health care policy in future syria
DESCRIPTION
Fundamental deficiencies that exist in the current Syrian health care system will be thoroughly discussed along with proposed policy recommendations and a road map to help eliminate or diminish them. The paper will outline policies needed to develop and achieve a health care quality that meets the World Health Organisation standards and performance measures and form health information systems that facilitate the achievement of goals and objectives. Considering the fact that health care reform in Syria is certainly a major task, a comprehensive feasibility study will be essential. Such study will be detailed and will evaluate the demands of change, the available and needed resources and prospects of success.TRANSCRIPT
Transitional Period Policy Research
Health Care Policy in Future Syria
Written by Safwan Kassas, MD
Reviewed by Ammar Kahf, Ph.D
Edited by Ausama Monajed

Safwan Kassas, MD. Dr. Kassas completed his medical degree at
Damascus University School of Medicine and trained in internal medicine,
cardiovascular medicine and interventional cardiology in the United States.
He is the founder and director of the cardiovascular stem cell therapy
program, Michigan Cardiovascular Institute and practices interventional
cardiology at Michigan Cardiovascular Institute where he serves as
the catheterisation laboratory director. Dr. Kassas is also founder and
director of the cardiovascular stem cell therapy programme at Michigan
Cardiovascular Institute. In addition to his clinical practice, Dr. Kassas has
an interest in clinical cardiovascular research and has participated as a
principal investigator in many trials. Dr. Kassas is also SRCC’s associated
expert in health sector reform.
Strategic Research & Communication Centrewww.strescom.org
© 2012 Strategic Research and Communication Centre.
All rights reserved.

1Transitional Period Policy Research
Health Care Policy in Future Syria
Contents
Executive Summary ................................................................................................................ 2
I. Introduction ........................................................................................................................ 3
II. Understanding Health Care and Health Care Systems ........................................................ 5
A- Health care system structural pillars .......................................................................... 5
B- Assessing health care systems .................................................................................... 6
C- Assessing health care quality ..................................................................................... 7
D- Benefits of health information system ....................................................................... 7
III. Health care system in Syria today ..................................................................................... 9
A- Analytic view ............................................................................................................. 9
B- Structural deficiencies in the current Syrian health care system ............................... 10
IV. Health care quality in Syria today .................................................................................... 12
V. The need for health care policy reform ............................................................................. 13
VI. Quality assurance program in Syrian health care system ................................................ 14
A- General overview ..................................................................................................... 14
B- Syrian challenges ..................................................................................................... 14
C- Impact of quality assurance programs on health care expenditure .......................... 16
D- Performance measures that can be followed by QA programs ................................. 16
VII. Health insurance program in Syria ................................................................................. 18
The national health insurance model ............................................................................ 19
The out-of-pocket model .............................................................................................. 19
VIII. Health care facilities accreditation process ................................................................... 21
IX. Addressing disparity in health care in Syria..................................................................... 22
X. Assessing physicians shortage and surplus ...................................................................... 24
Estimating demand....................................................................................................... 24
Estimating supply ......................................................................................................... 25
Determining shortage or surplus .................................................................................. 25
XI. Necessary steps for creating medical research, development and innovation program .. 26
XII. Proposed changes to reform current health care policy ................................................. 28
XIII. Need for a feasibility study ........................................................................................... 31
XIV. Conclusion .................................................................................................................... 32
References ........................................................................................................................... 33

Strategic Research & Communication Centre
Health Care Policy in Future Syria
2
Executive Summary
This policy paper is intended for policy makers and strategic planners during the transitional period who are
involved in health care policies, as well as those involved in administering health care in Syria. Any effort aiming
to evaluate current health care policies in Syria must analyse its three different components that are closely
interdependent:
1. Health that is defined by the World Health Organisation (WHO) as a state of complete physical, mental, and
social wellbeing, and not merely the absence of disease.
2. Health care system which is defined as a structure within which people, governmental policies, and
organisations interact to assure the right of access to quality health for all citizens at an economical cost.
3. Health care information system which is the process by which information about the status of the health care
system and quality is timely and reliably collected, analysed and provided to policy makers.
Fundamental deficiencies that exist in the current Syrian health care system will be thoroughly discussed along
with proposed policy recommendations and a road map to help eliminate or diminish them. The paper will outline
policies needed to develop and achieve a health care quality that meets the WHO standards and performance
measures and form health information systems that facilitate the achievement of goals and objectives.
Even though a new health care policy will require financing which will be derived from the government health care
expenditure, the expected cost saving that can be realized after the implementation of the suggested programs
can be quite significant.
Considering the fact that health care reform in Syria is certainly a major task, a comprehensive feasibility study
will be essential. Such study will be detailed below(1) and will evaluate the demands of change, the available and
needed resources and the prospects of success.
(1) The United Nations Industrial Development Organization (UNIDO) http://www.unidoitpo.org.cn/EnAboutus.asp?id=3

3Transitional Period Policy Research
Health Care Policy in Future Syria
I. Introduction
Public health and health care policy in any country are of critical importance that far exceeds the individual sense
of wellbeing. This can be readily appreciated upon examining the health sector’s contributions to the overall
economy in developed countries.
In the European Union, for example(2), the health sector is one of the largest service industries and one of the
most important sectors, where its output accounts for 7% of GDP which is larger than the 5% accounted for by
the financial services, and it employs approximately 9% of all workers in these same countries(3).
The size of the health sector is just one reason to its importance. A robust and significant direct relation was
noted in a number of studies between the state of health in a country and what is called in economy the "human
capital". The basis for this relation is that good health increases the probability of participating in the labour force
while poor health on the contrary can predict early retirement and exit from the labour force.
A direct relation also exists between the state of health in a society and the educational level of workers. A higher
level of health correlates with more educated workers who are naturally more productive and able to obtain
higher earnings. Some of these higher earnings are either invested in improving individual skills and education
(intellectual capital) or invested directly back in the overall economy.
In an additional dimension of importance, good health in childhood was found to enhance cognitive functions
and reduce school absence, hence children with better health are able to attain higher education levels and be
more productive in the future.
A robust correlation is also believed to exist between the performance of the health sector and the competitiveness
of the overall economy via its effect on labour cost, labour market flexibility and the allocation of resources at the
macroeconomic level.
Many countries around the world today are experiencing health care challenges which are mostly related to
unsustainable health care expenditures. A prominent European health care expert (Albert de Rosa) has warned of
these challenges when he said "The world’s health systems will, within the next 15 years, find themselves in an
unsustainable situation if they do not carry out a number of important changes in their health policies."
(2) The contribution of health care to the economy, Marc Suhrcke, Martin McKee, August 23, 2005.
(3) Costs and Benefits of Health Information Technology Prepared for: Agency for Healthcare Research and Quality U.S. Department of
Health and Human Services, 540 Gaither Road, Rockville, MD 20850.

Strategic Research & Communication Centre
Health Care Policy in Future Syria
4
Syria is no different than most other countries in that regard, except that in Syria there are additional critical
flaws and challenges in the infrastructure of the Syrian health care system which compound the problem and
affect quality.
This paper will examine in details the existing deficiencies and provide recommendations to establish reform
in the Syrian health care system while keeping in mind that health care expenditures have to remain
under control.
5Transitional Period Policy Research
Health Care Policy in Future Syria
II. Understanding Health Care and Health Care Systems
Prior to discussing the existing health care policy in Syria and providing recommendations on how to restructure
the health care system one must know the traditional health care system structural pillars, learn how to
assess health care systems and how to assess health care quality and finally appreciate the benefits of health
information systems.
A- Health care system structural pillars:
Health care systems can vastly vary from nation to nation, National Health Insurance model
with a universal coverage, compulsory insurance coverage with a third party payer, out of
pocket system or a model that is a mixture of all the above are just few common examples
among the many different systems that exist in the world today.
Irrespective of their design, modern health care systems share common structural pillars which
are considered today critical to their success.
According to the Disease Control Priorities Project, DCPP, there are very important pillars to
health care systems (the DCPP is an on-going effort to assess disease control priorities and
produce evidence-based analysis and resource materials to inform health policymakers in
developing countries)(4). These pillars are:
1. Information surveillance and research: Reliable, precise and timely data acquisition in the health sector
is essential in the policy making process (health care system and health care quality data). Focus of data
compilation in Syria however has often been for the mere purpose of acquisition, and not for a policy design
objective. According to the Health Matrix Network (HMN) one cannot assume responsibilities nor achieve
results without information.
2. Health information management: This will provide reliable and timely analysis of collected data to industry,
policy makers and health care administrators for review and implementation of new and responsive policy
(4) Dean T. Jamison, Joel G. Breman, Anthony R. Measham, George Alleyne, Mariam Claeson, David B. Evans, Prabhat Jha, Anne Mills,
Philip Musgrove, "Pillars of the Health System." 2006. Priorities in Health, ed. 155-178. New York: Oxford University Press. DOI:
10.1596/978-0-8213-6260-0/Chpt-7.
Irrespective of their design, modern health care systems share common structural pillars which are considered today critical to their success.
Strategic Research & Communication Centre
Health Care Policy in Future Syria
6
changes and regulations. The management team will also maintain health records by traditional (paper-
based) or electronic means in hospitals, at physician's offices and other health care facilities.
3. Management and administration: In general the managerial and administrative component of a
modern health care system is comprehensive and inclusive permitting the participation and collaboration
among government policy makers, health care scientists and academicians, health care information system
specialists, representatives of the health care industry, and financial analysits and statisticians. Collaboratively
this administrative team can provide the policies needed for the advancement of the health care sector in
the country.
4. Human resources: In addition to furnishing qualified and competitive workforce, the human resources
division will manage this workforce designing performance goals and providing incentives for competencies.
In addition, human resources departments should be able to apply creative and new approaches to enhance
competitiveness and increase inter-organisational mobility and furnish adequate training for employees in
career development and new technology adaptation.
5. Financing: This reflects the total health expenditure as a percentage of GDP. Balancing expenditures with
revenues is critical to sustain any health care system over time. Selecting a successful working health care
coverage system, implementing new quality and system information programs which might have some
inherent initial cost but a future significant cost savings and relieving the government of the burden of an
entirely free public health care are all steps which can assist in the stability of the financial structure of the
health sector.
B- Assessing health care systems:
Despite the complexity and variations among the different health care systems the WHO has adapted an
assessment methodology to assess these systems. This methodology is based on several indicators(5).
Among these indicators is the "overall level of population health" which answers the question of how well
the population good health is being achieved. WHO has chosen to use the measure of disability – adjusted life
expectancy (DALE) which is directly comparable to life expectancy and is readily compared across populations.
Health inequalities (or disparities) within the population is another indicator which addresses regional disparities
in the access to and quality of health care, such as in urban and rural areas.
To examine the availability of resources and the responsiveness of these resources to people’s needs requires an
additional indicator called the "overall level of health system responsiveness", which also involves the respect
(5) World health organization, programs and projects. World Health Organization Assesses the World's Health Systems.
7Transitional Period Policy Research
Health Care Policy in Future Syria
for persons (including dignity, confidentiality and autonomy of individuals and families to decide about their own
health).
Another health care system assessment indicator is the "distribution of responsiveness" within the population
which answers the question of how well the people of varying economic status find that they are served by the
health system.
It is insufficient to protect or improve the average health of the population, if – at the same time – inequality
remains high. Gain occasionally is acquired disproportionately by those already enjoying the better health.
The health system has the responsibility to try to reduce inequalities by prioritizing actions that improve the health
of the worse-off, wherever these inequalities are caused by conditions amenable to intervention.
The objective of a good health care system is really twofold:
A- The best attainable average level of health – goodness.
B- The smallest feasible differences among individuals and groups – fairness.
A gain in either one of these two goals, without a gain in the other is an insufficient improvement.
The last indicator used in assessing health care systems is the "distribution of the system's financial burden within
the population" (who pays the cost). The WHO measurement of the financial burden is based on the fraction
of the spending household's capacity (income minus food expenditure) that goes on health care. An annual
expenditure of less than 60 dollars per person on health correlates with the population’s inability to access health
services from an adequately performing health system.
C- Assessing health care quality:
WHO has formulated a comprehensive database of quality indicators that assesses mortality, morbidity, risk
factors, demographic and socioeconomic statistics, women health, and infant health among many other indicators.
Individual countries can measure the quality of their administered heath care by examining their own indicators
comparing them to other nations or to suggested bench marks.
D- Benefits of health information system:
The benefits of health information system can be divided into three categories:(6)
1. Strategic planning benefits at the governmental level: An information system will provide government
and strategic planners with timely and meaningful information of the current state of health care in the
(6) Costs and Benefits of Health Information Technology Prepared for: Agency for Healthcare Research and Quality U.S. Department of
Health and Human Services, 540 ither Road, Rockville, MD 20850.

Strategic Research & Communication Centre
Health Care Policy in Future Syria
8
country. It will convert collected raw data into useful analysed information that can be used in the decision
making process of planning and cost containment.
2. Health care quality and safety benefits: Several mechanisms can attribute to such benefits such as the
ability to monitor compliance with the prevention and disease-management guidelines, and the ability to
measure performance and target outcomes which satisfy approved bench marks of performance.
Safety benefits can also be acquired via other mechanisms such as error reduction by providing Computerized
Physician Order Entry for medications that are accompanied by built in alerts and reminders, and by providing
Decision Support Systems thus improving health care quality.
Health information system can also assist in disease prevention by scanning patient records for risk factors and
subsequently recommending appropriate preventive services, such as vaccinations and certain monitoring
measures.
The challenge of managing chronic-diseases can be greatly facilitated by implementing health information
system and identifying patients in need for tests or other services, and ensuring consistent recording of
results, thus reducing hospitalization rate, improving health and reducing cost.
Finally practicing physicians will quickly realize the benefits and practicality of health information system
when able to coordinate and share patient’s data with other providers and practice medicine within the
standardization of patient care.
3. Cost saving benefit: Any new health program will have two objectives, quality improvement and cost
saving benefits as well.
Cost saving benefits of health information system can be tremendous despite the initial cost and can be
derived from several avenues.
"Efficiency" (performing the same work with fewer resources) is well known to correlate with cost savings;
implementing a health information system will lead to less needed nurses, less administrative time, and more
efficient drug utilization.
Improved safety in health care and reducing hospital errors and the associated prolonged hospitalization and
increased cost can lead to significant cost savings. Additionally the enhancement of disease prevention and
disease screening will lead to tremendous net savings as well.

9Transitional Period Policy Research
Health Care Policy in Future Syria
III. Health care system in Syria today
A- Analytic view:
Evaluating the Syrian health care system can be very challenging due to several reasons(7). Among them is the
complete lack of efficient monitoring procedures of both health care outcomes and other regulatory matters. When
such procedures are lacking, the compliance, integrity and the accuracy of data reporting cannot be adequately
trusted. Furthermore, data collection does take place in Syria and rather massive amount of data is collected
by the Central Bureau of Statistics (CBS). However, collected information is not provided for analysis and policy
making but rather maintained for the mere purpose of data acquisition without a clear utilization objective. This
makes any reliable statistical and data-based policies very rare to come by.
Another challenge is the lack of Information and data that pertain to a large section of the population due to the
presence of what is called the informal sector. According to the Syrian government this sector involves no less
than 43% of workers (those who are playing a role in the economic activities outside the institutions).
When there is difficulty in obtaining reliable information and entrusting the collected data there will be significant
difficulties in launching new programs or enacting accurate policies. This was clearly illustrated when the Health
Matrix Network (HMN) program (WHO global partnership program dedicated to strengthening national health
information systems through a network of global, regional and country partners) launched a program in 2005
in conjunction with the Syrian Ministry of Health, the program focused on the creation of a national strategy for
health information system in the country(8). Assessing their results later and during the course of the program few
conclusions were drawn:
1. A bias in the reported information was observed due to decision-makers having either no idea about all details
of the real situation of the health information system, or because there were concerns with information
reliability.
2. HIS (health information system) in Syria scored badly on data management (almost "non-functional").
3. Resources, dissemination, and use of information scores were stated to be clearly "inadequate."
(7) UNFPA Recommendation by the Executive Director Assistance to the Government of the Syrian Arab Republic (DP/FPA/SYR/6) 15
August 2001.
(8) Health matrix network, 8th Board Meeting, 23–24 July, Seattle, Washington, USA, 8/6/2007.
Strategic Research & Communication Centre
Health Care Policy in Future Syria
10
What we now know is that despite prior programs and initiatives by the Ministry of Health such as, the multiple
5-year plans (FYP), partnership with WHO for over 50 years, assistance by international experts such as the
European Commission and the activities under the MEDA program (European Mediterranean partnership program),
and despite establishing a national health committee by the Ministry of Health to develop a national strategy for
health information, as well as several modernization and reform programs the health care system in Syria today
continues to suffer from major structural and organisational deficiencies which will be summarized next.
B- Structural deficiencies in the current Syrian health care system:
4. Lack of adequate funding is a major deficiency in the current Syrian health care system. Monitoring the
2010 Legatum prosperity index from the Legatum Institute (this index is the world's only global assessment
of wealth and wellbeing)(9), the annual health expenditure per capita is just $110 (PPP) (purchasing power
parity per capita). The overall ranking of Syria among 110 world countries was 83 and in the health category
was 86(10).
Syria has been grappling with an increasing budget deficit over the last few years and associated decrease in
health care expenditure while there is a marked increase in demand due to demographic change.
When we compare health care expenditure in Syria regionally to neighbouring countries such as Jordan and
Lebanon, Syria does have significantly lower health expenditures. Internationally and according to a WHO 2006
ranking of 194 registered countries, Syria came at number 128 in health care expenditure at 3.9 % of GDP and in
2009 this further dropped to 2.9%(11). If we look at the period between 2000 and 2005, Syria ranked # 153 among
193 countries registered in the WHO with expenditure in 2005 of 4.1% indicating 20% decline in expenditure
from 2003 (5.1%), trailing behind Yemen, Afghanistan, and Jamaica. In 2006 and 2009 the percentage further
dropped to 3.9% and 2.9% respectively.
The widespread fraud and abuse in the health care sector in Syria are additional unfortunate realities. While there
are no reliable statistics to address the magnitude of this widespread problem in the country’s health care sector,
we can appreciate the profound magnitude of this problem by monitoring the index comparisons ranking system
by the Legatum Prosperity Index where Syria ranked 127 among 178 listed countries in Corruption Perceptions
Index and only 9.6% of Syrian people find others to be trust worthy.
(9) The Legatum Institute, the 2011 Legatum prosperity index.
(10) OECD Health Division (June 2011) "OECD Health Data ". Paris, and WHO Department of Health Statistics and Informatics (May 13,
2011). World health statistics 2011. Geneva.
(11) "Total expenditure on health as % of GDP by country", World Health Organization. Retrieved from: http://www.NationMaster.com/
graph/hea_tot_exp_on_hea_as_of_gdp-health-total-expenditure-gdp
11Transitional Period Policy Research
Health Care Policy in Future Syria
The lack of an insurance coverage program has led to a tremendous financial burden on both the population and
the government. Less than 5% of Syrians subscribe to insurance programs resulting in a large number of people
preferring free health services in government-run hospitals which significantly increase the demand on an already
strained funding.
The critically needed health information system as detailed above continues to be lacking. In 2003 the Syrian
Ministry of Health entertained the idea of establishing a health information system; however, to date Syria still
lacks a reliable and effective system. The difficulties encountered according to the Ministry of Health were financial,
electronic legislations, human obstacles and spatial obstacles. In addition to other structural and organisational
deficiencies that exist today in the Syrian health sector, there is an inadequate level of qualified managerial and
administrative skills needed for data processing and planning purposes.
The lack of a health information system and qualified managerial and administrative skills has created a
compromised policy making process which naturally has become very unreliable. Policy makers who might lack
adequate qualifications in the field in the first place do not additionally have reliable, analysed and processed
data to base their policies upon.
The inadequate planning factor in the national demographic change such as the rising youth unemployment,
increasing aging population, and the associated impact on health care demands has been a challenge that has
compounded the decreasing health care funding.
Many other structural deficiencies do exit as well such as the disparity in health care (inadequate geographical
distribution of human resources and health care facilities), lack of an effective quality assurance program, lack of
a modern credentialing process for both health care facilities and individual physicians, insufficient coordination
between the different departments within the Ministry of Health and a low level of qualified nurses and
paramedical staff; are all important deficiencies which need to be addressed.
The absence of a scientific medical research and development program is often overlooked. The establishment
of such program can be a valuable component not only to the quality of health care and medical education but
rather to the overall economic development and competitiveness.

Strategic Research & Communication Centre
Health Care Policy in Future Syria
12
IV. Health care quality in Syria today
The Syrian Ministry of Health is required to annually publish the various health care indicators which can be
reviewed on its official web site. Health care indicators (mortalities and morbidities indicators) as set by the WHO
are usually used to evaluate and rank patient care quality in a particular system or country.(12)
Evaluating health care quality in Syria, however, is very cumbersome and difficult to undertake. The evaluation
process simply requires adequate credibility of the process of indicators data collection. Many reviewers have
significant difficulty accepting the reported data by the Ministry of Health as a solid and reliable data, due to the
lack of accurate and reliable data acquisition processes.
Today in Syria there is no reliable data collection process that involves both public and private health sectors. In
the private sector, there is no obligation or incentive for either physicians or health care facilities to report data
on outcomes for monitoring and analysis purposes. In the public sector there is significant scepticism about
the integrity of the government system reporting process. To further compound the problem of the already
compromised collected data, a reliable data analysis system is effectively lacking as well.
The evaluation of health care quality in Syria is also challenged by the lack of a quality assurance
program that monitors outcome, complications and malpractice.
Finally, the Syrian health care sector is no different from other government agencies where
the lack of adequate accountability is a significant obstacle on the way of quality assessment.
Today, the majority of people in the capital city Damascus, for example, (where health care
services are believed to be better than other cities) will rank the provided patient care as
unsatisfactory. Many of the financially capable Syrians including government officials will elect
when possible to seek their own individual health care needs outside the country.
(12) World health organization, programs and reports. Global Health Observatory GHO, World Health Statistics, and Syria, World Bank data.
The Syrian health care sector is no different from other government agencies where the lack of adequate accountability is a significant obstacle on the way of quality assessment.

13Transitional Period Policy Research
Health Care Policy in Future Syria
V. The need for health care policy reform
History makes it clear that failing to act on health reform has serious and far reaching economic and social
ramifications. The longer the wait to address the underlying problems the more drastic measures need to be taken.
Overall, the objectives of change are very clear:
A. Establish a health care system that fulfills the WHO system assessment indicators criteria as mentioned
above.
B. Deliver a high quality administered health care which fulfils the WHO health quality indicators and
performance measures.
Both objectives are to be achieved in a cost effective manner to both government and population.
Strategic Research & Communication Centre
Health Care Policy in Future Syria
14
VI. Quality assurance program in Syrian health care system
A- General overview:
A quality assurance (QA) program is a critical component of any modern health care system. Its significance
extends beyond achieving an acceptable quality health care. The WHO, for example, suggests that quality
assurance programs should make improvements in six aspects of quality:
1. Effectiveness where health care adheres to evidence base principles leading to improved health outcomes.
2. Efficiency which maximises resource use and avoids waste.
3. Accessibility where the administered health care is not only timely but also geographically reasonable.
4. Acceptable and patient-centred care that takes into account the preferences and aspirations of individuals
and communities.
5. Equitability with no variation in health care delivery among the societal components.
6. Safety that minimises risks and harm to service users.
Establishing a viable QA program in the Syrian health sector, especially in the public sector, has been one of the
objectives targeted by the Syrian Ministry of Health.
B- Syrian challenges:
The modernisation program of health care was initiated in Syria and it included several QA initiatives some of
which were initiated in partnership with international health organisations such as the WHO and the Health Care
International Organisation which assists public, private, and community organisations to achieve their strategic
objectives and improve their performance and outcome. These programs stressed on the importance of health
care quality assurance programs and addressed some of the structural and organisational needs necessary to
create QA programs.
Today however and despite these efforts, Syrian hospitals and Syrian physicians are still not governed by any
practical or enforceable QA measures that mandate participation and reporting.
15Transitional Period Policy Research
Health Care Policy in Future Syria
The reason to why the Syrian Ministry of Health did not achieve the objective of creating a reliable health care QA
program might be multifactorial. The roles and responsibilities within the various parts of the QA system in Syria
might not be well defined [policy and strategic development specialists, health service providers (physicians and
health care facilities) and communities and service users (patients)].
Additionally there is a lack of a review process which monitors the roles and responsibilities of all the responsible
persons, committees, and institutions. This review process should monitor the processes of policy/strategy
development for quality, quality standard development, quality Control, etc.
Furthermore, the connection between these various parts might be insufficient, for example, decision-makers
cannot hope to develop and implement new strategies for quality without properly engaging health-service
providers, communities, and service users. By the same standards, health-service providers need to operate within
an appropriate policy environment for quality, and with a proper understanding of the needs and expectations
of those they serve in order for them to deliver the best results. Communities and service users in turn need to
influence both quality policy and the way in which health services are provided to them, if they are to improve
their own health outcomes.
Another obstacle in the Syrian health care QA program is that both hospitals and physicians today are still not
mandated to report to any government or private health insurance agencies.
It is not also known if Syria today has a National Quality Management Strategy defining realistic goals for quality
assurance program, taking into account the available man power (managers, clinicians and other front liners),
financial resources and time (such a plan if it does exist is not published). Additionally, training of the required
man power, local staff and experts in the field of QA has not adequately taken place. It is also unknown if the
Syrian Ministry of Health has formulated a legal and operational framework and a work manual that can serve in
pilot quality assurance projects at certain medical institutions. A design and development of standards, protocols,
guidelines and bench marks that govern the QA program is still lacking as well.
One additional critical deficiency as well is the lack of well-defined mandatory self-assessment and external
pear review processes, where both hospitals and individual physicians can accurately assess their own level of
performance against established standards and bench marks.
A national team of experts in quality assurance which is also necessary in the process of creating a QA program
is not available in Syria today; such a team can be formed after adequate training and can serve as an expert
resource panel. But more importantly, there is no health information system that will collect the data, analyse
it and provide it to policy makers for accurate quality assurance policies. Finally, more developed and matured
processes of utilization reviews, audits, peer reviews, mortality and morbidity reviews, reviews on the quality of
nursing care and reviews on staff and patients satisfaction by simple standardized tools are needed and can be
necessary in the development process of a successful quality assurance program.
Strategic Research & Communication Centre
Health Care Policy in Future Syria
16
In conclusion, like any institutional or governmental system the health care system in any country including Syria
cannot achieve its goals of delivering effective, efficient, accessible, safe, patient oriented and equitable health
care without a well-designed quality assurance program, such program should remain as a top priority of any
health care reform in Syrian.
C- Impact of quality assurance programs on health care expenditure:
The additional cost of hospital acquired conditions and complications can be very substantial. A QA program can
significantly offset the majority of it by means of two main mechanisms:
1- Identification of hospital acquired conditions and complications that are high in cost or volume in adjunction
with a reporting process to the Ministry of Health or the insurance providing organisations which in turn can either
adjust payments to a lower level or deny payments for any avoidable or preventable conditions or complications.(13)
Examples of avoidable hospital acquired conditions are:
1. Foreign object retained after surgery.
2. Air embolism.
3. Blood incompatibility.
4. Stage III and IV pressure ulcers.
5. Falls and trauma (including fracture, dislocation, intracranial injury, crushing injury, burn, and other
injuries).
6. Vascular catheter-associated infection.
7. Catheter-associated urinary tract infection.
8. Manifestations of poor glycemic control (including diabetic ketoacidosis, non-ketotic hyperosmolar
coma, hypoglycemic coma, secondary diabetes with ketoacidosis, and secondary diabetes with
hyperosmolarity.
2- QA programs will assess performance measures and quality indicators and report them to the Ministry of
Health or insurance providers that can in turn adjust payment coverage to a lower level for facilities or providers
who do not meet the standard quality performance measures.
D- Performance measures that can be followed by QA programs:
In all developed countries and many developing nations there are universally approved sets of performance
measures and quality indicators that are constantly being monitored by the various QA programs.
(13) CMS Hospital-Acquired Condition Measures for the Hospital Inpatient Quality Reporting Program [https://www.qualitynet.org].

17Transitional Period Policy Research
Health Care Policy in Future Syria
For illustration purposes, in the case of Myocardial infarction the use of ASA, ACEI, B Blockers, and timing to receive
PCI or lytic therapy and the use of statin drugs on discharge are all quality indicators that can be monitored. In the
case of a stroke the use of thrombolytic therapy and anticoagulation therapy for ischemic stroke, the use of statin
drugs, patient education and referral to rehabilitation programs are also quality indicators that can be monitored
to assure quality.
A complete list of performance and quality indicators that are currently being used for example by CMS (Centre
for Medicare and Medicaid Services) in the United States can be reviewed by visiting CMS web site.(14)
(14) CMS Medicare, Hospital IQR quality measures for payment determination.

Strategic Research & Communication Centre
Health Care Policy in Future Syria
18
VII. Health insurance program in Syria
Before addressing the needs and benefits of a health insurance system in Syria we need to briefly learn first the
patterns and objectives of the various health insurance systems and plans in general.
A main intent of a health insurance system is to provide universal access to good quality health care. To sustain
this objective, insurance providers will need to carefully balance cost control for the insurer and good quality care
for the insured. This balance relies on several important concepts such as: coordination of care, prioritization of
prevention and wellness, effective care for better outcome, efficient use of resources, responsiveness to patients’
concerns, and finally the recognition that the creation of a value in the system and achieving the objectives of the
health insurance system does not necessarily correlate with more spending.
Furthermore, coordination of care is an important component of any health insurance system. There is ample
evidence to suggest that only through the coordination of care will the insurance system be able to reduce waste,
decrease cost and reduce the overall health expenditure. For example, a small percentage of chronically ill persons
consume a very disproportionate share of resources, a cost which can be significantly minimized by improved
coordination of care.
Care coordination is more practical if based on improved electronic medical record infrastructure and more
beneficial if valued as a fundamental part of administering health care. The prioritization of prevention and
wellness measures can result in a great return and cost control. In developed countries such as the United States
it is recognized that for every dollar spent on prevention, a 2.5% return on investment is achieved. In general,
there is no greater investment that a society can make than that in prevention and wellness for its citizens.
Providing universal coverage is a noble cause and probably the most important pillar; how the country can achieve
this goal is tightly linked to how the country will finance its health system and its insurance coverage program.
There are about 200 countries registered with the United Nations today, and each country devises its own set of
arrangements for providing coverage to its citizens. Most of these systems, however, have their own variations of
four common specific patterns.
In the British national health system (the Beveridge model, named after its designer) health care is provided and
financed by the government through tax payments, just like any government agency. Many, but not all, hospitals
and clinics are owned by the government; some doctors are government employees, but there are also private
doctors who collect their fees from the government. In Britain, you never get a doctor bill. These systems tend to
19Transitional Period Policy Research
Health Care Policy in Future Syria
have low costs per capita, because the government, as the sole payer, controls what doctors can do and what
they can charge.
The Bismarck model (Bismarck invented the welfare state as part of the unification of Germany in the 19th
century) uses an insurance system that utilizes a fund which is financed jointly by employers and employees
through payroll deduction. This model has some similarities to the United States model except that in the Bismarck
- type health insurance plans everybody is covered and these plans don't make a profit. In this system the country
ends up in a multi-payer model with multiple funds. Even though doctors and hospitals tend to be private, tight
regulation gives government much of the cost-control clout that the single-payer Beveridge Model provides. The
Bismarck model is found in Germany, France, Belgium, the Netherlands, Japan, Switzerland, and, to a degree, in
Latin America.
The national health insurance model
This system has elements of both Beveridge and Bismarck and uses private-sector providers just like the Bismarck
model, but payment comes from a single payer (the government) through a government-run insurance program
that every citizen pays into (the Beveridge model). Since there's no need for marketing, no financial motive to deny
claims and no profit, these universal insurance programs tend to be cheaper and much simpler administratively
than American-style for-profit insurance.
The single payer tends to have considerable market power to negotiate for lower prices. Canada's system, for
example, has negotiated very low prices from pharmaceutical companies. National health insurance plans also
control costs by limiting medical services they will pay for, or by making patients wait to be treated. The classic
NHI system is found in Canada.
The out-of-pocket model
Only developed and industrialized countries (perhaps 40 of the world's 200 countries) have established health
care systems and health insurance plans to provide coverage to their citizens. Most of the nations on the planet
are too poor and too disorganized to provide any kind of mass medical care. The basic rule in such countries is
that the rich get medical care; the poor stay sick or die.
In rural regions of Africa, India, China and South America, hundreds of millions of people go their whole lives
without ever seeing a doctor. If they have nothing, they don't get medical care.
One might add a fifth model of insurance coverage which is a combination and mixture of all the above resulting
in a health care system similar to what is in the United States today or in a reality multiple systems in one country.
In the Unites States, when it comes to treating veterans, the Beveridge model comes into play (employed doctors
and a single government payer). For Americans over the age of 65 on Medicare, the system becomes similar to the

Strategic Research & Communication Centre
Health Care Policy in Future Syria
20
Canadian National Health care insurance system. For working Americans who get insurance on the job the system
is similar to a German Bismarck model.
For the 15 per cent of the population who have no health insurance, the United States is similar to Cambodia or
rural India with the only access to health care is via out of pocket mechanism.
Syria is yet to appreciate the benefits of health insurance where a good segment of the population struggles with
out of pocket coverage for its health needs. A large number of people prefer free health services at government-
run hospitals and less than 5 per cent of the total patients in the country pay through insurance. Today in Syria the
general government expenditure and contribution on health as a percentage of the total expenditure on health
is annually decreasing. According to the WHO Global Health Observatory Data Repository, the Syrian government
expenditure in 2009 was 31% while in 2005 it was 50.5%, this is while simultaneously the Private expenditure on
health as a percentage of total expenditure on health rose to 69% in 2009 and the out-of-pocket expenditure as
a percentage of the private expenditure component was100% for the same year, indicating that private prepaid
plans (third party private insurance programs) as a percentage of the private expenditure on health was 0%. From
this data we can realize how people with inability to pay will have tremendous reduction in their ability to access
health care.
Reforms are needed to meet this heavy health burden on public hospitals. In 2010, the government introduced a
number of initiatives to improve the quality and access to public health services. These initiatives divide coverage
into three categories. The first offers free treatment to poor people. The second is based on a commission system
where patients pay less than the actual cost, and finally a third category where financially capable people pay
the full cost of the treatment. In a different initiative the government also launched a National Health Insurance
scheme to cover all government servants and public sector employees. Government employees contribute SYP
250 (USD 5) annually towards the insurance while the government pays rest of the amount.
In examining these reform initiatives we can see that they don’t follow a particular recognized pattern of
insurance system but rather divide the society into classes and provide a different kind of coverage to each class.
How will the government be certain in its accuracy classifying the large non-government sector (more than 40%
of workers) among these different classes is a big challenge. The social and financial divisions in any society are
very dynamic and a constantly changing phenomenon, that no government is able to track and monitor. One
advantage of this system, however, will be to offload the tremendous financial burden on the public health sector
and another advantage will be giving an opportunity to public hospitals to make a profit that theoretically can be
re-invested in a better quality health care. Will public hospitals be able to make a profit however remains so far
a theoretical possibility.
In a further examination of the reform initiatives we can recognize that different initiatives apply to different
sectors; government employees, for example, will be covered under a national health insurance system while the
non-government population will not. It is also not clear if the National Health Insurance system that provides
21Transitional Period Policy Research
Health Care Policy in Future Syria
coverage to government employees will allow these employees and families to seek health care in the non-
government private health care facilities or not (patient responsiveness of the system). However, it will be
inaccurate to pass judgment on these initiatives since they were passed in 2010 and have not been implemented
yet since Syria today is in a growing political crisis.
VIII. Health care facilities accreditation process
Two types of accreditation standards can be designed:
1. Hospital accreditation standards that are patient’s care centred focus on functions related to providing
patient care; certainly the JCI (Joint Commission International) in partnership with the WHO can be of great
assistance in the accreditation process.
2. Hospital accreditation standards that focus on non-patient’s care related hospital departments such as
accounting and human resources, the ISO (International Organization for Standardization) can be very
helpful.
Strategic Research & Communication Centre
Health Care Policy in Future Syria
22
IX. Addressing disparity in health care in Syria
In order to quantify the need for physicians and health care facilities among the different
geographical regions in Syria and among the different populations within the Syrian society
without disparity, we first need to learn about the concept of health care disparities in general.(15)
Disparity in health care reflects the differences that exist in a health care system within a
society in not only access to health care (issues related to whether persons can get health care
or even experience barriers accessing care), but also in the quality of the administered health
care. Disparity can have many dimensions; urban vs. rural communities, low vs. high income
population groups, ethnic minority groups, women vs. men, the elderly population, children,
and the disabled population.
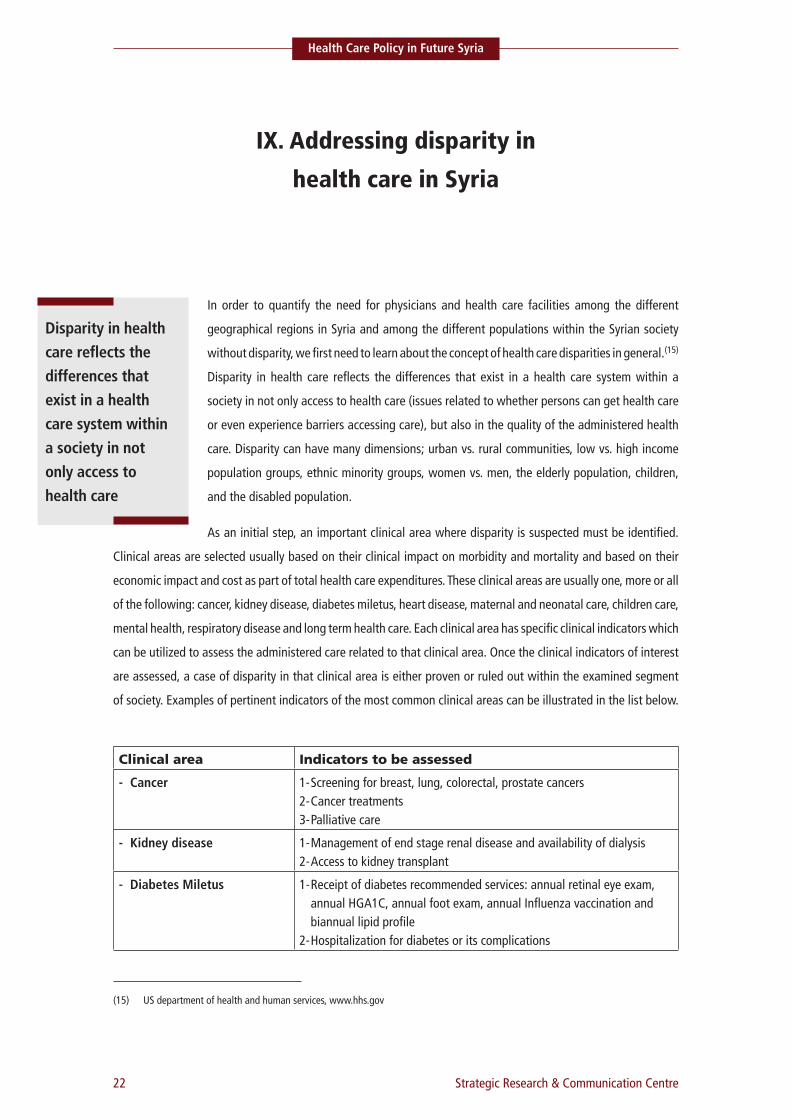
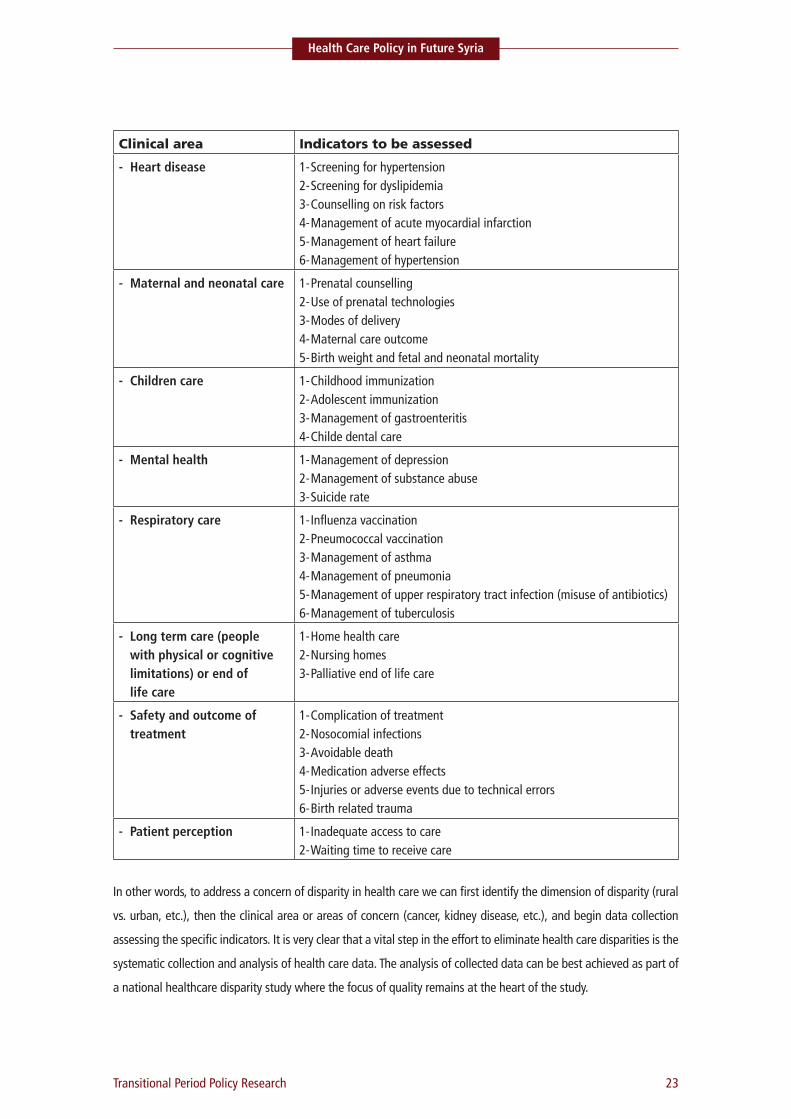
As an initial step, an important clinical area where disparity is suspected must be identified.
Clinical areas are selected usually based on their clinical impact on morbidity and mortality and based on their
economic impact and cost as part of total health care expenditures. These clinical areas are usually one, more or all
of the following: cancer, kidney disease, diabetes miletus, heart disease, maternal and neonatal care, children care,
mental health, respiratory disease and long term health care. Each clinical area has specific clinical indicators which
can be utilized to assess the administered care related to that clinical area. Once the clinical indicators of interest
are assessed, a case of disparity in that clinical area is either proven or ruled out within the examined segment
of society. Examples of pertinent indicators of the most common clinical areas can be illustrated in the list below.
Clinical area Indicators to be assessed- Cancer 1- Screening for breast, lung, colorectal, prostate cancers
2- Cancer treatments3- Palliative care
- Kidney disease 1- Management of end stage renal disease and availability of dialysis 2- Access to kidney transplant
- Diabetes Miletus 1- Receipt of diabetes recommended services: annual retinal eye exam, annual HGA1C, annual foot exam, annual Influenza vaccination and biannual lipid profile
2- Hospitalization for diabetes or its complications
(15) US department of health and human services, www.hhs.gov
Disparity in health care reflects the differences that exist in a health care system within a society in not only access to health care
23Transitional Period Policy Research
Health Care Policy in Future Syria
Clinical area Indicators to be assessed- Heart disease 1- Screening for hypertension
2- Screening for dyslipidemia3- Counselling on risk factors4- Management of acute myocardial infarction5- Management of heart failure6- Management of hypertension
- Maternal and neonatal care 1- Prenatal counselling2- Use of prenatal technologies3- Modes of delivery4- Maternal care outcome5- Birth weight and fetal and neonatal mortality
- Children care 1- Childhood immunization2- Adolescent immunization3- Management of gastroenteritis4- Childe dental care
- Mental health 1- Management of depression2- Management of substance abuse3- Suicide rate
- Respiratory care 1- Influenza vaccination2- Pneumococcal vaccination3- Management of asthma4- Management of pneumonia5- Management of upper respiratory tract infection (misuse of antibiotics)6- Management of tuberculosis
- Long term care (people with physical or cognitive limitations) or end of life care
1- Home health care2- Nursing homes3- Palliative end of life care
- Safety and outcome of treatment
1- Complication of treatment2- Nosocomial infections3- Avoidable death4- Medication adverse effects5- Injuries or adverse events due to technical errors6- Birth related trauma
- Patient perception 1- Inadequate access to care2- Waiting time to receive care
In other words, to address a concern of disparity in health care we can first identify the dimension of disparity (rural
vs. urban, etc.), then the clinical area or areas of concern (cancer, kidney disease, etc.), and begin data collection
assessing the specific indicators. It is very clear that a vital step in the effort to eliminate health care disparities is the
systematic collection and analysis of health care data. The analysis of collected data can be best achieved as part of
a national healthcare disparity study where the focus of quality remains at the heart of the study.

Strategic Research & Communication Centre
Health Care Policy in Future Syria
24
A national health care disparity study can help policymakers and researchers discern the areas of greatest need,
monitor trends over time, and identify successful programs for addressing those needs. This study can best be
conducted as a collaborative effort between the Ministry of Health, the office of planning and development,
the office of statistics and development, and the administrators and representatives of the disparity dimension
population being studied. The data for such critical study is usually extracted from surveys from samples of various
sources:
– Civilian and non-institutionalized populations.
– Health care facilities (hospitals, ambulatory care facilities, nursing homes, dialysis units, etc.).
– Administrative data systems (Ministry of Health and its sub-organisations).
– Office of Surveillance and Epidemiology.
Once data is collected and analysed, the needs for physicians and health care facilities are identified and plans
can be prepared to meet such deficiencies.
X. Assessing physicians shortage and surplus
Estimating physician requirements (general practice or specialists) is usually based on estimating demands and
supplies. However, it is strongly advised that this estimate is only completed after a detailed national disparity
study is finalized. This will also enable the transitional government to address differences in access to care and
quality of care within the different components of society(16) (detailed below).
Estimating demand:
This can be computed according to the following method: estimate the annual average of all types of patients’
visits to all types of physicians by one individual in the service area being studied, then multiply the above average
by the population number in the examined service area, which will provide an estimate of all physicians’ office
visits generated by local residents each year or the local demand for all physician services. It is also useful to
estimate the demand by physician specialties and particularly primary care specialties (family/general physicians,
internists, paediatricians, and obstetricians/gynaecologists) to better approximate rural communities demand.
(16) Volume I:122 On the Average I P per C, http://www.dartmouth.edu

25Transitional Period Policy Research
Health Care Policy in Future Syria
Estimating supply:
The first step to compute supply is to approximate the number of office visits a physician in a particular primary
or specialty care practice can handle annually. Example estimates of the number of annual visits that can be
handled by a family physician have ranged from 4200 to 5400 office visits per year averaging around 4800, while
the estimated patients for a midlevel provider (physician assistant or a nurse practitioner) is estimated at 3000
office visits a year.
Now if we multiply the above average by the number of available practitioners we will have an estimate of the
supply. We need to keep in mind however that this average estimates the potential supply and not necessarily
the actual supply since some physicians might like to see more than this average and some prefer a lighter load.
Therefore, to plug the actual supply it might be more accurate to plug in the actual number office visits for each
available health care provider.
Determining shortage or surplus:
The next step is to compare the total supply to demand to determine the degree of physician shortage or surplus.
This is done by subtracting the supply number from the demand number. If the number of unmet visits is greater
than 4,800 then we need one additional primary care physicians. If the number is less than 4,800, but greater
than 3000 we can then meet the shortage utilizing a physician assistant or a nurse practitioner. If the number is
above zero but less than 3000 we can consider part-time provider options, and certainly if the number is negative
we then have a surplus of providers.

Strategic Research & Communication Centre
Health Care Policy in Future Syria
26
XI. Necessary steps for creating medical research, development
and innovation program
Research and development (R&D) is defined as discovering new knowledge about products and services, and
applying that knowledge to create new and improved products, processes, and services that fill market needs.
R&D is not just an academic interest or a university prestige, but rather several significant benefits can be derived
from it.
R&D significantly contributes to the economic growth of a country through technology discovery and ownership;
it further increases employment and enhances competitiveness not only among Syrian universities but also within
the health care industry (pharmaceutical and medical device and products manufacturers). Health care R&D can
prepare and position Syrian universities and Syrian companies to engage partnerships with world universities and
multi-national companies which can be a very valuable opportunity to enter and compete in the global market.
Syria does not lack the intellectual capital needed to imitate a health care R&D program. Below are some
Recommendations that can be considered when initiating a health care R&D program in Syrian medical schools
and the Syrian health care industry:
1. Government can take action to provide dedicated funding for both basic sciences and applied research.
Very few Middle Eastern countries (Turkey for example) have realised the importance of dedicated funding
and as a result were able to significantly increase their production of original scientific papers. Dedicated
government funding for R&D is usually a percentage of the GDP and in the modern world it can range
between 2 and 4%.
2. Expand the function of medical schools so it is not just limited to teaching and patient care but for teaching,
patient care and research.
3. Provide an environment that assures complete independence for university professors, scientists and
researchers where they are protected from any political pressure or requirement to have a certain political
affiliation.
4. Promotions and career advancements can only be linked to performance and achievements.
27Transitional Period Policy Research
Health Care Policy in Future Syria
5. Take measures to encourage and facilitate the return of skilled Syrian manpower and intellectuals from
abroad.
6. Policy makers should pass and enforce patent laws to protect intellectual properties; this will encourage
Syrian corporations and investors to invest in R&D knowing that any potential profit is lawfully protected.
7. Create a national science board that consists of scientists, researchers, government strategic planners and
private investors or corporations where research proposals can be submitted for scientific and economical
evaluation prior to approval and funding support.
8. Encourage collaboration and joint research projects with adjacent regional or world universities and
corporations.
9. Government can take action and pass policies to encourage greater intellectual interchange between
industries and academia.
10. Government can take advantage of globalization; many world companies are establishing offshore research
facilities where it is more cost effective and Syrian universities once ready can be considered for such scientific
collaboration.
11. Government can enact laws that will provide incentives such as tax or custom incentives to corporations
which invest or finance approved R&D projects.
Strategic Research & Communication Centre
Health Care Policy in Future Syria
28
XII. Proposed changes to reform current health care policy
The following objectives can be incorporated into any reform or restructuring programs of the Syrian health care
policy:
1. Funding: This is one of the pillars of any health care system as declining or inadequate health care spending
will hinder all attempts to improve quality of care indicators or provide a viable and modern health care
system. Controlling the escalating health care costs will be a central component of the economics of health
care. Programs such as health information system and QA can lead to significant cost and expenditure savings
despite their inherent initial cost. The establishment of a health insurance system (private and government)
that can free the health care system from the tremendous financial burden of the widely spread free services
in government health facilities can also contribute to the control of the rapidly increasing health care costs.
2. Reliable health information system where information and data from all hospitals and medical facilities can
be reliably reported, analysed, and provided to policy makers. This system has a tremendous positive impact
on the quality of health care and health care expenditure.
3. Training of highly qualified health information managers and health care system administrators where
collected data can be skilfully and professionally analysed to identify areas of weaknesses and strengths.
4. Establishing a health care policy department run by highly qualified and specialized academicians, physicians,
economists, statisticians and politicians, where policies pertaining to health care financing, delivery of health
care, quality of care, special health care projects and access to care can all be developed.
5. Enforcing accountability where healthcare fraud and abuse can be aggressively targeted.
6. Creating accreditation standards for all hospitals and medical facilities in the country. These standards
will be mandatory and aim to achieve high quality of patient care services. The benefits of accreditation
standards are numerous and can be realized by learning that accredited hospitals offer higher quality of care
to their patients. Accreditation in general provides a competitive advantage in the health care industry and
strengthens community confidence in the quality and safety of care, treatment, and services.
7. Creating QA programs that must be set for both hospitals and physicians and have mandatory reporting
requirement to government and private health insurance agencies. Such programs can have several benefits:
- They assure the most achievable result for every patient.
29Transitional Period Policy Research
Health Care Policy in Future Syria
- They assist in the prevention of iatrogenic (physician-induced) complications.
- They help provide expert attention to patients.
- Enforcing QA programs can result in health care expenditure reduction as will be detailed below.
QA programs can help both hospitals and individual physicians to accurately assess their level of performance
in relation to established standards and to implement ways for continuous improvement. They can involve
both self-assessment and external pear reviews.
Certainly and as a possible road map aiming to establish QA programs in the country, a city like Damascus
can be selected where multiple governmental and private health care providers exist. A particular provider
can be chosen to implement a comprehensive QA program in its structure and subsequently introduce it to
the market place and the rest of the country as a model program.
8. Establish a health insurance system where patients can have the opportunity to seek care in private medical
facilities and thus reducing some of the expensive demand on free government hospitals. A national insurance
system can be a hybrid of both government medical services and government coverage in addition to private
insurance programs and it can aim to:
(1) Preventing the deprivation of care because of a patient's inability to pay.
(2) Avoiding wasteful spending.
(3) Providing quality care that meets standard health care indicators.
Re-assessing the free medical services currently provided in public government hospitals will be needed in
any reform program aiming to diminish the tremendous financial burden on government as a result of these
services. (Please see the health care insurance program below)
9. Mandate a clear credentialing and privileging department in each hospital, where the objective is to assure
that physicians are qualified and competent. The sets of criteria used for credentialing are determined by
the discipline society guidelines and recommendations. Other variables play a role as well in the process of
evaluation before privileges are granted including medical license, continuing medical education requirements,
training, malpractice and adverse clinical occurrences. Credentialing should apply to physicians, nurses and
all health care workers.
10. Establish a system of practice guidelines and recommendations. Relying on local research and medical society
guidelines, local guidelines can then be developed and implemented.
11. Create medical research as well as development and innovation programs.
12. Create a reliable and national emergency response process.
13. Establish high standards for nursing education and training schools. Nursing is a viable and critical component
of heath care and without such component providing a high quality patient care will be very challenging
Strategic Research & Communication Centre
Health Care Policy in Future Syria
30
if not impossible. In addition to contributing to patient care quality it is well established that high quality
nursing does have an economical value of reducing overall health care expenditures.
14. Eliminating disparity in health care: As mentioned before, the objective of a good health is really twofold:
A- The best attainable average level: goodness.
B- The smallest feasible differences among individuals and groups: fairness.
A gain in either one of these, with no change in the other, constitutes an improvement even though it is an
insufficient one.
31Transitional Period Policy Research
Health Care Policy in Future Syria
XIII. Need for a feasibility study
Health care restructuring in Syria is a major task. It is fragmented with many challenges in
both government and private sectors. Any effort of reform or restructuring has to be realistic
and practical. Changing from poor quality but free government health care services to high
quality and well organized system and incorporating private insurance providers as well as
government programs has to be a very well-studied project.
A comprehensive feasibility study will be essential to evaluate the demands and needed
resources of such change, assess the already existing resources and shed light on the prospects
for success. This feasibility study can be designed according to the methodology described in
the United Nations Industrial Development Organisation (UNIDO) "manual for the preparation
of industrial feasibility studies" where feasibility studies are in general divided into 3 stages
(pre-feasibility studies, the feasibility study, and Annexes).(17) Not different from any other industrial feasibility
studies, the proposed study will require:
1. Extensive research and evaluation of the existing health care system in Syria as it is today to reveal its
weaknesses and strengths.
2. Extensive planning and detailing of any proposed restructuring programs.
3. Economic feasibility evaluation: resources needed to carry through the proposed change (development cost
and operating cost to complete the proposed change).
4. Policy feasibility: examines the need for new policies or the need to modify existing policies to achieve the
proposed change.
5. Human resources feasibility: examines the human resources requirements needed to succeed in achieving
the proposed change.
6. Time feasibility: this means how long the proposed reform or restructuring will take to develop and become
operational, usually most projects will run the risk of failing if it takes too long for them to be completed
and useful.
(17) The United Nations Industrial Development Organization (UNIDO) http://www.unidoitpo.org.cn/EnAboutus.asp?id=3
Health care restructuring in Syria is a major task. It is fragmented with many challenges in both government and private sectors.
Strategic Research & Communication Centre
Health Care Policy in Future Syria
32
7. Prospects of success: Answers the questions whether the new system solves the problems which have been
already identified and will it improve the quality of health care in the country as quantified by the WHO
health care indicators.
XIV. Conclusion
Health care reform and the enactment of a new health care policy in Syria is of critical importance not only to
improve the physical and mental health of the Syrian people and enhance their sense of wellbeing but also due
to the significant contribution of the health care sector to the overall health and competitiveness of the economy.
Many deficiencies and obstacles do exist today and need to be identified, addressed and resolved in order to
achieve a desirable health care system and health quality that meet the people and government approval.
Realising all the challenges, one can conclude that the health and the future of the Syrian state and the Syrian
people are not only in the hands of the Syrian government but universities, scientists, the private sector and the
Syrian people themselves all bear the responsibility as well.

33Transitional Period Policy Research
Health Care Policy in Future Syria
1. Dean T. Jamison, Joel G. Breman, Anthony R. Measham, George Alleyne, Mariam Claeson, David B. Evans, Prabhat Jha, Anne Mills, Philip Musgrove, "Pillars of the Health System." 2006. Priorities in Health,ed. 155-178. New York: Oxford University Press. DOI: 10.1596/978-0-8213-6260-0/Chpt-7.
2. UNFPA Recommendation by the Executive Director Assistance to the Government of the Syrian Arab Republic (DP/FPA/SYR/6) 15 August 2001
3. The Legatum Institute, the 2011 Legatum prosperity index
4. World health organisation, programs and projects. World Health Organization Assesses the World›s Health Systems.
5. World health organisation, programs and reports. Global Health Observatory GHO, World Health Statistics.
6. Health matrix network, 8th Board Meeting, 23–24 July, Seattle, Washington, USA, 8/6/2007
7. "Total expenditure on health as % of GDP by country", World Health Organization. Retrieved from http://www.NationMaster.com/graph/hea_tot_exp_on_hea_as_of_gdp-health-total-expenditure-gdp
8. OECD Health Division (June 2011) "OECD Health Data". Paris.
9. WHO Department of Health Statistics and Informatics (May 13, 2011). World health statistics 2011. Geneva
10. Syria, World Bank data.
11. The United Nations Industrial Development Organization (UNIDO) http://www.unidoitpo.org.cn/EnAboutus.asp?id=3
12. The contribution of health care to the economy, Marc Suhrcke, Martin McKee, August 23, 2005.
13. US department of health and human services, www.hhs.gov
14. Volume I:122 On the Average I P per C, http://www.dartmouth.edu
15. Costs and Benefits of Health Information Technology Prepared for: Agency for Healthcare Research and Quality U.S. Department of Health and Human Services, 540 ither Road, Rockville, MD 20850.
16. CMS Hospital-Acquired Condition Measures for the Hospital Inpatient Quality Reporting Program [https://www.qualitynet.org].
17. CMS Medicare, Hospital IQR quality measures for payment determination
References

Strategic Research & Communication Centre90 Hatton Garden, Holborn
London EC1N 8PN, United KingdomEmail: [email protected]
Telephone: +442030868989 Website: www.strescom.orgAll rights reserved for
Strategic Research and Communication Centre © 2012
Strategic Research & Communication Centre
The Strategic Research and Communications Center (SRCC) was founded in 2010 to provide high-quality
research and media services to media outlets, government departments, academic institutions and
research centers through research, information, analysis and commentary on Syria. SRCC produced a
series of original studies examining the main political and socio-economic challenges in Syria – poverty,
unemployment, social and political repression.
While this work is of great value and significance as an aid to understanding the region, Syria itself
suffers from a shortage of political and social research. Local researchers must therefore participate in
bridging this information gap. A deeper understanding of the issues affecting the country can be attained
through pairing the philosophy and methodology of Western research with a firsthand knowledge of the
situation, and information gathered in the field. The Strategic Research and Communication Centre has
therefore joined forces with Syrian and Western researchers and academics in order to achieve this result.
The political, economic and social data and the strategic studies will be made available to policy makers,
correspondents, journalists, academics with an interest in Syrian affairs, and to all stakeholders.
About Transitional Period Policy Research
In light of the current changes and challenges in Syria, SRCC launched a research and policy-oriented
programme to revisit the related issues within the transitional research field in order to be a primary
resource for the new transitional government, civic groups and activists. The SRCC will convene the
most important indigenous stakeholders to formulate policy recommendations and implementation
strategies, serve as a platform for dialogue about competing approaches and publish papers that outline
the impending transition of power after President Bashar al-Assad vacates the office. The programme
focuses on the following areas: rule of law, national reconciliation, armed forces, economic and political
development, foreign policy, energy, health, education, water and agriculture, environment and tourism.