health benefits of herbs and spices: the past, the present
TRANSCRIPT

University of Wollongong University of Wollongong
Research Online Research Online
Faculty of Health and Behavioural Sciences - Papers (Archive) Faculty of Science, Medicine and Health
2006
Health benefits of herbs and spices: the past, the present, the future Health benefits of herbs and spices: the past, the present, the future
Linda C. Tapsell University of Wollongong, [email protected]
Ian Hemphill Herbie’s Spices, Sydney
Lynne Cobiac CSIRO
David R. Sullivan Royal Prince Alfred Hospital
Michael Fenech CSIRO
See next page for additional authors
Follow this and additional works at: https://ro.uow.edu.au/hbspapers
Part of the Arts and Humanities Commons, Life Sciences Commons, Medicine and Health Sciences
Commons, and the Social and Behavioral Sciences Commons
Recommended Citation Recommended Citation Tapsell, Linda C.; Hemphill, Ian; Cobiac, Lynne; Sullivan, David R.; Fenech, Michael; Patch, Craig S.; Roodenrys, Steven; Keogh, Jennifer B.; Clifton, Peter M.; Williams, Peter G.; Fazio, Virginia A.; and Inge, Karen E.: Health benefits of herbs and spices: the past, the present, the future 2006. https://ro.uow.edu.au/hbspapers/1397
Research Online is the open access institutional repository for the University of Wollongong. For further information contact the UOW Library: [email protected]

Health benefits of herbs and spices: the past, the present, the future Health benefits of herbs and spices: the past, the present, the future
Abstract Abstract The purpose of this supplement is to provide medical and health professionals with a review of the health benefits of herbs and spices.
The University of Wollongong, partner organisation of the National Centre of Excellence in Functional Foods, managed the development of the supplement through a committee comprising Professor Linda Tapsell, Dr Craig Patch and Ms Virginia Fazio.
Key academics and clinicians with expertise in health and nutrition were invited to review the health aspects of predominantly culinary herbs and spices, using scientific search strategies and National Health and Medical Research Council guidelines for assessing levels of evidence.
The resulting individual contributions were submitted to the management committee for the development of summary positions.
This supplement was supported by an educational grant from Gourmet Garden. The views expressed in this supplement are those of the authors. Gourmet Garden had no influence on the content.
Disciplines Disciplines Arts and Humanities | Life Sciences | Medicine and Health Sciences | Social and Behavioral Sciences
Publication Details Publication Details Tapsell, L. C., Hemphill, I., Cobiac, L., Sullivan, D. R., Fenech, M., Patch, C. S., Roodenrys, S., Keogh, J. B., Clifton, P. M., Williams, P. G., Fazio, V. A. & Inge, K. E. (2006). Health benefits of herbs and spices: the past, the present, the future. Medical Journal of Australia, 185 (4), S1-S24. © Copyright 2006. The Medical Journal of Australia - reproduced with permission.
Authors Authors Linda C. Tapsell, Ian Hemphill, Lynne Cobiac, David R. Sullivan, Michael Fenech, Craig S. Patch, Steven Roodenrys, Jennifer B. Keogh, Peter M. Clifton, Peter G. Williams, Virginia A. Fazio, and Karen E. Inge
This journal article is available at Research Online: https://ro.uow.edu.au/hbspapers/1397

www.mja.com.auPRINT POST APPROVED PP255003/00505
ESTABLISHED IN 1914
JOURNAL OF THE AUSTRALIAN
MEDICAL ASSOCIATION
MJA S U P P L E M E N T 2 1 A U G U S T 2 0 0 6
THE MEDICAL JOURNAL OF AUSTRALIA V O L U M E 1 8 5 N U M B E R 4
Health benefits of herbs and spices:the past, the present, the future
MJA • Volume 185 Number 4 • 21 August 2006 S1
HEALTH BENEFITS OF HERBS AN D SPICES: THE PAST, TH E PRESENT, THE FUTURE
The Medical Journal of Australia ISSN: 0025-729X 21 August 2006 185 4 1-24©The Medical Journal of Australia 2006www.mja.com.auSupplement
The purpose of this supplement is to provide medical and health professionals with a review ofthe health benefits of herbs and spices.
The University of Wollongong, partner organisation of the National Centre of Excellence in Functional Foods,managed the development of the supplement through a committee comprising
Professor Linda Tapsell, Dr Craig Patch and Ms Virginia Fazio.
Key academics and clinicians with expertise in health and nutrition were invited to review the health aspects of predominantly culinary herbs and spices, using scientific search strategies and
National Health and Medical Research Council guidelines for assessing levels of evidence.
The resulting individual contributions were submitted to the management committee for the development of summary positions.
This supplement was supported by an educational grant from Gourmet Garden.The views expressed in this supplement are those of the authors. Gourmet Garden had no influence on the content.
Health benefits of herbs and spices: the past, the present, the future

S2 MJA • Volume 185 Number 4 • 21 August 2006
SU PPLEMENT
Health benefits of herbs and spices:the past, the present, the future
Panel contributors
Guest editorProfessor Linda C Tapsell, PhD, MHPEd, DipNutrDiet, FDAA, Director, National Centre of Excellence in Functional Foods, University of Wollongong, Wollongong, NSW.
Panel membersMr Ian Hemphill, Director, Herbie’s Spices, Sydney, NSW.
Dr Lynne Cobiac, PhD, MBA(Advanced), PostGradDipNutrDiet, Business Manager, Preventative Health National Research Flagship, CSIRO, Adelaide, SA.
Associate Professor David R Sullivan, FRACP, FRCPA, FCANZ, Clinical Associate Professor, Department of Clinical Biochemistry, Royal Prince Alfred Hospital, Sydney, NSW.
Dr Michael Fenech, PhD, Principal Research Scientist, CSIRO Human Nutrition, Adelaide, SA.
Dr Craig S Patch, PhD, MBA, GradDipNutrDiet, Industry Projects Manager, National Centre of Excellence in Functional Foods, University of Wollongong, Wollongong, NSW.
Associate Professor Steven Roodenrys, PhD, Associate Professor, School of Psychology, University of Wollongong, Wollongong, NSW.
Ms Jennifer B Keogh, MSc, DipDiet, Research Dietitian, CSIRO Human Nutrition, Adelaide, SA.
Professor Peter M Clifton, PhD, FRACP, Theme Leader Obesity, CSIRO Human Nutrition, Professor of Medicine, University of Adelaide, Adelaide, SA.
Associate Professor Peter G Williams, PhD, MHP, DipNutrDiet, Director, Smart Foods Centre, University of Wollongong, Wollongong, NSW.
Ms Virginia A Fazio, MSc, MBA, GradDipDiet, Senior Consultant Dietitian, Institute of Health and Fitness, Melbourne, VIC.
Ms Karen E Inge, BSc, DipDiet, Director, Institute of Health and Fitness, Melbourne, VIC.
FacilitatorDr Craig S Patch, PhD, MBA, GradDipNutrDiet, Industry Projects Manager, National Centre of Excellence in Functional Foods, University of Wollongong, Wollongong, NSW.
Correspondence:Dr Craig S Patch, National Centre of Excellence in Functional Foods, University of Wollongong, Wollongong, NSW 2522.Phone: +61 2 4221 5125; Fax: +61 2 4221 [email protected]

MJA • Volume 185 Number 4 • 21 August 2006 S3
HEALTH BENEFITS OF HERBS AN D SPICES: THE PAST, TH E PRESENT, THE FUTURE
Contents
Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . S4
Linda C Tapsell
Background. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . S5
The historical and cultural use of herbs and spices . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . S5
Ian Hemphill and Lynne Cobiac
Herbs and spices as functional foods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . S6
Linda C Tapsell
The health benefits of herbs and spices: how strong is the evidence? . . . . . . . . . . . . . . . . . . . . . . . . . . . . S7
Cardiovascular disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . S7
Craig S Patch and David R Sullivan
Cancer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . S7
Michael Fenech
Mental health and cognition . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . S12
Steven Roodenrys
Type 2 diabetes mellitus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . S14
Jennifer B Keogh and Peter M Clifton
Osteoarthritis and inflammatory response . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . S15
Craig S Patch
Public health . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . S17
Peter G Williams
Dietary implications . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . S19
Virginia A Fazio and Karen E Inge
Moving forward . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . S21
Linda C Tapsell
Competing interests. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . S22
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . S22

S4 MJA • Volume 185 Number 4 • 21 August 2006
SU PPLEMENT
Summary
Linda C Tapsell
Herbs and spices have a traditional history of use, with strong rolesin cultural heritage, and in the appreciation of food and its links tohealth. Demonstrating the benefits of foods by scientific meansremains a challenge, particularly when compared with standardsapplied for assessing pharmaceutical agents. Pharmaceuticals aresmall-molecular-weight compounds consumed in a purified andconcentrated form. Food is eaten in combinations, in relativelylarge, unmeasured quantities under highly socialised conditions.The real challenge lies not in proving whether foods, such as herbsand spices, have health benefits, but in defining what thesebenefits are and developing the methods to expose them byscientific means.
Cultural aspectsThe place of herbs and spices in the diet needs to be considered inreviewing health benefits. This includes definitions of the foodcategory and the way in which benefits might be viewed, andtherefore researched. Research may focus on identifying bioactivesubstances in herbs and spices, or on their properties as a wholefood, and/or be set in the context of a dietary cuisine.
The role of herbs and spices in healthThe antioxidant properties of herbs and spices are of particularinterest in view of the impact of oxidative modification of low-density lipoprotein cholesterol in the development of atherosclero-sis. There is level III-3 evidence (National Health and MedicalResearch Council [NHMRC] levels of evidence1) that consuming ahalf to one clove of garlic (or equivalent) daily may have acholesterol-lowering effect of up to 9%. There is level III-1evidence that 7.2 g of aged garlic extract has been associated withanticlotting (in-vivo studies), as well as modest reductions inblood pressure (an approximate 5.5% decrease in systolic bloodpressure).
A range of bioactive compounds in herbs and spices have beenstudied for anticarcinogenic properties in animals, but the chal-lenge lies in integrating this knowledge to ascertain whether anyeffects can be observed in humans, and within defined cuisines.
Research on the effects of herbs and spices on mental healthshould distinguish between cognitive decline associated withageing and the acute effects of psychological and cognitive func-tion. There is level I and II evidence for the effect of some herbalsupplements on psychological and cognitive function.
There is very limited scientific evidence for the effects of herbsand spices on type 2 diabetes mellitus, with the best evidencebeing available for the effect of ginseng on glycaemia, albeit based
on four studies. More research is required, particularly examiningthe effects of chronic consumption patterns.
With increasing interest in alternatives to non-steroidal anti-inflammatory agents in the management of chronic inflammation,research is emerging on the use of food extracts. There is level IIevidence for the use of ginger in ameliorating arthritic knee pain;however, the improvement is modest and the efficacy of gingertreatment is ranked below that of ibuprofen. More definitiveresearch is required.
Public health and dietary implications
Recommendations for intakes of food in the Australian guide tohealthy eating2 do not yet include suggested intakes of herbs andspices. Future consideration should be given to including moreexplicit recommendations about their place in a healthy diet.
In addition to delivering antioxidant and other properties, herbsand spices can be used in recipes to partially or wholly replace lessdesirable ingredients such as salt, sugar and added saturated fat in,for example, marinades and dressings, stir-fry dishes, casseroles,soups, curries and Mediterranean-style cooking. Vegetable dishesand vegetarian options may be more appetising when preparedwith herbs and spices.
Future directions
As several metabolic diseases and age-related degenerative disor-ders are closely associated with oxidative processes in the body, theuse of herbs and spices as a source of antioxidants to combatoxidation warrants further attention. Immediate studies shouldfocus on validating the antioxidant capacity of herbs and spicesafter harvest, as well as testing their effects on markers ofoxidation. This will work in parallel with clinical trials that areaiming to establish antioxidants as mediators of disease prevention.
From a dietary perspective, the functionality of herbs and spiceswill be exposed through consideration of their properties as foods.As with most foods, the real benefits of including them in the dietare likely to emerge with a better understanding of the attributes ofhealth that are best supported by food, and in methodologicaldevelopments addressing the evidence base for their effects.3,4
These developments are well underway through evidence-basedframeworks for substantiating health claims related to foods.5 Atpresent, recommendations are warranted to support the consump-tion of foods rich in bioactive components,6 such as herbs andspices. With time, we can expect to see a greater body of scientificevidence supporting the benefits of herbs and spices in the overallmaintenance of health and protection from disease.

MJA • Volume 185 Number 4 • 21 August 2006 S5
HEALTH BENEFITS OF HERBS AN D SPICES: THE PAST, TH E PRESENT, THE FUTURE
Background
The historical and cultural use of herbs and spices Ian Hemphill and Lynne Cobiac
Generally, the leaf of a plant used in cooking may be referred to asa culinary herb, and any other part of the plant, often dried, as aspice. Spices can be the buds (cloves), bark (cinnamon), roots(ginger), berries (peppercorns), aromatic seeds (cumin), and eventhe stigma of a flower (saffron). Many of the aromatic seeds knownas spices are actually gathered from plants when they have finishedflowering. A familiar example would be coriander, with the leavesbeing referred to as a herb, and the dried seeds as a spice. Whenreferring to the stem and roots of coriander, which are used incooking, and to onions, garlic and the bulb of fennel, these parts ofthese plants tend to be classified along with herbs, as they are oftenused fresh and applied in a similar way to cooking.
Herbs and spices have a long history of both culinary use and ofproviding health benefits, as well as acting as preservatives.Ancient Egyptian papyri from 1555 BCE record the use of corian-der, fennel, juniper, cumin, garlic and thyme.7 It is reported thatthe Sumerians were using thyme for its health properties as early as5000 BCE, and the farmers of Mesopotamia were growing garlic asearly as 3000 BCE. An international trade in spices dates back to4500–1900 BCE, mainly with Ethiopia. The ancient Egyptiansworshipped garlic, and garlic cloves were found in the tomb ofKing Tutankhamen. Other Egyptians had wooden cloves of garlicin their tombs to keep the future meals of the afterlife tasty,wholesome and long-lasting.8 Dried mint leaves have been foundin Egyptian pyramids dating around 1000 BCE.9 The Egyptiansreportedly fed large amounts of radishes, onions and garlic to theirslaves, ostensibly to keep them healthy.7 Cardamom and cinnamon(traded from Ethiopia) were also used extensively in ancient Egyptas spices, but less so for medicinal purposes. The Assyrians inMesopotamia (a country now incorporated by modern day Iraqand Iran) also developed knowledge around the health benefits ofherbs, and refer to juniper, saffron, and thyme around this time.7
In ancient Greece and Rome, herbs appear to have been usedmore than spices. Hippocrates (460–377 BCE) had a repertoire of300 remedies that included garlic, cinnamon and rosemary, all ofwhich were locally available.7 He reportedly used garlic to treatuterine cancer. Mint was highly valued for its positive effects on thedigestive system, and liquorice was used as a sweet, but also as aherb for its anti-inflammatory actions and for asthma, chestproblems and mouth ulcers. Rosemary was used to improve andstrengthen memory — and is sometimes still burnt in the homes ofGreek students taking exams. Around the first century CE, Pedan-ius Dioscorides — Greek physician, botanist, pharmacologist andsurgeon — published the first plant monograph that included 600herbs, describing how to choose, store and apply plants for a rangeof health benefits. Another Greek physician, Galen (131–200 CE),who lived in Rome from 162 CE, had a strong influence on thedevelopment of herbal remedies, but used complicated mixtures,containing up to 100 ingredients.7 Dioscorides’ monograph wasused as a principal reference in Europe until the 17th century.9
In China, the use of plants for health benefits is shrouded inlegend. Two legendary Chinese emperors are credited with discov-ering and recording the medicinal properties of herbs — Sheng
Nong, the Divine Husbandman (2838–2698 BCE), and Huang Di,the Yellow Emperor (2698–2598 BCE).7 Traditionally, the Chinesehave integrated food, nutrition and health, and will often includeherbs and spices in specially prepared soups, dishes or beveragesfor both sustenance and for purported health benefits. Ginsengand Ginkgo biloba are reportedly used to improve stamina andcognitive performance, respectively. Other examples include theuse of galangal for abdominal pain, nutmeg for diarrhoea, andcinnamon for colds and flu.7
In India, the traditional medicine, Ayurveda, evolved more than5000 years ago in the Himalayas, with knowledge transmitted orallyuntil it was written down in Sanskrit poetry — the Vedas — around1500 BCE. It flourished in the 7th century. Ayurveda focuses ondisease prevention and health promotion, with an emphasis ondiet.10,11 Examples of Ayurvedic use of herbs and spices for healtheffects include turmeric for jaundice, basil to protect the heart, macefor stomach infections, cinnamon to stimulate circulation, andginger as the universal medicine, in particular for relieving nauseaand indigestion. Many of these herbs and spices are used in Indiancooking to impart flavour, and significant quantities can be con-sumed in one meal. It has been reported that such herbs and spicescan supply reasonable quantities of nutrients as well, such as iron. Ithas been estimated that an adult in India can eat as much as 4 g ofturmeric daily, which could provide 80–200 mg/day of the bioactivecomponent curcumin. Some Indians have been reported to eat asmuch as 50 g of garlic in a week.12
With the decline of the Roman Empire around 476 CE, thedevelopment of Arabic medicine in 500–1300 CE preserved someof the knowledge surrounding the health benefits of herbs andspices, and built on the knowledge of Galen.7 The spread ofIslamic culture into north Africa had profound effects in theregion, blending their knowledge with that from China and India.
In the 9th century, the Emperor Charlemagne is quoted assaying, “a herb is a friend of physicians and the praise of cooks”,suggesting that the dual role of herbs and spices for flavouring andfor health benefits was still recognised. During the 11th century,the knowledge of Arabic medicine filtered back to Europe, and bythe 13th century, trade with Africa and Asia was bringing in newherbs and spices. Around this time, galangal was called the “spiceof life”.7 Garlic was used by herbalists during the plague.7 Later,Louis Pasteur (1822–1895 CE) found that it killed bacteria, and itwas even used on the battlefields to prevent gangrene.
Mediterranean diets have been associated with reduced incidence ofsome chronic diseases, such as heart disease and cancer.13 Whiledietary studies are complex, Mediterranean diets do include consider-able amounts of garlic, rosemary, basil and thyme, among other herbs,which may help to explain some of the protective effects observed inpopulations following more traditional Mediterranean diets.
In Australia, the Indigenous population developed its own localherbal medicine based on the plants that were available. Theirisolation meant that the Indigenous population did not encounterWestern diseases, and so the use of herbs and plants wasdeveloped for less serious disorders. Examples include the use ofriver mint for coughs and colds, and wattle and eucalyptus fordiarrhoea, fever, headache, and a range of other ailments.14
Given the long history of use of herbs and spices, they may beconsidered one of the first ever recorded functional foods.

S6 MJA • Volume 185 Number 4 • 21 August 2006
SU PPLEMENT
Herbs and spices as functional foodsLinda C Tapsell
Examining herbs and spices from a functional food perspectivemight begin with how herbs and spices are used in the diet. Thereis no single definition of functional foods, but there are manycontexts in which the concept is played out, including scientificendeavour, technological advancement, food marketing, and foodstandards regulation.15 From a scientific perspective, functionalfoods have been defined as “foods that provide benefit beyondbasic nutrition”.16 This definition draws on notions of food (ie, arecognisable unit of consumption in contradistinction to drugs),notions of benefits (which implies the need for scientific evidence),and the notion of “basic nutrition” (a concept open to interpreta-tion). In some ways, basic nutrition might actually reflect thecurrent depth of nutrition knowledge and practice. Thus, meetingrequirements for vitamins and minerals (which have recom-mended reference values)17 could be considered basic nutrition.The underlying view is that these nutrients are required tomaintain normal bodily function. However, the way in which foodcomponents of today are studied is not limited to concepts ofpreventing clinical deficiency and maintaining homeostasis, butincludes a growing recognition of the way in which food compo-nents actively interact with the body to support health and preventabnormality and overt disease.18
Herbs and spices fit into this picture in a number of ways. In thissupplement, the focus is on their role in the diet rather than theiruse as medicines. Establishing this role would involve identifyingunique bioactive compounds to help identify target benefits.Research would then be conducted on the food itself (supple-ments), a meal based on the food (acute effects), or the food in awhole diet in which the observed benefits can be attributed to thespecified combination. The traditional use of foods in variouscultures provides many clues to this development. For example,certain meals in traditional Thai cuisine have a cultural history ofsupporting health based on their combination of herbs, spices andother foods,19 so that it might be better for dietary guidelines toreference dishes, rather than single foods as we do in Westernsocieties (which tend to focus on targeted nutrients being deliveredby core food groups). The real challenge then comes from definingbenefits and providing the scientific evidence for these benefits.
In this supplement, the evidence for the benefits of herbs andspices is reviewed in the areas of cardiovascular and metabolichealth, healthy ageing and cancer, and mental health and cogni-tion. Applying nutrition knowledge about herbs and spices inpublic health guidelines and dietary practice is also considered.The supplement outlines the many ways in which the functionalityof herbs and spices could be considered, providing direction forfuture research and developing an appreciation of the potentialcontributions of herbs and spices to health and wellbeing.

MJA • Volume 185 Number 4 • 21 August 2006 S7
HEALTH BENEFITS OF HERBS AN D SPICES: THE PAST, TH E PRESENT, THE FUTURE
The health benefits of herbs and spices:how strong is the evidence?
Cardiovascular diseaseCraig S Patch and David R Sullivan
Most evidence concerning the cardiovascular effects of culinaryherbs and spices relates to the possible impact of garlic and garlicoil. Consumption of garlic or garlic oil has been associated with areduction in total cholesterol, low-density lipoprotein (LDL) cho-lesterol, and triglyceride levels. Studies suggest that an intake ofbetween half and one garlic clove per day can reduce cholesterol by9%.20,21 This finding is consistent with a more recent meta-analysisof 13 placebo-controlled trials involving 781 patients taking garlicsupplements. The authors concluded that intake of 600–900 mg ofstandardised garlic extract per day was associated with a modest0.41 mmol/L decrease in serum cholesterol level.22 Although thiswas verified in the most current and comprehensive review,23 theauthors highlighted that the six most rigorous trials showed a non-significant trend (Box 1).24-29
It has been suggested that this variation of effect may reflect aloss of active compounds during processing, or an inhibition in theenzymatic release of the active compounds from garlic.25 Allicinhas been proposed as the primary active compound, although themechanism of action is still not well understood. Allicin is notpresent in fresh garlic and is converted from the precursor alliinwithin seconds of being crushed or chewed. Allicin is rapidlyabsorbed in the small intestine and converted to allyl mercaptanand allyl methyl sulfide soon after absorption.30 In addition,factors related to food preparation, manufacturing, and in-vivometabolism affect the bioactivity of allicin and may explain someof the heterogeneity of results found in these meta-analyses.21,22
With few exceptions, the more recent published trials have useddietary supplemental forms of garlic, rather than garlic as a food.30
This has significant implications, as a study found that the allicinyield of 24 commercial brands of garlic tablets averaged 14% of theamount claimed on the label.21,31 Of the brands used in most ofthe clinical trials since 1995, the active ingredient was found to beonly 2%–18% of that claimed on the label.32
A number of clinical trials have examined the effect of garlic oncardiovascular risk factors other than lipoproteins and lipid levels.Garlic extracts have been associated with anticlotting effects,33 as wellas modest reductions in blood pressure (about a 5.5% decrease insystolic pressure).34 However, of the 33 published studies with dataon blood pressure, only four included patients with hypertension.6
Data on the effects of other herbs and spices are limited. In onetrial, participants with hypercholesterolaemia who consumed140 mg of lemon grass (Cymbopogon citratus) oil daily experienced adrop in cholesterol concentrations by up to 38 mg/dL, but this trialhad no control group.35 Spice components like ginger, capsaicinand curcumin have been associated with a decrease in LDLcholesterol and an increase in high-density lipoprotein cholesterollevels, but these results have been limited to rat studies.36,37
The putative protective heart health benefits of antioxidants suchas flavonoids have been extensively studied. A longitudinal study of805 elderly men found that daily flavonoid intake from fruit,vegetables and tea of 25.9 ±14.5 mg (mean ± SD) was inversely
associated with heart disease mortality.38 Herbs and spices have animportant role in dietary flavonoid intake. Chamomile, liquorice,onions, rosemary, sage and thyme have high flavonoid contents, butthere is little evidence apart from epidemiological studies tosupport a direct cardiovascular health benefit from these herbs andspices.
In recent years, a substantial body of evidence has indicated thatfree radicals contribute to cardiovascular disease.39 Oxidative mod-ification of LDL is hypothesised to play a key role during thedevelopment of atherosclerosis. The use of antioxidants fromdietary sources, including herbs and spices, is a promising alterna-tive to the use of antioxidant supplements. In general, herbs andspices have high antioxidant concentrations that have the potentialto inhibit the oxidation of LDL.40,41 Like fruits and vegetables,herbs and spices contain many different classes of antioxidants invarying amounts. It has been shown that the intake of herbs cancontribute significantly to the total intake of plant antioxidants.42 Astudy found that the total phenolic content of culinary herbs rangedfrom 0.26 mg to 17.51 mg of gallic acid per gram fresh weight(Box 2).43 These values were also found to be higher thantraditional medicinal herbs.25 At this stage, evidence of benefit fromany form of antioxidant intake is restricted to surrogate markers ofcardiovascular disease, such as oxidative damage, rather thanclinical outcomes.
Obesity-related insulin resistance has emerged as a potent riskfactor for cardiovascular disease. Dietary factors that affect satietyand thermogenesis could play an important role in determining theprevalence and severity of this problem. Herbs and spices may havea role to play in this regard. More data are also required onbioavailability, bioactivity, and efficacy of culinary herbs on out-comes.
Summary
• There is level III-3 evidence that a half to one clove of garlic (orequivalent) daily may have a cholesterol-lowering effect of up to9%.• There is level III-1 evidence that 7.2 g of aged garlic extract hasbeen associated with anticlotting (in-vivo studies), as well asmodest reductions in blood pressure (about a 5.5% decrease insystolic pressure).• More evidence is required to determine any cardiovascularhealth effects attributable to herb and spice antioxidants.
CancerMichael Fenech
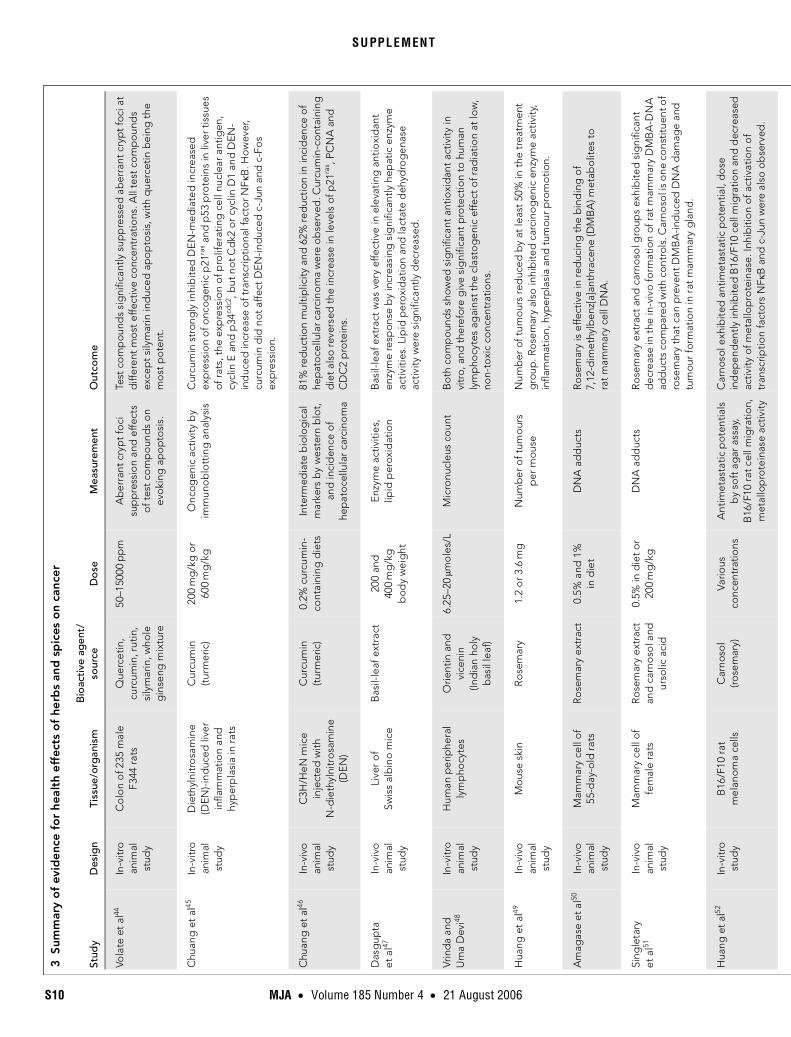
As yet, there are no data indicating that herbs and spices have ananticarcinogenic effect in humans, but there are several in-vitrostudies and rodent in-vivo studies suggesting that certain herbsand spices may have a chemopreventive effect against the earlyinitiating stages of cancer (Box 3).

S8 MJA • Volume 185 Number 4 • 21 August 2006
SU PPLEMENT1
Sum
mar
y o
f ev
iden
ce f
or
heal
th e
ffe
cts
of
gar
lic a
nd
gar
lic e
xtra
cts
on
low
erin
g c
hole
ste
rol l
eve
ls
Stud
yD
esig
nSt
udie
s/p
arti
cip
ants
Sour
ceD
ose
Mea
sure
men
tO
utco
me
War
shaf
sky
et a
l21M
eta-
anal
ysis
5 ho
mo
gen
ous
stu
die
sG
arlic
Vario
us d
oses
Cho
lest
ero
l lev
elPa
tient
s tr
eate
d w
ith g
arlic
sho
wed
a g
reat
er d
ecre
ase
in t
otal
ch
oles
tero
l lev
els
com
par
ed w
ith t
hose
rece
ivin
g p
lace
bo
. Net
ch
oles
tero
l dec
reas
e at
trib
utab
le t
o g
arlic
was
est
imat
ed t
o b
e 0.
59m
mo
l/L.
Stev
inso
n et
al22
Met
a-an
alys
is13
tria
lsG
arlic
Vario
us, f
rom
0.
25m
g/k
g t
o
900
mg
dai
ly
Tota
l cho
lest
ero
l le
vel
Gar
lic re
duc
ed t
ota
l cho
lest
ero
l lev
el fr
om
bas
elin
e si
gni
fican
tly
mo
re t
han
pla
ceb
o, b
ut th
e si
ze o
f eff
ect
was
mo
des
t an
d th
e ro
bus
tnes
s of
the
effe
ct is
deb
atab
le.
Ack
erm
ann
et a
l23R
evie
w a
rtic
le45
ran
do
mis
ed
cont
rolle
d t
rials
last
ing
at l
east
4
wee
ks
Gar
lic
pre
par
atio
nVa
rious
Tota
l cho
lest
erol
, LD
L, H
DL
and
tr
igly
cerid
e le
vels
, p
late
let a
gg
reg
atio
n an
d b
lood
pre
ssur
e
Gar
lic m
ay le
ad t
o s
mal
l red
uctio
ns in
tot
al c
hole
ster
ol le
vels
at
1 m
ont
h an
d 3
mo
nths
, but
no
t at 6
mo
nths
. Cha
nges
in L
DL
and
trig
lyce
ride
leve
ls p
aral
lelle
d to
tal c
hole
ster
ol r
esul
ts.
No
sig
nific
ant c
hang
es in
HD
L le
vels
wer
e o
bse
rved
. Red
uctio
n in
p
late
let a
gg
reg
atio
n w
as o
bse
rved
and
eff
ects
on
blo
od
pre
ssur
e w
ere
mix
ed.
Sim
ons
et a
l24R
and
om
ised
, d
oub
le-b
lind
, p
lace
bo
-co
ntro
lled
, cr
oss
ove
r tr
ial
28 p
artic
ipan
ts w
ith
mild
to
mo
der
ate
hyp
erch
ole
ster
ola
emia
Gar
lic
po
wd
er
tab
lets
300
mg
thr
ee t
imes
d
aily
Plas
ma
lipid
leve
ls
and
blo
od p
ress
ure
No
sig
nific
ant d
iffer
ence
s in
pla
sma
cho
lest
ero
l, LD
L, H
DL,
p
lasm
a tr
igly
cerid
es, l
ipo
pro
tein
(a) c
onc
entr
atio
ns o
r b
lood
p
ress
ure.
The
re w
as n
o d
emo
nstr
able
eff
ect
of g
arlic
on
oxi
dis
abili
ty o
f LD
L.
Isaa
cso
hn
et a
l25R
and
om
ised
, d
oub
le-b
lind
, p
lace
bo
-co
ntro
lled
, 12
-wee
k, p
aral
lel
trea
tmen
t tria
l
50 p
artic
ipan
tsG
arlic
p
ow
der
300
mg
thr
ee t
imes
d
aily
(eq
uiva
lent
to
2.
7g
gar
lic o
r 1
clo
ve
of g
arlic
per
day
)
Plas
ma
lipid
and
lip
op
rote
in le
vels
No
sig
nific
ant l
ipid
or l
ipop
rote
in c
hang
es in
eith
er t
he g
arlic
-tr
eate
d o
r p
lace
bo
gro
ups,
and
no
sig
nific
ant d
iffer
ence
bet
wee
n ch
ang
es in
the
pla
ceb
o-tr
eate
d g
roup
co
mp
ared
with
cha
nges
in
the
gar
lic-t
reat
ed p
arti
cip
ants
wer
e o
bse
rved
.
Sup
erko
and
K
raus
s26R
and
om
ised
, d
oub
le-b
lind
p
lace
bo
-co
ntro
lled
tria
l
50 p
artic
ipan
ts w
ith
mo
der
ate
hyp
erch
ole
ster
ola
emia
Gar
lic30
0m
g t
hree
tim
es
dai
lyTo
tal c
hole
ster
ol,
LDL,
HD
L an
dtr
igly
cerid
e le
vels
No
sig
nific
ant c
hang
es in
pla
sma
lipid
leve
ls a
fter
inte
rven
tion
wer
e ob
serv
ed. G
arlic
ther
apy
had
no
effe
ct o
n m
ajor
pla
sma
lipo
pro
tein
s.
Gar
dne
r et
al27
Ran
do
mis
ed,
do
uble
-blin
d,
pla
ceb
o-
cont
rolle
d, p
aral
lel
trea
tmen
t tria
l
51 p
artic
ipan
tsG
arlic
p
ow
der
500
mg
and
100
0m
gPl
asm
a lip
id le
vels
Red
uctio
n o
f LD
L ch
ole
ster
ol l
evel
in fu
ll d
ose
gro
up w
as n
ot
sig
nific
antly
diff
eren
t fro
m t
he o
ther
gro
ups.
No
sig
nific
ant
diff
eren
ces
in t
ota
l cho
lest
ero
l, H
DL
and
trig
lyce
ride
leve
ls
wer
e ob
serv
ed.
Gor
e an
d
Dal
en20
Rev
iew
pap
erG
UST
O a
ngio
gra
phi
c tr
ial
Gar
licO
ne-h
alf t
o o
ne c
love
p
er d
ayC
hole
ster
ol l
evel
Cho
lest
ero
l lev
els
can
be
red
uced
by
up to
9%
by
the
cons
ump
tion
of o
ne-h
alf t
o o
ne c
love
of g
arlic
per
day
.
Ber
tho
ld
et a
l28R
and
om
ised
, d
oub
le-b
lind
, p
lace
bo
-co
ntro
lled
tria
l
25 p
artic
ipan
ts
with
mo
der
ate
hyp
erch
ole
ster
ola
emia
Gar
lic o
il p
rep
arat
ion
5m
g t
wic
e d
aily
Seru
m li
po
pro
tein
le
vels
, cho
lest
ero
l ab
sorp
tion,
ch
ole
ster
ol
synt
hesi
s
Lip
opro
tein
leve
ls w
ere
virt
ually
unc
hang
ed a
t th
e en
d o
f bo
th
trea
tmen
t p
erio
ds.
Cho
lest
ero
l ab
sorp
tion,
cho
lest
ero
l syn
thes
is,
mev
alon
ic a
cid
sec
retio
n, a
nd c
hang
es in
the
ratio
of l
atho
ster
ol
to c
hole
ster
ol i
n se
rum
wer
e no
t diff
eren
t in
gar
lic a
nd p
lace
bo
tr
eatm
ent.
LDL
=lo
w-d
ensi
ty li
po
pro
tein
. HD
L=
hig
h-d
ensi
ty li
pop
rote
in. G
UST
O=
Glo
bal
Util
izat
ion
of S
trep
toki
nase
and
Tis
sue
Plas
min
og
en A
ctiv
ator
for
Occ
lud
ed C
oro
nary
Art
erie
s.◆

MJA • Volume 185 Number 4 • 21 August 2006 S9
HEALTH BENEFITS OF HERBS AN D SPICES: THE PAST, TH E PRESENT, THE FUTURE
Herbs may act through several mechanisms to provide protec-tion against cancer. Certain phytochemicals from herbs or herbextracts have been shown to inhibit one or more of the stages ofthe cancer process (ie, initiation, promotion, growth and meta-stases).62-65 Inhibition of phase I (procarcinogen activation) andinduction of phase II (carcinogen deactivation) metabolic enzymesby herbal products may account for some of the preventive effectsagainst the induction of gene or chromosomal mutations that mayinitiate cancer.62,63 For example, diallyl sulfide, a compound ingarlic, is an efficient inhibitor of the phase I enzyme cytochromeP450 (CYP)3 IIE1 and significantly increases a variety of phase IIenzymes, including glutathione S-transferase, quinone reductaseand uridine diphosphate-glucuronosyltransferase, which areresponsible for the detoxification of carcinogens.63
Herbs may also protect against oxidative stress and inflamma-tion, both of which are risk factors for cancer initiation andpromotion as well as other pathological conditions.64-67 An imbal-ance between the generation of reactive oxygen species (eg,hydroxyl radical and superoxide radical anion) and cellular anti-oxidant capacity leads to a state of oxidative stress. Herbs andspices contain several natural water-soluble phenolic acids andflavonoids, such as caffeic acid and quercetin, that can scavengereactive oxygen species, as well as containing lipid-soluble com-pounds such as tocopherols, carotenoids and sterols that mayprotect against the generation of genotoxic lipid peroxidationproducts, such as trans-4-hydroxy-2-nonenal.
Pro-oxidant and pro-inflammatory stimuli induce the mitogen-activated protein and nuclear factor κB inhibitory protein (IκB)kinases that activate nuclear factor κB (NFκB), enabling its translo-cation into the nucleus where it causes activation of cyclo-oxygenase-2 (COX-2) expression, subsequent prostaglandin pro-
duction, and excessive stimulation of cell division that can lead togrowth of adenomas.64-67 The pro-inflammatory and pro-oxidanteffect on increased cell proliferation, combined with oxidative-stress-induced chromosomal instability, increases risk for carcino-genesis (Box 4). The number of herbs with potential anti-inflam-matory activity is impressive. Natural anti-inflammatorycompounds found in herbs and spices (such as curcumin, gingeroland capsaicin) appear to operate by inhibiting one or more of thesteps linking pro-inflammatory stimuli with COX activation, suchas the blocking by curcumin of NFκB translocation into thenucleus. It has been shown recently that the natural anti-inflam-matory compounds quercetin, curcumin and silymarin were aseffective as indomethacin (a non-steroidal anti-inflammatory drug)in inhibiting aberrant crypt foci in the rat.44
Herbs and spices (or their fractions and constituents) withknown anticarcinogenic effects in animal models of cancer includeturmeric, basil, rosemary, mint and lemon grass, but there are nopublished reports on potential chemopreventive effects againstcancer for other common spices such as thyme, coriander and dill.Turmeric has been widely used as a spice and colouring agent infoods. Recently, turmeric was found to have chemopreventiveeffects against cancers of the skin, forestomach, liver and colon,and oral cancer in mice.44-46
Oral treatment with basil-leaf extract significantly elevated theactivities of cytochrome P450, aryl hydrocarbon hydroxylase, andglutathione S-transferase, all of which are important in the detoxi-fication of carcinogens as well as mutagens. Moreover, basil-leafextract was effective in inhibiting carcinogen-induced early-stagecancers in the skin and forestomach of mice.47,68 Orientin andvicenin, two water-soluble flavonoids isolated from the leaves ofIndian holy basil (Ocimum sanctum), have shown significantprotection against radiation-induced lethality and chromosomalaberrations in vivo.48
A methanol extract of the leaves of the plant Rosmarinusofficinalis L. (rosemary) and its constituent carnosol (a phenolicditerpene) inhibited 12-O-tetradecanoylphorbol-13-acetate (TPA)-induced ornithine decarboxylase activity (a promoter of celldivision via polyamine synthesis), TPA-induced inflammation,arachidonic acid-induced inflammation, TPA-induced hyperplasia,and TPA-induced tumour promotion in mouse skin.49 Commer-cially available ground rosemary powder was shown to inhibit in-vivo binding of 7,12-dimethylbenz[a]anthracene (DMBA) metabo-lites to mammary cell DNA in rats,50 suggesting that componentsof rosemary may inhibit breast cancer. In fact, dietary rosemaryand carnosol were both shown to inhibit rat mammary carcinogen-esis when DMBA was used as the carcinogen.51 Using the C57BL/6J/Min/+ (Min/+) mouse, a model of colonic tumorigenesis, it wasfound that dietary administration of 0.1% carnosol decreasedintestinal tumour multiplicity by 46%, potentially via its ability toenhance E-cadherin-mediated adhesion and suppress β-catenintyrosine phosphorylation.69 Carnosol has been shown to inhibitthe invasion of highly metastatic mouse melanoma B 16/F10 cellsin vitro.52 Furthermore, it has been shown to have antioxidantactivity and suppresses nitric oxide production and iNOS geneexpression by inhibiting NFκB activation, which suggests possiblemechanisms for its anti-inflammatory and chemopreventiveaction.53
Geraniol, an acyclic monoterpene alcohol found in lemon grass(Cymbopogon citratus), was shown to inhibit growth and polyaminebiosynthesis in human colon cancer cells.54 Citral (3,7-dimethyl-
2 Total phenolic content of common herbs and spices43
Herb or spice Botanical name
Total phenolic content
(mg of gallic acid/g fresh weight) (Mean ±SEM)
Basil (Sweet) Ocimum basilicum L. 2.23 ± 0.15
Coriander (Vietnamese)
Polygonum odoratum 3.09 ± 0.12
Chives Allium schoenoprasum 1.05 ± 0.05
Dill Anethum graveolens 3.12 ± 0.06
Marjoram (hard sweet)
Origanum x majoricum 11.65 ± 0.29
Oregano (Cuban) Plectranthus amboinicus
0.34 ± 0.00
Oregano (Mexican)
Poliomintha longiflora 17.51 ± 0.22
Parsley Petroselinum crispum 1.12 ± 0.01
Rosemary Rosmarinus officinalis L. 2.19 ± 0.15
Spearmint Mentha spicata 0.94 ± 0.15
Thyme (Lemon) Thymus x citriodorus 1.78 ± 0.03
Garlic Allium sativum L. 1.03 ± 0.10
SEM = standard error of the mean. ◆
S10 MJA • Volume 185 Number 4 • 21 August 2006
SU PPLEMENT3
Sum
mar
y o
f ev
iden
ce f
or
heal
th e
ffec
ts o
f he
rbs
and
sp
ices
on
canc
er
Stud
yD
esig
nTi
ssue
/org
anis
mB
ioac
tive
ag
ent/
so
urce
Do
seM
easu
rem
ent
Out
com
e
Vola
te e
t al
44In
-vitr
o
anim
al
stud
y
Co
lon
of 2
35 m
ale
F344
rats
Que
rcet
in,
curc
umin
, rut
in,
sily
mar
in, w
hole
g
inse
ng m
ixtu
re
50–1
5000
pp
mA
ber
rant
cry
pt
foci
su
pp
ress
ion
and
effe
cts
of t
est
com
po
und
s o
n ev
oki
ng a
po
pto
sis.
Test
co
mp
ound
s si
gni
fican
tly s
upp
ress
ed a
ber
rant
cry
pt
foci
at
diff
eren
t m
ost
effe
ctiv
e co
ncen
trat
ions
. All
test
co
mp
oun
ds
exce
pt
sily
mar
in in
duc
ed a
po
pto
sis,
with
que
rcet
in b
eing
the
m
ost
po
tent
.
Chu
ang
et
al45
In-v
itro
an
imal
st
udy
Die
thyl
nitr
osa
min
e (D
EN)-
ind
uced
live
r in
flam
mat
ion
and
hy
per
pla
sia
in ra
ts
Cur
cum
in
(tur
mer
ic)
200
mg
/kg
or
600
mg
/kg
Onc
ogen
ic a
ctiv
ity b
y im
mun
ob
lott
ing
ana
lysi
sC
urcu
min
str
ong
ly in
hib
ited
DE
N-m
edia
ted
incr
ease
d
exp
ress
ion
of o
ncog
enic
p21
ras a
nd p
53 p
rote
ins
in li
ver t
issu
es
of r
ats,
the
exp
ress
ion
of p
rolif
erat
ing
cel
l nuc
lear
ant
igen
, cy
clin
E a
nd p
34cd
c2, b
ut n
ot C
dk2
or
cycl
in D
1 an
d D
EN-
ind
uced
incr
ease
of t
rans
crip
tiona
l fac
tor N
F κB
. Ho
wev
er,
curc
umin
did
no
t affe
ct D
EN-in
duc
ed c
-Jun
and
c-F
os
exp
ress
ion.
Chu
ang
et
al46
In-v
ivo
an
imal
st
udy
C3H
/HeN
mic
e in
ject
ed w
ith
N-d
ieth
ylni
tro
sam
ine
(DE
N)
Cur
cum
in(t
urm
eric
)0.
2% c
urcu
min
- co
ntai
ning
die
tsIn
term
edia
te b
iolo
gic
al
mar
kers
by
wes
tern
blo
t,
and
inci
den
ce o
f he
pat
oce
llula
r ca
rcin
om
a
81%
red
uctio
n m
ultip
licity
and
62%
red
ucti
on in
inci
den
ce o
f he
pat
oce
llula
r car
cino
ma
wer
e o
bse
rved
. Cur
cum
in-c
ont
aini
ng
die
t als
o re
vers
ed t
he in
crea
se in
leve
ls o
f p21
ras , P
CN
A a
nd
CD
C2
pro
tein
s.
Das
gup
ta
et a
l47In
-viv
o
anim
al
stud
y
Live
r o
f Sw
iss
alb
ino
mic
eB
asil-
leaf
ext
ract
200
and
40
0m
g/k
g
bod
y w
eig
ht
Enz
yme
activ
ities
, lip
id p
erox
idat
ion
Bas
il-le
af e
xtra
ct w
as v
ery
effe
ctiv
e in
ele
vati
ng a
ntio
xid
ant
enzy
me
resp
onse
by
incr
easi
ng s
igni
fican
tly h
epat
ic e
nzym
e ac
tiviti
es. L
ipid
per
oxi
dat
ion
and
lact
ate
deh
ydro
gen
ase
activ
ity w
ere
sig
nific
antly
dec
reas
ed.
Vrin
da
and
U
ma
Dev
i48In
-vitr
o
anim
al
stud
y
Hum
an p
erip
hera
l ly
mp
hocy
tes
Orie
ntin
and
vi
ceni
n (In
dia
n ho
ly
bas
il le
af)
6.25
–20
μmo
les/
LM
icro
nucl
eus
coun
t B
oth
co
mp
oun
ds
show
ed s
igni
fican
t an
tioxi
dan
t ac
tivity
in
vitr
o, a
nd t
here
fore
giv
e si
gni
fican
t p
rote
ctio
n to
hum
an
lym
pho
cyte
s ag
ains
t th
e cl
asto
gen
ic e
ffect
of r
adia
tion
at lo
w,
non-
toxi
c co
ncen
trat
ions
.
Hua
ng e
t al
49In
-viv
o
anim
al
stud
y
Mo
use
skin
Ro
sem
ary
1.2
or 3
.6m
gN
umb
er o
f tum
our
s p
er m
ouse
Num
ber
of t
umo
urs
red
uced
by
at le
ast
50%
in t
he t
reat
men
t g
roup
. Ro
sem
ary
also
inhi
bite
d c
arci
nog
enic
enz
yme
acti
vity
, in
flam
mat
ion,
hyp
erp
lasi
a an
d t
umou
r p
rom
otio
n.
Am
agas
e et
al50
In-v
ivo
an
imal
st
udy
Mam
mar
y ce
ll o
f 55
-day
-old
rat
sR
ose
mar
y ex
trac
t0.
5% a
nd 1
%
in d
iet
DN
A a
dd
ucts
Ro
sem
ary
is e
ffect
ive
in re
duc
ing
the
bin
din
g o
f 7,
12-d
imet
hylb
enz[
a]an
thra
cene
(DM
BA
) met
abo
lites
to
ra
t m
amm
ary
cell
DN
A.
Sing
leta
ry
et a
l51In
-viv
o
anim
al
stud
y
Mam
mar
y ce
ll o
f fe
mal
e ra
tsR
ose
mar
y ex
trac
t an
d c
arno
sol a
nd
urso
lic a
cid
0.5%
in d
iet o
r 20
0m
g/k
gD
NA
ad
duc
tsR
ose
mar
y ex
trac
t an
d c
arno
sol g
roup
s ex
hib
ited
sig
nific
ant
dec
reas
e in
the
in-v
ivo
form
atio
n of
rat
mam
mar
y D
MB
A-D
NA
ad
duc
ts c
om
par
ed w
ith c
ontr
ols.
Car
noso
l is
one
co
nstit
uent
of
rose
mar
y th
at c
an p
reve
nt D
MB
A-i
nduc
ed D
NA
dam
age
and
tu
mou
r fo
rmat
ion
in r
at m
amm
ary
gla
nd.
Hua
ng e
t al
52In
-vitr
o
stud
yB
16/F
10 r
at
mel
anom
a ce
llsC
arno
sol
(rose
mar
y)Va
rious
co
ncen
trat
ions
Ant
imet
asta
tic p
oten
tials
b
y so
ft a
gar
ass
ay,
B16
/F10
rat c
ell m
igra
tion,
m
etal
lop
rote
inas
e ac
tivity
Car
noso
l exh
ibit
ed a
ntim
etas
tatic
po
tent
ial,
do
se
ind
epen
den
tly in
hib
ited
B16
/F10
cel
l mig
ratio
n an
d d
ecre
ased
ac
tivity
of m
etal
lop
rote
inas
e. In
hib
itio
n o
f act
ivat
ion
of
tran
scrip
tion
fact
ors
NF κ
B a
nd c
-Jun
wer
e al
so o
bse
rved
.

MJA • Volume 185 Number 4 • 21 August 2006 S11
HEALTH BENEFITS OF HERBS AN D SPICES: THE PAST, TH E PRESENT, THE FUTURE
Lo e
t al
53In
-vit
ro
stud
yM
ous
e m
acro
pha
ges
Car
noso
l (ro
sem
ary)
Vario
us
conc
entr
atio
nsA
ntio
xid
ant
and
en
zym
e ac
tiviti
esC
arno
sol s
upp
ress
ed th
e ni
tric
oxi
de
pro
duc
tion
and
iNO
S g
ene
exp
ress
ion
by
inhi
biti
ng N
F κB
act
ivat
ion,
and
pro
vid
ed
po
ssib
le m
echa
nism
s fo
r its
ant
i-inf
lam
mat
ory
and
ch
emo
pre
vent
ive
actio
n.
Car
nese
cchi
et
al54
In-v
itro
st
udy
Hum
an c
olo
n ca
ncer
cel
l lin
eG
eran
iol a
nd
othe
r m
ono
terp
enes
400
mol
es/L
Can
cer
cell
gro
wth
, ap
op
tosi
s an
d e
nzym
e ac
tiviti
es
Ger
anio
l cau
sed
a 7
0% in
hib
itio
n o
f cel
l gro
wth
and
co
nco
mita
nt in
hib
itio
n o
f DN
A s
ynth
esis
. No
sig
ns o
f cy
toto
xici
ty o
r ap
op
tosi
s w
ere
det
ecte
d. A
50%
dec
reas
e in
en
zym
es w
hich
enh
ance
can
cer
gro
wth
was
als
o o
bse
rved
.
Nak
amur
a et
al55
In-v
itro
st
udy
No
rmal
rat
live
r ep
ithel
ial c
ell l
ine,
R
L34
cells
Citr
al
(lem
on g
rass
)Va
rious
co
ncen
trat
ions
GST
(g
luta
thio
ne S
-tra
nsfe
rase
) ac
tivity
Ele
ctro
phi
lic p
rop
erty
cha
ract
eris
ed b
y th
e re
activ
ity w
ith
intr
acel
lula
r nu
cleo
phi
les
incl
udin
g p
rote
in t
hio
l or g
luta
thio
ne
pla
ys a
n im
po
rtan
t ro
le in
the
ind
uctio
n o
f GST
.
Puat
anac
hokc
hai
et a
l56In
-viv
o an
d
in-v
itro
st
udy
Mal
e F3
44 ra
tsLe
mo
n g
rass
ex
trac
tD
ieta
ry
conc
entr
atio
ns
of 0
, 0.2
%, 0
.6%
o
r 1.
8%
8-hy
dro
xyd
eoxy
gua
nosi
ne
pro
duc
tion
Inhi
bito
ry e
ffect
s o
f lem
on
gra
ss e
xtra
ct h
app
ened
on
the
early
p
hase
hep
ato
carc
ino
gen
esis
in r
ats.
Suae
yun
et a
l57In
-viv
o
anim
al
stud
y
F344
rats
Eth
ano
l ext
ract
of
lem
on
gra
ss0.
5 or
5g
/kg
b
ody
wei
ght
DN
A a
dd
ucts
and
ab
erra
nt
cryp
t fo
ci a
naly
sis
Lem
on
gra
ss t
reat
men
t si
gni
fican
tly in
hib
ited
DN
A a
dd
uct
form
atio
n in
bot
h th
e co
loni
c m
uco
sa a
nd m
uscu
lar
laye
r, b
ut
not
in t
he li
ver.
Lem
on g
rass
ext
ract
als
o ex
hib
ited
ant
ioxi
dan
t ac
tivity
.
Lant
ry e
t al
58In
-viv
o
anim
al
stud
y
(C3H
/HeJ
X A
/J)
F1 h
ybrid
mic
e Pe
rilly
l alc
oho
lVa
rious
do
ses
Max
imum
tol
erat
ed d
ose
o
f per
illyl
alc
oho
l, tu
mo
ur in
cid
ence
, tu
mo
ur m
ultip
licity
Max
imum
to
lera
ted
do
se w
as 7
5m
g/k
g b
od
y w
eig
ht; 2
2%
red
uctio
n in
tum
our
inci
den
ce a
nd 5
8% re
duc
tion
in t
umou
r m
ultip
licity
wer
e d
emo
nstr
ated
.
Yu e
t al
59In
-vit
ro
bac
teria
l m
utag
enic
ity
stud
y
Salm
onel
la
typ
him
uriu
m s
trai
n TA
98
Wat
er e
xtra
ct o
f sp
earm
int
5%
(wei
ght
/vol
ume)
Act
ivity
ag
ains
t m
utag
ens
NPD
(4-n
itro
-1,2
-p
heny
lene
dia
min
e) a
nd
N-O
H-I
Q (2
-hyd
roxy
amin
o-
3-m
ethy
l-3H
-imid
azo[
4,5-
f]-
qui
nolin
e)
No
n-to
xic
conc
entr
atio
ns in
hib
ited
mut
agen
ic a
ctiv
ity
of
N-O
H-IQ
in a
co
ncen
trat
ion-
dep
end
ent
fash
ion
but
had
no
effe
ct a
gai
nst
NPD
. Chl
oro
form
and
met
hano
l ext
ract
s of
sp
earm
int
also
po
sses
sed
ant
imut
agen
ic a
ctiv
ity a
gai
nst
N-O
H-IQ
.
Yu e
t al
59In
-viv
o
anim
al
stud
y
F344
rats
Wat
er e
xtra
ct o
f sp
earm
int
2% (w
eig
ht/
volu
me)
as
the
sole
so
urce
of
drin
king
flui
d
bef
ore
, dur
ing
, an
d a
fter
2-w
eek
trea
tmen
t w
ith
IQ (2
-am
ino
-3-
met
hylim
idaz
o-
(4,5
-f)q
uino
line,
a ca
rcin
og
en in
co
oke
d m
eat)
.
Red
uctio
n in
ab
erra
nt c
ryp
t fo
ci in
col
on
(a c
olo
n ad
eno
ma
mod
el)
Col
oni
c ab
erra
nt c
ryp
t fo
ci in
the
rats
giv
en s
pea
rmin
t wat
er
extr
act a
nd IQ
wer
e in
hib
ited
sig
nific
antly
at
8 w
eeks
(P<
0.05
) co
mp
ared
with
rats
giv
en IQ
alo
ne.
Zhen
g e
t al
60In
-viv
o
anim
al
stud
y
Mou
se ta
rget
tis
sue
Myr
istic
in(p
arsl
ey, n
utm
eg)
2.5–
20m
gA
bili
ty t
o in
duc
e in
crea
sed
ac
tivit
y of
the
det
oxi
fyin
g
enzy
me
syst
em.
Myr
istic
in s
how
ed h
igh
activ
ity a
s a
glu
tath
ione
S-t
rans
fera
se
ind
ucer
in t
he li
ver
and
sm
all i
ntes
tinal
muc
osa
.
Ahm
ad e
t al
61In
-viv
o
anim
al
stud
y
Mo
use
liver
Myr
istic
in(p
arsl
ey, n
utm
eg)
5–50
mg
Mec
hani
sm o
f ind
uctio
n o
f GST
Myr
istic
in in
crea
sed
GST
act
ivity
by
4–14
-fo
ld o
ver c
ont
rol
tissu
e. T
reat
men
t ca
used
a s
light
cha
nge
in t
he G
ST- π
leve
ls
whi
le t
he le
vels
of G
ST- α
sho
wed
a m
od
est
incr
ease
.

S12 MJA • Volume 185 Number 4 • 21 August 2006
SU PPLEMENT
2,6-octadienal), isolated from the methanol extract of lemon grass,was identified as a novel inducer of the phase-2 enzyme glutath-ione S-transferase.55 Lemon grass extract reduced the number ofputatively preneoplastic lesions and the level of oxidative hepato-cyte nuclear DNA injury, as assessed in terms of 8-hydroxydeoxy-guanosine production in the liver of male Fischer 344 rats.56
Inhibitory effects of lemon grass extract on the formation ofazoxymethane-induced DNA adducts and aberrant crypt foci (apreneoplastic lesion) were recently demonstrated in the ratcolon.57
Perillyl alcohol, a naturally occurring monoterpene found inlavender, cherries and mint, caused a 22% reduction in tumourincidence and a 58% reduction in tumour multiplicity in a mouselung tumour bioassay.58 Rats given spearmint water extract (2%weight/volume) as the sole source of drinking fluid before, during,and after 2-week treatment with a colon carcinogen derived fromcooked meat, showed significant reductions in colonic aberrantcrypt foci compared with rats given water only.59
As a culinary herb, parsley is regularly consumed and parsley-leaf oil is also used extensively for garnishing and seasoning.Myristicin, a major volatile aroma constituent of parsley, showedhigh activity as an inducer of the phase 2 enzyme glutathione S-transferase in the liver and small intestinal mucosa of strain A/Jalbino mice,60,61,70 and a 65% inhibition of tumour multiplicity ina rodent lung cancer model.70
The results of studies cited above indicate the potential forherbs and spices in chemoprevention of cancer in vitro and inrodent cancer models. However, there is as yet no reliableevidence for beneficial effects in humans in vivo at customaryintake levels. There is clearly a need for placebo-controlledclinical trials to determine safety and optimal dosage, bioavail-
ability and bioefficacy of herbs and spices and their componentsas chemopreventive agents against the various stages of cancerdirectly in humans.
Summary• There is potential for herbs and spices in chemoprevention ofcancer in vitro and in rodent cancer models.• There is as yet no reliable evidence for beneficial effects inhumans in vivo at customary intake levels.
Mental health and cognitionSteven Roodenrys
There is a very long history in traditional medicine of the use ofplants to influence psychological states and processes as well asphysical health. In particular, the traditional practices of Ayurvedicmedicine in India and Chinese medicine have included treatmentsfor psychological conditions such as anxiety, and preparations toenhance cognitive processes such as memory and attention. Recentdecades have seen an increased use of herbal preparations for bothof these purposes in Western society despite relatively littlescientific research having been conducted to investigate theirefficacy.
The herbs that have received the most scientific attention inregard to influencing psychological processes have been drawnfrom the traditional medicines rather than the culinary herbs. Asearch of MEDLINE and PsycINFO using the various herb names(eg, basil, coriander) and the terms cognition, memory, attention,dementia and anxiety found only one study of the effect of any ofthese herbs on psychological processes — it investigated thehypnotic and anxiolytic effects of lemon grass. In this placebo-controlled, double-blind study, lemon grass was taken as a herbaltea for 2 weeks; no effects were found.71
The use of herbal treatments for anxiety is probably the mostcommon example of a herbal influence on mental health. Passifloraincarnata, or passionflower, is approved for use as a sedative by theGerman Commission E (an expert committee commissioned bythe German Government in 1978 to evaluate herbal drugs andpreparations from medicinal plants). Valeriana officinalis, or vale-rian, is probably one of the most widely available herbal treat-ments, and has been shown to have sedative effects in humans. Areview of evidence for behavioural effects and possible chemicalpathways for their action concludes that compounds in valerianinteract with GABA systems (widespread systems affected by γ -amino butyric acid) in the brain; however, despite identifyingflavonoids in passionflower as the likely agent, they do not appearto act on GABA receptors.72
More recently, herbs drawn from traditional Chinese medicine,such as Ginkgo biloba and ginseng, have been advocated for areputed beneficial effect on cognitive processes.73 There is level Ievidence to support the claim that ginkgo can amelioratecognitive decline in dementia1,74 and level II evidence that it canimprove some aspects of memory function in healthy adults.1,75
Further, an extract from ginkgo has been shown to affect cerebralcirculation, activity in the cholinergic system, and to haveantioxidant properties, all of which may contribute to effects oncognitive function (Box 5).81 However, a population-based study
4 Effect of pro-inflammatory stimuli on chromosomal instability and increased cell proliferation which, in combination, increase the risk of carcinogenesis.
Denotes steps in this carcinogenic process that may be inhibited by certain constituents of herbs and spices. ◆
Increased oxidative stress
DNA oxidationBreaks in chromosomes
Telomere shortening
Chromosomalinstability
Mitogen-activated protein kinases
Nuclear factor κB activation
Increased cyclo-oxygenase-2
expression
Increased cell proliferation
Pro-inflammatory stimuli
Increased cancer risk

MJA • Volume 185 Number 4 • 21 August 2006 S13
HEALTH BENEFITS OF HERBS AN D SPICES: THE PAST, TH E PRESENT, THE FUTURE
failed to find an effect on the recall ofnewly learned information after a shortdelay and the efficiency of workingmemory processes after a 30-day inter-vention.75
Consuming herbs can be expected tobenefit cognitive function to the extentthat they benefit cerebral circulation.For example, it has been shown thatpeople with hypertension performmore poorly on a range of cognitivetasks,82 and cardiovascular disease isassociated with impaired cognition.83
Dietary factors that promote cardiovas-cular health will therefore also maintaincognitive function, although the effectof any single foodstuff is likely to besmall.
Perhaps more importantly, antioxi-dant intake is related to cognitive func-tion because it protects againstneuronal degeneration. A review ofstudies of the effects of antioxidants onAlzheimer’s disease shows quite mixedresults; this is attributed to the factthat most studies involve participantswho have already been diagnosed withdementia, while epidemiological stud-ies suggest that the most likely benefitof antioxidants is in preventingdementia.76 Some epidemiologicalstudies have shown a relationshipbetween plasma levels of antioxidantsand dementia and cognitive impair-ment.84 At this point in time, theevidence suggests that total antioxi-dant intake may influence cognitivedecline with age through the neuro-protective action of antioxidants.
Summary• There is little evidence that culinaryherbs and spices directly influence cog-nition.• There is level I and II evidence forthe effect of some herbal supplementson psychological and cognitive func-tion.• Total antioxidant intake (to whichherbs and spices contribute) may influ-ence cognitive decline with age throughthe neuroprotective action of antioxi-dants.• Randomised, placebo-controlled in-tervention studies of the effects of culi-nary herbs and herbal supplements arerequired.5
Sum
mar
y o
f ev
iden
ce f
or
heal
th e
ffe
cts
of
herb
s an
d s
pic
es o
n c
og
nit
ive
func
tio
n a
nd m
enta
l hea
lth
Stud
yD
esig
nTi
ssue
/org
anis
m/
par
tici
pan
tsB
ioac
tive
ag
ent/
so
urce
Do
seM
easu
rem
ent
Out
com
e
Car
lini72
Revi
ew a
rtic
le
In-v
itro
stu
dy
Pass
iflor
a in
carn
ata
(pas
sion
flow
er)
extr
act
Not
m
entio
ned
Sed
ativ
e an
d
anxi
oly
tic e
ffect
sFl
avo
noid
s ap
pea
red
to b
e re
spon
sib
le fo
r the
an
xiol
ytic
and
sed
ativ
e ef
fect
s. F
ind
ing
s o
n th
e m
echa
nism
s o
f act
ion
wer
e m
ixed
.
Fran
k an
d G
upta
76Re
view
art
icle
Mo
use
hip
po
cam
pal
cel
l m
odel
of o
xid
ativ
e st
ress
Rat m
od
el o
f acu
te a
nd
chro
nic
stre
ss
Ag
ed g
arlic
ex
trac
t N
ot
men
tione
dA
ntio
xid
ativ
ean
d
stre
ss le
vel
effe
cts
Flav
ono
ids
in a
ged
gar
lic e
xtra
ct p
rote
cted
p
rimar
y ne
uro
ns fr
om
glu
tam
ate
toxi
city
and
ox
idat
ive
inju
ries.
Ani
mal
mo
del
of
Alz
heim
er’s
dis
ease
Cur
cum
in fr
om
gin
ger
or
turm
eric
Not
m
entio
ned
Pro
tect
ion
agai
nst
dam
age
ind
uced
by
amyl
oid
β-p
rote
in
Sup
erio
r re
sults
wer
e o
bta
ined
with
cur
cum
in
(co
mp
ared
with
ibup
rofe
n).
In-v
itro
stu
dy
Feru
lic a
cid
N
ot
men
tione
dA
ntio
xid
ativ
eef
fect
sFe
rulic
aci
d, b
eing
a p
ote
nt a
ntio
xid
ant,
in
hib
ited
lip
id p
ero
xid
atio
n.
In-v
itro
stu
dy
Poly
phe
nolic
co
mp
oun
ds
Not
m
entio
ned
Cyt
oto
xici
ty, a
po
pto
tic
feat
ures
and
an
ti-o
xid
ativ
e ac
tivity
Form
atio
n o
f fA
bet
a ( β
-am
ylo
id fi
bril
s) w
as
inhi
bite
d a
nd p
refo
rmed
fAb
eta
was
d
esta
bili
sed
in a
do
se-d
epen
den
t m
anne
r.
Eid
i et a
l77A
nim
al s
tud
y19
0 m
ale
Wis
tar r
ats
Etha
nolic
sa
ge-
leaf
ext
ract
3.5
gsi
ngle
do
seLo
ng-t
erm
mem
ory
re
tent
ion
test
Eth
ano
lic e
xtra
ct in
crea
sed
mem
ory
rete
ntio
n.
Akh
ond
zad
eh e
t al
784-
wee
k d
oub
le-b
lind
, ra
ndo
mis
ed t
rial
36 o
utp
atie
nts
with
g
ener
alis
ed a
nxie
ty
dis
ord
er
Pass
ionf
low
er
extr
act
45 d
rop
s p
er d
ay
Ham
ilto
n A
nxie
ty
Rat
ing
Sca
lePa
ssio
nflo
wer
ext
ract
is e
ffect
ive
for m
anag
ing
g
ener
alis
ed a
nxie
ty d
iso
rder
.
Akh
ond
zad
eh e
t al
794-
mon
th d
oub
le-
blin
d, r
and
om
ised
, p
lace
bo-
cont
rolle
d t
rial
42 p
atie
nts
with
m
ild t
o m
oder
ate
Alz
heim
er’s
dis
ease
Sag
e ex
trac
t60
dro
ps
per
day
Cha
nges
in t
he
Alz
heim
er’s
Dis
ease
A
sses
smen
t Sc
ale
and
C
linic
al D
emen
tia R
atin
g
Sag
e ex
trac
t pro
duc
ed a
sig
nific
antly
bet
ter
cog
nitiv
e fu
nctio
n o
utco
me
than
pla
ceb
o.
Rah
man
80Re
view
art
icle
No
t rev
eale
dVa
rious
com
po
und
s d
eriv
ed fr
om g
arlic
Not
m
entio
ned
Cer
ebra
l fu
nctio
nTh
e ro
le o
f gar
lic in
pre
vent
ing
cer
ebra
l ag
eing
thro
ugh
its a
ntio
xid
atio
n p
rop
ertie
s is
su
pp
ort
ed b
y a
few
stu
die
s.

S14 MJA • Volume 185 Number 4 • 21 August 2006
SU PPLEMENT
Type 2 diabetes mellitusJennifer B Keogh and Peter M Clifton
The biguanide drug metformin, a popularfirst-line treatment for diabetes, was devel-oped from French lilac (Galega officinalis). Todate, this is the only plant-derived treatmentfor diabetes. At present, the best clinicalevidence available for culinary herbs andspices in the treatment of diabetes is forcinnamon, and that is not very convincing.Early in-vitro studies of spices such as cinna-mon, cloves, bay leaves and turmeric haveshown that they display insulin-enhancingactivity.85,86 Mechanistic studies suggest thatextracts of cinnamon increase in-vitro glu-cose uptake and glycogen synthesis andincrease insulin-receptor phosphoryla-tion.87-89 A recent study tested the hypothe-sis that cinnamon would lead to improvedglucose tolerance in people with type 2diabetes mellitus.89 Sixty men and womenwere randomly assigned to one of sixgroups. The first three groups were given 1,3 or 6 g of cinnamon (Cinnamomum cassiaextract in capsules) or placebo (samenumber of capsules). After 40 days, all threedoses of cinnamon improved fasting glucoselevels (by 18%–29%; P < 0.05).89 However,20 days later, glucose levels were still lowerwith the lowest dose only, so it is not clear ifany of the effects were due to the spice. Inaddition, glycated haemoglobin (HbA1c) lev-els were not measured. It is not clear fromthis study whether less than 1 g of cinnamonper day would also be beneficial, and this isan important question given that an intakeof more than 1 g of cinnamon daily wouldrequire supplementation. Triglyceride andLDL cholesterol levels were also lowered bycinnamon, and this again persisted 20 daysafter cessation of the spice in the two lowestdoses, suggesting that a reduction in energyand fat intake had occurred in this group,and this would account for the effects onglucose. A second, double-blind randomisedcrossover study of 29 postmenopausalwomen with type 2 diabetes published thisyear showed that 1.5 g of cinnamon dailyhad no effect on whole-body insulin sensi-tivity or oral glucose tolerance, and lipidlevels were also unchanged. In conclusion,the effect of cinnamon is still unproven.90
There are many examples of non-culinaryherbs that have been tested for their effectson blood glucose, but many of the data arevery poor. The 10 most popular plant prepa-rations prescribed by herbalists in Italy forglucose control are gymnema, psyllium,fenugreek, bilberry, garlic, Chinese ginseng,
6Su
mm
ary
of
evid
ence
fo
r he
alth
eff
ect
s o
f he
rbs
and
sp
ices
on
typ
e 2
dia
bet
es
Stud
yD
esig
nPa
rtic
ipan
tsB
ioac
tive
ag
ent/
so
urce
Do
seM
easu
rem
ent
Out
com
e
Vuks
an e
t al94
Ran
do
mis
ed,
pla
ceb
o-co
ntro
lled
, cr
oss
ove
r tr
ial
19; 1
0 w
itho
ut d
iab
etes
an
d 9
wit
h ty
pe
2 d
iab
etes
Gin
seng
or
pla
ceb
o
3g
Are
a un
der
cur
ve o
f b
lood
sam
ple
s b
efor
e an
d a
t 15
, 30,
45,
60,
90
and
120
min
utes
af
ter
glu
cose
cha
lleng
e
Are
a un
der
cur
ve re
duc
ed b
y 18
%±3
1%
(mea
n±S
D) i
n th
ose
with
out
dia
bet
es w
hen
gin
seng
was
tak
en 4
0 m
inut
es b
efor
e g
luco
se. A
rea
und
er c
urve
red
uced
by
19%
±22%
and
22%
±17%
in th
ose
wit
h ty
pe
2 d
iab
etes
whe
n ta
ken
with
or
bef
ore
glu
cose
, res
pec
tivel
y.
Vuks
an e
t al95
Mul
tiple
occ
asio
ns,
rand
om
ised
, p
lace
bo
-co
ntro
lled
tr
ial
10 w
itho
ut d
iab
etes
Am
eric
an g
inse
ng
or
pla
ceb
o3,
6 o
r 9
g o
f gro
und
g
inse
ng ro
ot p
owd
erA
rea
und
er c
urve
o
f cap
illar
y b
lood
g
luco
se le
vels
bef
ore
an
d a
t 0,
15,
30,
45,
60
and
90
min
utes
aft
er
glu
cose
cha
lleng
e
All
thre
e d
ose
s o
f Am
eric
an g
inse
ng
red
uced
glu
cose
leve
ls a
t 30
, 45
and
60
min
utes
; 3 a
nd 9
g r
educ
ed g
luco
se le
vels
at
90
min
utes
(P<
0.05
). A
t 60
min
utes
, 9g
o
f Am
eric
an g
inse
ng re
duc
ed g
luco
se
leve
ls m
ore
tha
n 3
g (P
<0.
05).
All
do
ses
red
uced
are
a un
der
cur
ve (3
g, 2
6.6%
; 6g
, 29
.3%
; 9g
, 38.
5%; P
<0.
05).
Sota
niem
i et a
l96D
oub
le-b
lind
, p
lace
bo
-co
ntro
lled
tr
ial
36 w
ith t
ype
2 d
iab
etes
Gin
seng
100
mg
and
200
mg
Fast
ing
blo
od
glu
cose
le
vel,
gly
cate
d
haem
og
lob
in (H
bA
1c)
leve
l, b
od
y w
eig
ht
Gin
seng
red
uced
fast
ing
blo
od g
luco
se
and
Hb
A1c
leve
ls a
nd b
od
y w
eig
ht.
Plac
ebo
als
o re
duc
ed b
od
y w
eig
ht, b
ut d
id
not
alte
r fas
ting
blo
od g
luco
se le
vels
.
Vuks
an e
t al97
Ran
do
mis
ed,
pla
ceb
o-co
ntro
lled
, cr
oss
ove
r tr
ial
12 w
itho
ut d
iab
etes
Am
eric
an g
inse
ng0,
1, 2
and
3g
A
rea
und
er c
urve
o
f cap
illar
y b
lood
g
luco
se le
vels
bef
ore
an
d a
t 0,
15,
30,
45,
60
and
90
min
utes
aft
er
glu
cose
cha
lleng
e
Glu
cose
leve
ls re
duc
ed o
ver
the
last
45
min
utes
of t
he t
est a
fter
1, 2
and
3g
of
gin
seng
co
mp
ared
with
pla
ceb
o (P
<0.
05);
no d
iffer
ence
s w
ere
foun
d b
etw
een
do
ses.
In
the
last
60
min
utes
, glu
cose
and
are
a un
der
cur
ve w
ere
low
er w
hen
gin
seng
was
ta
ken
40 m
inut
es b
efo
re g
luco
se c
halle
nge
than
whe
n ta
ken
at 2
0, 1
0 o
r 0
min
utes
b
efo
re (P
<0.
05).

MJA • Volume 185 Number 4 • 21 August 2006 S15
HEALTH BENEFITS OF HERBS AN D SPICES: THE PAST, TH E PRESENT, THE FUTURE
dandelion, burdock, prickly pear cactus and bitter melon.91
Although there is also some evidence for the clinical efficacy ofginseng in managing diabetes, there are concerns about thereproducibility of its effect based on batch, dose and time of takingthe herb.92 A 2004 study reported differences in glycaemic effectaccording to the type of ginseng tested, suggesting that theantihyperglycaemic effect of ginseng can be highly variable.93 Arandomised clinical trial in 2000 evaluated ginseng in 19 leanpeople; 10 without, and 9 with diabetes (Box 6).94 They received3 g of ginseng or placebo 40 minutes before, or with, 25 g ofglucose. Participants (both with and without diabetes) takingginseng 40 minutes before the glucose showed a significantreduction in glucose level compared with those taking placebo(P < 0.05). There were also reductions in the area under theglycaemic curve for both those with and without diabetes mellitus.In a further study, 10 people without diabetes received, in randomorder on 12 occasions, 0, 3, 6 or 9 g of ginseng at 40, 80, or 120minutes before 25 g of glucose. Ginseng reduced postprandialglucose levels (P < 0.05), and 9 g had a slightly greater effect than3 g.95
Only one study has reported the effect of ginseng ingestion onHbA1c. A 1995 report investigated the effect of ginseng in peoplenewly diagnosed with type 2 diabetes mellitus.96 Over 8 weeks, 36participants were randomly assigned to receive either ginseng(100 mg or 200 mg) or placebo. Overall, ginseng reduced fastingblood glucose levels and body weight, and the group taking200 mg of ginseng also showed reduced HbA1c levels. Theseresults suggest that ginseng may have a delaying effect on gastricemptying, although a sulfonylurea-like activity may also play apart.96 In conclusion, evidence supporting the efficacy of non-culinary herbal treatments is limited and, at present, the bestevidence for clinical efficacy is for ginseng.
Summary
• Studies of herbal treatments in diabetes are often very small,and extrapolating the results to the general population of peoplewith diabetes is not appropriate.• The best evidence for effect on glycaemia is for ginseng (fourstudies, with one reasonable sized study showing a reduced HbA1clevel with 200 mg of ginseng).• Longer, larger randomised trials with acceptable clinical end-points are needed to clarify the chronic effects of these herbs.
Osteoarthritis and inflammatory responseCraig S Patch
The role that diet plays in minimising the negative effects of ageinghas been extensively investigated. Target health issues related tothe ageing process include the process of oxidation, the promotionof bone health, memory retention and cognition. With respect toculinary herbs and spices, the best evidence is associated with anti-inflammatory effect, particularly in mediating osteoarthritic painreduction.
Therapy for osteoarthritis is directed at symptoms, as there is noestablished disease-altering treatment. Currently, treatment
options are confined to pharmacological interventions such asanalgesia, anti-inflammatory and intra-articular regimens.98 How-ever, the recent withdrawal of cyclo-oxygenase inhibitors has ledmany consumers to herbal remedies such as ginger. What followsis a review of the evidence for efficacy of ginger in treatingsymptomatic osteoarthritis.
Ginger (family Zingiberaceae) is a mixture of over severalhundred known constituents, including gingerols, β-carotene,capsaicin, caffeic acid, curcumin and salicylate.99 Animal modelshave been used for in-vitro and in-vivo testing of formulations andpowders of ginger, and have shown that it acts as a duel inhibitorof both cyclo-oxygenase and lipo-oxygenase,100 as well as being aninhibitor of leukotriene synthesis.101 Three trials have tested theeffects of ginger extract on pain. A randomised, placebo-controlledcrossover study of 46 patients with knee pain showed that gingerhad no effect. It was suggested that there may have been a carry-over effect of the ginger extract which blurred the results, asexplorative statistics before the crossover suggested a positiveeffect.102 However, in subsequent studies, ginger extract was foundto have a statistically significant effect in reducing knee pain, butthe effect was only moderate.103-105 An interesting recent trial of aproprietary combination of iso-α-acids from hops, rosemaryextract and oleanolic acid (440 mg/day for 8 weeks) suggested abeneficial effect on pain in patients with arthritis.106 Althoughthese findings seem promising, there is much more to be done inthis area. The relative effectiveness of different extracts isunknown, and there are methodological limitations in measuringthis. More clinical studies are needed to confirm these results,considering the confounding effects of the total diet.
A few studies, mostly randomised controlled trials, investigatingthe effect of ginger on osteoarthritis and rheumatoid arthritis havebeen identified (Box 7).102-104,107,109 Various doses of gingerextract, ranging from 510 mg to 1 g per day, were tested. Pain levelwas assessed by various validated measures of pain, such as visualanalogue scales, Western Ontario and McMaster Universities(WOMAC) osteoarthritis index total score, and SF-12 HealthSurvey. These trials found that the pain level of the participants inthe intervention group was significantly lower than that in theplacebo group, and suggests level II evidence1 for the efficacy ofginger in this setting (P < 0.05). In addition, decreased use of non-steroidal anti-inflammatory drugs and analgesics was alsoobserved. However, this improvement was modest103 and theefficacy of ginger treatment was ranked below that of ibuprofen.102
Experimental studies have shown that ginger inhibits theinflammation process. Ginger constituents are duel inhibitors ofarachidonic-acid metabolism (a key pathway in inflammation).110
Similar anti-inflammatory activity shown with turmeric (a memberof the ginger family) is also suggestive of a potential healthbenefit.111 In addition, epidemiological studies have indicated thatpopulations that consume foods rich in specific polyphenols (suchas ginger) have lower incidences of inflammatory disease.112
Many questions remain to be answered about the effects ofantioxidants and the inflammatory process. Future interventionstudies should include a detailed assessment of the bioavailabilityof antioxidants in addition to polyphenols. Beyond clinical trialscarried out with antioxidant-rich foods such as ginger, morestudies with pure, isolated compounds will also be needed toestablish their role in inflammatory diseases.

S16 MJA • Volume 185 Number 4 • 21 August 2006
SU PPLEMENT
Summary• Various doses of ginger extract, rangingfrom 510 mg to 1 g per day, reduce subjectivearthritic knee pain measures compared withplacebo (P < 0.05).• Decreased use of non-steroidal anti-inflam-matory drugs and analgesics has been observedin study participants taking ginger extract.• There is level II evidence for the use ofginger in ameliorating arthritic knee pain; how-ever, this improvement is modest, and theefficacy of ginger treatment is ranked belowthat of the ibuprofen prescribed to the partici-pants.
7Su
mm
ary
of
evi
de
nce
fo
r he
alth
eff
ects
of
herb
s an
d s
pic
es o
n ar
thri
tis
Stud
yD
esig
nPa
rtic
ipan
ts/o
rgan
ism
s/
tiss
ueB
ioac
tive
ag
ent/
sour
ceD
ose
Mea
sure
men
tO
utco
me
Wig
ler
et a
l104
6-m
ont
h ra
ndo
mis
ed,
dou
ble
-blin
d,
cont
rolle
d, c
ross
ove
r st
udy
29 p
atie
nts
with
sy
mp
tom
atic
go
nart
hriti
s
Gin
ger
ext
ract
v p
lace
bo
1g
/day
(2
50m
g c
apsu
le
four
tim
es d
aily
)
Pain
on
mo
vem
ent
and
of h
and
icap
(V
AS
of p
ain)
Sig
nific
antly
low
er p
ain
leve
l was
fo
und
in t
he g
ing
er g
roup
. No
sig
nific
ant
diff
eren
ce w
as fo
und
b
etw
een
gro
ups
at c
ross
ove
r.
Blid
dal
et
al10
2Ra
ndom
ised
, p
lace
bo
-con
trol
led
, cr
oss
ove
r st
udy
56 p
artic
ipan
tsw
ith
ost
eoar
thrit
is
Chi
nese
gin
ger
ext
ract
(E
V.E
XT3
3) c
apsu
le
v ib
upro
fen
v p
lace
bo
170
mg
gin
ger
ext
ract
th
ree
times
dai
ly;
400
mg
ibup
rofe
nd
aily
Pain
ass
essm
ent
(VA
S of
pai
n —
Fr
ied
man
tes
t)
Effi
cacy
of t
reat
men
t ran
ked
ib
upro
fen
abo
ve g
ing
er a
nd
gin
ger
ab
ove
pla
ceb
o. N
o
sig
nific
ant
diff
eren
ce w
as fo
und
b
etw
een
ibup
rofe
n an
d g
ing
er
dur
ing
cro
sso
ver.
Altm
an a
nd
Mar
cuss
en10
36-
wee
k ra
ndo
mis
ed,
dou
ble
-blin
d, p
lace
bo
-co
ntro
lled
, mul
tice
ntre
, p
aral
lel-g
roup
stu
dy
247
pat
ient
s w
ith
oste
oar
thrit
is o
f the
kne
e an
dm
od
erat
e-to
-sev
ere
pai
n
Gin
ger
ext
ract
(EV.
EXT7
7)
cap
sule
255
mg
twic
e d
aily
Red
uctio
n in
“kn
ee
pai
n on
sta
ndin
g”
(VA
S o
f pai
n)
Sig
nific
ant
but
mo
des
t im
pro
vem
ent
was
foun
d in
th
e g
ing
er e
xtra
ct g
roup
.
Soha
il et
al10
78-
wee
k ra
ndo
mis
ed,
mul
ticen
tre
clin
ical
tria
l65
pat
ient
s w
ith
ost
eoar
thrit
is
and
rh
eum
ato
id a
rthr
itis
Stin
gin
g n
ettle
ext
ract
Dev
il’s
claw
ext
ract
Gin
ger
root
ext
ract
(as
atris
in c
apsu
le)
300
mg
200
mg
20m
g
(all
twic
e d
aily
)
Ass
essm
ent
of p
ain
and
func
tiona
l d
isab
ility
(V
AS
of p
ain)
Imp
rove
men
ts in
all
effic
acy
par
amet
ers
wer
e o
bse
rved
. Le
ss N
SAID
and
ana
lges
ic
med
icat
ions
wer
e us
ed b
y p
arti
cip
ants
.
Muh
lbau
er e
t al
108
In-v
ivo
ani
mal
stu
dy
11 W
ista
r Han
lbm
rat
sPo
wd
ered
sag
e,
rose
mar
y an
d t
hym
e1
gU
rinar
y ex
cret
ion
of [
3 H]-
tetr
acyc
line
Bo
ne re
sorp
tion
was
sig
nific
antly
re
duc
ed/i
nhib
ited
.
Ess
entia
l oil
extr
acte
d
fro
m s
age
and
ros
emar
yVa
rious
Urin
ary
excr
etio
n o
f [3 H
]-te
trac
yclin
eSi
gni
fican
t in
hib
itio
n o
f b
one
reso
rptio
n.
In-v
itro
ani
mal
stu
dy
Ost
eocl
asts
fro
m
Wis
tar
Han
lbm
rat
sM
ono
terp
enes
(bo
rneo
l, th
ymo
l and
cam
pho
r)1.
0m
mo
l/L
Bon
e re
sorp
tive
ac
tiviti
esD
irect
inhi
biti
on
of t
he
oste
ocl
ast r
esor
ptio
n p
it as
say.
EV.E
XT3
3 an
d E
V.EX
T77
are
pat
ente
d s
tand
ard
ised
gin
ger e
xtra
cts.
VA
S=
visu
al a
nalo
gue
sca
le. N
SAID
=no
n-st
ero
idal
ant
i-inf
lam
mat
ory
dru
g.
◆

MJA • Volume 185 Number 4 • 21 August 2006 S17
HEALTH BENEFITS OF HERBS AN D SPICES: THE PAST, TH E PRESENT, THE FUTURE
Public health
Peter G Williams
It is difficult to estimate the current level of consumption ofculinary herbs and spices by Australians. The Australian Bureauof Statistics trend data on apparent consumption of foods do notinclude herbs and spices,113 and results from the last NationalNutrition Survey (NNS) in 1995 provide only limited informa-tion on consumption — that median daily intake of herbs,spices, seasonings and stock cubes combined was estimated to be1.4 g per adult (declining with age from 4.2 g in 19–24-year-olds,to 0.7 g in those aged 65 years and older), with only 3.1% ofpeople reported consuming this category of food items on theday of survey.114 The separate intakes of herbs and spices aloneare not reported. Intake by males appeared to be higher than thatby females, but the low values make it difficult to assess thesignificance of this difference. In New Zealand, the consumptionof spices, estimated using import data, was 364 g per year, oraround 1g per day,115 a similar value to that reported in the NNS.
One comparison of spices used in representative vegetable-based and meat-based recipes from 36 different countries foundAustralia (with a mean of 3.4 spices per recipe) had a moderatelevel of use compared with the international mean of 3.9(ranging from 1.6 in Norway to 6.9 in Indonesia).116 However,increased use of herbs and spices as flavourings in foods is amajor trend worldwide,117 with sales growth of 20%–30% overthe past 5 years in both the United Kingdom and the UnitedStates.118 It has been suggested that this trend is partly driven bydemographics; as consumers age, their palates can become moreadventurous. Promotion can also be important — a recent UKadvertisement in which Jamie Oliver encouraged consumers toexperiment with nutmeg boosted sales of that spice fourfold.119
Based on retail sales data, consumption of herbs and spices inAustralia has increased in line with global trends, and this isexpected to continue. The market for local fresh-cut culinaryherbs was estimated to be worth over $62 million per year in2004 and continues to grow at 20% per annum.105 Informationfrom major supermarket sales in 2003 suggests that total retailsales of fresh herbs and spices were valued at $54 million, andsales for dried products were valued at a further $107 million.The sales volumes of fresh herbs are shown in Box 8.
Although there is increasing interest and research in thehealth-promoting and protective properties of herbs andspices,120-122 there are few authoritative recommendations aboutintake in existing national dietary guidelines. The first recom-mendation in the NHMRC dietary guidelines for Australianadults is “Enjoy a wide variety of nutritious foods”,123 and in theNHMRC dietary guidelines for older Australians, a food varietychecklist given in an appendix includes the recommendation touse herbs and spices regularly.124 The same food variety checklisthas also been used as the basis of a checklist to assess intakes ofphytochemical-dense foods, and herbs and spices make up 11out of the 64 foods in the checklist (basil, oregano, mint, dill/fennel, parsley, pepper, ginger, cumin, turmeric, coriander, rose-mary/thyme).125
The higher the score the more adequate the diet is suggested tobe in phytochemicals. However, it is acknowledged that such
food scores need to be further developed, and are not backed byany health outcome studies at this stage.
The two NHMRC dietary guidelines each have another recom-mendation for using herbs and spices. In the dietary guidelinesfor adults, the background chapter on choosing foods low in saltstates that among the recommended substitutes for salt areingredients such as curry spices, garlic and onion, and herbs.123
The guidelines for older Australians note particularly that age-related sensory loss of smell and taste is common in older people,especially those who take many medications, and can haveadverse effects on overall nutrient intake. The guidelines recom-mend experimentation with new flavourings such as herbs andspices to stimulate appetite and support adequate overallintakes.124
A few other countries have made similar recommendationsabout herbs and spices. In the 2005 revision of the Dietaryguidelines for Americans, the chapter on choosing a diet moderatein salt and sodium recommends flavouring with herbs andspices.126 Perhaps the country with the most direct recommenda-tion about the health benefits of culinary herbs is Greece. Theirdietary guidelines not only refer to the usefulness of herbs as saltsubstitutes, but also state: “oregano, basil, thyme and other herbsgrown in Greece are good sources of antioxidant compounds”.127
This emphasis on the health-promoting properties of herbs is ofinterest, given research in Australia that has found that firstgeneration Greek migrants have 35% lower mortality fromcardiovascular and overall mortality than Australian-born con-trols, despite high prevalence of risk factors such as obesity,smoking and sedentary lifestyles. It has been suggested that oneof the dietary factors contributing to this lower mortality couldbe their high intake of antioxidant-rich plant foods, includinggarlic and herbs.128
Despite the generally supportive statements in the dietaryguidelines, the quantitative recommendations for intakes of food
8 Major supermarket sales of fresh herbs and spices in Australia 2003105
Herb or spice Amount sold (kg) Retail sales value
Garlic 1 767 000 $7 941 100
Ginger 592 900 $7 259 900
Chilli 425 000 $3 755 300
Basil 74 200 $7 373 200
Coriander 73 900 $8 860 600
Parsley 30 500 $8 415 000
Mint 18 800 $2 151 500
Chives 18 400 $2 225 500
Lemon grass 17 400 $950 300
Rosemary 15 200 $1 169 700
Oregano 9 700 $594 700
Dill 6 100 $1 074 900
Thyme 3 600 $693 300
Other 845 800 $9 104 000

S18 MJA • Volume 185 Number 4 • 21 August 2006
SU PPLEMENT
in the Australian guide to healthy eating do not yet includesuggested intakes of herbs and spices.129 Those recommendationsaim primarily to ensure adequate intakes of nutrients for whichrecommended dietary intakes have already been established, andit is probably too early for there to be more definitive recommen-dations about foods based on their content of other phytochemi-cals. It should also be borne in mind that there are possibleadverse effects of some spices (such as chilli and peppers) ifconsumed in large quantities,121 although this is unlikely to be asignificant risk at normal levels of use. Thus, the apparentincreasing consumption of culinary herbs and spices is certainly awelcome trend that is worthy of closer monitoring, and in future,
more explicit recommendations about their place in a healthy dietshould be included.
Summary
• Recommendations for intakes of food in the Australian guide tohealthy eating do not yet include suggested intakes of herbs andspices.• Future consideration should be given to including moreexplicit recommendations about the place of herbs and spices in ahealthy diet.

MJA • Volume 185 Number 4 • 21 August 2006 S19
HEALTH BENEFITS OF HERBS AN D SPICES: THE PAST, TH E PRESENT, THE FUTURE
Dietary implications
Virginia A Fazio and Karen E Inge
Food variety and diversity
The use of herbs and spices can assist in increasing the consump-tion of vegetables and fruit. Many national nutrition guidelinesstress the importance of consuming a wide variety of food,including the Australian guide to healthy eating,2 Eat well Australia130
and Dietary guidelines for Americans.126 The healthy nutritionmessage is now one of increasing food variety and diversity tomaximise the range of nutrients consumed on a regular basis.Internationally, there are programs such as the “Go for 2&5”campaign in Australia131 and “5 a day the color way” in the US.132
Herbs and spices naturally fit within such programs, as theyencourage increased use of vegetables by adding flavour andinterest to the diet.
Campaigns throughout the world encouraging an increase in theconsumption of fruits and vegetables are consistent with thedietary guidelines promoted by the World Health Organization.133
There are multiple factors that influence the quantity and variety ofvegetables consumed. Research from the US suggests that factorssuch as age, education, and percentage of income spent on food athome are all positive influences on the amount and variety ofvegetables consumed. This research also shows that the number ofchildren in large households reduces the variety of vegetablesconsumed.134 In addition, an analysis by the Australian Institute ofHealth and Welfare of the 2001 National Health Survey found thatthe percentage of people who consumed fewer than four serves ofvegetables a day decreased with age. In addition, 76.8% of thoseaged 19–34 years were low vegetable consumers, as were 62.4% ofthose aged 75 years and over.135 One of the barriers to increasingconsumption is the limited range of preparation techniques(including interesting flavours) that people feel confident in usingwith fruit and vegetables.135
Herbs and spices increase bioavailability of other nutrients
The nutrients and other biologically active components (such asantioxidants) in food do not always show the same health benefitswhen the active substance is isolated from food and ingested as apure compound.136 There are synergistic effects between nutrientsthat affect absorption and bioavailability.136 Salad dressings con-taining herbs and spices can increase the antioxidant capacity ofthe salad.137 Marjoram, for example, has been shown to increasethe antioxidant capacity by 200%137 (ie, a 200 g portion of a saladenriched with 3 g of marjoram equated to an intake of 4000oxygen radical absorbance capacity units).137 On the other hand,the presence of herbs and spices will not always result in improvedabsorption of nutrients. Just as some vegetables can limit theabsorption of calcium, zinc and iron, research has shown, forexample, that a reduction in non-haem iron absorption can beseen in the presence of rosemary oil.138
Practical application
The use of herbs and spices may help to lower salt, fat and sugarintake. Some practical advice includes:
• Stir fries can have meat or chicken or fish marinated beforecooking in minimal oil. These dishes often include the addition ofgarlic, ginger and chilli.• Curries can be based on either meat or vegetables. Low-fatcurries rely on minimal use of coconut milk or cream, but manytraditional curries and their accompaniments are low in fat. Herbsand spices are integral to the seasoning of these dishes.• There is an enormous variety of Mediterranean dishes. Many ofthe recipes have high proportions of vegetables and rice, pasta orcouscous. The oils used are generally heart-friendly.• Fresh herbs are usually better added towards the end ofcooking or just before serving to preserve their flavour. Parsley canbe added at any time.• Amounts of fresh herbs used are usually 2–4 times more thandried herbs. Some herbs like basil darken when bruised but thisdoes not change the flavour. All fresh herbs should be preparedjust before using.• Dried herbs can be added at any stage of cooking, but useshould be guided by recipes as some herbs, such as bay leaves, areadded very early in cooking. Some dried spices are heated at thebeginning of cooking to release their flavours. More flavour isreleased by grinding with a mortar and pestle.• Garlic releases more flavour when it has been chopped ormashed. It should not be overheated as it may burn and becomebitter.• The hottest parts of chillies are the seeds and white internalmembranes. Removing them will result in a milder flavour.
Understanding food combinations is important in cooking withherbs and spices. Traditional use matches them with certain foods,but this is not meant to be restrictive. Herbs are clustered intofamilies, so the traditional combinations can be exchanged withothers from the same family for variety or personal taste prefer-ences.
Parsley family• Parsley — in multiple forms, used raw and in cooking withmeat, fish, chicken and vegetables.• Dill — used in salads, sauces and with fish, sour cream, and incheese and potato dishes.• Coriander (cilantro) — popular in Mexican cooking and manyAsian and Middle Eastern cuisines. Useful in marinades, dressings,salsas and in cooked dishes. Leaves, roots and seeds are used.
Mint family• Mint — many forms with slightly different tastes are used rawand in cooking, dressings, marinades, drinks, yoghurt, desserts,sauces, vegetable dishes and salads.• Basil — used with tomatoes (fresh and in sauces) and in soups and casseroles with tomato. Also used in salad dressings, pesto,and with pasta, rice, vegetables, meat, chicken and seafood, and inSouth-East Asian cooking in curries, soups and noodle dishes.• Marjoram — used in meat, fish, egg, and cheese dishes, and inpizza.• Oregano — essential for Italian and Greek dishes, but also usedin cheese and egg dishes.• Sage — used with veal, and in stuffing and cheese dishes.

S20 MJA • Volume 185 Number 4 • 21 August 2006
SU PPLEMENT
• Thyme — used in casseroles, soups, and poultry stuffing.• Rosemary — used in marinades, sauces and stuffing, and withfish, poultry and soups.
Allium family
• Chives — used in salad dressings, soups, light sauces, and withegg, cheese, fish and chicken.• Garlic — included in almost every cuisine from Asian toMediterranean. Used in marinades, dressings, sauces, and in stir-fried and slow-cooked dishes.
Other
• Bayleaves — generally used in slow-cooked meat and soupdishes.• Chilli — used with meat, chicken and poultry, shellfish, tomatodishes, and curries. Popular in Asian, Mexican, African andCaribbean cooking.
• Ginger — used in many Asian dishes, but also in cakes,biscuits, desserts and with fruit and juices.• Lemon grass — can be used as a tea or beverage and is includedin many Asian dishes.• Tarragon — used with chicken and fish and in salad dressingsand egg dishes.
Summary• The use of herbs and spices may encourage variety in foodintake. Herbs and spices support nutrient diversity by encouragingnew food choices.• Higher vegetable intakes are linked with improved health.Vegetarian options and vegetable dishes may be more appetisingwhen prepared with herbs and spices.• Many low-fat cooking methods are improved by using herbsand spices in soups, casseroles, marinades and dressings.• Herbs and spices are a healthy alternative to salt as a seasoning.

MJA • Volume 185 Number 4 • 21 August 2006 S21
HEALTH BENEFITS OF HERBS AN D SPICES: THE PAST, TH E PRESENT, THE FUTURE
Moving forward
Linda C Tapsell
Herbs and spices have only recently captured the attention of thescientific community as providing potential health benefits. As aresult, there needs to be a significant investment in human clinicaltrials to substantiate many of the hypothesised health benefits.Nevertheless, this review provides encouragement for furtherscientific inquiry. The evidence presented in this review suggeststhat most of the health effects of herbs and spices on cancer,cardiovascular disease, arthritis and mental health protection maybe mediated through their potent antioxidant effects, given therange of activity across the group as a whole (Box 9).42 As scienceuncovers the role of antioxidants in many degenerative diseasesassociated with ageing, herbs and spices may have a place as animportant source of antioxidants in the diet.
While the bioactivity of individual antioxidants may be known,their effects on health may not be as significant as the combinationof the whole class of bioactives working through multiple mecha-nisms of action. This may well be the case in nutrition generally,where, for example, it is now being argued that the health benefitsof n-3 fatty acids are attributed to moderate health effects mediatedthrough multiple pathways rather than a single significant mecha-nism.139 Like the work undertaken with these essential fatty acids,research is required to uncover the mechanisms by which antioxi-dants deliver health benefits, and then the impact of exogenousantioxidants in this context. A deeper understanding of this rolewill help to establish recommended intakes, as has been the case forvitamins and minerals. Finally, an understanding of how antioxi-dant-rich foods (such as herbs and spices) fit within the context ofthe whole diet, in balance with all other requirements, will enableresearch at the clinical level to establish the evidence for theirputative place in health promotion and disease prevention.
In summary, as several metabolic diseases and ageing-relateddegenerative disorders are closely associated with oxidative pro-cesses in the body, the use of herbs and spices as a source of
antioxidants to combat oxidation warrants further attention.Immediate studies should focus on validating the antioxidantcapacity of herbs and spices after harvest, as well as testing theireffects on markers of oxidation. This will work in parallel withclinical trials that are aiming to establish antioxidants as mediatorsof disease prevention.
9 Antioxidant activity of common dried herbs and spices.42
Common name Botanical nameAntioxidant
activity*
Clove Syzygium aromaticum 465.3 mmol/100 g
Oregano Origanum vulgare 137.5 mmol/100 g
Cinnamon Cinnamomum zeylanicum 98.4 mmol/100 g
Peppermint Mentha piperita 78.5 mmol/100 g
Thyme Thymus vulgaris L. 74.6 mmol/100 g
Rosemary Rosmarinus officinalis L. 66.9 mmol/100 g
Marjoram (sweet) Origanum majorana 55.8 mmol/100 g
Basil Ocimum basilicum L. 30.9 mmol/100 g
Ginger Zingiber officinale 22.5 mmol/100 g
Dill Anethum graveolens 15.9 mmol/100 g
Curry Murraya koenigii L. 13.0 mmol/100 g
Chives Allium schoenoprasum 7.1 mmol/100 g
Parsley Petroselinum crispum 3.6 mmol/100 g
Coriander Coriandrum sativum L. 3.3 mmol/100 g
Vanilla seeds Vanilla planifolia 2.6 mmol/100 g
Garlic Allium sativum L. 2.1 mmol/100 g
* Mean total antioxidant activity per 100 g. ◆

S22 MJA • Volume 185 Number 4 • 21 August 2006
SU PPLEMENT
Competing interestsGourmet Garden (manufacturer of fresh herb products) has provided financefor the cost of the review and honoraria ($800 per section) to the contributingauthors. Gourmet Garden has paid the University of Wollongong, partner inthe National Centre of Excellence in Functional Foods, a consultancy fee todevelop further materials including consumer education that may referencethis publication. Ian Hemphill owns Herbie’s Spices, which is a retail outletselling herbs and spices in Sydney, mainly to the food service industry. He isa recognised expert in this area and has written books on the subject. PeterClifton recently completed a consultancy with Gourmet Garden, analysingthe antioxidant content of its major herbs. Virginia Fazio and Karen Ingeconsult to Gourmet Garden on the communication of the application ofherbs and spices. Gourmet Garden did not influence the authorship norcomment on any draft of the manuscript.
References1 National Health and Medical Research Council. How to review the
evidence: systematic identification and review of the scientific literature.Canberra: NHMRC, 2000.
2 Australian guide to healthy eating. Canberra: Australian GovernmentDepartment of Health and Family Services, 1998.
3 Jacobs DR, Steffen LM. Nutrients, foods, and dietary patterns as expo-sures in research: a framework for food synergy. Am J Clin Nutr 2003; 78:508S-513S.
4 Liu RH. Health benefits of fruit and vegetables are from additive andsynergistic combinations of phytochemicals. Am J Clin Nutr 2003; 78:517S-520S.
5 Contor L, Asp NG. Process for the assessment of scientific support forclaims on foods (PASSCLAIM) phase two: moving forward. Eur J Nutr2004; 43 Suppl 2: ii3-ii6.
6 Kris-Etherton PM, Hecker KD, Bonanome A, et al. Bioactive compoundsin foods: their role in the prevention of cardiovascular disease andcancer. Am J Med 2002; 113 Suppl 9B: 71S-88S.
7 Bellamy D, Pfister A. World medicine: plants, patients and people.Oxford: Blackwell Publishers, 1992.
8 Block E. Antithrombotic agent of garlic: a lesson from 5000 years of folkmedicine. In: Steiner RP, editor. Folk medicine, the art and the science.Washington DC: American Chemical Society, 1986: 125-137.
9 Chevallier A. The encyclopedia of medicinal plants. London: DorlingKindersley, 1996.
10 Govindarajan R, Vijayakumar M, Pushpangadan P. Antioxidant approachto disease management and the role of ‘Rasayana’ herbs of Ayurveda. JEthnopharmacol 2005; 99: 165-178.
11 Thatte UM, Dahanukar SA. Ayurveda and contemporary scientificthought. Trends Pharmacol Sci 1986; 7: 247-251.
12 Sainani GS, Desai DB, Gorhe NH, et al. Effect of dietary garlic and onionon serum lipid profile in Jain community. Ind J Med Res 1979; 69: 776-780.
13 Keys A. Seven countries: a multivariate analysis of death and coronaryheart disease. Cambridge, Mass: Harvard University Press, 1980.
14 Hostettmann K, Marston A. Australian medical plants. In: Steiner RP,editor. Folk medicine, the art and the science. Washington DC: AmericanChemical Society, 1985: 215.
15 Katan MB, De Roos NM. Promises and problems of functional foods. CritRev Food Sci Nutr 2004; 44: 369-377.
16 Palou A, Serra F, Pico C. General aspects on the assessment of functionalfoods in the European Union. Eur J Clin Nutr 2003; 57: S12-S17.
17 National Health and Medical Research Council. Nutrient reference valuesfor Australia and New Zealand including recommended dietary intakes.Canberra: NHMRC, 2006.
18 Corthésy-Theulaz I, den Dunnen JT, Ferré P, et al. Nutrigenomics: theimpact of biomics technology on nutrition research. Ann Nutr Metab2005; 49: 355-365.
19 Kosulwat V, Ganjanasuntorn N, Charoenkiatkul S, et al. The culturalperspective of Thai diet. Proceedings of the 5th International Conferenceon Dietary Assessment Methods; 2003 Jan 26–29; Chiang Rai, Thailand.2003.
20 Gore JM, Dalen JE. Cardiovascular disease. JAMA 1994; 271: 1660-1661.21 Warshafsky S, Kamer RS, Sivak SL. Effect of garlic on total serum
cholesterol: a meta-analysis. Ann Intern Med 1993; 119: 599-605.
22 Stevinson C, Pittler MH, Ernst E. Garlic for treating hypercholesterolemia.A meta-analysis of randomized clinical trials. Ann Intern Med 2000; 133:420-429.
23 Ackermann RT, Mulrow CD, Ramirez G, et al. Garlic shows promise forimproving some cardiovascular risk factors. Arch Intern Med 2001; 161:813-824.
24 Simons LA, Balasubramaniam S, von Konigsmark M, et al. On the effectof garlic on plasma lipids and lipoproteins in mild hypercholesterolae-mia. Atherosclerosis 1995; 113: 219-225.
25 Isaacsohn JL, Moser M, Stein EA, et al. Garlic powder and plasma lipidsand lipoproteins: a multicenter, randomized, placebo-controlled trial.Arch Intern Med 1998; 158: 1189-1194.
26 Superko HR, Krauss RM. Garlic powder, effect on plasma lipids, postpran-dial lipemia, low-density lipoprotein particle size, high-density lipopro-tein subclass distribution and lipoprotein(a). J Am Coll Cardiol 2000; 35:321-326.
27 Gardner CD, Chatterjee LM, Carlson JJ. The effect of a garlic preparationon plasma lipid levels in moderately hypercholesterolemic adults.Atherosclerosis 2001; 154: 213-220.
28 Berthold HK, Sudhop T, von Bergmann K. Effect of garlic oil preparationon serum lipoproteins and cholesterol metabolism: a randomized, pla-cebo-controlled trial. JAMA 1998; 279: 1900-1902.
29 Neil HA, Silagy CA, Lancaster T, et al. Garlic powder in the treatment ofmoderate hyperlipidaemia: a controlled trial and meta-analysis. J R CollPhysicians Lond 1996; 30: 329-334.
30 Gardner CD, Messina M, Lawson LD, et al. Soy, garlic and ginkgo biloba:their potential role in cardiovascular disease prevention and treatment.Curr Atheroscler Rep 2003; 5: 468-475.
31 Lawson LD, Wang ZJ. Low allicin release from garlic supplements: amajor problem due to the sensitivities of allinase activity. J Agric FoodChem 2001; 49: 2592-2599.
32 Lawson LD, Wang ZJ, Papadimitriou D. Allicin release under stimulatedgastrointestinal conditions from garlic powder tablets employed inclinical trials on serum cholesterol. Planta Medica 2001; 67: 13-18.
33 Steiner M, Khan AH, Holbert D, et al. A double-blind crossover study inmoderately hypercholesterolemic men that compared the effect of agedgarlic extract and placebo administration on blood lipids. Am J Clin Nutr1996; 64: 866-870.
34 Silagy CA, Neil HA. A meta-analysis of the effect of garlic on bloodpressure. J Hypertens 1994; 12: 463-468.
35 Elson CE, Underbakke GL, Hanson P, et al. Impact of lemongrass oil, anessential oil, on serum cholesterol. Lipids 1989; 24: 677-679.
36 Gujaral S, Bhumra N, Swaroop M. Effect of ginger oleoresin on serumand hepatic cholesterol levels in cholesterol fed rats. Nutr Rep Int 1978;17: 183.
37 Sambaiah K, Satyanarayana MN. Influence of red pepper and capsaicinon body composition and lipogenesis in rats. J Biosci 1982; 4: 425-430.
38 Hertog MG, Feskens EJ, Hollman PC, et al. Dietary antioxidant flavo-noids and risk of coronary heart disease: the Zutphen Elderly Study.Lancet 1993; 342: 1007-1011.
39 Young IS, Woodside JV. Antioxidants in health and disease. J Clin Pathol2001; 54: 176-186.
40 Schwarz K, Bertelsen G, Nissen LR, et al. Investigation of plant extractsfor the protection of processed foods against lipid oxidation. Compari-son of antioxidant assays based on radical scavenging, lipid oxidationand analysis of the principal antioxidant compounds. Eur Food ResTechnol 2001; 212: 319-328.
41 Tanabe H, Yoshida M, Tomita N. Comparison of the antioxidant activitiesof 22 commonly used culinary herbs and spices on the lipid oxidation ofpork meat. Anim Sci J 2002; 73: 389-393.
42 Dragland S, Senoo H, Wake K, et al. Several culinary and medicinal herbsare important sources of dietary antioxidants. J Nutr 2003; 133: 1286-1290.
43 Zheng W, Wang SY. Antioxidant activity and phenolic compounds inselected herbs. J Agric Food Chem 2001; 49: 5165-5170.
44 Volate SR, Davenport DM, Muga SJ, Wargovich MJ. Modulation ofaberrant crypt foci and apoptosis by dietary herbal supplements (querce-tin, curcumin, silymarin, ginseng and rutin). Carcinogenesis 2005; 26:1450-1456.
45 Chuang SE, Cheng AL, Lin JK, Kuo ML. Inhibition by curcumin ofdiethylnitrosamine-induced hepatic hyperplasia, inflammation, cellulargene products and cell-cycle-related proteins in rats. Food Chem Toxicol2000; 38: 991-995.

MJA • Volume 185 Number 4 • 21 August 2006 S23
HEALTH BENEFITS OF HERBS AN D SPICES: THE PAST, TH E PRESENT, THE FUTURE
46 Chuang SE, Kuo ML, Hsu CH, et al. Curcumin-containing diet inhibitsdiethylnitrosamine-induced murine hepatocarcinogenesis. Carcinogene-sis 2000; 21: 331-335.
47 Dasgupta T, Rao AR, Yadava PK. Chemomodulatory efficacy of basil leaf(Ocimum basilicum) on drug metabolizing and antioxidant enzymes, andon carcinogen-induced skin and forestomach papillomagenesis. Phyto-medicine 2004; 11: 139-151.
48 Vrinda B, Uma Devi P. Radiation protection of human lymphocytechromosomes in vitro by orientin and vicenin. Mutat Res 2001; 498: 39-46.
49 Huang MT, Ho CT, Wang ZY, et al. Inhibition of skin tumorigenesis byrosemary and its constituents carnosol and ursolic acid. Cancer Res 1994;54: 701-708.
50 Amagase H, Sakamoto K, Segal ER, Milner JA. Dietary rosemary sup-presses 7,12-dimethylbenz(a)anthracene binding to rat mammary cellDNA. J Nutr 1996; 126: 1475-1480.
51 Singletary K, MacDonald C, Wallig M. Inhibition by rosemary andcarnosol of 7,12-dimethylbenz[a]anthracene (DMBA)-induced rat mam-mary tumorigenesis and in vivo DMBA-DNA adduct formation. CancerLett 1996; 104: 43-48.
52 Huang SC, Ho CT, Lin-Shiau SY, Lin JK. Carnosol inhibits the invasion ofB16/F10 mouse melanoma cells by suppressing metalloproteinase-9through down-regulating nuclear factor-kappa B and c-Jun. BiochemPharmacol 2005; 69: 221-232.
53 Lo AH, Liang YC, Lin-Shiau SY, et al. Carnosol, an antioxidant in rosemary,suppresses inducible nitric oxide synthase through down-regulatingnuclear factor-kappaB in mouse macrophages. Carcinogenesis 2002; 23:983-991.
54 Carnesecchi S, Schneider Y, Ceraline J, et al. Geraniol, a component ofplant essential oils, inhibits growth and polyamine biosynthesis in humancolon cancer cells. J Pharmacol Exp Ther 2001; 298: 197-200.
55 Nakamura Y, Miyamoto M, Murakami A, et al. A phase II detoxificationenzyme inducer from lemongrass: identification of citral and involvementof electrophilic reaction in the enzyme induction. Biochem Biophys ResCommun 2003; 302: 593-600.
56 Puatanachokchai R, Kishida H, Denda A, et al. Inhibitory effects of lemongrass (Cymbopogon citratus, Stapf) extract on the early phase of hepato-carcinogenesis after initiation with diethylnitrosamine in male Fischer 344rats. Cancer Lett 2002; 183: 9-15.
57 Suaeyun R, Kinouchi T, Arimochi H, et al. Inhibitory effects of lemon grass(Cymbopogon citratus Stapf) on formation of azoxymethane-inducedDNA adducts and aberrant crypt foci in the rat colon. Carcinogenesis1997; 18: 949-955.
58 Lantry LE, Zhang Z, Gao F, et al. Chemopreventive effect of perillylalcohol on 4-(methylnitrosamino)-1-(3-pyridyl)-1-butanone induced tum-origenesis in (C3H/HeJ X A/J)F1 mouse lung. J Cell Biochem Suppl 1997;27: 20-25.
59 Yu TW, Xu M, Dashwood RH. Antimutagenic activity of spearmint.Environ Mol Mutagen 2004; 44: 387-393.
60 Zheng G, Kenney PM, Lam LK. Myristicin: a potential cancer chemopre-ventive agent from parsley leaf oil. J Agric Food Chem 1992; 40: 107-110.
61 Ahmad H, Tijerina MT, Tobola AS. Preferential overexpression of a classMU glutathione S-transferase subunit in mouse liver by myristicin. Bio-chem Biophys Res Commun 1997; 236: 825-828.
62 Potter JD, Steinmetz K. Vegetables, fruit and phytoestrogens as preven-tive agents. IARC Sci Publ 1996; (139): 61-90.
63 Wargovich MJ, Woods C, Hollis DM, Zander ME. Herbals, cancerprevention and health. J Nutr 2001; 131 (11 Suppl): 3034S-3036S.
64 Surh YJ, Kundu JK, Na HK, Lee JS. Redox-sensitive transcription factorsas prime targets for chemoprevention with anti-inflammatory and antiox-idative phytochemicals. J Nutr 2005; 135 (12 Suppl): 2993S-3001S.
65 Surh YJ. Anti-tumor promoting potential of selected spice ingredientswith antioxidative and anti-inflammatory activities: a short review. FoodChem Toxicol 2002; 40: 1091-1097.
66 Surh YJ, Lee E, Lee JM. Chemoprotective properties of some pungentingredients present in red pepper and ginger. Mutat Res 1998; 402: 259-267.
67 Surh Y. Molecular mechanisms of chemopreventive effects of selecteddietary and medicinal phenolic substances. Mutat Res 1999; 428: 305-327.
68 Banerjee S, Prashar R, Kumar A, Rao AR. Modulatory influence ofalcoholic extract of Ocimum leaves on carcinogen-metabolizing enzymeactivities and reduced glutathione levels in mouse. Nutr Cancer 1996; 25:205-217.
69 Moran AE, Carothers AM, Weyant MJ, et al. Carnosol inhibits β-catenintyrosine phosphorylation and prevents adenoma formation in the C57BL/6J/Min/+ (Min/+) mouse. Cancer Res 2005; 65: 1097-1104.
70 Zheng G, Kenney P, Zhang J, Lam LK. Inhibition of benzo[a]pyrene-induced tumorigenesis by myristicin, a volatile aroma constituent ofparsley leaf oil. Carcinogenesis 1992; 13: 1921-1923.
71 Leite JR, Seabra Mde L, Maluf E, et al. Pharmacology of lemongrass(Cymbopogon citratus Stapf.). III. Assessment of eventual toxic, hypnoticand anxiolytic effects on humans. J Ethnopharmacol 1986; 17: 75-83.
72 Carlini EA. Plants and the central nervous system. Pharmacol BiochemBehav 2003; 75: 501-512.
73 Gold PE, Cahill L, Wenk GL. Ginkgo biloba: a cognitive enhancer? PsychSci Public Interest 2002; 3: 2-11.
74 Birks J, Grimley EV, Van Dongen M. Ginkgo biloba for cognitive impair-ment and dementia. Cochrane Database Syst Rev 2002; (4): CD003120.
75 Stough C, Clarke J, Lloyd J, Nathan PJ. Neuropsychological changesafter 30-day Ginkgo biloba administration in healthy participants. Int JNeuropsychopharmacol 2001; 4: 131-134.
76 Frank B, Gupta S. A review of antioxidants and Alzheimer’s disease. AnnClin Psychiatry 2005; 17: 269-286.
77 Eidi M, Eidi A, Bahar M. Effects of Salvia officinalis L. (sage) leaves onmemory retention and its interaction with the cholinergic system in rats.Nutrition 2006; 22: 321-326.
78 Akhondzadeh S, Naghavi H, Vazirian M, et al. Passionflower in thetreatment of generalized anxiety: a pilot double-blind randomized con-trolled trial with oxazepam. J Clin Pharm Ther 2001; 26: 363-367.
79 Akhondzadeh S, Noroozian M, Mohammadi M, et al. Salvia officianalisextract in the treatment of patients with mild to moderate Alzheimer’sdisease: a double blind, randomized and placebo-controlled trial. J ClinPharm Ther 2003; 28: 53-59.
80 Rahman K. Garlic and aging: new insights into an old remedy. Ageing ResRev 2003; 2: 39-56.
81 Howes MJ, Houghton PJ. Plants used in Chinese and Indian traditionalmedicine for improvement of memory and cognitive function. PharmacolBiochem Behav 2003; 75: 513-527.
82 Saxby BK, Harrington F, McKeith IG, et al. Effects of hypertension onattention, memory and executive functions in older adults. HealthPsychol 2003; 22: 587-591.
83 van Exel E, Gussekloo J, Houx P, et al. Atherosclerosis and cognitiveimpairment are linked in the elderly. The Leiden 85-plus Study. Athero-sclerosis 2002; 165: 353-359.
84 Cherubini A, Martin A, Andres-Lacueva C, et al. Vitamin E levels,cognitive impairment and dementia in older persons: the InCHIANTIstudy. Neurobiol Aging 2005; 26: 987-994.
85 Khan AH, Bryden NA, Polansky MM, Anderson RA. Insulin potentiatingfactor and chromium content of selected foods and spices. Biol TraceElem Res 1990; 24: 183-188.
86 Broadhurst CL, Polansky MM, Anderson RA. Insulin-like biological activityof culinary and medicinal plant aqueous extracts in vitro. J Agric FoodChem 2000; 48: 849-852.
87 Imparl-Radosevich J, Deas S, Polansky MM, et al. Regulation of PTP-1and insulin receptor kinase by fractions from cinnamon: implications forcinnamon regulation of insulin signalling. Horm Res 1998; 50: 177-182.
88 Jarvill-Taylor KJ, Anderson RA, Graves DJ. A hydroxychalcone derivedfrom cinnamon functions as a mimetic for insulin in 3T3-L1 adipocytes. JAm Coll Nutr 2001; 20: 327-336.
89 Khan A, Safdar M, Ali Khan MM, et al. Cinnamon improves glucose andlipids of people with type 2 diabetes. Diabetes Care 2003; 26: 3215-3218.
90 Vanschoonbeek K, Thomassen BJ, Senden JM, et al. Cinnamon supple-mentation does not improve glycemic control in postmenopausal type 2diabetes patients. J Nutr 2006; 136: 977-980.
91 Cicero AF, Derosa G, Gaddi A. What do herbalists suggest to diabeticpatients in order to improve glycemic control? Evaluation of scientificevidence and potential risks. Acta Diabetol 2004; 41: 91-98.
92 Vuksan V, Sievenpiper JL. Herbal remedies in the management ofdiabetes: lessons learned from the study of ginseng. Nutr MetabCardiovasc Dis 2005; 15: 149-160.
93 Sievenpiper JL, Hawkins F, Perez C, et al. A systematic quantitativeanalysis of the literature of the high variability in ginseng (Panax spp.):should ginseng be trusted in diabetes? Diabetes Care 2004; 27: 839-840.
94 Vuksan V, Sievenpiper JL, Koo VY, et al. American ginseng (Panaxquinquefolius L) reduces postprandial glycemia in nondiabetic subjects
S24 MJA • Volume 185 Number 4 • 21 August 2006
SU PPLEMENT
and subjects with type 2 diabetes mellitus. Arch Intern Med 2000; 160:1009-1013.
95 Vuksan V, Stavro MP, Sievenpiper JL, et al. American ginseng improvesglycemia in individuals with normal glucose tolerance: effect of dose andtime escalation. J Am Coll Nutr 2000; 19: 738-744.
96 Sotaniemi EA, Haapakoski E, Rautio A. Ginseng therapy in non-insulin-dependent diabetic patients. Diabetes Care 1995; 18: 1373-1375.
97 Vuksan V, Sievenpiper JL, Wong E, et al. American ginseng (Panaxquinquefolius L) attenuates postprandial glycemia in a time-dependentbut not dose-dependent manner in healthy individuals. Am J Clin Nutr2001; 73: 753-758.
98 Lozada CJ, Altman RD. Management of osteoarthritis. In: Koopman WJ,editor. Arthritis and allied conditions: a textbook of rheumatology.Baltimore: Lippincott, Williams & Wilkins; 2001: 2246-2263.
99 Schulick P. Ginger: common spice and wonder drug. Brattleboro, Vt:Herbal Free Press, 1996.
100 Mustafa T, Srivastava KC, Jensen KB. Drug development report 9.Pharmacology of ginger, Zingiber officinale. J Drug Dev 1993; 6: 25-39.
101 Kiuchi F, Iwakami S, Shibuya M, et al. Inhibition of prostaglandin andleukotriene biosynthesis by gingerols and diarylheptanoids. ChemPharm Bull (Tokyo) 1992; 40: 387-391.
102 Bliddal H, Rosetzsky A, Schlichting P, et al. A randomized, placebo-controlled, cross-over study of ginger extracts and ibuprofen in osteoar-thritis. Osteoarthritis Cartilage 2000; 8: 9-12.
103 Altman RD, Marcussen KC. Effects of a ginger extract on knee pain inpatients with osteoarthritis. Arthritis Rheum 2001; 44: 2531-2538.
104 Wigler I, Grotto I, Caspi D, Yaron M. The effects of Zintona EC (a gingerextract) on symptomatic gonarthritis. Osteoarthritis Cartilage 2003; 11:783-789.
105 Parker J. Culinary herbs. In: Salvin S, Bourke M, Byrne T, editors. Thenew crop industries handbook. RIRDC Publication No. 04/125. Can-berra: Rural Industries Research and Development Corporation, 2004:236-243.
106 Lukaczer D, Darland G, Tripp M, et al. A pilot trial evaluating Meta050, aproprietary combination of reduced iso-alpha acids, rosemary extractand oleanolic acid in patients with arthritis and fibromyalgia. PhytotherRes 2005; 19: 864-869.
107 Sohail M, Chaudhry M, Usman M, et al. Efficacy and tolerance of atrisinin degenerative and inflammatory joint disorders. Phytother Res 2005;19: 365-368.
108 Muhlbauer RC, Lozano A, Palacio S, et al. Common herbs, essential oils,and monoterpenes potently modulate bone metabolism. Bone 2003;32: 372-380.
109 Grzanna R, Lindmark L, Frondoza CG. Ginger — an herbal medicinalproduct with broad anti-inflammatory actions. J Med Food 2005; 8: 125-132.
110 Flynn DL, Rafferty MF, Boctor AM. Inhibition of human neutrophil 5-lipoxygenase activity by gingerdione, shogaol, capsaicin and relatedpungent compounds. Prostaglandins Leukot Med 1986; 24: 195-198.
111 Chainani-Wu N. Safety and anti-inflammatory activity of curcumin: acomponent of turmeric (Curcuma longa). J Altern Complement Med2003; 9: 161-168.
112 Manach C, Mazur A, Scalbert A. Polyphenols and prevention of cardio-vascular diseases. Curr Opin Lipidol 2005; 16: 77-84.
113 Australian Bureau of Statistics. Apparent consumption of foodstuffs,Australia, 1997–98 and 1998–99. Canberra: ABS, 2000. (Cat. No. 4306.0.)
114 Australian Bureau of Statistics. National Nutrition Survey: foods eaten,Australia, 1995. Canberra: ABS, 1999. (Cat. No. 4804.0.)
115 Fowles J, Mitchell J, McGrath H. Assessment of cancer risk fromethylene oxide residues in spices imported into New Zealand. FoodChem Toxicol 2001; 39: 1055-1062.
116 Sherman PW, Hash GA. Why vegetable recipes are not very spicy. EvolHum Behav 2001; 22: 147-163.
117 Sloan AE. The top 10 functional food trends. Food Technol 2005; 59: 20-32.
118 Global Information, Inc. Seasonings — UK — August 2005. MintelInternational Group Ltd. http://www.the-infoshop.com/study/mt32490-seasonings.html (accessed Jul 2006).
119 Sector insight: seasonings — added spice. Marketing 2005; 16: 36.120 Craig WJ. Health-promoting properties of common herbs. Am J Clin
Nutr 1999; 70 (3 Suppl): 491S-499S.121 Lampe JW. Spicing up a vegetarian diet: chemopreventive effects of
phytochemicals. Am J Clin Nutr 2003; 78 (3 Suppl): 579S-583S.122 Billing J, Sherman PW. Antimicrobial functions of spices: why some like
it hot. Q Rev Biol 1998; 73: 3-49.123 National Health and Medical Research Council. Food for health —
dietary guidelines for Australian adults. Canberra: NHMRC, 2003.124 National Health and Medical Research Council. Dietary guidelines for
older Australians. Canberra: NHMRC, 1999.125 Wahlqvist M, Wattanapenpaiboon N, Kannar D, et al. Phytochemical
deficiency disorders: inadequate intake of protective foods. Curr Ther1998; July: 53-60.
126 US Department of Health and Human Services; US Department ofAgriculture. Dietary guidelines for Americans 2005. Washington DC: USDepartment of Health and Human Services, 2005. http://www.health-ierus.gov/dietaryguidelines/ (accessed Jul 2006).
127 Ministry of Health and Welfare Supreme Scientific Health Council.Dietary guidelines for adults in Greece. Arch Hellen Med 1999; 16: 516-524.
128 Kouris-Blazos A. Morbidity mortality paradox of 1st generation GreekAustralians. Asia Pac J Clin Nutr 2002; 11 Suppl 3: S569-S575.
129 Smith A, Kellett E, Schmerlaib Y; Children’s Health Development Foun-dation; Deakin University. The Australian guide to healthy eating.Background information for nutrition educators. Canberra: AustralianGovernment Department of Health and Family Services, 1998. http://www.health.gov.au/internet/wcms/publishing.nsf/Content/health-pubhlth-publicat-document-fdeduc-cnt.htm (accessed Jul 2006).
130 National Public Health Partnership. Eat well Australia: an agenda foraction for public health nutrition, 2000–2010. http://www.nphp.gov.au/publications/ (accessed Jul 2006).
131 Australian Government, State and Territory health initiative. Go for 2&5[website]. http://www.gofor2and5.com.au/index.asp (accessed Feb2006).
132 Produce for Better Health Foundation. 5 a day the color way [website].http://www.5aday.org (accessed Feb 2006).
133 WHO Study Group. Diet, nutrition and the prevention of chronicdiseases. Geneva: World Health Organization, 1990.
134 Stewart H, Harris JM, Guthrie J. What determines the variety of ahousehold’s vegetable purchases? Agric Info Bull 2004; No. 792-3: 1-4.http://www.ers.usda.gov/publications/aib792/aib792-3/aib792-3.pdf(accessed Aug 2006).
135 Australian Institute of Health and Welfare. Low fruit and vegetableconsumption. Percentage of people with a low intake of fruit andvegetables by age, 2001. http://www.aihw.gov.au/riskfactors/statistics/RFtable2.cfm (accessed Feb 2006).
136 Fuhrman B, Volkova N, Rosenblat M, Aviram M. Lycopene synergisticallyinhibits LDL oxidation in combination with vitamin E, glabridin, ros-marinic acid, carnosic acid, or garlic. Antioxid Redox Signal 2000; 2: 491-506.
137 Ninfali P, Mea G, Giorgini S, et al. Antioxidant capacity of vegetables,spices and dressings relevant to nutrition. Br J Nutr 2005; 93: 257-266.
138 Samman S, Sandström B, Toft MB, et al. Green tea or rosemary extractadded to foods reduces nonheme-iron absorption. Am J Clin Nutr 2001;73: 607-612.
139 Harrison N, Abhyankar B. The mechanism of action of omega-3 fattyacids in secondary prevention post-myocardial infarction. Curr Med ResOpin 2005; 21: 95-100. ❏

MJAAMPCo
Australasian Medical Publishing Company Proprietary Limited • ABN 20 000 005 854 • Level 2, 26-32 Pyrmont Bridge Road, Pyrmont, NSW 2009 AustraliaTelephone: 02 9562 6666 • International: +61 2 9562 6666 • Facsimile: 02 9562 6600 • Email: [email protected]
Copyright: Australasian Medical Publishing Company Proprietary Limited
The National Centre of Excellence in Functional Foodsis an initiative of the National Food Industry Strategy supported by the
Australian Government Department of Agriculture, Fisheries and Forestry.It is a joint venture between the University of Wollongong, CSIRO Human Nutrition,
Food Science Australia and the Department of Primary Industries, Victoria.This supplement was managed by the University of Wollongong.