 Level of medical adherence (n=226) 42
4.10 Medical adherence (n=226) 42
4.11 Depression (n=226) 44
4.12 Level of family supports (n=226) 45
4.13 Family supports (n=226) 46
4.14 Level of peer supports (n=226) 47
4.15 Peer supports (n=226) 48
4.16 Sources of information 49
4.17 Level of Health care provider-patient communication (n=226) 50
4.18 Health care provider-patient communication (n=226) 51
4.19 Level of satisfaction (n=226) 52
4.20 Satisfaction to services (n=226) 53
4.21 Comparison of self-care behaviors by various characteristics of Type 2 Diabetes 55
4.22 Pearson Correlations between each quantitative factors and self-care
behaviors of 226 Type 2 Diabetes 57
4.23 Multiple linear regression analysis for self-care behaviors of 226 Type 2 Diabetes 58
4.24 Pearson Correlations between FBS and self-care behaviors of Type 2 Diabetes 59
Ref. code: 25606017090090UFM

(8)
LIST OF FIGURES
Figures Page
2.1 Diabetes patients at OPD in Mahosot Hospital (Personal contact, OPD
report, 2017)(16) 9
2.2 Smokes with non-Diabetes, Diabetes not checking and Diabetes diagnosed in 16
Ref. code: 25606017090090UFM

(9)
LIST OF ABBREVIATION
Abbreviations Terms
WHO World Health Organization
NCDs Non-Communicable Disease
IDF International Diabetes Federation
ADA American Diabetes Association
OPD Out-Patient Department
GDM Gestational Diabetes Mellitus
IGT Impaired Glucose Tolerance
IFG Impaired Fasting Glycaemia
CVD Cardiovascular Disease
LDL Low Density Lipoprotein
HDL High Density Lipoprotein
AHA American Heart Association
FBS Fasting Blood Sugar
BMI Body Mass Index
Ref. code: 25606017090090UFM

1
CHAPTER 1
INTRODUCTION
1.1 Rationale and Justification
Diabetes mellitus is a chronic disease that the pancreas cannot produce
enough insulin or human body cannot manage the insulin after production. Insulin is a
hormone to control blood glucose in the human body. Therefore, the body cannot
control the levels of insulin a long time which can harm human body’s system such as
neuropathy and blood pressure. In addition, Diabetes Mellitus is one of four problems
of non-communicable diseases (NCDs) worldwide(1)
In 2014, the global report showed adults living with diabetes were 442
million people compared with 108 million in 1980. The global prevalence of Diabetes
in the adult population since 1980 had been increasing from 4.7% to 8.5% in 2014.
Therefore, this shows the cause effect in associated with risk factors among population
being overweight or obese especially in the low and middle-income(1). In addition, the
percentage of deaths attributable to high blood glucose or Diabetes that occurs prior to
age 70 is higher in low and middle-income countries compared to high-income countries.
Diabetes can be undiagnosed for several years, until complications have already arisen.
For many years Type 2 Diabetes was seen only in adults but it has begun to occur in
children(2).
International Diabetes Foundation (IFD) estimates in the 2013 that China
was the top of the global list of countries for the number of people with Diabetes came
after by India(3). In addition, only 33% of China diabetes patients had regular foot care
and only 13% of diabetes patients could do regular blood glucose self-testing, so it is
important that health care provider should understand factors influencing self-care
behaviors(4). Moreover, the proportion of people with Type 2 Diabetes and obesity in
the Asia have increased, the International Diabetes Foundation found that Asia was
emerging as the epicenter of diabetes and some of the most population countries in the
world(5). Also, the burden of Diabetes complications affected health care system
globally(6). Moreover, patients had low Type 2 diabetes knowledge for glycemic control
Ref. code: 25606017090090UFM
2
were likely to have low standard for self-care efficacy and self-care behaviors(7).
Lao PDR reported that Diabetes prevalence was 5.6% in adult population,
and 2% of Lao people died from Diabetes each years. Lao government has started to
focus on diabetes as an important health concern in the country in 2014. World Diabetes
Foundation-funded project was conducted to strengthen the Diabetes health care system
in Lao PDR(8).
Regarding to the STEP survey on NCDs, it was recommended that mass
education program to prevent chronic diseases should be set up. Moreover, the studies
should be conducted to investigate the potential risk factors for Type 2 Diabetes among
Lao people(9).
Lao PDR is a country has land-linked with 5 countries such as China,
Myanmar, Thailand, Vietnam and Cambodia. Lao PDR has population nearly 7 million
people. Newly, there were some research had been conducted, as a results could show
some information to approach for health policy in Lao(10).
Mahosot Hospital is an international hospital located in central of Lao PDR.
The capacity is 365 beds, where provide primary-tertiary, specializing in internal
medicine(10). Out Patients Department (OPD) is one of 33 departments where deliver
service to the patients who need to check up and there are many rooms for checking up
by specialist. There is also DM clinic on working days. A vast majority of patients visit
to Mahosot hospital is in the form of outpatient visits whereby the patients seeks
diagnosis or treatment but are not hospitalized over-night(11).
The basic health believe model is known as the motive of people to process
in doing something and make sure perceive of individuals can show the motivation and
act with some cause of behaviors, so that the model can show the association between
health believe and self-behaviors. A result on the study of health believe model and
self-care behavior among Type 2 Diabetes showed that health believe model could
explain 29.6% of the variance in self-care behaviors in Type 2 diabetes(12). Inadequate
self-care in diabetes is a major problem which health care providers encounter. This
issue not only has an impact on mortality rates, but also increases treatment costs. The
results of several studies show that diabetes patients need to follow medical adherence,
not only treatment(13).
Ref. code: 25606017090090UFM
3
1.2 Objectives
- To evaluate health care provider-patient communication and self- care
behaviors among Type 2 Diabetes
- To determine the relationship between personal characteristics, medical
status, social supports, health care provider-patient communication and
self-care behaviors among Type 2 Diabetes
1.3 Variables of the study
Independent variables
Personal characteristics
- Age
- gender
- Marital status
- Education
- Occupation
- Religion
- Family income
- BMI
Diabetes status
- Diabetes duration
- Current medication
- Use of alternative medicine
- Co-morbidity
- Type 2 Diabetes complications
Social supports
- Family supports
- Peer supports
- Source of Diabetes Mellitus information
Ref. code: 25606017090090UFM
4
Health care provider-patient communication
- physicians
- Nurses
- Pharmacists
- Nutritionists
Dependent variables
A. Self-care behaviors
- Diet
- Physical activities
- Self-monitoring of blood glucose
- Foot care
- Regular medication
B. Fasting Blood Sugar
1.4 Operational definitions
Type 2 Diabetes Mellitus: refers to the people who have chronic disease
related with abnormally high levels of the glucose in the blood, diagnosed as diabetes
type 2 by medical doctor, taking anti-hyperglycemic and have treatment at the hospital.
Body Mass Index: Refers to weight in kilograms divided by square of
height in the meter of the patients being recorded when visiting clinic. According to the
WHO, the classification of BMI to the Asia-Pacific population is as follows:
Underweight < 18.5 kg/m2
Normal weight 18.5 – 22.9 kg/m2
Overweight 23.0 – 24.9 kg/m2
Obese ≥ 25 kg/m2
Diabetes duration: refers to the approximate year from the date of the
diagnosis of Type 2 Diabetes by medical doctors until the date of study.
Current medication: refer to the anti-diabetic drug to control for normal
glycemic levels into two classes such as oral anti-diabetic drugs and injectable anti-
diabetic drugs.
Ref. code: 25606017090090UFM
5
Use alternative medicine: refers to using a non-mainstream approach
instead of conventional medicine.
Co-morbidity: refers to the occurrence of one or more chronic conditions
in the same person with an index-disease, occurs frequently among Type 2 Diabetes. In
this study, Diabetes-related co-morbidity included obesity, hypertension and
dyslipidemia. Type 2 Diabetes co-morbidities were approved in the patients’ medical
records.
Type 2 Diabetes complications: refers to the presence of any diabetes of
complications in the patients at the time of the study that are already diagnosed by
medical doctors and known by the patient. These complications include (Coronary
Heart disease, Hypertension, Peripheral Vascular Disease, Peripheral Neuropathy,
Nephropathy, Retinopathy and Diabetes foot)
Social supports: refers to various forms of help or assistance including:
emotional, tangible, and guidance support provided by the persons from spouse or
family members or relatives and peer.
Family supports: refers to the patient’s perception of support from their
family members, including feeling of being care, aided, and praised from family members.
Peer supports: refers to the person to given some information may help
the patients with Type 2 Diabetes effectively manage and reduce risks associated with
their Type 2 Diabetes.
Source of Diabetes information: refers to the information to get from
health care providers, television, radio, and social media.
Health care provider: refers to the persons inform the information of heath
care in public health such as physician, nurses, pharmacists and nutritionists.
Physician-patient communication: refers to the patient’s perception
about the quality of their communication with physicians including physician’s
explanation of Type 2 Diabetes and medical care, physicians listening and
responsiveness to patient’s problem and concerns about Diabetes self-care.
Self-care behaviors: Refers to set of behaviors that patients with Type 2
Diabetes perform daily to achieve Diabetes control. These recommended specific
activities include (diet, physical activities, self-testing of blood glucose, foot care and
regular medication)
Ref. code: 25606017090090UFM

6
Diet: refers to simply means eating the healthiest foods in moderate amounts
and sticking to regular mealtimes and the based on eating three meals a day at regular times.
Physical activities: refers to the moderate intensity exercise such as
jogging, walking, swimming etc. at least 3 times per week and also daily physical
activities for house work or recreation.
Self-monitoring of blood glucose: refers to the patients practicing of home
testing of blood glucose to adjust medication and life style accordingly to achieve a
target level of glycemic control.
Foot care: Refers to the patient’s behavior in taking care of their foot to
protect from injury by regular checking, cleaning, drying, careful nail cutting and
wearing suitable or special shoes.
Regular medications: refer to the continuous and regular taking of the
anti-hyperglycemic medication or insulin doses at the time of the study according to the
medical doctor prescription.
Fasting blood sugar: refers the level is the result of a blood sample taken
after a patient fasts for at least 8 hours. A normal fasting blood sugar level for patients
without Diabetes is less than 100 mg/dl.
Ref. code: 25606017090090UFM
7
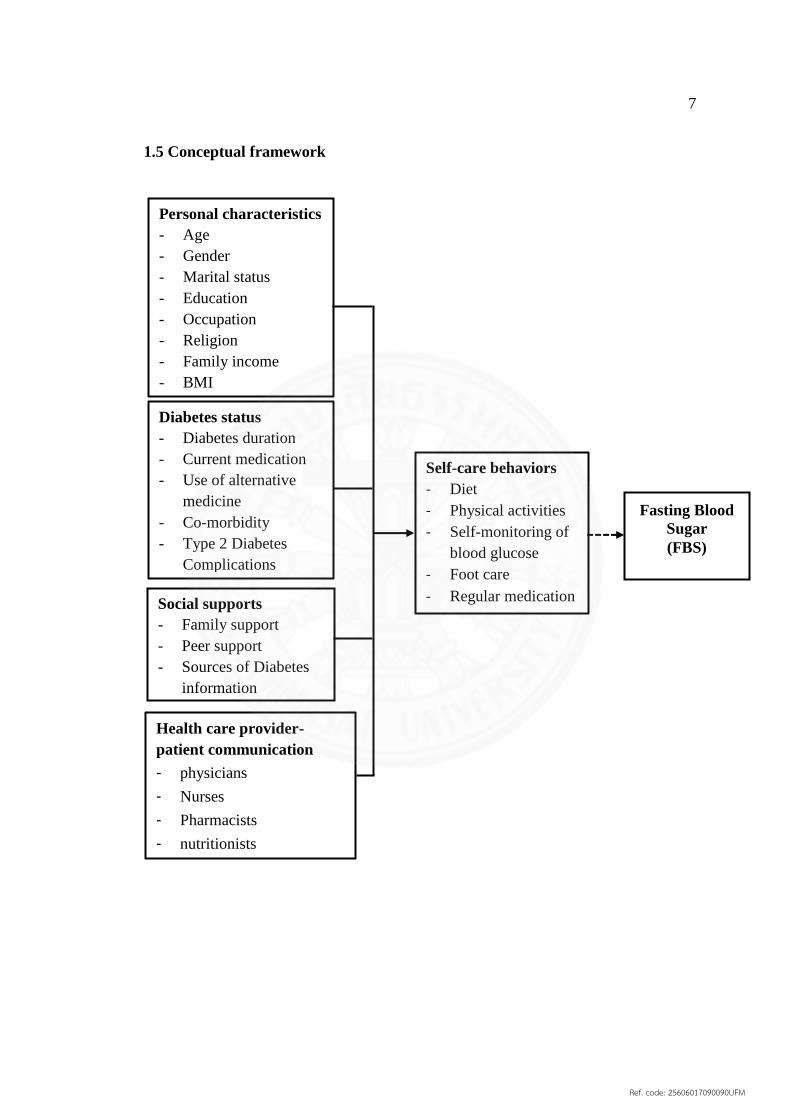
1.5 Conceptual framework
Personal characteristics
- Age
- Gender
- Marital status
- Education
- Occupation
- Religion
- Family income
- BMI
Self-care behaviors
- Diet
- Physical activities
- Self-monitoring of
blood glucose
- Foot care
- Regular medication
Health care provider-
patient communication
- physicians
- Nurses
- Pharmacists
- nutritionists
Diabetes status
- Diabetes duration
- Current medication
- Use of alternative
medicine
- Co-morbidity
- Type 2 Diabetes
Complications
Social supports
- Family support
- Peer support
- Sources of Diabetes
information
Fasting Blood
Sugar
(FBS)
Ref. code: 25606017090090UFM

8
CHAPTER 2
LITERATURE REVIEW
The content of literature review included the following topics.
2.1 Situation of Diabetes Mellitus in Lao PDR
2.2 Diabetes Mellitus
2.3 Type 2 Diabetes Mellitus
2.4 Theory of self-care
2.5 Self-care behaviors
2.6 Social supports
2.7 Health care provider-patient communication
2.8 Review of relevant research
2.1 Situation of Diabetes Mellitus in Lao PDR
Regarding to WHO statistics in 2016 the population of Lao PDR was
6,802,000. The number of deaths between diabetes during aged 30-69 years was 450
people among these, 280 people was female. The number of deaths people for more
than 70 years was 470, which 310 was female. Therefore, the proportional mortality
estimate of diabetes was 2% of all causes. Moreover, the cause of Diabetes Mellitus
diabetes and related risk factors were diabetes (5.6%), overweight (16.8%), obesity
(3.0%) and physical inactivity (9.0%)(14).
The study of Chanthon X, Et al case-control study to find the risk factors
related with Type 2 Diabetes in Lao patients at OPD in Setthathilath Hospital. As a
result, the levels of education of participants were not different while compared for case
and control (p>0.05). Mean of year of cases had education (Mean=7.60, 95%CI=7.40-
8.40) and group control (Mean=7.30, 95%CI=7.00-7.60) year (p=0.06). Nearly ¼ of
participants was illiterate, 39% was secondary school, 17% was primary school, 15%
was high school, and only 6% was university(15)
Ref. code: 25606017090090UFM

9
Figure 2.1 Diabetes patients at OPD in Mahosot Hospital (Personal contact, OPD
report, 2017)(16)
2.2 Diabetes Mellitus
Diabetes Mellitus refers to a number of chronic disorders commonly
characterized by the pancreas does not produce enough insulin or the human body
cannot productively used the insulin from the pancreas, it is the cause for
hyperglycemia, which can be unusual of body system function such as blood vessel,
eyes kidney and nerves, there are many commons was long time can effectively to the
complications such as microvascular disease, retinopathy(17). According to the
American Diabetes Association (ADA) and the World Health Organization bases on 4
etiologies of the diabetes are as follows:
Type 1 Diabetes Mellitus
Type 1 Diabetes Mellitus is caused from an autoimmune reaction that the
body's immune system were bear down the beta cell that producing insulin in the
pancreatic. Therefore, the human body cannot produce insulin or none to very tittle
insulin with insufficiency insulin(18).
Type 2 Diabetes Mellitus
According the Type 2 Diabetes for around 90% of all Type 2 Diabetes
cases. Therefore, hyperglycemia is caused of the pancreas cannot producing insulin or
the body cannot ability to respond fully to insulin, defined as insulin resistance. While
48385132
6237
2995 30143606
18432118
2631
0
1000
2000
3000
4000
5000
6000
7000
Year 2015 Year 2016 Year 2017
Nu
ber
of
DM
Total Female Male
Ref. code: 25606017090090UFM

10
a state of insulin resistance, insulin is ineffective and as a results initially inspire an
increase in insulin production to reduce increasing glucose levels but for a long time a
state of relative inadequate production of insulin can develop(18).
Gestational Diabetes Mellitus
Gestational Diabetes is the first ascertained during pregnancy is sorted as
either Gestational Diabetes Mellitus (GDM). Women with triflingly elevated blood
glucose levels are sorted as having GDM and women with large elevated blood glucose
levels are sorted as women with hyper-glycemic in pregnancy. there were estimated
that 75-90% of cases were high blood glucose during pregnancy are Gestational
Diabetes(18).
Specific Types of Diabetes to other causes
The specific Type of Diabetes to other causes are raised blood glucose
levels above the normal range and below the Diabetes Diagnostic thresholds meet
criteria for impaired glucose tolerance (IGT) based on a two hours post 75g oral, load
or impaired fasting tolerance (IGT). These conditions are also called intermediate
hyperglycemic or prediabetes(18).
2.3 Type 2 Diabetes Mellitus
Type 2 Diabetes is based on blood glucose checking with diagnosis, which,
wherever possible, should use venous samples. Newly, the American Diabetes
Association (ADA) re-investigated the criteria for impaired fasting glycaemia (IFG)
and suggested that the cut-point for IFG should be lowered to a fasting plasma glucose
(FPG) ≥ 5.6 mmol/L (100 mg/dl)(18).
The Values for diagnosing diabetes mellitus, diagnosis criteria have been
debated and updated over decades, WHO state that diabetes is diagnosed by observing
raised levels of blood sugar(18).
Evidence of weight loss and dehydration may be present, and the breath
may smell ketones if the patient presented with ketoacidosis. Older patients may present
with established complications, and the presence of the characteristic retinopathy is
diagnostic for diabetes. Patients with severe insulin resistance may have Acanthosis
Nigerian(19).
Ref. code: 25606017090090UFM
11
Treatment of Type 2 Diabetes Mellitus
Diabetes is a chronic disease metabolic condition that cannot be completely
cured but the aim of treatment is to control the blood glucose level.
Firstly, Type 2 Diabetes need to adjust their lifestyle and follow the
treatment regularly, also follow the diet control and physical activities. If the blood
glucose level cannot control by the way, there should have to control by given
medicines to control blood glucose level targets, which the first case should give oral
medicines or injection to control blood glucose level(20).
Pharmacological therapy for Type 2 Diabetes
- Metformin, if not contraindicated and if tolerated, is the preferred
initial pharmacological agent for Type 2 Diabetes.
- The newly diagnosed Type 2 Diabetes and markedly symptomatic
and/or elevated blood glucose levels or A1C are test considered to use
insulin therapy (with or without additional agents).
- In case of noninsulin monotherapy at maximum tolerated doses cannot
achieved or maintained the A1C target over 3 months, add a second
oral agent, a Glucagon Like Peptide-1 (GLP-1) receptor agonist, or
basal insulin.
- A patient-centered approach should be used to guide choice of
pharmacological agents. Considerations include efficacy, cost,
potential side effects, weight, comorbidities, hypoglycemia risk, and
patient preferences.
- Due to the progressive nature of Type 2 Diabetes, insulin therapy is
eventually indicated for many patients with Type 2 Diabetes(21).
Type 2 Diabetes complications
Type 2 Diabetes complications is the chronic state of hyperglycemia in
Diabetes Mellitus has been a main problem to manage, the prevalence of Type 2
Diabetes complications is increasing, while probable the factors of uncontrolled blood
glucose with standard and self-care behaviors lifestyle changes for the long time(22).
People with Type 2 Diabetes have been increasing the risk of developing a number of
serious for many complications, which are mainly high blood glucose levels, lower
Ref. code: 25606017090090UFM

12
insulin for long time can predict cardiovascular disease, nephropathy, neuropathy,
diabetic foot. There are many severe complications from hyperglycemia(23).
Cardiovascular complication
Cardiovascular complications refer a major to showed the high diseases and
more death rate in people with diabetes and that is the main point of the primary
control(24). While includes cerebrovascular accident, coronary artery disease, and
peripheral artery disease, there are many cause for people with Diabetes compared
before doesn’t at risk(25).
Diabetic Neuropathy
Diabetic neuropathy occurred after people with Diabetes for a long time
was more than half of all individuals with Diabetes finally developing neuropathy, with
the cause of cases for lifetime one or more lower extremity elimination evaluated in
some population to be up to 15%(26). Diabetic neuropathy includes a wide range of
clinical and subclinical syndrome and effects all type of the peripheral nervous system
neurons. 50 to 75% of all ulcerations and non-trauma amputations result from Diabetic
neuropathy, and accounts for more hospital admissions that all the other Diabetic
complications collectively(27).
Diabetic Nephropathy
Diabetic nephropathy is very common effect in renal failure in many
countries, and there is the large burden of nephropathy in the Asia Pacific region. The
first stages are showing by an increase albumin in urinary (microalbuminuria), it can
effect to microalbuminuria. Therefore, creatinine is increasing in serum, ultimately
leading to renal failure and the need for dialysis and transplantation. In parallel to the
progressive decline in renal function(28).
Diabetic foot ulcer
Diabetes occur prone to multiple complications such as Diabetic foot ulcer.
There is many common complication of Type 2 Diabetes that has shown an increasing
trend over previous decades. It is estimated that 15% of Type 2 Diabetes suffer from
Diabetic foot ulcer during their lifetime. Although accurate figures are difficult to
obtain for the prevalence of Diabetic foot ulcer. The prevalence of Diabetic foot ranges
from 4%-27%(29).
Ref. code: 25606017090090UFM
13
2.4 Theory of self-care
The concept of self-care originated from the theory of self-care which was
formulated by Dorothea Orem in 1971 as a ground base for her nursing concept of
practice in which she described self-care as a human regulatory function and assumed
that people were distinct individuals and should be self-reliant and responsible for their
own care and others in the family needing care. Personal knowledge of potential health
problems is necessary for promoting self-care behaviors. Orem’s defines self-care as
the practice of activities that individuals initiate and perform on their own behalf in
maintaining life, health, and wellbeing. The theory includes three concepts, with are the
concept of self-care agency, the therapeutic self-care demand and the self-care
requisites. Self-care agency is defined for the human can engaging in self-care condition
by age development, life experience in socio-cultural orientation, health, and available
resource. Therapeutic self-care demand is the sum of self-care actions to be performed
in some duration in order to meet self-care requisites by using valid methods and related
sets of operations and actions. The self-care requisites are the actions directed towards
provision of self-care and divided into three categories which are Universal self-care
requisites, Developmental self-care requisites and health deviation of self-care.
Universal self-care requisites are the needs that are common to all individuals
associated with life processes and the maintenance of the integrity of human structure
and functioning, and identifies these requisites as the maintenance of sufficient air,
water and food, the provision of care associated with elimination process, the balance
between activity and rest, between solitude and social interaction, the prevention of
hazards to human life well-being, and promotion of human functioning. Developmental
of self-care requisites is associated with developmental processes, and derived from a
condition, or associated with an event such as adjusting body changes. Health deviation
are the needs resulting from disability, illness, or injury. These include; seeking and
securing appropriate medical assistance, effectively carrying out medically prescribed
measures, modifying self-concepts in accepting oneself as being in a particular state of
health and in specific forms of health care and learning to live with effects of pathologic
conditions(30).
Ref. code: 25606017090090UFM

14
For many individuals with Diabetes, the most challenging part of the
treatment plan is determining what to eat. It is the position of the American Diabetes
Association that there is not a one-size-fit-all eating pattern for individuals with
Diabetes. Therefore, it is important that all members of the health care team be
knowledgeable about Diabetes nutrition therapy and support its implementation(21).
2.5 Self-care behaviors
WHO defines self-care in health as any activities of individuals, families,
and communities undertaken with the intention of enhancing health, preventing disease,
limiting illness and restoring healthy. These activities are derived from knowledge, and
skills from the pool of both professional and lay experience. There are undertaken by
lay people on their own behalf, either separately or in participative collaboration with
professionals(31). The study of Nyunt SW, 2010 in YANGON, MYANMAR showed
that 30.8% had good self-care behaviors and 55.3% had fair self-care behaviors but the
prevalence of good glycemic control was 27.1% while was quite low. The patients had
inadequate diabetes self-care. Therefore, this low proportion of good glycemic control
was consistent with the low proportion of self-care for diet (33.8%) and physical
activities were 54.9%(32).
Self-care behaviors among Type 2 Diabetes were perception the information
form health care provider. Also, patients had experiences with Type 2 Diabetes Mellitus,
while opportunity to communication and shared experiences for self-care behaviors(33).
Self-care behaviors which are related to Type 2 Diabetes are these as
follow:
Diet
A suitable diet for Type 2 diabetes is considered the same as other without
Type 2 Diabetes. The diet for the patients with Diabetes is not different from that
considered healthy for everyone. The recommendation for Type 2 Diabetes is 1 gm of
protein/kg body weight and < 35% total energy intake for the total fat.
Dietary intake is one of the important aspect of maintaining blood glucose
level as well as intervention form prediabetes. In many countries, Medical Nutrition
Therapy is recommended for Diabetes patients and the effectiveness of the dietary plan
Ref. code: 25606017090090UFM

15
has been proven by many researches: the main goal of medical nutrition therapy is “to
achieve the optimal metabolic control by maintaining the blood glucose levels close to
normal as possible and prevent or treat the Diabetes complications and modify the food
intake as appropriate for the patient(34).
The American Heart Association (AHA) recommended that total carbohydrate
range from 45% of calories alone up to 100% combined with monounsaturated fat. Also,
fiber intake should be encouraged to take more since it slows the glucose and slower
digestion makes patients increase satiety(35). Moreover, Diabetes patients need to reduce
the fat intake especially reduce saturated fat and dietary cholesterol since it is the main
source to increases the plasma LDL cholesterol. Therefore, patients with Diabetes
appear to be more sensitive to dietary cholesterol than the general public. Major sources
of trans fatty acids in the diet includes products made from partially hydrogenated oils
such as baked (including crackers and other snack foods), cookies, doughnuts, breads,
and products like fries or chicken fries in hydrogenated shortening, animal sources,
including dairy products, provide smaller amounts or trans fatty acids. The effect of
Trans fatty is similar to saturated fats in raising plasma LDL cholesterol. In acids is
lower plasma HDL cholesterol. Therefore, intake of intake of trans fatty acids should
be limited(36).
Diet control was consistently described by the participants as: reducing
their food intake and avoiding sweet food and drinks in order to maintain good intake
good glycemic control. The interview data indicated that patients had a clear
understanding of the types of foods that increase their blood sugar levels, such as: rice
and bread, which are high in carbohydrates, sweet cakes their blood sugary drinks. This
understanding was reflected in their practice, where they were concerned about
controlling their sugar level by reducing their practice, where they were concerned
about controlling their sugar levels by reducing their intake of rice, sweet foots and
sweet drinks. However, the patterns of diet control among the participants in this study
varied. From the data, it can be observed that the patients’ responses on adherence to
diet control varied, and included following a strict diet, a moderately flexible diet, or a
very flexible diet(37).
Ref. code: 25606017090090UFM

16
Smoking
Smokes with Diabetes have high risks for serious complications, including
heart and kidney disease. Poor blood how in the legs and feet that can lead to infectious,
ulcer, and possible complications. In fact, smokers are 30–40% more likely to develop
type 2 diabetes than nonsmokers. And patients with Diabetes who smoke are more
likely than nonsmokers to have trouble with insulin dosing and with controlling blood
glucose level. The more cigarettes to smoke, the higher the risk for Type 2 Diabetes
and makes Diabetes harder to control. If Type 2 Diabetes and smoke are more likely to
have serious health problems.
Thailand populations with Diabetes (those who have never been diagnosed
and who have been diagnosed) have history with diagnosed with heart disease and
stroke have been smoking were 11.1%, 13.2% 31.4% 8.8% and 20.4% respectively, the
proportion of smoking by male were high more than female, there are have classify
with persons have been diagnosed and the persons never check were prevalence of
smoking similar. But the person who are aware of disease have a lower prevalence of
smoking than the persons who do not following the disease(38) as shown in figure 2.1.
Figure 2.2 Smokes with non-Diabetes, Diabetes not checking and Diabetes diagnosed in
Thailand(38)
Alcohol drinking
Alcohol drinking is a factor of important for the risk of Type 2 Diabetes.
Important aspects include the influence of high versus moderate alcohol consumption,
different susceptibilities for male and female and the magnitude of any protective effect
31.9%
1.9%
16.5%
31.2%
0.5%
15.5%18.3%
1.6%
7.9%
0
5
10
15
20
25
30
35
Male Female Total Male Female Total Male Female Total
Non Diabetes Diabetes not checking Diabetes and Diagnosed
Ref. code: 25606017090090UFM
17
of alcohol consumption. The purpose of this commentary is to provide a better
understanding of the epidemiological literature, including the aspects mentioned, by
using meta-analysis(39).
The relationship between alcohol consumption and risk of Type 2 Diabetes
after adjustment for multiple confounders, including body mass index, smoking,
physical activity, and family history of Diabetes (quadratic trend P=.003), compared
with lifelong abstainers, the adjusted relative risk (95% confidence intervals) were 0.08
(0.66-0.96) for those consuming 0.1 to 4.9 g/d, 0.67 (0.50-0.89) for those consuming
5.0 to 14.9 g/d, 0.42 (0.20-0.90 for those consuming 15.0 to 29.9 g/d, and 0.78 (0.34-
1.78) for those consuming 30.0 g/d or more(40).
Physical Activities
Regular physical activity is an important part of the Diabetes management
plan and physical activities can have benefits as well as risk for Diabetes patients. Based
on patients should be encouraged to increase the level of their physical activities, but
the participation in more specific formal exercise program is best. Both aerobic and
resistance training improve insulin sensitivity and metabolic control in Type 1 and Type
2 Diabetes. Several trials have shown that regular exercise reduce the risk of
progression to Type II Diabetes Mellitus by 30 – 60%, and lower long-term
complications and mortality is seen on those with established disease who have the
highest levels of cardio respiratory fitness(19).
Glycemic control
The clinical implication of the favorable impact of Diabetes self-
management education on reductions in glycemic control is critically important because
glycemic control is among the strongest predictors of disease progression and
development of microvascular and macrovascular complications in individuals with
Type 2 Diabetes, suggests that this level of additional improvement in HbA1c would
be associated with better outcomes of significance to patients(41).
In addition to this, ADA recommends to have tight glycemic control which
means keeping the blood glucose level as close to normal as possible and tight control
can prevent or slow the progress the complications of Diabetes for many years. This
means levels between 70 and 130 mg/dl before meals, and less than 180 mg/dl two
hours after starting a meal, with a glycated hemoglobin levels less than 7 percent(42).
Ref. code: 25606017090090UFM
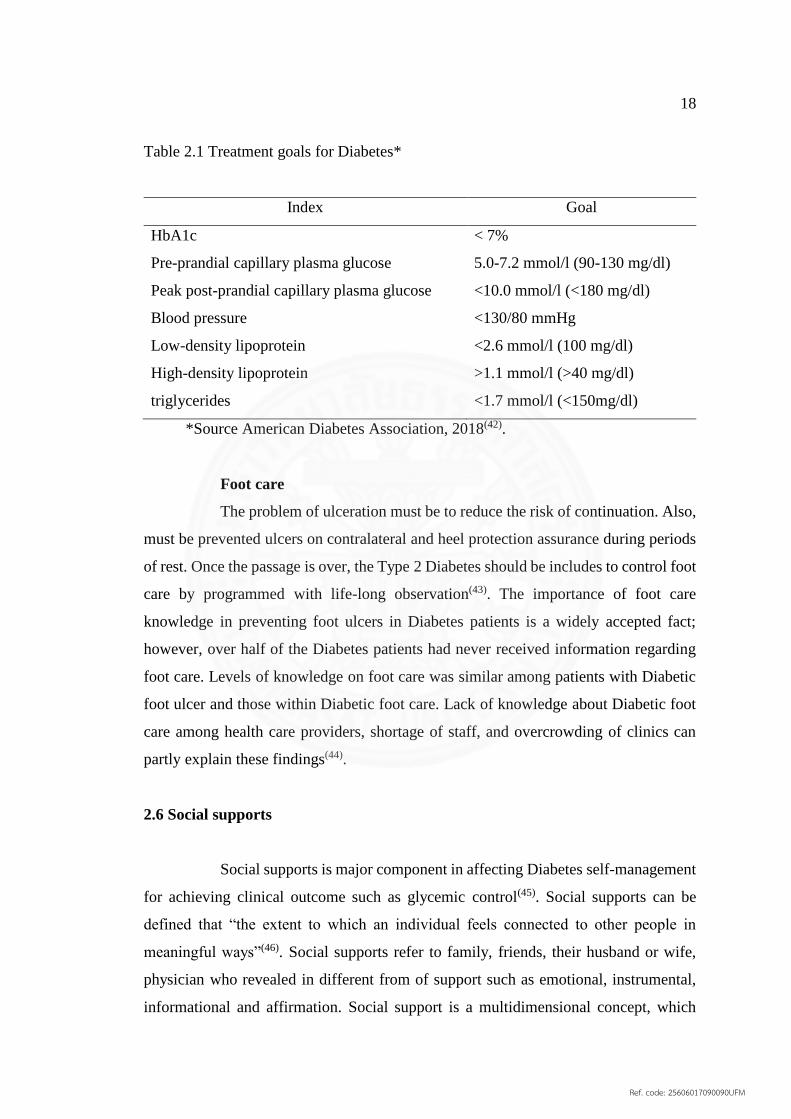
18
Table 2.1 Treatment goals for Diabetes*
Index Goal
HbA1c
Pre-prandial capillary plasma glucose
Peak post-prandial capillary plasma glucose
Blood pressure
Low-density lipoprotein
High-density lipoprotein
triglycerides
< 7%
5.0-7.2 mmol/l (90-130 mg/dl)
<10.0 mmol/l (<180 mg/dl)
<130/80 mmHg
<2.6 mmol/l (100 mg/dl)
>1.1 mmol/l (>40 mg/dl)
<1.7 mmol/l (<150mg/dl)
*Source American Diabetes Association, 2018(42).
Foot care
The problem of ulceration must be to reduce the risk of continuation. Also,
must be prevented ulcers on contralateral and heel protection assurance during periods
of rest. Once the passage is over, the Type 2 Diabetes should be includes to control foot
care by programmed with life-long observation(43). The importance of foot care
knowledge in preventing foot ulcers in Diabetes patients is a widely accepted fact;
however, over half of the Diabetes patients had never received information regarding
foot care. Levels of knowledge on foot care was similar among patients with Diabetic
foot ulcer and those within Diabetic foot care. Lack of knowledge about Diabetic foot
care among health care providers, shortage of staff, and overcrowding of clinics can
partly explain these findings(44).
2.6 Social supports
Social supports is major component in affecting Diabetes self-management
for achieving clinical outcome such as glycemic control(45). Social supports can be
defined that “the extent to which an individual feels connected to other people in
meaningful ways”(46). Social supports refer to family, friends, their husband or wife,
physician who revealed in different from of support such as emotional, instrumental,
informational and affirmation. Social support is a multidimensional concept, which
Ref. code: 25606017090090UFM
19
expects the positive or negative health resulting depend on the quality of patient’s
received social support, the satisfaction of patients in receive the support, or
positive/negative association king of behavior from their source of social support.
However, there are was significant association between social supports and Diabetes
specific quality of life and they also suggest that “social support may positively
influence the initiation and maintenance of Diabetes self-care behaviors”(47). Moreover,
this studied effects of the Diabetic patients’ perceived social support on their quality of
life. It was found that social support could enhance quality of life among those patients.
They also suggested that social support increased in Diabetes self-management could
improve glycemic control among those Diabetes Mellitus patients(48).
Peer supports to concern people depicting on lived experience or shared
attribute to provide knowledge, experiences, sensational assistance, help skill practical,
and social interaction to help each other’s. Therefore, the information to support is a
similar person with significantly experiences. Peer supports is one important way that
individuals, families and communities can manage their own health and wellbeing(49).
2.7 Health care provider-patient communication
A study suggested that Health care provider and Diabetes self-care
communication are related significantly with health status among diabetes patients, but
these related are independent. Thus, the results of communication cannot be explained
by good self-care. The important of clinical implication to requires more than clear
communication set up and important effective patterns of Diabetes self-care(50). The
Health care provider-patients communication offers an ideal opportunity to address
patient nonadherence cause of health care providers communication skills contribute to
as much as 50% of the quality of care patients receive(51).
The therapeutic potential of the relationship is based on an intimate
knowledge of the patient and family, their illness and their coping strategies, and an
appreciation of the importance to that individual of a range of psychological, social,
environmental and spiritual factors(52).
Ref. code: 25606017090090UFM

20
Physician-patient communication
Physician-patient communication were has been for a long time pretended
to be a straightforward relation and confront between an expert in medicine and the
patients in need of medical care. In the past, rapid changes in the health care delivery
system and the social climate have resulted in considerable strain on this relationship.
Ironically, these challenges have also led to increased recognition of the relationship’s
deeper dimension as an intimate interaction between two human beings in issues of
health, illness and sometimes death(53).
Nurse-patient communication
Nurse-patient communication to review possible effective communication
methods. the most important communication obstacle are lack of skills and self-
efficacy, possibly because nurses work in a context where they have to perform
biomedical examinations and then perform patient-centered counseling from a
biopsychosocial approach. Training in patient-centered counseling does not seem
helpful in overcoming this paradox. Rather, patient-centeredness should be regarded as
a basic condition for counseling, whereby nurses and patients seek to cooperate and
share responsibility based on trust(54).
Pharmacist-patient communication
Pharmacists have important roles in managing the therapy of patients with
Type 2 Diabetes and improving patient care. Pharmacists titrate medications; reinforce
patient education; and address care gaps, such as medication adherence, through these
efforts and more, pharmacists help to improve patient care. Thus, it is important to
demonstrate improved health outcomes through pharmacist contributions to diabetes
management(55).
Nutritionist-patient communication
Information concerning the nature of nutritionist-patient relationships is
very limited. Nutritionist’s skills, attributes, and beliefs towards nutrition counseling
during a lifestyle modification intervention program, and whether this affected the
patient’s weight outcome(56).
Ref. code: 25606017090090UFM

21
2.8 Review of relevant studies
2.8.1 Personal characteristics and self-care behaviors
A study found age associated with self-care behaviors which was
similar to another study in Thai population which showed patients who 60 years or
older had better self-care behaviors more than patients were less than 60 years(57). In
addition, the study that long duration of Diabetes and being female associated with
poorer self-care among adolescents with Type 1 Diabetes(58). Moreover, the study that
self-care behavior scores were significantly influenced with social support, genders,
education, economical status, and religious beliefs of older diabetic patients in
Taiwan(59). McCollum et al, found that female Diabetic scored less than male on
measurement of health status and functioning which could affect self-care activities(60).
Dupre and Matthew E, who studied a 20-year longitudinal data suggested that education
related to both individuals and accumulated number of behavioral, social, and economic
health-risks, which in turn, were related to increasing educational differences in rate of
Diabetes incidence and survival. For hypertension, behavioral risks fully account for
education’s negative affect on Diabetes onset whereas education differences in survival
are best explained by the accumulation of social and economic risks. For heart attack,
a combination of behavioral, social and economic risks mediate the association between
education and incidence, but neither the individual nor the accumulated health-risks
could account for education’s positive affect on surviving after a heart attack. Similar
findings for Diabetes and stroke are also discussed(61). The study of Khonrom M,
Showed that gender was not significant with self-care behaviors of diabetes mellitus
patients in Bangnampriew Distritct, Chachoengsao Province(62).
2.8.2 Co-morbidity and self-care behaviors
Co-morbidity among patients with Type 2 Diabetes was both minor
and main depression are strongly associated with increased mortality. Further research
will be necessary to disentangle causal relationships among depression, behavior risk
factors, Diabetes complications, and mortality(63). The researcher identified raised rates
of depression in Type 2 Diabetes, though there is a need to well controlled and better-
Ref. code: 25606017090090UFM
22
reported studies to inform the development of effective treatments for depression in
these patients(64).
Hypertension: The coexistence of Diabetes and hypertension, especially
when they are not adequately controlled, substantially increases the risk for onset and
progression of chronic kidney disease and cardiovascular morbidity and mortality.
Although current therapeutic options may slow progression of Diabetic-hypertensive
nephropathy, many of these patients ultimately progress to end-stage renal disease(65).
The threshold for instituting blood pressure-lowering strategies and the target BP for
those on treatment should be 140/80 mmHg in patient with Diabetes because of the
vulnerability of their vascular endothelium. This threshold should be lowered 10 mmHg
in those who already have evidence of complications.
Obesity: The link between obesity, poor health outcomes and all-cause
mortality is well established. Obesity increases the likelihood of Diabetes. It also
negatively affects reproductive performance. Overweight and obesity for example:
BMI ≥25 kg/m2 and ≥30 kg/m2 respectively were estimated to account for 3.4 million
deaths per year and 93.6 million daily’s in 2010. To achieve optimal health, the median
BMI for adult populations should be in the range 21–23 kg/m2, while the goal for
individuals should be to maintain a BMI in the range 18.5−24.9 kg/m2. The risk of
comorbidities increases with a BMI in the range 25.0−29.9 kg/m2, and the risk is
moderate to severe with a BMI greater than 30 kg/m2
Dyslipidemia: Type 2 Diabetes have a high residual risk for cardiovascular
disease (CVD) and adverse outcomes despite statin therapy and lifestyle modifications.
Particular to individuals with Diabetes is the pattern of elevated triglycerides, small
dense low density low density lipoprotein cholesterol, and reduced levels of high
density lipoprotein cholesterol, described as dyslipidemia of Diabetes(66).
2.8.3 Family supports and self-care behaviors
Tang et al, conducted an observational cross-sectional study to
examine the relationship of social support and Diabetes specific quality of life and self-
care behaviors among African American with Type 2 Diabetes. The finding indicated
that social support influence Diabetes specific quality of life and self-care behaviors
through different dimensions of support. Satisfaction with support was a predictor for
Ref. code: 25606017090090UFM

23
improved Diabetes specific quality of life and blood glucose monitoring. Positive
support behavior predicts healthy eating and physical activities(47).
2.8.4 Physician-patient communication and self-care behaviors
Physician- patient communication of Piette et al to conducted a cross-
sectional survey among ethnically diverse population to examine the relation between
general and specific physician-patient communication with Diabetes Mellitus self-care
and the result was that both dimensions of communication were both independently
associated with self-care(67). Aikens et al, demonstrated that general physician-patient
communication was association with mental functioning, while Diabetes specific
physician-patient communication was associated with glycemic control, but these
associations were not mediated by self-care behaviors, which were independently
associated with Diabetes outcome(50). Remember of self-care information given during
communication with health care provider was associated with an increased home based
self-care by patients and their families. By consulting with Diabetes educator had a
significant role in improving patient self-care(68).
Ref. code: 25606017090090UFM
24
CHAPTER 3
MATERIALS AND METHODS
The content of material and methods included the following:
3.1 Study design
3.2 Study site
3.3 Population
3.4 Sample size
3.5 Inclusion and exclusion criteria
3.6 Research Instrument
3.7 Ethical consideration
3.8 Data collection
3.9 Data management and analysis
3.1 Study design
This cross-sectional study aimed to determine self-care behaviors among
Type 2 Diabetes.
3.2 Study site
Mahosot Hospital in Vientiane Capital, Lao PDR
3.3 Population
Type 2 Diabetes who attended OPD Mahosot Hospital, Vientiane Capital,
Lao PDR in April 2018.
3.4 Sample size
A sample size was calculated by the following formula:
Ref. code: 25606017090090UFM
25
𝑛 =𝑍𝛼/2
2 𝑃 ( 1−𝑃 )
𝑑2 =1.962(0.369)(1−0.369)
(0.066)2 = 205
𝛼 = significance level set at 5%
Zα/2 = the standard normal score at 𝛼 2⁄ = 1.96
P = Proportion of poor control blood glucose level among Type 2 Diabetes at 36.9%(69)
d = different between estimated proportion and true proportion in population (maximum
allowable error = 6.6%)
An estimated sample size was calculated as 205 Type 2 Diabetes and included with
10% which produced a total sample size was 226.
3.5 Inclusion and exclusion criteria
Inclusion criteria:
Type 2 Diabetes who had been diagnosed by doctor, who attended at
OPD in Mahosot Hospital, Vientiane Capital, Lao PDR.
Patients who had been treated with anti-hyperglycemic medications for
at least 6 months.
Age 30 years or older and able to communicate in Lao language.
Exclusion criteria:
Type 2 Diabetes who was in severe condition that could not give
information
3.6 Research Instrument
A structured questionnaire had been developed in English with consultation
of experts for content validity. Then it was translated into Lao language. It included 5
parts as following:
Part I General characteristics of the patient consisted of age, gender,
marital status, education, occupation, religion, family income, Health security and
history of Diabetes Mellitus among family member.
Part II Medical status consisted of duration of Type 2 Diabetes, current
medication, use alternative medicine, co-morbidity, Type 2 Diabetes complication,
Ref. code: 25606017090090UFM
26
blood glucose level, and body mass index (BMI) was checked from the laboratory
report and filled in the space provided in the questionnaire.
Part III Self-care behaviors: self-care behaviors of Type 2 Diabetes in the
last one month for each questions followed by diet, physical activities, self-monitoring
of blood glucose, foot care and regular medication. There were consisted of 23 items,
range of score was from “0” to “3” and 2 items not score. The score range 0 to 63. The
total score for each individuals was calculated and classified into three levels. As
modify from Benjamin Bloom classification(69):
- Poor levels <60% of total score (0 - 36)
- Moderate levels 60-80% of total score (37 - 50)
- Good levels >80% of total score (52 - 63)
Part IV Social supports: Social supports consisted of 13 items of family
supports received by the Type 2 Diabetes. Range of scores are from “0” to “2” and
scores was given as followed for every questions: never=0, sometimes=1, always=2. If
questions did not applied to the respondent, she/he could choose N/A (not applicable)
and score of “0” was be given. The score of family supports range 0 to 26. The total
score for each individuals was calculated and classified into three levels. Benjamin
Bloom classification:
- Poor levels <60% of total score (0 – 14)
- Moderate levels 60-80% of total score (15 – 20)
- Good levels >80% of total score (21 – 26)
Peer supports consisted 6 items received by the Type 2 Diabetes. Range of
scores are from “0” to “2” and scores was given as followed for every questions:
never=0, sometimes=1, always=2 and score of “0” was be given. The score of family
supports range 0 to 12. The total score for each individuals was calculated and classified
into three levels. Benjamin Bloom classification:
- Poor levels <60% of total score (0 – 6)
- Moderate levels 60-80% of total score (7 – 9)
- Good levels >80% of total score (10 – 12)
Sources information consisted of 2 items followed by some information on
Type 2 Diabetes Mellitus from where and what to known.
Ref. code: 25606017090090UFM
27
Part V Health care provider-Patient communication: this part were
conducted with communication with Type 2 Diabetes by physicians, nurses,
pharmacists and nutritionists. The questionnaires consisted of 13 items for health care
provider-patient communication. Score 0 to 2 was assigned as followed for every
question: never=0, sometimes=1, and always=2. Minimum score was 0 and maximum
score was 26. The total score for each individuals was calculated and classified into
three levels.
The satisfaction to health care provider clinic services consisted of 14 items
in a 5 points Likert scale range from Satisfaction levels: 1= not very satisfed, 2= not
satisfied, 3= moderate, 4= satisfied, 5= very satisfied. Range of scores are from “1” to
“70”. The total score for each individuals was calculated and classified into three levels.
Benjamin Bloom classification:
- Poor levels <60% of total score (1 – 41)
- Moderate levels 60-80% of total score (42 – 56)
- Good levels >80% of total score (57 – 70)
3.7 Ethical consideration
An ethical clearance from National Ethic Committee for Health Research
of Lao PDR had reviewed and approved which the certificate approval was
No.044/NECHR. Also requested to submit the research proposal to Administrators of
Mahosot Hospital. During the interview the researcher informed participants the
objectives of this study and allowed them to ask any questions. The researcher answered
any questions until participants totally understood. The participants could stop
answering questions at all time during the interview without giving any reasons. All
individual information were not disclosed to others or public. The result was showed as
a whole without identify of individual patient.
Ref. code: 25606017090090UFM

28
3.8 Data collection
Data collection started after obtaining an approval of National Ethic
Committee for Health Research, Lao PDR. The permission from Mahosot Hospital was
also obtained before conducting the study. Two nurses were recruited as assistants for
data collection who worked at Infectious Department, Mahosot Hospital. The
researcher explained clearly to 2 assistants. Data collection with Type 2 Diabetes were
interviewed followed by inclusion and exclusion criteria. The service hour of OPD at
Mahosot Hospital for Type 2 Diabetes is opened three days a week; Tuesday in the
afternoon at 1:00 pm until 4:00 pm, Wednesday all day and Friday all day. The number
of participants to interview were 50 cases per day. Each questionnaire took around 15
minutes to be completed.
3.9 Data management and analysis
After data collection, researcher checked questionnaires for its completion.
All questionnaires were coded and scored. The data were entered by using Epi-Data
program. Descriptive statistics were utilized in order to describe each variables
followed the conceptual framework. Measure of central tendency which including
frequency, percentage, mean, standard deviation, and minimum and maximum.
Inferential statistics: ANOVA and multiple linear regression were used to determine
associations between independent and dependent variables. The significantly level was
set at 5%.
Ref. code: 25606017090090UFM

29
CHAPTER 4
RESULTS AND DISCUSSIONS
This study was conducted at Mahosot Hospital. Total of 226 Type 2 Diabetes
were included into the study. The results were presented as following:
4.1 Personal characteristics
4.2 Diabetes status
4.3 Self-care behaviors
4.4 Social supports
4.4.1 Family supports
4.4.2 Peer supports
4.4.3 Source of information of Type 2 Diabetes Mellitus
4.5 Health care provider-patient communication
4.6 Satisfaction to health services system
4.7 Factors associated with self-care behaviors
4.8 Self-care behviors and Fasting Blood Sugar
4.9 Discussion
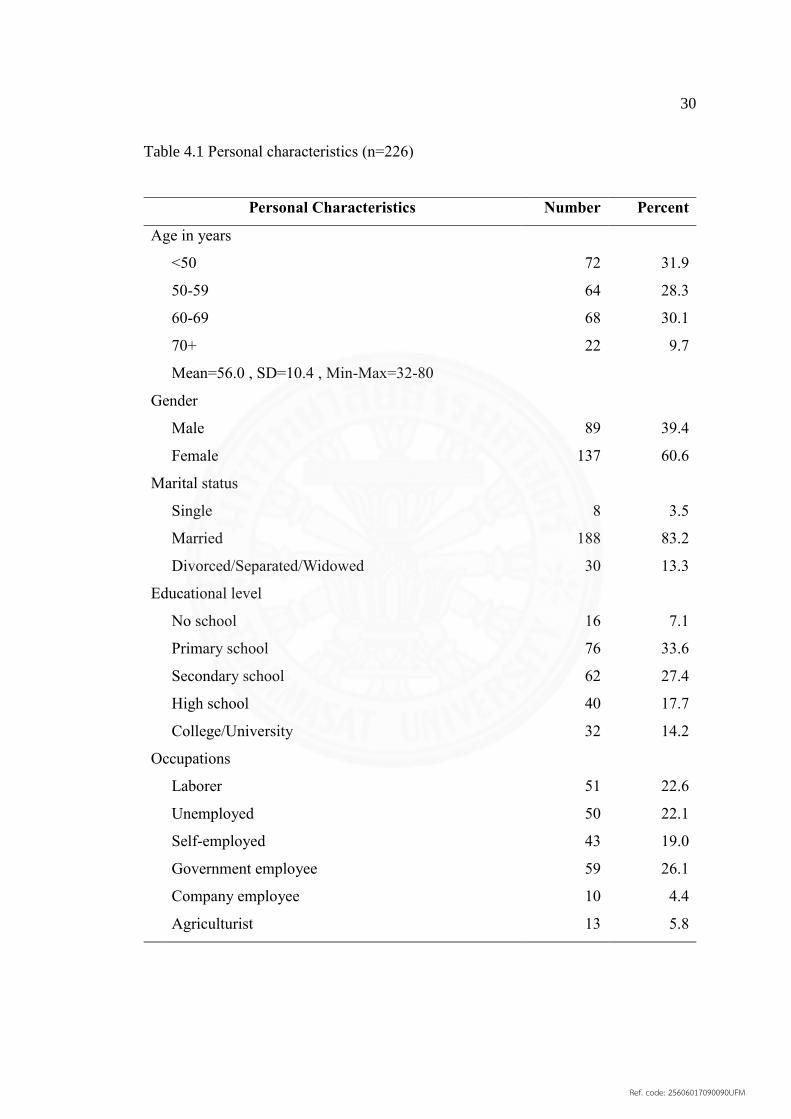
4.1 Personal characteristics
Most of participants had 60.2% were age 32-59 years. Most of them
(60.6%) were famale. The majority of them were married (83.2%). Most participants
attended primary school and scondary school accounting for 33.6% and 27.4%
respectively. Government employee were 26% which followed by laborer group
(22.6%) and unemployed group (22.1%). Most of participants were buddhist (94.2%).
Most of participants (26.5%) had family income between 500,000 – 1 M LAK/month,
and 20.8% which their income was more than 2.5 M LAK/month. 135(59.7%) of
participants had no health insurance. 79.1% of participants who had health security was
public social security. 152(67.3%) of participants had no history of Diabetes Mullitus
among family mambers. 50% of participants had history of DM was mother and 25.7%
was father as described in Table 4.1
Ref. code: 25606017090090UFM
30
Table 4.1 Personal characteristics (n=226)
Personal Characteristics Number Percent
Age in years
<50 72 31.9
50-59 64 28.3
60-69 68 30.1
70+ 22 9.7
Mean=56.0 , SD=10.4 , Min-Max=32-80
Gender
Male 89 39.4
Female 137 60.6
Marital status
Single 8 3.5
Married 188 83.2
Divorced/Separated/Widowed 30 13.3
Educational level
No school 16 7.1
Primary school 76 33.6
Secondary school 62 27.4
High school 40 17.7
College/University 32 14.2
Occupations
Laborer 51 22.6
Unemployed 50 22.1
Self-employed 43 19.0
Government employee 59 26.1
Company employee 10 4.4
Agriculturist 13 5.8
Ref. code: 25606017090090UFM

31
Table 4.1 Personal characteristics (n=226) (cont.)
Personal Characteristics Number Percent
Religion
Buddhist 213 94.2
Christian 3 1.3
Animist 10 4.4
Family income (LAK/Month)
500,000 – 1,000,000 60 26.5
1,100,000 – 1,500,000 39 17.3
1,600,000 – 2,000,000 45 19.9
2,100,000 – 2,500,000 35 15.5
>2,500,000 47 20.8
Health security
No 135 59.7
Yes 91 40.3
Public Social Security 72 79.1
Corporate Social Security 13 14.3
Social Security for people 4 4.4
Community Social Security 2 2.2
History of DM among family member
No 152 67.3
Yes* 74 32.7
Father 19 25.7
Mother 37 50.0
Brothers 15 20.3
Sisters 18 24.3
Grandparents 8 10.8
*multiple responses
Ref. code: 25606017090090UFM

32
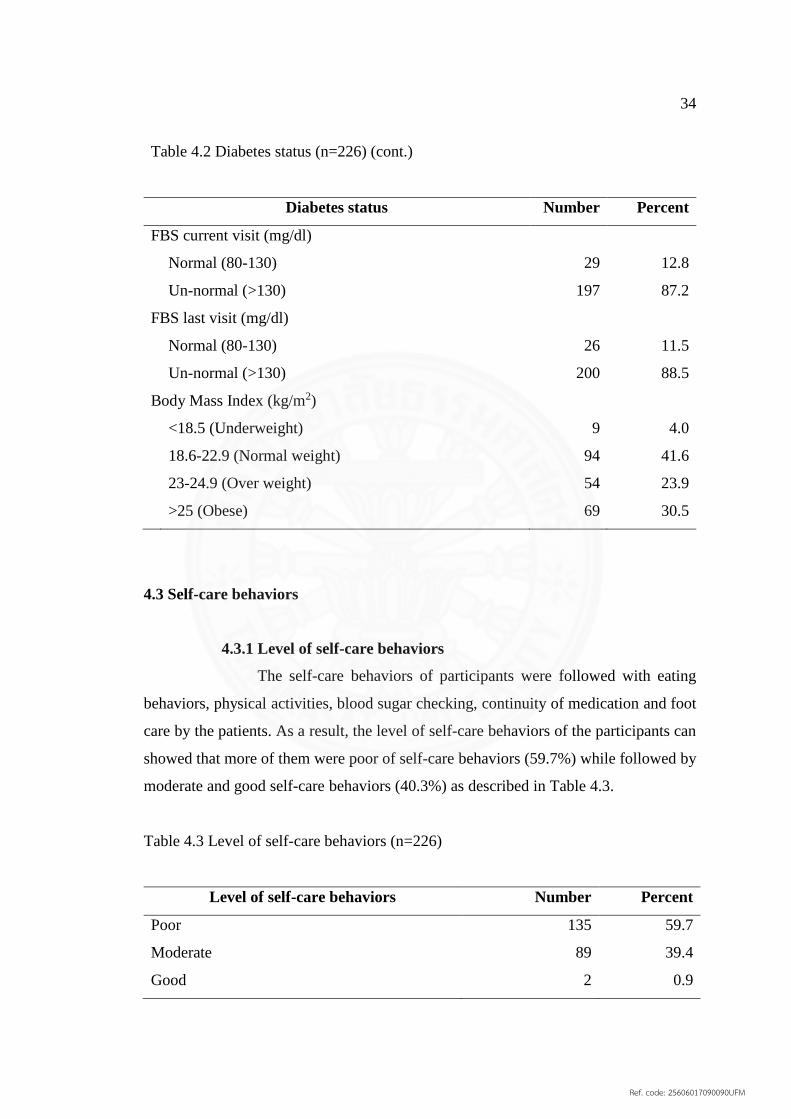
4.2 Diabetes status
The duration of being diagnosed as Type 2 DM range from 1-31 years with
an average 5.89 years. The common of current medications were sigle oral
hyperglycemic (45.1%), combination of OHA (23.9%), and insulin injection (239%).
About 50(22.1%) informed using alternative medicine, and herbal drugs (19.5%) was
the commonest. Slightly more than half (54.0%) experiences co-morbidities were
Diabetic Neuropathy (38.9%) and Diabetic Retinopathy (28.8%).
Fasting Blood Sugar are taken from the medical recored at last and current
visits, majortly of them (88.5%) and (87.2%) were more than 130mg/dl. In regarding
to Body Mass Index, 54.4% was overwight and Obese. Only 41.6% was at normal
weight as described in Table 4.2
Table 4.2 Diabetes status (n=226)
Diabetes status Number Percent
Duration of Type 2 DM (years)
1 36 15.9
2 40 17.7
3 31 13.7
4 17 7.5
5-9 52 23.0
10-19 40 17.7
20 + 10 4.4
Mean=5.89, SD=5.63, Min=1, Max=31
Current medication
Single oral hyperglycemic agent (OHA) 102 45.1
Combination of (OHA) 54 23.9
Insulin injection 54 23.9
(OHA) and Insulin injection 13 5.8
No medication 3 1.3
Ref. code: 25606017090090UFM

33
Table 4.2 Diabetes status (n=226) (cont.)
Diabetes status Number Percent
Using of alternative medicine
No 176 77.9
Yes* 50 22.1
Herbal 44 19.5
Healthier foods 5 2.2
Moxibustion 3 1.3
Acupuncture 2 0.9
Co-morbidity
No 104 46.0
Yes* 122 54.0
Hypertension 100 82.0
Dyslipidemia 55 45.1
Obesity 15 12.3
Other(Gastrilitis,Allergic,Hypotension,Tryglyceride,
Hyperthyriodism,TB) 7 5.7
Type 2 Diabetes complications
No 102 45.1
Yes* 124 54.9
Diabetic Neuropathy 88 38.9
Diabetic Retinopathy 65 28.8
Heart disease 22 9.7
Diabetic Nephropathy 18 8.0
Diabetes foot/amputation 15 6.6
Peripheral vascular disease 8 3.5
Vertigo 1 0.4
*multiple responses
Ref. code: 25606017090090UFM
34
Table 4.2 Diabetes status (n=226) (cont.)
Diabetes status Number Percent
FBS current visit (mg/dl)
Normal (80-130) 29 12.8
Un-normal (>130) 197 87.2
FBS last visit (mg/dl)
Normal (80-130) 26 11.5
Un-normal (>130) 200 88.5
Body Mass Index (kg/m2)
<18.5 (Underweight) 9 4.0
18.6-22.9 (Normal weight) 94 41.6
23-24.9 (Over weight) 54 23.9
>25 (Obese) 69 30.5
4.3 Self-care behaviors
4.3.1 Level of self-care behaviors
The self-care behaviors of participants were followed with eating
behaviors, physical activities, blood sugar checking, continuity of medication and foot
care by the patients. As a result, the level of self-care behaviors of the participants can
showed that more of them were poor of self-care behaviors (59.7%) while followed by
moderate and good self-care behaviors (40.3%) as described in Table 4.3.
Table 4.3 Level of self-care behaviors (n=226)
Level of self-care behaviors Number Percent
Poor 135 59.7
Moderate 89 39.4
Good 2 0.9
Ref. code: 25606017090090UFM

35
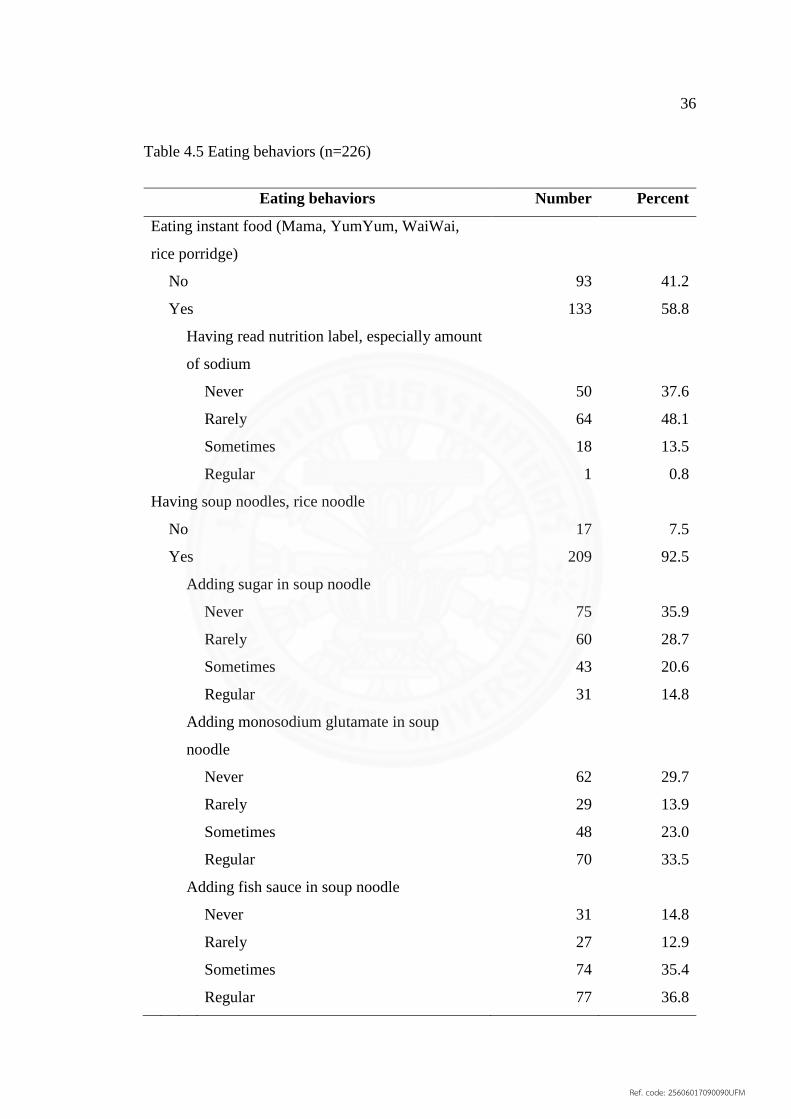
4.3.2 Eating behaviors
As a result, for the levels of eating behaviors, more than half of
participants poor (62.4%) while followed by moderate eating behaviors (30.5%) as
dscribed in Table 4.4
Table 4.4 Level of eating behaviors (n=226)
Level of eating behaviors Number Percent
Poor 141 62.4
Moderate 69 30.5
Good 16 7.1
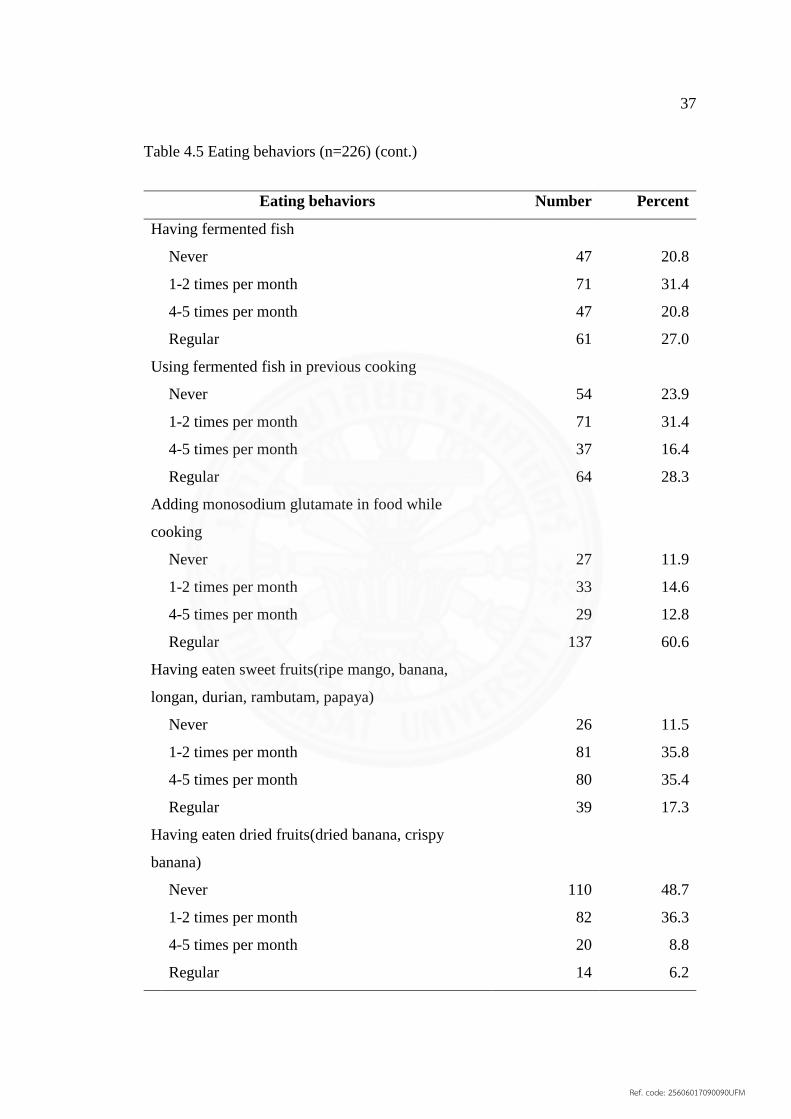
For the eating behaviors, 87.2% of Type 2 Diabetes had meals 3 times a
day, 53.5% of participants eating on times were sometimes, 58.8% of participants had
eating instant food while read nutrition label, especially amount of sodium (48.1%)
were rarely. Also, (92.5%) having soup noodles while (35.9%) never were adding
sugar, (33.5%) regular were adding monosodium glutamate, and (36.8%) regular were
adding fish sauce which followed by sometimes (35.4%). In addition, 31.4% of
participants had fermented fish were 1-2 times per month and 27.0% with regular. Also,
using fermented fish in previous (31.4%) were cooking 1-2 times and (28.3%) were
regular. Moreover, there are adding monosodium glutamate in food while cooking
(60.6%) were regular. For patients were having eaten sweet fruits (ripe mango, banana,
longan, durian, rambutan, papaya…) were (35.8%) 1-2 times per month and (35.4%)
4-5 times per month. Also, nearly half of eaten dried friut (dried banana, crispy
banana,…) (48.7%) were never. Therefore, the patients were to having eaten fish
(34.5%) 3-4 times per week, (27.0%) 5-6 times per week and (26.5%) everyday.
Morever, for eating high fast foods (fried banana, french, fries, coconut milk, fresh
butter,…) (44.7%) were 1-2 times per week while for eaten green vagetables (morning
glory, broccoli, cabbage,…) (33.2%) were 1-2 times per week which followed by
(23.5%) were 5-6 times per week and the same (23.5%) were everyday. However, there
are having eaten food outside home (37.2%) duration 1 day in a week (64.3%) with the
favorite foods were spicy food (38.1%) and fat food (33.3%) as described in Table 4.5.
Ref. code: 25606017090090UFM
36
Table 4.5 Eating behaviors (n=226)
Eating behaviors Number Percent
Eating instant food (Mama, YumYum, WaiWai,
rice porridge)
No 93 41.2
Yes 133 58.8
Having read nutrition label, especially amount
of sodium
Never 50 37.6
Rarely 64 48.1
Sometimes 18 13.5
Regular 1 0.8
Having soup noodles, rice noodle
No 17 7.5
Yes 209 92.5
Adding sugar in soup noodle
Never 75 35.9
Rarely 60 28.7
Sometimes 43 20.6
Regular 31 14.8
Adding monosodium glutamate in soup
noodle
Never 62 29.7
Rarely 29 13.9
Sometimes 48 23.0
Regular 70 33.5
Adding fish sauce in soup noodle
Never 31 14.8
Rarely 27 12.9
Sometimes 74 35.4
Regular 77 36.8
Ref. code: 25606017090090UFM
37
Table 4.5 Eating behaviors (n=226) (cont.)
Eating behaviors Number Percent
Having fermented fish
Never 47 20.8
1-2 times per month 71 31.4
4-5 times per month 47 20.8
Regular 61 27.0
Using fermented fish in previous cooking
Never 54 23.9
1-2 times per month 71 31.4
4-5 times per month 37 16.4
Regular 64 28.3
Adding monosodium glutamate in food while
cooking
Never 27 11.9
1-2 times per month 33 14.6
4-5 times per month 29 12.8
Regular 137 60.6
Having eaten sweet fruits(ripe mango, banana,
longan, durian, rambutam, papaya)
Never 26 11.5
1-2 times per month 81 35.8
4-5 times per month 80 35.4
Regular 39 17.3
Having eaten dried fruits(dried banana, crispy
banana)
Never 110 48.7
1-2 times per month 82 36.3
4-5 times per month 20 8.8
Regular 14 6.2
Ref. code: 25606017090090UFM

38
Table 4.5 Eating behaviors (n=226) (cont.)
Eating behaviors Number Percent
Having eaten fish
Never 8 3.5
1-2 times per week 19 8.4
3-4 times per week 78 34.5
5-6 times per week 61 27.0
Everyday 60 26.5
Having eaten high fat foods(fried banana, French
fries, coconut milk, fresh butter)
Never 87 38.5
1-2 times per week 101 44.7
3-4 times per week 27 11.9
5-6 times per week 7 3.1
Everyday 4 1.8
Having eaten green vegetables (morning glory,
broccoli, cabbage...)
Never 12 5.3
1-2 times per week 75 33.2
3-4 times per week 33 14.6
5-6 times per week 53 23.5
Everyday 53 23.5
Having eaten food outside home
No 142 62.8
Yes 84 37.2
Duration in a week
1 day 54 64.3
2 days 17 20.2
3 days 10 11.9
4 days 3 3.6
Ref. code: 25606017090090UFM

39
4.3.3 Health behaviors
For smoking of participants, 36(15.9%) were having ever smoking,
most of them had 41.7% were quit smoking less than 5 years. In addition, 15(6.6%) of
participants were having smoking 1 pack a day (86.7%), but compared to last 6 months
had 46.7% were less heavy smoking as desribed in Table 4.6
Table 4.6 Smoking habits (n=226)
Smoking Number Percent
Smoking
Never 175 77.4
Having ever smoking 36 15.9
Current smoking 15 6.6
Having ever smoking (n=36)
Duration of quit smoking among ex-smoker
0-4 Years 15 41.7
5-10 Years 12 33.3
>10 Years 9 25.0
Current smoking a day (n=15)
Amount among current smoker
1 pack 13 86.7
2 packs 2 13.3
Smoking as compare to last 6 months
Less heavy smoking 7 46.7
Same heavy smoking 5 33.3
Heavies smoking 3 20.0
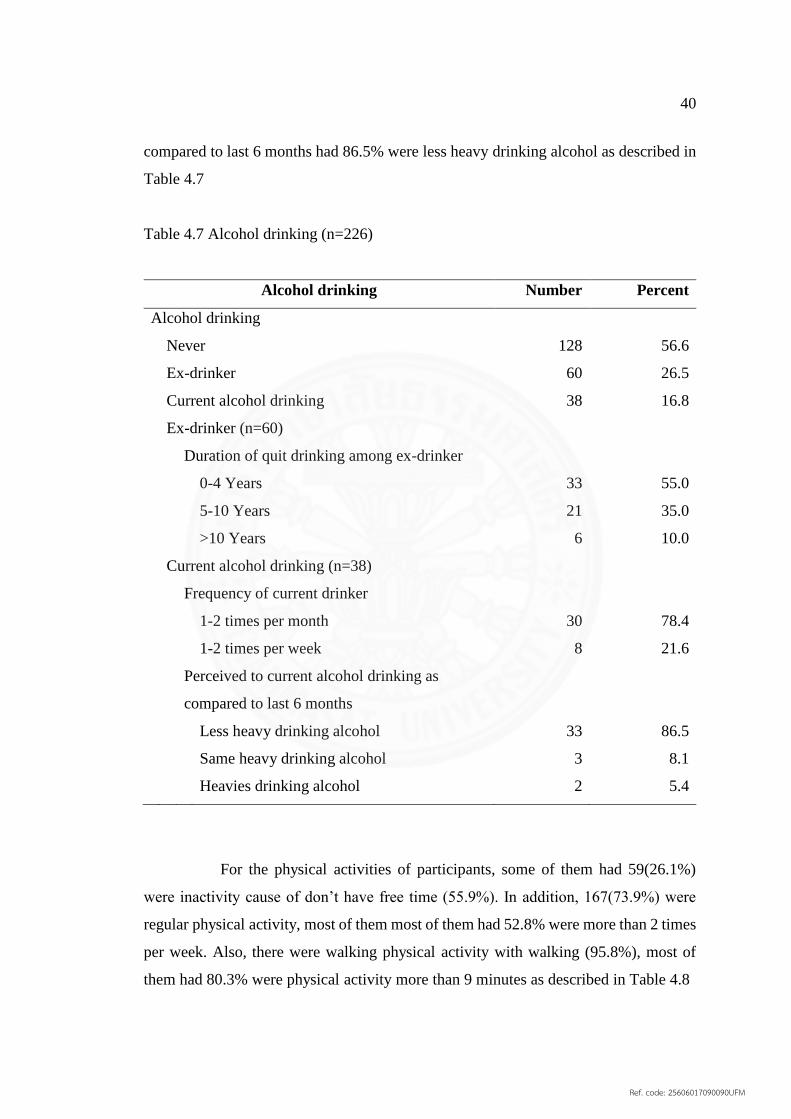
For alcohol drinking of participants, 128(56.6%) were never smoking.
60(26.5%) of participants were ex-drinker, most of them had 55.7% were quit drinking
less than 5 years. In addition, 38(16.8%) of participants were current alcohol drinking,
the frequency of participants drinking had 78.4% were 1-2 times per month, but
Ref. code: 25606017090090UFM
40
compared to last 6 months had 86.5% were less heavy drinking alcohol as described in
Table 4.7
Table 4.7 Alcohol drinking (n=226)
Alcohol drinking Number Percent
Alcohol drinking
Never 128 56.6
Ex-drinker 60 26.5
Current alcohol drinking 38 16.8
Ex-drinker (n=60)
Duration of quit drinking among ex-drinker
0-4 Years 33 55.0
5-10 Years 21 35.0
>10 Years 6 10.0
Current alcohol drinking (n=38)
Frequency of current drinker
1-2 times per month 30 78.4
1-2 times per week 8 21.6
Perceived to current alcohol drinking as
compared to last 6 months
Less heavy drinking alcohol 33 86.5
Same heavy drinking alcohol 3 8.1
Heavies drinking alcohol 2 5.4
For the physical activities of participants, some of them had 59(26.1%)
were inactivity cause of don’t have free time (55.9%). In addition, 167(73.9%) were
regular physical activity, most of them most of them had 52.8% were more than 2 times
per week. Also, there were walking physical activity with walking (95.8%), most of
them had 80.3% were physical activity more than 9 minutes as described in Table 4.8
Ref. code: 25606017090090UFM
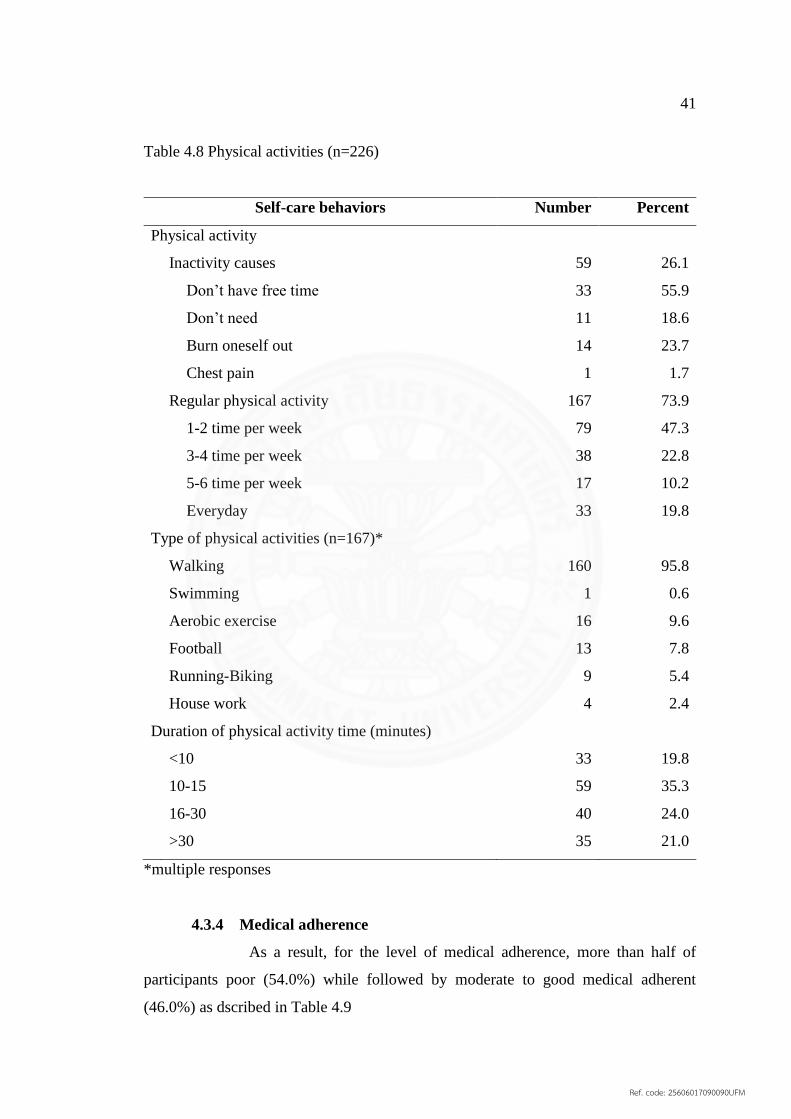
41
Table 4.8 Physical activities (n=226)
Self-care behaviors Number Percent
Physical activity
Inactivity causes 59 26.1
Don’t have free time 33 55.9
Don’t need 11 18.6
Burn oneself out 14 23.7
Chest pain 1 1.7
Regular physical activity 167 73.9
1-2 time per week 79 47.3
3-4 time per week 38 22.8
5-6 time per week 17 10.2
Everyday 33 19.8
Type of physical activities (n=167)*
Walking 160 95.8
Swimming 1 0.6
Aerobic exercise 16 9.6
Football 13 7.8
Running-Biking 9 5.4
House work 4 2.4
Duration of physical activity time (minutes)
<10 33 19.8
10-15 59 35.3
16-30 40 24.0
>30 35 21.0
*multiple responses
4.3.4 Medical adherence
As a result, for the level of medical adherence, more than half of
participants poor (54.0%) while followed by moderate to good medical adherent
(46.0%) as dscribed in Table 4.9
Ref. code: 25606017090090UFM

42
Table 4.9 Level of medical adherence (n=226)
Level of medical adherence Number Percent
Poor 122 54.0
Moderate 40 17.7
Good 64 28.3
For medical adherence with checking blood sugar at home, most of them
had 177(78.3%) were no checking at home cause no equipment (75.2%) whereas total
of not checking blood sugar at home. However, for checking blood sugar at home
(21.7%) with 1 time a day (17.3%) whereas total of checking blood sugar at home. In
addition, for foot care of participants were never examined feet for sores or wounds
(58.0%), but some of them had 21.2% were rugular examoned feet for sores or wounds.
Moreover, the participants were never forgotten to take Diabetes drug (65.5%). But,
some of them had 78(34.5%) were forgotten to take disbetic drug and more of them had
18.1% were 1 times per week. As a result, for the recall of taking drug among 78(34.5%)
participants had 48.7% were does nothing. Also, 99(44.0%) of participants were
spending overnight in other places while there were bring drug along with regular
(20.4%) as described in Table 4.10
Table 4.10 Medical adherence (n=226)
Medical adherence Number Percent
Blood sugar checking at home
No 177 78.3
no equipment 170 75.2
not sure to testing 7 3.1
Yes 49 21.7
1 time a day 39 17.3
2 times a day 5 2.2
3 times a day 5 2.2
Ref. code: 25606017090090UFM
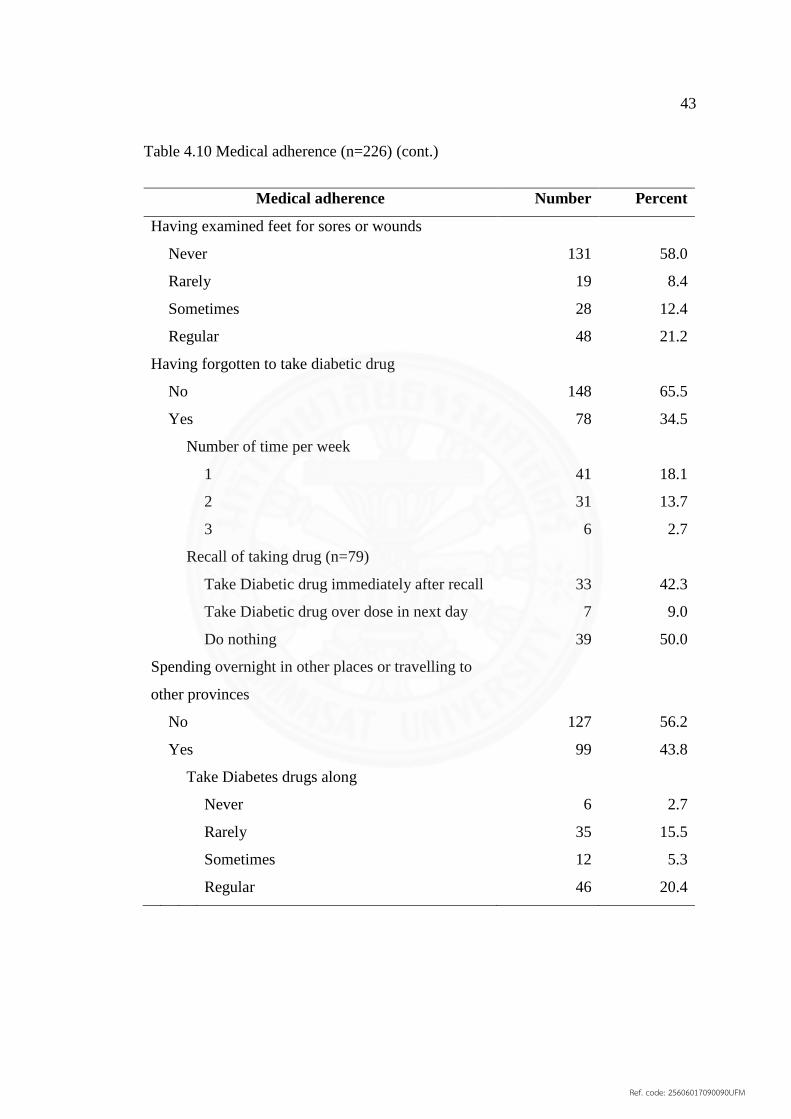
43
Table 4.10 Medical adherence (n=226) (cont.)
Medical adherence Number Percent
Having examined feet for sores or wounds
Never 131 58.0
Rarely 19 8.4
Sometimes 28 12.4
Regular 48 21.2
Having forgotten to take diabetic drug
No 148 65.5
Yes 78 34.5
Number of time per week
1 41 18.1
2 31 13.7
3 6 2.7
Recall of taking drug (n=79)
Take Diabetic drug immediately after recall 33 42.3
Take Diabetic drug over dose in next day 7 9.0
Do nothing 39 50.0
Spending overnight in other places or travelling to
other provinces
No 127 56.2
Yes 99 43.8
Take Diabetes drugs along
Never 6 2.7
Rarely 35 15.5
Sometimes 12 5.3
Regular 46 20.4
Ref. code: 25606017090090UFM
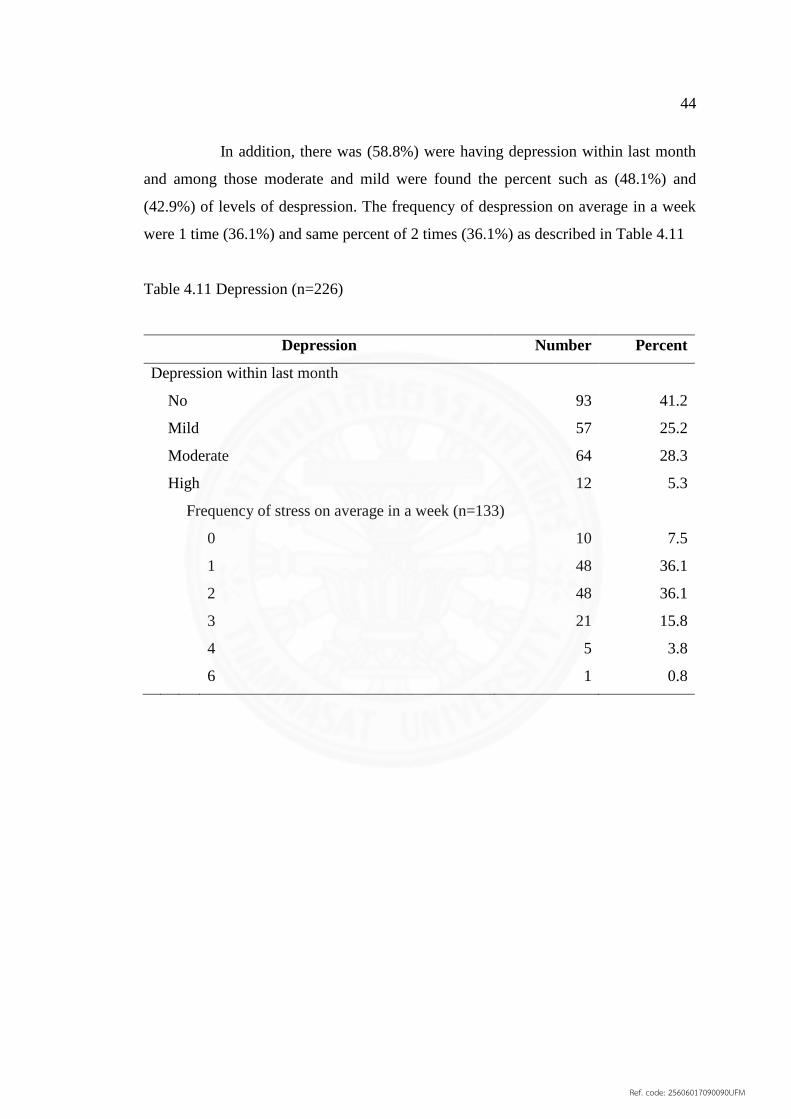
44
In addition, there was (58.8%) were having depression within last month
and among those moderate and mild were found the percent such as (48.1%) and
(42.9%) of levels of despression. The frequency of despression on average in a week
were 1 time (36.1%) and same percent of 2 times (36.1%) as described in Table 4.11
Table 4.11 Depression (n=226)
Depression Number Percent
Depression within last month
No 93 41.2
Mild 57 25.2
Moderate 64 28.3
High 12 5.3
Frequency of stress on average in a week (n=133)
0 10 7.5
1 48 36.1
2 48 36.1
3 21 15.8
4 5 3.8
6 1 0.8
Ref. code: 25606017090090UFM
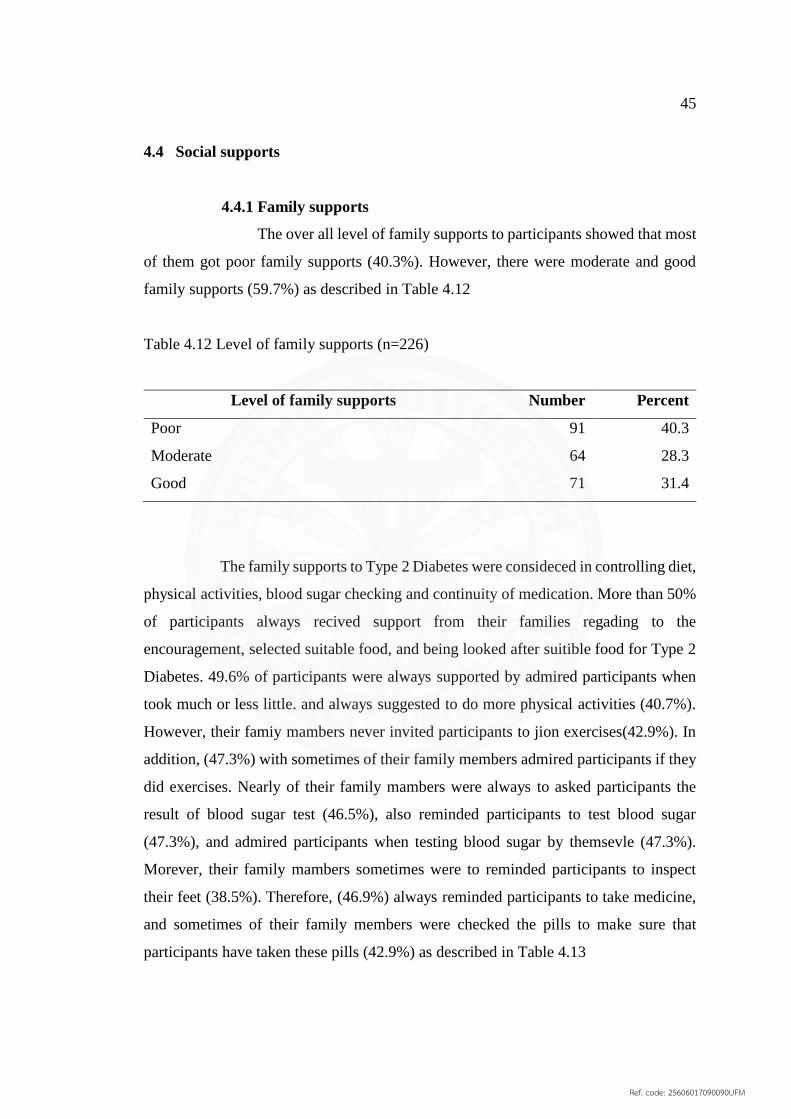
45
4.4 Social supports
4.4.1 Family supports
The over all level of family supports to participants showed that most
of them got poor family supports (40.3%). However, there were moderate and good
family supports (59.7%) as described in Table 4.12
Table 4.12 Level of family supports (n=226)
Level of family supports Number Percent
Poor 91 40.3
Moderate 64 28.3
Good 71 31.4
The family supports to Type 2 Diabetes were consideced in controlling diet,
physical activities, blood sugar checking and continuity of medication. More than 50%
of participants always recived support from their families regading to the
encouragement, selected suitable food, and being looked after suitible food for Type 2
Diabetes. 49.6% of participants were always supported by admired participants when
took much or less little. and always suggested to do more physical activities (40.7%).
However, their famiy mambers never invited participants to jion exercises(42.9%). In
addition, (47.3%) with sometimes of their family members admired participants if they
did exercises. Nearly of their family mambers were always to asked participants the
result of blood sugar test (46.5%), also reminded participants to test blood sugar
(47.3%), and admired participants when testing blood sugar by themsevle (47.3%).
Morever, their family mambers sometimes were to reminded participants to inspect
their feet (38.5%). Therefore, (46.9%) always reminded participants to take medicine,
and sometimes of their family members were checked the pills to make sure that
participants have taken these pills (42.9%) as described in Table 4.13
Ref. code: 25606017090090UFM
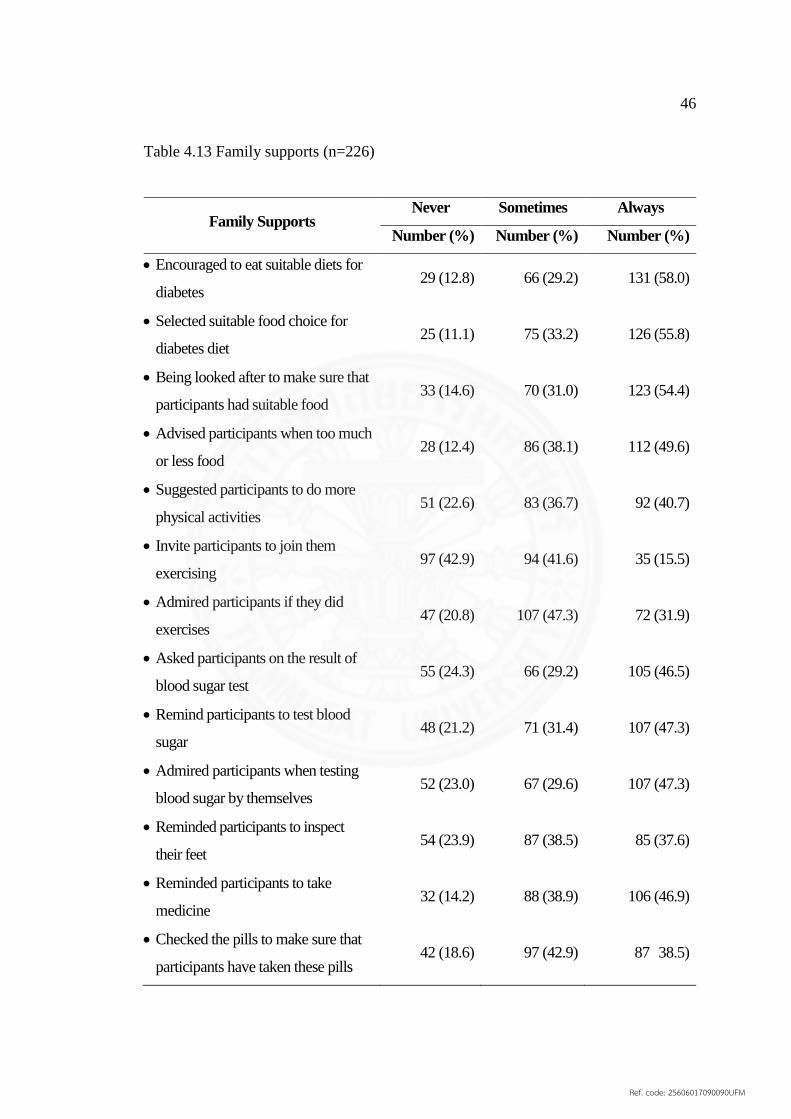
46
Table 4.13 Family supports (n=226)
Family Supports Never Sometimes Always
Number (%) Number (%) Number (%)
Encouraged to eat suitable diets for
diabetes 29 (12.8) 66 (29.2) 131 (58.0)
Selected suitable food choice for
diabetes diet 25 (11.1) 75 (33.2) 126 (55.8)
Being looked after to make sure that
participants had suitable food 33 (14.6) 70 (31.0) 123 (54.4)
Advised participants when too much
or less food 28 (12.4) 86 (38.1) 112 (49.6)
Suggested participants to do more
physical activities 51 (22.6) 83 (36.7) 92 (40.7)
Invite participants to join them
exercising 97 (42.9) 94 (41.6) 35 (15.5)
Admired participants if they did
exercises 47 (20.8) 107 (47.3) 72 (31.9)
Asked participants on the result of
blood sugar test 55 (24.3) 66 (29.2) 105 (46.5)
Remind participants to test blood
sugar 48 (21.2) 71 (31.4) 107 (47.3)
Admired participants when testing
blood sugar by themselves 52 (23.0) 67 (29.6) 107 (47.3)
Reminded participants to inspect
their feet 54 (23.9) 87 (38.5) 85 (37.6)
Reminded participants to take
medicine 32 (14.2) 88 (38.9) 106 (46.9)
Checked the pills to make sure that
participants have taken these pills 42 (18.6) 97 (42.9) 87 38.5)
Ref. code: 25606017090090UFM
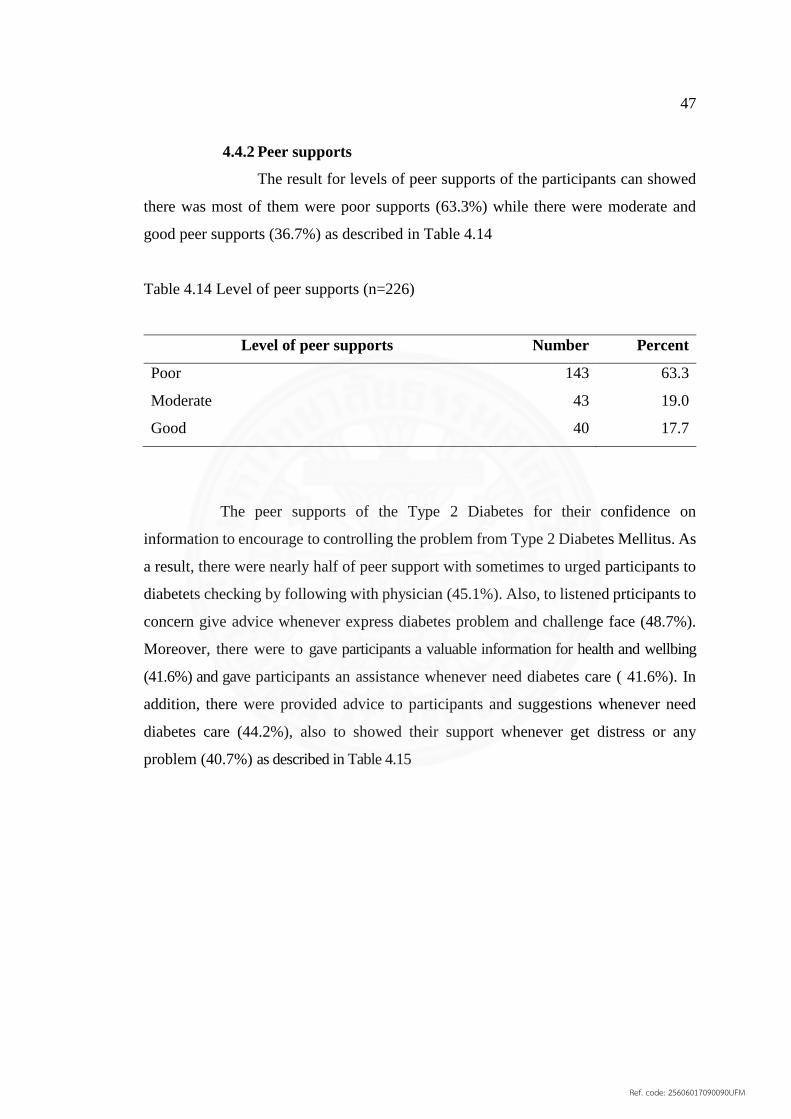
47
4.4.2 Peer supports
The result for levels of peer supports of the participants can showed
there was most of them were poor supports (63.3%) while there were moderate and
good peer supports (36.7%) as described in Table 4.14
Table 4.14 Level of peer supports (n=226)
Level of peer supports Number Percent
Poor 143 63.3
Moderate 43 19.0
Good 40 17.7
The peer supports of the Type 2 Diabetes for their confidence on
information to encourage to controlling the problem from Type 2 Diabetes Mellitus. As
a result, there were nearly half of peer support with sometimes to urged participants to
diabetets checking by following with physician (45.1%). Also, to listened prticipants to
concern give advice whenever express diabetes problem and challenge face (48.7%).
Moreover, there were to gave participants a valuable information for health and wellbing
(41.6%) and gave participants an assistance whenever need diabetes care ( 41.6%). In
addition, there were provided advice to participants and suggestions whenever need
diabetes care (44.2%), also to showed their support whenever get distress or any
problem (40.7%) as described in Table 4.15
Ref. code: 25606017090090UFM
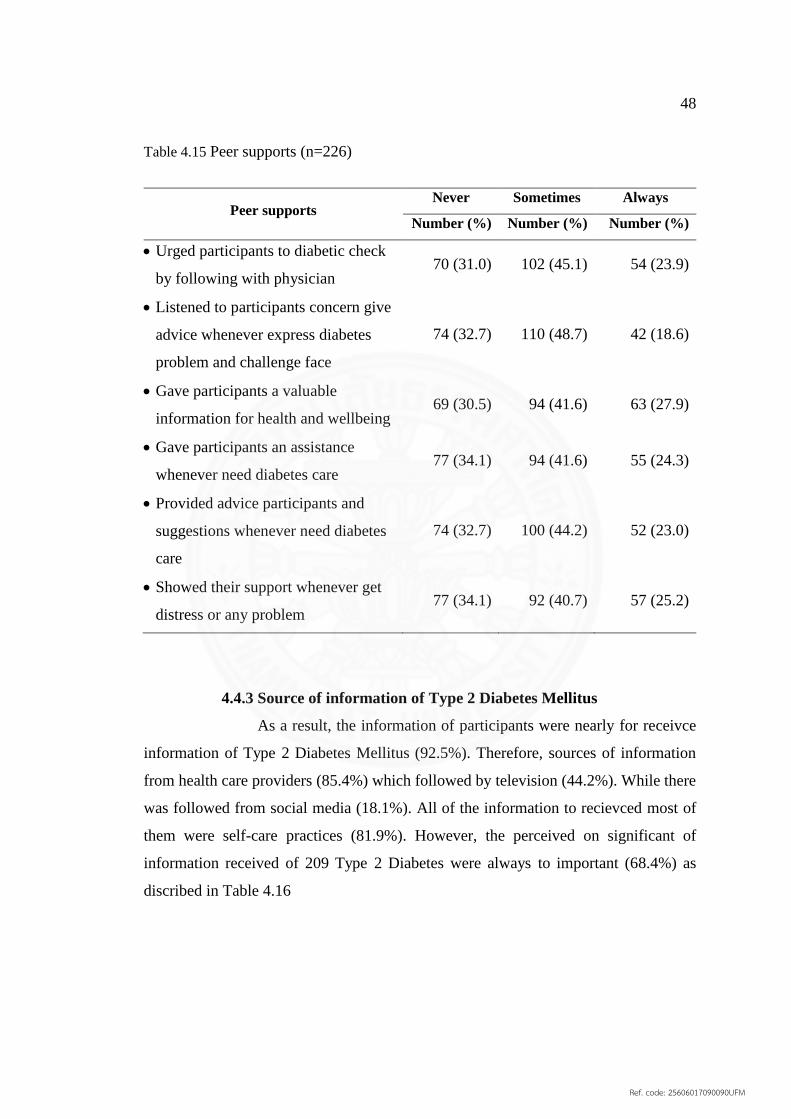
48
Table 4.15 Peer supports (n=226)
Peer supports Never Sometimes Always
Number (%) Number (%) Number (%)
Urged participants to diabetic check
by following with physician 70 (31.0) 102 (45.1) 54 (23.9)
Listened to participants concern give
advice whenever express diabetes
problem and challenge face
74 (32.7) 110 (48.7) 42 (18.6)
Gave participants a valuable
information for health and wellbeing 69 (30.5) 94 (41.6) 63 (27.9)
Gave participants an assistance
whenever need diabetes care 77 (34.1) 94 (41.6) 55 (24.3)
Provided advice participants and
suggestions whenever need diabetes
care
74 (32.7) 100 (44.2) 52 (23.0)
Showed their support whenever get
distress or any problem 77 (34.1) 92 (40.7) 57 (25.2)
4.4.3 Source of information of Type 2 Diabetes Mellitus
As a result, the information of participants were nearly for receivce
information of Type 2 Diabetes Mellitus (92.5%). Therefore, sources of information
from health care providers (85.4%) which followed by television (44.2%). While there
was followed from social media (18.1%). All of the information to recievced most of
them were self-care practices (81.9%). However, the perceived on significant of
information received of 209 Type 2 Diabetes were always to important (68.4%) as
discribed in Table 4.16
Ref. code: 25606017090090UFM

49
Table 4.16 Sources of information
Information of Type 2 Diabetes Mellitus Number Percent
Have ever received information about DM (n=226)
No 17 7.5
Yes 209 92.5
Source of information*
Health care providers 193 85.4
Television 100 44.2
Radio 24 10.6
Newspapers 32 14.2
Social media 41 18.1
Type of information*
Cause of Type 2 Diabetes Mellitus 126 55.8
Effective of Type 2 Diabetes Mellitus 120 53.1
Type 2 Diabetes complications 121 53.5
Self-care practices 185 81.9
Usefulness of information received (n=209)
Never 3 1.4
Sometimes 63 30.1
Always 143 68.4
*multiple responses
4.5 Health care provider-patient communication
As a result, the levels of health care provider-patient communication of the
participants can showed there was most of them were good (58.0%) while followed by
moderate (25.2%) and poor communication (16.8%) as described in Table 4.17
Ref. code: 25606017090090UFM

50
Table 4.17 Level of Health care provider-patient communication (n=226)
Health care provider-patients communication Number Percent
Poor 38 16.8
Moderate 57 25.2
Good 131 58.0
For health care provider-patient communication. Firstly, most of
participants had 78.3% were acknowledge from physician always explained to how to
take medicine, but there were always trouble understanding physician explanation on
how to take medicine (63.3%). While 74.3% were got from physician always informed
about diabetes status. In addition, 68.1% of participants were from physician always
thoroughly explained why a test was being done, 67.3% were from physician always
explained for take care of health, 61.9% were from physician always answered to
questions and address concern. Moreover, 58.8% were from physician always paid
attention to response and explanation, but 49.6% were physician sometimes spent
plently of time to talk with diabetes. Secondly, most of participants had 61.1% were
from nurses always helpfully answered to questions and addresed concern about hralth,
60.6% were from nurses always paid attention to response and explanation. In addition,
62.4% were from phramacists always clearly explained on how to take medicine on
prescription. Finally, 55.3% of participants were from nutritionist always helpfully
answered diabetes diet when not sure and 51.3% were from nutritionist always provide
information on diet. In short, health care provider-patient communiation were good
communicate form physician, nurses and nutritionist as described in Table 4.18
Ref. code: 25606017090090UFM

51
Table 4.18 Health care provider-patient communication (n=226)
Health care provider-patient
communication
Never Sometimes Always
Number (%) Number (%) Number (%)
Physician informed about diabetes
status 8 (3.5) 50 (22.1) 168 (74.3)
Physician explained to how to take
medicine 4 (1.8) 45 (19.9) 177 (78.3)
Trouble understanding physician
explanation on how to take medicine 3 (1.3) 80 (35.4) 143 (63.3)
Physician paid attention to response
and explanation 3 (1.3) 90 (39.8) 133 (58.8)
Physician answered to questions and
addresses concern 5 (2.2) 81 (35.8) 140 (61.9)
Physician thoroughly explained why
a test was being done 6 (2.7) 66 (29.2) 154 (68.1)
Physician explained for take care of
heath 6 (2.7) 68 (30.1) 152 (67.3)
Physician spent plenty of time to talk
with diabetes 27 (11.9) 112 (49.6) 87 (38.5)
Nurses helpfully answered to
questions and addressed concern
about health
6 (2.7) 82 (36.3) 138 (61.1)
Nurses paid attention to response and
explanation 3 (1.3) 86 (38.1) 137 (60.6)
Pharmacist clearly explained on how
to take medicine on prescription 4 (1.8) 81 (35.8) 141 (62.4)
Nutritionist provide information on
diet 13 (5.8) 97 (42.9) 116 (51.3)
Nutritionist helpfully answered
diabetes diet when not sure 14 (6.2) 87 (38.5) 125 5.3)
Ref. code: 25606017090090UFM

52
4.6 Satisfaction to health services system
As a result, for levels of satisfaction to health services system of
participants can showed over half of them were moderate satisfaction (56.2%) while
followed by good satisfacction (24.3%) and poor satisfaction (19.5%) as described in
Table 4.19
Table 4.19 Level of satisfaction (n=226)
Satisfaction to services system Number Percent
Poor 44 19.5
Moderate 127 56.2
Good 55 24.3
The satisfaction of Type 2 Diabetes for health system services following by
the situation at OPD in Mahosot Hospital. Firstly, Type 2 Diabetes had satisfied for the
patients registration system (35.4%). Also, there was satisfied the health registration
place (35.4%). In addition, there were moderate for waiting area to see a physician
(36.3%) and waiting area to collect the drug (48.2%). Secondarly, there were half of
the patients had satisfied among those nurses services, physician services, pharmacists
services, and polite, humility, verbal speech of them were found to be the percentage
such as (54.9%), (50.0%), (52.2%), and (57.1%) respectively. In addition, there were
more than of patients had satisfied for responding to their concerns and relatives
willingly (61.1%). However, there was satisfied for provide information respect on
request (48.7%). Finally, more than half of patients had satisfied for knowledge of the
health care providers (56.6%). Therefore, patients had for received respect and equate
treatment from health care providers (58.0%). Moreover, patients had satisfied for
health care providers with the quikly and availability of services (36.3%). For the
service of making an opportunity with a physician to patients were satisfied (48.7%).
In conclusion, more than of the patients had moderate for the health system services at
OPD in Mahosot Hospital as described in Table 4.20
Ref. code: 25606017090090UFM

53
Table 4.20 Satisfaction to services (n=226)
Satisfaction
not very
satisfied not satisfied moderate satisfied
very
satisfied
Number
(%)
Number
(%)
Number
(%)
Number
(%)
Number
(%)
Patients registration
system 11 (4.9) 25 (11.1) 77 (34.1) 80 (35.4) 33 (14.6)
The health
registration place 4 (1.8) 41 (18.1) 70 (31.0) 80 (35.4) 31 (13.7)
Waiting area to see
a physician 1 (0.4) 44 (19.5) 82 (36.3) 54 (23.9) 45 (19.9)
Waiting area to
collect the drug 2 (0.9) 23 (10.2) 109 (48.2) 75 (33.2) 17 (7.5)
Nurses services 1 (0.4) 11 (4.9) 35 (15.5) 124 (54.9) 55 (24.3)
Physician services 1 (0.4) 7 (3.1) 32 (14.2) 113 (50.0) 73 (32.3)
Pharmacists
services 1 (0.4) 12 (5.3) 71 (31.4) 118 (52.2) 24 (10.6)
Polite, humility,
verbal speech of them 5 (2.2) 10 (4.4) 31 (13.7) 129 (57.1) 51 (22.6)
Responding to
your concerns and
relatives willingly
3 (1.3) 10 (4.4) 29 (12.8) 138 (61.1) 46 (20.4)
Provide information
respect your request 1 (0.4) 12 (5.3) 43 (19.0) 110 (48.7) 60 (26.5)
Knowledge of the
health care
providers
1 (0.4) 8 (3.5) 35 (15.5) 128 (56.6) 54 (23.9)
You received
respect and
equate treatment
from health care
providers
2 (0.9) 6 (2.7) 35 (15.5) 131 (58.0) 52 (23.0)
Ref. code: 25606017090090UFM
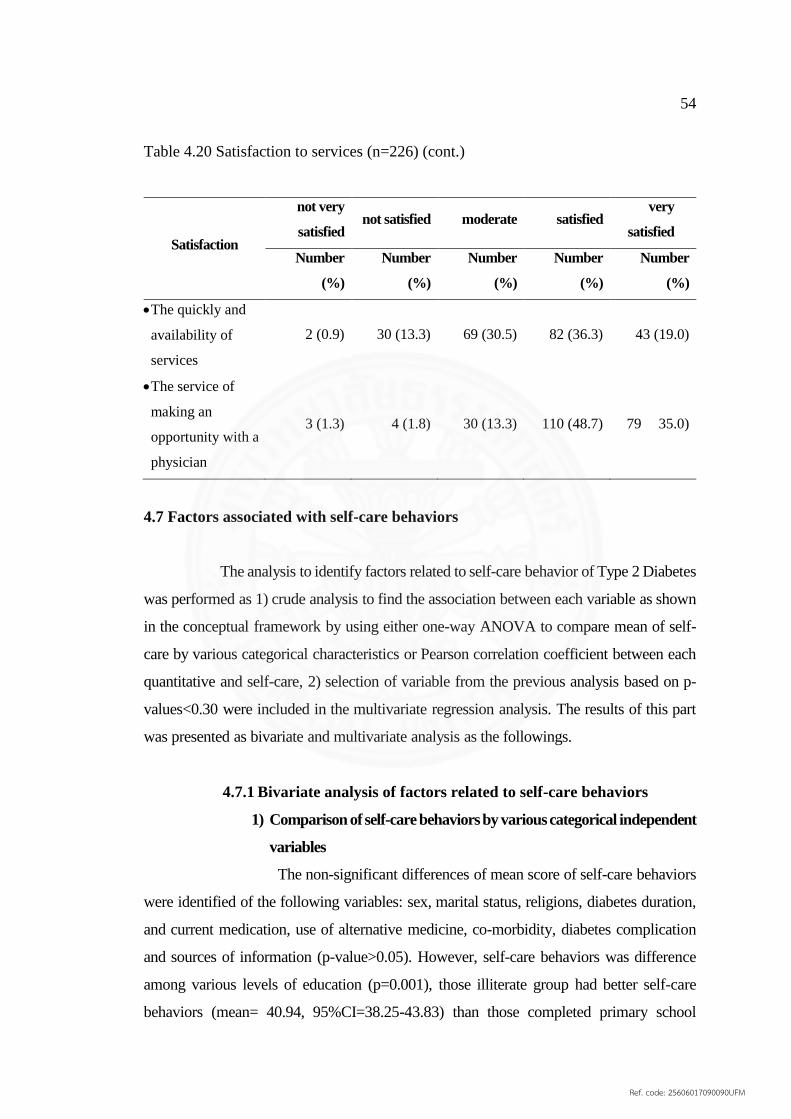
54
Table 4.20 Satisfaction to services (n=226) (cont.)
Satisfaction
not very
satisfied not satisfied moderate satisfied
very
satisfied
Number
(%)
Number
(%)
Number
(%)
Number
(%)
Number
(%)
The quickly and
availability of
services
2 (0.9) 30 (13.3) 69 (30.5) 82 (36.3) 43 (19.0)
The service of
making an
opportunity with a
physician
3 (1.3) 4 (1.8) 30 (13.3) 110 (48.7) 79 35.0)
4.7 Factors associated with self-care behaviors
The analysis to identify factors related to self-care behavior of Type 2 Diabetes
was performed as 1) crude analysis to find the association between each variable as shown
in the conceptual framework by using either one-way ANOVA to compare mean of self-
care by various categorical characteristics or Pearson correlation coefficient between each
quantitative and self-care, 2) selection of variable from the previous analysis based on p-
values<0.30 were included in the multivariate regression analysis. The results of this part
was presented as bivariate and multivariate analysis as the followings.
4.7.1 Bivariate analysis of factors related to self-care behaviors
1) Comparison of self-care behaviors by various categorical independent
variables
The non-significant differences of mean score of self-care behaviors
were identified of the following variables: sex, marital status, religions, diabetes duration,
and current medication, use of alternative medicine, co-morbidity, diabetes complication
and sources of information (p-value>0.05). However, self-care behaviors was difference
among various levels of education (p=0.001), those illiterate group had better self-care
behaviors (mean= 40.94, 95%CI=38.25-43.83) than those completed primary school
Ref. code: 25606017090090UFM

55
(mean= 37.41, 95%CI=35.94-38.96), secondary group (mean=36.71, 95%CI= 35.03-
38.39), high school (mean= 35.45, 95%CI= 33.23-37.70), and college or university (mean=
32.44, 95%CI= 29.93-35.15). It can be concluded that the lower the educational attainment
was the better the self-care behaviors, as the detailed shown in Table 4.21
Table 4.21 Comparison of self-care behaviors by various characteristics of Type 2 Diabetes
Factors Simple
size Mean SEM
95% CI 1
p-value 2
LB UB
Total 226 36.42 0.47 35.50 37.36
Sex 0.280
Male 89 35.79 0.75 34.24 37.23
Female 137 36.82 0.60 35.63 38.03
Marital status 0.192
Single 8 32.00 2.54 26.60 36.75
Married 188 36.53 0.52 35.48 37.54
Divorced/Separated/Widowed 30 36.87 1.24 34.42 39.33
Educational attainment 0.001
Illiterate 16 40.94 1.44 38.25 43.83
Primary school 76 37.41 0.76 35.94 38.96
Secondary school 62 36.71 0.82 35.03 38.39
High school 40 35.45 1.16 33.23 37.70
College/University 32 32.44 1.35 29.93 35.15
Religion 0.515
Buddhist 213 36.44 0.48 35.48 37.42
Christian 3 32.00 4.16 24.00 38.00
Animist 10 37.30 2.32 32.34 41.92
Diabetes duration(Years) 0.233
01 Year 36 35.42 0.93 33.62 37.23
02 Years 40 35.25 1.23 32.82 37.62
03 Years 31 35.06 1.43 32.39 38.05
04 Years 17 39.47 1.12 37.33 41.76
05-09 Years 52 36.75 0.99 34.83 38.68
10-19 Years 40 37.90 1.18 35.31 40.10
>20 Years 10 36.00 1.75 32.25 39.17
1 by Bootstrap
2by ONEWAY ANOVA
Ref. code: 25606017090090UFM
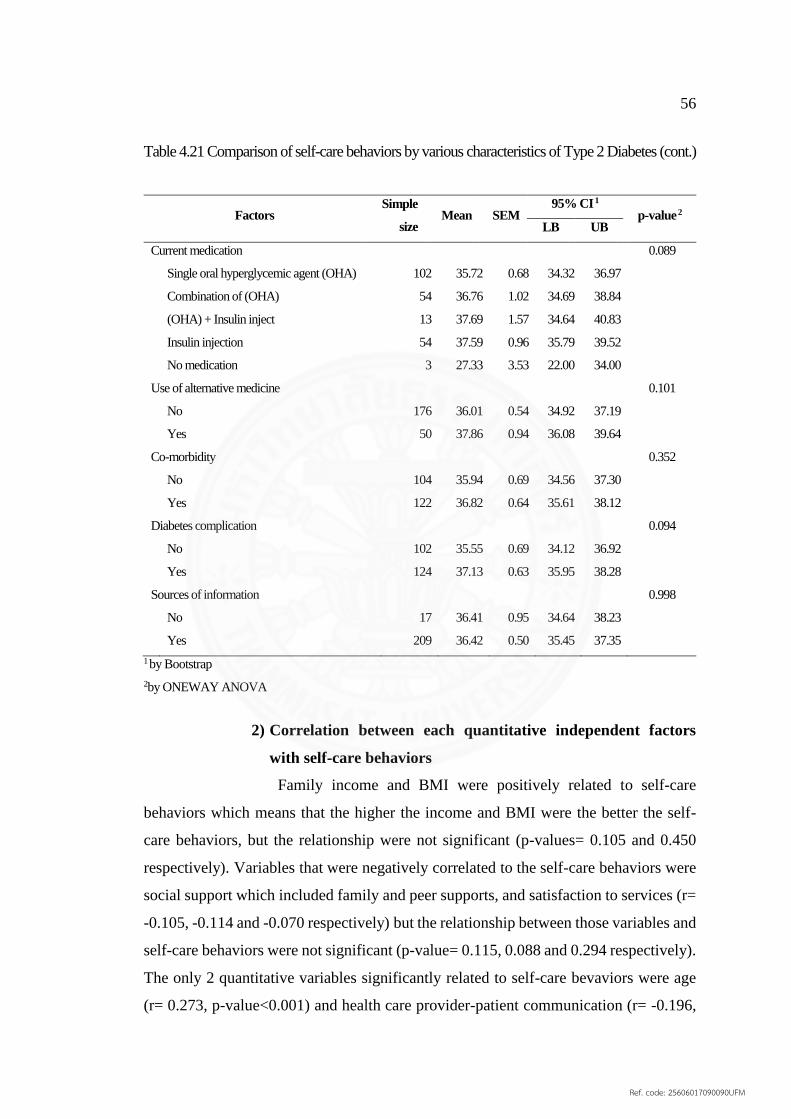
56
Table 4.21 Comparison of self-care behaviors by various characteristics of Type 2 Diabetes (cont.)
Factors Simple
size Mean SEM
95% CI 1
p-value 2
LB UB
Current medication 0.089
Single oral hyperglycemic agent (OHA) 102 35.72 0.68 34.32 36.97
Combination of (OHA) 54 36.76 1.02 34.69 38.84
(OHA) + Insulin inject 13 37.69 1.57 34.64 40.83
Insulin injection 54 37.59 0.96 35.79 39.52
No medication 3 27.33 3.53 22.00 34.00
Use of alternative medicine 0.101
No 176 36.01 0.54 34.92 37.19
Yes 50 37.86 0.94 36.08 39.64
Co-morbidity 0.352
No 104 35.94 0.69 34.56 37.30
Yes 122 36.82 0.64 35.61 38.12
Diabetes complication 0.094
No 102 35.55 0.69 34.12 36.92
Yes 124 37.13 0.63 35.95 38.28
Sources of information 0.998
No 17 36.41 0.95 34.64 38.23
Yes 209 36.42 0.50 35.45 37.35
1 by Bootstrap
2by ONEWAY ANOVA
2) Correlation between each quantitative independent factors
with self-care behaviors
Family income and BMI were positively related to self-care
behaviors which means that the higher the income and BMI were the better the self-
care behaviors, but the relationship were not significant (p-values= 0.105 and 0.450
respectively). Variables that were negatively correlated to the self-care behaviors were
social support which included family and peer supports, and satisfaction to services (r=
-0.105, -0.114 and -0.070 respectively) but the relationship between those variables and
self-care behaviors were not significant (p-value= 0.115, 0.088 and 0.294 respectively).
The only 2 quantitative variables significantly related to self-care bevaviors were age
(r= 0.273, p-value<0.001) and health care provider-patient communication (r= -0.196,
Ref. code: 25606017090090UFM

57
p-value<0.001). The higher the age was the better the self-care behaviors and the more
of the communication between the health care provider and the patient was the poorer
the self-care behaviors. The detail was showed in Table 4.22
Table 4.22 Pearson Correlations between each quantitative factors and self-care
behaviors of 226 Type 2 Diabetes
Factors
Self-care behaviors
r p-value*
(2-tailed)
95%CI**
LB UB
Age 0.273 <0.001 0.138 0.396
Family income 0.108 0.105 -0.019 0.230
BMI 0.051 0.450 -0.083 0.189
Family support -0.105 0.115 -0.235 0.024
Peer support -0.114 0.088 -0.242 0.024
Health care provider-patient communication -0.196 0.003 -0.305 -0.075
Satisfaction to health service -0.070 0.294 -0.175 0.037
**95%CI by Bootstrap analysis
*by t-Test
4.7.2 Multiple Linear Regression analysis
From multiple regression analysis of factors related to self-care
behaviors of Type 2 Diabetes was shown in Table 4.23, there was gender, marital status,
educational attaiment, use of alternative medicine, co-morbidity and ever received
information about the sickness. For quantitative predictors, actual measurement were
put into the multiple regression model. For one year increased of age, the self-care
behaviors was significantly increased 0.16 score when controlled for other variables in
the model. The higher the age was, the better the self-care behaviors when controlled
for other factors in the model. Other factors significantly related to self-care were
educational attainment and health care provider-patient communication. Education
showed an opposite relationship to self-care behaviors. The higher educational backgroud
was the poorer self-care behaviors. Furthermore, the more communication with health
Ref. code: 25606017090090UFM
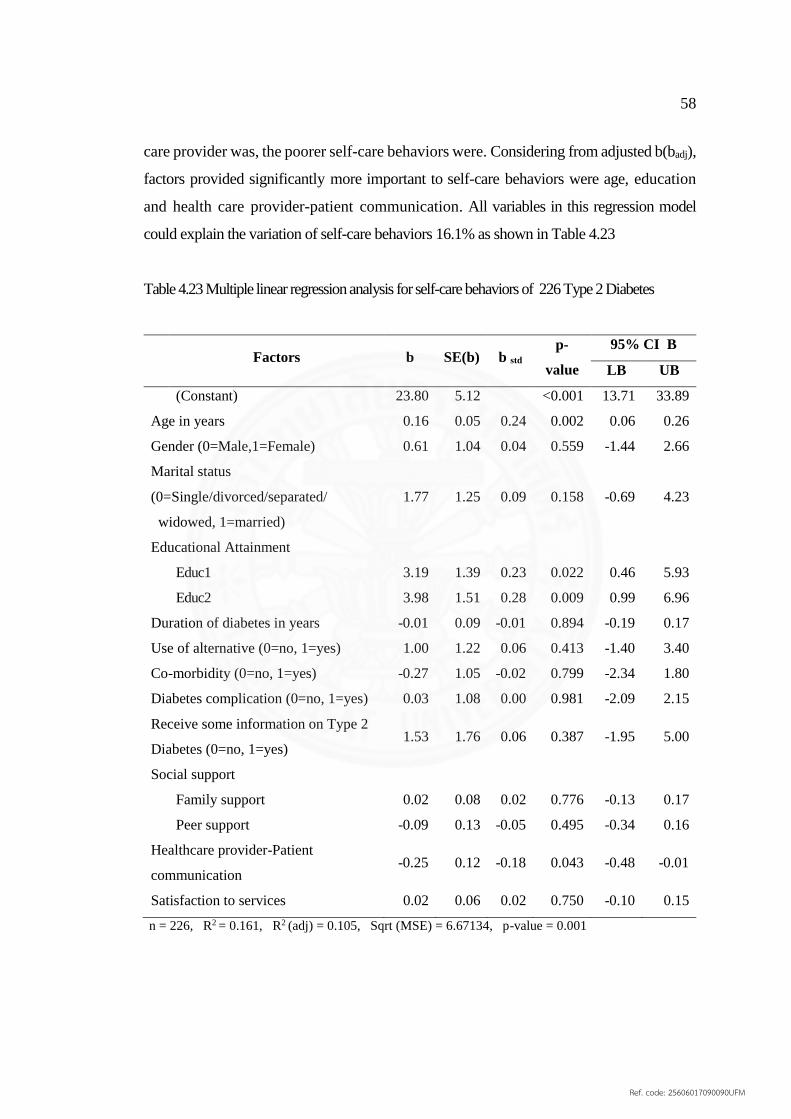
58
care provider was, the poorer self-care behaviors were. Considering from adjusted b(badj),
factors provided significantly more important to self-care behaviors were age, education
and health care provider-patient communication. All variables in this regression model
could explain the variation of self-care behaviors 16.1% as shown in Table 4.23
Table 4.23 Multiple linear regression analysis for self-care behaviors of 226 Type 2 Diabetes
Factors b SE(b) b std
p-
value
95% CI B
LB UB
(Constant) 23.80 5.12 <0.001 13.71 33.89
Age in years 0.16 0.05 0.24 0.002 0.06 0.26
Gender (0=Male,1=Female) 0.61 1.04 0.04 0.559 -1.44 2.66
Marital status
(0=Single/divorced/separated/
widowed, 1=married)
1.77 1.25 0.09 0.158 -0.69 4.23
Educational Attainment
Educ1 3.19 1.39 0.23 0.022 0.46 5.93
Educ2 3.98 1.51 0.28 0.009 0.99 6.96
Duration of diabetes in years -0.01 0.09 -0.01 0.894 -0.19 0.17
Use of alternative (0=no, 1=yes) 1.00 1.22 0.06 0.413 -1.40 3.40
Co-morbidity (0=no, 1=yes) -0.27 1.05 -0.02 0.799 -2.34 1.80
Diabetes complication (0=no, 1=yes) 0.03 1.08 0.00 0.981 -2.09 2.15
Receive some information on Type 2
Diabetes (0=no, 1=yes) 1.53 1.76 0.06 0.387 -1.95 5.00
Social support
Family support 0.02 0.08 0.02 0.776 -0.13 0.17
Peer support -0.09 0.13 -0.05 0.495 -0.34 0.16
Healthcare provider-Patient
communication -0.25 0.12 -0.18 0.043 -0.48 -0.01
Satisfaction to services 0.02 0.06 0.02 0.750 -0.10 0.15
n = 226, R2 = 0.161, R2 (adj) = 0.105, Sqrt (MSE) = 6.67134, p-value = 0.001
Ref. code: 25606017090090UFM

59
Dummy variables for levels of educational attainment
Educational attainment Educ1 Educ2
College/University 0 0
Secondary school/High school 1 0
Illiterate/Primary school 0 1
4.8 Self-care behaviors and Fasting Blood Sugar
Self-care behaviors was negatively correlated to Fasting Blood Sugar on
current visit by positively associate with Fasting Blood Sugar (r= -0.053 and 0.076,
respectively). However, the relationships between self-care behaviors and fasting blood
sugar at two visits were not significantly (p-values>0.254) as shown in Table 4.24
Table 4.24 Pearson Correlations between FBS and self-care behaviors of Type 2 Diabetes
Factors
Self-care behaviors
r p-value*
(2-tailed)
95%CI**
LB UB
FBS on current visit -0.053 0.428 -0.190 0.067
FBS last visit 0.076 0.254 -0.57 0.203
**95%CI by Bootstrap analysis
*by t-Test
4.9 Discussion
The objective of this study was to evaluate health care provider-patient
communication and self- care behaviors among Type 2 Diabetes among at Mahosot
Hospital, Vientiane Capital, Lao PDR.
Ref. code: 25606017090090UFM
60
4.9.1 Prevalence of self-care behaviors
As a result, self-care behaviors of 226 Type 2 Diabetes were followed
with dietary, physical activities, blood sugar checking, continuity of medication and
foot care examination.
The self-care behaviors of 226 Type 2 Diabetes were followed with
dietary, physical activities, blood sugar checking, continuity of medication and foot
care by the patients. As a result, more than half of participants were poor self-care
behaviors (59.7%). Moreover, there were indentify by groups as showed that self-care
behaviors with dietary of participants were poor (62.4%). Self-care behaviors with
physical activities, most of them were regular physical activity (73.9%). Similar the
study of Nazila N et al, 2017(13) and different to the study of Riangkam C et al, 2016(70).
Its might the participants could not performed from health care providers such as eating
of participants were not followed on times. In addition, more of them were eaten instant
food and soup noodles with adding sugar, monosodium glutamate and fish sauce.
Moreover, most participants were having eaten sweet fruits and high fat foods. In
addition, some of them were smoking and alcohol drinking. Therefore, thoses were the
main cause could affected to poor self-care behaviors of participants.
For medical adherence, more than half of participants were poor
(54.0%). Because the most of participants could not self-monitoring for blood sugar
checking at home, it’s the main problems can affecting to participants. In addition, some
of them forgotten to take diabetic drug and do nothing or take diabetic drug immediately
after recall. Therefore, thoses was cause missing medical adherence.
4.9.2 Factors association with self-care behaviors
(1) Age
The age of participants were signicantly associated with self-care
behaviors (p= 0.002) could show the higher the age were, the more likely that better
self-care behaviors were when controlled for other variables. Similarly to the study of
Nyunt SW et al, 2010 in YANGON, MYANMAR showed that elderly patients showed
the better self-care behaviors than the youngers(32) and similar to the study of Supreeya
S, 2017 in Thailand(57).
Ref. code: 25606017090090UFM
61
(2) Gender
The gender of participants were not significant associated with
self-care behaviors, but it could showed that female was had self-care behaviors more
than male. This similar to the study of Khomron Mutasin, 2557(62) and Supreeya S,
2017(57) in Thailand. This may due to female were most to had the factors with diabetes,
so female was more concern to self-management.
(3) Marital stauts
Regarding marital status of participants were not significant
associated with self-care behaviors. However, the marital status of participants were
married had better more than other groups. this may due to married group had body to
encourage and remind or help they to self-management.
(4) Educational attainment
Educational attainment among participants were significantly
associated with self-care behaviors. This could show that the illiterate group had better
self-care behaviors than those who completed primary school, secondary school, high
school and college or university. It can be concluded that the lower the educational
attainment was better the self-care behaviors, whereas the study of Chanthon
XAISANAVONG, 2012 in Setthathilath Hospital, Laos PDR, showed the different
finding. The case-control study to find the risk factors related to Type 2 Diabetes in Lao
patients, levels of education of participants were not different while compared to cases
and control(15). This may due to illiterate group had possibly to take their time for self-
management, and they followed health care provider’s advice. However, the high
knowledge of the participants may not controlled for self-care behaviors. In addition, it
may cause from self-care awareness of participants.
(5) Family supports
Family supports is very important because they are close relatives
with the participants. From multiple linear regression model, family supports were not
significantly associated with self-care behaviors (p= 0.776). However, family supports
was high, and self-care behaviors was high too. We can improve family supports though
physical activities.
Ref. code: 25606017090090UFM
62
(6) Peer supports
For peer supports of participants, for multiple linear regression
model of participants were not significant associated with self-care behaviors (p=
0.495). In addition, there were negative to self-care behaviors. Because Vientiane
Capital is the big downtown, most of people were take their time for their work. In
addition, there were not enough health volunteer to communicate for information of
Type 2 DM. This is the point to missing from peer supports.
(7) Health care provider-patient communication
For health care provider-patient communication were negative
significantly associated with self-care behaviors (b= -0.25, p= 0.043), which could
show higher patients’ percetion on the communication with health care provider. But
self-care behaviors were poor. Incontrast with the study of Nantiya Watthayu, 2011 in
Thailand, it showed that patient-provider communication for the score of diabetes self-
management of the subjects were good levels (b= 0.191, p<0.05), that means had more
comunication were increas the score of diabetes self-management(71). Because the Type
2 Diabetes who were poor self-care practices with fasting blood sugar were higher,
health care provider should be take the time to provided the information by
communication, anothers reason with over half of participants had Type 2 Diabetes
complications.
4.9.3 Limitation
As a limitation of a cross-sectional study, the relationship between
independent and dependent variables might not be able to determine the cause and
effect of the relationship. Moreover, self-care behavior was self-reported which might
vary among individuals.
Ref. code: 25606017090090UFM

63
CHAPTER 5
CONCLUSION AND RECOMMENDATION
This is the very first study of self-care behaviors on Type 2 Diabetes in
Mahosot Hospital, Lao PDR. The study was aimed to evaluate health care provider-
patient communication and self-care behaviors among Type 2 Diabetes at Mahosot
Hospital, Vientiane Capital, Lao PDR. This study recruited 226 participants who
attended OPD in Mahosot Hospital. The analysis was performed by correlation and
multiple linear regression.
5.1 Conclusion
Out of 226 Type 2 Diabetes, most of them were 32-59 years of age (60.2%),
and 60.6% were famale. The majority were married (83.2%). Most participants attended
primary school and scondary school accounting for 33.6% and 27.4% respectively.
Government employee were 26% which followed by laborer group (22.6%) and
unemployed group (22.1%). Most of participants were buddhist (94.2%). Most of
participants (26.5%) had family income between 500,000 – 1 M LAK/month, and
20.8% which their income was more than 2.5 M LAK/month. 59.7% of participants had
no health insurance. 79.1% of participants who had health security was public social
security. 152(67.3%) of participants had no history of Diabetes Mullitus among family
mambers. 50% of participants had history of DM was mother and 25.7% was father.
The duration of being diagnosed as Type 2 DM range from 1-31 years with
an average 5.89 years. The common of current medications were sigle oral
hyperglycemic (45.1%), combination of OHA (23.9%), and insulin injection (239%).
About 50(22.1%) informed using alternative medicine, and herbal drugs (19.5%) was
the commonest. Slightly more than half (54.0%) experiences co-morbidities were
Diabetic Neuropathy (38.9%) and Diabetic Retinopathy (28.8%).
Fasting Blood Sugar were taken from the medical records at last and current
visits, majority of them (88.5%) and (87.2%) were more than 130mg/dl. In regarding to
Body Mass Index, 54.4% was overwight and Obese. Only 41.6% was at normal weight.
Ref. code: 25606017090090UFM
64
Regarding self-care behaviors, over half of the participants were poor
(59.7%). Therefore, there were identify for self-care behaviors with dietary, more than
half of participants poor (62.4%) while followed by moderate self-care behaviors with
dietary (30.5%). In addition, for smoking of participants, 15(6.6%) of participants were
having smoking 1 pack a day (86.7%). Also, for alcohol drinking of participants,
38(16.8%) of participants were current alcohol drinking. For the physical activities of
participants, some of them had 59(26.1%) were inactivity cause of don’t have free time
(55.9%). For medical adherence with checking blood sugar at home, most of them had
177(78.3%) were no checking at home cause no equipment (75.2%). Also, for foot care
of participants were never examined feet for sores or wounds (58.0%). In addition, some
of them had 78(34.5%) were forgotten to take disbetic drug, most of them were poor
medical adherence (54.0%) while followed by moderate to good medical adherent
(46.0%). In addition, over half of participants had 58.8% were having depression.
Regarding family supports, more than half of participants had 59.7% were
poor to good. Moreover, 63.3% of participants were poor peer supports. Participants
were receivce information of Type 2 Diabetes Mellitus (92.5%) and sources of
information from health care providers (85.4%). All of the information to recievced
(81.9%) were self-care practices. Perceived on significant of information received of
209 Type 2 Diabetes (68.4%) were always to important. Health care provider-patient
communication levels (58.0%) were good communication. Satisfaction levels of the
participants, over half were moderate satisfaction (56.2%) and good satisfacction
(24.3%).
As a results, the variable was significantly related to self-care behaviors
was age. Therefore, this variable could show the higher the age was the better the self-
care behaviors when control other variables. In addition, education was significantly
related to self-care behaviors, the finding could show that illiterate had better self-care
behaviors than other groups. Moreover, for health care provider-patient communication
were significantly related to self-care behaviors. Therefore, it could show more of the
patients perceived communication from health care provider, patients was poor self-
care behaviors.
Ref. code: 25606017090090UFM
65
5.2 Recommendation
For implementation
Based on the findings from this study, over half of the participants were
those who had poor self-care behaviors. The strategy for improving of self-care
behaviors among Type 2 Diabetes in order to control fasting blood sugar and reduce
complications is essential. The recommentation are as following:
Health care provider can focus on Type 2 Diabetes with high education
to adjust their lifestyles in order to improve awarness on self-care behaviors.
Health care provider can encourage Type 2 Diabetes to have regular
physical activities and good dietary practices in order to control their fasting blood
sugar.
Peer supports can be improved by health volunteers and community
leaders in order to give DM information or suggestion for Type 2 Diabetes on diabetes
management.
Capacity building among health care providers can help improve their
skill to provide diabetes mellitus information among patients who had poor self-care
especially among patients with young age.
For further study
This study shows a poor self-care behaviors among Type 2 Diabetes.
Therefore, a study which can increase an awareness of Type 2 Diabetes for self-care
practices is necessary to reduce severe illness or complications. A comparison between
Type 2 Diabetes with complications and Type 2 Diabetes with no complication can be
assessed to find a good self-care management.
A study should be conducted on data collection in a one-year period
which can explore more Type 2 Diabetes which a large number of them may show
wider characteristics and seasonal variation of their self-care management on diabetes.
A qualitative study can be performed to explore more details on self-
care behaviors by using observation, focus group, or etc.
Ref. code: 25606017090090UFM

66
REFERENCES
1. World Health Organization. Global report on diabetes:; 2016.
2. World Health Organization. Global report on diabetes:; 2016. 21-3 p.
3. Guariguata L, Whiting DR, Hambleton I, Beagley J, Linnenkamp U, Shaw JE.
Global estimates of diabetes prevalence for 2013 and projections for 2035. Diabetes
research and clinical practice. 2014;103(2):137-49.
4. Gao J, Wang J, Zheng P, Haardörfer R, Kegler MC, Zhu Y, et al. Effects of self-
care, self-efficacy, social support on glycemic control in adults with type 2 diabetes.
BMC family practice. 2013;14(1):66.
5. Sicree R. The global burden of diabetes. Diabetes atlas. 2003.
6. Ramachandran A, Wan Ma RC, Snehalatha C. Diabetes in Asia. The Lancet.
2010;375(9712):408-18.
7. D'Souza MS, Karkada SN, Parahoo K, Venkatesaperumal R, Achora S,
Cayaban ARR. Self-efficacy and self-care behaviours among adults with type 2
diabetes. Applied Nursing Research. 2017;36:25-32.
8. WHO. Increasing public sector capacity for diabetes management in Laos,
WDF16-1419. 2016.
9. Phoxay C, Thongsana S, Sombandith X, Sisamouth B, Manivong V,
Boundachoundar I. Report on STEPS Survey on Non Communicable Diseases Risk
Factors in Vientiane Capital city, Lao PDR. 2010.
10. MOTMRU. Lao-Oxford-Mahidol Hospital Wellcome Trust Research Unit;
2018.
11. Sirisopha B, Latdaphone B, Ronny M, Anching S, Gregory O, Soudasack S, et
al. Hospital Industry in Vientiane Capital, Lao PDR. Korea Trade-Investment
Promotion Agency (KOTRA) 2013.
12. Vazini H, Barati M. The Health Belief Model and self-care behaviors among
Type 2 diabetic patients. Iranian Journal of Diabetes and Obesity. 2014;6(3):107-13.
13. Nejaddadgar N, Solhi M, Jegarghosheh S, Abolfathi M, Ashtarian H. Self-Care
and Related Factors in Patients with Type 2 Diabetes. Asian Journal of Biomedical and
Pharmaceutical Sciences. 2017;7.
14. WHO. Diabetes country profiles, Lao People's Democratic Republic, 2016.
Ref. code: 25606017090090UFM
67
15. Chanthon X. Factors association with Type 2 Diabetes Mellitus among Lao
patients at OPD, Setthathilath Hospital, Vientiane Capital, Lao PDR.
16. Mahosot Hospital, OPD. Annual report 2017.
17. Goldenberg R, Punthakee Z. Definition, classification and diagnosis of diabetes,
prediabetes and metabolic syndrome. Canadian journal of diabetes. 2013;37:S8-S11.
18. International Diabetes Federation. DIABETES ATLAS Eighth edition 2017.
19. Parveen K, Michaeil C. Clinical Medicine. Seventh ed. London2009.
20. ADA. Clinical Practice Guideline for Diabetes 2017. Diabetes Association of
Thailand; 2017.
21. ADA. Standards of medical care in diabetes—2015 abridged for primary care
providers. Clinical diabetes: a publication of the American Diabetes Association.
2015;33(2):97.
22. Tan MY. The relationship of health beliefs and complication prevention
behaviors of Chinese individuals with Type 2 Diabetes Mellitus. Diabetes Research and
Clinical Practice. 2004;66(1):71-7.
23. Schlienger J-L. Type 2 diabetes complications. Presse Med. 2013;42(5):839-48.
24. Stirban AO, Tschoepe D. Cardiovascular complications in diabetes. Diabetes
Care. 2008;31(Supplement 2):S215-S21.
25. Makarof L. Diabetes and cardiovascular disease. 2016.
26. Forbes JM, Cooper ME. Mechanisms of diabetic complications. Physiological
reviews. 2013;93(1):137-88.
27. Vinik AI, Nevoret M-L, Casellini C, Parson H. Diabetic neuropathy.
Endocrinology and Metabolism Clinics. 2013;42(4):747-87.
28. WHO. Type 2 diabetes: practical targets and treatments. Melbourne:
International Diabetes Institute (IDI); Singapore: In Vivo Communications (Asia) Pte
Limited; 2005. p. 37.
29. Yazdanpanah L, Nasiri M, Adarvishi S. Literature review on the management
of diabetic foot ulcer. World journal of diabetes. 2015;6(1):37.
30. Orem D. Nursing: concept of practice, 6th ed. St Louis, Missory: Mosby. 2001.
31. WHO Report. Self-care in the context of primary healh care. Bangkok; 2009.
32. Nyunt SW, Howteerakul N, Suwannapong N, Rajatanun T. Self-efficacy, self-
care behaviors and glycemic control among type-2 diabetes patients attending two
Ref. code: 25606017090090UFM

68
private clinics in Yangon, Myanmar. Southeast Asian Journal of Tropical Medicine and
Public Health. 2010;41(4):943.
33. Krisana K. Health Behaviors of Diabetic Patient in the Diabetes Mellitus Clinic
of Kangsanamnang Hospital, Nakhonratchasima Province. Thai Journal of Nursing
Council. 2011;31(1):19-31.
34. Group DPPR. The Diabetes Prevention Program (DPP): description of lifestyle
intervention. Diabetes care. 2002;25(12):2165-71.
35. Bell EA, Roe LS, Rolls BJ. Sensory-specific satiety is affected more by volume
than by energy content of a liquid food. Physiology & Behavior. 2003;78(4-5):593-600.
36. Care D. Nutritions Principle and Recommendations in Diabetes. 2018. Report
No.: 1935-5548.
37. Meetoo D. Dietary pattern of self-care among Asian and Caucasian diabetic
patients. British Journal of Nursing (BJN). 2004.
38. Wichai A. Thai National Health Examination Survey 5th. Health Systems
Research Institute2014. p. 54-5.
39. Carlsson S, Hammar N, Grill V. Alcohol consumption and type 2 diabetes.
Diabetologia. 2005;48(6):1051-4.
40. Wannamethee SG, Camargo CA, Manson JE, Willett WC, Rimm EB. Alcohol
drinking patterns and risk of type 2 diabetes mellitus among younger women. Archives
of Internal Medicine. 2003;163(11):1329-36.
41. Chrvala CA, Sherr D, Lipman RD. Diabetes self-management education for
adults with type 2 diabetes mellitus: a systematic review of the effect on glycemic
control. Patient education and counseling. 2016;99(6):926-43.
42. ADA. Tight Diabetes Control: American Diabetes Association. 2018.
43. Bakker K, Apelqvist J, Schaper NC. Practical guidelines on the management
and prevention of the diabetic foot 2011. Diabetes/metabolism research and reviews.
2012;28(S1):225-31.
44. Chiwanga FS, Njelekela MA. Diabetic foot: prevalence, knowledge, and foot
self-care practices among diabetic patients in Dar es Salaam, Tanzania–a cross-
sectional study. Journal of foot and ankle research. 2015;8(1):20.
45. Strom JL, Egede LE. The impact of social support on outcomes in adult patients
with type 2 diabetes: a systematic review. Current diabetes reports. 2012;12(6):769-81.
Ref. code: 25606017090090UFM
69
46. Oftedal B, Bru E, Karlsen B. Social support as a motivator of self‐management
among adults with type 2 diabetes. Journal of Nursing and Healthcare of Chronic
Illness. 2011;3(1):12-22.
47. Tang TS, Brown MB, Funnell MM, Anderson RM. Social support, quality of
life, and self-care behaviors among African Americans with type 2 diabetes. The
Diabetes Educator. 2008;34(2):266-76.
48. Göz F, Karaoz S, Goz M, Ekız S, Cetın I. Effects of the diabetic patients’
perceived social support on their quality‐of‐life. Journal of clinical nursing.
2007;16(7):1353-60.
49. Tran Graham J, Rutherford K. The Power of Peer Support. Nesta Health Lab;
2016. Report No.: 7706036.
50. Aikens JE, Bingham R, Piette JD. Patient-provider communication and self-care
behavior among type 2 diabetes patients. The Diabetes Educator. 2005;31(5):681-90.
51. Schoenthaler A, Knafl GJ, Fiscella K, Ogedegbe G. Addressing the social needs
of hypertensive patients: the role of patient–provider communication as a predictor of
medication adherence. Circulation: Cardiovascular Quality and Outcomes.
2017;10(9):e003659.
52. Wiechula R, Conroy T, Kitson AL, Marshall RJ, Whitaker N, Rasmussen P.
Umbrella review of the evidence: what factors influence the caring relationship between
a nurse and patient? Journal of advanced nursing. 2016;72(4):723-34.
53. Chin JJ. Doctor-patient relationship: a covenant of trust. Singapore Med J.
2001;42(12):579-81.
54. Mulder BC, Lokhorst AM, Rutten GE, van Woerkum CM. Effective nurse
communication with type 2 diabetes patients: a review. Western journal of nursing
research. 2015;37(8):1100-31.
55. Benedict AW, Spence MM, Sie JL, Chin HA, Ngo CD, Salmingo JF, et al.
Evaluation of a Pharmacist-Managed Diabetes Program in a Primary Care Setting
Within an Integrated Health Care System. Journal of managed care & specialty
pharmacy. 2018;24(2):114-22.
56. Lok KY, Chan RS, Sea MM, Woo J. Nutritionist’s variation in counseling style
and the effect on weight change of patients attending a community based lifestyle
modification program. International journal of environmental research and public
Ref. code: 25606017090090UFM

70
health. 2010;7(2):413-26.
57. Siangdung S. Self-care Behaviors of Patients with Uncontrolled DM. The
Southern College Network Journal of Nursing and Public Health. 2017;4(1):191-204.
58. Austin S, Senécal C, Guay F, Nouwen A. Effects of gender, age, and diabetes
duration on dietary self-care in adolescents with type 1 diabetes: a self-determination
theory perspective. Journal of Health Psychology. 2011;16(6):917-28.
59. Bai YL, Chiou CP, Chang YY. Self‐care behaviour and related factors in older
people with Type 2 diabetes. Journal of clinical nursing. 2009;18(23):3308-15.
60. McCollum M, Hansen LB, Lu L, Sullivan PW. Gender differences in diabetes
mellitus and effectson self-care activity. Gender Medicine. 2005;2(4):246-54.
61. Dupre ME. Educational differences in health risks and illness over the life
course: A test of cumulative disadvantage theory. Social Science Research.
2008;37(4):1253-66.
62. Khomron M. SELF HEALTH CARE BEHAVIOR OF DIABETES
MELLITUS PATIENTS IN BANGNAMPRIEW DISTRICT, CHACHOENGSAO
PROVINCE. 2557.
63. Katon WJ, Rutter C, Simon G, Lin EH, Ludman E, Ciechanowski P, et al. The
association of comorbid depression with mortality in patients with type 2 diabetes.
Diabetes care. 2005;28(11):2668-72.
64. Ali S, Stone M, Peters J, Davies M, Khunti K. The prevalence of co‐morbid
depression in adults with Type 2 diabetes: a systematic review and meta‐analysis.
Diabetic Medicine. 2006;23(11):1165-73.
65. Wang Z, do Carmo JM, Aberdein N, Zhou X, Williams JM, da Silva AA, et al.
Synergistic Interaction of Hypertension and Diabetes in Promoting Kidney Injury and
the Role of Endoplasmic Reticulum StressNovelty and Significance. Hypertension.
2017;69(5):879-91.
66. Warraich HJ, Rana JS. Dyslipidemia in diabetes mellitus and cardiovascular
disease. Cardiovascular Endocrinology & Metabolism. 2017;6(1):27-32.
67. Piette JD, Schillinger D, Potter MB, Heisler M. Dimensions of Patient‐provider
Communication and Diabetes Self‐care in an Ethnically Diverse Population. Journal of
General Internal Medicine. 2003;18(8):624-33.
Ref. code: 25606017090090UFM
71
68. Bundesmann R, Kaplowitz SA. Provider communication and patient
participation in diabetes self-care. Patient education and counseling. 2011;85(2):143-7.
69. CHAISIN C. Ordinal logistic regression for predicting controllability of glyceic
level among Type 2 Diabetes Patients at Sisaket Hospital. Mahidol University: Mahidol
University; 2014.
70. Riangkam C, Wattanakitkrileart D, Ketcham A, Sriwijitkamol A. Health
literacy, self-efficacy, age and visual acuity predicting on self-care behaviors in patients
with type 2 diabetes. Journal of Nursing Science. 2016;34(4):35-46.
71. Phetarvut S, Watthayu N, Suwonnaroop N. Factors predicting diabetes self-
management behavior among patients with diabetes mellitus type 2. Journal of Nursing
Science. 2011;29(4):18-26.
Ref. code: 25606017090090UFM

APPENDICES
Ref. code: 25606017090090UFM
72
APPENDIX A
Questionnaire (English)
IDNumber: ……………
Health care provider-patient communication and self-care behaviors among
Type 2 Diabetes at Mahosot Hospital, Vientiane Capital, Lao PDR
Date of data collection: ……………………. HN: ……………………………
Pleases fill in the space or mark (√) on the questionnaire as appropriate.
Part I: Personal Characteristics
1.1 Age: ……….years
1.2 Gender: 1 Male 2 female
1.3 Marital status:
1 Single 2 married 3 divorced/separated
4 widowed
1.4 Educational levels:
1 Illiterate
2 primary school 3 Secondary school 4 High school
5 College/university
1.5 Occupations
1 Laborer
2 self-employed 3 government employee
4 Company employee 5 Agriculturist
6 other (specify) …………….
1.6 Religion
1 Buddhist
2 Christian 3 Animist 4 Other (specify): ……………
1.7 Family income (per month)
1 500,000 – 1,000,000 kip
2 1,100,000 – 1,500,000 kip
3 1,600,000 – 2,000,000 kip
4 2,100,000 – 2,500,000 kip
5 > 2,500,000 kip
Ref. code: 25606017090090UFM

73
1.8 Do you have any health security?
1 No
2 Yes If “yes”, please specify type of health security.
1 Public Social Security
2 Corporate Social Security
3 Social Security for people
4 other (specify) …………
1.9 History of blood related member Diabetes Mellitus
1 No
2 Yes “If yes “, who are they (multiple responses)
1 Father
2 Mother 3 Brothers
4 Sisters
5 Other (specify): …………..
Part II: Diseases status
2.1 Duration of diabetes …………years
2.2 Current medication
1 Single oral hyperglycemic agent (OHA)
2 Combination of (OHA)
3 (OHA) + Insulin inject
4 Insulin injection
5 life style modification only (no medication)
2.3 Use of alternative medicine
1 No
2 Yes what do you use? (Multiple responses)
1 acupuncture
2 moxibustion
3 herbal
4 healthier foods
2.4 Co-morbidity
1 No
2 Yes “If yes”, copy all co-morbidities (multiple responses)
1 Obesity 2 Hypertension 3 Dyslipidemia 4 Other………
2.5 Diabetes complications
1 No
2 Yes “If yes”, what are they (multiple responses)
1 Diabetic Retinopathy
2 Diabetic Neuropathy
3 Diabetic Nephropathy
4 Heart disease
5 Peripheral vascular disease
6 Diabetes foot/amputation
7 other (specify) ………………
Ref. code: 25606017090090UFM

74
2.6 FBS1 …………… (Date of FBS1 date……/month ……/year ………) In Current
FBS2 …………… (Date of FBS2 date……/month ……/year ……….) Last visit
2.7 Weight _ _._ kgs. Height _ _ _ cms (in current visit)
Part III: Self-care behaviors
What you have been doing in the past month. For each questions below
place a (√) in the box that best answers to your situation.
3.1 How many times you have meal a day?
1 1 time
2 2 times 3 3 times
4 4 times
3.2 Which time you have meal following by times?
1 Never
2 Rarely 3 Sometimes
4 Regular
3.3 Have you ever eaten instant food (Mama, YumYum, WaiWai, rice porridge)?
1 No
2 Yes Have you ever read nutrition label, especially amount of sodium?
1 Never 2 Rarely 3 Sometimes 4 Regular
3.4 Have you ever eaten the cooked food (noodle soup, rice noodles…etc)?
1 No
2 Yes did you add sugar in the cooking food?
1 Never
2 Rarely 3 Sometimes
4 Regular
Did you add as monosodium glutamate in the cooking food?
1 Never
2 Rarely 3 Sometimes
4 Regular
Did you add fish sauce in the cooking food?
1 Never
2 Rarely 3 Sometimes
4 Regular
3.5 Have you eat fermented fish?
1 Never 2 1-2 times per month
3 4-5 times per month
4 Regular
3.6 Do you add fermented fish in while you are cooking food?
1 Never 2 1-2 times per month
3 4-5 times per month
4 Regular
3.7 Do you add monosodium glutamate in any kinds of your cooking food?
1 Never 2 1-2 times per month
3 4-5 times per month
4 Regular
Ref. code: 25606017090090UFM
75
3.8 Have you ever eaten sweet fruits (ripe mango, banana, longan, durian, rambutan,
papaya)?
1 Never 2 1-2 times per month
3 4-5 times per month
4 Regular
3.9 Have you ever eaten dry fruits (dries banana, crispy banana)?
1 Never 2 1-2 times per month
3 4-5 times per month
4 Regular
3.10 Have you ever eaten fish?
1 Never 2 1-2 times per week
3 3-4 times per week
4 5-6 times per week
4 everyday
3.11 Have you ever eaten high fat foods (fried banana, French fries, coconut milk, fresh
butter …)
1 Never 2 1-2 times a week 3 3-4 times a week 4 5-6 times a week
5 everyday
3.12 Have you ever eaten green vegetables (morning glory, broccoli, cabbage …)
1 Never 2 1-2 times a week 3 3-4 times a week
4 5-6 times a week
5 everyday
3.13 Did you eaten out?
1 No
2 Yes how often did you eaten out an a week?
1 1 day
2 2 days 3 3 days
4 4 days
What kind of food would you like when you eaten out?
1 salt food
2 spicy food 3 fat food 4 sweet food
3.14 Do you smoke?
1 Never
2 Quit smoking when did you quit smoking? ….. Years …… months
3 Current smoking how much do you smoking a day?
1 1 pack
2 2 packs
3 3 packs
4 > 3 packs
Your current smoking compared to last 6 months.
1 Less heavy smoking 2 Same heavy smoking
3 Heavies smoking
Ref. code: 25606017090090UFM

76
3.15 Do you drink alcohol?
1 Never
2 Quit drinking when did you quit drinking alcohol? ….. Years …… months
3 Current drinking how often did you drinking?
1 1-2 times per month
2 1-2 times per week
3 everyday
4 other (specify) …………
Your current alcohol drinking compared to last 6 months.
1 Less heavy drinking alcohol
2 Same heavy drinking alcohol
3 Heavies drinking alcohol
3.16 Have you ever done physical activity?
1 No if No, why? (Next to 19)
1 don’t have free time
2 don’t need
3 burn oneself out
4 other (specify) …………..
2 Yes if Yes, how often did you done physical activity?
1 1-2 time per week 2 3-4 time per week
3 5-6 time per week 4 everyday
3.17 What kind of your daily physical activities? (multiple respond)
1 walking
2 swimming 3 aerobics
4 football
5 other (specify) ……………
3.18 How long you physical activity?
1 < 10 minutes 2 10-15 minutes
3 16-30 minutes 4 > 30 minutes
3.19 Do you check your blood sugar at home?
1 No Why?
1 no equipment 2 not sure to testing 3 other (specify)…………
2 Yes “if yes” how often did you have blood sugar checked?
1 1 time a day 2 2 times a day
3 3 times a week
Ref. code: 25606017090090UFM

77
3.20 Have you ever examined your feet for sores or wounds?
1 No
2 Yes “if yes” how often do you have examined?
1 Rarely
2 Sometimes 3 Regular
3.21 Have you ever forgotten to take diabetic drug?
1 No
2 Yes 1) how often did you forget on average in a week? ……. Times/week
2) What do you do after recall?
1 Take Diabetic drug immediately after recall
2 Take Diabetic drug over dose in next day
3 Do nothing
3.22 Have you ever spent overnight in other places or travelling to other provinces?
1 No
2 Yes Do you bring diabetes drugs along?
1 Never
2 Rarely 3 Sometimes
4 Regular
3.23 Do you have stress in the last 1 months?
1 No
2 Yes 1) What was your stress level?
1 mild
2 moderate 3 high
2) Frequency of stress on average in a week.………. Days/week
Part IV: Social supports
We would like to know how your family responds to your diabetes self-care
program. Read each questions and check (√) the box that corresponds best to your
situation.
No How often……… Never Sometimes Always
4.1 Your family member encourage you to eat
the right foods for diabetes diet.
1
2 3
4.2 Your family member selects food choices
required for diabetes diet.
1
2 3
4.3 Your family member watch what you eat to
make sure that you eat the right food.
1
2 3
Ref. code: 25606017090090UFM

78
4.4 You family member tell you when you’ve
eaten too much or too little food
1
2 3
4.5 Your family members suggest you to do
more physical activities.
1
2 3
4.6 Your family member invite you to join them
exercising.
1
2 3
4.7 Your family member congratulate or praise
you whenever you exercising regularly
1
2 3
4.8 Your family member ask you about the
results of your blood tests
1
2 3
4.9 Your family member remind you to test
your blood sugar
1
2 3
4.10 Your family member praise you when you
testing your blood sugar by yourself
1
2 3
4.11 Your family members remind you to inspect
your feet.
1
2 3
4.12 Your family members remind you to take
your medicine.
1
2 3
4.13 Your family members check the pill after
you’ve taken your medicine to make sure
that you have done
1
2 3
We would like to know how your peer responds to your diabetes self-care program
No How often……… Never Sometimes Always
4.14 Your peer urge you to diabetic check by
following with physician
1
2 3
4.15 Your peer listen to your concern give
advice whenever you express your diabetes
problem and challenge you face
1
2 3
4.16 Your peer give you a valuable information
for your health and wellbeing
1
2 3
Ref. code: 25606017090090UFM
79
4.17 Your peer give you an assistance whenever
you need diabetes care
1
2 3
4.18 Your peer provide advice and suggestions
whenever you need diabetes care
1
2 3
4.19 Your peer show their support whenever you
get distress or any problem
1
2 3
Sources information among Type 2 Diabetes Mellitus
4.20 Did you receive some information on Type 2 Diabetes Mellitus?
1 No (Next Part V)
2 Yes where did you receive? (Multiple respond)
1 Health care providers
2 Television 3 Radio
4 Newspapers 5 social media
6 other (specific)………...
What is the following topic that you have to know? (Multiple respond)
1 cause of Type 2 Diabetes
2 effective of Type 2 Diabetes
3 Type 2 Diabetes complications
4 self-care practices
5 other (specific) ………………..
4.21 Did information you received are important to you?
1 Never 2 Sometimes
3 always
Part V: Health care provider-Patient communication
The next questions are about your experiences in talking with your
physician at this hospital during the last 6 months. Please check mark (√) on next box
in front of the word or phrase that matches your situation.
No How often……… Never Sometimes Always
5.1 Your physician informed you about your
diabetes status.
1
2 3
5.2 Your physician at this hospital explained to
how to take medicine.
1
2 3
5.3 You were in trouble understanding your
physician explanation on how to take
medicine.
1
2 3
Ref. code: 25606017090090UFM
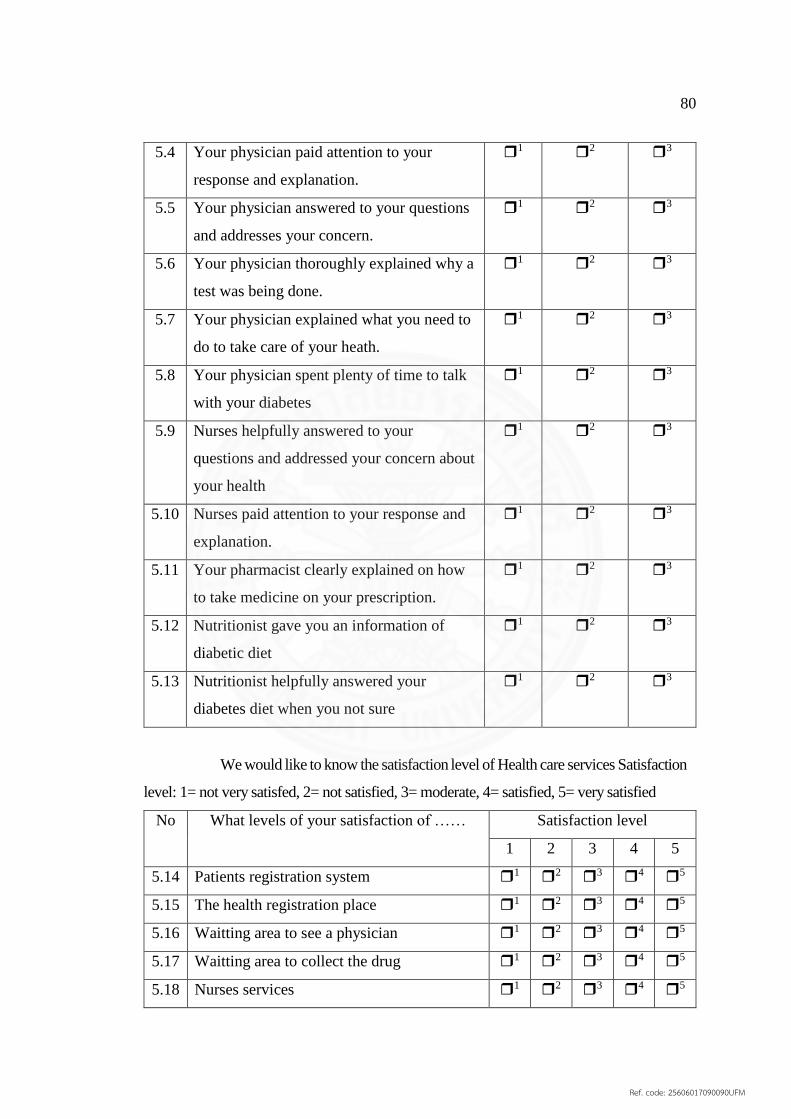
80
5.4 Your physician paid attention to your
response and explanation.
1
2 3
5.5 Your physician answered to your questions
and addresses your concern.
1
2 3
5.6 Your physician thoroughly explained why a
test was being done.
1
2 3
5.7 Your physician explained what you need to
do to take care of your heath.
1
2 3
5.8 Your physician spent plenty of time to talk
with your diabetes
1
2 3
5.9 Nurses helpfully answered to your
questions and addressed your concern about
your health
1
2 3
5.10 Nurses paid attention to your response and
explanation.
1
2 3
5.11 Your pharmacist clearly explained on how
to take medicine on your prescription.
1
2 3
5.12 Nutritionist gave you an information of
diabetic diet
1
2 3
5.13 Nutritionist helpfully answered your
diabetes diet when you not sure
1
2 3
We would like to know the satisfaction level of Health care services Satisfaction
level: 1= not very satisfed, 2= not satisfied, 3= moderate, 4= satisfied, 5= very satisfied
No What levels of your satisfaction of …… Satisfaction level
1 2 3 4 5
5.14 Patients registration system 1
2 3
4 5
5.15 The health registration place 1
2 3
4 5
5.16 Waitting area to see a physician 1
2 3
4 5
5.17 Waitting area to collect the drug 1
2 3
4 5
5.18 Nurses services 1
2 3
4 5
Ref. code: 25606017090090UFM

81
5.19 Physician services 1
2 3
4 5
5.20 Pharmacists services 1
2 3
4 5
5.21 Polite, humility, verbal speech of them 1
2 3
4 5
5.22 Responding to your concerns and relatives
willingly
1
2 3
4 5
5.23 Provide information respect your request 1
2 3
4 5
5.24 Knowledge of the health care providers 1
2 3
4 5
5.25 You received respect and and equaty
treatment from health care providers
1
2 3
4 5
5.26 The quickly and availability of services 1
2 3
4 5
5.27 The service of making an opportunity with a
physician
1
2 3
4 5
Thank you so much
Ref. code: 25606017090090UFM
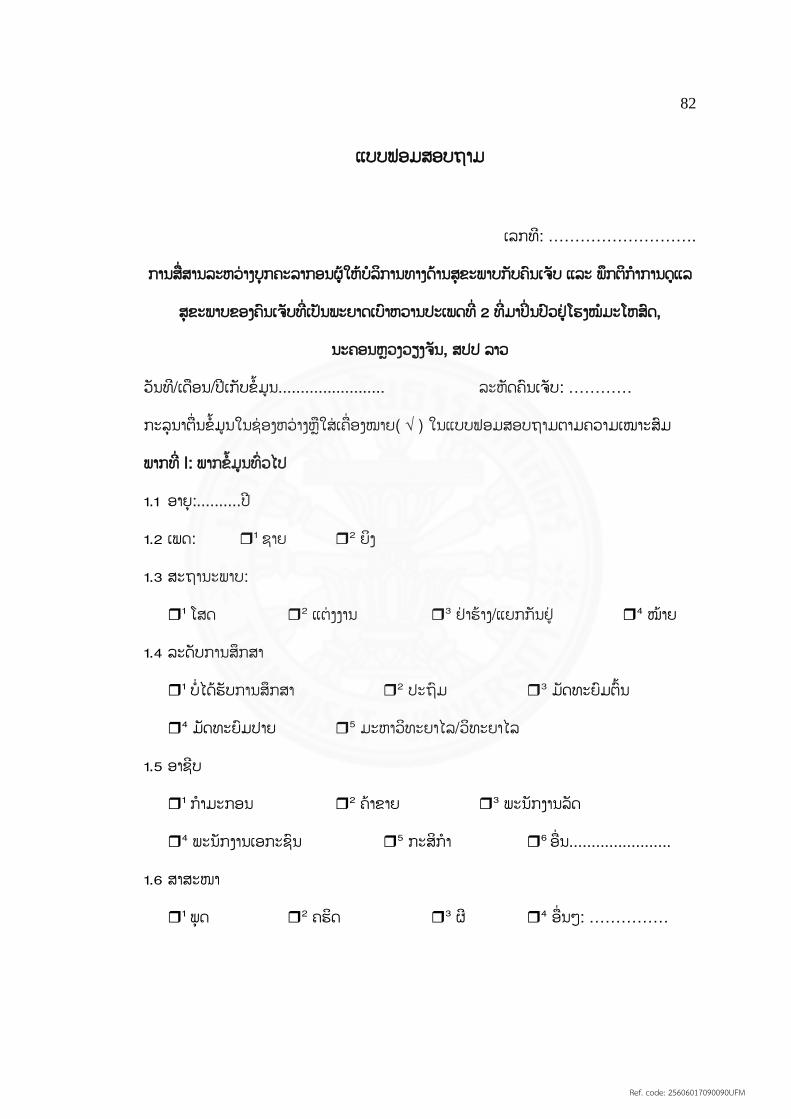
82
ແບບຟອມສອບຖາມ
ເລກທ:ີ ……………………….
ການສ ື່ ສານລະຫວື່ າງບຸກຄະລາກອນຜູ ູ້ໃຫ ູ້ບໍລກິານທາງດ ູ້ານສຸຂະພາບກບັຄນົເຈບັ ແລະ ພກຶຕກິາໍການດູແລ
ສຸຂະພາບຂອງຄນົເຈບັທີື່ ເປັນພະຍາດເບາົຫວານປະເພດທີື່ 2 ທີື່ ມາປິື່ ນປົວຢູື່ ໂຮງໝໍມະໂຫສດົ,
ນະຄອນຫຼວງວຽງຈນັ, ສປປ ລາວ
ວນັທ/ີເດ ອນ/ປີເກບັຂໍ ູ້ມູນ........................ ລະຫດັຄນົເຈບັ: …………
ກະລຸນາຕ ື່ ນຂໍ ູ້ມູນໃນຊື່ ອງຫວື່ າງຫຼ ໃສື່ ເຄ ື່ ອງໝາຍ( √ ) ໃນແບບຟອມສອບຖາມຕາມຄວາມເໝາະສມົ
ພາກທີື່ I: ພາກຂໍ ູ້ມນູທົື່ ວໄປ
1.1 ອາຍຸ:..........ປີ
1.2 ເພດ: 1 ຊາຍ
2 ຍງິ
1.3 ສະຖານະພາບ:
1 ໂສດ
2 ແຕື່ ງງານ 3 ຢື່ າຮ ູ້າງ/ແຍກກນັຢູື່
4 ໝູ້າຍ
1.4 ລະດບັການສກຶສາ
1 ບໍື່ ໄດ ູ້ຮບັການສກຶສາ
2 ປະຖມົ 3 ມດັທະຍມົຕົ ູ້ນ
4 ມດັທະຍມົປາຍ
5 ມະຫາວທິະຍາໄລ/ວທິະຍາໄລ
1.5 ອາຊບີ
1 ກາໍມະກອນ
2 ຄ ູ້າຂາຍ 3 ພະນກັງານລດັ
4 ພະນກັງານເອກະຊນົ
5 ກະສກິາໍ 6 ອ ື່ ນ.......................
1.6 ສາສະໜາ
1 ພຸດ
2 ຄຮດິ 3 ຜ ີ
4 ອ ື່ ນໆ: ……………
Ref. code: 25606017090090UFM

83
1.7 ລາຍຮບັຄອບຄວົ (ເທົື່ າໃດຕໍື່ ເດ ອນ)
1 500,000 – 1,000,000 ກບີ
2 1,100,000 – 1,500,000 ກບີ
3 1,600,000 – 2,000,000 ກບີ
4 2,100,000 – 2,500,000 ກບີ
5 > 2,500,000 ກບີ
1.8 ທື່ ານໄດ ູ້ໃຊ ູ້ບດັປະກນັສຸຂະພາບບໍ
1 ບໍື່ ໃຊ ູ້
2 ໃຊ ູ້ ຖູ້າໃຊ ູ້ ທື່ ານໃຊ ູ້ບດັປະກນັສຸຂະພາບພາກສື່ ວນໃດ?
1 ປະກນັສງັຄມົລດັ
2 ປະກນັສງັຄມົເອກະຊນົ
3 ປະກນັສັງັຄມົສື່ ວນບູກຄນົ
4 ອ ື່ ນໆ ……………
1.9 ສະມາຊກີຄອບຄວົທື່ ານມປີະຫວດັເປັນພະຍາດເບາົຫວານບໍ?
1 ບໍື່
2 ມ ີ “ຖູ້າມ ີ“, ໃຜທີື່ ເປັນ (ສາມາດເລ ອກໄດ ູ້ຫຼາຍຂໍ ູ້)
1 ພໍື່
2 ແມື່ 3 ອ ູ້າຍ/ນ ູ້ອງຊາຍ
4 ເອ ູ້ອຍ/ນ ູ້ອງສາວ
5 ພໍື່ ຕູ ູ້ແມື່ ຕູ ູ້
ພາກທີື່ II: ສະຖານະພາບຂອງພະຍາດ (ຈາກປ ູ້ມບນັທ ກຄນົເຈບັ)
2.1 ໄລຍະການເປັນພະຍາດເບາົຫວານ ..........ປີ
2.2 ການກນີຢາໃນປັດຈບຸນັ
1 ຢາກນີລດົນໍ ູ້າຕານໃນເລ ອດ
2 ກນີຢາລດົນໍ ູ້າຕານໃນເລ ອດຮື່ ວມກບັຢາທີື່ ບໍື່ ແມື່ ນປົວເບາົຫວານ
3 ກນີຢາລດົນໍ ູ້າຕານໃນເລ ອດຮື່ ວມກບັສກັຢາອນິຊູລນິ
4 ສກັຢາອນິຊູລນິຢື່ າງດຽວ
5 ບໍື່ ໄດ ູ້ກນີຢາ
Ref. code: 25606017090090UFM
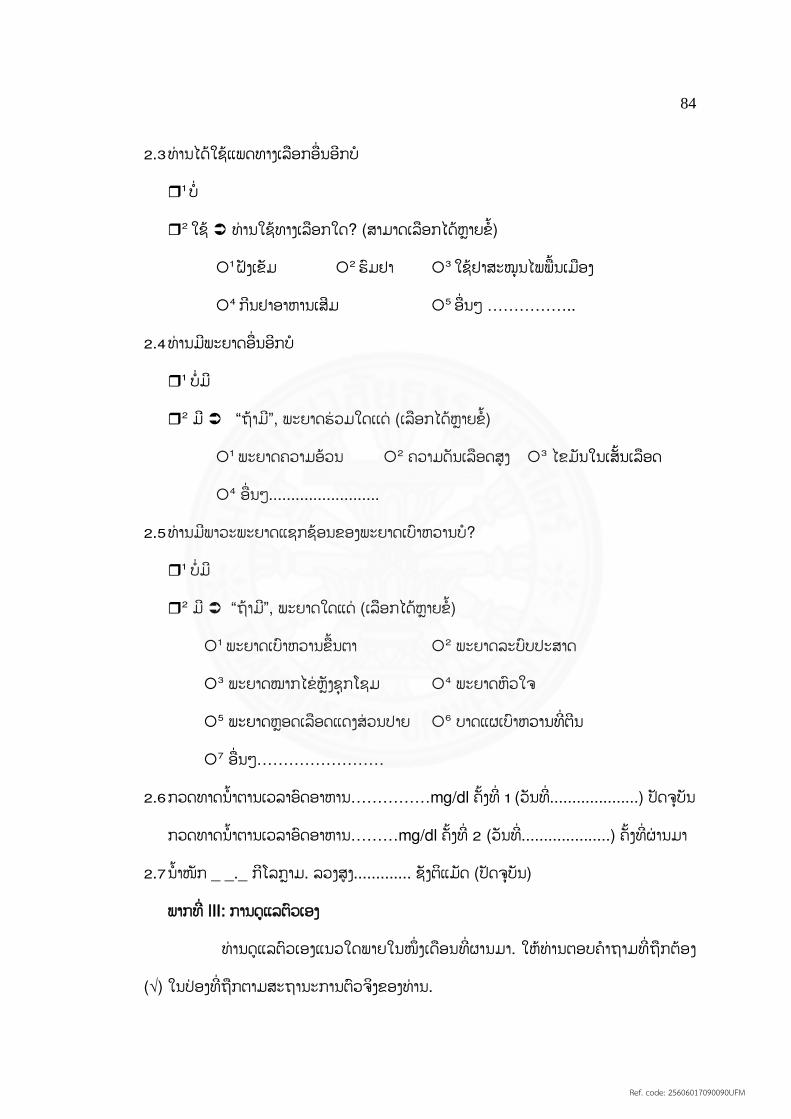
84
2.3 ທື່ ານໄດ ູ້ໃຊ ູ້ແພດທາງເລ ອກອ ື່ ນອກີບໍ
1 ບໍື່
2 ໃຊ ູ້ ທື່ ານໃຊ ູ້ທາງເລ ອກໃດ? (ສາມາດເລ ອກໄດ ູ້ຫຼາຍຂໍ ູ້)
1 ຝັງເຂມັ
2 ຮມົຢາ 3 ໃຊ ູ້ຢາສະໝຸນໄພພ ູ້ນເມ ອງ
4 ກນີຢາອາຫານເສມີ
5 ອ ື່ ນໆ ……………..
2.4 ທື່ ານມພີະຍາດອ ື່ ນອກີບໍ
1 ບໍື່ ມ ີ
2 ມ ີ “ຖູ້າມ”ີ, ພະຍາດຮື່ ວມໃດເເດື່ (ເລ ອກໄດ ູ້ຫຼາຍຂໍ ູ້)
1 ພະຍາດຄວາມອ ູ້ວນ
2 ຄວາມດນັເລ ອດສູງ 3 ໄຂມນັໃນເສັ ູ້ນເລ ອດ
4 ອ ື່ ນໆ.........................
2.5 ທື່ ານມພີາວະພະຍາດແຊກຊ ູ້ອນຂອງພະຍາດເບາົຫວານບໍ?
1 ບໍື່ ມ ີ
2 ມ ີ “ຖູ້າມ”ີ, ພະຍາດໃດແດື່ (ເລ ອກໄດ ູ້ຫຼາຍຂໍ ູ້)
1 ພະຍາດເບາົຫວານຂ ູ້ນຕາ
2 ພະຍາດລະບບົປະສາດ
3 ພະຍາດໝາກໄຂື່ ຫຼງັຊຸກໂຊມ
4 ພະຍາດຫວົໃຈ
5 ພະຍາດຫຼອດເລ ອດແດງສື່ ວນປາຍ
6 ບາດແຜເບາົຫວານທີື່ ຕນີ
7 ອ ື່ ນໆ……………………
2.6 ກວດທາດນໍ ູ້າຕານເວລາອດົອາຫານ……………mg/dl ຄັ ູ້ງທີື່ 1 (ວນັທີື່ ....................) ປັດຈບຸນັ
ກວດທາດນໍ ູ້າຕານເວລາອດົອາຫານ………mg/dl ຄັ ູ້ງທີື່ 2 (ວນັທີື່ ....................) ຄັ ູ້ງທີື່ ຜື່ ານມາ
2.7 ນໍ ູ້າໜກັ _ _._ ກໂີລກາຼມ. ລວງສູງ............. ຊງັຕແິມດັ (ປັດຈບຸນັ)
ພາກທີື່ III: ການດູແລຕວົເອງ
ທື່ ານດູແລຕວົເອງແນວໃດພາຍໃນໜຶື່ ງເດ ອນທີື່ ຜານມາ. ໃຫ ູ້ທື່ ານຕອບຄໍາຖາມທີື່ ຖ ກຕ ູ້ອງ
(√) ໃນປື່ ອງທີື່ ຖ ກຕາມສະຖານະການຕວົຈງິຂອງທື່ ານ.
Ref. code: 25606017090090UFM

85
3.1 ທື່ ານກນີເຂົ ູ້າຈກັຄາບຕໍື່ ມ ູ້
1 1 ຄາບ
2 2 ຄາບ 3 3 ຄາບ
4 4 ຄາບ
3.2 ທື່ ານກນີເຂົ ູ້າແຕື່ ລະຄາບຖ ກຕາມເວລາບໍ?
1 ບໍື່
2 ດນົໆເທ ື່ ອໜຶື່ ງ 3 ຖ ກບາງຄັ ູ້ງຄາວ
4 ຖ ກທຸກໆຄັ ູ້ງ
3.3 ທື່ ານກນີອາຫານສໍາເລດັຮູບ (ໝມີາມື່ າ, ໝຍີາໍຍາໍ, ໝີື່ ໄວໄວ, ໂຈ໋ກ .........)
1 ບໍື່ ເຄຍີ
2 ເຄຍີ ທື່ ານເຄຍີອື່ ານສື່ ວນປະກອບອາຫານໂດຍສະເພາະປະລມິານເກ ອໂຊດຽມບໍ
1 ບໍື່ 2 ດນົໆຄັ ູ້ງໜຶື່ ງ 3 ອື່ ານບາງຄັ ູ້ງຄາວ 4 ອື່ ານທຸກຄັ ູ້ງ
3.4 ທື່ ານໄດ ູ້ກນີອາຫານປະເພດເປັນເສັ ູ້ນ (ເຝີ, ເຂົ ູ້າປຽກ, ເຂົ ູ້າປຸູ້ນ)
1 ບໍື່
2 ໄດ ູ້ ທື່ ານໄດ ູ້ປຸງນໍ ູ້າຕານໃສື່ ບໍ?
1 ບໍື່ 2 ດນົໆຄັ ູ້ງໜຶື່ ງ
3 ປຸງບາງຄັ ູ້ງຄາວ 4 ປຸງທຸກຄັ ູ້ງ
ທື່ ານໄດ ູ້ປຸງແປູ້ງນວົໃສື່ ບໍ?
1 ບໍື່ 2 ດນົໆຄັ ູ້ງໜຶື່ ງ
3 ປຸງບາງຄັ ູ້ງຄາວ 4 ປຸງທຸກຄັ ູ້ງ
ທື່ ານໄດ ູ້ປຸງນໍ ູ້າປາໃສື່ ບໍ?
1 ບໍື່ 2 ດນົໆຄັ ູ້ງໜຶື່ ງ
3 ປຸງບາງຄັ ູ້ງຄາວ 4 ປຸງທຸກຄັ ູ້ງ
3.5 ທື່ ານກນີປາແດກບໍ?
1 ບໍື່
2 1-2 ຄັ ູ້ງຕໍື່ ເດ ອນ 3 4-5 ຄັ ູ້ງຕໍື່ ເດ ອນ
4 ໃສື່ ທຸກຄັ ູ້ງ
3.6 ທື່ ານໄດ ູ້ປຸງປາແດກໃສື່ ໃນອາຫານທີື່ ແຕື່ ງສຸກບໍ?
1 ບໍື່
2 1-2 ຄັ ູ້ງຕໍື່ ເດ ອນ 3 4-5 ຄັ ູ້ງຕໍື່ ເດ ອນ
4 ໃສື່ ທຸກຄັ ູ້ງ
3.7 ທື່ ານໄດ ູ້ປຸງແປູ້ງນວົໃສື່ ອາຫານທີື່ ແຕື່ ງສຸກບໍ?
1 ບໍື່
2 1-2 ຄັ ູ້ງຕໍື່ ເດ ອນ 3 4-5 ຄັ ູ້ງຕໍື່ ເດ ອນ
4 ໃສື່ ທຸກຄັ ູ້ງ
Ref. code: 25606017090090UFM

86
3.8 ທື່ ານກນີໝາກໄມ ູ້ທີື່ ມລີດົຫວານ (ໝາກມື່ ວງສຸກ, ໝາກກ ູ້ວຍ, ລໍາໃຍ, ທຸລຽນ, ໝາກຮຸື່ ງ)?
1 ບໍື່
2 1-2 ຄັ ູ້ງຕໍື່ ເດ ອນ 3 4-5 ຄັ ູ້ງຕໍື່ ເດ ອນ
4 ກນີປະຈາໍ
3.9 ທື່ ານກນີໝາກໄມ ູ້ແຫ ູ້ງບໍ (ກ ູ້ວຍຕາດ, ກ ູ້ວຍປື່ ຽນ.......)
1 ບໍື່
2 1-2 ຄັ ູ້ງຕໍື່ ເດ ອນ 3 4-5 ຄັ ູ້ງຕໍື່ ເດ ອນ
4 ກນີປະຈາໍ
3.10 ທື່ ານກນີປາບໍ
1 ບໍື່
2 1-2 ຄັ ູ້ງຕໍື່ ອາທດິ 3 3-4 ຄັ ູ້ງຕໍື່ ອາທດິ
4 5-6 ຄັ ູ້ງຕໍື່ ອາທດິ
5 ທຸກໆມ ູ້
3.11 ທື່ ານມກັກນີອາຫານທີື່ ມມີນັ (ທອດໝາກກ ູ້ວຍ, ທອດມນັຝຣັື່ ງ, ກະທ,ິ ເນຍີ ...)
1 ບໍື່
2 1-2 ຄັ ູ້ງຕໍື່ ອາທດິ 3 3-4 ຄັ ູ້ງຕໍື່ ອາທດິ
4 5-6 ຄັ ູ້ງຕໍື່ ອາທດິ
5 ທຸກໆມ ູ້
3.12 ທື່ ານກນີຜດັ (ຜກັບົ ູ້ງ, ຜກັກະລໍື່ າປີ, ຜກັກາດນາ,ຜກັບວົ,ຜກັຕໍານນີ ....)
1 ບໍື່
2 1-2 ຄັ ູ້ງຕໍື່ ອາທດິ 3 3-4 ຄັ ູ້ງຕໍື່ ອາທດິ
4 5-6 ຄັ ູ້ງຕໍື່ ອາທດິ
5 ທຸກໆມ ູ້
3.13 ທື່ ານໄດ ູ້ອອກໄປກນີເຂົ ູ້ານອກບ ູ້ານບໍ?
1 ບໍື່
2 ໄດ ູ້ ຈກັມ ູ້ອາທດິ?
1 1 ມ ູ້
2 2 ມ ູ້ 3 3 ມ ູ້
4 4 ມ ູ້
ອາຫານປະເພດໃດທີື່ ທື່ ານມກັອອກໄປກນີຢູື່ ນອກບ ູ້ານ
1 ອາຫານປະເພດເຄມັ
2 ອາຫານປະເພດເຜດັ 3 ອາຫານປະເພດມນັ
4 ອາຫານປະເພດຫວານ
Ref. code: 25606017090090UFM
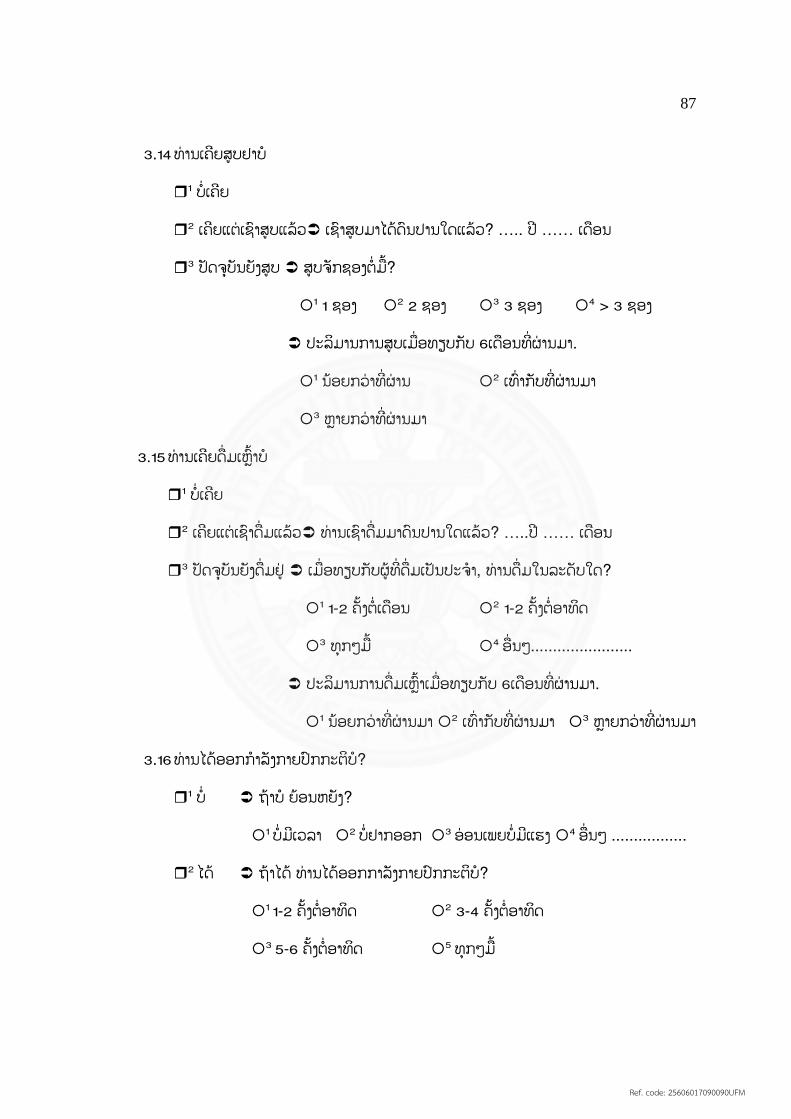
87
3.14 ທື່ ານເຄຍີສູບຢາບໍ
1 ບໍື່ ເຄຍີ
2 ເຄຍີແຕື່ ເຊາົສູບແລ ູ້ວ ເຊາົສູບມາໄດ ູ້ດນົປານໃດແລ ູ້ວ? ….. ປີ …… ເດ ອນ
3 ປັດຈບຸນັຍງັສູບ ສູບຈກັຊອງຕໍື່ ມ ູ້?
1 1 ຊອງ
2 2 ຊອງ 3 3 ຊອງ
4 > 3 ຊອງ
ປະລມິານການສູບເມ ື່ ອທຽບກບັ 6ເດ ອນທີື່ ຜື່ ານມາ.
1 ນ ູ້ອຍກວື່ າທີື່ ຜື່ ານ
2 ເທົື່ າກບັທີື່ ຜື່ ານມາ
3 ຫຼາຍກວື່ າທີື່ ຜື່ ານມາ
3.15 ທື່ ານເຄຍີດ ື່ ມເຫຼົ ູ້າບໍ
1 ບໍື່ ເຄຍີ
2 ເຄຍີແຕື່ ເຊາົດ ື່ ມແລ ູ້ວ ທື່ ານເຊາົດ ື່ ມມາດນົປານໃດແລ ູ້ວ? …..ປີ …… ເດ ອນ
3 ປັດຈບຸນັຍງັດ ື່ ມຢູື່ ເມ ື່ ອທຽບກບັຜູ ູ້ທີື່ ດ ື່ ມເປັນປະຈາໍ, ທື່ ານດ ື່ ມໃນລະດບັໃດ?
1 1-2 ຄັ ູ້ງຕໍື່ ເດ ອນ
2 1-2 ຄັ ູ້ງຕໍື່ ອາທດິ
3 ທຸກໆມ ູ້
4 ອ ື່ ນໆ.......................
ປະລມິານການດ ື່ ມເຫຼົ ູ້າເມ ື່ ອທຽບກບັ 6ເດ ອນທີື່ ຜື່ ານມາ.
1 ນ ູ້ອຍກວື່ າທີື່ ຜື່ ານມາ 2 ເທົື່ າກບັທີື່ ຜື່ ານມາ 3 ຫຼາຍກວື່ າທີື່ ຜື່ ານມາ
3.16 ທື່ ານໄດ ູ້ອອກກາໍລງັກາຍປົກກະຕບໍິ?
1 ບໍື່ ຖ ູ້າບໍ ຍ ູ້ອນຫຍງັ?
1 ບໍື່ ມເີວລາ 2 ບໍື່ ຢາກອອກ 3 ອື່ ອນເພຍບໍື່ ມແີຮງ 4 ອ ື່ ນໆ .................
2 ໄດ ູ້ ຖ ູ້າໄດ ູ້ ທື່ ານໄດ ູ້ອອກກ າລງັກາຍປົກກະຕບໍິ?
1 1-2 ຄັ ູ້ງຕໍື່ ອາທດິ
2 3-4 ຄັ ູ້ງຕໍື່ ອາທດິ
3 5-6 ຄັ ູ້ງຕໍື່ ອາທດິ
5 ທຸກໆມ ູ້
Ref. code: 25606017090090UFM

88
3.17 ທຸກໆມ ູ້ຂອງທື່ ານມກັອອກກາໍລງັກາຍປະເພດໃດ
1 ຍື່ າງ
2 ລວຍນໍ ູ້າ 3 ເຕັ ູ້ນແອໂລບກິ
4 ເຕະບານ
5 ອ ື່ ນໆ .................
3.18 ແຕື່ ລະເທ ື່ ອທື່ ານໃຊ ູ້ເວລາຈກັນາທ?ີ
1 < 10 ນາທ ີ
2 10-15 ນາທ ີ 3 16-30 ນາທ ີ
4 > 30 ນາທ ີ
3.19 ທື່ ານໄດ ູ້ກວດນໍ ູ້າຕານໃນເລ ອດທີື່ ບ ູ້ານບໍ
1 ບໍື່ ເຄຍີ ຍ ູ້ອນຫຍງັ?
1 ບໍື່ ມອຸີປະກອນ
2 ບໍື່ ໝັື່ ນໃຈວທິກີວດ 3 3 ອ ື່ ນໆ....................
2 ໄດ ູ້ກວດ “ຖູ້າກວດ” ທື່ ານໄດ ູ້ກວດເລ ື່ ອຍໆປານໃດ?
1 1 ຄັ ູ້ງຕໍື່ ມ ູ້
2 2 ຄັ ູ້ງຕໍື່ ມ ູ້ 3 3 ຄັ ູ້ງຕໍື່ ມ ູ້
3.20 ທື່ ານເຄຍີກວດວື່ າມບີາດແຜທີື່ ຕນີຂອງທື່ ານບໍ
1 ບໍື່ ເຄຍີ
2 ເຄຍີ “ຖູ້າເຄຍີ” ທື່ ານກວດເລ ູ້ອຍໆບໍ
1 ດນົໆເທ ື່ ອໜຶື່ ງ
2 ກວດບາງຄັ ູ້ງຄາວ 3 ກວດເປັນປະຈາໍ
3.21 ທື່ ານເຄຍີລ ມກນິຢາລດົເບາົຫວານບໍ?
1 ບໍື່ ເຄຍີ
2 ເຄຍີ 1) ທື່ ານມກັລ ມເລ ື່ ອຍປານໃດຕໍື່ ອາທດິ…….ຄັ ູ້ງ/ອາທດິ
2) ທື່ ານເຮດັແນວໃດເມ ື່ ອທື່ ານລ ມກນີຢາ?
1 ກນີຢາລດົເບາົວານທນັທຫຼີງັຈາກທື່ ານຮູ ູ້ວື່ າລ ມກນີ
2 ກນີຢາລດົເບາົຫວານເພີ ູ້ມສອງເທົື່ າໃນມ ູ້ທກັໄປ
3 ອ ື່ ນໆ…………………………………
Ref. code: 25606017090090UFM
89
3.22 ທື່ ານເຄຍີອອກໄປພກັຄ ູ້າງຄ ນຕື່ າງແຂວງບໍ?
1 ບໍື່ ເຄຍີ
2 ເຄຍີ ທື່ ານໄດ ູ້ເອາົຢາປິື່ ນປົວເບາົຫວານໄປນາໍບໍ?
1 ບໍື່ 2 ດນົໆຄັ ູ້ງໜຶື່ ງ
3 ບາງຄັ ູ້ງຄາວ 4 ເອາົໄປທຸກຄັ ູ້ງ
3.23 ໃນໄລຍະ 1 ເດ ອນຜື່ ານມານີ ູ້ທື່ ານເຄຍີມຄີວາມຄຽດບໍ?
1 ບໍື່ ເຄຍີ
2 ເຄຍີ 1) ລະດບັຄວາມຄຽດຂອງທື່ ານຢູື່ ໃນລະດບັໃດ?
1 ໜູ້ອຍໜຶື່ ງ
2 ພໍສມົຄວນ 3 ຄຽດຫຼາຍ
3.24 ຄວາມຖີື່ ສະເລື່ ຍມ ູ້ທື່ ານມຄີວາມຄຽດຕໍື່ ອາທດິ ........ມ ູ້/ອາທດິ
ພາກທີື່ IV: ການສົື່ ງເສມີທາງດ ູ້ານສງັຄມົ
ພວກເຮາົຢາກຮູ ູ້ວື່ າຄອບຄວົຂອງທື່ ານໄດ ູ້ເອາົໃຈໃສື່ ໃນການດູແລທື່ ານເປັນແນວໃດ.ໃຫ ູ້
ທື່ ານຕອບຄໍາຖາມທີື່ ຖ ກຕ ູ້ອງ (√) ໃນປື່ ອງທີື່ ຖ ກຕາມສະຖານະການຕວົຈງິຂອງທື່ ານ.
ລໍາດບັ ການສົື່ ງເສມີຈາກ...... ບໍື່ ເຄຍີ ບາງຄັ ູ້ງຄາວ ທຸກຄັ ູ້ງ
4.1 ສະມາຊກີຄອບຄວົຂອງທື່ ານໄດ ູ້ຊູກຍູ ູ້ໃຫ ູ້ທື່ ານກນີ
ອາຫານໃຫ ູ້ເໝາະກບັເພ ື່ ອຫຼກີລ ູ້ຽງອາການພະຍາດ
ເບາົຫວານ
1
2 3
4.2 ສະມາຊກີຄອບຄວົຂອງທື່ ານໄດ ູ້ເລ ອກອາຫານທີື່ ເໝາະ
ສມົສໍາລບັທື່ ານບໍ
1
2 3
4.3 ສະມາຊກີຄອບຄວົຂອງທື່ ານໄດ ູ້ເບີື່ ງວື່ າອາຫານປະເພດ
ໃດທີື່ ທື່ ານຄວນກນີໄດ ູ້
1
2 3
4.4 ສະມາຊກີຄອບຄວົຂອງທື່ ານໄດ ູ້ບອກທື່ ານບໍເວລາທີື່ ທື່ ານ
ກນີອາຫານຫຼາຍເກນີໄປຫຼ ນ ູ້ອຍເກນີໄປ
1
2 3
Ref. code: 25606017090090UFM

90
4.5 ສະມາຊກີຄອບຄວົຂອງທື່ ານໄດ ູ້ແນະນາໍກດິຈະກາໍການ
ອອກກາໍລງັກາຍໃຫ ູ້ທື່ ານ
1
2 3
4.6 ສະມາຊກີຄອບຄວົຂອງທື່ ານໄດ ູ້ພາທື່ ານໄປອອກກາໍລງັ
ກາຍຮື່ ວມກນັ
1
2 3
4.7 ສະມາຊກີຄອບຄວົຂອງທື່ ານຍນີດຫຼີ ໃຫ ູ້ການສະໜບັສະ
ໜຸນທື່ ານໃນການອອກກາໍລງັກາຍປົກກະຕ ິ
1
2 3
4.8 ສະມາຊກີຄອບຄວົຂອງທື່ ານໄດ ູ້ຖາມກື່ ຽວກບັຜນົກວດ
ລະດບັນໍ ູ້າຕານໃນເລ ອດຂອງທື່ ານບໍ
1
2 3
4.9 ສະມາຊກີຄອບຄວົຂອງທື່ ານໄດ ູ້ເຕ ອນໃຫ ູ້ທື່ ານກວດ
ລະດບັນໍ ູ້າຕານໃນເລ ອດບໍ
1
2 3
4.10 ສະມາຊກີຄອບຄວົຂອງທື່ ານໄດ ູ້ໃຫ ູ້ຄວາມສນົໃຈໃນ
ການກວດລະດບັນໍ ູ້າຕານໃນເລ ອດຂອງທື່ ານບໍ
1
2 3
4.11 ສະມາຊກີຄອບຄວົຂອງທື່ ານໄດ ູ້ເຕ ອນໃຫ ູ້ທື່ ານກວດວື່ າ
ມບີາດແຜຕນີຂອງທື່ ານບໍ
1
2 3
4.12 ສະມາຊກີຄອບຄວົຂອງທື່ ານໄດ ູ້ເຕ ອນໃຫ ູ້ທື່ ານກນີຢາ
ລດົເບາົຫວານປະຈາໍບໍ
1
2 3
4.13 ສະມາຊກີຄອບຄວົຂອງທື່ ານໄດ ູ້ກວດເບີື່ ງຢາຫຼງັຈາກ
ທື່ ານກນີຢາລດົເບາົຫວານແລ ູ້ວຫຼ ຍງັ
1
2 3
ພວກເຮາົຢາກຮູ ູ້ວື່ າເພ ື່ ອນຂອງທື່ ານໄດ ູ້ສະໜບັສະໜຸນໃນການດູແລຂອງທື່ ານເປັນແນວໃດ
ລໍາດບັ ການສົື່ ງເສມີຈາກ...... ບໍື່ ບາງຄັ ູ້ງຄາວ ທຸກຄັ ູ້ງ
4.14 ເພ ື່ ອນຂອງທື່ ານໄດ ູ້ແນະນາໍໃຫ ູ້ທື່ ານໄປຕດິຕາມພະຍາດ
ເບາົຫວານກບັທື່ ານໝໍ
1
2 3
Ref. code: 25606017090090UFM
91
4.15 ເພ ື່ ອນຂອງທື່ ານໄດ ູ້ຮບັຟັງແລະໃຫ ູ້ຄໍາແນະນາໍໃຫ ູ້ທື່ ານ
ເວລາທີື່ ທື່ ານມບີນັຫາກື່ ຽວກບັພະຍາດເບາົຫວານແລະສິື່ ງ
ທກັທາຍທີື່ ທື່ ານບໍື່ ຄາດຄດິ
1
2
3
4.16 ເພ ື່ ອນຂອງທື່ ານໄດ ູ້ໃຫ ູ້ຂໍ ູ້ມູນທີື່ ມປີະໂຫຍດທາງດ ູ້ານ
ສຸຂະພາບ ແລະ ຄຸນນະພາບຊວີດິທີື່ ດຂີ ູ້ນ
1
2 3
4.17 ເພ ື່ ອນຂອງທື່ ານໄດ ູ້ໃຫ ູ້ຄວາມຊື່ ວຍເຫຼ ອເມ ື່ ອທື່ ານທີື່
ຕ ູ້ອງການຈະດູແລພະຍາດເບາົຫວານ
1
2 3
4.18 ເພ ື່ ອນຂອງທື່ ານໄດ ູ້ໃຫ ູ້ຄໍາແນະນາໍແລະຂໍ ູ້ສະເໜແີນະຕື່ າງໆ
ໃຫ ູ້ທື່ ານໃນການດູແລຕວົເອງຂອງພະຍາດເບາົຫວານ
1
2 3
4.19 ເພ ື່ ອນຂອງທື່ ານໄດ ູ້ສະໜບັສະໜຸນທຸກຄັ ູ້ງເມ ື່ ອທື່ ານມີ
ຄວາມກງັວນົຫຼ ມບີນັຫາ
1
2 3
ຂໍ ູ້ມູນຂື່ າວສານກື່ ຽວກບັການເບີື່ ງແຍງສຸຂະພາບຂອງຄນົເຈບັທີື່ ເປັນພະຍາດເບາົຫວານ
ປະເພດທີື່ 2
4.20 ທື່ ານໄດ ູ້ຮບັຂໍ ູ້ມູນກື່ ຽວກບັພະຍາດເບາົຫວານປະເພດທີື່ 2ບໍ
1 ບໍື່ ເຄຍີ (ຂ ູ້າມໄປພາກທີື່ V)
2 ເຄຍີ ໄດ ູ້ຮບັຂໍ ູ້ມູນມາຈາກໃສ? (ເລ ອກໄດ ູ້ຫຼາຍຂໍ ູ້)
1 ຜູ ູ້ໃຫ ູ້ບໍລກິານທາງດ ູ້ານສຸຂະພາບ
2 ໂທລະທດັ 3 ວທິະຍຸ
4 ໜງັສ ພມີ
5 ສ ທາງສງັຄມົ 6 ອ ື່ ນໆ………………..
ຂໍ ູ້ມູນທີື່ ທື່ ານຮູ ູ້ເວົ ູ້າເລ ື່ ອງຫຍງັ (ເລ ອກໄດ ູ້ຫຼາຍຂໍ ູ້)
1 ສາເຫດຂອງພະຍາດເບາົຫວານປະເພດທີື່ 2 2ຜນົສະທ ູ້ອນຂອງພະຍາດເບາົຫວານ
3 ອາການແຊກຊ ູ້ອນຂອງພະຍາດເບາົຫວານ 4 ການປະຕບິດັດູແລສຸຂະພາບ
5 ອ ື່ ນໆ………………..
Ref. code: 25606017090090UFM
92
4.21 ຂໍ ູ້ມູນທີື່ ທື່ ານໄດ ູ້ຮບັມປີະໂຫຍດຕໍື່ ທື່ ານບໍ?
1 ບໍື່
2 ເປັນສື່ ວນໃດສື່ ວນໜຶື່ ງ 3 ເປັນຫຼາຍ
ພາກທີື່ V: ການສ ື່ ສານລະຫວື່ າງຜູ ູ້ໃຫ ູ້ບໍລກິານທາງດ ູ້ານສຸຂະພາບກບັຄນົເຈບັ
ຄໍາຖາມຕໍື່ ໄປນີ ູ້ກື່ ຽວກບັປະສບົການຂອງທື່ ານໃນການຖາມກບັຜູ ູ້ໃຫ ູ້ບໍລກິານທາງດ ູ້ານສຸຂະພາບ
ທີື່ ໂຮງໝໍໃນຊື່ ວງໄລຍະ 6 ເດ ອນຜື່ ານມາ. ກາລຸນາໃສື່ ເຄ ື່ ອງໝາຍ (√)ໃນປື່ ອງທີື່ ຖ ກຕາມສະຖານະການຕວົຈງິ
ຂອງທື່ ານ
ລໍາດບັ ໃຫ ູ້ບໍລກິານທາງດ ູ້ານສຸຂະພາບ ບໍື່ ເຄຍີ ບາງຄັ ູ້ງຄາວ ທຸກຄັ ູ້ງ
5.1 ທື່ ານໝໍໄດ ູ້ແຈ ູ້ງອາການສະພາບການເປັນ
ເບາົຫວານຂອງທື່ ານ.
1
2 3
5.2 ທື່ ານໝໍໄດ ູ້ອະທບິາຍວທິກີານກນີຢາປົວພະຍາດ
ເບາົຫວານໃຫ ູ້ທື່ ານ
1
2 3
5.3 ທື່ ານເຂົ ູ້າໃຈເວລາທີື່ ທື່ ານໝໍອະທບິາຍວທິກີານ
ກນີຢາ
1
2
3
5.4 ທື່ ານໝໍມເີວລາໃນການອະທບິາຍຄໍາຕອບຂອງ
ທື່ ານໃຫ ູ້ທື່ ານເຂົ ູ້າໃຈບໍ
1
2 3
5.5 ທື່ ານໝໍໄດ ູ້ຕອບຄໍາຖາມຂອງທື່ ານ ແລະ ໄດ ູ້ແກ ູ້
ໄຂຄວາມກງັວນົຂອງທື່ ານບໍ
1
2
3
5.6 ທື່ ານໝໍໄດ ູ້ອະທບິາຍລະອຽດບໍວື່ າເປັນຫຍງັຈຶື່ ງມາ
ກວດຕດິຕາມລະອຽດ
1
2 3
5.7 ທື່ ານໝໍໄດ ູ້ອະທບິາຍສິື່ ງທີື່ ທື່ ານຕ ູ້ອງປະຕບິດັໃນ
ການດູແລຕນົເອງກື່ ຽວກບັພະຍາດເບາົຫວານ
1
2
3
5.8 ທື່ ານໝໍມເີວລາຈາໍກດັໃຫ ູ້ທື່ ານບໍ 1
2 3
Ref. code: 25606017090090UFM
93
ລໍາດບັ ໃຫ ູ້ບໍລກິານທາງດ ູ້ານສຸຂະພາບ ບໍື່ ເຄຍີ ບາງຄັ ູ້ງຄາວ ທຸກຄັ ູ້ງ
5.9 ທື່ ານໝໍການຢາຜູ ູ້ທີື່ ໃຫ ູ້ຢາໃຫ ູ້ທື່ ານໄດ ູ້ອະທບິາຍ
ວທິກີານກນີຢາລະອຽດໃຫ ູ້ທື່ ານບໍເວລາທື່ ານໄປຊ ູ້
ຢາ
1
2
3
5.10 ພະຍາບານໄດ ູ້ຕອບຄໍາຖາມຂອງທື່ ານ ແລະໄດ ູ້
ແກ ູ້ໄຂຄວາມກງັວນົຂອງທື່ ານບໍ
1
2 3
5.11 ພະຍາບານມເີວລາໃນການອະທບິາຍຄໍາຕອບຂອງ
ທື່ ານໃຫ ູ້ທື່ ານເຂົ ູ້າໃຈບໍ
1
2 3
5.12 ນກັໂພຊະນາການໄດ ູ້ໃຫ ູ້ຂໍ ູ້ມູນທາງດ ູ້ານອາຫານ
ການກນີສໍາລບັຄນົເຈບັທີື່ ເປັນພະຍາດເບາົຫວານ
ໃຫ ູ້ທື່ ານ
1
2
3
5.13 ນກັໂພຊະນາການໄດ ູ້ຕອບຄໍາຖາມຂອງທື່ ານເວລາ
ທື່ ານບໍື່ ໝັ ູ້ນໃຈໃນການກນີອາຫານສໍາລບັຄນົ
ເຈບັເປັນພະຍາດເບາົຫວານ
1
2 3
ພວກເຮາົຢາກຮູ ູ້ລະດບັຄວາມເພີື່ ງພໍໃຈຂອງການໃຫ ູ້ບໍລກິານທາງດ ູ້ານການປິື່ ນປົວຂອງຜູ ູ້ໃຫ ູ້
ບໍລກິານດ ູ້ານສຸຂະພາບ. ລະດບັຄວາມເພີື່ ງພໍໃຈ 1: ບໍື່ ພໍໃຈຫຼາຍ, 2: ບໍື່ ພໍໃຈ, 3: ພໍໃຈປານກາງ, 4: ພໍໃຈ, 5:
ພໍໃຈຫຼາຍ
ລໍາດບັ ຄວາມເພິື່ ງພໍໃຈຈາກ..... ລະດບັຄວາມເພີື່ ງພໍໃຈ
1 2 3 4 5
5.14 ລະບບົການລງົທະບຽນຄນົເຈບັ 1
2 3
4 5
5.15 ສະຖານທີື່ ໃຫ ູ້ບໍລກິານດ ູ້ານສຸຂະພາບ 1
2 3
4 5
5.16 ຊື່ ວງເວລາລໍຖູ້າກວດນາໍທື່ ານໝໍ 1
2 3
4 5
Ref. code: 25606017090090UFM

94
ລໍາດບັ ຄວາມເພິື່ ງພໍໃຈຈາກ..... ລະດບັຄວາມເພີື່ ງພໍໃຈ
1 2 3 4 5
5.17 ຊື່ ວງເວລາລໍຖູ້າຮບັຢາ 1
2 3
4 5
5.18 ການໃຫ ູ້ບໍລກິານຂອງພະຍາບານ 1
2 3
4 5
5.19 ການໃຫ ູ້ບໍລກິານຂອງທື່ ານໝໍ 1
2 3
4 5
5.20 ການໃຫ ູ້ບໍລກິານຂອງການຢາ 1
2 3
4 5
5.21 ມາດລະຍາດ, ຖະໜອມຖອມຕວົ, ລກັສະນະ
ການເວົ ູ້າ
1
2 3
4 5
5.22 ການຕອບສະໜອງຄວາມກງັວນົ ແລະ ມຄີວາມ
ສໍາພນັທີື່ ເປັນມດິ
1
2 3
4 5
5.23 ການໃຫ ູ້ຂໍ ູ້ມູນຕາມທີື່ ທື່ ານຢາກຮູ ູ້ 1
2 3
4 5
5.24 ລະດບັຄວາມຮູ ູ້ຄວາມສາມາດໃນການບໍລກິານ 1
2 3
4 5
5.25 ຄວາມເທົື່ າທຽມໃນການຮບັບໍລກິານຈາກບຸກ
ຄະລາກອນຜູ ູ້ໃຫ ູ້ບໍລກິານດ ູ້ານສຸຂະພາບ
1
2 3
4 5
5.26 ຄວາມວື່ ອງໄວ ແລະ ການເຂົ ູ້າເຖງິການບໍລກິານ
ກບັບຸກຄະລາກອນທາງດ ູ້ານສຸຂະພາບ
1
2 3
4 5
5.27 ການນດັກວດຄ ນກບັທື່ ານໝໍ 1
2 3
4 5
ຂໍຂອບໃຈ
Ref. code: 25606017090090UFM

95
APPENDIX B
Certificate of Appraisal by National Ethic Committee
Ref. code: 25606017090090UFM
96
APPENDIX C
Information Sheet
1. Title of research project:
Health care provider-patient communication and self-care behaviors among
Type 2 Diabetes at Mahosot Hospital, Vientiane Capital, Lao PDR
2. This project is conducted by: Mr. Kengher VAXENG under the supervision of
major advisor: Lect. Dr. Pornthip Chompook, Ph.D and co-advisor: Associate professor
Chaweewon Boonshuyar, M.S.P.H. Faculty of Public Health, Thammasat University.
3. Invitation to Research
You are being invited to take part in a research project because you are
Type 2 Diabetes to attending at Mahosot Hospital in Vientiane Capital. Before you
decide to participate it is important for you to understand why the research is being
done and what it will involve. Please take time to read the following information
carefully and do not hesitate to ask if anything is unclear or if you would like more
information.
4. Rational and justification.
In 2014, the global report showed adult living with diabetes was 442
million people compared with 108 million in 1980. The global prevalence of Diabetes
in the adult population since 1980 had been increasing from 4.7% to 8.5% in 2014.
Therefore, this shows the cause effect in associated with risk factors among population
being overweight or obese especially in the low and middle-income.
Lao PDR reported that Diabetes prevalence was 5.6% in adult population,
and 2% of Lao people died from Diabetes each year. Lao government started to focus
on diabetes as an important health concern in the country in 2014. World Diabetes
Foundation-funded project was conducted to strengthen the Diabetes health care system
in Lao PDR.
Mahosot Hospital is an international hospital care located in central of Lao
PDR. The capacity is 365 beds, where provide primary-tertiary, specializing in internal
medicine. Out Patients Department (OPD) is one of 33 department where deliver
service to the patients who need to check up and there are many rooms for checking up
by specialist. There is also DM clinic on working days. A vast majority of patient visits
Ref. code: 25606017090090UFM
97
to Mahosot hospital is in the form of outpatient visits whereby the patient seeks
diagnosis or treatment but is not hospitalized over-night.
5. Objectives of the project.
1. To evaluate personal characteristics, medical status and social supports among
Type 2 Diabetes
2. To determine the relationship between personal characteristics, medical status,
social supports, health care provider-patient communication and self-care
behaviors among Type 2 Diabetes
6. Inclusion and exclusion criteria
Inclusion Criteria
Type 2 Diabetes who had been diagnosed by doctor, who attended at
OPD in Mahosot Hospital, Vientiane Capital, Lao PDR.
Patients who had been treated with anti-hyperglycemic medications for
at least 6 months.
Age 30 years or older and able to communicate in Lao language.
Exclusion criteria:
Type 2 Diabetes who was in severe condition that could not give
information
7. Procedure upon participants.
I volunteered to participate in this project. As stated in the research content
that volunteer has submitted, I am willing to take the time to answer the questionnaire,
once every 86 questions, totaling 30 minutes. Upon completion of the research,
information related to research volunteers. Will be destroyed within 1 year after the
research is completed.
8. Hazards or risks that may arise for research volunteers.
You will not have any risk to your body, mind, society and the economy or
beliefs because the mostly conduct is interview, but however, it may take up about 30
minutes to complete the questionnaire.
9. Benefit of the project.
1) Health care provider can encourage Type 2 Diabetes to have regularly physical
activities and good dietary practices in order to control their fasting blood sugar and
control the prevalence of Type 2 Diabetes complications.
Ref. code: 25606017090090UFM

98
2) Capacity building among health care providers can improve their skill to
provide diabetes mellitus information among patients who had poor self-care and
communicate focus with young group age.
10. keeping Information related directly to participant
The researcher will use the code as a reference number for your name to
retain this information. The researcher will not put your name on the questionnaire.
Access information, translate and record all the data acquired by researcher and experts
only to avoid ignoring your secrets. After that, researcher will analyze data and explain
the results of education. All collected data will be destroyed after the report has been
completed.
11. Process of providing information to participant volunteers.
As a participant in the research project. You will receive information from
the research assistant as follows.
1. You will be aware of the nature and purpose of this research.
2. You will be provided with a description of the research methodology and data collection.
3. You will be provided with a description of the risks and discomfort that you
may receive from the research.
4. You will be provided with a description of the benefits that you may receive
from the research.
5. You will have the opportunity to ask questions about the research or related procedures.
6. You can withdraw from the project at any time, so you will not be affected.
7. You will received a copy of the descriptive document for the participant, a
signed and dated consent form.
8. You have the right to decide whether or not to participate in the research.
Without intimidation or deception.
Finally, state that if researcher does not perform upon participants
as indicated in the information, the participants can report the incident to the
Ethics Review Sub-Committee for Research Involving Human Research
Subjects of University of Health Sciences, Vientiane Capital, Lao PDR,
Samsaenthai Road, Phiawat Campus, Vientiane Capital Tel: +856(0)21 22 28
83, Fax +856(0)21 21 40 55, Email [email protected]
Ref. code: 25606017090090UFM
99
APPENDIX D
Informed Consent Form
Instruction: Please modify this form accordingly
Address ………………………………
Date ………………………………….
Code number of participant …………………………………………………
I who have signed here below agree to participate in this research project
Title “Health care provider-patient communication and self-care behaviors among Type 2
Diabetes at Mahosot Hospital, Vientiane Capital, Lao PDR”
Principle researcher’s name Mr. Kengher VAXENG
Contact address: 99 Moo 18 Paholyothin Road, Klong Luang, Rangsit, Prathumthani 12121
Thailand
Telephone 8562091934368 (Lao), 0944363758 (Thai)
I have (read or been informed) about rationale and objectives of the project,
what I will be engaged with in details, risk/ham and benefit of this project. The researcher has
explained to me and I clearly understand with satisfaction.
I willingly agree to participate in this project and consent the researcher to
interview the total of 86 questionnaires were included, once a total of 30 minutes. Upon
completion of the research, information related to research volunteers will be destroyed within
1 year after the research is completed.
I have the right to withdraw from this research project at any time as I wish with
no need to give any reason. This withdrawal will not have any negative impact upon me
(eg: still receive the usual services).
Researcher has guaranteed that procedures acted upon me would be exactly the
same as indicated in the information. Any of my personal information will be kept
confidential. Results of the study will be reported as total picture. Any of personal information
which could be able to identify me will not appear in the report.
If I am not treated as indicated in the information sheet, I can report to the
Ethics Review Sub-Committee for Research Involving Human Research Subjects of
Ref. code: 25606017090090UFM
100
University of Health Sciences, Vientiane Capital, Lao PDR, Samsaenthai Road, Phiawat
Campus, Vientiane Capital Tel: +856(0)21 22 28 83, Fax +856(0)21 21 40 55, Email
I also have received a copy of information sheet and informed consent form
Sign …………………..…………… Sign …………………..……………
(………………………..………) (………………………..………)
Researcher Participant
Sign …………………..…………… Sign …………………..……………
(………………………..………) (………………………..………)
Witness Witness
Ref. code: 25606017090090UFM
101
BIOGRAPHY
Name Mr. Kengher VAXENG
Date of Birth 12 Aug 1990
Educational attainment Academic Year: 2017
Scholarship Year 2017: Asia Deverlopment Bank
Work experiences 2016 work at Sikhottabong District Hospital,
Vietiane Capital, Lao PDR
Ref. code: 25606017090090UFM