health assessment for tajikistan - the health cluster lead
TRANSCRIPT

Health Assessment for Tajikistan
NOVEMBER 2008
WITH SPECIAL THANKS TO:
UNFPA
MERCY CORPS
MEDICAL TEAMS INTERNATIONAL
THE HEALTH CLUSTER
LEAD BY
WORLD HEALTH ORGANIZATION – TAJIKISTAN COUNTRY OFFICE
IN COLLABORATION WITH THE
MINISTRY OF HEALTH OF THE REPUBLIC OF TAJIKISTAN
MINISTRY OF HEALTH

Address requests about publications of the WHO Regional Office for Europe to: Publications WHO Regional Office for Europe Scherfigsvej 8 DK-2100 Copenhagen Ø, Denmark Alternatively, complete an online request form for documentation, health information, or for permission to quote or translate, on the Regional Office web site (http://www.euro.who.int/pubrequest).
© World Health Organization 2010
All rights reserved. The Regional Office for Europe of the World Health Organization welcomes requests for permission to reproduce or translate its publications, in part or in full.
The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters.
All reasonable precautions have been taken by the World Health Organization to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either express or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall the World Health Organization be liable for damages arising from its use. The views expressed by authors, editors, or expert groups do not necessarily represent the decisions or the stated policy of the World Health Organization.

Table of Contents
I. Introduction Survey Objective …………………………………………….……. 3
ASSESSMENT METHODOLOGY ……………………………… 3 Guiding Principles Data collection. Standard measures Limitations Study coverage
II. Context and Background Country profile …………………………………………………….. 6 Demographics History of disaster Winter‐crisis/Compound crisis Role of the State Stakeholders and development assistance Possible scenarios for the near future Early Warning Capabilities HEALTH STATUS OF POPULATION Main causes of mortality ……………………………………. 10 Nutrition Morbidity Diarrhoeal disease Measles Acute respiratory illness Malaria HIV
FACTORS CONTRIBUTING TO ILL HEALTH Environmental health ……………………………………….… 12 Food security Poverty Climate/temperature Shelter/housing Livelihoods and employment Education Health services performance EMS, emergency care and referral services Human resources Availability of drugs and supplies Skilled birthing/maternal care
III. Survey Results
AVAILABLE RESOURCES Physical access ……………………………………………….... 16 Medical transport Communication Community health Planned activities/ Current humanitarian interventions
INFRASTRUCTURE Available resources …………………………………….……… 17 Availability of water Power supplies to facilities Heating systems Alternative heating stocks Sanitation Food stocks Essential medical equipment Availability of drugs and consumables Availability of consumables Personnel
HEALTH PROFILE Mortality ……………………………………..…………………….. 21 Morbidity Outbreaks Trends in morbidity Vaccination coverage Performance of health facilities Functioning of sectors and sub‐sectors
IV. Analysis Affected population……………………………………………. 24 Ongoing impact of the compound crisis/ Lessons learned from the winter crisis………… Needs and resources Capacities Current Reponses
CONCLUSIONS AND RECOMMENDATIONS Impact of current conditions ………………………..……. 26 Current state of the health delivery system Disabled access Continuing or emerging threats Immediate health gaps Response strategy Forthcoming reports
ANNEXES ………………………………………………..………….. 32

Tajikistan Rapid Health Assessment, October – November 2008
4
I. Introduction
Survey Objective: The Rapid Health Assessment was initiated on the behalf of the Health Cluster to establish systemic
links between three categories of health needs ‐ health risks, available health care, and health status ‐ and to define
the possible role of humanitarian aid to improve the health status of the affected population, addressing its
determinants in a systemic way1. We will illustrate and differentiate between basic emerging needs (not covered
owing to the limited or decreased capacity of health services), pre‐existing needs that are exacerbated by the disaster
(e.g. infrastructure) and additional needs created by the disaster (e.g. injuries).
The assessment concentrates on Primary Health Care and Emergency Services, in particular access to care;
infrastructure (energy/electricity and water supply and structural/functional resilience); mother and child
malnutrition and illness; morbidity and mortality related to communicable diseases; health care management,
performance and human resources; provision of medicines and medical commodities; coordination and disaster
readiness. The assessment will yield evidence based data on the current public health profile and operational
situation for an up to date analysis of the current challenges and gaps faced by the health sector as a whole and its
ability to provide patient care services during an emergency. This information and analysis is provided to support the
on‐going planning and response efforts of the MoH RT and the Health Cluster partners.
We intend to answer the following questions:
What has happened? Is there an emergency situation and, if so, what are its key features?
How has the population been affected by the emergency?
Are interventions required to prevent further harm or loss of life? If so, what are top priorities?
What are continuing or emerging threats that may escalate the emergency?
What resources and capacities are already present (e.g., infrastructure and institutions) that could contribute to
the response, and what are the immediate capacity gaps?
ASSESSMENT METHODOLOGY
Guiding Principles: The health sector assessment was designed in such a way as to include a review of existing
information, interviews and observations:
cover the whole country, focusing the analysis on the current situation in Tajikistan;
to yield valid evidence on the current operational situation;
report on health status and risks, health resources (including services being delivered), health system performance, and the progress and effectiveness of health responses;
pay particular attention to the key and critical health care facilities and their ability to function in crisis;
provide up to date information as a follow‐up to the recent Multi‐cluster Assessment;
use a recognized survey tool, the IASC RHA questionnaire, with situation specific modifications was used with format modifications for ease of data entry and modifications and additions in collaboration with the MoH and agency partners (Annex 12);
follow a purposive sampling approach based on well‐defined criteria;
involve the MoH RT and International Health Cluster partner agencies in questionnaire development, assessment interviews and analysis;
identify varying levels of severity for comparison and targeting purposes;
make the analysis relevant for decision‐making and programming.
1 Global Health Cluster Rapid Health Assessment, M. Michael, February 2007

Tajikistan Rapid Health Assessment, October – November 2008
5
Data collection: Field interviews began with questionnaire testing, which resulted in the format modifications;
questionnaires were available in Russian. All interviews were conducted by WHO, UNFPA, Mercy Corps, Medical
Teams International and MoH staff; who received specific instruction and briefings on the process. Chief Doctors (or
their Deputies if not available) were interviewed along with chiefs of clinical care and administrative managers. The
survey was conducted during the end of October into November 2008.
Limitations: There are certain limitations regarding the data sources and the background documents that have been
consulted and used for this assessment. The format of the questionnaire and RHA method tends to be more
qualitative than quantitative, and therefore subject to biases, measurement errors and the pitfalls of convenience
sampling. For example one of the biggest limitations of the survey was that people who collected data were often not
familiar with what should be in place and could not use “observation” technique, e.g. medical waste management.
Chief Doctors expressed their opinion; it was not based on observation of facts by someone familiar with what
medical waste management should be.The quality of medical and demographic information is partially of insufficient
reliability. The available country information is generally limited due to the lack of sophisticated information systems
and the limited local capacity. Time and travel distances limited access to some areas.
Study coverage: The analysis presented is based on the data of 107 questionnaires, which have been filled out in the
framework of the rapid assessment of the access of population to health services, population health profile and
effectiveness and management of health services. There are a very large number of health facilities in the country,
over 2500 in total; the purposive sampling used in this study focused on the key and critical facilities in each Region
(Oblast) and District (Rayon), and specific National level referral facilities in Dushanbe. The primary focus was on
District level hospitals, referred to as Central Rayon Hospitals (CRH), considered key for primary and emergent care;
and in the mountainous areas of southern Sogd a representative systematic sampling (by Mercy Corps) of village level
facilities (SUB and RHC) including a small number of “Rural Medical Houses” was made. In total the following facilities
were assessed:
Diagram 1. Distribution by level of facilities (throughout Tajikistan) Diagram 2. Distribution by regions
Dushanbe: 10 facilities, seven are republican designation, three “city” hospitals; Seven of these are in‐patient; three
are ambulatory clinics. The hospital organizational structure in Dushanbe retains the specialisation structure from the
soviet period, which is a subject of reform efforts; only two of the facilities here are general (primary care) and five
are specialised institutions. There are two medical facility “campuses” in Dushanbe, from one of these several critical
care departments (which are run as separate hospitals) were interviewed and combined into a facility profile.
Khatlon Province2: 27 facilities were assessed in Khatlon province; out of them two are oblast level, one city level and
24 district level types. All health facilities are general (primary care) hospitals.
2 Kulyab, Qurgan‐Tube, Kulyab district, Muminabad, Sarband, Bokhtar, A,Jami.
10
17
37
27
16 Dushanbe
RRS
Sogd
Khatlon
GBAO

Tajikistan Rapid Health Assessment, October – November 2008
6
Sogd Province3: In total 37 health facilities were studies in Sogd Province; five are oblast level type, two are
operational at city level, 11 facilities are district based (9 Central Rayon Hospitals and 2 SES), and 19 are village level.
18 of the facilities are hospitals and 19 are ambulatory clinics.
RRS4: in total 17 health facilities were researched in RRS; 6 facilities are hospitals, and 11 are ambulatory clinics.
GBAO5: situation in GBAO was analyzed in 16 facilities. There are 10 oblast level health facilities, seven of which are
specialized hospitals, only one general (primary care), and two are specialized out‐patient clinics. Also surveyed were
one city level ambulatory clinic, three CRH and one village clinic.
Official data (country level) Total Surveyed %
Medical facilities in cities | towns 48 14 32%
Regional (Oblast) 40 17 42%
District (CRH and SES) 57 43 75%
Village (SUB and RHC) 746 14 2%
Rural medical houses 1692 19 1%
Table 1: number of health facilities nation wide | surveyed during RHA
The greatest focus was on District level health facilities which as described below provide the majority of primary care
within the country and serve as the initial referral base for villages and districts. Then a large representative sampling
of larger tertiary care centers at the Regional, city and National level was taken; along with a sampling of village and
rural facilities in two regions following sampling methodology to provide even and representative coverage in those
districts taken to represent the most geographically isolated locations.
The population coverage of visited health facilities varies from more than 1000 people, Medical Houses and
approximately 6000 for Rural Health Centers; up to overall population of the district at the Central Rayon Hospital,
and Sanitary Epidemiological Stations, city health facilities, oblast facilities or republic health facilities.
The IASC RHA assessment tool was applied, with minor modifications, countrywide with significant time spent with
MoH staff in collaboration with their own efforts in winter preparation during what is considered an ongoing
compound crisis. Preliminary data was used immediately and during the analysis process in support of the CAP
(Consolidated Appeals Process) revision in late 2008. It is hoped that this data and analysis of current evidence will
continue the process of review and targeted response by the humanitarian community.
3 Khojent, Isfara, Kanibadam, Matcha, Shahristan, Spitamen, Ganchi, Istravshan, Asht, J.Rasulov, Kayrakum. 4 Shahrinav, Gissar, Rudaki, Vakhdat. 5 Khorog, Darvaz, Sjugnan, Roshtkala, Rushan.
Tajikistan Rapid Health Assessment, October – November 2008
7
II. Context and Background
This section summarizes information relevant to understanding the context and progression of events leading to the
current conditions faced in Tajikistan which impact on health and well‐being and the delivery of health care; section
three details the observations and data collected in October – November 2008.
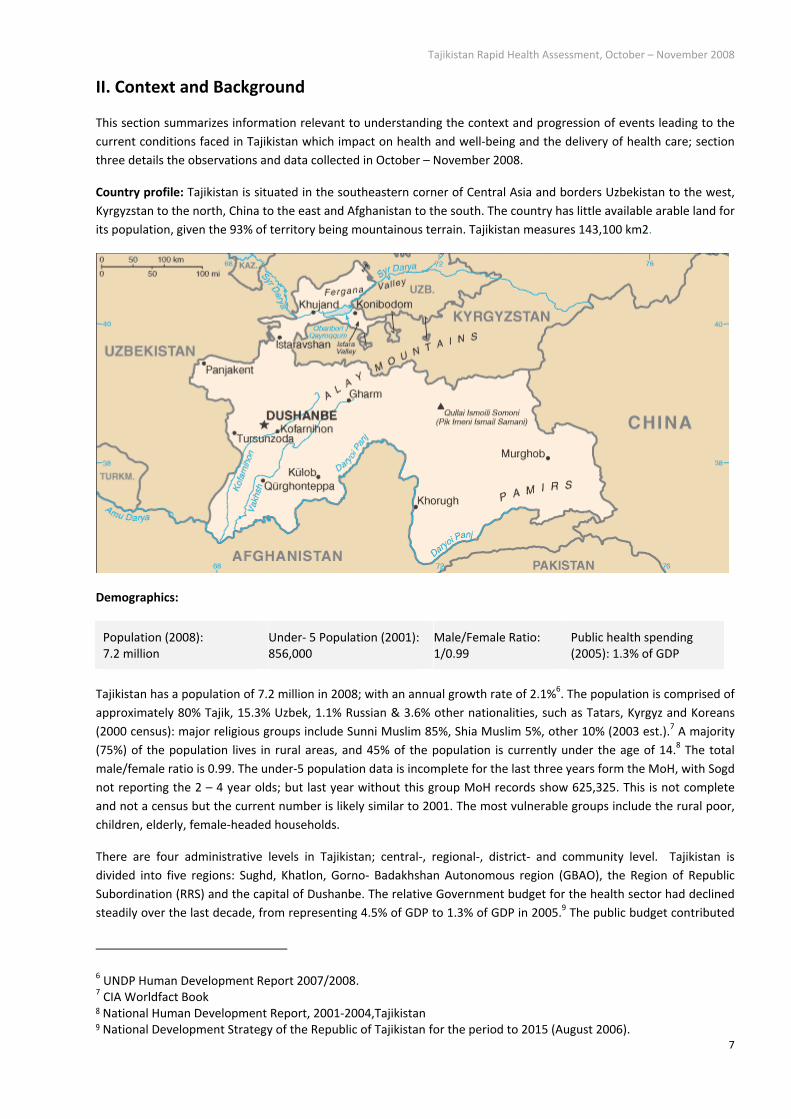
Country profile: Tajikistan is situated in the southeastern corner of Central Asia and borders Uzbekistan to the west,
Kyrgyzstan to the north, China to the east and Afghanistan to the south. The country has little available arable land for
its population, given the 93% of territory being mountainous terrain. Tajikistan measures 143,100 km2.
Demographics:
Population (2008): 7.2 million
Under‐ 5 Population (2001): 856,000
Male/Female Ratio: 1/0.99
Public health spending (2005): 1.3% of GDP
Tajikistan has a population of 7.2 million in 2008; with an annual growth rate of 2.1%6. The population is comprised of
approximately 80% Tajik, 15.3% Uzbek, 1.1% Russian & 3.6% other nationalities, such as Tatars, Kyrgyz and Koreans
(2000 census): major religious groups include Sunni Muslim 85%, Shia Muslim 5%, other 10% (2003 est.).7 A majority
(75%) of the population lives in rural areas, and 45% of the population is currently under the age of 14.8 The total
male/female ratio is 0.99. The under‐5 population data is incomplete for the last three years form the MoH, with Sogd
not reporting the 2 – 4 year olds; but last year without this group MoH records show 625,325. This is not complete
and not a census but the current number is likely similar to 2001. The most vulnerable groups include the rural poor,
children, elderly, female‐headed households.
There are four administrative levels in Tajikistan; central‐, regional‐, district‐ and community level. Tajikistan is
divided into five regions: Sughd, Khatlon, Gorno‐ Badakhshan Autonomous region (GBAO), the Region of Republic
Subordination (RRS) and the capital of Dushanbe. The relative Government budget for the health sector had declined
steadily over the last decade, from representing 4.5% of GDP to 1.3% of GDP in 2005.9 The public budget contributed
6 UNDP Human Development Report 2007/2008. 7 CIA Worldfact Book 8 National Human Development Report, 2001‐2004,Tajikistan 9 National Development Strategy of the Republic of Tajikistan for the period to 2015 (August 2006).

Tajikistan Rapid Health Assessment, October – November 2008
8
US$4 per capita to health expenditures, just 20 percent of the total; whereas household out‐of‐pocket spending
accounted for most (70 %) of health expenditures. Tajikistan is among the lowest spenders on health care in the world
spending just under $16 per capita (or $62 PPP) on health care.10 Despite a moderate rise in revenues the burden of
healthcare continues to shift onto the public leaving most families vulnerable to catastrophic illness; and without
effective social protection.
Tajikistan ranks 122 of 177 on the UNDP Human Development Index; with one of the lowest per capita GDPs among
the 15 former Soviet republics. The 2005 GDP per capita (PPP) was 1,356 USD.11 More than two thirds of the
population continues to live on less than $2.15 per day.
History of disaster: The residents of Tajikistan have historically experienced many natural and man‐made disasters
and events, which have significantly impacted health and security.
Tajikistan gained its independence in 1991 and faced not only economical difficulties, but also political and ethnic
controversies, which led to a five‐year civil war 1992‐1997. The civil war severely damaged the already weak
economic and social infrastructure. The country is prone to many types of hazards, including floods, mudflows,
landslides (mudslides), epidemics, drought, earthquakes, avalanches, insect infestation and windstorms.
According to the Global Seismic Hazard Map (GSHAP 1999), the whole country is located in the high to very high‐risk
earthquake zone. A large number of both seismic and non‐seismic landslides occur annually and threaten settlements
and industrial constructions. Floods occur either in spring following heavy rains, or as a result of melting snow during
the summer. Flash floods in narrow valleys are particularly destructive. Heavy rainfall and the release of water
contained behind dammed watercourses due to landslides, glaciers and accumulation of loose debris result in
extremely destructive mudflows. The severe hazard posed by the Sarez Lake is a stark example of this. Most
avalanches are observed in February and March and pose direct hazards to settlements and access by road. Tajikistan
faced a second year of severe drought in 2007 and annually faces locust invasion threatening crops, livelihoods and
food availability. High winds are encountered annually in many areas of the country with associated damage to crops
and structures.
The result of last winter’s severe winter, drought conditions, locust infestation, and insufficient agricultural input is an
expected 40% reduction in agricultural output in 2008 (30% of wheat, 35% of potato, 14% of vegetables and 40% of
fruit stocks); this comes on top production losses in 2006/200712.
Winter‐crisis/Compound crisis: The current crisis situation, as summarized in the “Tajikistan Humanitarian Food
Security Appeal 2008‐2009”, has been described as a “compound” crisis, with one stress on the already fragile state
impacting on the last, resulting in a multiplying effect on the state of well being of Tajikistan and its residents.
The deteriorating situation and eventual crisis began with rising world food prices and increasing fuel prices in late
2007 which spurred higher transportation and food costs nationwide, in turn leading to deterioration in rural food
security. Continued drought in the spring and summer of 2007, impacted as well by a locust invasion, further
stretched the household coping capacities. Compounding this situation in early 2008, Tajikistan experienced the worst
winter in 44 years. In early January heavy snowfall and avalanches blocked several areas of the country, limiting
access and causing several casualties, while the cold spell throughout the country during most of January, reached
temperatures of ‐15°C during daytime and ‐25°C at night. An energy crisis started in December 2007 and has been
progressively worsening since, whereby most rural areas have been cut off from electricity supplies. By late 2008, the
Nurek hydroelectric dam had regained only minimal capacity necessary to cover electricity needs for a large part of
the country; most rural areas continue to face power for lighting and water supply systems. Energy supplies from
neighbouring Kyrgyzstan and Uzbekistan have been suppressed; resulting in further shortages of gas and electricity.
10 Tajikistan National Health Accounts updated 14 February 2007, NHA unit, EIP/HSF/CEP, World Health Organization, Geneva 11 UNDP Human Development Report 2007/2008 12 Government and FAO assessments.

Tajikistan Rapid Health Assessment, October – November 2008
9
Internal, regional and global economic stresses continue to adversely affect food supplies and prices. The
exceptionally cold weather had a number of serious impacts:
Agricultural assets (e.g., crops, orchards and livestock) were damaged or destroyed, worsening food
availability;
An aging energy infrastructure could not meet demand for electrical power necessary to heat urban centres
including medical facilities;
An already failing water and sanitation infrastructure, especially in healthcare faculties was damaged by frozen
pipes and pressure surges from on again‐off again electrical supply, further adding to existing problems with
the availability of safe drinking water and sanitation;
Residents and State facilities faced a lack of conventional fuel supplies and non‐functioning central heating
systems, dangerous alternative and makeshift heating methods were used;
There were increases in cases of burns and frostbite (reported by some facilities);
Access to basic health care was severely reduced as many hospitals and health centres closed or worked
during restricted hours, and in some cases discharged patients, as the severe weather limited the availability of
electricity, heating and running water.
The impact of the severe winter conditions on vulnerable populations was particularly acute. Vulnerable households
in rural areas saw their stocks of food and seed destroyed. In urban areas the most vulnerable were forced to spend
their income on alternative heating, leaving less for food and healthcare. Prolonged exposure to cold temperatures,
the use of alternative heating devices at home (gas, kerosene, stoves with wood and charcoal), the lack of running
water and isolation or over‐crowding of people, adversely affected the health status of the general population. The
winter‐compound crisis also had a significant impact on already poor health care services, on essential drugs and
vaccines supply and on the access to health care facilities. Vulnerable groups including pregnant women, children,
elderly and mentally disabled people were particularly at risk. Based on reports during the winter crisis conditions
resulted in a higher incidence of acute respiratory diseases, worse hygiene standards, increased incidence of water‐
borne diseases, the worsening of chronic diseases and an increased incidence of preventable maternal and infant
deaths and unsafe deliveries.13
Role of the State in disaster mitigation and response:
The Committee of Emergency Situations and Civil Defense of the Republic of Tajikistan (CoES), is the national body
that has been given the responsibility for national management and coordination of all disaster‐related activities.
During emergency situations, 15 state services may be activated to respond including the Ministry of Health (MoH).
The MoH has its own Division on Emergency Situations established in 2001. A strategic document, “The National
Health Crisis Management Plan” was first adopted in 2005 and is under further development in collaboration with
WHO. The Tajikistan Disaster Management Partnership – Rapid Emergency Assessment and Coordination Team
(REACT) was set up in 2000. The objectives of REACT are Disaster Response Preparedness in Tajikistan to improve the
coordination and information sharing amongst all actors in the field of disaster management, as well as to strengthen
the MoES leadership in disaster management activities. REACT in Dushanbe has around 65 partners including MoH
and WHO; and is chaired by CoES. The Cluster System was activated in February 2008 during the Compound Winter
Crisis; WHO serves as the lead agency for the Health Cluster. The MoH and WHO co‐chair the Health Coordination
meetings and activities.
13 WHO Tajikistan Office situation summary, February 2008

Tajikistan Rapid Health Assessment, October – November 2008
10
Stakeholders and development assistance: International assistance has been an important source of funds for the
public sector in Tajikistan. The Health Cluster (and health sector) comprises some 35 agencies and donors and has
active collaboration and support of the MoH RT. Major donor agencies include: ECHO, Swiss Development and
Cooperation Agency, World Bank, ADB, USAID, Aga Khan Foundation, DFID, Islamic Bank of Reconstruction and
Development, Global Fund, among others. Major partner agencies include: ACTED, Caritas, FOCUS, GRC, Medical
Teams International, Mercy Corps, NLRC, PSF, RCST, Save the Children, UNFPA, UNICEF and WHO.
Possible scenarios for the near future:
Extreme and sustained cold winter conditions remain a concern, with potential additional infrastructure damage,
adverse health effects and damage to food stocks. Food insecurity is expected to continue and may worsen, with
economic stresses further impacting income available for health care and non‐food items. Regional and global
economic and trade stressors will continue. Environmental health factors and endemic diseases with epidemic
potential remain constant threats.
Recent multi‐cluster work on the Interagency Contingency Plan has indicated that the following four potential
disasters should be considered as the “worse likely case” threats to Tajikistan: Earthquake in Dushanbe, research
suggests that a significant earthquake is likely to affect Dushanbe or another Central Asian capital in the near future;
Epidemic (Avian Influenza), The geographical location of Tajikistan puts the country at high risk of an avian influenza
outbreak; Economic crisis, would result in limited purchasing power (and likely price but not wage increases) affecting
access to basic needs (food, water, medicine, health care) and Regional Instability.
Early Warning Capabilities: REACT monitors five “Early Warning Indicators” including precipitation, remittances, basic
food commodity prices, water volume in Nurek Reservoir, and Electricity generation in Tajikistan. The Republican SES
and regional monitoring stations monitor and collect a wide range of epidemiological data. Progress is being made to
narrow and better define the monitored diseases and improve data collection methods.
Shown here is one of the REACT Early‐
Warning Indicators for power generation for
the largest Hydro‐electric plant in Tajikistan.
There is one remaining avalanche station in
GBAO. It has limited capacity and there is no
functioning avalanche prevention activity;
such as controlled release.

Tajikistan Rapid Health Assessment, October – November 2008
11
HEALTH STATUS OF POPULATION
Most health status indicators characterize Tajikistan as a country with low health status compared with CEE countries
and other NIS countries; the health status of the people of Tajikistan remains precarious.
Crude mortality 6.9 per 1,000 United States Census Bureau (BUCEN), International Database. February 2008
Under‐5 mortality 68 per 1,000
93 per 1,000
UNICEF 2006 data http://www.unicef.org/infobycountry/Tajikistan_statistics.html
World Bank 2007 data http://devdata.worldbank.org/genderstats/
genderRpt.asp?rpt=basic&cty=TJK,Tajikistan&hm=home2
Infant Mortality Rate (IMR)
56 per 1,000 live births
75 per 1,000 live births
UNICEF 2006 data http://www.unicef.org/infobycountry/Tajikistan_statistics.html
World Bank 2007 data http://devdata.worldbank.org/genderstats/
genderRpt.asp?rpt=basic&cty=TJK,Tajikistan&hm=home2
Maternal Mortality Ratio 170 deaths per 100,000 live births
43 deaths per 100,000 live births
WHO/Hill 2005: Maternal Mortality in 2005: Estimates developed
by WHO, UNICEF, UNFPA and The World Bank
WHO, 2006: http://data.euro.who.int/hfadb/
Statistics from January – February 2008 from the MoH illustrated a significant increase in mortality compared to the
same months in 2007 among infants, children and mothers. Official state reporting on under‐5 mortality though much
lower than shown in international surveys, a countrywide average of 17.9/1000 in 2007 and 21.2/1000 during the first
two months of 2008, showed an increase for 2008 in four out of five oblasts, including highest rates for Sogd (23.7 in
2008 with 20.2 in 2007). State reporting indicated a 50% increase of infant mortality in RRS state health facilities from
70 – in 2007 to 106 – in 2008 for the same reporting period. GBAO health facilities reported almost a doubled
increase in infant mortality from 6 in 2007 to 10 in 2008. The largest percentage of infant mortality (under 12 months)
cases is registered in state health facilities in Sogd oblast (37%), followed by Khatlon (36%), RRS (18%), Dushanbe (7%)
and GBAO (2%). The situation with maternal mortality was reported as deteriorating with almost a four‐fold increase
of maternal mortality cases only for January 2008 when compared with the same month in 2007. Twelve cases of
maternal mortality cases were reported in January (as opposed to 4 in 2007) and followed only with 2 cases in
February 2008. The largest percentage of maternal mortality cases is in Sogd health facilities (43%), followed by 29% ‐
Khatlon, 21% ‐ RRS, and 7% ‐ GBAO. No cases of maternal mortality were registered in Dushanbe health facilities.14
Main causes of mortality: The main causes of deaths for children under‐5 are, besides neonatal causes, are
pneumonia (20%) and diarrhoeal diseases (16%).15 The most common cause of maternal deaths for reported cases is
bleeding (37%) followed by eclampsia (19%) and infection (16%).16 Leading causes among adults include
cardiovascular related diseases and trauma.
Nutrition: In rural areas, chronic malnutrition among children (27% stunted) has not diminished in three years, and
the prevailing food insecurity situation and inadequate food consumption is likely to reinforce existing vitamin and
mineral deficiencies. Children suffering from acute malnutrition (4.7% wasted in rural areas) suffer from a
combination of very poor diet and infections. Harmful feeding practices for children between 6‐24 months put them
at high risk for serious and irreparable damage to their health and growth. Previous nutritional surveys on women
14 Medical‐information statistical centre of the Ministry of Health of Tajikistan 15 World Health Statistics 2006, Mortality Country Fact Sheet for Tajikistan 16 Republican Center of Medical Statistics

Tajikistan Rapid Health Assessment, October – November 2008
12
and children also indicated significant Iodine, Vitamin A and Iron deficiencies.17 More than half a million people (7.4%)
in Tajikistan has only one meal a day.18
MORBIDITY
The risk of infectious disease is high. The food or waterborne diseases of highest prevalence are bacterial diarrhea,
hepatitis A, and typhoid fever; and the vector‐borne disease being malaria. Cardiovascular disease is the leading cause
of death in the older population. Traumatic injury is prevalent.
2007 (12 months) 2008 (11 months)
Acute diarrhea 57,142 65,237
Dysentery 1,931 1,602
ARI («Viral» Illness) 276,592 266,732
Tuberculosis 3,955 4,836
*MoH RT data
2007 P. falciparum 2008 (11 months) P. falciparum Malaria 616 4 301 2
According to the World Malaria Report 2005 (UNICEF/WHO) in 2003 there were 5,428; of which 250 cases were P. falciparum or mixed.
2007 (WHO) 2008 (11 months) (MoH RT data) Measles 219 0
HIV: Present HIV prevalence is low at less than 1% and by January 2008, the Government of Tajikistan had reported a
cumulative total of 1,049 HIV cases, including 339 new cases for 200720. However UNAIDS estimates the real number
of HIV cases in Tajikistan is 10 times higher than the official data. In Tajikistan, HIV testing is offered free of charge at
140 testing facilities. According to national HIV testing policies, partner notifications are mandatory and anonymous.
Immunization:
2005 WHO/UNICEF * 2006 WHO/UNICEF* 2006 Official Government reports
MCV 86% 87% 96%
HepB3 85% 86% 94%
DPT1 92% 93% 98%
DPT3 85% 86% 96%
Pol3 82% 81% 95%
BCG 98% 94% 94%
*WHO/UNICEF Coverage Estimates: Review of National Immunization Coverage, August 2007
17 Joint Food Security, Livelihoods, Agriculture and Nutrition assessment, May 2008 18 Tajikistan Living Standards Survey 2007 19 WHO (http://www.who.int/vaccines/globalsummary/immunization/countryprofileresult.cfm?C=%27tjk%27) 20 UNAIDS. National report for Tajikistan on implementation of UNGASS HIV/AIDS declaration. 31st January 2008.

Tajikistan Rapid Health Assessment, October – November 2008
13
FACTORS CONTRIBUTING TO ILL HEALTH
Environmental health and access to clean water: Only 59% of the population use and improved an improved drinking
water source, 8% use wells, 6% use bore‐holes; a third of the population get their water supplies from unreliable
sources.21 Bacteriological sample analysis in 2004 demonstrated that more than 40% of the samples were
unacceptable for use.22 Air pollution is reported to be high associated with industrial sites with little regulatory
control; and hazardous substances such as e.g. nitrogen oxide, sulphur dioxide and formaldehydes are released into
the atmosphere from outdated industrial equipment and installations. Arable soil contains high concentrations of
chemicals and salt due to historical agricultural practices.
Food security: A rural joint food security, livelihoods, agriculture and nutrition needs assessment carried out by the
Food Security Cluster and the Government in April/May 2008, found 12% of the rural population (0.6 million) to be
severally food insecure with a food consumption highly likely to be below the standard food intake requirement of
2,100 Kcal/day, compounded by low and unreliable income sources; another 22% (1.1 million) were moderately food
insecure, with a diet still low in kilocalories and nutritional quality, and low or irregular incomes. Even more alarming,
a similar assessment of urban areas in June 2008 revealed that 15% of the people were severely food insecure (0.2
million) and 22% (0.3 million) were moderately food insecure. These findings put some 2.2 million people – 34% of
the rural population (1.7 million) and 37% (0.5 million) of the urban population in a seriously compromised nutritional
and economic situation. During the 2007 – 2008 winter crisis the price of bread and cooking oil doubled, while prices
for most other basic commodities increased by 50%. Regional politics and trade policies are also compounding the
situation; with the sudden export ban in April 2008 on wheat from Kazakhstan, one of Tajikistan’s primary suppliers
serving as an example.
Poverty (defined as <186 per capita per month or $1.32 per capita per day) and extreme poverty (defined as <89 per
capita per month or $0.85 per capita per day) rates in November 2007 estimated as 53% and 17% respectively. Rural
areas account for 71.4% and 75.6% of national poverty and extreme poverty incidence respectively; the poorest being
Sogd region. Households with large number of children, female‐headed households, households with less educated
heads, households with not employed heads are more vulnerable to poverty.23 Many potentially compounding factors
threaten to increase the vulnerability of the poor, as well as driving more households into poverty within Tajikistan.
Climate/temperature: Like most of Central Asia and parts of China, Tajikistan experienced an atypical and severe
winter, reportedly the coldest in its history. Heavier‐
than‐normal snowfall occurred across the country and
isolated many communities. It also hampered travel
between major commercial centers. According to the
Tajik Hydro‐Meteorological Agency, with the exception
of Gorno‐Badakhshan Autonomous Oblast (GBAO)
province where precipitation was below norm, snow falls
in all areas of the country in December was 245% above
the average for many years of observations. At
Tajikistan's lower elevations, the average temperature
range is ‐1° to 3°C in January. But temperatures in
January 2008 averaged around ‐15°C, with some wide
variation within the country. Rural areas experienced
lows of ‐25°C, whilst Dushanbe experienced ranges of ‐8°C during the day to ‐15°C at night. This colder‐than‐normal
weather continued until the end of February.24
21 UNDP Human Development Report 2007/2008 22 Information Platform on Tajikistan, Dushanbe, November, 2004 23 Tajikistan Living Standards Survey 2007 24 Tajikistan Compound Crisis Flash Appeal Revision, March 2008

Tajikistan Rapid Health Assessment, October – November 2008
14
Shelter/housing:
Last winter’s conditions exacerbated the weakness of the infrastructure to provide basic living conditions for many,
especially significant vulnerable groups. The over reliance on electricity for heating, a result of the breakdown and
unserviceable conditions of centralized heating and gas supplies to households creates significant vulnerability among
the population. In terms of this specific vulnerability to the problematic supply of electricity this coming winter, 93%
of respondents in Dushanbe reported that they use electrical heating.25 This result highlights that as urban residents
living in apartment blocks have few heating alternatives aside from electricity or natural gas which may be available
or the standard source of heat in rural areas.
67% of respondents of the recent multi‐cluster assessment indicate that they did not have sufficient fuel for the
coming winter, and 95% of respondents indicated that they would not be able to buy sufficient fuel for the coming
winter. Expenditures on food from disposable income averages 64%; but the most vulnerable groups spend up to 75%
on food.26 This leaves little for heating, or other needs, during the winter. Families facing severe food intake shortages
will also be facing severe limits on their ability to ensure adequate heating given their overall severely limited asset
base and high fuel and food costs. Respondents indicated that they expected up to 64% of their disposable income
would be required for heating alone.27 During the multi‐cluster survey 41% of facilities stated windows and doors
were lacking or in disrepair and offered insufficient protection form the elements.
Livelihoods and employment: The unemployment rate is officially reported as 2.6%; unofficial unemployment rate is
estimated at 48.2%28. Not all those registered receive unemployment benefits from the Social Protection Fund, as it
has been in deficit. An estimated 12.2%29 of the Tajikistan population has migrated, primarily to the Russian
Federation, to seek work opportunities. Remittances from abroad are a significant source of income; and play a
significant role in reducing poverty. Conversely one consequence of the high level of migration is that Tajikistan has
the highest number of female‐headed households compared to other countries in Central Asia putting additional
burdens on women who are already disproportionately affected by poverty and discrimination. Remittances
themselves comprise 17% of disposable income, with wages comprising 49% and self‐produced food 24%. Food is the
largest expenditure, representing 64% of the total with health comprising 4%.30
Education: Primary and secondary school education is compulsory in the country, and the completion rate is above 90
percent. The population is highly literate (99.5%). The percentage of 25+ attending post‐secondary education is
11.7%, compared with an NIS average of 13; Gender Parity Index ‐ Net Enrollment Ratio 0.96 (2005).31 During the
2007 – 2008 winter crisis education was severely disrupted with many schools closing or operating in temperatures
below freezing. Attendance records dropped between 40 to 50%32.
Health services performance:
Central District Hospitals (CRH) and Village Medical Houses (SUBs) are the basic hospital facilities delivering qualified,
specialized hospital care to rural population at the first and second levels.33 SUBs and CRH account for 60.8% of health
facilities; many SUBs are in unsatisfactory condition, most of them do not conform to minimal conditions for patient
treatment; lacking proper water and sanitary services, equipment and supplies, with buildings which are in very poor
condition. Activity of 90 % SUBs is inefficient and as a rule, patients neglect the given level and address directly to
25 Multi‐Cluster Assessment, UNDP DRMP, October 2008 26 Tajikistan Living Standards Survey 2007 27 Multi‐Cluster Assessment, UNDP DRMP, October 2008 28 UNESCO 2008. National Report on Adult Education 29 World Bank Fact Book 2008. 30 Tajikistan Living Standards Survey 2007 31 UNESCO EFA Global Monitoring Report 2008 32 UNICEF country office data 2008 33 Population and public health in Tajikistan (1990‐2003), Republican Center for Medical Statistics, Dushanbe 2004.

Tajikistan Rapid Health Assessment, October – November 2008
15
Central District Hospital34. Republican and Regional hospitals, along with approximately 80 specialized treatment
clinics deliver mainly specialized care and the expanded set of health services to population. There are also a large
number of small Rural Medical Houses with very limited care capacity. In total there are more than 3011 primary
health facilities in Tajikistan, out of them 448 are in‐patient hospitals, 80 children hospitals and units, 75 maternity
hospitals (MHs).
Tajikistan inherited an extensive hospital based system with up to 80% of patients going to hospitals; bypassing initial
level health facilities. Research has shown that each third hospital patient could receive treatment in out‐patient ‐
polyclinic conditions.35 The MoH and international partners are engaged in several health care system reform
activities. Since 1992 there has been progress on reducing the number of hospital beds and admissions and promoting
out‐patient care. This reducing hospital beds is being combined with other reform and development strategies such as
managerial and clinical training. Tajikistan has chosen to promote family practice, as the core component of the
primary care strategy; retraining of specialist is a major component.
EMS, emergency care and referral services: (Based on the 2008 EMS survey in Tajikistan) The pre‐hospital system has
no clear organizational concept and a significant area of the country is not covered by proper medical emergency
response system. A very large number of hospitals cannot provide proper emergency care to the population due to
lack of funding, equipment, properly trained and organized providers among other factors. The system lacks a clear
emergency department organizational structure. During this survey no critical patient transfer guidelines were
identified. Specialty care is lacking either due to lack of equipment and supplies for them to function or the lack of
human resources in certain specialties. Key recommendations focused on communications, training, standard patient
guidelines and resources.36 There has been recognition by the MoH that EMS reform is needed and some limited
reorganization has begun. There are also active training activities for medical professionals and laypersons in
emergency medicine; along with a recognition and interest in institutionalization by the post‐qualification medical
education system. RCST has attained official legal status of their First Aid training for laypersons, the first in the
Republic. Non‐medically trained persons such as firefighters still do not have official standing to provide medical
assistance.
Human resources:
In 2005, Tajikistan had 203 physicians per 100,000 compared with NIS average of 372, and an EU average of 317 per
100,000. Of these 54% worked in hospitals, and about 11% worked as general practitioners. Physician training is very
specialized according to the Soviet model. The medical consists of a five year course, followed by a two‐year hospital
residency. Postgraduate Training is conducted through a separate institution. Consensus supports efforts to increase
the number of general practitioners to deliver primary health care; a faculty of Family Medicine opened in 1999. MoH
reports 41.2 nurses per 10,000 people in 2006. There are efforts to improve nursing training and give more
responsibility to nurses. Feldshers’ (doctor assistants) training was upgraded in 1996 to a four‐year course in medical
college; given the scarcity of physicians in rural areas these practitioners fill an important need in these areas.
Skilled birthing/maternal care: Official reports of home deliveries 2007 comprise 27% of deliveries; other estimates
fall about 38%, reaching 80% in some districts. Skilled attendance rates increase in urban locations, higher education
and higher income levels. In 2008 the MoH enforced door‐to‐door registration of home‐based newborn deliveries.
Overall there were 27,074 live births registered in January‐February 2008; the largest numbers of home births were
registered for Khatlon oblast (2227 cases). By region home based deliveries occur most often in GBAO with 33.1% of
all deliveries taking place outside the state health facility premises; followed by 31.3% in RRS, 24.7% in Khatlon, 4.8% ‐
Sogd and 1.2% ‐ Dushanbe.37
34 Tajikistan health sector reform concept, MoH RT and WHO, Dushanbe, 2002 35 Tajikistan health sector hospital rationalization strategy for 2006‐2010 36 Analysis of the Emergency care capacity, Raed Arafat MD, Tajikistan WHO office 2008 37 Medical‐information statistical centre of the Ministry of Health of Tajikistan

Tajikistan Rapid Health Assessment, October – November 2008
16
Data and analysis is limited regarding complications and causes of death in home deliveries overall, but assumptions
can be made looking at increases in mortality rates during the peak of the winter crisis when the in‐hospital
conditions deteriorated. Increased infant mortality registered in large facilities was attributed to hospital conditions,
limitations in management of pregnancy complications and late hospital admission by a WHO MCH assessment of the
situation during the crisis in early 2008. The legal status of layperson midwives is in question even though several
projects are moving forward with promotion and training activities. Several agencies have been very active in IMCI
and skilled birthing training supporting family practice involvement and increased access to skilled emergency
intervention.
Availability of drugs and supplies: The [Soviet] centralized system for purchase and distribution has broken down so that drug supply is inadequate and
irregular. The government provided drug supply now relies on aid from external donors for about 40% of
pharmaceuticals in some areas. In 1998 the government spent just US$ 0.49 per capita on pharmaceuticals.
Consequently funds received by facilities are inadequate to purchase an adequate supply of drugs, so many patients,
even those in hospital have to purchase their own, as do ambulatory care patients; again shifting the burden onto the
public. The government has set criteria for drug regulation, but these are not strictly enforced, so that many
unregistered drugs are on the market; many of which are ineffective or possibly hazardous. A National Drug
Procurement Agency was established in 2004 to ensure quality control of imported drugs. This agency and the
Republican Medicines Procurement Center have contributed to control and distribution improvements through
international technical support. An essential drug list and national drug policy are in place.

Tajikistan Rapid Health Assessment, October – November 2008
17
0
10
20
30
Dushanbe RR
SSogd
Khatlon
GBAO
Easy
With obstacles
Very difficult
III. Survey Results
This section presents the data gathered through the survey of 107 health facilities (Dushanbe, Rayons of Republican
Subordination (RRS), Sogd Province, Khatlon Province and Gorno Badakhshan Autonomous Oblast (GBAO).
Access
In order to adequately assess the real level of physical access of the population to health services, it is important to
take into account a number of factors, including travel time, availability of public transport (or alternative community
derived transport), road conditions and maintenance, geographical impedances, and communication. Although, the
majority of republican, regional and district health facilities, which are generally centred in cities or larger
settlements, pointed out that the level of access is “easy”, the above mentioned factors make the access difficult for
the majority of the population.
Physical access to health facilities varies from “easy” (72 cases or 67%) to “difficult” (25 cases or 28%). In five cases
(5%), the access was reported to be very difficult38. Accessibility depends on geographical coverage: 0.5 km for first
medical aid facilities up to 560 km and more for oblast and republican level facilities, as well as geographical
characteristics, road conditions and availability of
transport.
Medical transport for transportation of patients is
mentioned only in 8% of surveyed institutions. Although
each CRH has special transport, majority of respondents
marked that patients are transported by private vehicles.
Nearly 70 vehicles have been planned for distribution
within the Global Fund activities for the last few years, and
FOCUS has distributed ambulances in GBAO.
Table 1: Access to health facilities
Dushanbe RRS Sogd Khatlon GBAO Totals
Easy 8 5 26 18 15 72
With obstacles 0 11 7 7 0 25
Very difficult 0 1 2 1 1 5
Questionnaires without answer 2 0 2 1 0 5
Total 107
Communication systems (telephone lines) are necessary requirements of access to services. Nearly 24% of facilities,
mainly at the village level, do not have telephone connection. However, there are examples of potential solutions in
this regard – e.g. availability of mobile phones in five village level facilities in Sugd. This solution is not without its own
drawbacks, including it is self‐funded and the phones owned by the clinic staff who may leave employment, they
require charging and there are many areas without cell coverage. As an example 21% of ambulance staff indicated
that mobile phones of the emergency workers are being used for communication, in only 2% of those cases specially
allocated mobile phones are used; and only 8% of ambulances are confirmed to have radios on them.39 There is a
long‐wave radio system used for communication which has been very successful in the mountainous regions.
Community health: Community health workers (CHW) provide services in 84% of facilities. These CHW promote
health education, healthy life style, prenatal care as well as vaccination and breast‐feeding. In addition, traditional
38 RRS (1 case): Rasht, Safebod village; Sogd Province (2 cases): SUB village clinic in Asht, Shahristan, Kuli Kuton; Khatlon Province (1
case): CRH of Nasiri Khusav District; GBAO (1 case): Oblast Cardiology Centre 39 Analysis of the Emergency care capacity, Raed Arafat MD, Tajikistan WHO office 2008

Tajikistan Rapid Health Assessment, October – November 2008
18
healers and traditional birth attendants (TBAs) are also providing health services as recorded in RRS, Khatlon and Sugd
(27 questionnaires – 25%). Training and involvement of CHWs and TBAs improve preventative health practices and
patient outcomes through peer‐based education and skilled care. However, there is no mention of CHWs at the level
of city facilities, and some districts, e.g. Rudaki; likely due to reluctance to use such services in areas which they have
not been promoted.
Planned activities and current humanitarian interventions: Nearly all assessed facilities were covered by
international development projects, which also led to the increase of the access of the population to medical services.
International projects while improving conditions and care also improve the standing image of the facility and
increase confidence in the patient population, increasing facility use. The number of the humanitarian organizations
providing support to medical institutions varies from 1 to 4 per institution. Staff and layperson training on disease
prevention and other health issues are an important contribution in provision of improved access to quality services
and proper seeking of care. Respondents have also marked that Ministry of Health and its international donors and
partner agencies have provided humanitarian assistance. Their activities include provision of medicines, vaccination,
medical equipment and other materials as well as assistance in building repairing and renovations; some agencies also
provide fuel. In Sogd Region Mercy Corps helped develop a very good functioning model for community level medical
transport. In almost 90% of facilities improvement activities are conducted by local city government bodies
(Khukumats) (77%), national government (29%), and community residents (25%).
Available resources
Infrastructure
Out of 107 surveyed facilities: 65 (61%) described
themselves as functioning, 14 require various types of
renovations and repairing, 13 are in poor conditions, and
two are located in adapted facilities. Only 40 facilities
(37%) have sustainable access to water. In 15 cases water
supply is shortly available and in 48 cases system is not
working at all (see attached Annex 2: list of health
facilities that experience shortage of drinking water
supply). This is relevant to the majority parts of the
country. Almost 80% of such medical facilities are at the
District level (CRH) and village level. Again the District
level hospitals provide in‐patient and critical care the majority of patients.
Table 3: Physical conditions of assessed health facilities | buildings
Dushanbe RRS Sogd Khatlon GBAO Totals
Functioning 9 13 24 17 2 65
Needs repair 0 1 6 5 2 14
In poor condition | non functioning 1 1 0 2 9 13
Questionnaires without answer 2 7 3 3 15
Total 107
In villages Vorinj and Safebod, Rasht Valley, two village health centres do not have building at all, and are located
within the territory of school and dekhkan farm. 13 facilities in GBAO, six in Sugd, and four in RRS require
reconstruction and renovation. Refer to the Annex 3 of the health facilities that need repair and are in poor physical
conditions.
05
1015202530
Dushanbe RR
SSogd
Khatlon
GBAO
Functioning
Needs repair
In poor condition| non functioning

Tajikistan Rapid Health Assessment, October – November 2008
19
Availability of water was subjective in this study, 38% of facility managers reported adequate water available.
Table 4:Availablity of water supply in health facilities
Dushanbe RRS Sogd Khatlon GBAO Totals
Available 10 4 12 11 3 40
Shortly available 0 2 4 8 1 15
Not available 0 11 19 6 12 48
Questionnaires without answer 2 2 4
Total 107
Availability of hot water is mentioned only in 10 cases. Seven of these facilities are located in Dushanbe, one in Sugd,
one in RRS and one Khatlon.
Power supplies to facilities: Nearly 100% of medical facilities at republican, regional and district levels have
agreement with electricity supplier – companies like Barki Tojik | Pamir Energy. There are no agreements at the
village level; however existence of agreements does not guarantee uninterrupted electricity provision and without
payments made for electricity the suppliers have threatened to shut off power.
Almost all Regional and District (CRH) facilities have generators. Some of them have up to 7 generators from 1.5 to 70
KW. 59 health facilities have generators and 44 do not have (three left without response). Out of these 44 facilities 13
are based at district, oblast and national levels; showing that the deficit in generators is primarily in the rural or village
facilities. This focus on providing alternative power to major in‐patient facilities has its merits, but it leaves remote
and often isolated populations without minimal conditions for modern medical care. 10 of them are out‐patient type
facilities, but three are CRHs in GBAO (Darvaz, Roshtkala and Shugnan) which must provide high levels of care in their
remote districts. Several facilities have developed intricate power utilization schemes for various modes of operation
from full operations, energy savings, curtailed supply and full operation on generators.
The fuel for generators for operation during 10 days period of time is not available in only 9 (16.7%) cases out of 60.
The lists of health facilities which do not have electric generators and those which have generators but lacking of fuel
for generators are presented in Annexes 4 and 5. The international community provided a large number of
generators for health facilities in response to last winter’s crisis.
Table 5: Availability of generators in health facilities
Dushanbe RRS Sogd Khatlon GBAO Totals
Available 8 4 17 27 4 60
Not available 2 12 18 0 12 44
Questionnaires without answer 1 2 3
Total 107
Table 6: Fuel availability for existing generators
Dushanbe RRS Sogd Khatlon GBAO Totals
Available for 10 days operation 8 2 16 22 3 51
Not available 2 1 5 1 9
Total 60
Heating systems: It was revealed that only 17% of facilities have functioning heating system and have alternate
sources of heating. In 2 cases (RRS and Sogd) heating system is functioning but there are no alternative methods
available in the health facility, in 35 cases only alternatives are available. In 37 cases there is neither central heating
nor alternatives are available (list of health facilities is described in Annex 6). There are missing answers on the
question on heating system in 15 questionnaires. 12 of these facilities are District level hospitals (CRH); showing that
approximately 20% of these key in‐patient care facilities are without heat even in normal winter conditions.

Tajikistan Rapid Health Assessment, October – November 2008
20
Alternative heating stocks: 12 (70%) facilities in RRS and 24 (89%) facilities in Khatlon have coal stocks. Nearly all
facilities in Sugd have stocks of coal, wood and alternative sources of heating (70%); only 6 (37%) facilities in GBAO
have coals stocks. Thus, overall 70% facilities mentioned that they have coal stocks. Overall there was a good effort to
comply with Government/MoH preparation plans and stock requirements given the available resources. The most risk
remain in those isolated sites which if they consume the whole of their stock or are without before a crisis, it may be
impossible to resupply them in a timely manner. See Annex 8 on the list of facilities without coal and wood stocks.
Table 9: Availability of coal & wood stock
Dushanbe RRS Sogd Khatlon GBAO Totals
Available 3 12 26 24 6 71
Not available 7 4 7 3 9 30
Questionnaires without answer 1 4 1 6
Total 107
Sanitation
Only 43% of the facilities were found to have functioning toilets and sewage systems; including latrines in rural areas.
In a small number of cases the system needs repair.
Table 7. Toilets & Sewage System
Dushanbe RRS Sogd Khatlon GBAO Totals
Functioning 9 5 20 10 2 46
Needs repair 0 2 0 4 0 6
Not functioning 1 10 13 11 14 49
Questionnaires without answer 4 2 6
Total 107
Waste utilisation at the regional and district levels is organised through special furnaces, while at the village level, this
is done in a specially allocated area. This occurs in more than 53%; in 45 cases specialized and controlled medical
waste management systems do not function (list of health facilities is presented at Annex 7).
Table 8: Waste Management | Utilisation
Dushanbe RRS Sogd Khatlon GBAO Totals
Functioning 10 7 20 16 3 56
Needs repair 0 0 0 0 0 0
Not functioning 0 10 13 9 13 45
Questionnaires without answer 4 2 6
Total 107
Availability of food stocks was calculated only for in‐patient facilities only (71=100%); as for out‐patient facilities (SES,
RHC, Medical House it was not relevant). Food stocks are available in 47 (out of 71) facilities that should have food.
Only 5 out of 12 facilities in GBAO have food stock. 20 facilities (out of 27) in Khatlon also have available food stocks.
In Sugd region 9 facilities (out of 18) have food stocks. Only one (out of 6) facility in RRS has available food stocks. 7
(out of 8) facilities in Dushanbe also have food stocks. Refer to Annex 9 for the list of facilities without food stock.
Table 10: Availability of food stock
Dushanbe RRS Sogd Khatlon GBAO Totals
Available 7 6 9 20 5 47
Not available 0 5 8 5 6 24
Total which require food stocks on hand 71

Tajikistan Rapid Health Assessment, October – November 2008
21
Essential medical equipment
There is functioning essential medical equipment available at the regional and republican levels, however, there are
no adequate funds to cover maintenance and repairing costs. There is also functioning equipment at CRH level, with
occasional lack of or not functioning refrigerators in “cold chain”, ventilators, sterilizing machines and other
equipment. Some specialized facilities require glucometers, Ultrasound, ventilators, cardiac monitors. There is often
disconnect between available equipment and the patient. The usable equipment may not be of adequate number, or
is being saved for extreme cases, often maintenance or calibration is not done as required, staff may not have training
in use or maintenance of the equipment, disposable components or reagents may not be available or simply there is
no power available to operate the equipment.
Availability of drugs and vaccines consumables
Out of 107 surveyed facilities: 30 – have all the essential drugs queried in the survey; 48 have stock deficiencies of
essential drugs, 24 facilities do not have any essential drug stock, including five facilities that do not have drugs
required for their specialized tasks, such as SES. Regional distribution of facilities lacking essential drugs are as follows:
Sugd and RRS ‐ 29%, Dushanbe – 11%, Khatlon – 4%, GBAO – 43%. See Annex 10 for additional information on health
facilities without essential drugs stocks.
Table 11: Essential drug supply
Dushanbe RRS Sogd Khatlon GBAO Totals
Available 6 3 10 9 2 30
Partly available 3 9 14 15 7 48
Not available 1 5 10 1 7 24
Questionnaires without answer 3 2 5
Total 107
Antibiotics for pneumonia, GI infection and cholera are available, or partially available at almost all facilities at the
village level. Oral rehydration salts were available only in two medical houses.
Vaccines are available in nearly all facilities that are tasked with child immunization. At the same time, some facilities
have suffered from interruption of vaccine provision – e.g. Darvaz district was nor receiving vaccines for two months
in winter due to the closure of road communication. There are problems with vaccines provision to primary health
care facilities, especially in mountain regions due to lack of funds allocated for fuel.
Availability of consumables
In 58 cases respondents mark that consumables are partially available, 32 facilities confirm that consumables are fully
provided and 9 facilities claim that there are no consumables available (list of health facilities provided in Annex 11).
Representatives of six health facilities did not answer this question.
Table 12: Availability of consumables
Dushanbe RRS Sogd Khatlon GBAO Totals
Available 3 6 12 6 5 32
Partly available 6 9 18 18 7 58
Not avaialable 1 0 3 1 4 9
Questionnaires without answer 4 2 6
Total 107
Respondents located at the level of CRH and village level who responded that they experience shortages of medical
consumables which include dressing, syringes and suture materials. This is attributed to the lack of funds allocated for
this particular budget line.

Tajikistan Rapid Health Assessment, October – November 2008
22
Birth kits are not available in almost 90% of village facilities of Rasht. The absence of birth kits (Rural District Hospital
2 out of 2, RHC – 2 out of 2, MH – 8 out of 9) and antiseptics (in MH in RRS – 5 out of 9).
Personnel
Medical facilities lack properly qualified staff in every region. This is, in particular, relevant to remote and
mountainous districts. For example, Murgab district of GBAO lacks 28 doctors, and there are no gynaecologists in
Roshtkala district for many years. 57 doctors are needed in Ganch district of Sugd region, 62 – in Muminabad district
of Khatlon, 28 – in Gissar of RRS.
Table 13: Human Resources
Dushanbe RRS Sogd Khatlon GBAO Totals
All type of staff are available 0 1 12 0 1 14
Physicians & nurses are partly available 1 9 7 4 4 25
All types of staff are missing 2 5 13 18 8 46
7 2 5 5 3 85
There are 14 facilities (1 in RRS, 12 in Sogd and 1 in GBAO) that confirm full availability of required staff. In 77 cases
there was lack of all type of staff (middle and junior), e.g. in Khatlon 22 health facilities, in Sogd in 22, in RRS in 14
cases and in GBAO in 12 cases.
Health profile
Mortality
The majority of questionnaires did not contain an answer and many stated that death records were reported through
the city government at the community level. However, most of questionnaires do not have all necessary information
(causes of death, or number of cases etc. are not mentioned), or contain data for 2007. Nearly 100% responded that
there were no changes in mortality rate trends. Please refer to the background data found on page nine.
Morbidity
Main reported health problems among children are: acute respiratory infection (30 to 95%), diarrhea (10 to 40%),
anemia ‐ malnutrition (5 to 20%). This was observed in all regions at all levels.
Main health problems among women are: anemia (40 to 85%), gynecological disorders and pregnancy complications
(20 to 50%), endocrine system diseases (5 to 10%), kidney disorders and urinary tracts (16 to 40%).
Main health problems among adults are: cardiovascular diseases (10 to 50%), gastrointestinal diseases (15 to 60%),
urinary diseases (10 to 25%), respiratory diseases and infectious diseases (10 to 70%).
Unfortunately the respondents did not offer details to the actual disease or illness within the groups except for
children. The family of cardiovascular diseases, hypertension, coronary disease and stroke are all very prevalent. The
specialization of many facilities made interpretation difficult as well, for example trauma is underrepresented.
Outbreaks:
The following districts covered by the rapid health assessment reported outbreaks and increase of morbidity rates in
more than 29 cases in the first 9 months of 2008:
Hepatitis А: 76 cases in Gissar, 90 – Shahrinav, 129 – Istravshan, 96 случаев ‐ Spitamen. Increase of morbidity cases
observed in Khorog – 73 cases, Bokhtar – 8 cases, Isfara – 21, and Shahristan.
Typhoid: Gissar (64 cases), Shahrinav (27), Boktar (19) and Isfara (23).
Brucellosis: Gissar (40), Rudaki, Dushanbe (100 ‐ 200), Istravshan (32), Ganchi, Spitamen (37), Shahristan, Matcha,
darvaz (58).

Tajikistan Rapid Health Assessment, October – November 2008
23
Diarrhoea: Jabbar Rasulov (1363).
Leptospirosis: Vahdat.
ARI: Dushanbe
Trends in Morbidity
Analysis of country‐wide aggregate numbers of injuries, burns, gas poisoning and other non‐communicable diseases
in 2008 compared to 2007 did not reveal any major changes in trends. However, detailed reports of some of the
facilities reveal that there have been some differences in this regard. Likely this is due to inadequacies in data
available in combination with reporting style variance between facilities and staff. Those which did offer comparative
data from patient records generally did show statistically significant changes. The study focused on comparing the
first 6 months of 2007 and 2008.
In accordance with the data from the Dushanbe City Emergency Hospital, the number of recorded ambulance calls
increased by 9% in the first 6 months of 2008 verses 2007 (19,666 in 2007 to 21,815 in 2008). The number of appeals
for emergency medical aid increased from 48.7/1000 in the first 6 months of 2007 to 52/1000 in 2008. ORV morbidity
rates increased by 53% in the first half of the year compared to 2007 (1242 and 2350). The number of cases of burns,
injuries and frostbites increased from 425 to 734 cases during the first 6 months of 2007 and 2008respectively. In
accordance with the data of the City Infectious Hospital, increase of ORV morbidity rate in the first six months of 2007
‐ 2008 was 44%; from 339 to 770 respectively. In accordance with the data from National Training Clinical Centre of
Family Medicine, the number of visits to family doctors in the first 9 months of 2007 was 7004, while in 2008 this
number increased to 10,506. The number of ARI cases increased by 56%; from 233 to 414 cases. The number of out‐
patient visits may be related to an increase in willingness or desire to seek treatment in an out‐patient setting thus
avoiding a hospital stay in harsh conditions, none the less a 56% increase in ARI’s treated is indicative of a significant
change in disease pattern.
There is also increase in cases of typhoid, Hepatitis A, acute intestinal diseases, zoonotic disease and helminthes
invasion in 9 months of 2008 compared to the same period in 2007.
Overall number of cases of acute and chronic malnutrition is about 60‐100 cases. However, these figures are doubtful,
since nutrition and anemia are reported to be the main health problems among children and women.
Vaccination coverage rates are very high at the level of CRH in almost all regions ‐ 93‐97% per each vaccine. Around
Dushanbe the level of vaccination for measles, pentavaccine, poliomyelitis, and BCG is from 99 to 100% of coverage;
hepatitis B is from 80 – 93%; Sogd Province the lowest coverage is for pentavaccice (Karyakum City Hospital – 24%)
and for measles (48% ‐ Shahristan CRH), in Spitamen the lowest indicator is for hepatitis B – 61%, poliomyelitis and
BCG is from 71 – 100%. Around Khatlon Province the level of penta vaccination is 6.6% in Jomi CRH and 100%
coverage was confirmed in Muminobad CRH. The indicator for Measles, Hepatitis B, Poliomyelitis and BCG is consists
of 67 – 100%. In GBAO for pentavaccine is the lowest level in Roshtkala & Darvaz (40 – 45%), measles, BCG and
poliomyelitis the level of vaccination coverage is from 80 – 100% and in Darvaz the BCG vaccination indicator is 60%.
RRS indicators are as following: measles from 22‐25% up to 100%, penta‐vaccine is from 38 – 48%, hepatitis B is from
15 – 100%, poliomyelitis is from 20 – 100% and BCG is from 47 – 91%.
However, this indicator is much lower at the level of village facilities. This may be attributed to the fact that instead of
stating the percentage of vaccinated children, respondents marked the actual number of vaccinated children. Since
there is less population at the village level, there are less children covered by these facilities, thus absolute
vaccination figures seem to be inadequate. However, some cases (e.g. measles) reveal that there is a need to improve
the supervision over the expanded immunization programme.
There was a break in immunization programme implementation only in two cases. Immunization programme was
suspended for two months in Darvaz district due to cold weather and road closure. In other cases, suspension of the

Tajikistan Rapid Health Assessment, October – November 2008
24
programme included decrease of visits by population, termination of training contracts and postponement of the
programme to the later stage.
Performance of health facilities
A low number, 33 facilities use standardised protocols, with more than 25 more using them occasionally in their work.
These are mainly primary healthcare facilities that use them to define and treat malaria cases, IMCI and DOTS. These
are primarily in use in less specialised and general hospitals, which indicate use of standard protocols. Standard
protocols for other common hospitalized cases have not been developed, or have not been disseminated throughout
the country.
In accordance with the responses, referral system in 19 facilities (21% of answered to this question) needs
improvement. A defined referral system with a concrete diagnosis can become a major factor in improving access of
the population to the specialists of various profiles.
Ambulatory registers and hospital records, as well as drugs management system require improvement in 40% of cases
at all levels. Accurate registration and proper hospital records are also important indicators of the quality of health
services. These records should be regularly analysed in order to define any trends in visits and admissions of patients
for further introduction of necessary prevention measures.
Drug management system requires improvement in 30% of cases at all levels. Improved drugs management system
serves to define the use and needs in drugs and medicines, which leads to the improved performance of the medical
facilities and access of the population to medical services.
Hospital hygiene responses at the Republican and regional level facilities stated hand washing practices is satisfactory;
CRH and rural facilities respondents marked that this procedure requires further improvement.
Emergency preparedness is also one of the important criteria for assessing the performance of medical facility. As
experience shows, some events (like disasters) can evolve with the unpredictable speed, thus it is important that
preparedness process includes development and agreement of the plan of actions, evacuation plan and organization
of emergency trainings. While 70% of facilities claim the existence of the plan of actions during emergencies, only in
20% of cases any regular trainings on emergencies were conducted. Only 5% of facilities have emergency funds.
Functioning of sectors and sub‐sectors
Assessment of the functioning of sectors and services revealed that overall clinical services and child health care
function at the normal level, while such services as obstetrics, infections and non‐infectious diseases, nutrition and
sanitary, laboratories and psychological health were reported by hospital staff themselves to have a low level of
functioning. This is especially relevant for rural facilities. There is a need for thorough analysis of the situation in these
sectors and adoption of concrete measures for their improvement, especially in obstetrics, psychological health and
sanitary.

Tajikistan Rapid Health Assessment, October – November 2008
25
IV. Analysis
This analysis focuses and is based on the situation at the time the survey was completed in November 2008. The
winter 07‐08 brought many systemic weaknesses to the forefront and is a consideration for analysis but is not the
primary focus of this assessment.
Affected population (How has the population been affected by the emergency? Who is likely to be most
vulnerable and why? How many people were affected, and where are they?)
The poor state of the health system, its limited functioning capacity diminishes its ability to function in crisis and
adversely impacts all of the residents under its care. The entire population of Tajikistan faces multiple factors which
adversely affect their state of health and well being. Several groups are especially vulnerable to factors which
negatively impact and endanger health and life; these include the very young, the elderly, those in poverty, those
without access to safe water and those who are food insecure.
Ongoing impact of the compound crisis and lessons learned from the winter crisis
The winter crisis of 2007‐08 has brought to the attention of the humanitarian community Tajikistan’s systemic gaps in
the health system. Health services suffer shortages of medicines, limited capacities for surveillance, lack of qualified
health personnel, laboratory and especially emergency care40.
The ongoing global crises: financial, food and energy constitute the existing compound emergency; contribute to
further impoverishment of the population, increase health risks and capacity of health system leaving it unable to
respond to growing health needs of the population. Still now a significant number of health facilities lack heating
capacity and dramatic increase in fuel prices will have further affects on capacity of health system to respond to
health needs. 41
Economic accessibility was not specifically assessed in the interviews, but the current available evidence on economic
conditions and food‐security point out a deterioration in the individual or household’s ability to afford medications
and medical care, and the State’s limitations to properly fund the public health system.
The winter crisis of 2007‐2008 exacerbated chronic underlying health system problems, limiting access to health care,
and worsening the performance of health care and the conditions under which patient care was delivered,
particularly in rural areas. The power shortages denied heating, lighting and water supplies to hospitals, maternity
wards and cold chain stations. The most dramatic result in this context was an 8‐fold increase in infant deaths in
Shurobad (Khatlon) and 4‐fold in Spitamen (Sogd)42. It is estimated that in the worst phase of the 2007‐2008 winter
crisis, only 5‐10% of patients had their needs covered on admission; many patients were discharged early due to lack
of suitable conditions in health facilities.
At the community level, the winter crises increased previous negative health factors and highlighted cold crisis health
risks, such as burns and injuries related to the use of alternative sources of heating. During the winter of 2007‐2008
there was a reported increase of 30% in the incidence of acute respiratory infections43.
The Impact of cold and energy crisis on population was evident throughout the country. Although retrospective data
varies, field data during the crisis indicated an increase in the cases of ARI morbidity rates, home birthing, as well as
shortened period of stay in maternity houses, and increased mother and child mortality rates in the country. It may
be suggested that due to freeze and collapse of water supply systems, there has been lack of safe drinking water,
which led to the increase of water born diseases, such as diarrhea, hepatitis and typhoid.
40 Analysis of the Emergency Care Capacities of the pre‐hospital and hospital care system. WHO, 2008 41 Multi‐Cluster assessment, REACT, Oct 2008 42 Ministry of Health statistics, Aug 2008 43 Rapid Health Assessment. WHO, February 2008

Tajikistan Rapid Health Assessment, October – November 2008
26
This analysis shows that with even normal winter conditions and the electrical shortages due to this year’s drought
conditions, the underlying health system problems constitute a state of emergency with health facilities and
caregivers unable to meet the basic health needs of the population. The communities and individual coping and
reserve capacities which would provide them the ability to care for their own health has been significantly reduced
due to the compound crisis and lingering effects of last winter leaving them more exposed and vulnerable.
Needs and resources
Needs in the health sector as a whole are widespread and multi‐factorial; these include deficiencies in all sub‐sector
functional and managerial levels of the system and community infrastructure. Serious gaps exist in community
provision of clean water, sanitation systems and disease prevention; the health system lacks sufficient finances,
infrastructure and management resources; providers lack appropriate resources and opportunity for up‐to‐date
medical information. Proper health care remains unaffordable and inaccessible for many.
There is a need to improve water supply, heating, sewage and waste management systems in the assessed facilities.
Lack of resources to purchase medicines, medical tools and equipment, and to maintain its proper functioning is also
noted. Financial resources of these institutions are very limited; rationalization and optimization of the service
provision and management would help to cut down on wasteful expenditures. Still, it is not reflected in the work
plans of these facilities. Increasing primary health care provision with a focus on family practice and emergency
services should continue to be a priority; this requires provider education, public education and restructuring.
Capacities (What resources and capacities are already present (e.g., infrastructure and institutions) that could
contribute to the response; what are the immediate capacity gaps?)
Human resources continue to have the most potential to improve the situation but are under constant stressors.
Providers and support staff occupy a key element of the health services provision, and make the difference in routine
service provision, system improvement and crisis response. The lack of availability of medical staff is a critical issue at
all levels of the system. The main reasons of health staff outflow are low salaries, difficult working conditions and lack
of benefits. As the result of wide spread labour migration the brain‐drain is increasing and it is forecasted that the
situation will become more challenging.
The majority of facilities have sufficient areas to be able to both accommodate large number of patients and to
develop additional activities. These activities may not directly relate to health services; however, they could serve as
an additional source of support to improve the work of facilities. It is particularly important for the key institutions at
the district level such as all Central Rayon Hospitals and also for some of the regional facilities.
Surge capacity is extremely low or non‐existent, as well even small‐scale emergencies overtax the system;
compounding this is the current compound crisis which is tapping the country’s limited coping capacity.
Current Reponses
The Flash Appeal made a difference for the health sector. The resources that it mobilized allowed the local health
authorities to address the most urgent priority needs and overcome difficulties related to the crisis. Humanitarian
assistance included essential medicines for 120,000 people for three months, generators and heating supplies for
hospitals that sustained essential health services in the most affected regions. Projects were launched on training of
2,748 community health workers to promote and support communicable disease prevention and first aid. All above
activities saved lives; however, humanitarian interventions did not address the underlying chronic health system
issues leaving it in a precarious state with limited capacity to respond to further crises.
Through the Health Cluster, the partners continue to keep each other and the UN Country Team updated on their
progress in project implementation. As lead agency, WHO ensures that Ministry of Health co‐chairs the cluster
meetings and that appropriate mechanisms are in place to support health coordination also at provincial level and
coordination between health and other clusters. WHO, as the provider of last resort, within the limits allowed by the

Tajikistan Rapid Health Assessment, October – November 2008
27
resources available and external constraints, supports partners to overcome obstacles in the implementation of
projects, and to ensure coordinated action to respond to unforeseen gaps or emerging needs.
At the present time, the senior management and the staff promptly respond to emerging problems such as outbreaks
and increase of morbidity rates, collapse of utility systems and damaged equipment. Staff has to deal with these
issues with their own resources and within their capacities with some support from local governments, central
institutions within the system of the Ministry of Health, and through project and programs of local and international
non‐government organizations. Many facilities have received generators provided by the international organizations
to ensure availability of alternative energy sources. Support is also provided to purchase diesel for these generators.
Moreover, general population (usually relatives of patients) also contributes to purchase of diesel for generators, fuel
for transportation of patients, and wood and coal for stoves. Drugs, medical materials and equipment, as well as
trainings of medical and management staff are also provided through various projects and programs. It is also
essential that support is provided to prepare and train the population on health education issues.
The MoH RT has developed plans to mitigate this winter’s impact on health delivery, but due to limited resources the
level of implementation is low especially in rural areas.
Conclusions and Recommendations
Impact of current conditions (What has happened? Is there an emergency situation and, if so, what are its key
features?)
Tajikistan faces deteriorating conditions on multiple levels, which continue to be compounded by both internal and
external factors; all off these have detrimental effects on health status and quality of care, constituting roots causes
of poor health in the country.
It is widely recognised that infant and children under five mortality rates are good indicators of health system’s
performance. In Tajikistan, mortality rates for infants and children under five are the worst in the CIS region44 (65 and
79 per 1,000 live births respectively).
Increasing food and fuel prices, general inflation and global economic conditions, the potential decrease in
remittances, and unemployment serve to increase expenditures while decreasing income; forcing harsh choices for
basic needs. Often health care falls to the side when these choices must be made, but in the most vulnerable groups
cuts are made to food, shelter and basic necessities as well which directly impacts health and resilience to crisis. For
those living below US$ 1 per day there is a recognized close alignment with the lack of adequate water and sanitation
which places this population at high or very high risk for fecal‐oral disease; a case linking a causal relationship can be
made underweight children living under <US$2 per day.45 Until reform and major investment in the agriculture and
food production sectors reverses this downward spiral food insecurity threatens the health and well being of the
population and requires emergency intervention.
The consequences of poorly heated living quarters are well understood. Cold quarters increase the need for calories
to stay warm, thus increasing the need for food expenditures to maintain adequate nutrition. Cold quarters increase
the risk of respiratory illnesses and exacerbate other health problems, a life threatening outcome for the critically ill,
elderly and disabled. Poorly designed and inefficient alternative heat‐sources can also be hazardous producing
pollutants and as a potential cause of trauma. Individuals living below poverty levels are at an increased risk of
exposure to indoor air pollution and the health conditions related to it such as childhood asthma.46
More than a third of the population does not have access to clean drinking water; even improved sources are subject
to breakage and contamination due to the poor state of the delivery infrastructure. This places the population at
44 MICS. UNICEF, 2006 45 Comparative Quantification of Health Risks, Ezzati, M. et al., WHO 2004 46 Comparative Quantification of Health Risks, Ezzati, M. et al., WHO 2004

Tajikistan Rapid Health Assessment, October – November 2008
28
serious risk for disease and is illustrated by the over 1100 documented cases of typhoid occurring in 2008.
Documented cases of diarrheal disease significantly increased during 2008 indicating deterioration in the health
status and increased public health risk.
The growth in infectious diseases is linked to: a) poor or late diagnosis; b) lack of public awareness on disease
prevention; c) high treatment costs. Wide ranges in immunization coverage, including disconcerting districts with low
level of measles vaccination, indicate outlying areas that have significant gaps in vaccination efforts that need to be
sought out and addressed to avoid future outbreak in particularly vulnerable communities.
Malnutrition and micronutrient disorders particularly among pregnant and lactating women and children under 5,
remains a serious problem which has increased during the past ten years. Morbidity in children follow expected
patterns considering food insecurity, prevailing water, sanitation and hygiene conditions. Anemia as reported in
women is concerning especially in women of childbearing age as micronutrient requirements are increased in this
population group.
Population health profile is determined based on the dynamic indicators of morbidity, mortality among different age
groups, and the level of children vaccination and can provide important information which directs adequate
responses and adoption timely decisions. Health information collection and monitoring systems remain weak; it is
necessary to work towards improvement of reliability and regularity of data collection and analysis. This requires
political will, funding and training for data collection, reporting and decision‐making. General practitioners are needed
to fill gaps in patient care delivery. Training should also be provided in emergency care and stabilization, especially to
remote providers of all levels; this is not currently part of the formal medical education system.
Current state of the health delivery system
National, regional and central district hospitals are central in the provision of primary and tertiary health services in
normal conditions and emergency situations. These facilities have adequate space and buildings, more staff and have
better equipment and materials. However, primary health facilities – SUB, rural health centers and medical houses
are much closer to rural population; serving the majority of rural people. Provision of quality and timely primary
health services by these facilities is indispensable for the provision of public health and family centered health care.
Increased attention should be paid to provision of infrastructure and maintenance of water supply system, heating
system, energy, sewage system and waste utilization, as well as to financial resources and human capacities at this
level.
Analysis of available questionnaires showed that there is a high level of access of the population to specialized
facilities at the national and regional levels. Almost half of district and rural facilities are easily accessible for the
population. However, assessment of access to health is not as straightforward as it may seem, this requires further
definition of criteria for accessibility; and a closer look at this issue. It is important to take into account such factors
like financial capacities of the population, roads conditions, state of communication system, referral system
regulations, and links between various facilities; all of these factors are in poor conditions and many types of
impedances to care are actually the case.
Another important factor contributing to improving access to the services is availability of medical transport.
However, apart from physical availability of vehicles, there should also be enough resources to maintain them in
working conditions; which is not generally the case. Rationalization of transport usage and control over it to ensure
vehicles are used according to their purpose is important to maintain response capacities for emergency situations.
Finally medical transport requires specially trained medical providers, with sufficient and appropriate equipment at
their disposal to effectively render emergency medical care. These system components are also lacking as also
indicated by the 2008 “Analysis of the Emergency care capacity”.
While not specifically addresses in the survey, disabled access was identified by several survey teams as an important
issue which was noted during interviews that also influences the accessibility of health facilities, but is usually
neglected – needs of disabled people (some data suggests that there are 2% of disabled people in Tajikistan ‐ 150

Tajikistan Rapid Health Assessment, October – November 2008
29
000). However, it is suggested that this data does not reflect the real situation, since international experience shows
that percentage of disabled population in countries is usually from 5 to 10 %. A household survey in 2008 identified
175 disabled individuals in 1154 households surveyed.47
Land‐line communication remains the most reliable and in many instances only proper maintenance, hook‐ups and
budgeted funds are needed to restore connection. Direct communication for EMS, including base to ambulance to
incident command, should be provided; without proper communication the system is unable to function with any
degree of efficiency.
The Availability of water was subjective in this study, 38% reported adequate water available; but the findings were
similar to the Multi‐Cluster Assessment where only 46% of 184 facilities reported availability of 60 liters per patient
per day. Of note in consideration of the Multi‐Cluster Assessment, their study had a much higher number of rural
medical houses, primarily situated in Zarafshon Valley, represented in the survey than the RHA.
Although, the state of water system, heating, sewage and waste management have been marked as functioning in the
most facilities at the national, municipal and district levels, compared to rural facilities, however, the quality of these
systems is not satisfactory not only in emergency cases but also in regular activities. (Illustrated in Annex XII) Medical
facilities with little to no funding for repairs or winterization available are subject to cold conditions despite
functioning heat sources, which may be minimal. Compounding this is the increasing cost of fuels in general.
District and rural facilities are better supplied with coal and wood which shows their greater capacities to use stoves
and better provision of financial resources for these purposes. Central heating is absent even in cities.
Alternative sources of electric energy are available in the most district, regional and republican facilities. However,
fuel provision as well as repairing and maintenance are still weak. Rural facilities majority of which are outpatient
settings work during the day time. Rural hospitals are provided with generators only in few cases.
Drug supply, storage deficiencies especially in the regions, quality and the burden of costs remain detrimental factors
in patients receiving proper medical treatment. Although in a number of facilities there is a stock of medicines for
emergency cases, the provision of medicines and medical tools as well as the state of equipment is a big issue at all
levels. According to the staff, one of the reasons is lack of budget resources to purchase. There is a need to assess the
availability of essential drugs, medical assets and equipment based on the existent regulations and list of equipment
approved by the Ministry of Health for the facilities of particular level. In the absence of latter, such lists to be
developed, approved and distributed among health facilities for guidance.
Existence of programmes on prevention of diseases, HIV/AIDS, family planning and others are mentioned by the
majority of facilities.
Attraction, motivation and retention of health workers is required within all health sectors; including providers and
management. This is dependent on cooperation with all partners and stakeholders to increase staff status, salary
levels and benefits. Human resources forms the basis for system reform and individual patient care and will depend
on the engagement and ownership of the process by staff at all levels.
What are continuing or emerging threats that may escalate the emergency?
Common and recurring hazards include floods, mudflows, landslides, epidemics, drought, earthquakes, avalanches,
insect infestation and windstorms. Current interagency contingency planning focuses on: a) earthquake, b) epidemic
(avian influenza, c) economic collapse and d) regional instability, as the most likely scenarios with high impact
potential. Cold‐crisis has received much attention after last winter exemplified the real impact extreme cold weather
for an extended period of time can have on service delivery and morbidity; this continues to be a likely scenario due
to the fact that the most recent interventions are short‐term in nature, carrying with them their own high costs, such
47 Multi‐Cluster Assessment, UNDP DRMP, October 2008

Tajikistan Rapid Health Assessment, October – November 2008
30
as fuel. Long‐term durable solutions encompass improvements and interventions that would strengthen the entire
system against multiple threats and increase base‐line operating levels and efficiency.
Clean water and sanitary conditions continue as daily threats for disease to the population as a whole. In the case of
earthquake the resulting infrastructure collapse would immediately create untenable conditions for water availability
and shelter, besides further collapse of the health delivery system. Influx of refugees would create similar conditions
not only for the displaced population but stress the resources of the current resident population.
Nearly 4.5 million people, or more than 70 % of the total population of the country, live in areas at risk of malaria,
making it a priority public health problem. The government shows strong political commitment to roll back malaria,
and national authorities work closely with the WHO Regional Office for Europe in areas of disease management,
vector control, training, surveillance, operational research, health education and community participation. Current
statistics show a significant improvement.
Immediate health gaps
The main health sector gaps are systemic in nature, but are at a critical level with little capacity to cope with crisis.
These underlying chronic health system problems constitute a state of emergency; which require urgent action.
In this respect, the immediate emergency health gaps are:
High‐levels of threat of communicable and non‐communicable diseases due to:
o Very limited clean water supply and poor sanitary services (facilities and practices)
o Nutritional and micro‐nutrient deficiencies especially in vulnerable groups
o Low levels of malaria prevention actions; and gaps in immunization
Health infrastructure unable to provide essential health services for most vulnerable groups, namely maternal
and child health, targeted emergency medical care facilities, communicable and neglected diseases due to:
o Poor structural conditions including water supply, sanitary systems, heating systems, electric supply
o Physical and economic impedances to health care
o Limited availability of equipment (items and maintenance), supplies and medications
o Inefficient medical transport, EMS services and referral services
Poor capacities of health workers and communities to cope and care for the needs of most vulnerable; severely
impacting maternal and child care and critical life‐saving medical interventions due to:
o Inefficient functioning structure, including managerial and financial
o Human resources shortages in critical and isolated areas
o Limited existence and application of standard care guidelines, along with related training of providers
Limited capacity to respond during acute crisis situations and disaster due to:
o Less than fully functional EMS and emergency care services
o Limited or no surge capability in the system
o Limited monitoring and notification system
Response strategy to immediate health gaps (Are interventions required to prevent further harm or loss of life? If so,
what are top priorities?)
As a matter of urgent priority, the response strategy should concentrate on addressing set objectives in critical areas
for the most vulnerable groups:

Tajikistan Rapid Health Assessment, October – November 2008
31
Collaborative efforts with government, donor community and WATSAN cluster partners to find and support
durable solutions to provide clean water and sanitary services. These solutions may entail large infrastructure
support but current conditions require early recovery approaches for provision at the point of consumption and
use.
Ensuring functionality of key health facilities in cases of acute crisis situations. This entails having in place health
service delivery systems in priority maternity hospitals, targeted emergency medical care facilities, and
institutions for communicable and neglected diseases. Development of a fully functional EMS and related
emergency services for daily response is needed to have the ability to respond to and mitigate extraordinary
events.
Providing health workers and community with skills needed to cope with acute crisis situations. This entails
training selected health workers in life‐saving health operations in crises, training and allowing “non‐medical”
responders to provide medical care and providing community volunteers with specific emergency life‐saving
skills. Development and utilization of patient care guidelines for critical care should be standardized across
service levels.
Development of a responsive and efficient health care structure. This entails continuing to bolster and accelerate
the current system reform and reorganisation efforts with concentration on primary and emergency care. It
requires commitment and funds to improve and provide adequate facilities and infrastructure elements to safely
provide care.
Focus, recognition and support for human resources. This involves organizational changes, financial support,
training and provision of resources such as equipment and supplies for staff motivation and retention. Here again
guidelines are needed to standardize care.
Prevention programs. Continued support and expansion of prevention programmes to fill coverage gaps can
significantly influence the health profile of the population.
To implement this strategy and effect real change and outcomes bilateral collaboration must support coordinated
efforts and be aligned with the ongoing health sector reform process. Rapid and mid‐term funding is required to
provide timely critical interventions, tied with sustainable changes and improvements, to prevent escalation of the
chronic disaster and further degradation of the health system. Interventions should focus on multiple levels of care
considering donor and recipient matching aligning this with health care and community structures.
Durable early recovery mechanisms of humanitarian response to rapidly decrease threats to health such as
unsafe water consumption and unsafe and poorly functioning facilities.
Development programs promoting community health programs should be expanded and encouraged; such skills
and activities greatly improve community level coping practices in crisis.
Increased awareness and acknowledgement of infrastructure gaps must lead to serious collaborative planning
with commitments from all sides to make necessary improvements.
Channelling methods of support through with consideration to system structure and relationship to government
and community such as at the National and oblast levels through health system finance reforms; and village level,
through self‐sustaining initiatives, utilizing durable solutions and renewable energy sources (high efficiency stoves
with fuel compactor; from which excess fuel can be sold, clinic owned improved water source, water driven
electric generator; excess power may be sold back to system).
Continue system reforms to increase efficiency and reduce waste through increased managerial capacity,
rationalization and transparency; interventions must consider human resource needs, budget sources, patient
access (physical isolation, financial) and referral services.
Critical services improvements including primary care and EMS development. Early actions should target durable
solutions for maternal and child medical care, emergency intervention, appropriate referrals, preventative
medicine and retaining operational capacity in crisis.

Tajikistan Rapid Health Assessment, October – November 2008
32
Annexes
I. Health facilities with certain humanitarian needs
II. Health facilities that experience shortage of drinking water supply
III. Health facilities that need repair and are in poor physical conditions
IV. Health facilities (44) which do not have electric generators
V. Health facilities (60) which have generators but lacking of fuel for generators
VI. Health facilities (37) which have neither central heating nor other alternatives
VII. Health facilities (45) where waste utilisation is not available | in poor condition | not functioning
VIII. Health facilities (29) without coal and wood stocks
IX. Health facilities (31) without food stock
X. Health facilities (21) without essential drug stocks
XI. Health facilities (9) that confirmed unavailability of supplies – consumables
XII. Comparison of critical infrastructure, supplies and indicators between differing levels of facilities
XIII. Questionnaire

Tajikistan Rapid Health Assessment, October – November 2008
33
Annex I: Health facilities with certain humanitarian needs (Note: health facilities are placed in high‐priority order in different geographical areas)
Оblast/District management coverage availability building heating water sewerage medicine connection Emergency funds
Sogd (37)
1. Zafarabad, Rural District Hospital, Baht
MoH/OHD/CRH/SUB
1308 easy Building n/ a
печное n N missing n n
2. Zafarabad, Rural District Hospital, Sari Bog
MoH/OHD/CRH/SUB
663 easy destroyed y n N Partly available
n n
3 Asht, Rural Health Centre, Gulshan
MoH/OHD/CRH 5479 With obstacles
Damaged/malfunct
‐/altern n N Partly available
n n
4. Spitamen, Health Centre,Platina
MoH/OHD/CRH/RHC
680 easy Damaged/malfunct
‐/n. altern ‐ N Partly available
n n
5. Asht, Rural District Hospital MoH/OHD/CRH 17 992 Very difficult
Damaged/malfunct
‐/altern n Y Partly available
y n
6. Zafarabad, Health Centre, Mirzoobod
MoH/OHD/CRH/SUB
986 easy Damaged/malfunct
n/altern n Y Partly available
n n
7. Matcha, CRH MoH/OHD 97 124 Very difficult
Intact/functioning
n n N Partly available
y n
8. Asht, Rural Health Centre, Аppok
MoH/OHD/CRH 4952 With obstacles
Intact/functioning
n n Y Partly ailable
n n
9. Isfara, CRH MoH/OHD 222601 easy ‐ damaged y Y Partly available
y n
10. Asht, Health Centre, Hishthona MoH/OHD/CRH/RHC
3080 easy Intact/functioning
n/altern n Y Partly available
n n
11. Shahristan, Health Centre,Kuli Kuton
MoH/OHD/CRH 901 Very difficult
Intact/functioning
n n ‐ Partly available
mobile n
12. Spitamen, Rural Health Centre, Akteppa
MoH/OHD/CRH 7826 easy Intact/functioning
damaged n Y Partly available
n n
13. Isfara, Rural Health Centre, Lakkon
MoH/OHD/CRH 6250 Very difficult
Intact/functioning
y/altern n N Partly available
y n
14. Isfara, SES MoH/OHD easy
15. Kanibadam SES MoH/OHD easy
16. Kanibadam CRH MoH/OHD 176 300 easy Intact/functioning
damaged Y Partly available
y y
17. Asht/CRH MoH 128 000 easy Intact/functioning
y/altern N f N f Partly available
y y
18. Asht, Rural Health Centre, Marhamat
MoH/OHD/CRH 4200 easy Intact/functioning
n n Y Partly available
y n

Tajikistan Rapid Health Assessment, October – November 2008
34
Оblast/District management coverage availability building heating water sewerage medicine connection Emergency funds
Sogd (37 Con’t)
19. Asht, Rural Health Centre, Dusti
MoH/OHD/CRH 3200 easy Intact/functioning
n n Y Partly available
y n
20. Asht, Rural Health Centre, Bobodarhon
MoH/OHD/CRH 3900 With obstacles
Intact/functioning
‐/altern n Y Partly available
y n
21. Asht, Health Centre, Dahana MoH/OHD/CRH/RHC
2200 easy Intact/functioning
n n N Partly available
n n
22. Asht, Health Centre, Shaymok MoH/OHD/CRH/RHC
2539 easy Intact/functioning
n n Y Partly available
n n
23. Zafarabad, Rural District Hospital,Baht
MoH/OHD/CRH 4100 easy Intact/functioning
печное n N Partly available
n n
24. Shahristan/CRH MoH/local Hukumat
32219 With obstacles
Intact/functioning
y N f Y ‐ y n
25. Shahristan, Health Centre, Sarabi
MoH/OHD/CRH 2126 With obstacles
Intact/functioning
n n ‐ Partly available
mobile n
26. Spitamen, CRH MoH/OHD 110625 easy Intact/functioning
‐/altern y Y available y y
27. Spitamen, Health Centre No 1Nau
MoH/OHD/CRH 22965 easy Intact/functioning
n/altern y Y Partly available
n n
28. Kayrakum/ Central City Hospital
MoH 38300 easy Intact/functioning
y/altern N f N f available y Y (WHO)
29. Khudjand/ Oblast Clinical Hospital
MoH ‐ easy Intact/functioning
y/altern N f Y Partly available
y Y/ stock
30. Khudjand / Oblast Endocrinological Centre
OHD 2111,2 easy Intact/functioning
y/not altern
f Y available y ‐
31. Khudjand / Oblast Maternity House
MoH/OHD ‐ easy Intact/functioning
y/altern f Y available ‐ ‐
32. Khudjand / Oblast Onkological Centre
MoH 2 200000 easy ‐ ‐ f y available y ‐
33. Khudjand / Child Oblast Clinic Hosp.
MoH ‐ easy Intact/functioning
y/altern f Y available ‐ y
34. Ganchi/CRH MoH/local Hukumat
135 492 easy Intact/functioning
y/altern f y available y n
35. Istravshan/CRH MoH/local Hukumat
215 600 With obstacles
Intact/functioning
y/not altern
N f Y Partly available
y n
36. J.Rasulov/CRH MoH/local Hukumat
112 000 ‐ Intact/functioning
y/altern f Y Partly available
y Y (WHO, RC
37. Khudjand / City Hospital MoH/local Hukumat
2 000000 easy Intact/functioning
y/altern f Y Partly available
y y

Tajikistan Rapid Health Assessment, October – November 2008
35
Оblast/District management coverage availability building heating water sewerage medicine connection Emergency funds
II Khatlon (27)
1. Khamadoni/CRH MoH 120183 easy Damaged/malfunct
‐ N f N f available y y
2. Vakhsh/ CRH MoH/OHD 17245 easy Damaged/malfunct
n/altern N f Y available n n
3. N. Khusrav/ CRH MoH/OHD/local Hukumat
‐ Very difficult
Damaged/malfunct
n N f N f Partly available
‐ n
4 Shahritus/ CRH MoH/OHD 95010 easy Damaged/malfunct
n/altern f Y available n y
5. Jilikul/ CRH MoH/OHD 89500 easy Damaged/malfunct
n/altern N f Y available n ‐
6 Kulyab zone CRH MoH/OHD 83 530 easy Intact/functioning/problem
n/altern N f N f Partly available
y n
7. Vose / CRH MoH 172120 With obstacles
Intact/functioning
n/altern f y y
8. Muminabad CRH MoH/OHD 73 794 easy n/altern N f N f Partly available
y n
9. Kulyab zone Оblast Hospital №2
MoH/OHD 850 000 easy Intact/functioning
n/altern reservoir available y y
10. Khovaling/ CRH MoH/HD/Obl &local Hukumat
43925 With obstacles
Intact/functioning
n N f N f Partly available
y y
11. Dangara/ CRH MoH 112067 easy ‐ n/altern N f F available y
12. Farkhor/ CRH MoH 132298 easy ‐ n/altern f N f Partly available
n ‐
13. Bohtar CRH MoH/OHD 206 000 Very difficult
Intact/functioning
n/altern y ‐ available y ‐
14. Jomi CRH MoH/OHD 128828 easy Intact/functioning
n/altern y Partly available
y n
15. Temurmalik CRH MoH ‐ With obstacles
Intact/functioning
n/altern N f N f Partly available
n n
16. Kabadiyan/ CRH MoH/OHD 142612 easy ‐ n/altern f ‐ available n ‐
17. KT Zone: Kurgan‐Tube Hospital №1
MoH/OHD 1120000 easy Intact/functioning
n/altern problem затрудн Partly available
y n
18. Pyandj CRH MoH/OHD 96 400 With obstacles
Intact/functioning
n y be out a repair
Partly available
n n
19. Yovon / CRH MoH/OHD/local Hukumat
‐ With obstacles
Intact/functioning
n/altern N f N f missing n n
20. Nurek/ CRH MoH/OHD 44937 easy Intact/functioning
alternat f F Partly available
n ‐

Tajikistan Rapid Health Assessment, October – November 2008
36
Оblast/District management coverage availability building heating water sewerage medicine connection Emergency funds
II Khatlon (27 Con’t)
21. Huroson/ CRH MoH/OHD 86500 easy Intact/functioning
alternat N f N f available n n
22. Baldjuvan/ CRH MoH ‐ With obstacles
Intact/functioning
y N f N f available n n
23. Shurobod/ CRH MoH 50600 With obstacles
Intact/functioning
y f ‐ available y y
24. Sarband CRH MoH/OHD 36417 easy Intact/functioning
y Y partly Partly available
y n
25. Kurgan‐Tube City Hospital MoH/OHD 200000 easy Intact/functioning
y/altern y f Partly available
y n
26. Kumsangir/ CRH MoH/CRH 99533 ‐ ‐ ‐ ‐ ‐ ‐ y
27. Rumi/ CRH MoH/OHD 147119 easy Intact/functioning
y/altern f f Partly available
n n
Оblast/District management coverage availability building heating water sewerage medicine connection Emergency funds
III RRS (17)
1. Rasht, RHC Vorinj MoH 1 586 With obstacles
Building n/ a
n n n Partly available
n n
2. Rasht, Health Centre Safedob MoH 765 With obstacles
Building n/ a
n n n missing n n
3. Rasht,Health Centre Voydara MoH 1 800 easy Damaged/malfunct
n n N f Partly available
n n
4. Rasht,Rural District Hospital MoH 13 000 easy Damaged/malfunct
damaged n n available n n
5. Hissar, CRH MoH 235 913 Very difficult
Intact/functioning
destroyed destroyed
f available y ‐
6. Rasht, Rural District Hospital, Yarhichi Miyona
MoH 1 200 easy Intact/functioning
7. Rasht, Health Centre Dahana MoH 424 easy Intact/functioning
n n n Partly available
n n
8. Rasht, Health Centre Varzigun MoH 734 With obstacles
Intact/functioning
n n n Partly available
n n
9. Rasht, Health Centre Mullobadal
MoH 516 With obstacles
Intact/functioning
n n n Partly available
n n
10. Rasht, Health Centre, Sangi Maliki
MoH 1 300 With obstacles
Intact/functioning
n n n missing y n
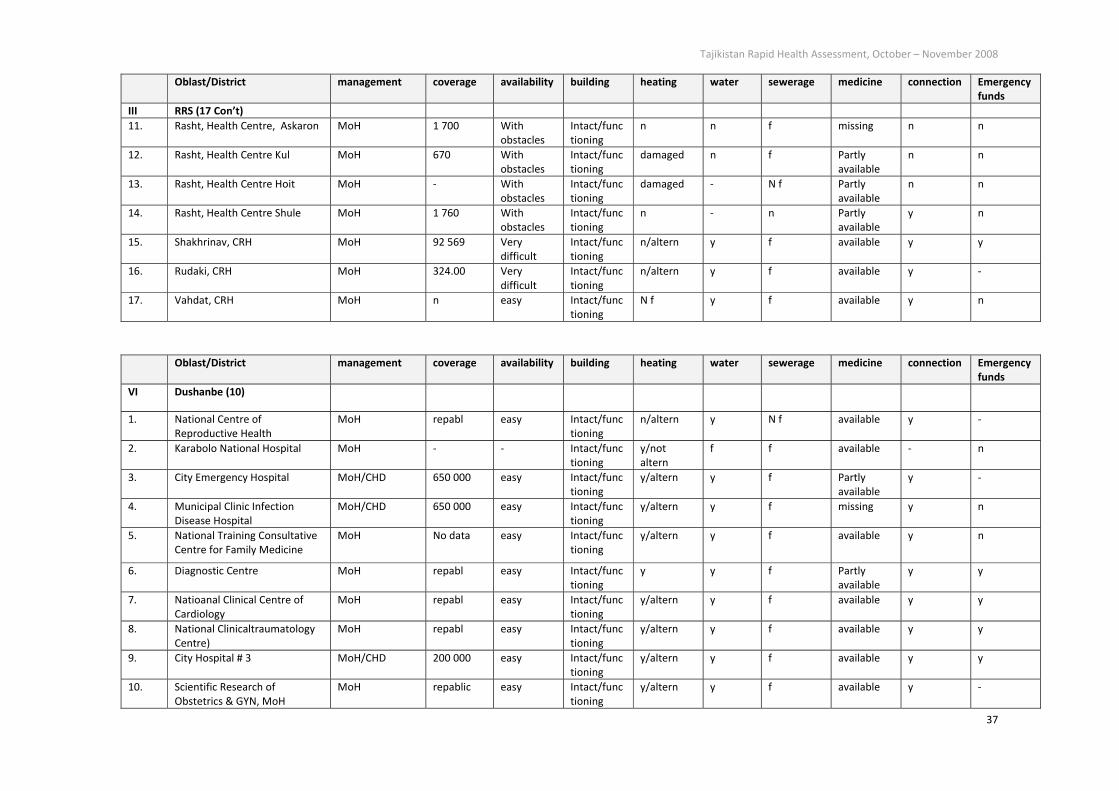
Tajikistan Rapid Health Assessment, October – November 2008
37
Оblast/District management coverage availability building heating water sewerage medicine connection Emergency funds
III RRS (17 Con’t)
11. Rasht, Health Centre, Askaron MoH 1 700 With obstacles
Intact/functioning
n n f missing n n
12. Rasht, Health Centre Kul MoH 670 With obstacles
Intact/functioning
damaged n f Partly available
n n
13. Rasht, Health Centre Hoit MoH ‐ With obstacles
Intact/functioning
damaged ‐ N f Partly available
n n
14. Rasht, Health Centre Shule MoH 1 760 With obstacles
Intact/functioning
n ‐ n Partly available
y n
15. Shakhrinav, CRH MoH 92 569 Very difficult
Intact/functioning
n/altern y f available y y
16. Rudaki, CRH MoH 324.00 Very difficult
Intact/functioning
n/altern y f available y ‐
17. Vahdat, CRH MoH n easy Intact/functioning
N f y f available y n
Оblast/District management coverage availability building heating water sewerage medicine connection Emergency funds
VI Dushanbe (10)
1. National Centre of Reproductive Health
MoH repabl easy Intact/functioning
n/altern y N f available y ‐
2. Karabolo National Hospital MoH ‐ ‐ Intact/functioning
y/not altern
f f available ‐ n
3. City Emergency Hospital MoH/CHD 650 000 easy Intact/functioning
y/altern y f Partly available
y ‐
4. Municipal Clinic Infection Disease Hospital
MoH/CHD 650 000 easy Intact/functioning
y/altern y f missing y n
5. National Training Consultative Centre for Family Medicine
MoH No data easy Intact/functioning
y/altern y f available y n
6. Diagnostic Centre MoH repabl easy Intact/functioning
y y f Partly available
y y
7. Natioanal Clinical Centre of Cardiology
MoH repabl easy Intact/functioning
y/altern y f available y y
8. National Clinicaltraumatology Centre)
MoH repabl easy Intact/functioning
y/altern y f available y y
9. City Hospital # 3 MoH/CHD 200 000 easy Intact/functioning
y/altern y f available y y
10. Scientific Research of Obstetrics & GYN, MoH
MoH repablic easy Intact/functioning
y/altern y f available y ‐

Tajikistan Rapid Health Assessment, October – November 2008
38
Оblast/District management coverage availability building heating water sewerage medicine connection Emergency funds
V GBAO (16)
1. Oblast Hospital, Khorog MoH/OHD 220 000 Very difficult
Damaged/malfunct
n d
Partly available
y n
2. TB CentralHospital MoH/OHD 220 000 Very difficult
Damaged/
malfunct
n
damaged
Not clear situation
Partly available
y ‐
3. Oblast Endocrinological Centre MoH/OHD 220 000 Very difficult
Damaged/
malfunct
n n Not clear situation
missing y ‐
4. Oblast oncology hospital MoH/OHD 220 000 Very difficult
Damaged/malfunct
N f N f N f Partly available
y n
5. Oblast Dermatovenerology department
MoH/OHD Very difficult
Damaged/malfunct
n y Not clear situation
Partly available
y n
6. Oblast Reproductive Centre MoH/OHD 220 000 Very difficult
destroyed N f f Not clear situation
missing y n
7. Shugnan, CRH MoH/OHD 34548 Very difficult
destroyed N f N f N f Partly available
y n
8. Oblast Narcological Dep't MoH/OHD 220 000 Very difficult
Damaged/malfunct
n/altern/boller sistem
n Not clear situation
missing y n
9. Oblast ophthalmologic hosp. MoH/OHD 220 000 Very difficult
Damaged/malfunct
y/not altern
partly f available y n
10. Rushan, Derrushan, MH MoH/OHD/CRH 1286 Very difficult
Damaged/malfunct
N f N f N f Partly available
n Funds in local Hukumat
11. Khorog, Murgab, CRH MoH/OHD 14013 Very difficult
Damaged/malfunct
n/altern N f N f Partly available
y n
12. Oblast Cardiological Centre MoH/OHD 220 000 Very difficult
норм
n y f Не доступ y n
13. Khorog, City Health Centre MoH/OHD 28 000 easy Intact/functioning
n N f N f Partly available
y n
14. Darvaz, CRH MoH/OHD 24700 Very difficult
Intact/functioning
N f f N f Partly available
y n
15. Roshtkala, CRH MoH/OHD 22155 Very difficult
Intact/functioning
n N f N f Partly available
y n
16. Oblast SES MoH/OHD 220 000 Very difficult
‐ y n Not clear situation
Not acceptable
y n

Tajikistan Rapid Health Assessment, October – November 2008
39
Annex II: Health facilities that experience shortage of drinking water supply
Water supply is shortly available | needs repair Water supply is not available | system doesn’t function
Sogd Province: Isfara Lakkon Health Centre, Asht
CRH, Kanibadam CRH, Kayrakum City Central
Hospital.
RRS: Kalai Surkh Sub‐District Hospital of Rasht valley,
Rudaki CRH, Khuroson CRH.
Khatlon Province: KT Oblast Hospital, Sarband CRH,
Rumi CRH, Jilikul CRH, Khamadoni CRH, Kulyab Oblast
Hospital and Kulyab CRH.
GBAO: Khorog Oblast Ophthalmology Hospital
Sogd: Spitamen District, Plotina Health Centre and
Rural Health Centre of Akteppa Jamoat, RHC of
Bobodarkhon, Appok, Gulshan, Dusti, Markhamat,
SUB village clinic, Medical Houses of Dahana,
Shaidok, Hishthona Jamoats of Asht district; CRH,
Medical Houses of Kuli Kuton & Sarobi of Shahristan
district, Matcha CRH, Rural District Hospital, three
Health Centres of Mirzoobod, Sariboh and Zafarabad
district.
RRS: HCs of Kul, Voidara, Askalon, Maliki, Safedob,
Varzigun, Mullobadan, Hoit Jamoats, RHCs of Vorinj,
Shule, Sub‐District Hospital of Miyona Jamoats of
Rasht Valley.
Khatlon Province: Yovon CRH, Vakhsh CRH, Nosiri
Khusrav CRH, Temurmalik CRH, Baljuvan and
Khovaling CRH.
GBAO: CRH of Roshtkala, Shugnan, Murgab, Khorog
TB Central Hospital, Oblast Narcological Department,
Oblast Oncology hospital, Oblast Dermatovenerology
Department, Oblast Reproductive Centre, Oblast
Endocrinological Centre, SES, City Health Centre.

Tajikistan Rapid Health Assessment, October – November 2008
40
Annex III: Health facilities that need repair and are in poor physical conditions
Geographical
Zone
Needs Repair In Poor Condition | Non‐
Functional
Doesn’t have its own
building
Sogd Province: (1) Khujand Oblast Clinic Hospital, (2)
Spitamen, Jamoat “Plotina”, (3) Asht
SUB village clinic, (4) Matcha CRH, in
Zafarabad Health Centres of (5)
Mirzoobod and (6) Saribogh Jamoats
‐ 0 ‐
(1) Health Centre of
Zafarobod district
RRS (1) Kalai Surkh Sub‐District Hospital (1) HC, Voidara Jamoat,
Rasht Valley
Rasht Valley: (2) Vorinj and
(3) Safebod village health
centres
Dushanbe ‐ 0 ‐ (2) National Centre of
Reproductive Health
‐ 0 ‐
Khatlon (1) Jilikul, (2) N. Khusrav, (3)
Khamadoni, (4) Kulyab district, (5)
Muminobad CRHs
(1) Vakhsh, (2) Shahritus
CRHs
‐ 0 ‐
GBAO (1) Shugnan CRH, (2) Oblast
Dermatovenerology Department in
Khorog
(1) Murgab CRH, (2) Khorog
Oblast Hospital, (3) TB
Central Hospital, (4) Oblast
Narcology Department, (5)
Oblast Oncology
Department, (6) Oblast
ophthalmologic hospital, (7)
Oblast Reproductive Centre,
(8) Oblast Endocrinological
Centre, (9) Medical House
of Derrushan Jamoat of
Rushan District

Tajikistan Rapid Health Assessment, October – November 2008
41
Annex IV: Health facilities (44) that do not have electric generators
Geographical zone Name of the health facility
Sogd Province Spitamen District: (1) Health Centre, Nau; (2) Health Centre Akteppa; (3) Health Centre,
Plotina;
Isfara District: (4) Health Centre of Lakkon Jamoat; (5) SES;
Asht District: (6) RHC, Bobodarkhon, (7) RHC Appok, (8) RHC Gulshan, (9) RHC Dusti, (10)
RHC Markhamat, (11) Medical Houses of Dahana, (12) Medical House Shaidok, (13)
Medical House of Hishthona;
Shahristan District: (14) Medical Houses of Kuli Kuton & (15) Sarobi;
Zafarabad District: Health Centres of (16) Saribogh, (17) Mirzoobod and (18) Zafarabad
district centre.
Rayons of Republican
Subordination (RRS)
Rasht Valley: (19) Sub‐District Hospitals of Khalai Surkh, (20) Yarhichi Miyona, (21) Rural
Health Centres of Shule, (22) Vorinj, Health Centres of (23) Varzigun, (24) Safedob, (25)
Sangi Maliki, (26) Askalon, (27) Kul, (28) Dahana, (29) Mullobadan and (30) Hait
Jamoats.
Dushanbe city (31) National Training Consultative Centre for Family Medicine, (32) National Centre on
Reproductive Health.
Gorno‐Badakhshan
Autonomous Oblast
(GBAO)
Roshtkala District: (33) CRH Roshtkala,
Shugnan District: (34) CRH Shugnan.
Khorog: (35) Oblast Ophthalmologic Hospital, (36) Oblast Narcological Department, (37)
Oblast Oncology Hospital, (38) Oblast Dermatovenerology Department, (39) Oblast
Reproductive Centre, (40) Oblast Endocrinological Centre, (41) SES, (42) Khorog City
Health Centre.
Darvaz District: (43) Darvaz CRH,
Rushan District: (44) Medical House of Derrushan Jamoat

Tajikistan Rapid Health Assessment, October – November 2008
42
Annex V: Health facilities (60) which have generators but lacking of fuel for generators
Geographical Zone Fuel available for 10 days operation Fuel is not available
Dushanbe (1) City Hospital No 3; (2) Natioanal Clinical Centre of
Cardiology; (3) Municipal Clinic Infection Disease
Hospital; (4) City Emergency Hospital; (5) National
Clinicaltraumatology Centre; (6) Diagnostic Centre;
(7) Karabolo National Hospital; (8) Scientific
Research of Obstetrics & GYN of the MoH
RRS (1) Hissar CRH; (2) Rudaki CRH (1); Vahdat CRH; (2) Voidara Jamoat,
Rasht Valley
Sogd Province Khujand city: (1) Oblast Clinical Hospital; (2) Child
Oblast Clinic Hospital; (3) Oblast Maternity House;
(4) Oblast Onkological Centre; (5) Spitamen CRH; (6)
Isfara CRH; Asht: (7) CRH, (8) SUB (Village Clinic); (9)
Shahristan CRH; (10) Matcha CRH; (11) J. Rasulov
CRH; (12) Istravshan CRH; (13) Ganchi CRH; (14)
Kanibadam CRH; (15) Kayrakum Central City
Hospital; (16) RDH, Baht Zafarabad District.
(1) Khujand City Hospital No1.
Khatlon Province CRHs: (1) Yovon, (2) Khuroson, (3) Jomi, (4) Bokhtar,
(5) Vakhsh, (6) Rumi, (7) Jilikul, (8) Kobodiyon, (9)
Shahrituz, (10) Pyandj; (11) Khamadoni, (12)
Dangara, (13) Nurek, (14) Kulyab District; (15) Kulyab
Oblast Hospital; (16) Khovaling, (17) Shurobod, (18)
Baljuvan, (19) Muminobad; (20); Temurmalik (21) KT
Oblast Hospital; (22) KT City Hospital.
(1) Farkhor CRH; (2) Vose CRH; (3) N.
Khusrav CRH; (4) Kumsangir CRH; (5)
Sarband CRH.
GBAO (1) CRH Murghab, (2) Khorog TB Central Hospital (1) Oblast Hospital; (2) Oblast
Cardiological Centre

Tajikistan Rapid Health Assessment, October – November 2008
43
Annex VI: Health facilities (37) which have neither central heating nor other alternatives
Geographical zone Name of the health facility
Dushanbe (1) (1) Scientific Research of Obstetrics & GYN of the MoH
RRS (12) (1) Shahrinav CRH, (2) Vahdat CRH, (3) Rudaki CRH; Rasht: HCs of (4) Kul, (5) Dahana, (6)
Mullobadan, (7) Hoit, (8) Shule Rural Health Centre, (9) Vorinj RHC, (10) Varzigun Health
Centre, (11) Safedob HC, (12) Sangi Maliki HC
Sogd (9) HCs of (1) Mirzoobod, (2) Saribogh, (3) Zafarabad district, (4) Matcha CRH, (5) Kuli Kuton &
(6) Sarobi MH of Shahristan district; (7) Dahana MH, (8) Appok RHC of Asht District and (9)
Plotina HC of Spitamen District.
Khatlon (2) (1) Khovaling CRH; (2) Bokhtar CRH
GBAO (13) (1) Derrushan MH of Rushan District; (2) Darvaz CRH; (3) Khorog City Health Centre; (4)
Oblast Cardiological Centre; (5) Oblast ophthalmologic hospital; (6) Oblast Narcological
Department; (7) Oblast oncology hospital; (8) Oblast Dermatovenerology Department; (9)
Oblast Reproductive Centre; (10) Oblast Endocrinological Centre; CRHs of (11) Roshtkala;
(12) Shugnan; (13) Murgab.
Annex VII: Health facilities (45) where waste utilisation is not available | in poor condition | not functioning
Geographical zone Name of the health facility
RRS (10) Rasht: (1) Kalai Surkh Sub‐District Hospital, RHC of (2) Shule & (3) Vorinj; HCs of (4) Varzigun,
(5) Safedob, (6) Sangi Maliki (7) Voidara, (8) Dahana, (9) Mullobadan, Hoit.
Sogd (13) (1) HC Plotina, Spitamen; (2) HC Lakkon, Isfara; (3) Asht CRH; (4) Gulshan & (5) Dusti RHC of
Asht; (6) Dahana MH of Asht; (7) Matcha CRH; (8) J. Rasulov CRH; (9) Kayrakum Central City
Hospital; (10) Baht RDH in Zafarabad; (11) Mirzoobod , (12) Saribogh and (13) Zafarabad
district HCs.
Khatlon (9) (1) Yovon CRH; (2) N. Khusrav CRH; (3) Nurek CRH, (4) Khamadoni CRH; (5) Temurmalik CRH,
(6) Farkhor CRH; (7) Khovaling CRH; (8) Shurobad CRH; (9) Baldjuvan CRH
GBAO (13) (1) Derrushan MH of Rushan District; (2) Oblast Dermatovenerology Department; (3) Oblast
Reproductive Centre; (4) Oblast Endocrinological Centre; (5) SES; (6) City Health Centre; (7)
Oblast Hospital; (8) TB CentralHospital; (9) Oblast Cardiological Centre; (10) Oblast
Ophthalmologic Hospital; (11) Oblast Narcological Department; (12) Roshtkala CRH; (13)
Shugnan CRH.

Tajikistan Rapid Health Assessment, October – November 2008
44
Annex VIII: Health facilities (29) without coal and wood stocks
Geographical zone Name of the health facility
Dushanbe (7) (1) Republican Cardiology Hospital; (2) Diagnostic Centre; (3)Republican Clinical Hospital #3
named after Dyakov; (4)National Traumatology Centre; (5)National Training and Clinical
Centre for Family Medicine; (6) Scientific and Research Centre for Mother and Child Health;
(7) National Reproductive Health Centre.
RRS (4) (1) Rasht, Medical House in Varzigun; (2) Rasht, Medical House in Sangi Maliki; (3) Rasht,
Medical House in Dagana; (4) Rasht, Medical House in Mulobadan.
Sogd (6) (1) Regional Clinical Hospital; (2) Regional Maternity House; (3) Regional Oncology Centre;
(4) Spitamen, Medical House ’Platina’; (5) Spitamen, Rural Health Centre #1; (6) Matcha,
CRH.
Khatlon (3) (1) Khatlon Regional Hospital; (2) Qurgan‐Tube City Hospital; (3) CRH, Sarband
GBAO (9) (1) Regional Cardiology Hospital; (2) Regional Ophthalmology Hospital; (3) Regional
Narcology Hospital; (4) Regional Oncology Hospital; (5) Regional Derma‐Venerological
Hospital; (6) Regional Endocrinology Hospital; (7) Regional Reproductive Health Centre; (8)
SES; (9) City Centre for Family Medicine.
Annex IX: Health facilities (31) without food stock
Geographical zone Name of the health facility
Dushanbe (7) (1) Republican Cardiology Hospital; (2) Diagnostic Centre; (3)Republican Clinical Hospital #3
named after Dyakov; (4)National Traumatology Centre; (5)National Training and Clinical
Centre for Family Medicine; (6) Scientific and Research Centre for Mother and Child Health;
(7) National Reproductive Health Centre.
RRS (5) (1) Rasht, SUB Kalai Surkh; (2) Rasht, SUB Yakhchii Miyona; (3) Sharinav, CRH; (4) Vahdat,
CRH; (5) Rudaki, CRH
Sogd (8) (1) Regional Maternity House; (2) Isfara, CRH; (3) Shahristan, CRH; (4) Matcha, CRH; (5)
J.Rasulov, CRH; (6) Zafarabad, SUB ‘Bakht’; (7) Zafarabad, Medical House Saribog; (8)
Zafarabad, Medical House, Mirzoobod
Khatlon (5) (1) Yavan, CRH; (2) Vakhsh, CRH; (3) Timur Malik, CRH; (4) Shurabad, CRH; (5) Boljuvan, CRH
GBAO (6) (1) Regional Hospital; (2) Regional TB Hospital; (3) Regional Cardiology Hospital; (4) Regional
Narcology Hospital; (5) Regional Oncology Hospital; (6) Regional Endocrinology Hospital

Tajikistan Rapid Health Assessment, October – November 2008
45
Annex X: Health facilities (21) without essential drug stocks
Geographical zone Name of the health facility
Dushanbe (1) (1) Scientific and Research Institute of Mother and Child Health
RRS (5) (1) Rasht, SUB Kalai Surh; (2) Rasht, Medical House Varzigun; (3) Rasht, Medical House
Safedoron; (4) Rasht, Medical House Askalon; (5) Rasht, Medical House Voidara
Sogd (8) (1) Asht, RHC Gulshan; (2) Asht, RHC Marhamat; (3) Asht, SUB; (4) Asht, Medical House
Dahana; (5) Asht, Medical House Shaimok; (6) Shahristan, Medical House Kuli Kuttan; (7)
Zafarabad, SUB Baht; (8) Zafarabad, Medical House Baht; (9) Zafarabad, Medical House
Mirzoobod; (10) Zafarabad, Medical House Saribog
Khatlon (1) (1) Yavan
GBAO (6) (1) Regional Cardiology Hospital; (2) Regional Narcological Hospital; (3) Regional Oncology
Hospital; (4) Regional Derma‐Venerological Hospital; (5) Regional Reproductive Health
Centre; (6) Regional Endocrinology Hospital
Annex XI: Health facilities (9) that confirmed unavailability of supplies ‐ consumables
Geographical zone Name of the health facility
Dushanbe (1) (1) Diagnostic Centre
Sogd (3) (1) Dahana MH, Asht, (2) Sarobi MH, Shahristan; (3) Saribogh HC, Zafarabad
Khatlon (1) (1) Nosiri Khusrav CRH
GBAO (4) (1) Khorog TB CentralHospital; (2) Oblast Cardiological Centre; (3) Oblast Narcological
Department; (4) Khorog City Health Centre

Tajikistan Rapid Health Assessment, October – November 2008
46
Annex XII: Comparison of critical infrastructure, supplies and indicators between differing levels of facilities
48 National level facilities – 7; Oblast level facilities – 17; City level facilities – 7: 31 facility = 100%. 49 CRH – 43 = 100%; 50 Rural level facilities ‐ 33 = 100%, including SUB = 4; RHC = 10; MH =19. 51 This is not applicable to Obast, National and City level facilities as vaccination is the major responsibility of outpatient facilities (polyclinics)
Oblast (%), including city &
national level facilities48
CRH (%)49 SUB/RMHs (%)50
1. Easy physical access 84 49 52
2. Medical transport available 19 42 15
3. Land‐line communication 71 67 3
4. Functioning infrastructure 58 60 67
5. Water available 61 44 6
6. Generator 65 86 9
7. Functioning heating system 35 14 9
Only alternative available 26 42 24
8. Coal or wood available 26 88 73
9. Functioning toilets 61 42 27
10. Functioning waste management 65 58 27
11. Essential drugs ‐available 29 35 9
‐ Partly available 45 51 46
12. Consumables ‐available 32 26 36
‐ Partly available 48 60 52
13. Staff ‐ available 10 2 27
‐ partly available 16 14 42
14. Measles coverage >90% N/A (16)51 42 58

Tajikistan Rapid Health Assessment, October – November 2008
47
Annex XIII: Rapid Health Assessment - Health Facility Questionnaire SURVEY OBJECTIVE: RAPID SURVEY OF THE FOLLOWING, WITH CONCENTRATION ON PRIMARY HEALTH CARE AND EMERGENCY
SERVICES, IN PARTICULAR, ACCESS TO QUALITY CARE; INFRASTRUCTURE (ENERGY/ELECTRICITY AND WATER SUPPLY AND STRUCTURAL/FUNCTIONAL RESILIENCE); MOTHER AND CHILD MALNUTRITION AND ILLNESS; MORBIDITY AND MORTALITY RELATED TO COMMUNICABLE DISEASES, FOCUSING ON SURVEILLANCE AND EARLY WARNING
SYSTEMS; MANAGEMENT, HUMAN RESOURCES, PROVISION OF MEDICINES AND MEDICAL COMMODITIES; COORDINATION AND DISASTER READYNESS;
TO YIELD EVIDENCE BASED DATA ON THE CURRENT OPERATIONAL SITUATION, BASED ON THE MOST RECENT DATA AVAILABLE, WITHIN
THE PAST WEEK OR MONTH.
OVERVIEW: DATA TIMEFRAMES ARE DEFINED IN THE PARTICULAR QUESTIONS; PERCENTAGES MAY BE ESTIMATED; INDICATE WHETHER
DATA IS TAKEN FROM PATIENT CARE RECORDS OR ESTIMATED IF DATA IS UNAVAILABLE, INDICATE IF FACILITY WILL PROVIDE WITHIN A FEW DAYS, UNKNOWN OR NOT APPLICABLE (N/A)
FOR THAT PARTICULAR FACILITY
1. PUBLIC HEALTH: QUESTIONS CONCERNING REGION/COMMUNITY/VILLAGE PUBLIC HEALTH SITUATION IN THE AFFECTED
AREA 1.1 ACCESS TO HEALTH SERVICES:
1.1.1 Place of interview: AREA TYPE (Region, district, rural):
Resource person Position/Title:
Assessor : Agency:
1.1.3 Who manages the facility?
□ Ministry of Health
□ Other (specify)
1.1.4 Physical access to that facility (check one):
□ Easy
□ With obstacles (Explain)
□ Very difficult (Explain)
Total area included (square km):
Furthest distance in km to the facility: ……
Greatest number of hours by normal means of transport (specify): …..
1.1.5 Who else provides health care services for the community?
□ Community Health Worker
□ Traditional Healer
□ Traditional Birth Attendant
□ Other

Tajikistan Rapid Health Assessment, October – November 2008
48
1.1.6 Are there any planned activities by the community/local/government?
□ Community
□ Local government
□ National government
□ Other
1.1.7 Current humanitarian interventions if any (includes human resources, medications, vaccines, mosquito nets, re-hydration salts for diarrhoea, blankets etc.)
Organization :
1
2
3
4
Main activity:
1.2 PUBLIC HEALTH PROFILE (FOR SURVEY AREA):
SOURCE: AREA TYPE (1.1.A):
Morbidity (disease in population)
1.2.1 Main health concerns for CHILDREN reported by health professionals
Typically includes malaria, diarrhoea, respiratory infections, malnutrition... (list) *from clinic records □
1.
%
2
%
3
%
1.2.2 Main health concerns for WOMEN reported by health professionals *from clinic records □
1.
%
2
%
3
%
1.2.3 Main health concerns for ADULT POPULATION reported by health professionals *from clinic records □
1.
%
2
%
3
%

Tajikistan Rapid Health Assessment, October – November 2008
49
1.2.4 Have there been any reports of any outbreaks or unusual increases in illness? These may include typhoid, cholera, measles, hepatitis, brucellosis; during the current year, include number of cases:
□ No
□ Yes (Specify)
1.2.5 Have there been cases of trauma or injury e.g. fractures, burns, fractures during the past month? If so, specify the main types and specify if few or many
□ No
□ Yes (Specify)
1.2.6 Were there cases of burns, frostbite or CO poisoning during the current year? If so, specify the main types and specify if few or many
□ No
□ Yes (Specify)
Burns: Frostbite: CO poisoning:
1.2.7 Have there been reports of sexual and gender based violence during the past month?
□ No
□ Yes (Specify)
1.2.8 Have there been reports of non-infectious agents (such as cold, heat, radiation, poisons or toxins) during the past month?
□ No
□ Yes (Specify)
1.2.9 Reported cases acute or chronic malnutrition during the past month? *from clinic records □
□ No
□ Yes (Specify population)
1.2.10 Current manifestations of psychosocial needs among the affected population the past month? If so, describe.
□ No
□ Yes (Specify)
1.2.11 Major causes of morbidity during the past month: *from clinic records □
1.
%
2.
%
3.
%
4.
%
5.
%
6.
%

Tajikistan Rapid Health Assessment, October – November 2008
50
1.2.12 Major documented changes in morbidity from clinic records (if known:
Hospital/clinic admissions 2007: year to date:
Cause: 2007 year to date:
Road accidents
Burns
Malaria
Diarrhoeal disease
Neonate fever/sepsis
Postpartum hemorrhage
Eclampsia
Suicide
Disease Control and Prevention
1.2.13 Local vaccination rate of under-5s. Rate = #of children from age 6 months-5 years vaccinated for measles/the total children age 6 months-5 years x 100.
Measles vaccination rate: ____ %
Pentavalent vaccination rate: ____ %
Hepatitis B/C vaccination rate: ____ %
Polio vaccination rate: ____ %
BCG vaccination rate: ____ %
1.2.14 Existence of special disease control programmes? Prevention programmes commonly include vaccinations, hygiene promotions, condoms from prevention of HIV/AIDS etc.(specify)
□ No
□ Yes Specify)
1.2.15 State any delay, disruption or cancellation of disease control programmes last winter 2007/2008? (specify)

Tajikistan Rapid Health Assessment, October – November 2008
51
MORTALITY (deaths). Crude Mortality Rate thresholds: General population: 1 x 10000/day; Under-5: 2 x 10000/day in the community (area surveyed)
1.2.16 Existence of mortality surveillance (is the community counting deaths?) □ Yes □ No
Crude:
Under‐5:
Infant:
FACILITY NAME AND TYPE (CENTRAL RAYON HOSPITAL, RURAL CLINIC,
MEDICAL HOUSES, RURAL DISTRICT HOSPITAL, OBSTETRIC ETC.):
1.2.17 Number of ADULT deaths (people aged 5 and over)and main 3 causes.
*from clinic records □
Last seven (7) days: September 2008
1.
%
2.
%
3.
%
1.2.18 Number of MATERNAL deaths due to lack of access to skilled health providers for a safe delivery
*from clinic records □
Last seven (7) days: September 2008
1.2.19 Number of CHILDREN UNDER-5 deaths in the last seven days and main 3 causes.
*from clinic records □
Last seven (7) days: September 2008
1.
%
2.
%
3.
%
1.2.20 Was there a change in the mortality pattern since the beginning of the current year?
□ No
□ Yes (Must Specify data source and specific timeframe used)
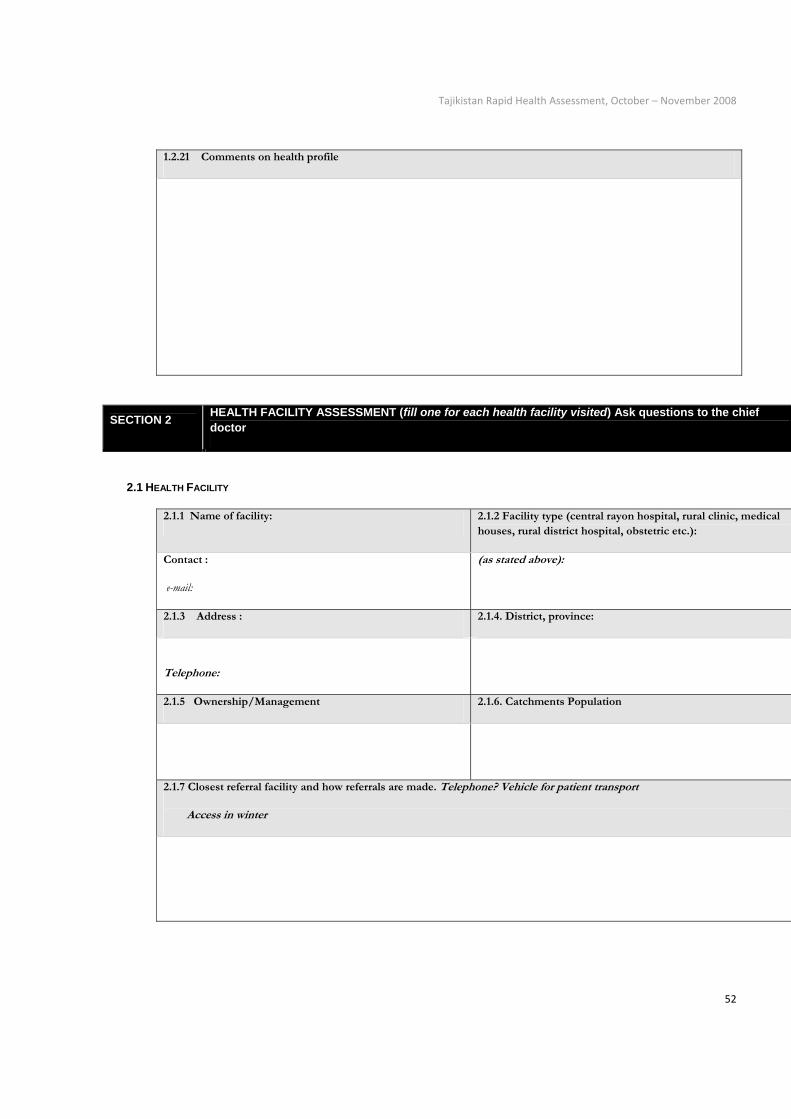
Tajikistan Rapid Health Assessment, October – November 2008
52
1.2.21 Comments on health profile
SECTION 2 HEALTH FACILITY ASSESSMENT (fill one for each health facility visited) Ask questions to the chief doctor
2.1 HEALTH FACILITY
2.1.1 Name of facility: 2.1.2 Facility type (central rayon hospital, rural clinic, medical houses, rural district hospital, obstetric etc.):
Contact :
e-mail:
(as stated above):
2.1.3 Address : 2.1.4. District, province:
Telephone:
2.1.5 Ownership/Management 2.1.6. Catchments Population
2.1.7 Closest referral facility and how referrals are made. Telephone? Vehicle for patient transport
Access in winter

Tajikistan Rapid Health Assessment, October – November 2008
53
2.2. RESOURCES
2.2.1 Infrastructure (e.g. building, heating, running water, sanitation, waste disposal, electricity):
Intact/functioning
Damaged/malfunctioning Destroyed
Availability of emergency operational funds Alternative heating devices Running water inside hospital Running water supplied to surgical department 60 litres per patient/day supplied Waste Disposal: Excreta disposal – presence or absence of functioning toilets, septic tanks; Sharps disposal – (syringes, glass) Is there is an agreement with the Power Energy Department on supply of
Electricity Hot water
State of the heating system Measures on power saving Back-up Generator present Number available
Fuel available (10 days of operation): Coal or wood stock Is there a stock of foodstuffs (potato, onion, oil, flour)?
□Yes □No What duration of time: from what level (source):
□Yes □No Fuel available: □Yes □ No specify type: □Yes □No Describe condition of water supplied and system:
□Yes □No
□Yes □No
□ Present □ Absent On every floor □Yes □ No □Yes □No □Yes □No □Yes □No Describe (give specifics) describe: □Yes □No If Yes, Specify:
□Yes □No Size(s): 1) 2) 3) # 4) 5) 6) □Yes □ No If Yes, Specify type: □Yes □ No □ N/A Specify: □Yes □ No If Yes, Specify:
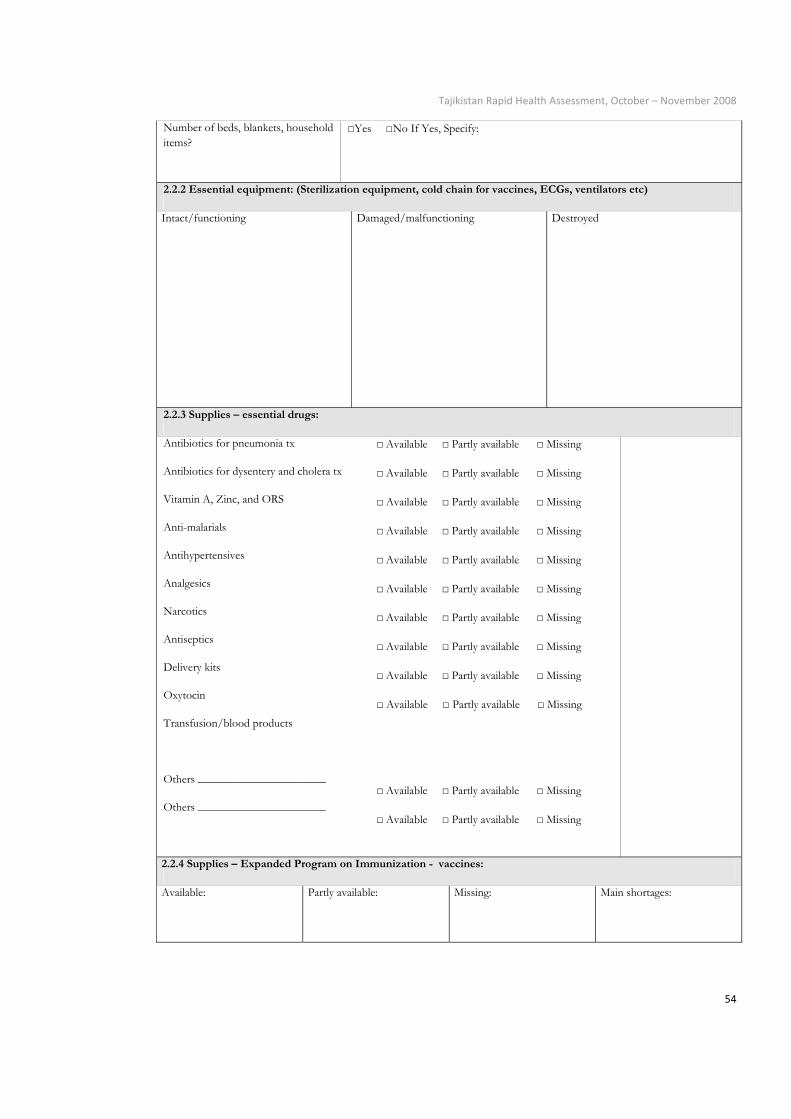
Tajikistan Rapid Health Assessment, October – November 2008
54
Number of beds, blankets, household items?
□Yes □No If Yes, Specify:
2.2.2 Essential equipment: (Sterilization equipment, cold chain for vaccines, ECGs, ventilators etc)
Intact/functioning
Damaged/malfunctioning Destroyed
2.2.3 Supplies – essential drugs:
Antibiotics for pneumonia tx
Antibiotics for dysentery and cholera tx
Vitamin A, Zinc, and ORS
Anti-malarials
Antihypertensives
Analgesics
Narcotics
Antiseptics
Delivery kits
Oxytocin
Transfusion/blood products
Others ______________________
Others ______________________
□ Available □ Partly available □ Missing
□ Available □ Partly available □ Missing
□ Available □ Partly available □ Missing
□ Available □ Partly available □ Missing
□ Available □ Partly available □ Missing
□ Available □ Partly available □ Missing
□ Available □ Partly available □ Missing
□ Available □ Partly available □ Missing
□ Available □ Partly available □ Missing
□ Available □ Partly available □ Missing
□ Available □ Partly available □ Missing
□ Available □ Partly available □ Missing
2.2.4 Supplies – Expanded Program on Immunization - vaccines:
Available:
Partly available: Missing: Main shortages:

Tajikistan Rapid Health Assessment, October – November 2008
55
2.2.5 Supplies – consumables (e.g. syringes, dressing material):
□ Available
□ Partly available □ Missing
Main shortages:
2.2.6 Human Resources
Physicians Main Shortages:
Nurses
Auxiliary Staff
Observations: Present external support with resources
2.3. PERFORMANCE
Quality Indicators
2.3.3. Standardised case management (case definition, treatment protocol for e.g. for malaria, IMCI, DOTs):
Case definition
□ Yes □ No
Malaria
□ Yes □ No
IMCI
□ Yes □ No
DOTs
□ Yes □ No
Other: ___________
□ Yes □ No
2.3.4. Referral mechanism:
□ Defined/Regular
□ Ad hoc/Irregular
□ None
2.3.5. Quality of outpatient registers and inpatient records
□ Satisfactory
□ To be improved
□ Substandard/Missing

Tajikistan Rapid Health Assessment, October – November 2008
56
2.3.6. Quality of drug management system (storage and record keeping):
□ Satisfactory
□ To be improved
□ Substandard/Missing
2.3.7 General hospital hygiene and sanitation:
Hand washing
□ Satisfactory
□ To be improved
□ Substandard
Sharps disposal
□ Satisfactory
□ To be improved
□ Substandard
Disinfection of equipment
□ Satisfactory
□ To be improved
□ Substandard
2.3.8 Disaster preparation:
Plan on‐site
□ Yes
□ No
□ Date (mm/yy): _____________
Evacuation plan
□ Yes
□ No
□ Date (mm/yy): _____________
□ Last practiced
(mm/yy): _______________
2.3.8 Observations :

Tajikistan Rapid Health Assessment, October – November 2008
57
2.4 FUNCTIONING OF SUB-SECTORS AND SERVICES
Sub-sectors and services
Normal DecreasedNot functioning
Does not apply
Other Observations :
2.4.1
General clinic services (outpatient and, where applicable inpatient
services, referral capacity) □ □ □ □
2.4.2
Child health (EPI, IMCI trained staff)
□ □ □ □
2.4.3
Nutrition (Management of moderate and acute malnutrition)
□ □ □ □
2.4.4
Infectious Disease
Communicable diseases (early warming for epidemics, TB, malaria, other locally prevalent conditions)
□ □ □ □
2.4.4a STI and HIV/AIDS (standard precautions, free condoms, VCT, PMTCT, ART)
□ □ □ □
2.4.5
Surgery □ □ □ □
2.4.6 Obstetrics and Gynecology:
- Maternal and newborn health
- Family planning and antenatal care
□ □ □ □
2.4.7
Sexual violence (clinical management of rape, emergency contraception, post exposure prophylaxis for STI and HIV)
□ □ □ □
2.4.8
Non-communicable diseases
Trauma
□ □ □ □

Tajikistan Rapid Health Assessment, October – November 2008
58
Cardiology
Endocrinology
2.4.9
Environmental health (health facility waste disposal)
□ □ □ □
2.4.10
Mental health (e.g., clinical care of pre-existing psychosis, severe depression, epilepsy; basic supports for people with acute emergency-induced anxiety)
□ □ □ □
2.4.11 Anaesthesia and Critical care □ □ □ □
2.4.12 Radiology/X-Ray □ □ □ □
2.4.13 Dispensary/Pharmacy □ □ □ □
2.4.14 Laboratory Services: Biochemistry/ Haematology/ Microbiology
□ □ □ □ Service 24/7 ‐ □Yes □No
2.4.15 Comments on sub-sectors and services: